Embed Size (px)
Citation preview

PEB
EttwmafptpfimAarsp�luapvaht
S
A
0d
roximal Migration and Endoleak: Impact ofndograft Design and Deployment Techniques
radley Thomas, MD, and Luis Sanchez, MD
Repair of abdominal aortic aneurysms by endovascular means is the preferred method inmost patients. Despite its popularity, questions remain about the long-term efficacy anddurability. Proximal migration and endoleak are associated with significant morbidity andmortality, and are two of the most important factors in achieving a successful outcome. Thetechnology associated with endovascular grafts continues to evolve rapidly, as does ourunderstanding of ideal deployment techniques. Both can impact the incidence of proximalmigration as well as endoleak and must be optimized to achieve ideal clinical outcomes.Semin Vasc Surg 22:201-206 © 2009 Published by Elsevier Inc.
DTmpfm1d“ldoaqtpdmmRGsmt(flficp
NDOVASCULAR REPAIR OF aortic aneurysms (EVAR)was first described by Parodi et al in 1991,1 and since
hen it has been embraced as a minimally invasive alternativeo open abdominal aortic aneurysm (AAA) repair in patientsith suitable anatomy. Because of lower rates of operativeortality and perioperative complications, the option of local
nesthesia, and faster recovery times, EVAR may be the pre-erred intervention for many patients. Knowledge of theathophysiology and forces that lead to migration is centralo its prevention, diagnosis, and treatment. Poor tissue incor-oration of the endograft, pulsatile blood flow, and limitedxation lengths at the proximal and distal ends of the deviceay contribute to downward displacement of all endografts.s an end result, migration can lead to repressurization of theneurysm sac, type I endoleak, aneurysm growth, and evenupture. Appropriate patient selection (based on prospectivetudies of approved devices) coupled with accurate graft de-loyment can lead to excellent results, with mortality rates2% and freedom from aneurysm rupture, aneurysm-re-
ated deaths, and conversion �95%.2-4 Our aim is to helpnderstand these issues with regard to proximal migrationnd endoleaks, and what can be done to minimize their im-act on patient outcomes. The choice of the appropriate de-ice for a repair as well as optimizing deployment techniquesre dependent on the implanting physician, but industry alsoas a vested interest in minimizing these complicationshrough design of better endografts.
ection of Vascular Surgery, Department of Surgery, Washington UniversitySchool of Medicine, St Louis, MO.
ddress reprint requests to Luis A. Sanchez, MD, Section of Vascular Sur-gery, Department of Surgery, Washington University School of Medi-cine; Campus Box 8109-Surgery, 660 South Euclid Avenue, St. Louis,
fMO 63110. E-mail: [email protected]
895-7967/09/$-see front matter © 2009 Published by Elsevier Inc.oi:10.1053/j.semvascsurg.2009.07.013
efining Proximal Migrationhere is no general agreement as to how far a device has toove in order for it to be considered to have migrated. Re-orts have ranged from any movement to as much as 10 mmrom its original deployment site to meet the definition ofigration. Reporting standards were initially described in
997 to help define immediate and midterm success of en-ografting and did not define a distance that qualified asfixation device failure.”5 The Steering Committee of the Life-ine Registry of Endovascular Aneurysm Repair defined en-ograft migration as the longitudinal movement of the graftr attachment system for a distance of �5 mm relative tonatomic landmarks determined before discharge.6 Subse-uently, the Society for Vascular Surgery/American Associa-ion for Vascular Surgery Committee for Reporting Standardsublished a description for migration in the reporting stan-ards for EVAR in 2002. This document defined migration asovement of �10 mm relative to anatomic landmarks or anyigration leading to symptoms or requiring intervention.7
ecognizing that there was some degree of inter-CT variance,reenberg et al8 went on to propose that proximal migration
hould be defined with respect to the origin of the superioresenteric artery as displacement of �10 mm, or more than
wo times the reconstructed resolution of the imaging studywhichever is less). Adherence to this definition, which dif-ered from previously published reporting standards, al-owed differentiation of the specific mechanisms of deviceailure. In their series, by Society for Vascular Surgery/Amer-can Association for Vascular Surgery standards, 24 of 704onsecutive patients had migration. Image analysis with ap-lication of the revised definition confirmed fixation system
ailure with respect to the native arterial system in only 12201

(vdasit
RMcfaGtstvagmmtoleiBw
APTma(te1fspfifmtrgsadagp6t
tmgwpsmc
PSpDotgplthSddncsswc.mtt(ma
ffilileagttdbiic
DTldn
202 B. Thomas and L. Sanchez
50%) of the 24 patients. The authors felt that informationiewed in this context would aid in the understanding ofevice strengths and weaknesses, potentially improve patientssessment, and encourage design modifications to addresspecific aspects relating to fixation failure, in addition to be-ng a more accurate way to consistently assess graft migra-ion.
