Embed Size (px)
Citation preview

Providing Quality Health Care with Providing Quality Health Care with CLAS:CLAS:
A Curriculum for Culturally and Linguistically A Curriculum for Culturally and Linguistically Appropriate ServicesAppropriate Services
Hendry Ton, MD MSHendry Ton, MD MSDirector of EducationDirector of Education
Sergio Aguilar-Gaxiola MD PhDSergio Aguilar-Gaxiola MD PhDDirectorDirector
UCDHS Center for Reducing Health DisparitiesUCDHS Center for Reducing Health Disparities

The TeamThe Team
Office of Multicultural Health, Dept. of Public Office of Multicultural Health, Dept. of Public HealthHealth
Center for Reducing Health Disparities, UCDCenter for Reducing Health Disparities, UCD Sergio Aguilar-Gaxiola, M.D., Ph.D, Director Hendry Ton M.D., M.S., Education Director Marbella Sala, Operations Manager Daniel Steinhart, CLAS Project Coordinator

Cultural differences are not a Cultural differences are not a national burden…national burden…
They are a national resource.They are a national resource.
Sen. Robert F. Kennedy, 1968

Culture is not talked about –- much of it is taken for granted (much like the air we breathe), and what is taken for granted is not discussed. Also, since culture is widely shared, it is uninteresting to talk about what everybody shares. This means, however, that people have little practice in discussing how culture affects their behavior, and so are ill-prepared to explain their culture to others.
Levine, 2001
Definition of CultureDefinition of Culture
Meanings, values, and behavioral norms Meanings, values, and behavioral norms that are learned and transmitted in that are learned and transmitted in society and within social groupssociety and within social groups
Powerfully influences cognition, feeling, Powerfully influences cognition, feeling, and self-conceptand self-concept
Strong impact on diagnostic processes Strong impact on diagnostic processes and treatment decisions and treatment decisions
Source: Guarnaccia, 2006

Culture Counts!Culture Counts!
“The main message of this Supplement—that culture counts—should echo through the corridors and communities of this Nation. In today’s multicultural reality distinct culture and their relationship to the broader society are not just important for mental health and the mental health system, but for the broader health care system as well.”
Source: Culture, Race, and Ethnicity; A Supplement to Mental Health: A Report of the Surgeon General, 2001
Source: Culture, Race, and Ethnicity; A Supplement to Mental Health: A Report of the Surgeon General, 2001

Culture influences:
How consumers/patients communicate and manifest their symptoms
Their style of coping
Their family and community support
Their willingness to seek treatment
Culture Counts!Culture Counts!
Source: Culture, Race, and Ethnicity; A Supplement to Mental Health: A Report of the Surgeon General, 2001
Source: Culture, Race, and Ethnicity; A Supplement to Mental Health: A Report of the Surgeon General, 2001

Language also Counts!Language also Counts!
Language is the core medium for the communication, creation, and transmission of culture
“Given the centrality of talking as a major form of mental health treatment, issues of language and culture appear particularly central in thinking about developing culturally competent mental health services” (Guarnaccia, et al., 1998; p. 424)

DefinitionsDefinitions
RaceRace major groups of people related by major groups of people related by
combination of physical characteristics and combination of physical characteristics and theoretically by ancestrytheoretically by ancestry
EthnicityEthnicity major groups of people with common major groups of people with common
behaviors, culture, beliefs, history and behaviors, culture, beliefs, history and ancestryancestry
Systems of Care as CultureSystems of Care as Culture
Behavioral normsBehavioral norms Clearly defined rolesClearly defined roles Belief system and Belief system and
valuesvalues Written and oral Written and oral
language traditionlanguage tradition Cultural eventsCultural events Changes due to other Changes due to other
cultural systemscultural systems
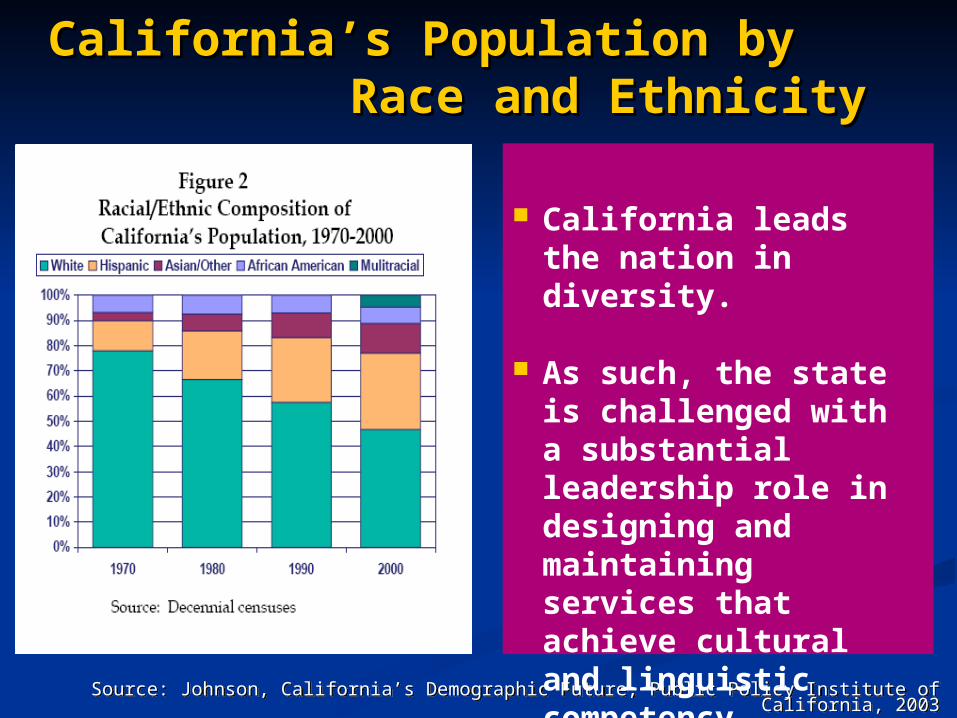
Source: Johnson, California’s Demographic Future, Public Policy Institute of California, 2003Source: Johnson, California’s Demographic Future, Public Policy Institute of California, 2003
California’s Population by California’s Population by Race and EthnicityRace and Ethnicity
California leads the nation in diversity.
As such, the state is challenged with a substantial leadership role in designing and maintaining services that achieve cultural and linguistic competency..

