Embed Size (px)
Citation preview

Psychological Disorders

• U – njustifiable• M – aladaptive• A – typical• D – istorted thinking, • D-isturbed

•Qualitatively
•Quantitatively

Etiology
• Psychoanalytic theory• Humanistic theory• Behavioral theory• Cognitive theory• Psychophysiological • Cultural

Classifying Psychological Disorders
• DSM IV TR– Classification orders and describes symptoms– Predicts its future course– Treatment– Stimulate research

Five Levels of Diagnosis
• Axis I: Is a clinical syndrome present?• Axis II: Is a personality disorder or mental
retardation present?• Axis III: General medical condition present?• Axis IV: Are psychosocial or environmental
problems present?• Axis V: What is the global assessment? 1-
100

Anxiety Disorders
- Most common disorder after substance abuse What differentiates phobias and normal fear?- Intensity- Length of anxiety- Able to adequately respond

Anxiety Disorders
• Generalized anxiety disorder – continuously tense
• Phobic disorder – irrational and intense fear of object
• Obsessive compulsive disorder – repetitive thoughts or actions
• Panic disorder – anxiety tornado– “fear of fear”, sudden episodes
• Post traumatic stress disorder – after trauma

• Panic Disorder:• Minute-long episodes of intense dread
which may include feelings of terror, chest pains, choking, or other frightening sensations.
• Anxiety is a component of both disorders (generalized anxiety disorder and panic disorder). It occurs more in the panic disorder, making people avoid situations that cause it.

• Post-traumatic stress disorder (PTSD)– Affects soldiers from Vietnam, Operation Desert
Storm, and Iraqi wars; also Nazi death camp and prison camp survivors)
– Suffering severe reactions years after traumatic event (some recover, some get worse over time)
– Experiences include: • Dreams with horror• Intense emotional bodily reactions• Difficulty concentrating or sleeping

Stressors Causing PTSD
• Combat-related events
• Sudden death of loved one
• Involved in or witnessing accidents
• Physical assault, rape, sexual molestation experienced by women
• Terrorism experiences
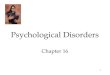
Who Develops PTSD
• Four factors involved•
– Severity of stress• Risk increased when physical injury occurs
– Person’s characteristics before event• Affects those with higher anxiety levels, lower
intelligence, previous mental health problems
– Social support• More support lessens risk
– Sex of the victim• Women more at risk

Etiology of Anxiety Disorders• Psychoanalytic –
– GAD – id overcomes ego => anxiety – Phobias – Little Hans– OCD – fixated an anal stage
• Behavioral – classical conditioning, modeling, reinforcement– Little Albert
• Humanistic – gap between one’s real self and ideal self• Cognitive – misinterpret bodily sensations, lack ability to cope with stress• Biomedical
– genetic predisposition, - Lower levels of GABA neurotransmitter – inhibitory “brakes of a car”- Malfunctions in amygdala – part of brain that deals with agression and fear
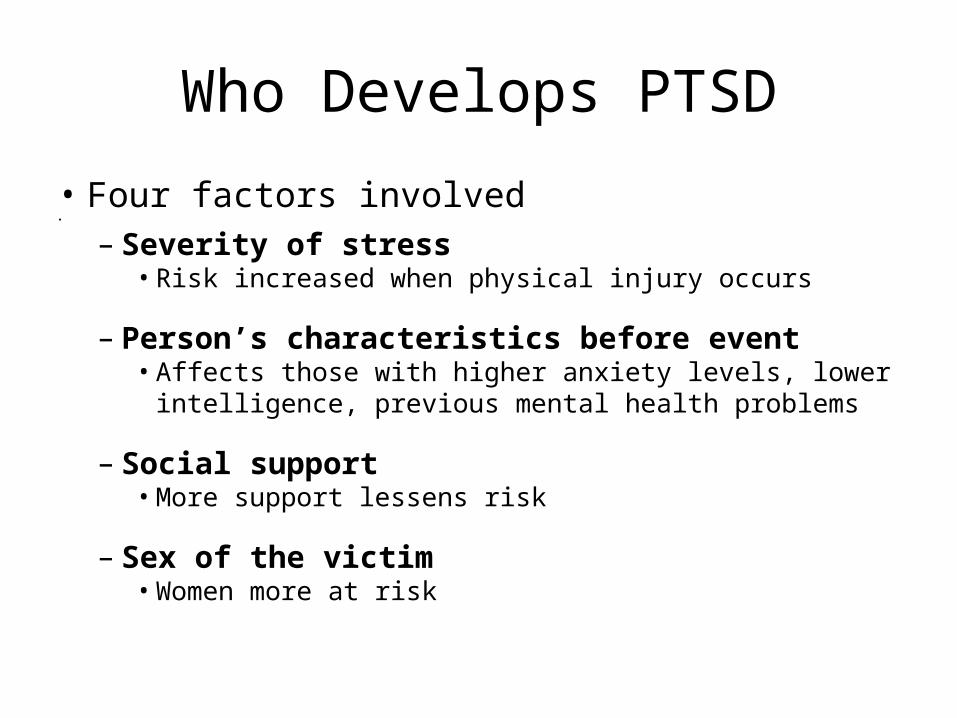
Kinds of Phobias- Intense, unrealistic or irrational fear
Phobia of blood.Hemophobia
Phobia of closed spaces.
Claustrophobia
Phobia of heights.Acrophobia
Phobia of open places.
Agoraphobia
Phobias
• Agoraphobia – fear of panic attacks in public places
• Social phobias – social anxiety disorders– More women than men– Irrational fear of being embarrassed, judged or
critically evaluated by others– Realize that their fear is excessive but they still
approach social situations with tremendous anxiety