easons for Migrationigration has been described in all current endografts, in-
luding early unibody designs, modular configurations, in-rarenal fixation, suprarenal fixation, active fixation, as wells endografts that have longitudinal columnar support.9-13
rafts with a unibody design with a bifurcation that sits onhe native aortic bifurcation may not fully migrate, but cantill fail at the proximal attachment site in similar ways. Mul-iple factors have been postulated to predict and affect endo-ascular graft migration. Patient selection, aortic neck andneurysm morphology, characteristics of individual endo-rafts, accuracy of deployment, postoperative neck enlarge-ent, and endoleak have all been shown to contribute toigration and proximal attachment failure. While most of
he factors have to do with various anatomic issues at the timef implantation, Mohan et al14 created a mathematical modelooking retrospectively at 2,862 patients who had 99 type Indoleaks and found that persistent hypertension and smok-ng may contribute to late changes in aneurysm morphology.oth may represent clinical factors significantly associatedith stent-graft migration.
natomyroximal Neck Fixation and Lengthhe length of the proximal neck above the aneurysmal seg-ent of the aorta is one of the key components in evaluatingpatient for endoluminal treatment. Instructions for use
IFU) for most devices call for 15-mm neck lengths, althoughhe Talent graft is approved for 10 mm currently. The An-uRx device (Medtronic, Santa Rosa, CA) initially required0 mm, but was later increased to 15 mm because of concernor migration and proximal attachment failure. A prospectivetudy by Zarins et al13 using the AneuRx device evaluated 94atients with migration (of 1,119 treated) and both proximalxation length and renal artery to stent-graft distance wereound to be independent risk factors for migration. Further-
ore, each millimeter increase in length of fixation decreasedhe risk of migration by 2.5% and each millimeter increase inenal artery to stent-graft distance increased the risk of mi-ration by 5.8%.13 Similar rates of increased migration withhorter proximal necks have been reported.13,15-17 Fulton etl15 have published results from a prospectively maintainedatabase and reported that patients with unfavorable necknatomy (outside the IFU for the AneuRx device) had a mi-ration rate of 24% and 42.1% at 2 and 4 years. By contrast,atients treated inside the IFU had migration rates of 0% and.1% at 2 and 4 years. Tonnessen et al17 looked at 235 pa-
ients comparing AneuRx and Zenith grafts and found that lhe preoperative neck length was shorter in patients withigration (22.1 � 2.1 mm v 31.2 � 1.2 mm; P � .02). Age,
ender, aneurysm diameter, neck diameter, and type of graftere not found to be associated with migration. These re-orts suggest that the effective proximal aortic neck (area ofeal and sometimes attachment) is critical and should beaximized by deploying the covered portion of the stents as
lose to the lowest renal artery as possible.
