-
Prostate Magnetic RChallenges of Im
Ronald Loch, MD, Kathryn FowJoseph Ippolito, MD, PhD, Cary
Sie
technology into an efcient multidisciplinary model ofpatient
care. This article reviews several of the challengesthat
radiologists should be aware of when integrating
identify patients who are appropriate for AS.9-1126There are
many arguments in favor of adding MPP-MRI to the AS algorithm.
Initial studies show thatMPP-MRI can more accurately classify
patients to ASwhen combined with clinical classication schemes(eg,
the D'Amico, Epstein, and Cancer of the ProstateRisk Assessment
systems).10 MPP-MRI may identifytumors and allow for targeted
biopsies, which is
Curr Probl Diagn Radiol 2015;44:2637.& 2014 Mosby, Inc. All
rights reserved.0363-0188/$36.00 +
0http://dx.doi.org/10.1067/j.cpradiol.2014.05.009
From the Mallinckrodt Institute of Radiology, Washington
UniversitySchool of Medicine, St. Louis, MO.Reprint requests:
Ronald Loch, MD, Mallinckrodt Institute of Radiology,510 South
Kingshighway Blvd, St. Louis, MO 63110. E-mail:
[email protected].
Curr Probl Diagn Radiol, January/February 2015screening have
shown increased diagnosis of prostatecancer in screened
populations, leading to increased
increasingly being used to document tumor burden inpatients and
offers a potentially powerful tool to helpprostate MRI into their
clinical practice.
IntroductionProstate cancer is a common cause of cancer
andcancer deaths among men in the United States, with anestimated
233,000 new cases and 29,480 deaths eachyear.1 In recent decades,
screening and diagnosis ofprostate cancer relied on serum
prostate-specic anti-gen (PSA) and digital rectal examination,
followed bytargeted or saturation biopsy for positive
screens.However, PSA screening has become controversial.Recent
randomized trials evaluating the utility of PSAProstate cancer is
among the most common causes ofcancer and cancer deaths in men.
Screening methods andoptimal treatments have become controversial
in recentyears. Prostate magnetic resonance imaging (MRI) is
gain-ing popularity as a tool to assist diagnosis, risk
assessment,and staging. However, implementation into clinical
practicecan be difcult, with many challenges associated withimage
acquisition, postprocessing, interpretation, repor-ting, and
radiologic-pathologic correlation. Although state-of-the-art
technology is available at select sites for target-ing tissue
biopsy and interpreting multiparametric prostateMRI, many
institutions struggle with adapting this newesonance
Imaging:plementation
ler, MD, Ryan Schmidt, MD,gel, MD, and Vamsi Narra, MD
interventions but no difference in prostate cancermortality or
all-cause mortality.2,3 The lack of survivalbenet and added
morbidity associated with interven-tion ultimately led to a grade D
recommendation4
against routine PSA screening by the U.S. PreventiveServices
Task Force (USPSTF).Beyond screening, the optimal treatment of
local-
ized prostate cancer is controversial with studiesdemonstrating
little or no mortality benet whencomparing radical prostatectomy
with observation.5-7
The inability to prospectively identify and
differentiatehigh-risk tumors from indolent tumors, many
times,leads to overtreatment and the psychological stressassociated
with a cancer diagnosis for patients.8
In the wake of the USPSTF recommendation againstroutine PSA
screening and the mounting evidenceagainst radical prostatectomy
for men with low-risktumors, there has been renewed interest in
observa-tional management. In particular, there is
increasingenthusiasm for active surveillance (AS) of
prostatecancer. AS denes monitoring and treatment triggersaimed at
minimizing interventions for indolent can-cers.9 Optimal monitoring
and treatment algorithms forAS are not yet well dened within the
urologycommunity. Gleason score on repeat biopsies, serialPSA
monitoring, and patient preferences play a keyrole in determining
treatment strategy. Multiparametricprostate magnetic resonance
imaging (MPP-MRI) is
-
important to accurately assess tumor grade given thatsaturation
biopsies randomly sample less than 0.5% ofthe gland. Early
retrospective studies have shown thatMPP-MRI may result in removal
of up to 29% ofpatients from AS after conrmatory repeat
biopsy.Likewise, MPP-MRI may provide a high negativepredictive
value for large or high-grade tumors,allowing patients to stay on
AS with more con-dence.11 Table 1 summarizes the potential roles
of
pathologic correlation. This article provides an
imaging (DWI) in addition to acquiring T2-weightedimages
(T2WIs), and more than half of centers useddynamic contrast
enhancement (DCE) in addition toT2WI and DWI. Only 21% of surveyed
centers usedMR spectroscopy, all of which were academic
centers.Guidelines and consensus statements for prostate
MRIacquisition and reporting have been proposed inEurope13-15 but
not yet by a North American society.These guidelines and a thorough
review of theliterature by Hoeks et al16 suggest that MPP-MRI
beperformed with a minimum of DWI and DCE inaddition to T2WI. We
therefore focus our discussionon these 3 techniques. The challenges
of prostate MRIprotocol design are discussed later with reference
tosupportive literature where available. We also discussour
approach and solutions to challenges at our own
both phased-array coil and an integrated endorectal-pelvic
phased-array coil system during the same
TABLE 1. Potential benets of MPP-MRI in ASImprove negative
predictive value of tumor burden assessmentImprove accuracy of
tumor grade determinationReduce unnecessary biopsiesContribute to
accurate assignment of patients to ASProvide a tool to follow up
patients noninvasively once diagnosis isestablished
D
EcS
189Noverview of the role of MPP-MRI in AS as well asthe
challenges associated with its implementation.