Percent distribution by race/ethnicity
0%
25%
50%
75%
100%
2000 2010 2020 2030 2040 2050
Other
AfricanAmerican
Asian
Latino
White
California Demographic TrendsCalifornia Demographic Trends

““Health DisparitiesHealth Disparities are systemic, avoidable, unfair and unjust
differences in health status and mortality rates and in the distribution
of disease and illness across population groups. They are sustained over time and generations and beyond
the control of individuals”
Adewale Troutman,M.D., M.A., M.P.H.

Racial and ethnic variation in quality of health care that are not due to
Access-related factors
Patient preferences
Clinical needs
Appropriateness of interventions
Recognizes role of SES associated with race/ethnicity as mediators of disparities
Health DisparitiesHealth Disparities
Source: “Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care”, IOM, 2002

Levels of Unmet Needs by Racial/Ethnic Groups
61.23%
68.99%
76.81%70.75%
74.66%
0%
20%
40%
60%
80%
100%
Non-Latino White Latinos Asians African Americans Afro-Caribbean
Not receiving specialty or generalist care in the past 12 months for those with any psychiatricdisorders in the past year

Drug Use by Ethnicity
High-Risk Populations American Indians Alaska Natives Pacific Islanders Multiethnic groups

Binge drinking by adults 18 years and over, Binge drinking by adults 18 years and over, by race/ethnicity, 2000by race/ethnicity, 2000
24.6
18.9
22.2
19.7
12.5
28.3
30.5
13.9
21.8
0 5 10 15 20 25 30 35 40
Percent* Can be of any race.
Note: Binge drinking is defined as having 5 or more drinks at once in the 30 days prior to the survey.
Source: National Household Survey on Drug Abuse, SAMHSA.
2010 target
Asian only
American Indian/Alaska Native only
Black only
White only
Female
Male
More than one race
All adults
Hispanic*
Source: Klein & Proctor, 2007
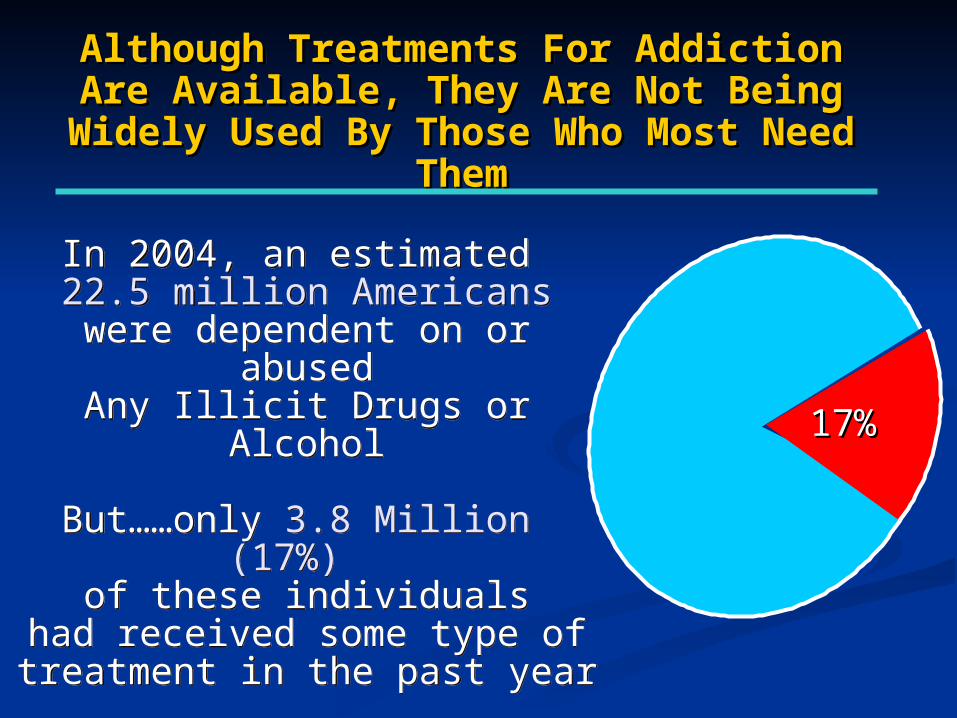
In 2004, an estimated 22.5 million Americans
were dependent on or abusedAny Illicit Drugs or Alcohol
But……only 3.8 Million (17%) of these individuals
had received some type oftreatment in the past year
In 2004, an estimated 22.5 million Americans
were dependent on or abusedAny Illicit Drugs or Alcohol
But……only 3.8 Million (17%) of these individuals
had received some type oftreatment in the past year
Although Treatments For Addiction Are Although Treatments For Addiction Are Available, They Are Not Being Widely Used Available, They Are Not Being Widely Used
By Those Who Most Need ThemBy Those Who Most Need Them
Although Treatments For Addiction Are Although Treatments For Addiction Are Available, They Are Not Being Widely Used Available, They Are Not Being Widely Used
By Those Who Most Need ThemBy Those Who Most Need Them
17%17%