roximal Neck Angulationignificant aortic neck angulation also seems to predisposeatients to problems after EVAR. Currently, US Food andrug Administration�approved devices require either �60r �45 degree of neck angulation relative to the long axis ofhe aneurysm. Angulation effectively reduces fixation length,raft wall apposition, and increases the downward force ap-lied to an endograft. Albertini et al18 found that neck angu-
ation was the variable that had the most significant associa-ion with type Ia endoleak and migration. This study,owever, was conducted using 184 homemade grafts. Later,ternberg et al described 81 patients treated with AneuRxevices during the trial that were classified into mild (�40egrees), moderate (40-59 degrees), or severe (�60 degrees)eck angulation.19 They found that early adverse events, in-luding death (P � .0007) and need for acute open conver-ion (P � .0007), were significantly greater in patients withevere aortic neck angulation (20% v 0%) when comparedith mild or moderate angulation. Late adverse events, in-
luding aneurysm expansion (P � .034), device migration (P �013), and type I endoleak (P � .033) were all significantly
ore common in patients with moderate or severe angula-ion when compared with those patients with mild angula-ion. The need for a secondary procedure increased fourfold5% v 18-20%) when comparing patients with mild versusoderate or severe angulation, but these differences did not
chieve statistical significance (P � .142).The addition of suprarenal fixation mechanisms can be
ound in both the Talent and Zenith devices. These proximalxation systems are based on principles of increased fixation
ength and fixation to a less diseased segment of the aorta toncrease positional stability of the graft. Robbins et al20
ooked at 289 patients treated with the Talent graft and cat-gorized them into one of four groups according to their neckngle: I (0-10 degrees); II (11-39 degrees); III (40-59 de-rees); or IV (60-85 degrees). Increasing aortic neck angula-ion was not associated with increased adverse outcomes inhe first 12 months with the Talent stent graft. The Aorfixevice (Lombard Medical, Oxfordshire, UK), with its flexibleut fully supported main body, is specifically being evaluated
n severely angulated necks (�60 degrees) and will providenteresting insights into the treatment of patients with thishallenging anatomy.
iameter of Proximal Neckhe diameter of the proximal neck may be predictive of prob-
ems associated with EVAR. Cao et al identified an initial neckiameter of �25 mm as an increased risk for development ofeck dilatation in the future.9 Limited data has been pub-
ished in the case of devices �28 mm in proximal diameter.

GZdlrdciw
PAwgotamatpcfpofcmh
smalca
PTboc
iratdtfwaeno
GHIgAtgnocbsTidrecbgcwtio
OTttbEetcdcumtms
F
Proximal migration and endoleak 203
oodman et al published their early experience with 36-mmenith devices and their results were comparable with smallerevices.21 In recent years, industry has been developing
arger proximal devices, with 36 mm being the largest infra-enal device, and operators have been using thoracic en-ograft components as proximal cuffs in order to treat diffi-ult patients with large neck diameters. It remains to be seenf results in these patients will differ significantly from thoseith smaller necks.
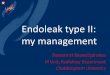
roximal Neck Configurationlbertini et al published a series of 184 patients implantedith a custom graft and reviewed their outcomes after cate-orizing them into several categories based on neck anat-my.18 The goal of the study was to analyze the anatomy ofhe neck in order to find which variables were significantlyssociated with type I endoleak and graft migration. Theyeasured the diameter of the neck at the level of the renal
rteries, at the distal neck just before the aneurysmal dilata-ion, and in between these two levels. They then classified allatients into one of the categories shown in Figure 1. Theonclusion of this study was that different adverse anatomicaleatures of the proximal neck did not have a significant im-act on device migration and endoleak. In this specific groupf patients, neck angulation seemed to be the most importantactor. When attempting to draw comparison to commer-ially available grafts, it should be noted that these home-ade grafts included the addition of four lateral attachmentooks and barbs.In clinical experience with approved devices, conical
hapes have been associated with an increased risk of distaligration, while other neck abnormalities have been associ-
ted with an increased risk of type Ia endoleaks. Endovascu-ar devices placed in these nonparallel aortic necks should beonsidered at higher risk of long-term failure at the proximalttachment site.
roximal Neck Dilatationhe role of late aneurysmal neck dilatation after EVAR haseen the subject of ongoing debate.11,17,22-27 A recent reviewf the literature by Diehm et al22 highlighted some of theonflicting information that has been published about both
bigure 1 Neck anatomy.