Challenges in AcquisitionThere is no uniformly agreed protocol
in the com-munity. In a survey of predominantly academiccenters,
there was a near-even split between acquiringimages using an
endorectal coil at 1.5 T, a pelvicphased-array coil at 3 T, and an
endorectal coil at3 T.12 Nearly all centers performed
diffusion-weighted
TABLE 2. Nominal MR parametersProtocols T2WI
Sequence type Turbo spin echoOptions Phase encoding in
left-right direction
which helps reduce motion artifactfrom rectal peristalsis
TR 4000-6000 msTE 90-120 msFlip angle 180 (4150)Echo train
length 8-16MPP-MRI in AS.In light of the possible clinical utility
of MPP-MRI,
the volume of imaging requests have gone up in manycenters, and
radiologists must be familiar with theperformance and
interpretation of these studies.MPP-MRI can be challenging for many
reasons,including issues related to technical acquisition,
post-processing, interpretation, reporting, and radiologic-Matrix
size 512 512 1Field of view (cm2) 16 16 1Number of averages 4
5Slice thickness (mm) 3 3
NA, not applicable.
Curr Probl Diagn Radiol, January/February 2015examination. The
endorectal coil images showed sig-nicantly improved prospective
diagnostic accuracy(from 59%-83%) and more importantly
specicity(from 62%-98%) of extracapsular extension detected
WI DCE
ho planar imaging Spoiled 3D gradient echopectral fat
saturation, partialFourier acquisition, b 0, 500,and 1000 s/mm2
Acquire T1 map before contrastadministration if a
quantitativeanalysis is desired
1,200 ms Minimal TR9 ms Minimal TE0 6-12A 128 128 256 2566 16 16
16
1-23
27institution. Table 2 shows typical sequence parame-ters. Table
3 shows some of the more commonchallenges encountered with the
various sequencesas well as potential solutions to these
challenges.
Field Strength and Coil SelectionMost academic centers use an
endorectal coil when
imaging at 1.5 T, and most of the literature supportsreasonable
accuracy for staging with this coil selec-tion.12,16 The
performances of endorectal coils andphased-array coils in the same
patient population at1.5 T was prospectively compared by 2
studies.17,18
In 1 study, 81 patients underwent prostate MRI using
-
endorectal coil. Placement requires radiologist pres-
TABLE 3. Challenges and solutionsSequence Challenge
Solutions
itionincrtal mectiotum
ducmotat whole-mount pathologic examination.18 The limi-tation
of this and other studies evaluating endorectalcoil at 1.5 T is
that the focus was on staging and notprospective diagnosis, hence
DWI and DCE sequen-ces were not performed (ie, the accuracy of
MPP-MRIwas not truly tested). At our institution, MPP-MRI at1.5 T
with an endorectal coil is reserved only forpatients who have (1) a
hip arthroplasty or othermaterials that may lead to excessive
artifact at 3 T or(2) MR-conditional surgical devices that may not
besafe at 3 T.Another parameter under debate is whether an
endorectal coil should be used when imaging at 3 T.Initially as
3 T scanners became more widely avail-able, several studies
compared performance of 1.5 Twith endorectal coil and 3 T with
phased-array coil. Intheory, the added signal-to-noise ratio (SNR)
fromimaging at higher eld strength may obviate the needfor an
endorectal coil. Initial studies demonstratedlittle difference in
diagnostic performance between1.5 T with endorectal and 3 T with
phased-arraycoil.19-21 As endorectal coils became available for3 T
systems, the question of coil selection wasrevisited. In a study of
46 men undergoing prostatec-tomy, performance of preoperative MRI
performedwithout and with an endorectal coil was evaluated,with
whole-mount pathologic correlation. The use ofan endorectal coil
improved image quality, tumordetection, and staging performance in
a subgroupanalysis of experienced radiologists.22 Again, this
T2WI Wrap artifact Increase FOV, phase oversample, and posT2WI
Motion artifact Reduce imaging time by parallel imaging,
Consider glucagon injection to reduce recAssign phase-encoding
in the right-left dir
DWI Susceptibilityartifact
Reduce rectal gas with enemas, empty recpatients with hip
arthroplasties
DCE Motion artifact Phase encoding in the left-right direction
resoftware for correction of gross patient
FOV, eld of view.study was focused primarily on staging with
T2WIand did not include DWI or DCE. A more recent studyaimed at
assessing the diagnostic value of MPP-MRI(including DWI and T2WI)
was performed in20 patients with 51 foci of cancer detected
onwhole-mount pathologic analysis.23 The authorsreported
signicantly improved sensitivity and pos-itive predictive value
when using an endorectal coil,with a trend of detecting more small
cancers with the
28ence at the imaging center; the retention balloon mustbe lled
with special media (peruorocarbon or a lessexpensive alternative
such as barium) at 3 T to preventdistortion from gas, and there is
added cost and time tothe overall examination. Additionally, the
coil maydistort the prostate gland, having implications
forradiologic-pathologic correlation and targeting biop-sies, which
are discussed in detail in the subsequentsections. Further
investigation is needed to draw moredenitive conclusions in this
area.
T2-Weighted ImagingT2WI is an essential part of MPP-MRI,
providing
anatomical detail of the entire prostatic gland. Sometypical
sequence parameters are reviewed in Table 2.Fast spin-echo
acquisitions are performed in at least2 planes including the
transverse plane. The transverseimages should be oriented
orthogonal to the long axisof the urethra (although the urethra
curves anteriorly atendorectal coil. Despite early evidence of
equivalence,of the 5 patients with extracapsular extension, 4
weredetected with the endorectal coil and only 1 wasdetected
without the endorectal coil.Although there is some evidence that
suggests the
use of an endorectal coil may improve imagingaccuracy, there are
other considerations to take intoaccount when designing a protocol.