59.3
22.1
13.7
2.2
1.1
1.7
0 10 20 30 40 50 60 70
White
Black
Hispanic
AI/AN
AAPI
Other
Percent
Treatment Admissions, 2005
Source: Office of National Drug Control Policy

Access to TreatmentAccess to Treatment
0
5
10
15
20
25
30
35
40
45
50
Detox Alone ResidentialTreatment
MethadoneTreatment
White
African American
Latino
Source: Ludgren et al, 2001

The Consequences of Drug Abuse and Addiction The Consequences of Drug Abuse and Addiction Disproportionately Affect Minority PopulationsDisproportionately Affect Minority Populations
The Consequences of Drug Abuse and Addiction The Consequences of Drug Abuse and Addiction Disproportionately Affect Minority PopulationsDisproportionately Affect Minority Populations
0%0%
20%20%
40%40%
60%60%
80%80%
100%100%
7070
1111
1212
66
Population Population
6565
1616
1515
44
Drug Abuse/ Drug Abuse/Dependence *Dependence *
WhiteWhite BlackBlack HispanicHispanic OtherOther
Incarcerated for Drug
Offense ***
Incarcerated for Drug
Offense ***
2323
5858
11
1919
Sources: * 2002 NSDUH, DHHS, SAMHSA, 2003. ** CDC HIV/AIDS Surveillance Report 2002. *** Prisoners in 2002, BJS Bulletin, DOJ/OJP, July 2003. (estimated number of sentenced prisoners under State jurisdiction, 2001)
Sources: * 2002 NSDUH, DHHS, SAMHSA, 2003. ** CDC HIV/AIDS Surveillance Report 2002. *** Prisoners in 2002, BJS Bulletin, DOJ/OJP, July 2003. (estimated number of sentenced prisoners under State jurisdiction, 2001)

Epidemiology of ImprisonmentEpidemiology of Imprisonment
General Population
White
69%
Other
6% Hispanic
13%
African
American
12%
Incarcerated
Hispanic18%
White35%
Other3% African
Americn44%
Source: Percentages calculated from data in Table 13, Department of Justice, Bureau of Justice Statistics, "Prison and Jail Inmates at Midyear 2002," April 6, 2003. White and Black excludes Hispanics.
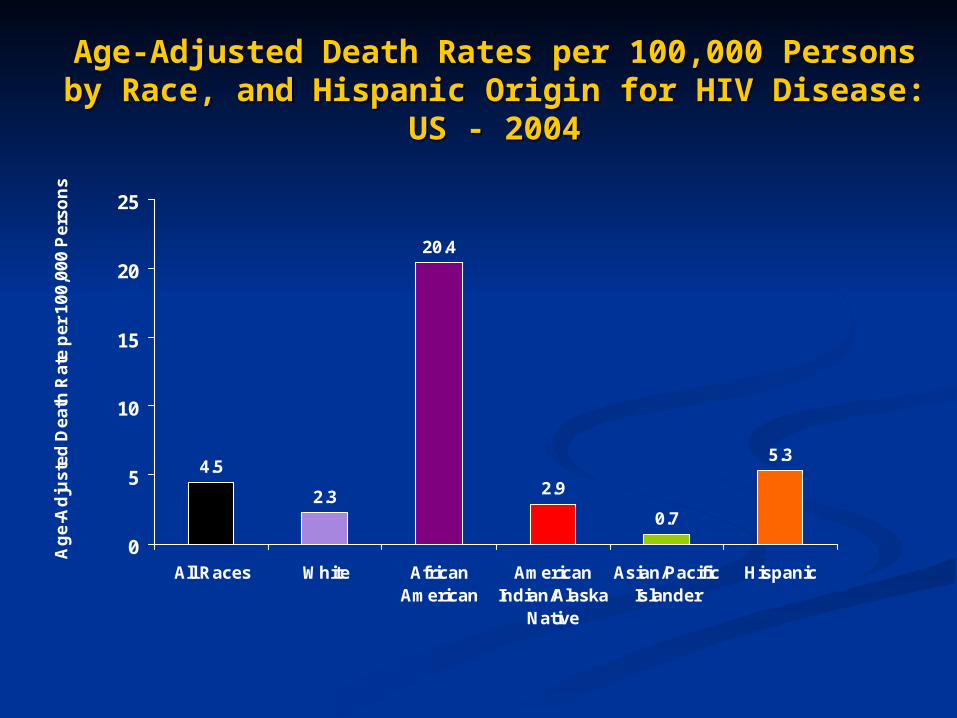
Age-Adjusted Death Rates per 100,000 Persons by Race, Age-Adjusted Death Rates per 100,000 Persons by Race, and Hispanic Origin for HIV Disease: US - 2004and Hispanic Origin for HIV Disease: US - 2004
4.5
2.3
20.4
2.9
0.7
5.3
0
5
10
15
20
25
All Races White AfricanAmerican
AmericanIndian/Alaska
Native
Asian/PacificIslander
Hispanic
Ag
e-A
dju
ste
d D
ea
th R
ate
pe
r 1
00
,00
0 P
ers
on
s
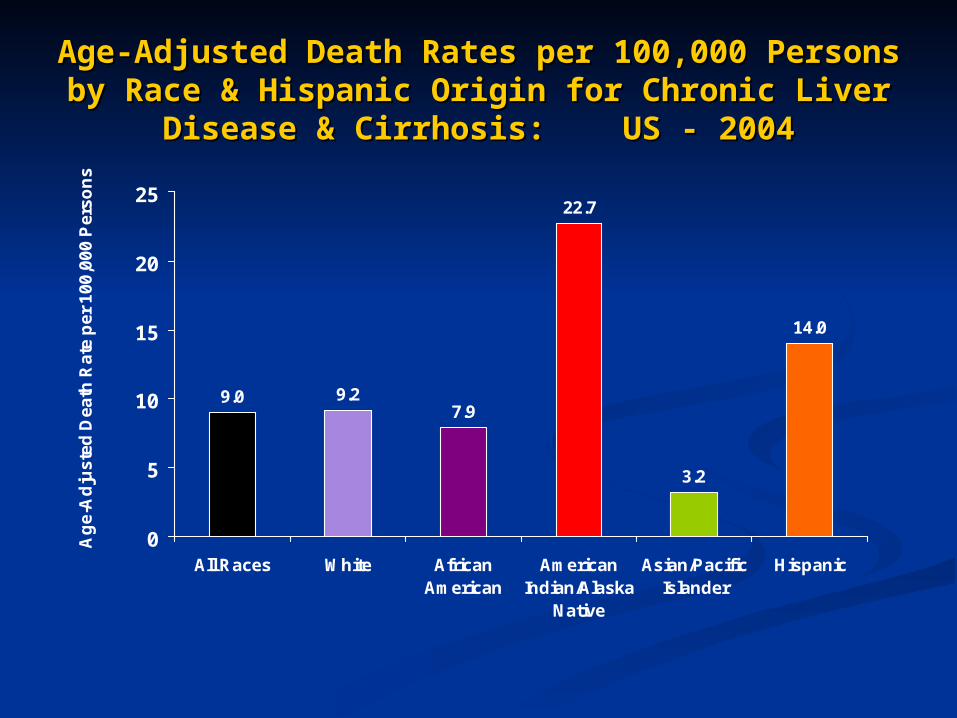
Age-Adjusted Death Rates per 100,000 Persons by Race & Age-Adjusted Death Rates per 100,000 Persons by Race & Hispanic Origin for Chronic Liver Disease & Cirrhosis: Hispanic Origin for Chronic Liver Disease & Cirrhosis:
US - 2004US - 2004
9.0 9.27.9
22.7
3.2
14.0
0
5
10
15
20
25
All Races White AfricanAmerican
AmericanIndian/Alaska
Native
Asian/PacificIslander
Hispanic
Ag
e-A
dju
ste
d D
ea
th R
ate
pe
r 1
00
,00
0 P
ers
on
s

