Embed Size (px)
Citation preview

CHAPTER:5PSORIASIS
BYMrs. K.SHAILAJA., M. PHARM.,LECTURERDEPT OF PHARMACY PRACTICE,SRM COLLEGE OF PHARMACY

OVERVIEW 2
5. Case studies
4. Managing psoriasis
3. Diagnosing psoriasis
2. Clinical presentation
1. Epidemiology and pathophysiology

WHAT IS PSORIASIS? 3
– Inflammatory and hyperplastic disease of skin1
– Characterised by erythema and elevated scaly plaques1
– Chronic, relapsing condition
– Course of disease often unpredictable

5
19
21
29
31
71
79
94
0 20 40 60 80 100
Other
Fatigue
Burning sensation
Bleeding
Tightness of skin
Skin redness
Itching
Scaling
Percentage of respondents (n = 17,425)
SYMPTOMS OF PSORIASIS 4
Most frequently experienced symptoms

SOCIAL IMPACT OF PSORIASIS
40
48
57
0 10 20 30 40 50 60Percentage of respondents with severe psoriasis (n = 502)
5
Psoriasis mistaken for other disease
Trouble receiving equal treatment in
service establishments (e.g. hair salons,
public pools)
Psoriasis mistaken as contagious

PSORIASIS AFFECTS EMOTIONAL STATE
54
75
81
88
0 20 40 60 80 100
Depression
Feelings of unattractiveness
Feelings of embarrassment
Concern that disease would worsen
Percentage of 18-to-34-year-old respondents with severe psoriasis (n not reported)
6

EPIDEMIOLOGY
• Common skin disorder
• Prevalence variable: ~ 0.3–2.5%1
• Prevalence equal in males and females2
• Estimated incidence: ~ 60 per 100,000 per year3
1. Plunkett A et al. Australas J Dermatol 1998; 39: 225–232. 2. Griffiths CEM et al. In: Burns T et al., eds. Rook’s textbook of dermatology. 8th ed. UK: Blackwell Publishing Ltd, 2010. 3. Bell LM et al. Arch Dermatol 1991; 127: 1184–7.
7

AGE OF ONSET
• Mean age: ~ 23–37 years1
• Current theory: 2 distinct peaks with possible genetic associations1
– Early onset (16–22 years)2
• More severe and extensive
• More likely to have affected first-degree family member
– Late onset (57–60 years)2
• Milder form
• Affected first-degree family members nearly absent
1. Plunkett A et al. Australas J Dermatol 1998; 39: 225-232. 2. Henseler T et al. J Am Acad Dermatol 1985; 13:450-6.
8
GENETIC INFLUENCE
• Evidence suggests strong genetic association
– Studies of monozygotic twins show concordance for psoriasis (e.g. 64% in a Danish Study)1
– Multiple susceptibility loci have been identified2
• Disease expression – likely result of genetic and environmental factors2
1.Brandup F et al. Acta Dermato-Vernerol 1982; 62L: 229–36. 2. Barker J. Clin Exp Dermatol 2001; 26(4): 321–5.
9

COMMON TRIGGER FACTORS FOR PSORIASIS1
• Infections (e.g. streptococcal, viral)• Skin trauma (Koebner phenomenon)• Psychological stress • Drugs (e.g. lithium, beta blockers)• Sunburn• Metabolic factors (e.g. calcium deficiency)• Hormonal factors (e.g. pregnancy)
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
10

