Embed Size (px)
Citation preview

NS3132(NURSING SCIENCES XI)
MENTAL HEALTH NURSING
Psychiatric disorders of infancy,
childhood & adolescence
1 Prepared by:CherryF@5/2013

LEARNING OBJECTIVES
At the end of this lecture, students will be able to:
� briefly explain types of psychiatric disorders in infancy, childhood & adolescence.
� state signs & symptoms of various types of psychiatric disorders in infancy, childhood & adolescence.
� state causes or risk factors of psychiatric disorders in � state causes or risk factors of psychiatric disorders in infancy, childhood & adolescence.
� explain medical & psychological management of children with psychiatric disorders.
� explain nursing care plan for children with psychiatric disorders.
2 Prepared by:CherryF@5/2013

Disorders of
childhood & adolescence
Mental
retardation
Pervasive
developmental
disorders
Prepared by:CherryF@5/20133
Speech &
language
disorders
Disorders of
scholastic skills
Attention deficit
hyperactivity
disorder
Conduct disorder

TYPES CLINICAL FEATURES
MENTAL RETARDATION Below-average intellectual function, impaired learning, communication, interpersonal interactions, & inability to function independently
ATTENTION-DEFICIT HYPERACTIVITY
DISORDER
One of the most frequently encountered childhood-onset neuro-behavioural disorders in primary care settingsIt has defining features of inattention, over-activity & impulsivity
PERVASIVE DEVELOPMENTAL
DISORDERS
Collection of neuropsychiatric disorders in which the child manifests deficits in a broad range of developmental areas such as communication, social interactions, cognitive skills & behaviour
Prepared by:CherryF@5/20134
as communication, social interactions, cognitive skills & behaviour that often is stereotypical
SPEECH & LANGUAGE DISORDERS
Unable to produce speech sounds correctly or fluently, or has problems with his or her voice & in understanding others (receptive language), or sharing thoughts, ideas, and feelings completely (expressive language)
DISORDERS OF SCHOLASTIC SKILLS
Impairment of reading, spelling and arithmetical skills development
CONDUCT DISORDERPresent mainly with a repetitive & persistent pattern of behaviour that violates both the basic rights of others & major age-appropriate societal norms & rules

MENTAL RETARDATION
Prepared by:CherryF@5/20135

Mild retardation
• Develop social & communication skills during preschool years
• Only minimal sensorimotor problems
• Acquire academic skills up to approximately the sixth-grade level
• In adulthood, achieve social & vocational skills adequate for minimum self-support
• Require some level of supervision, guidance, & assistance
Moderate retardation
Prepared by:CherryF@5/20136
Moderate retardation
• Acquire some communication skills during early childhood & benefit from vocational training
• Seldom advance academically beyond second-grade level
• With moderate supervision, able to provide for their own personal care & learn to travel in familiar areas
• Problems in recognizing & acquiring socially correct interactions
• During adulthood, perform unskilled or semiskilled work & live & function in the community in supervised settings

Severe retardation
• Acquire little if any communicative speech during early childhood
• Sometimes learn to use basic communication & develop elementary self-care skills in the school-age period
• Benefit from learning to sight-read some survival words
• In adulthood, some are able to perform simple skills in closely supervised settings
Prepared by:CherryF@5/20137
Profound retardation
• Most also have an identified neurological condition such as cerebral palsy, sensory deficits, epilepsy, & other neurological disorders
• Have sensorimotor problems recognized in early childhood (poor head control, feeding problems, & inability to roll over)
• Require a highly structured setting with constant monitoring & assistance for the best possible development

PERVASIVE DEVELOPMENTAL
DISORDERS
Prepared by:CherryF@5/20138

DSM-IV-TR CRITERIA (2000)
(AUTISTIC DISORDER)
A. A total of six (or more) items from criteria 1, 2, and 3, with at least two from criterion 1 and one each
from criteria 2 and 3:
1. Qualitative impairment in social interaction, as manifested by at least two of the following:
a. Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression,
body postures, and gestures to regulate social interaction
b. Failure to develop peer relationships appropriate to developmental level
c. A lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by a
lack of showing, bringing, or pointing out objects of interests)
d. Lack of social or emotional reciprocity
Prepared by:CherryF@5/20139
2. Qualitative impairments in communication as manifested by at least one of the following:
a. Delay in, or total lack of, the development of spoken language (not accompanied by an attempt to
compensate through alternative modes of communication such as gesture or mime)
b. In individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation
with others
c. Stereotyped and repetitive use of language or idiosyncratic language
d. Lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental
level

3. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as
manifested by at least one of the following:
a. Encompassing preoccupation with one or more stereotyped and restricted patterns of
interest that is abnormal either in intensity or focus
b. Apparently inflexible adherence to specific, nonfunctional routines or rituals
c. Stereotyped and repetitive motor mannerisms (e.g. hand or finger flapping or twisting, or
complex whole-body movements)
d. Persistent preoccupation with parts of objects
Prepared by:CherryF@5/201310
B. The client shows delays or abnormal functioning in at least one of the following areas,
with onset before age 3 years:
(1) social interaction, (2) language as used in social communication, or
(3) symbolic or imaginative play
C. The disturbance is not better accounted for by Rett’s disorder or childhood disintegrative
disorder

Asperger’s Disorder
� Many similar features of autistic disorder:
�Self-injuries & aggressive behavior
�Impairment in social interaction
�Restricted, repetitive patterns of behavior, interests &
activities
Prepared by:CherryF@5/201311
� No clinically significant delays in language, cognitive
development, age-appropriate self-help skills, adaptive
behavior, or curiosity about environment
� Better long-term outcome than Autistic disorder

DISORDERS OF INFANCY OR
CHILDHOOD
Prepared by:CherryF@5/201312

DSM-IV-TR CRITERIA (2000)
(SEPARATION ANXIETY)
A. Developmentally inappropriate & excessive anxiety concerning separation from home or from
those to whom the individual is attached, as evidenced by 3 or more of the following:
1. Recurrent excessive distress when separation from home or major attachment figures occurs
or is anticipated
2. Persistent & excessive worry about losing or possible harm befalling major attachment
figures
3. Persistent & excessive worry that an untoward event will lead to separation from a major
attachment figure (e.g. getting lost or being kidnapped)
4. Persistent reluctance or refusal to go to school or elsewhere because of fear of separation
Prepared by:CherryF@5/201313
4. Persistent reluctance or refusal to go to school or elsewhere because of fear of separation
5. Persistent & excessive fear or reluctance to be alone or without major attachment figures at
home or without significant adults in other settings
6. Persistent reluctance or refusal to go to sleep without being near a major attachment figure or
to sleep away from home
7. Repeated nightmares with the theme of separation
8. Repeated complaints of physical symptoms (such as headaches, stomachaches, nausea, or
vomiting) when separation from major attachment figures occurs or is anticipated

DSM-IV-TR CRITERIA (2000)
(SEPARATION ANXIETY)
B. The duration of the disturbance is at least 4 weeks.
C. The onset is before age 18.
D. The disturbance causes clinically significant distress or impairment in social, academic
(occupational), or other important areas of functioning.
E. The disturbance does not occur exclusively during the course of a pervasive developmental
disorder, schizophrenia, or other psychotic disorder &, in adolescents & adults, is not better
accounted for by panic disorder with agoraphobia.
Prepared by:CherryF@5/201314

TIC DISORDERS
Prepared by:CherryF@5/201315

DSM-IV-TR CRITERIA (2000)
(TOURETTE’S DISORDER)
A. Both multiple motor & 1 or more vocal tics have been present at some time during the illness,
although not necessarily concurrently. (A tic is a sudden, rapid, recurrent non-rhythmic,
stereotyped motor movement or vocalization.)
B. The tics occur many times a day (usually in bouts (short period or sessions)) nearly every day
or intermittently throughout a period of more than 1 year, & during this period there was
never a tic-free period of more than 3 consecutive months.
C. The disturbance causes marked distress or significant impairment in social, occupational, or
Prepared by:CherryF@5/201316
C. The disturbance causes marked distress or significant impairment in social, occupational, or
other important areas of functioning.
D. The onset is before age 18.
E. The disturbance is not due to the direct physiologic effects of a substance (e.g., stimulants) or
a general medical condition (e.g., Huntington’s disease or post-viral encephalitis).

