Embed Size (px)
Citation preview

ARRHYTHMIAS AND CONDUCRON DISTURBANCES
Prospective Evaluation of Day-t*Day Reproducibility of Upright Tilt-Table
Testing in Unexplained Syncope Ross Brooks, MD, MSC, Jeremy N. Ruskin, MD, Anne C. Powell, MBBS, John Newell, BA,
Hasan Gaian, MD, and Brian A. McGovern, MD
To evaluate the day-today reproducibility of up right tilt-table testing, 109 patients with unex- plained syncope prospectively underwent testbtg on 2 consecutive days using a uniform protocol. Results of testing on 2 separate days were concordant in 69 of 109 patients (63%), and dis- cordant in 46 of 109 patients (37%). Thirty-six of 109 patients (33%) had vasodepressoc syncope on 1 or both days of testing. Nineteen of 30 patients (63%) with vasodepressor responses on the Rrst day did not reproduce this response durbtg the second day of testing. An additional 6 patients with an initial negative tilt test had a vasodepres sor response on the second day. Only 11 of 36 pa tients (31%) had reproducible vasodepressor re sponses on both days of testing Patients with CB producible vasodepressor respomes had a significantly higher mean number of preceding clinical syncopal events than patients with 2 nor mal tests (p <0.02) or nonreproducible results (p ~0.64). In addition, these patients had a signifi- cantly longer duration of clinical symptoms rela tive to patients with 2 tests that yielded negative results (p <0.006) and nonreproducible results (p eO.01). The elapsed time between the most recent clinical event and the performance of tilttable testing was not signiticantly different among the 3 groups, and did not appear to influence the out- come of testing.
These data show that vasodepressor respons es elicited by upright tilt-table testiN show day- today variabilii in many patients, a filling that may limit the interpretation of initial and followup test results.
(AmJ Cardiol1993;71:1269-1292)
From the Cardiac Arrhythmia Service, Massachusetts General Hospi- tal, Boston, Massachusetts. Manuscript received September 10, 1992; revised manuscript received December 16, 1992, and accepted Decem- ber 22.
Address for reprints: Ross Broob, MD, MSc, Cardiac Unit, Massachu- setts General Hospital, Boston, Massachusetts 02114.
U pright tilt-table testing is being increasingly used as a provocative maneuver for uncovering vaso- depressor (“vasovagal”) responses in patients
with unexplained syncope. Vasodepressor responses are frequently elicited by tilt-table testing in patients with a history of syncope in whom other tests have failed to establish a cause, whereas these responses occur infre- quently during testing in asymptomatic persons.1-7 An important consideration is the day-to-day reproducibili- ty of these responses, which is not yet well defined.* An understanding of the reproducibility of these responses on different days is an important basic issue, and is fun- damental to the correct interpretation of repeat test re- sults, particularly after institution of therapy.+12 The purpose of the present study was to assess the day-to- day reproducibility of responses elicited by upright tilt- table testing in patients undergoing evaluation of unex- plained syncope.
METHODS Patients: The study population consisted of 109
consecutive patients undergoing upright tilt-table testing for 1 or more episodes of unexplained syncope or recur- rent presyncope who consented to this evaluation. Pa- tients with structural heart disease, abnormal left ven- tricular function or abnormal electrocardiograms under- went electrophysiologic testing as clinically indicated in addition to upright tilt-table testing. All 109 patients were prospectively studied on 2 consecutive days using a uniform protocol. Upright tilt-table testing was per- formed after an overnight fast in all patients. To mini- mize diurnal variation, both studies were performed at approximately the same time on both days (Table I). To limit hypovolemia, all patients were given 100 ml of 5% dextrose solution through a peripheral intravenous can- nula for each hour after 790 A.M. until the time of test- ing. All patients were monitored continuously during tilt-table testing using 3 electrocardiographic leads. Dur- ing tilt-table testing, arterial blood pressure was moni- tored noninvasively in 108 patients with an arm sphyg- momanometer, and invasively in 1 patient with a radial artery cannula. Tests were performed in a quiet room with dimmed lighting. Tilt-table testing was performed using an electrically controlled table with a footboard for weight bearing (G. E. Miller, Inc., Yonkers, New York). Baseline measurements were obtained during resting conditions over 15 minutes at O”, followed by upright tilt to 70” for a maximal duration of 25 minutes, or until hypotension and syncope occurred. Patients were stud-
TILT-TABLE TESTING 1289

ied while taking their usual medications, and no medi- cation changes were made between the 2 tilt-table tests. No patients were taking antianhythmic drugs or p block- ers at the time of tilt-table testing. A subset of 54 pa- tients with a second negative tilt test received an iso- proterenol infusion (mean dose 1.7 + 0.73 tq.zJrnin) after completion of the second baseline test. Isoprotercnol was infused through a peripheral arm vein for 10 min- utes in the supine position, followed by upright tilt-table testing for up to 15 minutes.