PSORIASIS IS A T-CELL MEDIATED, AUTOIMMUNE DISEASE1
• Current hypothesis:
– Unknown skin antigens stimulate immune response• Antigen-specific memory T-cells are primary mediators
– Leads to impaired differentiation and hyperproliferation of keratinocytes
1. Lee M et al. Australas J Dermatol 2006; 47: 151–9.
11
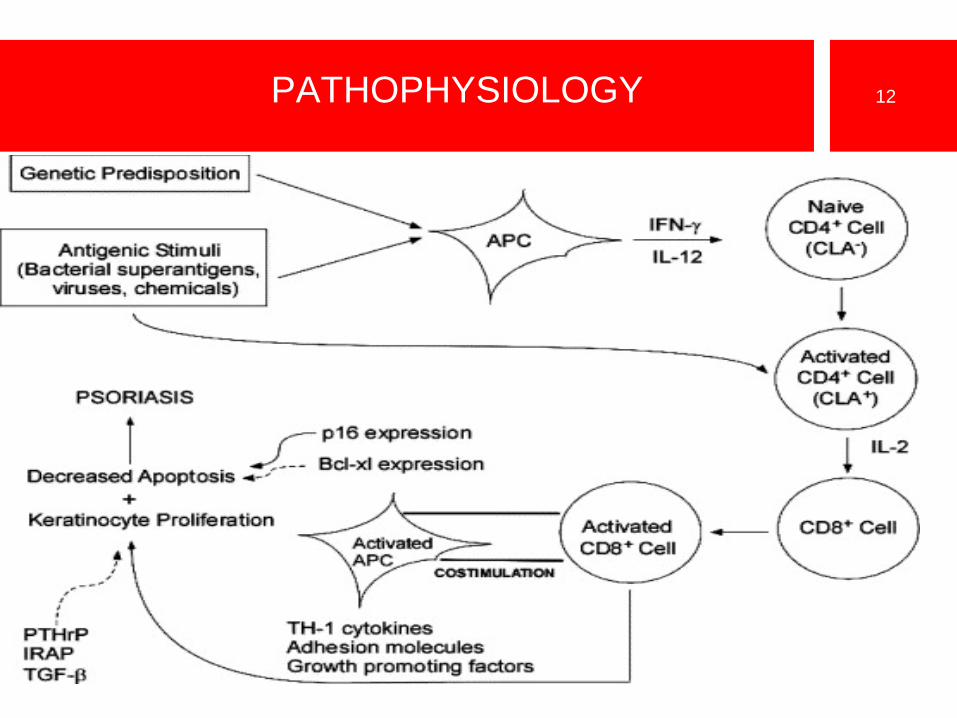
PATHOPHYSIOLOGY 12
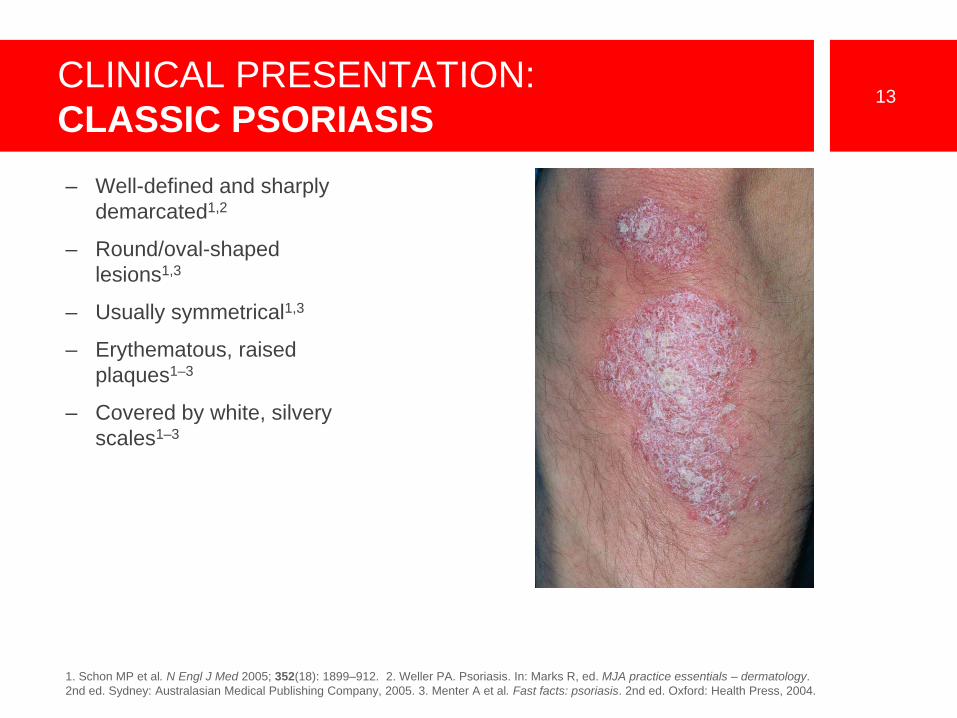
CLINICAL PRESENTATION: CLASSIC PSORIASIS
13
– Well-defined and sharply demarcated1,2
– Round/oval-shaped lesions1,3
– Usually symmetrical1,3
– Erythematous, raised plaques1–3
– Covered by white, silvery scales1–3
1. Schon MP et al. N Engl J Med 2005; 352(18): 1899–912. 2. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 3. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.

