Embed Size (px)
Citation preview

Psychopharmacology 1
Anti Psychotic ,
Mood Stabilizer
DR SEDDIGH

Classes of psychotropic medication
Antipsychotic medications Mood-stabilizing drugs Anti-anxiety medications Antidepressant medications Psychostimulants

Antipsychotic
medications

Antipsychotics:Diagnostic Indications
Psychiatric Schizophrenia Schizoaffective disorder Mood disorders with psychosis Delusional disorder
Nonpsychiatric Dementia/Delirium Psychosis secondary to a nonpsychiatric medical disorder Developmental disability with psychosis and/or aggression Tourette’s disorder Nausea, vomiting
4

Antipsychotic Agents
Antipsychotic agents have two major groupsConventional antipsychotics
Block dopamine receptors
Atypical antipsychotics
Moderate blockade of dopamine receptors

ANTIPSYCHOTICS
Pre-90’s– “Typical”, conventional, traditional neuroleptics,
major tranquilizors– Modeled on D2 antagonism– EPS/TD
Post-90’s– “Atypical”, novel, 2nd generation– Modeled on 5-HT2/D2 antagonism– Less EPS, prolactin effects– Weight gain, sedation, diabetes


Impact of antipsychotics..

Conventional Antipsychotic Agents Classification
– Low potency-Thioridazine– Medium potency-perphenazine– High potency-Halopridol
Mechanism of Action– Block receptors of dopamine, acetycholine,
histamine, norepinephrine

Typical antipsychotics– Phenothiazines
• e.g. chlorpromazine, fluphenazine, thioridazine
– Butyrophenones • e.g. haloperidol, droperidol
– Thioxanthines• e.g. chlorprotixen, thiothixene
Atypical antipsychotics
Clozapin
Risperidone
Olonzapin
Sertindole
Quetiapine
Classification of antipsychotic drugs

Overview of Antipsychotics
Conventional AntipsychoticsChem. Group Generic Name Trade Mark Dose (mg)
Phenothiazines
chlorpromazine LARGACTIL, MEGAPHEN,
200-800
thioridazine MELLERIL 100-600

Overview of Antipsychotics
Conventional AntipsychoticsChem. Group Generic Name Trade Mark Dose (mg)
Phenothiazines
Perphenazine PERFENAZIN, TRILAFON, PERATSIN
16-24
Prochlorperazine PROCHLORPERAZIN, STEMETIL
20-80
Fluphenazine MODITEN 2-16
trifluoperazine STELAZIN 10-50
Thioxanthenes flupenthixol FLUANXOL 6-18
Butyrophenoneshaloperidol HALOPERIDOL,
HALDOL, APO-HALOPERIDOL
2,5-10
melperone BURONIL 50-300
Diphenylbutylpiperidines
pimozide ORAP 2-10
fluspirilen IMAP 2-10
penfluridol SEMAP 2-60
Perathiepines oxyprothepin MECLOPIN 5-20

Antipsychotics of the 2nd Generation
Generic Name Trade Mark Dose (mg)
D2, D3 selective antagonists
sulpiride DOGMATIL, PROSULPIN 50-1200
amisulpride SOLIAN, DENIBAN 50-1200
SDA
risperidone RISPERDAL, RISPEN, RISPERDAL QUICKLET
4-8
ziprasidone ZELDOX 40-160
Sertindole SERDOLECT 12-20
MARTA
clozapine LEPONEX 200-600
olanzapine ZYPREXA i.m. inj. 10 mg 5-20
quetiapine SEROQUEL 300-600
zotepine ZOLEPTIL 75-300

Adverse Effects Summary
Sedation ‑ initially considerable; tolerance usually develops after a few weeks of therapy; dysphoria
Postural hypotension ‑ results primarily from adrenergic blockade; tolerance can develop
Anticholinergic effects ‑ include blurred vision, dry mouth, constipation, urinary retention; results from muscarinic cholinergic blockade
Endocrine effects ‑ increased prolactin secretion can cause galactorhea; results from antidopamine effect
Hypersensitivity reactions ‑ jaundice, photosensitivity, rashes, agranulocytosis can occur
Idiosyncratic reactions ‑ malignant neuroleptic syndromeWeight gain Neurological side effects - see next