Other Health DisparitiesOther Health Disparities
Homicide Rates between ages 15-44 Homicide Rates between ages 15-44 per 100,000per 100,000
White males: 2.8 - 3.2White males: 2.8 - 3.2 African American males: 11.5 - 14.5African American males: 11.5 - 14.5 Similar disparities for womenSimilar disparities for women
Suicide Rates between ages 15-24 Suicide Rates between ages 15-24 per 100,0000 (1997-per 100,0000 (1997-1999)1999)
White males: White males: 23 to 26 American Indians males: American Indians males: 36 to 42 Similar disparities for women

Black and White Differences in Specialty Procedure Utilization Among Medicare Beneficiaries Age 65 and Older, 1993
Black White Black-to-
White Ratio
Angioplasty (procedures per 1,000 beneficiaries per year)
2.5 5.4 0.46
Coronary Artery Bypass Graft Surgery (procedures per 1,000 beneficiaries per year)
1.9 4.8 0.40
Mammography (procedures per 100 women per year)
17.1 26.0 0.66
Hip Fracture Repair (procedures per 100 women per year)
2.9 7.0 0.42
Amputation of All or Part of Limb (procedures per 1,000 beneficiaries per year)
6.7 1.9 3.64
Bilateral Orchiectomy (procedures per 1,000 beneficiaries per year)
2.0 0.8 2.45
Source: Gornick et al., 1996

Evidence of Racial and Ethnic Evidence of Racial and Ethnic DisparitiesDisparities
Across a wide range of disease areas and clinical servicesAcross a wide range of disease areas and clinical services
Found even when clinical factors, such as stage of disease Found even when clinical factors, such as stage of disease presentation, co-morbidities, age, and severity of disease presentation, co-morbidities, age, and severity of disease are taken into accountare taken into account
Across a range of clinical settings, including public and Across a range of clinical settings, including public and private hospitals, teaching and non-teaching hospitals, etc.private hospitals, teaching and non-teaching hospitals, etc.
Associated with higher mortality among minorities (e.g., Associated with higher mortality among minorities (e.g., Bach et al., 1999; Peterson et al., 1997; Bennett et al., Bach et al., 1999; Peterson et al., 1997; Bennett et al., 1995)1995)
Magnified when taking into account poverty and level of Magnified when taking into account poverty and level of educationeducation