ATTENTION-DEFICIT AND DISRUPTIVE
BEHAVIORAL DISORDERS
Prepared by:CherryF@5/201317

DSM-IV-TR CRITERIA (2000)
(CONDUCT DISORDER)
A. A repetitive & persistent pattern of behavior in which the basic rights of others or major age-
appropriate norms or rules are violated, as manifested by the presence of 3 (or more) of the
following criteria in the preceding 12 months, with at least 1 criterion present in the preceding
6 months:
Aggression to people & animals:
1. Often bullies, threatens, or intimidates others
2. Often initiates physical fights
3. Has used a weapon that can cause serious physical harm to others (e.g., a bat, brick, broken
Prepared by:CherryF@5/201318
3. Has used a weapon that can cause serious physical harm to others (e.g., a bat, brick, broken
bottle, knife, gun)
4. Has been physically cruel to people
5. Has been physically cruel to animals
6. Has stolen while confronting a victim (e.g., mugging, purse snatching, extortion, armed
robbery)
7. Has forced someone into sexual activity

Destruction of property:
8. Has deliberately set fires with the intention of causing serious damage
9. Has deliberately destroyed others’ property (other than by setting fires)
Deceitfulness or theft:
10. Has broken into someone else’s house, building, or car
11. Often lies to obtain goods or favors or to avoid obligations (e.g., cons others)
12. Has stolen items of nontrivial value without confronting a victim (e.g., shoplifting, but
without breaking & entering; forgery)
Prepared by:CherryF@5/201319
Serious violations of rules:
13. Often stays out at night despite parental prohibitions, beginning before age 13 years
14. Has run away from home overnight at least twice while living in parental or parental
surrogate home (or once without returning for a lengthy period)
15. Is often truant from school, beginning before age 13 years

B. The disturbance in behavior causes clinically significant impairment in social, academic,
or occupational functioning.
C. If the individual is age 18 years or older, criteria are not met for antisocial personality
disorder.
Code based on age at onset:
Conduct disorder, childhood-onset type: Onset of at least 1 criterion characteristic of conduct
disorder before age 10 years
Conduct disorder, adolescent-onset type: Absence of any criteria characteristic of conduct
disorder before age 10 years
Conduct disorder, unspecified onset: Age at onset is not known
Prepared by:CherryF@5/201320
Conduct disorder, unspecified onset: Age at onset is not known
Specify severity:
Mild: Few if any conduct problems in excess of those required to make the diagnosis &
conduct problems cause only minor harm to others
Moderate: Number of conduct problems & effect on others intermediate between mild &
severe
Severe: Many conduct problems in excess of those required to make the diagnosis or conduct
problems cause considerable harm to others

DSM-IV-TR CRITERIA (2000)
(ATTENTION-DEFICIT / HYPERACTIVITY DISORDER)
A. Either criterion 1 or 2 is present:
1) 6 (or more) of the following symptoms of inattention have persisted for at least 6 months to a
degree that is maladaptive & inconsistent with developmental level:
INATTENTION
a) Often fails to give close attention to details or makes careless mistakes in schoolwork, work, or
other activities
b) Often has difficulty sustaining attention in tasks or play activities
c) Often does not seem to listen when spoken to directly
d) Often does not follow through on instructions & fails to finish schoolwork, chores, or duties in
Prepared by:CherryF@5/201321
d) Often does not follow through on instructions & fails to finish schoolwork, chores, or duties in
the workplace (not the result of oppositional behaviour or a failure to understand instructions)
e) Often has difficulty organizing tasks & activities
f) Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort (
such as schoolwork or homework)
g) Often loses things necessary for tasks or activities (e.g. toys, school assignments, pencils,
books, or tools)
h) Is often easily distracted by extraneous stimulus
i) Often forgetful in daily activities

2) 6 (or more) of the following symptoms of hyperactivity / impulsivity have persisted for at least 6
months to a degree that is maladaptive and inconsistent with developmental level:
HYPERACTIVITY
a) Often fidgets with hands or feet or squirms in seat
b) Often leaves seat in classroom or in other situations in which remaining seated is expected
c) Often runs about or climbs excessively in situations in which it is inappropriate (in adolescents
or adults, may be limited to subjective feelings of restlessness)
d) Often has difficulty playing or engaging in leisure activities quietly
e) Is often “on the go” or often acts as if “driven by a motor”
f) Often talks excessively
Prepared by:CherryF@5/201322
IMPULSIVITY
g) Often blurts out answers before questions have been completed
h) Often has difficulty awaiting turn
i) Often interrupts or intrudes on others (e.g. butts into conversations or games)