REACTION FEATURES TIME OF MAXIMAL RISK
PROPOSED MECHANISM
TREATMENT
Acute dystonia Spasm of muscles of tongue, face, neck, back; may mimic seizures; not hysteria
1 to 5 days Unknown Antiparkinsonian agents are diagnostic and curative
Akathisia Motor restlessness; not anxiety or "agitation"
5 to 60 days Unknown Reduce dose or change drug: antiparkinsonian agents,b benzodiazepines or propranololc may help
Parkinsonism Bradykinesia, rigidity, variable tremor, mask facies, shuffling gait
5 to 90 days Antagonism of dopamine
Antiparkinsonian agents helpful
Neuroleptic malignant syndrome
Catatonia, stupor, fever, unstable blood pressure, myoglobinemia; can be fatal
Weeks; can persist for days after stopping neuroleptic
Antagonism of dopamine may contribute
Stop neuroleptic immediately: dantrolene or bromocriptined may help: antiparkinsonian agents not effective
Perioral tremor ("rabbit" syndrome)
Perioral tremor (may be a late variant of parkinsonism)
After months or years of treatment
Unknown Antiparkinsonian agents often help
Tardive dyskinesia
Oral-facial dyskinesia; widespread choreoathetosis or dystonia
After 6 months or years of treatment (worse on withdrawal)
Excess function of dopamine hypothesized
Prevention crucial; treatment unsatisfactory
a. Many drugs have been claimed to be helpful for acute dystonia. Among the most commonly employed treatments are diphenhydramine hydrochloride, 25 or 50 mg intramuscularly, or benztropine mesylate, 1 or 2 mg intramuscularly or slowly intravenously, followed by oral medication with the same agent for a period of days to perhaps several weeks thereafter. b. For details regarding the use of oral antiparkinsonian agents, see the rest of slides c. Propranolol often is effective in relatively low doses (20-80 mg per day). Selective beta1-adrenergic receptor antagonists are less effective. d. Despite the response to dantrolene, there is no evidence of an abnormality of Ca2+ transport in skeletal muscle; with lingering neuroleptic effects, bromocriptine may be tolerated in large doses (10-40 mg per day).
Neurological Side Effects of antipsychotics

Phenothiazines - Side effects
Weight gain – 40% - weight gain now attributed to ratio of binding to D2 and 5-HT2 receptors; possibly also histamine (for newer antipsychotics anyway)
Sexual dysfunction
• result from NE and SE blockade
• erectile dysfunction in 23-54% of men
• retrograde ejaculation in
• loss of libido and anorgasmia in men and women
Seizures - <1% for generalized grand mal

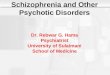
ESTIMATED MEAN WEIGHT GAIN AT 10 WEEKS ESTIMATED MEAN WEIGHT GAIN AT 10 WEEKS
Placeb
o
Placeb
o
Moli
ndon
e
Moli
ndon
e
Zipras
idone
Zipras
idone
Fluphe
nazin
e
Fluphe
nazin
e
Halope
ridol
Halope
ridol
Non-p
harm
cont
rol
Non-p
harm
cont
rol
Risper
idone
Risper
idone
Chlorp
rom
azine
Chlorp
rom
azine
Sertin
dole
Sertin
dole
Thiorid
azine
Thiorid
azine
Olanza
pine
Olanza
pine
Clozap
ine
Clozap
ine
00
11
22
33
44
55
-1-1Mea
n c
han
ge in
bo
dy w
eigh
t (kg
)M
ean
cha
nge
in b
ody
wei
ght (
kg)

Phenothiazines - Side effects
Neuroleptic malignant syndrome (1-2% early in trt)
• combination of motor rigidity, hyperthermia, and autonomic dysregulation of blood pressure and heart rate (both go up)
• can be fatal in 5-20% of cases if untreated
• treatment – discontinue meds; give trts for fever and cardiac problems

Sensitivity to sun
• some phenothiazines collect in skin (chlorpromazine)
• sunlight causes pigmentation changes – grayish-purple splotching (look bruised)
• can also occur in eye and cause brown in cornea(chlorpromazine) and retin (thioridazine)
•
Jaundice – elevated bilirubin in liver - < ½%

Limitations Of Conventional Antipsychotics
Approximately one-third of patients with schizophrenia fail to respond
Limited efficacy against– Negative symptoms– Affective symptoms– Cognitive deficits
High proportion of patients relapse
Side effects and compliance issues

Antipsychotic Drugs – New Generations „atypical“
clozapine risperidone olanzapine sertindole quetiapine etc.