IOM Model: Distinction between a Service IOM Model: Distinction between a Service Difference and a Service DisparityDifference and a Service Disparity
Qu
alit
y o
f H
e al t
h C
are
DifferenceClinical Appropriateness and Patient’s Need and Preferences
The Operation of Healthcare Systems and Legal and Regulatory Climate
Patient-Provider Interaction: Biases, Stereotyping, and Uncertainty
Disparity
No
n-M
ino
rity
Mi n
ori
t y
Populations with Equal Access to Health Care

Figure 1: Importance of the Operation of Community, Figure 1: Importance of the Operation of Community, Patient and Family Level Factors and Socio-contextual Patient and Family Level Factors and Socio-contextual
and Political Forces in Disparitiesand Political Forces in Disparities
Difference
Differences in Need and Patient Preferences
Operation of Healthcare Sys and Provider Organization
Discrimination: Biases, Stereotyping, & Uncertainty
Disparity
No
n-M
ino
rity
Mi n
ori
t y
Source: Gomes and McGuire, 2001, adapted by Alegria et al, 2004
Operation of Community System
Patient and Family Level Factors
Changes in socio-contextual, cultural and political forces
Healthcare Policies/Regulations
Qu
alit
y o
f H
e al t
h C
are
Populations with Equal Access to Health Care
Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999
The perception of illness and disease and their causes varies by culture;
Diverse belief systems exist related to health, healing and wellness;
Culture influences help seeking behaviors and attitudes toward health care providers;
The Challenge for Systems The Challenge for Systems of Care of Care

Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999 Source: Cohen & Goode, National Center for Cultural Competence, 1999
The Challenge for Systems The Challenge for Systems of Care of Care
Individual preferences affect traditional and non-traditional approaches to health care;
Consumers/patients must overcome personal experiences of biases within health care systems, and;
Health care providers from culturally and linguistically diverse groups are under-represented in the current service delivery system.
Source: Federal Register: December 22, 2000, Volume 65, Number 247, pages 80865-80879 www.omhrc.gov/CLAS
Purpose of the CLAS Standards Purpose of the CLAS Standards
Correct disparities in the provision of health services and make these services more responsive to the needs of patients / consumers;
Intended to be inclusive of all cultures and not limited to any particular population group;
Designed to address the needs of racial, ethnic, and linguistic population groups that experience unequal access to health services;
Contribute to the elimination of racial and ethnic health disparities.
Source: Office of Minority Health, U.S. Department of Health and Human Services. (2000).National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health Care. Federal Register, 65(247), 80865-80879.
http://www.omhrc.gov/clas/finalcultural1a.htm

Responding to demographic changes;
Eliminating disparities in the health status of people of diverse racial, ethnic, and cultural backgrounds;
Improving the quality of services and outcomes;
Meeting legislative, regulatory, and accreditation mandates;
Gaining a competitive edge in the marketplace;
Decreasing the likelihood of liability/malpractice claims.
Rationale for Culturally Rationale for Culturally Competent Health Care Competent Health Care
Source: Cohen E, Goode T. Policy Brief 1: Rationale for cultural competence in primary health care. Georgetown University Child Development Center, The National Center for
Cultural Competence. Washington, D.C., 1999.
The National Healthcare The National Healthcare Disparities 2007 ReportDisparities 2007 Report
Key themes:
Disparities still exist Some disparities are diminishing Information is improving
Key findings: Health care continues to improve
at a modest pace Disparities narrowing for many,
except for Hispanics Disparity has widened in both
access to and in quality of care measures
Key themes:
Disparities still exist Some disparities are diminishing Information is improving
Key findings: Health care continues to improve
at a modest pace Disparities narrowing for many,
except for Hispanics Disparity has widened in both
access to and in quality of care measures
OMH State Partnership Grant Program OMH State Partnership Grant Program to Improve Minority Healthto Improve Minority Health
Purpose:
A national strategy to facilitate the improvement of minority health and elimination of health disparities through the development of partnerships with established states and territorial offices of minority health.

OMH State Partnership Grant Program OMH State Partnership Grant Program to Improve Minority Healthto Improve Minority Health
A Partnership between:
CDHS Office of Multicultural Health
UC Davis’ Center for Reducing Health Disparities
Cultural Competency Toolkit/Curriculum Cultural Competency Toolkit/Curriculum Development ProjectDevelopment Project
Primary Goals:
Develop, implement, and evaluate a training curriculum for health service agencies and organizations based on the Culturally and Linguistically Appropriate Service Standards (CLAS)
Disseminate and provide technical assistance in an effort to improve mental health service outcomes for minority populations
Responding to demographic changes;
Eliminating disparities in the health status of people of diverse racial, ethnic, and cultural backgrounds;
Improving the quality of services and outcomes;
Meeting legislative, regulatory, and accreditation mandates;
Gaining a competitive edge in the marketplace;
Decreasing the likelihood of liability/malpractice claims.
Rationale for Culturally Rationale for Culturally Competent Health Care Competent Health Care
Source: Cohen E, Goode T. Policy Brief 1: Rationale for cultural competence in primary health care. Georgetown University Child Development Center, The National Center for
Cultural Competence. Washington, D.C., 1999.
A response to public and private providers, A response to public and private providers, organizations, and government agencies for organizations, and government agencies for culturally and linguistically appropriate standards culturally and linguistically appropriate standards in the provision of health care;in the provision of health care;
Emphasizes the importance of cultural and Emphasizes the importance of cultural and linguistic competence in health care;linguistic competence in health care;
Developed 14 standards which define key Developed 14 standards which define key concepts and issues, and discussion of critical concepts and issues, and discussion of critical implementation issues.implementation issues.
Culturally and Linguistically Appropriate Culturally and Linguistically Appropriate Services (CLAS) StandardsServices (CLAS) Standards
Source: Office of Minority Health, U.S. Department of Health and Human Services. (2000).National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health Care. Federal Register, 65(247), 80865-80879.
http://www.omhrc.gov/clas/finalcultural1a.htm