ncidence and adverse outcomes associated with late aneu-ysmal neck dilatation. One thing is certain, however, if theortic neck continues to expand after EVAR, then the long-erm durability of the repair is in question. Once the neckiameter exceeds that of the implanted graft, proximal fixa-ion and seal are compromised and the patient is again at riskor rupture. Late aneurysmal neck dilatation was associatedith graft migration in up to 35.3% of patients in one series,28
nd was identified as an independent predictor of type Indoleak and need for secondary intervention.27 Large aorticecks may be at higher risk for dilatation as the aortic wall isften more diseased and weaker.27
raft Designistory
n the United States, the two first commercially availablerafts were the Ancure (Guidant, Indianapolis, IN) and theneuRx endograft systems. The two devices had two dis-
inctly different designs that have influenced subsequentrafts in several ways. The other approved endografts, Ze-ith, Excluder, Talent, and Powerlink all share some featuresf both of these two grafts. The Ancure graft was designed tolosely resemble a surgical graft. It was constructed of a uni-ody bifurcated polyester graft with only proximal and distaltent support at the attachment sites and active hook fixation.he AneuRx graft is modular, requiring a contralateral dock-
ng limb, and is fully supported by a nitinol framework. Theevice, however, uses no barbs or hooks for fixation, butelies on the radial force and column strength of the stents tonsure adequate fixation and seal. The device was well-re-eived because of its smaller profile and ease of deployment,ut long-term data demonstrated a significantly higher mi-ration rate, which was associated in part with the deviceharacteristics and in part with the suboptimal anatomy inhich it was used in many cases.9,11,17 Subsequent modifica-
ion to the AneuRx device have made the device less rigid andmproved deployment techniques have no doubt improvedn these previous results.
ther Currently Available Deviceswo other devices enjoy widespread use in the United States
oday. Both the Excluder and the Zenith share some aspect ofhe AneuRx’s modular design as well as some version of thearbs and/or hooks of the Ancure for proximal fixation. Thexcluder requires a single docking limb and is constructed ofxpanded polytetrafluoroethylene (ePTFE). The porosity ofhe original ePTFE and related lack of sac shrinkage in someases have been eliminated with material modifications. Ad-itionally, the device has proximal caudally directed barbs toomplement its fixation. The Zenith graft extended the mod-lar design and has two docking limbs. The proximal deploy-ent of the Zenith also has a staged approach with the use of
rigger wires, which allows for more control during deploy-ent. The Zenith was also the first device to feature a bare
uprarenal stent at the proximal end of the graft containing
arbs for additional proximal fixation.
difnmd“m
tonad
LDZtewgaeg5aim
CBpcwwddveRct
DDtcitwifTm
aO�sttswTostat
IAssddncdlgVahwoMdhra31wemg7(adtisahtmt
204 B. Thomas and L. Sanchez
Another device, the Endologix Powerlink graft, was intro-uced about 5 years ago. Like the Ancure graft, the Powerlink
s a unibody construction. It is made of ePTFE but of a dif-erent type than the original Excluder. Although not origi-ally designed with this in mind, the graft is now deployed toake use of “anatomic fixation.” Basically, this involves theeployment of the graft so that the endograft bifurcationsits” on the aortic bifurcation and acts as a barrier to caudaligration of the entire graft.More recently, the Talent endograft became available in
he US market. The graft has been in widespread clinical useutside of the United States, but lacked the clinical trial dataecessary for US approval until April of 2008. This device hasbare suprarenal stent, but no hooks or barbs and a modularesign like the Excluder and AneuRx grafts.
essons Learnedeployment Techniques
arins et al found that low deployment of the graft and,herefore, short proximal fixation length were predictors ofndograft migration.13 Multiple reasons for low deploymentere postulated, including suboptimal imaging (quality, an-ulation, lack of magnified views, uncompensated parallax)nd downward displacement of the main body during deliv-ry. For each millimeter increase in the distance of the stentraft below the renal artery, the risk of migration increased by.8% in their analysis. It is for this reason that when patientnatomy already limits the amount of neck available for prox-mal fixation and seal, imaging and devices that allow the
ost accurate deployment are preferred.