Atypical antipsychotics
MARTA (multi acting receptor targeted agents) clozapine, olanzapine, quetiapine
SDA (serotonin-dopamine antagonists) risperidone, ziprasidone, sertindole
Selective D2/D3 antagonists sulpiride, amisulpiride

Clozapine (1989)
Selectively blocks dopamine D2 receptors, avoiding nigrostriatal pathway
Also blocks NE
More strongly blocks 5-HT2 receptors in
Among non-responders to first generation meds
or those who cannot tolerate side effects, about 30% do respond to Clozapine

Clozapine
Extrapyramidal side effects are minimal
May help treat tarditive dyskinesia
Still shows orthostatic hypotension effects, sedation, weight gain, increased heart rate
Increased risk for seizures (2-3%)
Agranulocytosis in 1%
Agranulocytosis risks increase when co-administered with carbamazepine
Interactions with SSRIs and valproic acid increase Clozapine levels and risks

Risperidone (Risperdal; 1994)Fewer side effects than Clozapine
Marketed as first line approach to treatment
Blocks selective D2, norepinephrine, and 5-HT2
Argued as effective for positive and negative symptoms (controversial)
Extrapyramidal side effects low (but are shown at high doses) - controversial
Shares sedation, weight gain, rapid heart beat, orthostatic hypotension, and elevated prolactin
No agranulocytosis risks
May cause anxiety/agitation (possible OCD)

Olanzipine - Zyprexa – 1996
• Same poorly supported arguments about improved negative symptom reduction
• Argued to be better than risperidone in extrapyramidal issues
• Does not cause prolactin elevation
•

Sertindole – Serlect – 1995
• concern about sudden cardiac death or episodes due to cardiac arrhythmia led to its voluntary removal in 1998
Quetiapine – Seroquel - 1997
in IranZiprasidone – 2001
Similar to advantages of others, but argued not to cause weight gain

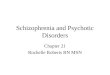
HaloperidolHaloperidol ClozapineClozapine RisperidoneRisperidone OlanzapineOlanzapine
QuetiapineQuetiapine ZiprasidoneZiprasidone
5HT2A D2 D1 Alpha 1 Musc H1 5HT1A (agonist)
Casey 1994Casey 1994
Atypical Antipsychotics In Vivo Binding Affinities

Mood StabilizersMood Stabilizers

Mood StabilizersMood Stabilizers
LithiumLithium AnticonvulsantsAnticonvulsants
– Valproic Acid [Depakote]Valproic Acid [Depakote]– Carbamazepine [Tegretol]Carbamazepine [Tegretol]– New Anticonvulsants (?):New Anticonvulsants (?):
• Lamotrigine [Lamictal]Lamotrigine [Lamictal]• Topiramate [Topamax]Topiramate [Topamax]• Gabapentin [Neurontin]Gabapentin [Neurontin]

LithiumLithium

Lithium: HistoryLithium: History Used since mid-XIX: gout, diabetes...Used since mid-XIX: gout, diabetes... For BP since 1960’s, FDA ‘74For BP since 1960’s, FDA ‘74 Effective Antimanic, mood stab, BP depr.Effective Antimanic, mood stab, BP depr. If Discontinued relapse near 100% 2 yrIf Discontinued relapse near 100% 2 yr Therapeutic Levels:Therapeutic Levels: 1-1.5 mEq/ml 1-1.5 mEq/ml Acute maniaAcute mania 0.4-0.8 mEq/ml 0.4-0.8 mEq/ml MaintenanceMaintenance
0.3-0.8 0.3-0.8 mEq/ml mEq/ml in elderlyin elderly
– Narrow therapeutic indexNarrow therapeutic index