Patient comfortand compliance may be reduced with the use of an
hands out of imaging planeeased echo train lengthotionn to
reduce rectal motion transmitted through the prostatebefore
imaging, displace gas with endorectal coil, and image at 1.5 T
in
es rectal motion artifact, antiperistaltic medications, and
postprocessingionthe level of the verumontanum prohibiting a
trueorthogonal plane throughout). The high-resolutionand small
eld-of-view requirements for this sequencepresent some unique
challenges. The phase-encodingdirection should ideally be oriented
right to left toprevent any motion artifact from rectal peristalsis
to betransmitted through the prostate. If inadequate eld ofview or
phase oversampling is selected, this can resultin wrap artifact or
aliasing such as from the arms
Curr Probl Diagn Radiol, January/February 2015
-
also aid in detection of transitional zone tumors.29
Some typical sequence parameters are reviewed in
values (41000 s/mm2). A major limitation of ultrahighalong the
patient's sides (Fig 1). Because the right-to-left direction is
often the longest dimension in thepelvis, this adds to the length
of the acquisition. Thelength of acquisition is important both for
workowefciency and to help prevent bulk motion, whichtends to
increase along with the time of the acquis-ition. Measures such as
parallel imaging, increasedecho train length, and partial k-space
lling acquis-itions can be implemented to shorten
acquisitionlength, but may come at the expense of decreasedSNR and
increased image blurring. Specic absorp-tion rate (SAR) at 3 T is
another issue, and some
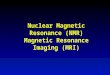
FIG 1. Small eld of view and left-right phase-encoding direction
usedon T2WI increases chances for wrap artifact (indicated by the
arrow) ifprotocol is not optimized. In this case, the patient's
hands werepositioned at the side. The patient's hands were
repositioned. Increas-ing FOV and phase oversampling are other
solutions to eliminatingwrap artifact. FOV, eld of view.vendors
provide solutions to SAR without compro-mising T2 contrast or
adding pauses, such ashyperecho-turbo spin-echo sequences and low
SARradiofrequency pulses.In addition to phase encoding in the
left-right
direction, agents that inhibit peristalsis (eg, glucagon)can be
given at the time of examination to reduce theeffect of rectal
peristalsis. The use of antiperistalticagents in the absence of an
endorectal coil isincompletely evaluated in the literature and is
oftendetermined by radiologist preference and
workowconsiderations.
Diffusion-Weighted ImagingThe addition of DWI to MPP-MRI can
improve
diagnostic accuracy,24,25 indicate information aboutGleason
grade26 and cellular density,27,28 and may
Curr Probl Diagn Radiol, January/February 2015b values (41000
s/mm2) is the relatively poor SNR,especially in the absence of an
endorectal coil. One ofthe initial studies using ultrahigh b values
reported thata b value of 1000 s/mm2 outperformed a b value of2000
s/mm2, but this study was limited by the use of alonger TE in the b
2000 s/mm2 acquisition.30 Subse-quent studies reported improved
performance of DWIacquired with high b values, but they did not
includeADC maps in their comparisons.31 When including
thecorresponding ADC maps, there have been mixedreports.32,33
Although there is no consensus in theliterature, at our
institution, we use 3 b values with amaximum of 1000
s/mm2.Optimization of DWI is perhaps the most impor-
tant component (and hence worth spending the mostacquisition
time on) of the MPP-MRI as it has shownthe highest diagnostic
accuracy.25 DWI in the pelvisis acquired as a free-breathing
sequence as respira-tory motion is not a major factor. Increasing
aver-ages, reducing TE, and optimizing echo spacing andnoise level
are important factors for improving theSNR. Most MRI vendors
provide the suggestedparameters.The greatest limitation of DWI
imaging relates to
echo planar pulse sequence design, making it sensitiveto
artifacts. Susceptibility artifacts related to rectal gasand metal
implants are the most commonly encoun-tered artifacts (Fig 2).
Strategies to reduce suscepti-bility artifact from gas in the
rectum include use ofenemas, instructions to empty the rectum
immediatelybefore imaging, or imaging with an endorectal coil.
Inpatients with hip prostheses, imaging at 1.5 T shouldbe
considered to reduce the associated susceptibilityartifact.
DCE ImagingDetection of prostate cancer with DCE relies on
the
increased vascular permeability of tumor neovascula-ture
typically seen in tumors, and has been shown toadd value to
MPP-MRI. Some typical sequence
29Table 2. DWI requires at least 2 acquisitions withdifferent b
values to calculate an apparent diffusioncoefcient (ADC). The
European guidelines suggestapplying diffusion gradients in 3
orthogonal directionswith b values14 of 0, 800, and 1000 s/mm2.
There havebeen conicting reports regarding the utility of high
b
-
10 seconds has been suggested.13-15 Gadolinium-based contrast is
typically injected via an antecubitalparameters are reviewed in
Table 2. DCE imagingrequires serial fast 3-dimensional (3D)
spoiledgradient-echo acquisitions over a period of approx-imately
4-6 minutes following administration of intra-venous gadolinium
contrast. Differentiation betweenthe vascularity of the tumor and
normal prostatenecessitates a high temporal resolution and
completecoverage of the gland, which comes at the cost ofspatial
resolution and SNR.Assigning optimal parameters can be
challenging
and often requires a compromise between T1 weight-ing, SNR, and
temporal resolution. Imaging for atleast 5 minutes with a temporal
resolution less than
FIG 2. Warped diffusion-weighted image (A) owing to air in
therectum (despite use of KY jelly). Gas in the rectum is a major
hurdle toimaging, as it results in phase distortion. In this case,
a Gleason9 adenocarcinoma (indicated by the arrow) was found in the
middleright peripheral zone on T2WI (B) but obscured on the DWI.
Use of anendorectal coil can displace gas in the rectum. Some
promote the useof KY jelly to displace gas from the rectum.
30vein at 2-4 mL/s, followed by a 20-mL saline ush.Choosing a
minimal TE improves T1 weighting butdecreases the SNR. Increasing
the ip angle increasesT1 weighting but decreases the SNR.