COMMON SITES AFFECTED BY PSORIASIS
14
• Can affect any part of the body –typically scalp, elbow, knees and sacrum1
• Extent of disease varies
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.

TYPES OF PSORIASIS
• Chronic plaque• Guttate• Flexural• Erythrodermic
• Pustular– Localised and generalised
• Local forms– Palmoplantar
– Scalp
– Nail (psoriatic onychodystrophy)
15
1. van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 2. Rossi S, ed. Australian medicines handbook. Adelaide: AMH, 2010.

CHRONIC PLAQUE PSORIASIS 16
– Most common type –affects approximately 85%1
– Features pink, well-defined plaques with silvery scale2
– Lesions may be single or numerous2
– Plaques may involve large areas of skin2
– Classically affects elbows, knees, buttocks and scalp3
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 3. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials –dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.

CHRONIC PLAQUE PSORIASIS 17

CHRONIC PLAQUE PSORIASIS 18

CHRONIC PLAQUE PSORIASIS 19

GUTTATE PSORIASIS 20
– Numerous and small lesions – ~ 1 cm diameter1,2,3
– Pink with less scale than plaque psoriasis1
– Commonly found on trunk and proximal limbs1,3
– Typically seen in individuals < 30 years4
– Often preceded by an upper respiratory tract streptococcal infection1,2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials –dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 4. Menter A et al. J Am Acad Dermatol 2008; 58(5): 826–50.

FLEXURAL PSORIASIS 21
– Lesions in skin folds1
– Particularly groin, glutealcleft, axillae and submammary regions
– Often minimal or absent scaling1,2
– May cause diagnostic difficulty when genital or perianal region is affected in isolation
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. SchonMP et al. N Engl J Med 2005; 352(18): 1899–912.

ERYTHRODERMIC PSORIASIS 22
– Generalised erythemacovering entire skin surface1,2
– May evolve slowly from chronic plaque psoriasis or appear as eruptive phenomenon1,3
– Patients may become febrile, hypo/hyperthermicand dehydrated3
– Complications include cardiac failure, infections, malabsorption and anaemia1
– Relatively uncommon
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials –dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.3. Menter A et al. J Am Acad Dermatol 2008; 58(5): 826–50.

PUSTULAR PSORIASIS 23
– Two forms:
• Localised form
• More common1,2
• Presents as deep-seated lesions with multiple small pustules on palms and soles1,2
• Generalised form
• Uncommon3
• Associated with fever and widespread pustules across inflamed body surface3
1. Buxton P et al. ABC of dermatology. 5th ed. UK: Wiley-Blackwell, 2009. 2. Griffiths CEM et al. Psoriasis. In: Burns T et al., eds. Rook’s textbook of dermatology. 8th ed. UK: Blackwell Publishing Ltd, 2010. 3. Menter A et al. J Am Acad Dermatol 2008; 58(5): 826–50.

PALMOPLANTAR PSORIASIS1 24
– Can be hyperkeratotic or pustular
– May mimic dermatitis –look for psoriatic manifestations elsewhere to aid diagnosis
– Possibly aggravated by trauma
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.

SCALP PSORIASIS 25
– Varies from minor scaling with erythema to thick hyperkeratotic plaques1,2
– May extend beyond hairline1,2
– Patient scratching may produce asymmetric plaques2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.

NAIL PSORIASIS1 26
– May be present in patients with any type of psoriasis
– Can take several forms:
• Pitting: discrete, well-circumscribed depressions on nail surface
• Subungual hyperkeratosis: silvery white crusting under free edge of nail with some thickening of nail plate
• Onycholysis: nail separates from nail bed at free edge
• ‘Oil-drop sign’: pink/red colour change on nail surface
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.

NAIL PSORIASIS 27

NAIL PSORIASIS 28

NAIL PSORIASIS 29

PSORIATIC ARTHRITIS 30
– Approximately 5–20% have associated arthritis1
– Five major patterns of psoriatic arthritis:2
• Distal interphalangealinvolvement
• Symmetrical polyarthritis
• Psoriatic spondylarthropathy
• Arthritis mutilans
• Oligoarticular, asymmetrical arthritis
– Clinical expressions often overlap2
1. Schon MP et al. N Engl J Med 2005; 352(18): 1899–912. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.