Lithium: PharmacologyLithium: Pharmacology
Not Not liver liver metabolized. metabolized. KidneyKidney excreted excreted Not Not proteinprotein bound bound 70-80% reabsorb prox Tubule, 70-80% reabsorb prox Tubule,
Na (dehydr, thiazide diuret) Na (dehydr, thiazide diuret) Li levelLi level ExcretionExcretion related to GFR: related to GFR:elder elder pregpreg Half-lifeHalf-life 24 hrs (HS), steady state 5 days 24 hrs (HS), steady state 5 days Peak LevelsPeak Levels 2 hrs, SR 4-4.5 2 hrs, SR 4-4.5
– fast release: N/V, slow rel: diarrheafast release: N/V, slow rel: diarrhea

Predictors: Good Li ResponsePredictors: Good Li Response
Past Li response (personal or family)Past Li response (personal or family) Euphoric, pure (classic) mania Euphoric, pure (classic) mania Sequence Mania-Depr-EuthymiaSequence Mania-Depr-Euthymia No psychosisNo psychosis No Rapid CyclingNo Rapid Cycling

Predictors: Poor Li ResponsePredictors: Poor Li Response[Good response to anticonvulsants][Good response to anticonvulsants]
Mixed mania (adolescents)Mixed mania (adolescents) Irritable maniaIrritable mania Secondary mania (geriatric)Secondary mania (geriatric) Psychotic SxPsychotic Sx Rapid CyclingRapid Cycling Depression-Mania-EuthymiaDepression-Mania-Euthymia Comorbid substance abuseComorbid substance abuse

Lithium: Lithium: CommonCommon Side Effects Side Effects
GI distressGI distress Polyuria / polydipsiaPolyuria / polydipsia Sedation-lethargySedation-lethargy Cognitive (memory, concentr, slow)Cognitive (memory, concentr, slow) Wt. GainWt. Gain Poor coordination, tremorPoor coordination, tremor Skin (worse acne)Skin (worse acne)

Lithium: Lithium: SeriousSerious SE SE Renal Renal
– nephrogenic diabetes insipidusnephrogenic diabetes insipidus– tubular interstitial nephritistubular interstitial nephritis
HypothyroidismHypothyroidism Psoriasis (onset or worsening)Psoriasis (onset or worsening) Cardiac: EKG flat T, SA dysfx, Cardiac: EKG flat T, SA dysfx,
tachicardiatachicardia Li ToxLi Tox. N/V/D, delirium, ataxia, stupor. N/V/D, delirium, ataxia, stupor
– Tx dyalisis if >3.0, correct fluid-electrolitesTx dyalisis if >3.0, correct fluid-electrolites

Li: Interactions & UseLi: Interactions & Use
Li levels: Li levels: • diuretics, diuretics, • NSAIDs (ASA, sulindac OK)NSAIDs (ASA, sulindac OK)• ACE-inhibitorsACE-inhibitors
Starting:Starting:– Baseline Renal, TFT, HCG, EKG >40yo, Baseline Renal, TFT, HCG, EKG >40yo,
UA, weight, medical Hx UA, weight, medical Hx – 300-600 mg/day divided doses300-600 mg/day divided doses– Levels in 5 daysLevels in 5 days– Increase 900-1200 mg/day Increase 900-1200 mg/day

Valproate NAValproate NA

Valproate [Depakote]Valproate [Depakote]
FDA Sz ‘78, BP ‘96FDA Sz ‘78, BP ‘96 Effective antimanic, BP depressionEffective antimanic, BP depression Therapeutic effect 2 d. level 50-125 Therapeutic effect 2 d. level 50-125
mg/lmg/l– oral loading 20-30 mg/kg/dayoral loading 20-30 mg/kg/day
Mixed, rapid cycling, schizoaffectiveMixed, rapid cycling, schizoaffective Closed had injury, EEG abnormalityClosed had injury, EEG abnormality

VPA: VPA: CommonCommon Side Effects Side Effects GI distressGI distress SedationSedation Liver transaminase elevationLiver transaminase elevation TremorTremor Hair lossHair loss Weight gain-increased appetiteWeight gain-increased appetite Thrombocitopenia (eldersThrombocitopenia (elders) Teratogenic: neural tube, cranio-facial