Phobias• More unusual phobias:
– Amathophobia- fear of dust– Amenophobia – fear of wind– Aphephobia – fear of being touched by another person– Bibliophobia- fear of books– Catotrophobia – fear of breaking a mirror– Ergophobia – fear of work or responsibility– Gamophobia – fear of marriage– Hypertrichophobia – fear of growing excessive amounts of body hair– Levophobia – fear of things being on the left side of your body– Phobophobia – fear of acquiring a phobia– Phonophobia – fear of sound of your own fource– Triskaidekaphobia – fear of the number 13

Phobias
– Humans are predisposed – biologically prepared to acquire certain fears
• Fear of particular situations – flying, driving, tunnels, bridges, elevators, crowds, enclosed places
• Fear of features of the natural environment – thunder, heights, water
• Fear of injury or blood – injections, needles, medical or dental procedures
• Fear of animals and insects – snakes, spiders, dogs, slugs, bats

• Agoraphobia – fear of panic attacks in public places
• Social phobias – social anxiety disorders– More women than men– Irrational fear of being embarrassed, judged or
critically evaluated by others– Realize that their fear is excessive but they still
approach social situations with tremendous anxiety

Somatoform Disorders– Experiencing symptoms of physical health problems with
psychological causes, Symptoms take a somatic (bodily) form without apparent physical cause
• Four types– Hypochondriasis – preoccupation with health – Conversion disorders – symptoms not medically possible
• person experiences very specific genuine physical symptoms for which no physiological basis can be found
– Somatoform pain disorders – primary symptom is pain with no physical cause
– Body dysmorphic disorder - exaggerated concern and preoccupation about minor or imagined defects in appearance

Somatoform Disorders
– Symptoms take a somatic (bodily) form without apparent physical cause
Conversion disorder: person experiences very specific genuine physical symptoms for which no physiological basis can be found
Hypocondriasis: person interprets normal physical sensations as symptoms of a disease
Body dysmorphic disorder: exaggerated concern and preoccupation about minor or imagined defects in appearance

Disassociative Disorders
• Broad category of loosely related conditions– Conscious awareness becomes separated
(dissociated) from previous memories, thoughts, and feelings. People lose contact with portions of their consciousness or memory, resulting in disruptions in their sense of identity
– Dissociative amnesia – psychological cause
– Dissociative fugue – complete loss of memory
– Dissociative identity disorder – once known as multiple personality disorder; very controversial issue

Criticism of DID
• Critics argue that the diagnosis of DID increased in the late 20th century. DID has not been found in other countries.– Role-playing by people open to a
therapist’s suggestion.– Learned response that reinforces
reductions in anxiety

• Extreme and persistent feelings of despondency, worthlessness and
hopelessness, causing…
impaired emotional, cognitive, behavioral and physical
functioning
Mood Disorders
Chronic shortness of breathGasping for air after a hard
run
Major Depressive DisorderBlue mood
Mood Disorders
• Extreme and persistent feelings of despondency, worthlessness and
hopelessness, causing…
impaired emotional, cognitive, behavioral and physical functioning

Types of mood disorders
• Major depression – “common cold” of psychological disorders
• Dysthymic disorder • Seasonal affect disorder – depression
associated with seasons• Bipolar – emotional roller coaster• Cyclothymic Disorder - moderate mood
swings