Utilization ofk-space undersampling techniques can help to
achievegood spatial resolution and SNR without loss oftemporal
resolution.34 In a detailed review and scien-tic article by Li et
al,35 the authors suggested using aip angle of twice the optimal
Ernst angle expectedbased on the precontrast images, as the Ernst
anglechanges with the arrival of contrast. In addition to theDCE
images, a T1 map, generated from multiple ipangle T1-weighted
sequences before contrast admin-istration, is required to derive
the relationship betweenvoxel signal intensity on postcontrast
images andgadolinium concentration. This relationship is neces-sary
for quantitative postprocessing.The serial acquisition over a
period of approxi-
mately 4-6 minutes makes DCE images particularlyvulnerable to
motion, including from the rectum,bladder, and gross patient
motion. Most postprocess-ing systems have rigid motion correction
that canrealign images.Interpretation of DCE images may be
intimidating
to some radiologists, especially those without experi-ence in
postprocessing this type of data set. DCEimages can be interpreted
using qualitative, semi-quantitative, or quantitative methods, and
an excep-tional review of these techniques is discussed byVerma et
al.36 There is no consensus regarding theuse of quantitative
methods in routine practice, butthere is support for performing at
least semiquantita-tive analysis.37 The most widely used model
forquantitative analysis is the Tofts model, which calcu-lates
Ktrans, Kep, and Ve. Ktrans represents the trans-fer constant from
the blood plasma space to theextracellular extravascular space. Kep
represents thetransfer constant of contrast in the opposite
direction.Ve represents the volume of the extracellular
extrava-scular space and equals Ktrans divided by Kep. Thismodel
requires an arterial input function (AIF), eitherfrom a region of
interest selection over the arteries inthe patient or a pooled
standardized AIF adjusted forindividual patient factors. Pooled
standardized AIFsare offered with some software packages and can
beadjusted based on the patient's weight and volume ofcontrast
injected. There are several commerciallyavailable and independent
institutional postprocessing
Curr Probl Diagn Radiol, January/February 2015
-
systems for prostate DCE. However, no single methodhas been
tested and shown to be superior. The
eligible for AS, 48.7% of patients with tumorso1 cm in diameter
measured on ADC maps hadcommercially available systems often offer
manymodeling options and differ mostly in their reportingfunctions,
usability, access to technical support, andcost. The decision to
purchase a postprocessing sys-tem should be supported by on-site
testing of thesystem whenever possible to ensure user
preference.
Challenges in Interpretation and ReportingProviding a clinically
meaningful interpretation of aprostate MRI examination begins with
knowledge ofthe patient's clinical history and the indication for
theexamination. Referring urologists may prefer theradiologist
tailoring the interpretation to focus onspecicity and staging
information, such as evaluationfor extracapsular extension in
patients being consid-ered for curative therapies. Alternatively,
in a patientwith rising PSA but negative random biopsies, thereport
should perhaps focus on sensitivity and detect-ing foci of
potential cancer. A multidisciplinaryapproach including the
radiologist, urologist, andpathologist is essential to developing a
reportingsystem that provides this information. The perform-ance of
prostate MRI under different clinical situationshas been
extensively studied and was thoroughlyreviewed by Hoeks et al.16 In
this section, we discussthe typical appearance of prostate cancer,
pitfalls, andcurrent approaches to reporting.
InterpretationThe classic features of prostate cancer include
dis-
crete hypointense lesions on T2WI, diffusion restric-tion on ADC
maps, and brisk enhancement followedby washout on the DCE images.
Signs of extracap-sular extension include asymmetric capsular
bulge,obliteration of the rectoprostatic angle, asymmetry ofthe
neurovascular bundle, and seminal vesicle inva-sion. Figure 3 shows
a tumor demonstrating classicfeatures on T2WI, the ADC map, and
processed DCEimages.There is a growing body of literature to
suggest that
in addition to diagnosis, prognostic information maybe acquired
by MPP-MRI. The T2 intensity of thecancer relative to muscle38 and
its ADC value26
inversely correlate with Gleason grade. The ADCvalue of focal
lesions may also correlate with like-lihood of repeat biopsy
showing adverse histology inlow-risk patients on AS.39 In a study
of patients
Curr Probl Diagn Radiol, January/February 2015insignicant
disease at prostatectomy vs only 24.7%of patients with tumors 41
cm.40 The ability forMPP-MRI to provide this additional information
ispromising and requires further validation.Although the classic
features of prostate cancer are
well documented in the literature, in practice there aremany
sources of error leading to both false-positive andfalse-negative
results.41 T2 hypointensity and possiblefalse-positive reading can
result in patients with pros-tatitis, hemorrhage from prior biopsy,
radiation, orhormonal-deprivation treatment. Wedge-shaped
lesionsand lesions with diffuse extension but no mass effect inthe
peripheral zone have been reported as signs ofbenignity.42 If
MPP-MRI is performed after a recentbiopsy, it should perhaps be
delayed 4-6 weeks to helpmitigate the effects of hemorrhage.
Although biopsycan complicate the interpretation, postbiopsy
hemor-rhage can also unmask a focus of cancer. This isreferred to
as the hemorrhage exclusion sign. Speci-cally, hemorrhage manifest
as T1 hyperintense bloodproducts (ie, methemoglobin) will appear as
hyper-intense on T1WIs and will outline a tumor
appearinghypointense on T2WI. This has been termed thehemorrhage
exclusion sign and has been reported ashighly specic when present
with a positive predictivevalue of 95%-96%.43 An example is shown
in Figure 4.False-negative results are also not uncommonly
encountered. Sparse or diffuse tumors have beenshown to have
signal intensity on T2WI and ADCssimilar to normal peripheral zone
parenchyma.27
Additionally, sensitivity for detection of tumorssmaller than 1
cm3 decreases in tumors with lowerGleason grades (such as Gleason
6).44 It may beargued that some of these are the tumors that do
notmerit intervention.40
The high incidence of benign prostatic hyperplasia(BPH)
complicates assessment of the transitional zoneand deserves special
attention. On T2WI, the presenceof homogeneously low signal,
ill-dened margins,lack of capsule, lenticular shape, and invasion
of theanterior bromuscular stroma have been studied assigns to
discriminate tumors from BPH nodules.45
There have been conicting reports regarding the useof MPP-MRI as
opposed to only T2WI, with somestudies reporting no signicant
improvement in diag-nostic accuracy when DWI and DCE are
added,25,46,47
despite a single study showing the promise of DCE inimproving
accuracy.48 There is, however, a growing
31
-
body of literature to suggest that the use of b values of1000
s/mm2 or greater may improve tumor detectionin the transitional
zone.29,31,49 Further research isneeded to verify the usefulness of
DWI in detectingtransitional zone tumors. In our practice, the T2WI
ismost important when assessing tumors within a regionof BPH.