VPA: VPA: LessLess Common SE Common SE
NeutropeniaNeutropenia Coagulopathies, Coagulopathies, platelet Functionplatelet Function endocrine abnormalitiesendocrine abnormalities
– Amenorrhea, policystic ovary?Amenorrhea, policystic ovary?– HypothyroidismHypothyroidism– HypocortisolemiaHypocortisolemia

VPA: VPA: Rare DangerousRare Dangerous SE SE Idiosincratic Hepatic FailureIdiosincratic Hepatic Failure
– lethargy, anorexia, N/V, jaund, bleed, edemalethargy, anorexia, N/V, jaund, bleed, edema– Risk: <3 y.o., many anticonvuls, Dev. DelayRisk: <3 y.o., many anticonvuls, Dev. Delay– Remote risk in >10yo psychiatric patientsRemote risk in >10yo psychiatric patients
Acute Hemorrhagic PancreatitisAcute Hemorrhagic Pancreatitis - Eatly 6 month,serum amylase level- Eatly 6 month,serum amylase level Bone Marrow SupressionBone Marrow Supression

VPA UseVPA Use Baseline:Baseline:
– Medical Hx, CBC-diff, LFT (LDH, SGOT, Medical Hx, CBC-diff, LFT (LDH, SGOT, SGPT, bili, Alk. Phos, GGT), HCG, SGPT, bili, Alk. Phos, GGT), HCG, PT,PTT if bleeding abnorm, amylase?PT,PTT if bleeding abnorm, amylase?
– Warn about hepatic, pancreatic, Warn about hepatic, pancreatic, hematologic, teratogenic riskshematologic, teratogenic risks
Monitor LFT, CBCMonitor LFT, CBC

CarbamazepineCarbamazepine

Carbamazepine [Tegretol]Carbamazepine [Tegretol]
FDA Trig Neuralg ‘68, TLE ‘74FDA Trig Neuralg ‘68, TLE ‘74 Effective antimanic, Tx-refract DeprEffective antimanic, Tx-refract Depr Onset 2 wks, antidepr 4-6 wkOnset 2 wks, antidepr 4-6 wk Ther. Levels: 4-12Ther. Levels: 4-12 Half life decreases to 12-17 hrsHalf life decreases to 12-17 hrs
– p450 liver inductionp450 liver induction

CBZ: Side EffectsCBZ: Side Effects
Less cognitive probl than LiLess cognitive probl than Li Less Wt gain, hair loss, tremor than VPALess Wt gain, hair loss, tremor than VPA Neuro: Diplopia,blurr vision, fatigue/sedNeuro: Diplopia,blurr vision, fatigue/sed GI: Naus/diarr, Dry mouthGI: Naus/diarr, Dry mouth Leukopenia, thrombocitopenia, rashLeukopenia, thrombocitopenia, rash LFTLFT Agranulocytosis (, Liver fail, pancreatitis, Agranulocytosis (, Liver fail, pancreatitis,
Stevens-JohnsonStevens-Johnson (exfol skin), (exfol skin), neuroteratogenicneuroteratogenic

CBZ: UseCBZ: Use Baseline: Medical Hx, CBC+diff,LFT, Baseline: Medical Hx, CBC+diff,LFT,
Renal, TFT, HCG, ferritinRenal, TFT, HCG, ferritin Start low:Start low:
– 100-400 mg/day, 100-400 mg/day, 100-200 mg every several days, bid 100-200 mg every several days, bid
(occasionally qd)(occasionally qd) Follow CBC, LFTFollow CBC, LFT
– clinical monitoring more effective than clinical monitoring more effective than labslabs

And Others …And Others … New AnticonvulsantsNew Anticonvulsants
• LamotrigineLamotrigine: ?Effective BP & depr, : ?Effective BP & depr, 10%rash, levels 10%rash, levels by CBZ, by CBZ, by VPAby VPA
• TopiramateTopiramate: wt loss, 1.5% renal stones: wt loss, 1.5% renal stones• GabapentinGabapentin: effective?? (open reports, add-: effective?? (open reports, add-
on)on)• TiagabineTiagabine, , VigabatrilVigabatril Ca Ca
Others:Others:• Ca-channelCa-channel blockers blockers• TamoxifenTamoxifen Prot Kinase-C inhibitor Prot Kinase-C inhibitor

THANKS FOR YOUR ATTENTION