ontrol of Orientationeing able to control the orientation of a device during de-loyment would improve the ability to deploy the device aslose to the renal arteries as possible in all planes of view. Thisould allow for the longest proximal seal zone in patientsith angulated necks and suboptimal anatomy. To date, noevice has the ability to completely control the orientationuring deployment, but it is a characteristic that would beery useful in future devices. Some devices currently undervaluation worldwide, like the Anaconda (Sulzer Vascutek,enfrewshire, Scotland) and the Aorfix devices, have in-reased control of the device orientation during deploymento improve deployment accuracy.
evice Oversizingata from the EUROSTAR registry suggest that the rate of
ype I endoleak diminishes as the amount of oversizing in-reases from 0 to 20%. Increased risk of type I endoleaks withnadequate oversizing has been emphasized by several inves-igators. Mohan et al14 found that the risk of type I endoleaksas substantially increased with oversizing of only 10%. Us-
ng a model derived from these clinical data, they predictedewer type I endoleaks with 10% to 20% device oversizing.he IFU of most manufacturers are in line with these recom-
endations. However, oversizing �20% has been postulated rs beneficial in patients with difficult aortic neck anatomy.n the other hand, Conners et al11 found an association of20% device oversizing with late aortic neck dilation and
ubsequent endograft migration. Based on available informa-ion a policy of 10-20% oversizing of the main body appearso be appropriate. We tend to favor 15% to 20% when pos-ible, but devices with limited radial force, like the Excluder,ill not tolerate as much oversizing without graft infolding.he same can be said for oversizing of the iliacs, where 10%versizing is probably ideal. In this location, especially inmall external iliac arteries, �20% oversizing may leado limb stenosis and occlusion. Larger oversizing can bechieved in ectatic common iliac arteries with “bell bottom”echniques.
deal Proximal Fixationlthough early devices had relatively high failure rates29,30,econd-, or third-generation endografts appear to demon-trate better results.2-4,31 The “gold standard” to which everyevice is compared is a sutured anastomosis. Resch et alesigned a method to evaluate the longitudinal tractioneeded to disrupt various endograft’s proximal fixation in aadaveric aorta.32 While 150 Newtons (N) was required toisrupt a sutured anastomosis, all endografts required much
ess (six times less for even the strongest endograft). Theroup tested included the Ancure, Talent abdominal, Zenith,anguard (Boston Scientific, Natick, MA), and a Palmaz stentttached to a Parodi device. In their model, stent grafts withooks or barbs required more force to dislodge than thoseithout. Of those tested, the Zenith required the most force,n average (24 N), while the Talent required the least (4.5 N).alina et al33 conducted a similar study. Sixteen to 24 mm
iameter grafts were deployed inside cadaveric aortas. One-undred and thirty-seven stent-graft deployments were car-ied out with modified self-expanding Z-stents with no hooksnd barbs (n � 75), 4- to 5-mm long hooks and barbs (n �9), 8- to 10-mm�long strengthened hooks and barbs (n �9), or hooks only (n � 4). Increasing longitudinal tractionas applied to determine the displacement force needed to
xtract the stent grafts. They found that the median displace-ent force needed to extract grafts anchored by the first stent
roup was 2.5 N (range, 2.0-3.4), in the second stent group.8 N (range, 7.4-10.8), and in the third stent group 22.5 Nrange, 17.1-27.9) (P � .001). Both hooks and barbs addednchoring strength. During traction, the weaker barbs wereistorted or caused intimal tears. The stronger barbs engagedhe entire aortic wall. The radial force of the stents had nompact on fixation, while aortic calcification and graft over-izing had marginal effects. The authors concluded that barbsnd hooks increased the fixation tenfold, but the radial forcead no impact. To replicate the sutured surgical attachment,he Aptus (Aptus Endosystems, Sunnyvale, CA) device usesultiple transaortic spiral staples distributed circumferen-
ially along the proximal attachment site. The device is cur-
ently under trial in the United States.