ReportingAs with any radiologic study, reports should be
well
structured and should highlight clinically relevantinformation
in a concise manner. The Prostate Imag-ing Reporting and Data
System was proposed by theEuropean Society of Urogenital
Radiology14 with agoal of reducing interreader variability,
improving
FIG 3. T2WI (A), ADC map (B), kTrans map (C), and area under
theadenocarcinoma demonstrating a triple parametric match involving
the anbromuscular stroma (indicated by the arrows). Owing to their
anterior locbiopsies or at prostatectomy with some partial
embedding protocols. (Colo
32diagnostic value, and improving communicationbetween
radiologists and urologists. In this system,the location, maximal
diameter, and a summed overallscore are assigned to each lesion
detected. The loca-tion is based on dividing the prostate into
either 16 or27 regions. The overall Prostate Imaging Reportingand
Data System score for a lesion is the sum ofscores given to lesions
for each technique. A lesion'sscore ranges from 1-5, with a score
of 5 given tolesions that are highly likely to contain
signicantcancer. Extracapsular extension, seminal vesicle
inva-sion, distal sphincter invasion, bladder invasion, andother
pertinent ndings such as osseous or nodaldisease are also reported.
Studies evaluating theaccuracy of this scale when correlated with
targetedbiopsies using MRI-3D ultrasound (US) fusion
curve (AUC) map (D). These images depict pathologically
proventerior horn of the peripheral zone on the left as well as the
anterioration, these tumors are more likely to be missed on random
transrectalr version of gure is available online.)
Curr Probl Diagn Radiol, January/February 2015
-
intermediate-risk groups, the performance of T2WI,DCE, and MR
spectroscopy were evaluated with
PZ, peripheral zone.guidance have demonstrated promising
results.50,51
In a study using MR-guided biopsies, there wasmoderate
interreader agreement, high sensitivity, andhigh negative
predictive values.52 This system maynot perform as well regarding
accuracy and interreaderagreement for transitional zone tumors, and
renementfor tumors in this location may be needed.53,54 Inaddition
to continued renement, the development ofan image-rich atlas
similar to the BI-RADS atlaswould likely be useful to radiologists
interpretingFIG 4. The hemorrhage exclusion sign. A large tumor
involving muchof the right PZ, anterior gland, and central gland is
outlined byhemorrhage in the uninvolved left peripheral zone on
this precontrastT1WI. The left border of the tumor is indicated by
the arrowhead andis visible owing to the hemorrhage in the normal
left peripheral zone,indicated by the arrow. T2WI, DCE, and DWI
showed typical ndings.prostate MRI.
Challenges in Radiology-PathologyCorrelationRadiology-pathology
correlation deserves specialmention as the accurate correlation of
radiologyinterpretations with pathologic results is necessaryfor
continued validation of new techniques as wellas for improving our
own diagnostic accuracy. Severalmethods of radiologic-pathologic
correlation appear inthe literature regarding the type of pathology
(whole-mount specimens vs biopsy), method of correlation(image
directed biopsy vs mapping based uponlocation coordinates), and
stringency with which thecorrelation method is interpreted. An
example ofcorrelation with a whole-mount specimen from ourown
institution is shown in Figure 5. In a prospectivestudy55 of 70
patients predominantly in low- to
Curr Probl Diagn Radiol, January/February 2015whole-mount
specimens as the reference standard. Morespecically, the prostate
was divided into 30 regionsbased on anatomical landmarks during
both imaginginterpretation and histopathologic examination. In araw
stringent approach, a true positive was onlycounted when a lesion
detected on imaging corre-sponded to a cancer found at
histopathologic examina-tion within the same region. In their
neighboringapproach, cancers found at histopathologic examinationin
an immediately adjacent region were also counted astrue positives.
This was argued to reduce the negativeeffect of prostate shrinkage
and deformation as well asdifferences in sectioning plane during
grossing of theprostatectomy specimens. The neighboring
approachyielded better performance measures. In an attempt toreduce
the error introduced when sectioning the prosta-tectomy specimen at
angles that may be different thanthe imaging planes, the same group
subsequentlyreported using a customized mold to guide the
section-ing.56 The mold was generated by a 3D printer and wasbased
on an individual's prostate contours as drawn onT2WI. These 2
sophisticated methods of correlatinghistopathologic ndings on
prostatectomy specimens areobviously ideal in research settings
when compared withother methods used in routine clinical practice,
such asthose involving partial embedding of the specimen,57
which may miss more anterior tumors. However, manyacademic and
private institutions are not equipped forthis type of tissue
processing.In practice, most histopathologic correlation will
be
from a combination of the systematic extended sextanttransrectal
USguided biopsies, MRI-US fusionguided biopsies, and in-bore
MRI-guided biopsies.Promising results have been reported with
bothMRI-US fusion-guided biopsies58,59 and in-boreMRI-guided
biopsies.60,61 An additional importantconsideration with MRI in the
setting of AS is that anegative MPP-MRI examination nding has
beenshown to have a high negative predictive value ofdetecting
clinically signicant disease at biopsy inlow-risk patients,
therefore allowing the urologist toavoid the unnecessary risks of
repeat biopsies.62
Regardless of the method of pathologic correlationused, whether
in research or clinical practice, it isimperative that
multidisciplinary teams criticallythink about their method of
validation to advanceemerging techniques and prove diagnostic
accuracyand repeatability.