Etiology of Mood Disorders
• Genetic predisposition• Disruptions in brain chemistry– Antidepressants – increase 2 neurotransmitters• Norepinephrine• Seratonin
– Lithium – regulates avaliability of NT called glutamate
• Stress
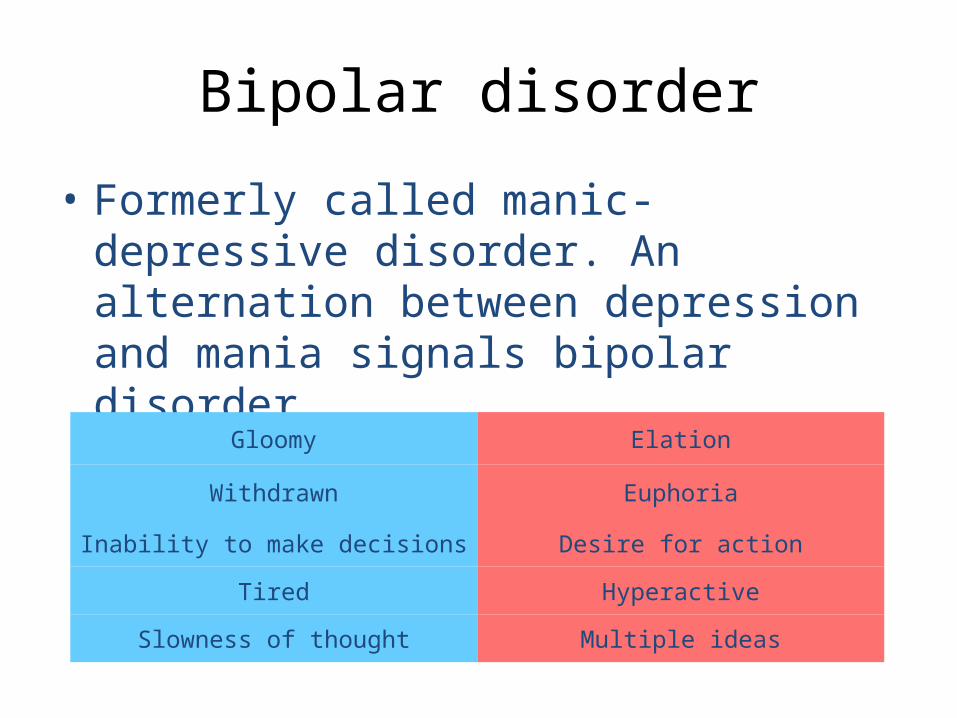
Bipolar disorder
• Formerly called manic-depressive disorder. An alternation between depression and mania signals bipolar disorder.
Multiple ideas
Hyperactive
Desire for action
Euphoria
Elation
Slowness of thought
Tired
Inability to make decisions
Withdrawn
Gloomy

Explaining Depression…
Cognitive BeckAttributions
Internal personal factors/external situational factorsStable or unstable over timeGlobal /specific implications
People who make global, stable, internal personal attribution => more prone to
depressionSeligman: learned helplessness
Depression is caused by person learning that his effort does not pay off “giving up behavior”
Originally conditioning => more cognitive slant

Etiology of Depression (con’t)• Cognitive
– Beck– Attributions
• Internal personal factors/external situational factors• Stable or unstable over time• Global /specific implications
People who make global, stable, internal personal attribution => more prone to
depression– Seligman: learned helplessness
• Depression is caused by person learning that his effort does not pay off “giving up behavior”– Originally conditioning => more cognitive slant

Etiology of Depression (con’t)
• Behavioral:– Inadequate social skills– Not enough reinforcement of social relationships– Depressed people can be depressing to be around

Social-Cognitive Perspective
• The social-cognitive perspective suggests that depression arises
partly from self-defeating beliefs and negative explanatory styles.

Disassociative Disorders
• People lose contact with portions of their consciousness or memory, resulting in disruptions in their sense of identity– Disassociatve amnesia– Disassociative fugue– Disassociatve Identity Disorder or Multiple
personality disorder

Schizophrenia
• “split mind” – split from reality– Disorganized thinking• Delusions -false beliefs, grandeur
– Disorganized perceptions• Hallucinations – sensory experiences without sensory
stimulation
– Inappropriate emotions or action• Laughing when inappropriate/flat affect

Subtypes of schizophrenia
• Paranoid• Disorganized• Catatonic• Undifferentiated

Schizophrenia
• “split mind” – split from reality– Disorganized thinking• Delusions -false beliefs, grandeur
– Disorganized perceptions• Hallucinations – sensory experiences without sensory
stimulation
– Inappropriate emotions or action• Laughing when inappropriate/flat affect