DIAGNOSING PSORIASIS
• Other dermatological disorders can resemble psoriasis
• Diagnosed clinically according to appearance, distribution, history of lesions and family history
• Important to consider non-cutaneouscomplications1
1. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials –dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.
31

DIFFERENTIAL DIAGNOSIS1,2
• Localisedpatches/plaques
– Tinea– Eczema– Superficial basal cell
carcinoma and Bowen’s disease
– Seborrhoeic dermatitis– Cutaneous T-cell lymphoma
(mycosis fungoides)
• Guttate– Pityriasis rosea– Drug eruption– Secondary syphilis
• Flexural– Tinea– Eczema– Candidiasis– Seborrhoeic dermatitis
• Erythrodermic– Eczema– Cutaneous T-cell lymphoma– Pityriasis rubra pilaris– Lichen planus– Drug
• Palmoplantar– Tinea
32
1. van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
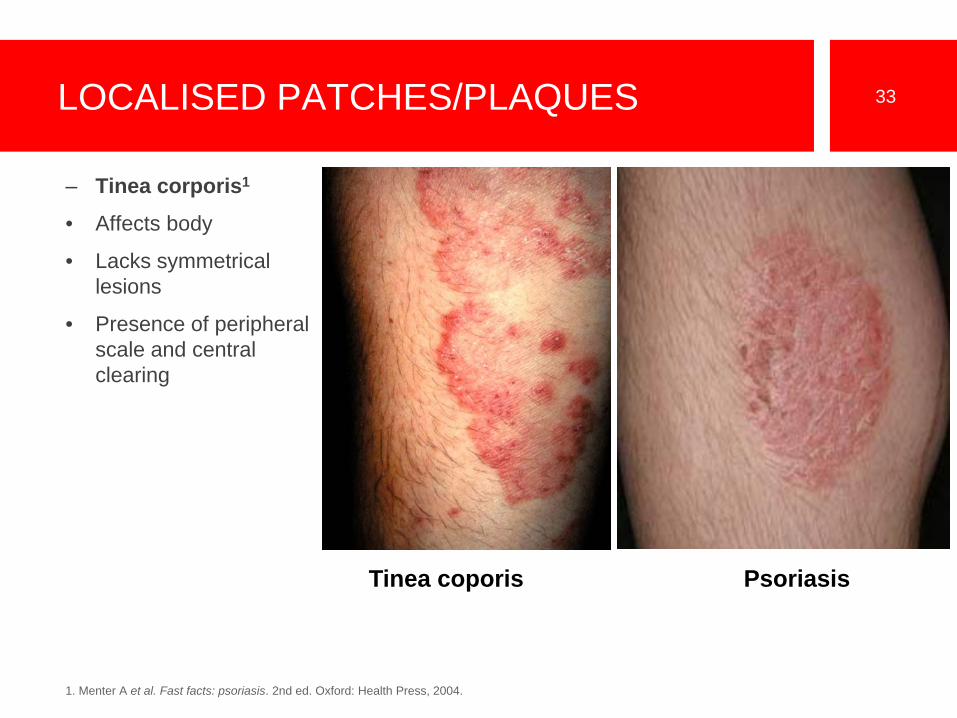
LOCALISED PATCHES/PLAQUES 33
– Tinea corporis1
• Affects body
• Lacks symmetrical lesions
• Presence of peripheral scale and central clearing
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Tinea coporis Psoriasis