33
-
Further Challenges in Implementation IntoRoutine PracticeCare
should be taken when interpreting the literatureand trying to
generalize results to one's own practice.For example, when
comparing reported performanceof techniques from different
publications, there areoften several variables that differ,
including patientpopulation characteristics, eld strength, coil
selec-tion, b values in DWI, postprocessing techniques inDCE,
denition of positive ndings, and method ofpathologic verication.
Additionally, most publishedexperience with prostate MRI represents
single insti-tution, often high-end academic centers with
smallsample sizes. Hence, the reproducibility of theseresults in
general practice remains to be shown.Similarly, although once
promising, standard ADC
FIG 5. Prostate adenocarcinoma suspected in the left peripheral
zone (indishown). This was conrmed when correlated with whole-mount
histopatholored. (Color version of gure is available online.)
34cutoff values reported in the literature cannot bereliably
applied to one's practice as ADC has beenshown to be dependent on b
values in addition to otherimaging parameters.63,64 Open discussion
with theurologists and pathologists is essential to
developrealistic expectations and determine the role thatprostate
MRI will play in our own institution.
ConclusionIn the post-USPSTF era of prostate cancer screeningand
diagnosis, urologists are seeking new tools to helpmanage patients
and avoid unnecessary treatments.MPP-MRI has a yet underdeveloped
but promisingrole in AS. There are several challenges
associatedwith implementing MPP-MRI in clinical practice. Amajor
barrier to general acceptance will be precise
cated by the arrows) on T2WI (A), ADC map (B), and DCE images
(notgic specimens (C). Note that the areas of conrmed tumor are
colored
Curr Probl Diagn Radiol, January/February 2015
-
radiologic-pathologic correlation, which has a majoreffect on
the perceived accuracy of MPP-MRI. Multi-
13. Dickinson L, Ahmed HU, Allen C, et al. Magnetic
resonanceimaging for the detection, localisation, and
characterisation ofprostate cancer: Recommendations from a European
consen-
15. Kirkham APS, Haslam P, Keanie JY, et al. Prostate MRI:Who,
when, and how? Report from a UK consensus meetingClin Radiol
2013;68(10):1016-23.sus meeting. Eur Urol 2011;59(4):477-94.14.
Barentsz JO, Richenberg J, Clements R, et al. ESUR prostate
MR guidelines 2012. Eur Radiol 2012;22(4):746-57.
Curr Probl Diagn Radiol, January/February 2015disciplinary
collaboration between urologists, radiol-ogists, and pathologists
is integral to the successfulimplementation of MPP-MRI.
REFERENCES1. Siegel R, Ma J, Zou Z, et al. Cancer statistics,
2014. CA
Cancer J Clin 2014;64(1):9-29.2. Andriole GL, Crawford ED, Grubb
RL 3rd, et al. Mortality
results from a randomized prostate-cancer screening trial.N Engl
J Med 2009;360(13):1310-9.
3. Rosario DJ, Lane JA, Metcalfe C, et al. Short term outcomesof
prostate biopsy in men tested for cancer by prostate specicantigen:
Prospective evaluation within ProtecT study. Br MedJ
2012;344:d7894.
4. Moyer VA. U.S. Preventive Services Task Force. Screeningfor
prostate cancer: U.S. Preventive Services Task Forcerecommendation
statement. Ann Intern Med 2012;157(2):120-34.
5. Iversen P, Madsen PO, Corle DK. Radical prostatectomyversus
expectant treatment for early carcinoma of the
prostate.Twenty-three year follow-up of a prospective
randomizedstudy. Scand J Urol Nephrol Suppl 1995;172:65-72.
6. Wilt TJ, Brawer MK, Jones KM, et al. Radical
prostatectomyversus observation for localized prostate cancer. N
EnglJ Med 2012;367(3):203-13.
7. Bill-Axelson A, Holmberg L, Ruutu M, et al. Radical
pros-tatectomy versus watchful waiting in early prostate cancer.N
Engl J Med 2011;364(18):1708-17.
8. Welch HG, Albertsen PC. Prostate cancer diagnosis
andtreatment after the introduction of prostate-specic
antigenscreening: 1986-2005. J Natl Cancer Inst
2009;101(19):1325-9.
9. Ganz PA, Barry JM, Burke W, et al. National Institutes
ofHealth State-of-the-Science Conference: Role of
activesurveillance in the management of men with localizedprostate
cancer. Ann Intern Med 2012;156(8):591-5.
10. Turkbey B, Mani H, Aras O, et al. Prostate cancer:
Canmultiparametric MR imaging help identify patients who
arecandidates for active surveillance? Radiology
2013;268(1):144-52.
11. Stamatakis L, Siddiqui MM, Nix JW, et al. Accuracy
ofmultiparametric magnetic resonance imaging in conrmingeligibility
for active surveillance for men with prostate cancer.Cancer
2013;119(18):3359-66.
12. Leake JL, Hardman R, Ojili V, et al. Prostate MRI: Access
toand current practice of prostate MRI in the United States.J Am
Coll Radiol 2014;11(2):156-60.16. Hoeks CMA, Barentsz JO, Hambrock
T, et al. Prostate cancer:Multiparametric MR imaging for detection,
localization, andstaging. Radiology 2011;261(1):46-66.
17. Hricak H, White S, Vigneron D, et al. Carcinoma of
theprostate gland: MR imaging with pelvic phased-array coilsversus
integrated endorectalpelvic phased-array coils. Radio-logy
1994;193(3):703-9.
18. Ftterer JJ, Engelbrecht MR, Jager GJ, et al. Prostate
cancer:Comparison of local staging accuracy of pelvic
phased-arraycoil alone versus integrated endorectal-pelvic
phased-arraycoils. Local staging accuracy of prostate cancer using
endor-ectal coil MR imaging. Eur Radiol 2007;17(4):1055-65.
19. Beyersdorff D, Taymoorian K, Knsel T, et al. MRI of
prostatecancer at 1.5 and 3.0 T: Comparison of image quality in
tumordetection and staging. Am J Roentgenol
2005;185(5):1214-20.
