Embed Size (px)
Citation preview

Pneumothorax
PST 421 – Cardiorespiratory Disorders and Rehabilitation
Miss Adebayo O.E

Pneumothorax
• Pneumothorax is defined as the presence of air in the pleural cavity (ie, the potential space between the visceral and parietal pleura of the lung), which can impair oxygenation and/or ventilation.
• If the air enters the pleural cavity, either from the outside (open pneumothorax) or from the lung (closed pneumothorax), the lung collapses and it becomes impossible for the person to breath, even if they have an open airway.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 2

The Pleural Space
The area between the two layers of pleuraVisceral pleura: covers the lungParietal pleura: lines the chest wall
The pleura space is normally filled with a small amount of fluid
PST 421 - Cardiorespiratory Disorders and Rehabilitation 3

Pneumothorax
• Pneumothorax may be classified as open or closed and as traumatic, spontaneous, or iatrogenic.
• Pneumothorax is classified as open or closed and according to the causative mechanism.
• Open pneumothorax results from a penetrating thoracic injury that permits entry of air into the chest
• closed pneumothorax is the accumulation of air originating from the respiratory system within the pleural space.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 4

Open Pneumothorax
• Open pneumothorax occurs when a wound on the chest is large enough to allow air to pass freely in and out of the pleural space.
• In this case the atmospheric pressure is in equilibrium with intrapleural pressure, blocking the lung inflation and alveolar ventilation.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 5

Types of pneumothorax
• Spontaneous • primary
• secondary
• Traumatic • blunt trauma
• penetrating wounds
• Iatrogenic
PST 421 - Cardiorespiratory Disorders and Rehabilitation 6

Iatrogenic pneumothorax
• Iatrogenic pneumothorax is in principle a traumatic pneumothorax that results from injury to the pleura, with air introduced into the pleural space secondary to diagnostic or therapeutic medical intervention.
• Risk of iatrogenic pneumothorax is 1.36% when performing invasive procedures like • Transthoracic lung biopsy
• Thoracentesis
• Cannulation of subclavian vein
• Mechanical ventilation
PST 421 - Cardiorespiratory Disorders and Rehabilitation 7

• Central venous catheter insertion
• Pacemaker implantation
• Transbronchial needle aspiration
• Laparoscopic surgery
PST 421 - Cardiorespiratory Disorders and Rehabilitation 8

Traumatic pneumothorax
• Traumatic pneumothorax results from blunt or penetrating chest trauma that disrupts the parietal or visceral pleura.
Main causes:
• Blunt chest trauma• Rib fractures• Rupture of the lung• Tracheobronchial rupture
• Penetrating chest injuriesStab woundGunshot injuryOther wounds
Oesophageal injuries
PST 421 - Cardiorespiratory Disorders and Rehabilitation 9

Spontaneous pneumothorax
• Spontaneous pneumothorax (SP) develops in people without an inciting event like trauma or underlying disease.
• Spontaneous pneumothorax can be further subdivided into: • Primary spontaneous pneumothorax • Secondary spontaneous pneumothorax
PST 421 - Cardiorespiratory Disorders and Rehabilitation 10

Primary spontaneous pneumothorax
• Primary spontaneous pneumothorax (PSP) occurs in people without underlying lung disease AND occurs most often in people between age 18 – 40
Risk Factors
• Smoking (risk of pneumothorax in healthy smoking male is 12% compared to 0.1% risk in non-smoker); risk is related to the intensity of smoking
• Young, tall, slim male (male female ratio 3-4 : 1) Mean age 28 years (range 13-67)
• Heredity
PST 421 - Cardiorespiratory Disorders and Rehabilitation 11

Spontaneous pneumothorax
• Secondary spontaneous pneumothorax (SSP) occurs in people with a wide variety of parenchymal lung diseases.
• occur more frequently after age 60 years.
• These individuals have underlying pulmonary pathology that alters normal lung structure
• Airway disease
• Chronic obstructive pulmonary disease
• Cystic fibrosis
• Status asthmaticus
PST 421 - Cardiorespiratory Disorders and Rehabilitation 12

Risk factors for SSP
• Chronic obstructive pulmonary disease is the most common lung disease causing secondary pneumothorax, accounting for around 57% of cases.
• The risk of pneumothorax seems to increase with worsening chronic obstructive pulmonary disease
• Other causes of secondary pneumothorax include asthma, cystic fibrosis, lung cancer, tuberculosis, interstitial lung disease, and endometriosis.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 13