The 14 Standards are organized by three themes:The 14 Standards are organized by three themes:
Culturally Competent CareCulturally Competent Care Standards 1-3Standards 1-3
Language Access ServicesLanguage Access Services Standards 4-7Standards 4-7
Organizational Supports Organizational Supports Standards 8-14Standards 8-14
CLAS Standards ThemesCLAS Standards Themes
Care compatible with culture and languageCare compatible with culture and language
Recruit, retain, and promote diverse staff Recruit, retain, and promote diverse staff and leadership and leadership
Ongoing education and training in CLAS Ongoing education and training in CLAS delivery.delivery.
Culturally Competent CareCulturally Competent Care

Language assistance services at all points of contact, in Language assistance services at all points of contact, in a timely manner during all hours of operation.a timely manner during all hours of operation.
Verbal and written information for clients about right to Verbal and written information for clients about right to receive language assistancereceive language assistance
Quality assurance that language assistance is of Quality assurance that language assistance is of acceptable qualityacceptable quality
Easily available and understandable patient-related Easily available and understandable patient-related materials and signage in client’s languagematerials and signage in client’s language
Language Access ServicesLanguage Access Services
Written Strategic PlanWritten Strategic Plan that outlines clear goals, policies, that outlines clear goals, policies, operational plans, and management accountability/oversight operational plans, and management accountability/oversight mechanisms to provide culturally and linguistically appropriate services.mechanisms to provide culturally and linguistically appropriate services.
Organizational Self-AssessmentsOrganizational Self-Assessments of CLAS-related activities of CLAS-related activities and are encouraged to integrate cultural and linguistic competence-and are encouraged to integrate cultural and linguistic competence-related measures into their internal audits, performance improvement related measures into their internal audits, performance improvement programs, patient satisfaction Assessments, and Outcomes-Based programs, patient satisfaction Assessments, and Outcomes-Based Evaluations.Evaluations.
Patient Demographic DataPatient Demographic Data on race/ethnicity, and spoken and on race/ethnicity, and spoken and written language are collected in health records, integrated into the written language are collected in health records, integrated into the organization's management information systemsorganization's management information systems
Demographic, Cultural, and EpidemiologicalDemographic, Cultural, and Epidemiological Profile of the CommunityProfile of the Community as well as a needs assessment to accurately plan for and implement as well as a needs assessment to accurately plan for and implement services that respond to the cultural and linguistic characteristics of the services that respond to the cultural and linguistic characteristics of the service area.service area.
Organizational SupportsOrganizational Supports

Community PartnershipsCommunity Partnerships should be developed should be developed utilizing a variety of formal and informal mechanisms to facilitate utilizing a variety of formal and informal mechanisms to facilitate community and patient involvement in designing and implementing community and patient involvement in designing and implementing CLAS-related activities.CLAS-related activities.
Grievance ProcessesGrievance Processes should be culturally and should be culturally and linguistically sensitive and capable of identifying, preventing, and linguistically sensitive and capable of identifying, preventing, and resolving cross-cultural conflicts or complaints by patients.resolving cross-cultural conflicts or complaints by patients.
Public Available InformationPublic Available Information about progress about progress and successful innovations in implementing the CLAS Standards and successful innovations in implementing the CLAS Standards and to provide public notice in their communities about the and to provide public notice in their communities about the availability of this information.availability of this information.
Organizational Supports (2)Organizational Supports (2)
Components of System Components of System ChangeChange
LeadershipLeadership
Leadership is the art of getting someone Leadership is the art of getting someone else to do something you want done else to do something you want done because he wants to do it. because he wants to do it.
You don't lead by hitting people over the You don't lead by hitting people over the head - that's assault, not leadership.head - that's assault, not leadership.
Dwight D. Dwight D. EisenhowerEisenhower
Components of System Components of System ChangeChange
TeamTeam
Group of staff working to implement and Group of staff working to implement and sustain a program.sustain a program.
““Five guys on the court working Five guys on the court working together can achieve more than together can achieve more than five talented individuals who come five talented individuals who come and go as individuals.”and go as individuals.”
Kareem Abdul-JabbarKareem Abdul-Jabbar

Components of System Components of System ChangeChange
Models and ProcessesModels and Processes
Models are approaches that have Models are approaches that have structure or serve as framework for structure or serve as framework for accomplishing goals. Processes are accomplishing goals. Processes are series of related tasks done in sequence series of related tasks done in sequence to achieve the goals.to achieve the goals.

Components of System Components of System ChangeChange
Organizational Systems and CultureOrganizational Systems and Culture
Systems refer to the organization’s processes, Systems refer to the organization’s processes, polices, forms and protocols. Organizational polices, forms and protocols. Organizational culture refers to the shared values of an culture refers to the shared values of an organization as well as how staff relate to each organization as well as how staff relate to each other, how they communicate, and how efforts other, how they communicate, and how efforts are coordinated.are coordinated.
Components of System ChangeComponents of System Change
Data Measurement and Reporting: Data Measurement and Reporting:
This refers to all aspects of data management This refers to all aspects of data management including what data is measured and how it is including what data is measured and how it is collected, stored, processed, updated, and collected, stored, processed, updated, and disseminated.disseminated.