LOCALISED PATCHES/PLAQUES 34
– Discoid eczema1
• Individualised patches more pruritic than psoriasis
• Lack silvery scale
• Less vivid colour than psoriasis
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Discoid eczema Psoriasis
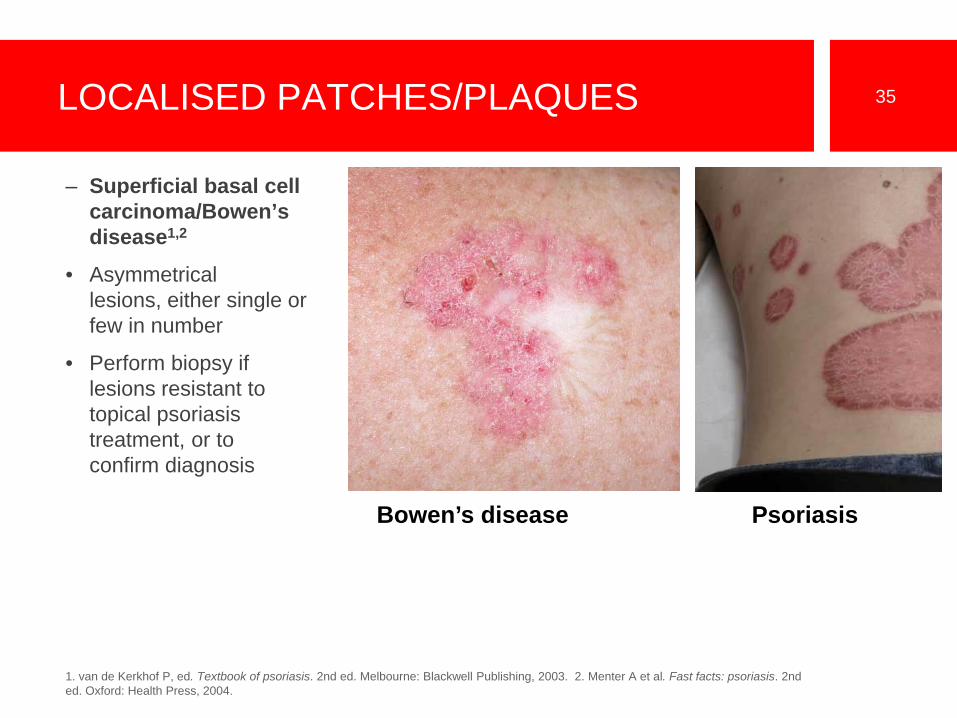
LOCALISED PATCHES/PLAQUES 35
– Superficial basal cell carcinoma/Bowen’s disease1,2
• Asymmetrical lesions, either single or few in number
• Perform biopsy if lesions resistant to topical psoriasis treatment, or to confirm diagnosis
1. van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Bowen’s disease Psoriasis
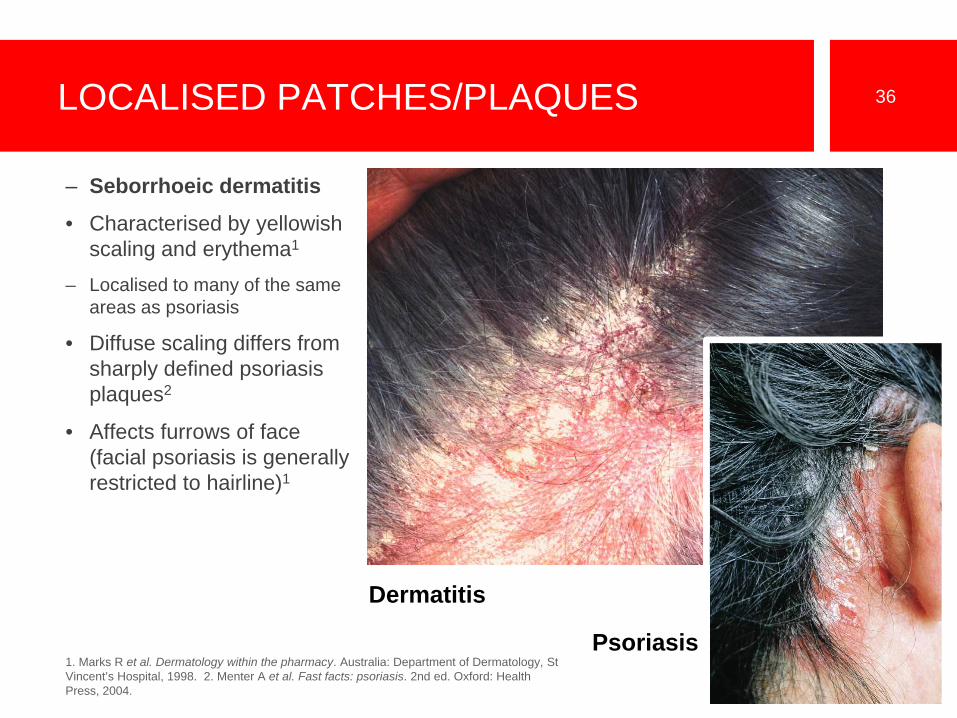
LOCALISED PATCHES/PLAQUES 36
– Seborrhoeic dermatitis
• Characterised by yellowish scaling and erythema1
– Localised to many of the same areas as psoriasis
• Diffuse scaling differs from sharply defined psoriasis plaques2
• Affects furrows of face (facial psoriasis is generally restricted to hairline)1
1. Marks R et al. Dermatology within the pharmacy. Australia: Department of Dermatology, St Vincent’s Hospital, 1998. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Dermatitis
Psoriasis