Causes of secondary pneumothorax
• Infectious lung disease
• Pneumocystis carinii pneumonia
• Necrotizing pneumonias
• Interstitial lung disease
• Sarcoidosis
• Idiopathic pulmonary fibrosis
• Pulmonary Langerhans cell histiocytosis
• Lymphangioleiomyomatosis
• Tuberous sclerosis
Connective tissue diseaseAnkylosing spondylitis, Polymyositis, Dermatomyositis, SclerodermaMarfan’s syndrome, CancerSarcomaLung cancer
PST 421 - Cardiorespiratory Disorders and Rehabilitation 14

Symptoms of spontaneous pneumothorax
• Sudden onset of chest pain (This is a sharp pain, which may lead to a feeling of tightness in the chest)
• Dyspnoea (shortness of breath)
• Tachycardia (rapid heart rate)
• Tachypnoea (rapid respiration rate)
• Coughing (dry)
• Fatigue
• Signs of respiratory distress (nasal flaring, anxiety etc)
• Hypotension
PST 421 - Cardiorespiratory Disorders and Rehabilitation 15

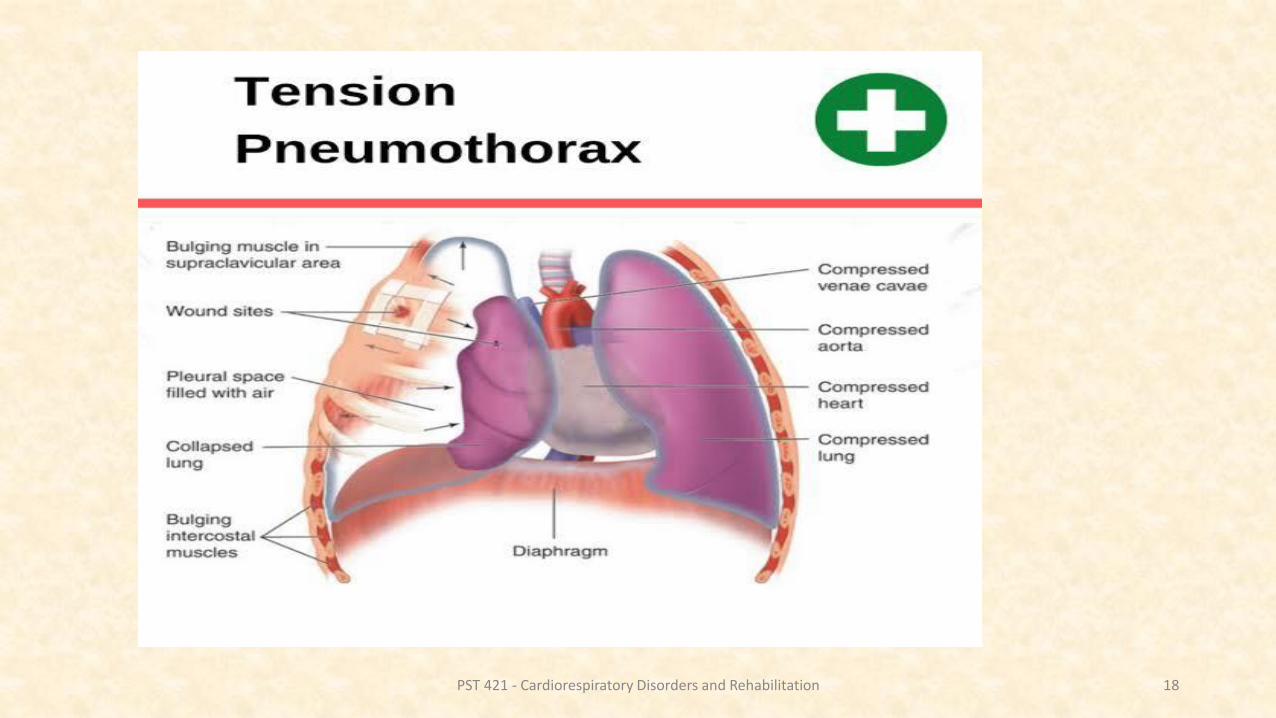
Tension pneumothorax
• Tension pneumothorax is a life threatening complication that requires immediate recognition and urgent treatment.
• Tension pneumothorax is caused by the development of a one way valve-like leak in visceral pleura, such that air escapes from the lung during inspiration but cannot re-enter the lung during expiration.
• This process leads to an increasing pressure of air within the pleural cavity and haemodynamic compromise because of impaired venous return and decreased cardiac output.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 16

Tension pneumothorax
• Radiographic features suggesting tension pneumothorax include: • cardiomediastinal shift away from the affected side and,
in some cases, • inversion of the hemidiaphragm• widening of intercostal spaces from the increased
pressure within the affected hemithorax.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 17
PST 421 - Cardiorespiratory Disorders and Rehabilitation 18

a. Tension pneumothorax in the left lungb. Condition after chest tube drainage in the leftlung. Complete re-expansion of the left lung
PST 421 - Cardiorespiratory Disorders and Rehabilitation 19