B. Some hyperactive-impulsive or inattentive symptoms that caused impairment were present
before age 7 years
C. Some impairment from the symptoms is present in 2 or more settings (e.g. at school [or work]
and at home).
D. There must be clear evidence of clinically significant impairment in social, academic, or
occupational functioning
Prepared by:CherryF@5/201323
E. The symptoms do not occur exclusively during the course of a pervasive developmental
disorder, schizophrenia, or other psychotic disorder and are not better accounted for by another
mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, or personality
disorder)

ADHD TYPES
COMBINED
TYPE
Prepared by:CherryF@5/201324
PREDOMINANTLY
INATTENTIVE
TYPE
PREDOMINANTLY
HYPERACTIVE-IMPULSIVE
TYPE

� Combined type:
� If both criteria A1 & A2 are met for the preceding 6 months
� Predominantly Inattentive type:
� If criterion A1 is met but criterion A2 is not met for the
preceding 6 months
Prepared by:CherryF@5/201325
� Predominantly Hyperactive-Impulsive type:
� If criterion A2 is met but criterion A1 is not met for the
preceding 6 months

ATTENTION-DEFICIT / HYPERACTIVITY
DISORDER....
Prepared by:CherryF@5/201326

OTHER DISORDERS….
Adolescent suicide
Youth violence
Prepared by:CherryF@5/201327
Adult disorders in children & adolescents• Substance abuse
• Depression
• Bipolar disorder
• Psychosis
• Anxiety disorders

Depression Substance abuse
Prepared by:CherryF@5/201328

Suicide Violence
Prepared by:CherryF@5/201329

Psychosis Anxiety
Prepared by:CherryF@5/201330

RISK FACTORS…
Events or circumstances during childhood
Events or circumstances during infancy & early childhood
Events or circumstances during preconception & prenatal period
Prepared by:CherryF@5/201331
Other risks affecting any age group
Events or circumstances during adolescence
Events or circumstances during childhood

Preconception & Prenatal
period Infancy & Early childhood
� Unwanted pregnancy or adolescence pregnancy
� Poor adaptation to pregnancy
� Risk for risky health behaviors during pregnancy & mental disorders
� Post-natal depression among new mother
� Limited skills & bonding in parenting or parents negative attitudes
� Separation from primary caregiver (parental absence or
Prepared by:CherryF@5/201332
� Malnutrition, low birth weight & certain micronutrient deficiencies
� Risky for brain development & may contribute to mental disorders
caregiver (parental absence or rejection)
� Maltreatment & neglect by caregivers
� Malnutrition or infectious diseases
� Affecting subsequent social & emotional development

Childhood Adolescence
� Negative experiences within the home or at school
o Family violence or conflict, negative life events (parental loss or abuse) & low sense of connection to schools or other learning environments (severe bullying, persistent beating)
� Peer pressure & media
influences
� Substance abuse
Lowered educational outcomes
Prepared by:CherryF@5/201333
� Poor socio-economic condition (poor housing or living conditions)
� Parents with mental illness or substance use disorder
� Affecting core cognitive & emotional skills
� Lowered educational outcomes
� More risky sexual behavior
� Heightened violence
� Contribute to mental disorders

Other risks…
� Racism or discrimination towards a particular group in society
� Cause social exclusion & economic adversity
� Socially-defined role, family violence & abuse towards women
� Substance abuse disorders in men
Prepared by:CherryF@5/201334
� Substance abuse disorders in men
� Exposure to violence, armed conflict & natural disasters
� Poverty & associated conditions of unemployment, low educational level,
deprivation & homelessness

MEDICAL MANAGEMENT
Many
medications
for adults are
also used for
children &
Stimulants
Antidepressants
Predominant classifications:
children &
adolescents
Prepared by:CherryF@5/201335
Antianxiety agents
Antipsychotics
Anticonvulsants

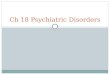
Management of ADHD (MOH, 2008)
Prepared by:CherryF@5/201336

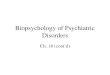
PHARMACOLOGICAL MANAGEMENT OF ADHD (MOH, 2008)
Prepared by:CherryF@5/201337