LOCALISED PATCHES/PLAQUES 37
– Cutaneous T-cell lymphoma (mycosis fungoides)
• Red, discoid lesions1
• Asymmetrical and less scaly than psoriasis1
• Lesions may present with fine atrophy and be resistant to antipsoriatic therapy2
• Biopsy to confirm diagnosis
1. Fry L. An atlas of psoriasis. Spain: Taylor & Francis, 2004. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Mycosis fungoides
Psoriasis

GUTTATE PSORIASIS 38
– Pityriasis rosea1
• Difficult to distinguish from acute guttate psoriasis
• Presents first as single large patch, progresses to a truncal rash of multiple red scaly plaques (‘Christmas tree’ distribution)
• Resolves over 8–12 weeks
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
< Psoriasis ^ Pityriasis rosea

GUTTATE PSORIASIS 39
– Secondary syphilis
• Search for characteristic primary syphilitic lesion, lymphadenopathy, and lesions of face, palm and soles1
• Conduct serology and skin biopsies to confirm1,2
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003.
< Psoriasis ^ Secondary syphilis

FLEXURAL PSORIASIS 40
– Atopic eczema1,2
• Often associated with asthma and hay fever
• Lacks classic psoriatic nail involvement and sharply demarcated scaly plaques
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Fischer, G. How to treat: atopic dermatitis. Australian Doctor. 16 April 2010: 29–36.
< Psoriasis ^ Atopic eczema

FLEXURAL PSORIASIS 41
– Candidiasis1,2
• Characteristic peripheral pustules and scaling differ to psoriasis
• Yeast cultures are diagnostic
– Seborrhoeic dermatitis2
1. Van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Flexural psoriasis

PALMOPLANTAR PSORIASIS 42
– Tinea manum1
• Ringworm of hands
• Fine powdery scale, particularly involving palms and palmar creases
• Usually asymmetrical
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Tinea corporis Psoriasis

PALMOPLANTAR PSORIASIS 43
– Hand and foot eczema
• Hyperkeratotic forms difficult to distinguish from psoriasis1,2
• Biopsies can assist diagnosis1
• Look for history of atopy, a lack of psoriasis elsewhere on body, and evidence of eczema elsewhere on skin1
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003.
Eczema
Psoriasis

PALMOPLANTAR PSORIASIS 44
– Pompholyx of palms and soles (dishydroticeczema)1
• Presents as clear vesicles – contrast to white/yellow pustules in pustularpsoriasis
• Accompanied by intense pruritus
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
Eczema
Psoriasis

DETERMINING PSORIASIS SEVERITY
• Psoriasis Area and Severity Index (PASI)1
– Score indicates severity of disease at a given time
– Single number that considers severity of lesions and extent of disease across four major body sites (head, trunk, upper limbs and lower limbs)
– Score ranges from 0 (no disease) to 72 (maximal disease)
1. Dubertret L. Psoriasis from clinic to therapy. France: Med’com, 2005.
45

MANAGING PSORIASIS
• Before starting treatment– Establish relationship of trust with patient1
– Provide patient with information
• Emphasise benign nature of disease2,3
• Explain that psoriasis tends to be chronic and recurrent2,3
1. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 3. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
46

MANAGING PSORIASIS
• Determine clinical setting before selecting treatment, considering
– Disease pattern, severity and extent1,2
– Sites of disease2
– Coexistent medical conditions1
– Patient’s perception of disease severity1
– Time commitments and treatment expense1,2
– Previous treatments for psoriasis1
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
47