Tension Pneumothorax
• Respiratory distress, tachycardia, hypotension, tracheal deviation, unilateral absence of breath sounds, neck vein distention, cyanosis
• Hyperresonance!
PST 421 - Cardiorespiratory Disorders and Rehabilitation 20

PST 421 - Cardiorespiratory Disorders and Rehabilitation 21

DIAGNOSIS OF PNEUMOTHORAX
• Chest X-ray
• The diagnosis of pneumothorax is established from the patients’ history and physical examination findings that reveal
• decreased movement of the hemithorax,
• decreased or absent fremitus,
• Hyper-resonance on percussion and
• decreased or absent breath sounds on auscultation
• Tachycardia
• Dyspnoea
PST 421 - Cardiorespiratory Disorders and Rehabilitation 22

PST 421 - Cardiorespiratory Disorders and Rehabilitation 23

Management
• The objective in treating a pneumothorax is
• to eliminate the air from the pleural space,
• to allow lung to re-expand, and
• to prevent recurrences.
• The best method for achieving this depends on
• the severity of the lung collapse,
• the type of pneumothorax,
• patient’s overall health and on
• the risk of complications.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 24

Management
Oxygen therapy
• Gas within the pleural cavity is absorbed by diffusion and can be facilitated by changing the composition of the intra-pleural cavity gas. Oxygen is absorbed 62 times faster than nitrogen, and carbon dioxide (CO2) is absorbed 23 times faster than oxygen.
• When the patient inhales 100% oxygen, nitrogen will disappear from the pleural cavity, leaving only oxygen, which is absorbed faster from the pleural cavity into veins.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 25

Management - aspiration
• Aspiration of a pneumothorax is performed using a small catheter.
• The catheter is inserted into the pleural cavity and either removed immediately after evacuating the air from the pleural cavity or left inserted while the patient if observed.
• When left inserted in the thoracic wall, the catheter is still considered a chest tube despite its small size.
• In patients diagnosed with spontaneous pneumothorax, the mean success rate of aspiration is between 53% and 58%.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 26

PST 421 - Cardiorespiratory Disorders and Rehabilitation 27

Pleurodesis
• Pleurodesis is a procedure that precipitates an inflammatory process leading to the adherence of parietal and visceral pleura, thereby obliterating the pleural space.
• This can be achieved through instillation of an agent such as talc or tetracycline derivatives through a chest drain (medical pleurodesis)
• or by mechanical abrasion of the pleura or instillation of a suitable agent during an operation (surgical pleurodesis).
PST 421 - Cardiorespiratory Disorders and Rehabilitation 28

Physiotherapy management
• Physiotherapy is involved in the acute management and rehabilitation of patients with pneumothorax
• Assessment
• Subjective assessment
• Objective assessment
• Auscultation, percussion, Breathing pattern, respiratory rate, exercise capacity, upper limb mobility e.t.c
PST 421 - Cardiorespiratory Disorders and Rehabilitation 29

Physiotherapy management
• Indications for Physiotherapy
• Lung collapse
• Increased work of breathing
• Impaired airway clearance
• Blood gas abnormalities
• Sputum retention
Goals for PhysiotherapyTo reinflate atelectatic lung areasTo improve ventilationTo increase oxygenationMaintain airway clearanceImprove exercise toleranceTo prevent musculoskeletal complications.
PST 421 - Cardiorespiratory Disorders and Rehabilitation 30

Physiotherapy Management
To reduce work and difficulty of breathing
• Body positioning
• Breathing control
• Relaxation technique
To improve ventilation
• Thoracic expansion exercise
• Deep breathing exercise
• Incentive spirometry
Sputum mobilisation techniquesPostural drainageActive cycle of breathingManual techniquesPercussion, shaking and vibrationsSputum removal techniquesCoughing and huffingAirway suctioning
PST 421 - Cardiorespiratory Disorders and Rehabilitation 31

Physiotherapy Management
• Upper limb range of motion exercise
• Graded exercise to improve exercise tolerance and capacity
PST 421 - Cardiorespiratory Disorders and Rehabilitation 32

Outcome AssessmentPhysiotherapy outcome evaluation includes
• Respiratory rate
• Breathing pattern
• Sputum quantity
• Auscultation
• Cough sound
• Oxygen requirement
• SpO2
• Arterial blood gases
• Chest x-ray changes
• Muscle strength
• Functional performance
PST 421 - Cardiorespiratory Disorders and Rehabilitation 33





