Medications for ADHD…
Stimulants
• Such as Methylphenidate [Ritalin, Concerta], Amphetamine salts [Adderall]
Noradrenergic Specific Reuptake Inhibitors (NSRIs)
• Such as Atomoxetine [Stratteral]
Prepared by:CherryF@5/201338
Adrenergic agents
• Such as Clonidine [Catapres]
Antidepressants
• Bupropion [Wellbutrin]
• Selective Serotonin Reuptake Inhibitors (SSRIs) such as Fluoxetine [Prozac]

Side effects of the medications….
• Hypertensive crisis may occur if combined or used within 14 days of MAOIs
• Abrupt withdrawal after prolonged use of high doses may
Stimulant / NSRIs
Prepared by:CherryF@5/201339
• Abrupt withdrawal after prolonged use of high doses may produce lethargy lasting for weeks
• Prolonged administration may inhibit growth
• Methyphenidate usage:• Increased risk of seizures
• Adverse changes in appetite, sleep, & levels of restlessness
• Develop new tics, exacerbation of previously existent mild tics
• Atomoxetine usage:• Increases suicidal thoughts in some children & adolescents

Side effects of the medications….
• Abrupt withdrawal may result in rebound hypertension
• Life-threatening elevations of BP with tricyclic antidepressants & beta-blockers
Adrenergic agents
Prepared by:CherryF@5/201340
• Central nervous system stimulants may potentiate action
New agent (Modafanil)

PSYCHOLOGICAL MANAGEMENT
• To develop positive peer communication & improve interpersonal relationships
• Enable the nurse to role model & teach new age-appropriate skills, reinforce positive behaviors & promote nurturing peer relationships
Group activities
Prepared by:CherryF@5/201341
positive behaviors & promote nurturing peer relationships
• The nurse will set limits in group play to promote safe environment & to demonstrate ways to show cooperation with & respect for peers
activities

• To enable the adolescent to develop interpersonal skills, give & accept feedback during communication with peers, practice more adult-like relationships, listen with empathy, achieve success, & learn appropriate ways to interact with the world
• It is normal for adolescents to question
Group activities
Prepared by:CherryF@5/201342
• It is normal for adolescents to question authority & test limits & rules• The nurse needs to establish rapport & a therapeutic alliance with them early in the course of treatment
• The nurse should maintain appropriate boundaries & not seek to behave as an adolescent or a friend to gain their acceptance
activities cont….

Behavior modification programs
• For the child approximately 3 to 11 years old
• A systematic & structured program that identifies developmental & age-appropriate goals that are observable & measurable within an established time frame
• Activities of daily living (ADLs), impulse control, & peer & sibling relationships
• A chart lists each goal, & the child is rewarded with stars, stickers, or colors to signify progress
Prepared by:CherryF@5/201343
Behavioral contract
• Often use for preadolescents & adolescents
• The contract emphasizes one to three goals that are more complex in nature e.g. will speak to others with respect
• Checkmark will be placed after each goal to signify accomplishment of the goal
• Rewards in the form of increased privileges e.g. later bedtime

• For the younger child
• Use recreational & creative play activities in relationships with peers & adults as they work to master new developmental tasks
• For expression of thoughts & emotions of the childTherapeutic
play
Prepared by:CherryF@5/201344
• The nurse observes & guides the child in play & interacts to modify distortions & reestablish healthy boundaries & safe limits as the child redefines behaviors through play
play

NURSING MANAGEMENT
Nursing Care PlanNursing Care Plan
Prepared by:CherryF@5/201345

Nursing assessment…
Thorough physical
assessment
• All body systems
Mental status examination
Alcohol & drug history
Prepared by:CherryF@5/201346
Developmental stage
Family life

Nursing diagnosis…
� All currently used NANDA-I nursing diagnoses are
applicable to children & adolescents
� SAFETY issues are most significant & a first priority
Prepared by:CherryF@5/201347
� Family problems & conflicts may be equally or more
relevant to consider than other client needs
� Ineffective role performance
� Impaired parenting
� Interrupted family processes

Nursing outcome examples…
Demonstrate a decrease or elimination of aggressive behaviors toward self & others.
Seek assistance & support from adults before losing self-control.
Identify triggers that provoke negative behavioral responses.
Client will….
Prepared by:CherryF@5/201348
Identify triggers that provoke negative behavioral responses.
Demonstrate age-appropriate relationships with adults.
Demonstrate age-appropriate relationships with peers.
Use age-appropriate play & recreational activities to express self.