Components of System ChangeComponents of System Change
Education and CoachingEducation and Coaching
This refers to how knowledge is This refers to how knowledge is generated, shared and used. It includes generated, shared and used. It includes aspects such as implementation aspects such as implementation assistance and support and may take the assistance and support and may take the form of seminars, staff development, and form of seminars, staff development, and individual consultationsindividual consultations

Providing Quality Care with Providing Quality Care with CLAS CurriculumCLAS Curriculum
Curricular ApproachCurricular Approach
Participant-centered, strength-based;Participant-centered, strength-based;
Emphasizes collaborative effort;Emphasizes collaborative effort;
Facilitates deeper understanding and creative Facilitates deeper understanding and creative solutions;solutions;
Allows for integration of CLAS standards into the Allows for integration of CLAS standards into the organization’s infrastructure, mission, and organization’s infrastructure, mission, and values.values.
Organizational AssessmentOrganizational Assessment
Needs AssessmentNeeds Assessment Institution as CultureInstitution as Culture
Identify key informants and gate keepersIdentify key informants and gate keepers Cultural Competence LeadersCultural Competence Leaders Institutional LeadersInstitutional Leaders Educational LeadersEducational Leaders
Look for synergy and interdependenceLook for synergy and interdependence Develop reputationDevelop reputation
““Do it right the first time”Do it right the first time”
Make it relevantMake it relevant
Four ModulesFour Modules
1.1. Overview and Foundation Overview and Foundation
2.2. CLAS in Context; Project DevelopmentCLAS in Context; Project Development
3.3. System Change and CLASSystem Change and CLAS
4.4. Project Evaluation and ImplementationProject Evaluation and Implementation
Module I: Overview and FoundationModule I: Overview and Foundation
Overview Overview Challenges of health systems to provide Challenges of health systems to provide
quality care to diverse communitiesquality care to diverse communities Rationale and intent of CLAS standardsRationale and intent of CLAS standards
Institutional Self AssessmentInstitutional Self Assessment Program values and missionProgram values and mission Impact on diverse communitiesImpact on diverse communities How close do we come to meeting the CLAS How close do we come to meeting the CLAS
standards?standards?
Module II: Quality of Care for Module II: Quality of Care for Diverse Patients Diverse Patients
Shifting to a patient-centered perspectiveShifting to a patient-centered perspective Personal experiencesPersonal experiences Case vignettesCase vignettes
Impact of cultural conflicts on quality of Impact of cultural conflicts on quality of carecare Language, acculturation, health Language, acculturation, health
beliefs, health literacy, SES factors, beliefs, health literacy, SES factors, racismracism
Organizational factorsOrganizational factors

Module III: Getting to Know the Module III: Getting to Know the CLAS StandardsCLAS Standards
In-depth study of each CLAS StandardIn-depth study of each CLAS Standard Rationale and intentRationale and intent Strategies to implementStrategies to implement
Review of model programs Review of model programs
Customizing to local settingCustomizing to local setting Assessment of applicability of various Assessment of applicability of various
standards standards Review applicable strategies and modelsReview applicable strategies and models
Session IV: System Change & Session IV: System Change & CLAS CLAS
Leadership and system changeLeadership and system change
Inter-program collaborationInter-program collaboration Leverage resourcesLeverage resources Minimize duplication of effortMinimize duplication of effort Build for synergyBuild for synergy Ripple EffectRipple Effect
Product: Strategic plan to implement CLAS Product: Strategic plan to implement CLAS standardsstandards

Maintaining MomentumMaintaining Momentum
Hold monthly meetingsHold monthly meetings
Develop planDevelop plan
Identify and solve challengesIdentify and solve challenges
Share successful strategiesShare successful strategies
Ownership of the CLAS ProjectOwnership of the CLAS Project

CLAS Implementation CLAS Implementation Evaluation ModelEvaluation Model
BenchmarksBenchmarks Participant:Participant:
Knowledge, Skills, Attitudes regarding health disparities and CLASKnowledge, Skills, Attitudes regarding health disparities and CLAS
Organizational:Organizational: Level of implementation of each of the 14 StandardsLevel of implementation of each of the 14 Standards
OutcomesOutcomes Participant:Participant:
Knowledge, Skills, Attitudes regarding health disparities and CLASKnowledge, Skills, Attitudes regarding health disparities and CLAS Ability to develop and implement CLAS-based improvement projects Ability to develop and implement CLAS-based improvement projects
Organizational:Organizational: Level of implementation of each of the 14 StandardsLevel of implementation of each of the 14 Standards

EvaluationEvaluation
Course EvaluationCourse Evaluation Overall Quality of Curriculum 3.6 out of 4Overall Quality of Curriculum 3.6 out of 4
[1 = poor 2 = fair 3 = good 4 = excellent][1 = poor 2 = fair 3 = good 4 = excellent]
41 out of 45 participants would recommend 41 out of 45 participants would recommend curriculum to colleaguescurriculum to colleagues
Response Rate: 93%Response Rate: 93%