MANAGING PSORIASIS
• Goals of management– Tailor management to individual and address both medical and
psychological aspects1–3
– Improve quality of life3
– Achieve long-term remission and disease control3
– Minimise drug toxicity3
– Evaluate and monitor efficacy and suitability of individual treatments3
– Remain flexible and respond to changing needs1–3
1.Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 3. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.
48

TREATMENT OPTIONS FOR PSORIASIS
• Stepwise approach is advised1
• Treatments include:1,2,3
– General measures and topical therapy
– Phototherapy
– Systemic and biological therapies
• Combination therapies may reduce toxicity and improve outcomes2
1. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
49

TREATING PSORIASIS: GENERAL MEASURES1,2
• Reduce/eliminate potential trigger factors:– Stress
– Smoking
– Alcohol
– Trauma
– Drugs
– Infections
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
50

TOPICAL THERAPIES
• Approximately 70% of patients with mild-to-moderate psoriasis can be managed with topical therapies alone1
• Tailor to needs of patient2
• Potency, delivery vehicle and patient motivation may affect compliance1
• Application may be time-consuming for patients1
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
51

TOPICAL THERAPIES: EMOLLIENTS
• Include aqueous cream, sorbolene cream, white soft paraffin and wool fats1
• Regular use can:– alleviate pruritus2
– reduce scale2
– enhance penetration of concomitant topical therapy2
– hydrate dry and cracked skin3
• Soap should be avoided4
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Rossi S, ed. Australian medicines handbook. Adelaide: AMH, 2010. 4. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.
52

TOPICAL THERAPIES: KERATOLYTICS
• Over-the-counter products include:1– Salicylic acid
– Urea
• Help dissolve keratin to soften and lift psoriasis scales1,2
• May enhance penetration of other actives1
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
53

TOPICAL THERAPIES: COAL TAR
• Help reduce inflammation and pruritus1
• May induce longer remissions2
• Use limited by distinctive smell and ability to stain clothing and skin1,2
• May cause local skin irritation2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.
54

TOPICAL THERAPIES: DITHRANOL
• Anti-proliferative properties1
• Particularly effective in thick plaque psoriasis1
• Initiate therapy at very low concentrations – can burn skin2
• Not suitable for face, flexures or genitals1,3
• Stains clothes permanently and skin temporarily1,2,3
1. Dermatology Expert Group. Therapeutic Guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Weller PA. Psoriasis. In: Marks R,ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005.
55

TOPICAL THERAPIES: TAZAROTENE
• Topical synthetic retinoid1,2
• For treatment of chronic plaque psoriasis1,2
• Applied once daily in evening1,2
• Commonly causes local irritation1,2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. ZoracProduct Information, 30 March 2007.
56

TOPICAL THERAPIES: CORTICOSTEROIDS
• Possess anti-inflammatory, antiproliferative and immunomodulatory properties1,2
• Reduce superficial inflammation within plaques3
• Potency choice depends on disease severity, location and patient preference2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Buxton P et al. ABC of dermatology. 5th ed. UK: Wiley-Blackwell, 2009.
57

TOPICAL THERAPIES: CORTICOSTEROIDS
• Adverse effects associated with long-term use include:1,2
– Skin atrophy and telangiectasia
– Hypopigmentation
– Striae
– Rapid relapse or rebound on stopping therapy
– Precipitation of pustular psoriasis
– Pituitary-adrenal axis suppression through significant systemic absorption (rare)
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
58

TOPICAL THERAPIES: CALCIPOTRIOL (DAIVONEX®)
• Synthetic vitamin D analogue1
• For chronic plaque-type psoriasis1
• Reverses abnormal keratinocyte changes by:1– Inducing differentiation
– Suppressing proliferation of keratinocytes
1. Daivonex Product Information, 23 September, 2006.
59
TOPICAL THERAPIES: CALCIPOTRIOL (DAIVONEX®)
• Response may require 4–6 weeks1,2
• Adverse effects include erythema and irritation3
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Weller PA. Psoriasis. In: Marks R, ed. MJA practice essentials – dermatology. 2nd ed. Sydney: Australasian Medical Publishing Company, 2005. 3. DaivonexProduct Information, 23 September, 2006.
60

