Embed Size (px)
Citation preview

PRP: WHERE ARE WE?
JeffreyRapaport,MD,PA
Fellow,AmericanAcademyofDermatologyFellow,AmericanSocietyforDermatologicSurgeryAADPresenta9onHandOuts2.17.2018

SmallVolume/SingleSpin/SimpleSystems
LargeVolume/DoubleSpin/ComplexSystems
VS.
ACPFloa%ngBuoySystems–BuffyCoat
SeparatorGelSystems
Designed for Orthopedics – Higher Platelet Concentration (5x+) – High inflammation – High RBC
and Granulocytes
Emcyte
Magellan
Harvest
Arthrex Angel
Designed for low to medium platelet Concentration (1.4X-4X) Less inflammation - Ideal for Dermatologic Applications
Designed for Orthopedics – Lower Platelet Concentration (2x) – Low inflammation – no
separator gel – easy to mix RBC
Floa%ngBuoySystems–BuffyCoat
Computer-Aided Systems

Patient Indication for PRP Treatment
§ Primary: Androgenic Alopecia (Lower Ludwig or Hamilton preferred)
§ Secondary: Alopecia Areata
§ Traction Alopecia
Scalp Disorders - Partial Effectiveness ?? § Telogen Effluvium
§ CCCA, Frontal Fibrosing Alopecia, Lichen Planopilaris,
Contraindications: Other § Pregnancy or breast feeding, cancer or chemotherapy, keloid
development, platelet count less than 105, local infection, hematologic/coagulation disorders, history of untreated thyroid disorders, untreated anemia, severe scalp psoriasis, history of untreated Vitamin D deficiency, body dysmorphic disorder, untreated Hyperandrogenism Syndromes