DTwloeepctTpiEsuspofitftai(amfitimimamioatt(ati
CSdwwdIsdn
prvaLisgbtspsb
R
1
1
1
1
1
1
1
Proximal migration and endoleak 205
istal Fixationhe positional stability of the entire stent graft is strongesthen the distal end of the stent graft is implanted in nondi-
ated arteries. Published series suggest that increased lengthf iliac fixation can contribute to the proximal stability of anndograft.34-36 Parodi et al’s initial description of six tubularndografts had only proximal attachment.1 Retrograde sacerfusion (type 1b) continued to leave patients at a signifi-ant risk of rupture. Additionally, the unattached end ofhese tube grafts is prone to migrate back into the aneurysm.he distal aorta is a suboptimal distal attachment site in mostatients and can lead to both early and late failures due to
nadequate length, mural thrombus, and heavy calcification.arly reports suggested that durability of these aorto-aortictents were limited37,38 and should be avoided except in un-sual anatomical circumstances. Bifurcated grafts are nowtandard and have the advantage of using distal fixationoints in the common iliac arteries, which adds a longer zonef fixation. The importance of the length of iliac fixation wasrst reported by Heikkinen in 2006.35 The authors reviewedhe outcomes of 173 patients treated from 1996 to 2003 andollow-up computed tomography scans were reviewed to de-ermine the proximal aortic and distal iliac fixation lengthsnd the proximity of the distal end of the stent graft to theliac bifurcation. Patients were grouped according to good�15 mm), intermediate, or bad (�10 mm) aortic fixationnd good (iliac fixation length �25 mm and iliac limbs �10m from iliac bifurcation), intermediate, or bad (�25 mmxation length) iliac fixation. Migration was seen in 17 pa-ients (�10 mm). Patients with no migration had a greaterliac fixation length (30 mm) than those with migration (22
m), and the distal ends of the iliac limbs were closer to theliac bifurcation (15 mm) than in patients with migration (25
m). Patients with no migration also had a greater proximalortic fixation length (23 mm) than migration patients (13m). There were no migrations among patients with good
liac fixation, whether aortic fixation was good, intermediate,r bad. Among patients with bad/intermediate iliac and goodortic fixation, there were 5 (9%) of 58 patients had migra-ions. Patients with both bad/intermediate iliac and bad/in-ermediate aortic fixation had the highest migration rate23%). In general, for all available devices, a longer seal andttachment zone is associated with a lower risk of limb re-raction and type 1 endoleaks while for fully-supported graftst also increases the stability of the implanted device.
onclusioneveral conclusions can be drawn regarding proximal en-oleak and graft migration. First, it is probably true thathen dealing with a long, straight neck, any available deviceill have good and comparable results. Differences from oneevice to another become more important in other situations.n short necks, a transrenal device is a better choice. In theseituations, where every millimeter of neck is important, aevice with a very accurate deployment is critical. In large
ecks, transrenal devices are also preferred in view of the 1otential for late neck dilatation and utilization of the supra-enal aorta for fixation. Transrenal fixation may also be ad-antageous in necks with a reverse taper or with thrombus. Inngled necks, no approved device will likely perform well.ong angled necks may be better suited for devices with
nfrarenal attachment. Ideal deployment of an appropriatelyelected endograft for a given anatomical situation can lead toood long-term results. However, when one begins to com-ine problematic anatomic characteristics in the same pa-ient, it can often lead to long-term endograft failure. Openurgical repair is still the best treatment option for complexatients until better endovascular devices, ie, infrarenal, tran-renal, fenestrated, and branched devices, are evaluated andecome more available.