20. Torricelli P, Cinquantini F, Ligabue G, et al.
Comparativeevaluation between external phased array coil at 3 T
andendorectal coil at 1.5 T: Preliminary results. J Comput
AssistTomogr 2006;30(3):355-61.
21. Park BK, Kim B, Kim CK, et al. Comparison of
phased-array3.0-T and endorectal 1.5-T magnetic resonance imaging
in theevaluation of local staging accuracy for prostate cancer.J
Comput Assist Tomogr 2007;31(4):534-8.
22. Heijmink SWTPJ, Ftterer JJ, Hambrock T, et al.
Prostatecancer: Body-array versus endorectal coil MR imaging at3
Tcomparison of image quality, localization, and stagingperformance.
Radiology 2007;244(1):184-95.
23. Turkbey B, Merino MJ, Gallardo EC, et al. Comparison
ofendorectal coil and nonendorectal coil T2W and diffusion-weighted
MRI at 3 Tesla for localizing prostate cancer:Correlation with
whole-mount histopathology. J Magn ResonImaging
2013;39(6):1443-8.
24. Langer DL, van der Kwast TH, Evans AJ, et al. Prostatecancer
detection with multi-parametric MRI: Logistic regres-sion analysis
of quantitative T2, diffusion-weighted imaging,and dynamic
contrast-enhanced MRI. J Magn Reson Imaging2009;30(2):327-34.
25. Delongchamps NB, Rouanne M, Flam T, et al. Multipara-metric
magnetic resonance imaging for the detection andlocalization of
prostate cancer: Combination of T2-weighted,dynamic
contrast-enhanced and diffusion-weighted imaging.BJU Int
2011;107(9):1411-8.
26. Hambrock T, Somford DM, Huisman HJ, et al.
Relationshipbetween apparent diffusion coefcients at 3.0-T MR
imagingand Gleason grade in peripheral zone prostate
cancer.Radiology 2011;259(2):453-61.
27. Langer DL, van der Kwast TH, Evans AJ, et al.
Intermixednormal tissue within prostate cancer: Effect on MR
imagingmeasurements of apparent diffusion coefcient and
T2-sparseversus dense cancers. Radiology 2008;249(3):900-8.
28. Zelhof B, Pickles M, Liney G, et al. Correlation of
diffusion-weighted magnetic resonance data with cellularity in
prostatecancer. BJU Int 2009;103(7):883-8.
29. Yoshizako T, Wada A, Hayashi T, et al. Usefulness
ofdiffusion-weighted imaging and dynamic contrast-enhanced
35
-
magnetic resonance imaging in the diagnosis of
prostatetransition-zone cancer. Acta Radiologica
2008;49(10):1207-13.
30. Kim CK, Park BK, Kim B. High-b-value diffusion-weighted
44. Vargas HA, Akin O, Shukla-Dave A, et al.
Performancecharacteristics of MR imaging in the evaluation of
clinicallylow-risk prostate cancer: A prospective study.
Radiologyimaging at 3 T to detect prostate cancer:
Comparisonsbetween b values of 1,000 and 2,000 s/mm2. Am J
Roent-genol 2010;194(1):W33-7.
31. Katahira K, Takahara T, Kwee TC, et al.
Ultra-high-b-valuediffusion-weighted MR imaging for the detection
of prostatecancer: Evaluation in 201 cases with histopathological
corre-lation. Eur Radiol 2011;21(1):188-96.
32. Kitajima K, Takahashi S, Ueno Y, et al. Clinical utility
ofapparent diffusion coefcient values obtained using highb-value
when diagnosing prostate cancer using 3 tesla MRI:Comparison
between ultra-high b-value (2000 s/mm2) andstandard high b-value
(1000 s/mm2). J Magn Reson Imaging2012;36(1):198-205.
33. Rosenkrantz AB, Hindman N, Lim RP, et al. Diffusion-weighted
imaging of the prostate: Comparison of b1000 andb2000 image sets
for index lesion detection. J Magn ResonImaging
2013;38(3):694-700.
34. Tudorica LA, Oh KY, Roy N, et al. A feasible
highspatiotemporal resolution breast DCE-MRI protocol for clin-ical
settings. Magn Reson Imaging 2012;30(9):1257-67.
35. Li X, Huang W, Rooney WD. Signal-to-noise ratio,
contrast-to-noise ratio and pharmacokinetic modeling considerations
indynamic contrast-enhanced magnetic resonance imaging.Magn Reson
Imaging 2012;30(9):1313-22.
36. Verma S, Turkbey B, Muradyan N, et al. Overview ofdynamic
contrast-enhanced MRI in prostate cancer diagnosisand management.
Am J Roentgenol 2012;198(6):1277-88.
37. Rosenkrantz AB, Sabach A, Babb JS, et al. Prostate
cancer:Comparison of dynamic contrast-enhanced MRI techniquesfor
localization of peripheral zone tumor. Am J
Roentgenol2013;201(3):W471-8.
38. Wang L, Mazaheri Y, Zhang J, et al. Assessment of
biologicaggressiveness of prostate cancer: Correlation of MR
signalintensity with Gleason grade after radical
prostatectomy.Radiology 2008;246(1):168-76.
39. Van As NJ, de Souza NM, Riches SF, et al. A study
ofdiffusion-weighted magnetic resonance imaging in men
withuntreated localised prostate cancer on active surveillance.
EurUrol 2009;56(6):981-7.
40. Lee DH, Koo KC, Lee SH, et al. Tumor lesion diameter
ondiffusion weighted magnetic resonance imaging could helppredict
insignicant prostate cancer in patients eligible foractive
surveillance: Preliminary analysis. J Urol 2013;190(4):1213-7.
41. Rosenkrantz AB, Taneja SS. Radiologist, be aware:
Tenpitfalls that confound the interpretation of
multiparametricprostate MRI. Am J Roentgenol
2014;202(1):109-20.