Nursing interventions…
• To observe interactions.
Conduct a thorough assessment with the parents/guardians & the client & then assess them separately if appropriate.
• To ensure the client’s safety & to prevent harm to others.
Assess for the presence of suicidal ideation & for past aggressive behaviors including triggers to aggressive behavior.
Prepared by:CherryF@5/201349
• To prevent violence & maintain a safe environment.
Maintain a safe environment by continually assessing for contraband (objects that are sharp, alcohol, or illicit drugs) & being aware of any behavioral changes or signals that may indicate increasing anger or aggression.
• To ensure consistency & security.
Establish a therapeutic alliance & maintain appropriate boundaries.

Nursing interventions…
• To foster self-esteem, self-assurance, & confidence.
Help the client to identify strengths & positive qualities.
• To assist the client in developing & redefining successful & positive relationships.
Demonstrate, teach, & reinforce cooperative, respectful & positive behaviors.
Prepared by:CherryF@5/201350
• To promote a safe environment & to develop trust.
Set clear & consistent limits in a calm & nonjudgmental manner.
• To channel excess energy & to prevent escalation.
Redirect disruptive behavior with recreational activities.

Nursing interventions…
• To allow the client the opportunity to respond & to express feelings & cognitively process options.
Inform the client of the consequences for not adhering to the limits.
• To give the client time to deescalate in a quiet environment & process the event.
Use timeouts or quiet time when the client does not respond to limits.
Prepared by:CherryF@5/201351
• To explore & reinforce alternative methods of coping.
Role play situations that trigger aggressivity or self-mutilation or encourage alcohol or illicit drug use.
• To lessen the feelings of powerlessness & prevent future escalation.
Teach anger management techniques.

Nursing interventions…
• To encourage the client to express thoughts & feelings in alternative ways in the absence of adequate language & to reestablish healthy boundaries.
For younger child, initiate therapeutic play.
• To reinforce positive behaviors & to enhance self-esteem & sense of self-accomplishment.
Establish a behavior modification program for the preschool & the school-aged child that rewards the client for expressing self-safely.
Prepared by:CherryF@5/201352
accomplishment.
• To reinforce positive behaviors & to enhance self-esteem & independence.
Involve the adolescent in developing a behavioral contract by identifying expected behaviors & privileges.
• To assist the client in developing positive peer communication & to improve social skills & motor skills.
Engage the client in group therapy & recreational activities.

Nursing interventions…
• To promote self-esteem & to reinforce positive behaviors.
Provide positive feedback & recognition when the client adheres to the behavioral program & treatment plan.
Teach the parents/guardians about the disorder, the importance of consistency & structure, & the significance of medication compliance if indicated.
Prepared by:CherryF@5/201353
• To minimize guilt, increase the knowledge base about the disorder & realistic expectations & reinforce the consequences of medication noncompliance.
• To increase the parents ability to cope & minimize feelings of isolation & guilt.
Assess the parents/guardians for available support systems & refer to support groups & individual & family therapy as needed.

Nursing evaluation…
To determine the effectiveness of the treatment plan.
� Documents the treatment progress, as evidenced by actual outcomes.
Prepared by:CherryF@5/201354
outcomes.
� To be communicated with the interdisciplinary team members as well as the caregivers.
� May need treatment plan modification

REFERENCESTownsend, M.C. (2009). Psychiatric mental health nursing: Concepts of care in evidence based practice (6th ed.). U.S: F. A. Davies.
Perawatan penyakit jiwa Handbook. (n.d.). Sekolah Latihan, Hospital Bahagia, Ulu Kinta, Perak, Malaysia: Perawatan penyakit jiwa Handbook.
Sulaigah Baputty, Sabtu Hitam, & Sujata Sethi. (2008). Mental health nursing.Selangor, Malaysia: Oxford Fajar.
Prepared by:CherryF@5/201355
Fortinash, K.M., & Holoday Worret, P.A. (2008). Psychiatric mental health nursing(4th ed.). Missouri: Mosby Elsevier.
Ministry of Health. (2008). Clinical Practice Guidelines: Management of attention deficit and hyperactivity disorder in children and adolescents (MOH/P/PAK/173.08(GU)). Putrajaya: Malaysia. Ministry of Health.
Risks to mental health: An overview of vulnerabilities and risk factors [World Health Organization]. (2012). Retrieved May 16, 2013, from http://www.who.int/mental_health/mhgap/risks_to_mental_health_EN_27_08_12.pdf