eferences1. Parodi JC, Palmaz JC, Barone HD: Transfemoral intraluminal graft im-
plantation for abdominal aortic aneurysms. Ann Vasc Surg 5:491-499,1991
2. Cook Medical: Zenith AAA Endovascular Graft Five-Year User Report2008. Available at http://www.cookmedical.com/ai/content/mmedia/Zenith5year.pdf. Accessed on January 28, 2009
3. Endologix: Endologix Powerlink System 2007 Annual Clinical Update.Available at http://www.endologix.com/fls/ClinicalUpdate07Web.pdf.Accessed on January 28, 2009
4. Gore: Annual Clinical Update: GORE EXCLUDER AAA Endoprosthe-sis. Available at http://www.goremedical.com/en/file/AH1406.pdf. Ac-cessed on January 28, 2009
5. Ahn SS, Rutherford RB, Johnston KW, et al: Reporting standards forinfrarenal endovascular abdominal aortic aneurysm repair. Ad HocCommittee for Standardized Reporting Practices in Vascular Surgery ofThe Society for Vascular Surgery/International Society for Cardiovas-cular Surgery. J Vasc Surg 25:405-410, 1997
6. Lifeline Registry: Collaborative evaluation of endovascular aneurysmrepair. J Vasc Surg 34:1139-1146, 2001
7. Chaikof EL, Blankensteijn JD, Harris PL, et al: Reporting standards forendovascular aortic aneurysm repair. J Vasc Surg 35:1048-1060, 2002
8. Greenberg RK, Turc A, Haulon S, et al: Stent-graft migration: a reap-praisal of analysis methods and proposed revised definition. J EndovascTher 11:353-363, 2004
9. Cao P, Verzini F, Zannetti S, et al: Device migration after endoluminalabdominal aortic aneurysm repair: analysis of 113 cases with a mini-mum follow-up period of 2 years. J Vasc Surg 35:229-235, 2002
0. Chuter TA, Wendt G, Hopkinson BR, et al: European experience witha system for bifurcated stent-graft insertion. J Endovasc Surg 4:13-22,1997
1. Conners MS 3rd, Sternbergh WC 3rd, Carter G, Tonnessen BH, Yo-selevitz M, Money SR: Endograft migration one to four years afterendovascular abdominal aortic aneurysm repair with the AneuRx de-vice: a cautionary note. J Vasc Surg 36:476-484, 2002
2. England A, Butterfield JS, Jones N, et al: Device migration after endo-vascular abdominal aortic aneurysm repair: experience with a talentstent-graft. J Vasc Interv Radiol 15:1399-1405, 2004
3. Zarins CK, Bloch DA, Crabtree T, Matsumoto AH, White RA, FogartyTJ: Stent graft migration after endovascular aneurysm repair: impor-tance of proximal fixation. J Vasc Surg 38:1264-1272, 2003
4. Mohan IV, Harris PL, Van Marrewijk CJ, Laheij RJ, How TV: Factorsand forces influencing stent-graft migration after endovascular aorticaneurysm repair. J Endovasc Ther 9:748-755, 2002
5. Fulton JJ, Farber MA, Sanchez LA, et al: Effect of challenging neckanatomy on mid-term migration rates in AneuRx endografts. J VascSurg 44:932-937, 2006
6. Sampaio SM, Panneton JM, Mozes G, et al: AneuRx device migration:incidence, risk factors, and consequences. Ann Vasc Surg 19:178-185,2005
7. Tonnessen BH, Sternbergh WC 3rd, Money SR: Mid- and long-term

1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
206 B. Thomas and L. Sanchez
device migration after endovascular abdominal aortic aneurysm repair:a comparison of AneuRx and Zenith endografts. J Vasc Surg 42:392-400, 2005
8. Albertini J, Kalliafas S, Travis S, et al: Anatomical risk factors for prox-imal perigraft endoleak and graft migration following endovascularrepair of abdominal aortic aneurysms. Eur J Vasc Endovasc Surg 19:308-312, 2000
9. Sternbergh WC, 3rd, Carter G, York JW, Yoselevitz M, Money SR:Aortic neck angulation predicts adverse outcome with endovascularabdominal aortic aneurysm repair. J Vasc Surg 35:482-486, 2002