Evaluation by Session
2.9
3
3.1
3.2
3.3
3.4
3.5
3.6
3.7
3.8
Session I Session II Session III Session IV
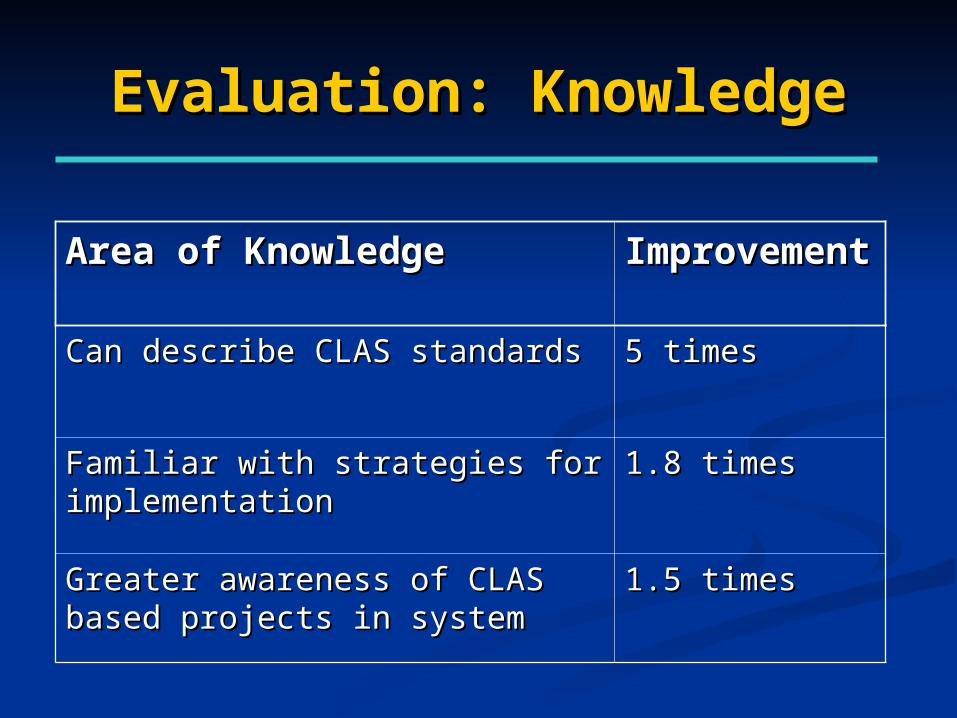
Evaluation: KnowledgeEvaluation: Knowledge
Area of KnowledgeArea of Knowledge ImprovementImprovement
Can describe CLAS standardsCan describe CLAS standards 5 times5 times
Familiar with strategies for Familiar with strategies for implementationimplementation
1.8 times1.8 times
Greater awareness of CLAS based Greater awareness of CLAS based projects in systemprojects in system
1.5 times1.5 times
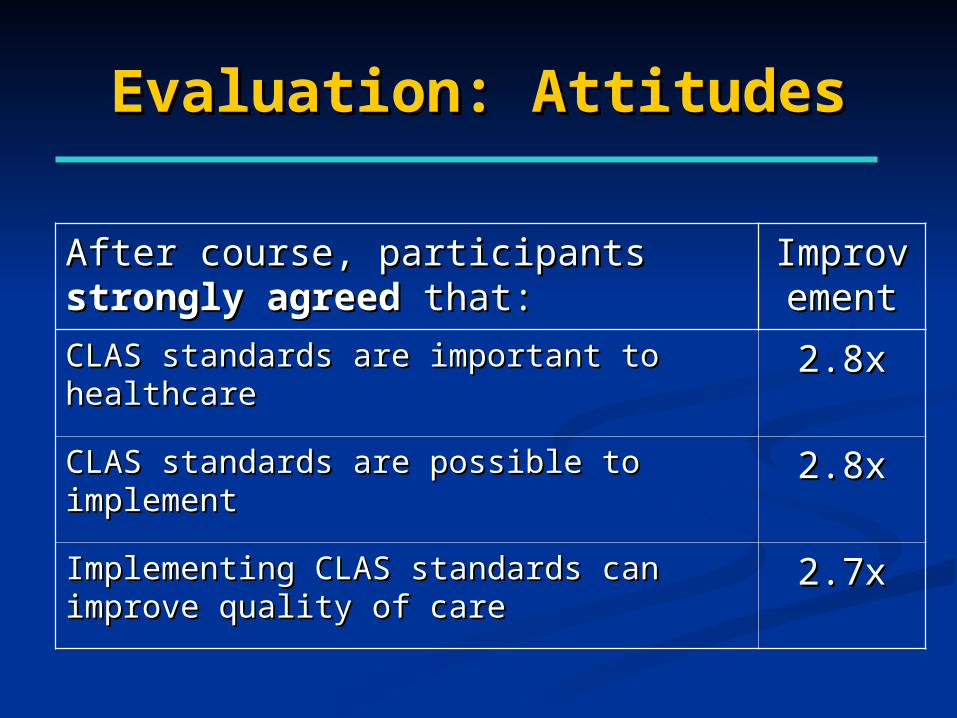
Evaluation: AttitudesEvaluation: Attitudes
After course, participants After course, participants strongly strongly agreedagreed that: that:
ImproveImprovementment
CLAS standards are important to healthcareCLAS standards are important to healthcare 2.8x2.8x
CLAS standards are possible to implementCLAS standards are possible to implement 2.8x2.8x
Implementing CLAS standards can improve Implementing CLAS standards can improve quality of carequality of care
2.7x2.7x
SummarySummary
Working knowledge of CLAS standards;Working knowledge of CLAS standards;
Practical plan for implementation of Practical plan for implementation of CLAS standards;CLAS standards;
Effective coordination for maximal Effective coordination for maximal effect.effect.