TOPICAL THERAPIES: CALCIPOTRIOL/BETAMETHASONEDIPROPIONATE OINTMENT (DAIVOBET®)
• For plaque-type psoriasis1
• Combination of calcipotriol and a potent topical corticosteroid (betamethasone dipropionate)1
– Stable formulation for both actives1
• Provides rapid, effective psoriasis control1,2
1. Daivobet Product Information, 3 December 2007. 2. Kaufmann R et al. Dermatology 2002; 205(4): 389–93.
61

TOPICAL THERAPIES: CALCIPOTRIOL/BETAMETHASONEDIPROPIONATE OINTMENT (DAIVOBET®)
Adapted from Kaufmann R et al. Dermatology 2002; 205(4): 389–93.
62
– Combination of calcipotriol and betamethasone dipropionate in Daivobet is more effective than either active constituent used alone
• 39.2% mean reduction in PASI score after 1 week
TOPICAL THERAPIES: CALCIPOTRIOL/BETAMETHASONEDIPROPIONATE OINTMENT (DAIVOBET®)
• Once-daily treatment with the potential to improve compliance1,2
• Can be used intermittently in 4-weekly cycles with Daivonex® used in between for maintenance1
• Most common adverse events include pruritus, rash and burning sensation1
1. Daivobet Product Information, 3 December 2007. 2. Kaufmann R et al. Dermatology 2002; 205(4): 389–93.
63

TOPICAL THERAPIES: CALCIPOTRIOL/BETAMETHASONE DIPROPIONATE GEL
• Newly TGA approved product not yet available in Australia
• Specially formulated for the scalp1
• Provides rapid, effective control of scalp psoriasis1,2,3
– More effective than treatment with individual actives alone
– 53.2% (more than half) of patients had absent or very mild disease after just two weeks of gel application1
• Once-daily formulation may encourage compliance2
1. Daivobet ®Gel Product Information, 14 July 2010. 2. van de Kerkhof et al. BJD 2008; 160: 170–6. 3. Jemec GBE et al. J Am Acad Dermatol 2008; 59:455-463.
64

OTHER THERAPIES
• Phototherapy
• Systemic therapies
• Biological agents
65

PHOTOTHERAPY
• For psoriasis resistant to topical therapy and covering > 10% of body surface area1
• Immunomodulatory and anti-inflammatory effects2
• Three main types of phototherapy:2– Broadband UVB
– Narrowband UVB
– PUVA (administration of psoralen before UVA exposure)
• Treatment usually administered 2–3 times/week1,2
1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004.2. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009.
66

SYSTEMIC THERAPIES
• Reserved for patients with widespread or severe psoriasis1
• Potentially serious adverse effects and drug interactions2
• Many require PBS authority prescription from dermatologist3
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 3. Department of Health and Ageing. Schedule of Pharmaceutical Benefits. http://www.pbs.gov.au (accessed online 14 August 2010).
67

SYSTEMIC THERAPIES: METHOTREXATE
• Most commonly used systemic treatment for psoriasis1
• Slows epidermal cell proliferationand acts as immunosuppressant1
• Closely monitor kidney, liver and bone-marrow function2
• Perform PASI score before starting treatment
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Methoblastin Product Information, 11 August 2004.
68
SYSTEMIC THERAPIES: CYCLOSPORIN
• Immunosuppressive agent1
• For patients with severe psoriasis that is refractory to other treatments2
• Requires ongoing monitoring of blood elements, and renal and liver function2
1. Dermatology Expert Group. Therapeutic guidelines: dermatology. Version 3. Melbourne: Therapeutic Guidelines Limited, 2009. 2. Neoral Product Information, 22 October 2009.
69

SYSTEMIC THERAPIES: ACITRETIN1
• Oral retinoid
• For treatment of all forms of severe psoriasis
• Once-daily oral therapy
• Teratogenic – pregnancy must be avoided
1. Neotigason Product Information, 18 March 2008.
70

BIOLOGICAL AGENTS
• Proteins derived from living organisms that exert pharmacological actions1
• For adults with moderate-to-severe chronic plaque-type psoriasis who are candidates for phototherapy or systemic therapy2–5
• Most administered sub-cutaneously2–5
1. Buxton P et al. ABC of dermatology. 5th ed. UK: Wiley-Blackwell, 2009. 2. Humira Product Information, 18 September 2009. 3. StelaraProduct Information, 15 July 2009. 4. Remicade Product Information, 17 September 2008. 5. Enbrel Product Information, 16 February 2010.
71





