Schizophrenia
• Subtypes– Paranoid schizophrenia
• False beliefs, delusions (grandeur, paranoia, persecution), hallucinations
– Disorganized schizophrenia• Delusions, hallucinations, cognitive processes highly
disorganized or fragmented• Extreme social withdrawal
– Catatonic schizophrenia• May have delusions and hallucinations; most abnormalities in
social interaction, body posture and movement (waxy flexibility in stupors)

Schizophrenics have inappropriate symptoms (hallucinations,
disorganized thinking, deluded ways) that are not present in normal
individuals (positive symptoms). Schizophrenics also have an absence
of appropriate symptoms (apathy, expressionless faces, rigid bodies) that
are present in normal individuals (negative symptoms).
38
Understanding Schizophrenia
Schizophrenia is a disease of the brain exhibited by the symptoms of the mind.
Dopamine Overactivity: Researchers found that schizophrenic patients express higher levels of dopamine D4 receptors in
the brain.
Brain Abnormalities

39
Abnormal Brain Activity
Brain scans show abnormal activity in the frontal cortex, thalamus, and amygdala of
schizophrenic patients. Adolescent schizophrenic patients also have brain
lesions. Paul Thompson and Arthur W
. Toga, UCLA Laboratory of N
euro Im
aging and Judith L. Rapport, National Institute of M
ental Health

40
Abnormal Brain Morphology
Schizophrenia patients may exhibit morphological changes in the brain like
enlargement of fluid-filled ventricles.
Both Photos: Courtesy of Daniel R. W
einberger, M.D., N
IH-N
IMH
/ NSC

41
Viral Infection
Schizophrenia has also been observed in individuals who contracted a viral
infection (flu) during the middle of their fetal development.

42
Genetic Factors
The likelihood of an individual suffering from schizophrenia is 50% if their
identical twin has the disease (Gottesman, 1991).
0 10 20 30 40 50Identical
Both parents
Fraternal
One parent
Sibling
Nephew or niece
Unrelated

43
Genetic Factors
The following shows the prevalence of schizophrenia in identical twins as seen
in different countries.

44
Psychological Factors
Psychological and environmental factors can trigger schizophrenia if the individual
is genetically predisposed (Nicols & Gottesman, 1983).
Genain Sisters
The genetically identical Genainsisters suffer from schizophrenia. Two more than others, thus there are contributing environmental
factors.Courtesy of G
enain Family

45
Personality Disorders
Personality disorders are
characterized by inflexible and
enduring behavior
patterns that impair social
functioning. They are usually
without anxiety, depression, or
delusions.
• Schizoid personality disorder– Blunted emotions, social
withdrawal, but no serious cognitive disturbances
• Antisocial personality disorder– Feel little guilt, exploit
others, frequent violation of social rules and laws
– Difficulty with personal relationships
– Low tolerance for frustration, lie easily/skillfully

Personality Disorders
• Inflexible, maladaptive patterns of thoughts, emotions, behavior and interpersonal functioning that are stable over time and across situations, and deviate from the expectations of the individual’s culture
• Person doesn’t consider his personality characteristics as problematic => don’
Types of Personality Disorders
•Paranoid Personality Disorder
•Schizoid Personality Disorder
•Schizotypal Personality Disorder
Odd, eccentric
•Antisocial Personality Disorder
•Borderline Personality Disorder
•Histrionic Personality Disorder
•Narcissistic Personality Disorder
Dramatic, emotional, erratic
•Avoidant Personality Disorder
•Dependent Personality Disorder
•Obsessive-Compulsive Personality Disorder
Anxious, fearful

48
Antisocial Personality Disorder
A disorder in which the person (usually men) exhibits a lack of conscience for wrongdoing, even toward friends and
family members. Formerly, this person was called a sociopath or psychopath.

49
Understanding Antisocial Personality Disorder
Like mood disorders and schizophrenia,
antisocial personality disorder has
biological and psychological
reasons. Youngsters, before committing a crime, respond with lower levels of stress
hormones than others do at their
age.

50
Understanding Antisocial Personality Disorder
PET scans of 41 murderers revealed reduced activity in the frontal lobes. In a follow-up study repeat offenders had 11%
less frontal lobe activity compared to normals (Raine et al., 1999; 2000).
Normal Murderer
Courtesy of Adrian Raine, U
niversity of Southern California

51
Understanding Antisocial Personality Disorder
The likelihood that one will commit a crime doubles when childhood poverty is
compounded with obstetrical complications (Raine et al., 1999; 2000).

52
Risk and Protective Factors
Risk and protective factors for mental disorders (WHO, 2004).

53
Risk and Protective Factors