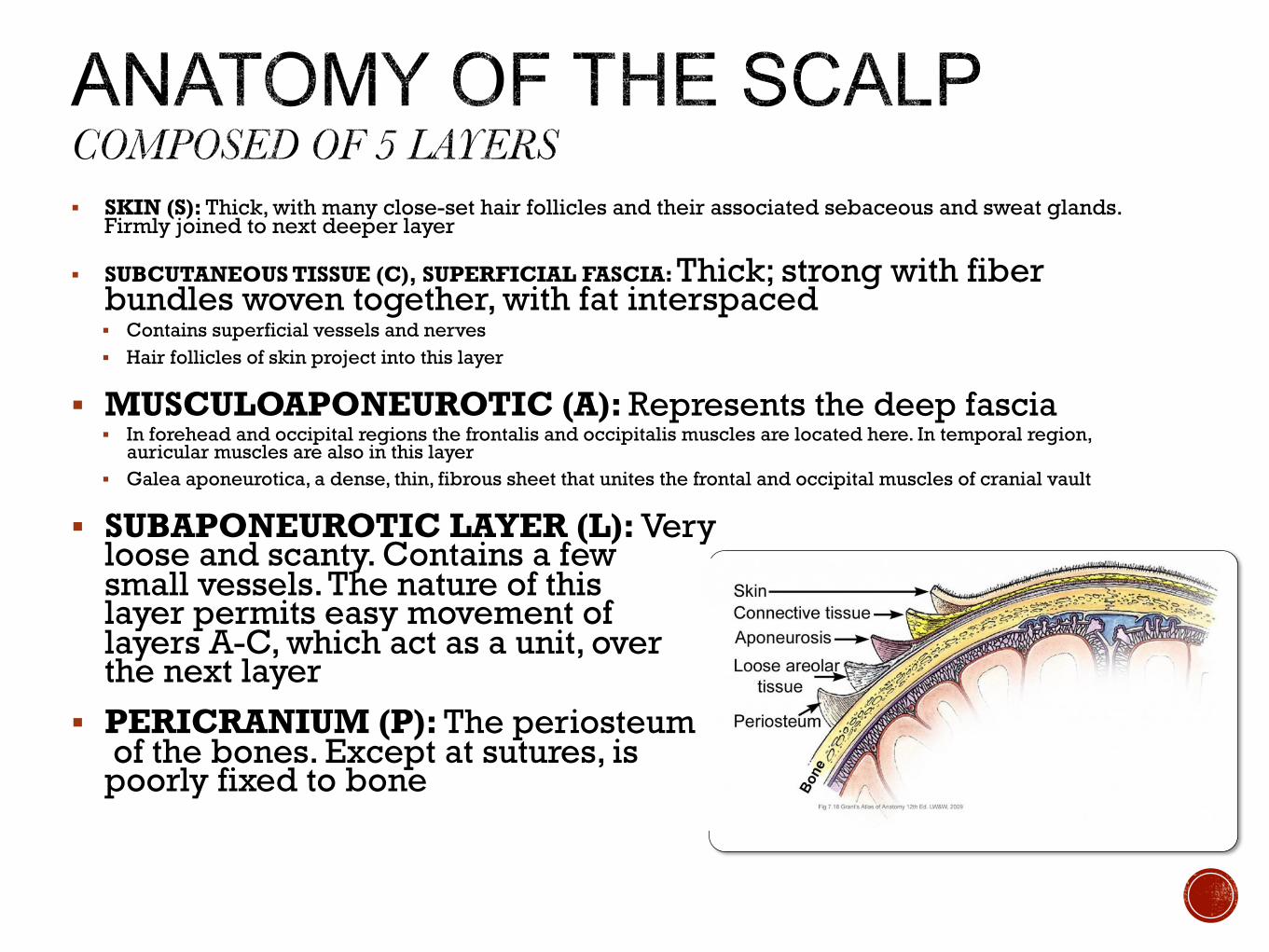
§ SKIN (S): Thick, with many close-set hair follicles and their associated sebaceous and sweat glands. Firmly joined to next deeper layer
§ SUBCUTANEOUS TISSUE (C), SUPERFICIAL FASCIA: Thick; strong with fiber bundles woven together, with fat interspaced § Contains superficial vessels and nerves § Hair follicles of skin project into this layer
§ MUSCULOAPONEUROTIC (A): Represents the deep fascia § In forehead and occipital regions the frontalis and occipitalis muscles are located here. In temporal region,
auricular muscles are also in this layer § Galea aponeurotica, a dense, thin, fibrous sheet that unites the frontal and occipital muscles of cranial vault
§ SUBAPONEUROTIC LAYER (L): Very loose and scanty. Contains a few small vessels. The nature of this layer permits easy movement of layers A-C, which act as a unit, over the next layer
§ PERICRANIUM (P): The periosteum of the bones. Except at sutures, is poorly fixed to bone
§ Numb patient’s scalp with a topical
numbing agent (optional)
§ Have patient sign two labels (One label
per tube)
§ Draw blood into appropriate size tube
(usually 22 mL)
§ PRP can be concentrated for better
outcomes
§ Centrifuge at for 3500 RPM for 10 minutes
(See centrifuge instructions)
§ Draw up platelet poor plasma (PPP) using
10 cc syringe and Rigid Needle, leave
platelet rich plasma (PRP)
§ Invert the tube 10-20 times and collect PRP
into syringe § Optional Add .1 mL lidocaine
§ Change needle to 27 or 30 x ½” gauge
§ Lie patient down
§ Remove topical anesthetic (optional) § Thoroughly rinse the scalp until no
numbing cream is left
§ Sanitize the scalp with alcohol. The hair
should be easily manipulated with a
comb.
§ Use 27 or 30 gauge x ½ inch needle and
3cc Syringe
§ Start Chiller or
§ 50% O2/50% N2O Analgesia
§ Have patient identify name and signature
§ Subdermal depo injection technique
§ Inject approximately .2 - .5 mL PRP distributed evenly in areas of hair loss
§ Schedule 3-4 monthly treatments followed by a 3-6 month maintenance interval
*For use with standard PRP. Not effective with activated PRP.

§ Mounting body of evidence FOR effectiveness of PRP for Hair Restoration
§ Increased critical scientific data needed
§ Standardization in PRP protocols including preparation, composition and activation
§ More human studies with quantitative analysis, control groups, blinding, longer time frames, single variables, larger sample sizes, standardized outcome assessment (allowing meta-analysis)





