42. Cruz M, Tsuda K, Narumi Y, et al. Characterization of
low-intensity lesions in the peripheral zone of prostate on
pre-biopsy endorectal coil MR imaging. Eur Radiol
2002;12(2):357-65.
43. Barrett T, Vargas HA, Akin O, et al. Value of the
hemor-rhage exclusion sign on T1-weighted prostate MR images forthe
detection of prostate cancer. Radiology 2012;263(3):751-7.
362012;265(2):478-87.45. Akin O, Sala E, Moskowitz CS, et al.
Transition zone prostate
cancers: Features, detection, localization, and staging
atendorectal MR imaging. Radiology 2006;239(3):784-92.
46. Haider MA, van der Kwast TH, Tanguay J, et al.
CombinedT2-weighted and diffusion-weighted MRI for localization
ofprostate cancer. Am J Roentgenol 2007;189(2):323-8.
47. Hoeks CMA, Hambrock T, Yakar D, et al. Transition
zoneprostate cancer: Detection and localization with 3-T
multi-parametric MR imaging. Radiology 2013;266(1):207-17.
48. Li H, Sugimura K, Kaji Y, et al. Conventional
MRIcapabilities in the diagnosis of prostate cancer in the
transitionzone. Am J Roentgenol 2006;186(3):729-42.
49. Oto A, Kayhan A, Jiang Y, et al. Prostate cancer:
Differentiationof central gland cancer from benign prostatic
hyperplasia byusing diffusion-weighted and dynamic
contrast-enhanced MRimaging. Radiology 2010;257(3):715-23.
50. Portalez D, Mozer P, Cornud F, et al. Validation of
theEuropean Society of Urogenital Radiology scoring system
forprostate cancer diagnosis on multiparametric magnetic reso-nance
imaging in a cohort of repeat biopsy patients. Eur
Urol2012;62(6):986-96.
51. Fiard G, Hohn N, Descotes J-L, et al. Targeted
MRI-guidedprostate biopsies for the detection of prostate cancer:
Initialclinical experience with real-time 3-dimensional
transrectalultrasound guidance and magnetic resonance/transrectal
ultra-sound image fusion. Urology 2013;81(6):1372-8.
52. Schimmller L, Quentin M, Arsov C, et al.
Inter-readeragreement of the ESUR score for prostate MRI
usingin-bore MRI-guided biopsies as the reference standard.
EurRadiol 2013;23(11):3185-90.
53. Rosenkrantz AB, Kim S, Lim RP, et al. Prostate
cancerlocalization using multiparametric MR imaging: Comparisonof
Prostate Imaging Reporting and Data System (PI-RADS)and Likert
scales. Radiology 2013;269(2):482-92.
54. Rosenkrantz AB, Lim RP, Haghighi M, et al. Comparison
ofinterreader reproducibility of the prostate imaging reportingand
data system and Likert scales for evaluation of multi-parametric
prostate MRI. Am J Roentgenol 2013;201(4):W612-8.
55. Turkbey B, Pinto PA, Mani H, et al. Prostate cancer: Value
ofmultiparametric MR imaging at 3 T for detection-histopathologic
correlation. Radiology 2010;255(1):89-99.
56. Turkbey B, Mani H, Shah V, et al. Multiparametric 3
Tprostate magnetic resonance imaging to detect cancer:
Histo-pathological correlation using prostatectomy specimens
proc-essed in customized magnetic resonance imaging basedmolds. J
Urol 2011;186(5):1818-24.
57. Sehdev AE, Pan CC, Epstein JI. Comparative analysis
ofsampling methods for grossing radical prostatectomy speci-mens
performed for nonpalpable (stage T1c) prostatic adeno-carcinoma.
Hum Pathol 2001;32(5):494-9.
58. Rastinehad AR, Turkbey B, Salami SS, et al.
Improvingdetection of clinically signicant prostate cancer:
MRI/TRUSfusion-guided prostate biopsy. J Urol
2013;191(6):1749-54.
Curr Probl Diagn Radiol, January/February 2015
-
59. Walton Diaz A, Hoang AN, Turkbey B, et al. Can
magneticresonance-ultrasound fusion biopsy improve cancer
detectionin enlarged prostates? J Urol 2013;190(6):2020-5.
60. Baur ADJ, Maxeiner A, Franiel T, et al. Evaluation of
theprostate imaging reporting and data system for the detectionof
prostate cancer by the results of targeted biopsy of theprostate.
Invest Radiol 2014;49(6):411-20.
61. Hoeks CMA, Somford DM, van Oort IM, et al. Value of
3-Tmultiparametric magnetic resonance imaging and
magneticresonance-guided biopsy for early risk restratication in
activesurveillance of low-risk prostate cancer: A prospective
multi-center cohort study. Invest Radiol 2014;49(3):165-72.
62. Numao N, Yoshida S, Komai Y, et al. Usefulness of
pre-biopsymultiparametric magnetic resonance imaging and
clinicalvariables to reduce initial prostate biopsy in men with
suspectedclinically localized prostate cancer. J Urol
2013;190(2):502-8.
63. Mazaheri Y, Vargas HA, Nyman G, et al. Diffusion-weightedMRI
of the prostate at 3.0 T: Comparison of endorectal coil(ERC) MRI
and phased-array coil (PAC) MRIThe impactof SNR on ADC measurement.
Eur J Radiol 2013;82(10):e515-20.
64. Peng Y, Jiang Y, Antic T, et al. Apparent diffusion
coefcientfor prostate cancer imaging: Impact of B values. Am
JRoentgenol 2014;202(3):W247-53.Curr Probl Diagn Radiol,
January/February 2015 37
Prostate Magnetic Resonance Imaging: Challenges of
ImplementationIntroductionChallenges in AcquisitionField Strength
and Coil SelectionT2-Weighted ImagingDiffusion-Weighted ImagingDCE
Imaging
Challenges in Interpretation and
ReportingInterpretationReporting
Challenges in Radiology-Pathology CorrelationFurther Challenges
in Implementation Into Routine PracticeConclusionReferences