0. Robbins M, Kritpracha B, Beebe HG, et al: Suprarenal endograft fixationavoids adverse outcomes associated with aortic neck angulation. AnnVasc Surg 19(2):172-177, 2005
1. Goodman M, Lawrence-Brown MM, Hartley D, Allen YB, Semmens JB:Treatment of infrarenal abdominal aortic aneurysms with oversized(36-mm) Zenith endografts. J Endovasc Ther 14:23-29, 2007
2. Diehm N, Dick F, Katzen BT, Schmidli J, Kalka C, Baumgartner I:Aortic neck dilatation after endovascular abdominal aortic aneurysmrepair: a word of caution. J Vasc Surg 47:886-892, 2008
3. Dalainas I, Nano G, Bianchi P, et al: Aortic neck dilatation and en-dograft migration are correlated with self-expanding endografts. J En-dovasc Ther 14:318-323, 2007
4. Litwinski RA, Donayre CE, Chow SL, et al: The role of aortic neckdilation and elongation in the etiology of stent graft migration afterendovascular abdominal aortic aneurysm repair with a passive fixationdevice. J Vasc Surg 44:1176-1181, 2006
5. Tonnessen BH, Sternbergh WC, 3rd, Money SR: Late problems at theproximal aortic neck: migration and dilation. Semin Vasc Surg 17:288-293, 2004
6. Sternbergh WC 3rd, Money SR, Greenberg RK, Chuter TA: Influence ofendograft oversizing on device migration, endoleak, aneurysm shrink-age, and aortic neck dilation: results from the Zenith Multicenter Trial.J Vasc Surg 39:20-26, 2004
7. Cao P, Verzini F, Parlani G, et al: Predictive factors and clinical conse-
quences of proximal aortic neck dilatation in 230 patients undergoingabdominal aorta aneurysm repair with self-expandable stent-grafts. JVasc Surg 37:1200-1205, 2003
8. Napoli V, Sardella SG, Bargellini I, et al: Evaluation of the proximal aorticneck enlargement following endovascular repair of abdominal aortic an-eurysm: 3-years experience. Eur Radiol. Aug 13:1962-1971, 2003
9. Resch T, Ivancev K, Brunkwall J, Nyman U, Malina M, Lindblad B:Distal migration of stent-grafts after endovascular repair of abdominalaortic aneurysms. J Vasc Interv Radiol 10:257-264, 1999
0. Schlensak C, Doenst T, Hauer M, et al: Serious complications thatrequire surgical interventions after endoluminal stent-graft placementfor the treatment of infrarenal aortic aneurysms. J Vasc Surg 34:198-203, 2001
1. Medtronic: Clinical Update Vol. IV: The ANEURX ® Stent Graft Sys-tem. Available at http://www.medtronic.com/physician/aneurx/AneuRx-Clin-Update-with-Brief.pdf. Accessed on January 28, 2009
2. Resch T, Malina M, Lindblad B, Malina J, Brunkwall J, Ivancev K: Theimpact of stent design on proximal stent-graft fixation in the abdominalaorta: an experimental study. Eur J Vasc Endovasc Surg 20:190-195,2000
3. Malina M, Lindblad B, Ivancev K, Lindh M, Malina J, Brunkwall J:Endovascular AAA exclusion: will stents with hooks and barbs preventstent-graft migration? J Endovasc Surg 5:310-317, 1998
4. Benharash P, Lee JT, Abilez OJ, Crabtree T, Bloch DA, Zarins CK: Iliacfixation inhibits migration of both suprarenal and infrarenal aortic en-dografts. J Vasc Surg 45:250-257, 2007
5. Heikkinen MA, Alsac JM, Arko FR, Metsanoja R, Zvaigzne A, Zarins CK:The importance of iliac fixation in prevention of stent graft migration. JVasc Surg 43:1130-1137, 2006
6. Arko FR, Heikkinen M, Lee ES, Bass A, Alsac JM, Zarins CK: Iliacfixation length and resistance to in-vivo stent-graft displacement. J VascSurg 41:664-671, 2005
7. May J, White GH, Waugh R, et al: Adverse events after endoluminalrepair of abdominal aortic aneurysms: a comparison during two suc-cessive periods of time. J Vasc Surg 29:32-37, 1999
8. Moore WS, Kashyap VS, Vescera CL, Quinones-Baldrich WJ: Abdom-inal aortic aneurysm: a 6-year comparison of endovascular versus trans-
abdominal repair. Ann Surg 230:298-306, 1999