Deflnitkn of v Vasodepressor syncope was defined as hypotension and relative bradycardia culmi- nating in loss of consciousness during tilt-table testing. Postural (orthostatic) hypotension was detined as a de- crease in mean blood pressure of >lO mm Hg during uptight tilt testing unaccompanied by deceleration of heart rate or development of syncope. A normal test was defined as absence of hypotension or syncope during tilt- table testing. A positive test was defined as a vasode- pressor response, while a negative test was defined as absence of a vasodepressor response.
SitaMdd analysis: Paired data were analyzed using the Student’s t test. Proportions were analyzed by Fish- er’s exact test. Comparison of group data was performed using l-way analysis of variance. Variables demonstrat- ing inhomogeneity of variance were log-transformed before the parametric tests. A p value 4.05 was con- sidered statistically significant. Data are presented as mean f SD.
TABLE I Comparison of Heart Rate (beats/min) and Mean Blood Pressure (mm Hg) Before and After One Minute of Upright Tilt During Testing on Two Consecutive Days
Day 1 Day 2 p Value
Heart rate (baseline) 70 k 13 70 + 14 0.73 Heart rate (first-minute tilt) 8Ok 15 81 A 16 0.15 Blood pressure (basehe) 952 13 94-e 19 0.43 Blood (first-mmute pressure tilt) 93 2 14 93 + 19 0.66 Time of day lo:42 10:50 0.25
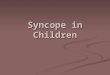
DAY 1 DAY 2
PH @
109 109 I FWJREl.RepodueibSIRydthS responssr~~plm~ wJletestblgaal2 fxmmadvedayavvru eponmsoccurmdin36pathts(33%)cmlabathtest
r&y mspomeswereonlyfoundhamhority
~,wh-=amaiolitr(WWhadmmt- d-V mspameaontho2testdayrN= normd;PN=poatudhypaten~vD=vasodepessor~ cope.
RESULTS The mean age of the study patients was 54 f 21
years, and the mean number of syncopal episodes per patient was 6.3 f 15. Fifty-six of 109 patients (51%) underwent electrophysiologic testing before tilt testing, with normal results in 53 of 56 (95%). No patient with a vasodepressor response had an abnormal electrophysi- ologic test result.
The results of upright tilt-table testing are shown in Figure 1. Results of testing on 2 separate days were con- cordant in 69 of 109 patients (63%) and discordant in 40 of 109 patients (37%). Thirty-five of 109 patients (32%) had vasodepressor syncope on 1 or both days. On the first day of testing, 30 of 109 patients (28%) had vasodepressor responses, 56 of 109 patients (51%) had normal responses, and 23 of 109 patients (21%) had pos- tural hypotension. On the second day of testing, 17 of 109 patients (16%) had vasodepressor responses, 70 of 109 patients (64%) had normal responses, and 22 of 109 (20%) had postural hypotension. The reproducibility of the initial test result was 80, 56 and 37%, respective- ly, for patients with normal, postural hypotension, and vasodepressor responses. Nineteen of 30 patients (63%) with vasodepressor responses on the first day did not reproduce this response during the second day of test- ing (Figure 1). Six of 79 patients (8%) with initial neg- ative tests had a vasodepressor response on the second day. Notably, only 11 of 36 patients (31%) with vasode- pressor syncope had reproducible responses on both days of testing (Figure 1). The average time to devel- opment of syncope in patients with vasodepressor re- sponses was 14 f 6 minutes (range 4 to 25 minutes). Twenty-six of 36 patients (72%) with vasodepressor re- sponses had a structurally normal heart, and all patients with these responses had normal left ventricular systolic function (left ventricular ejection fraction >SO%).
The average reduction in mean blood pressure in pa- tients with postural hypotension was 17 f 5 mm Hg, and the mean time after initiation of tilt to the nadir in blood pressure was 15 + 6 minutes. All patients with postural hypotension completed 25 minutes of testing, and none developed syncope. Postural hypotension was consid- ered a separate hemodynamic response to tilt, and dis- tinct from a vasodepressor response.
Sixteen of 109 patients (14%) underwent upright tilt- table testing on the first day after electrophysiologic test- ing, whereas 93 of 109 patients (86%) were studied before or unrelated to accompanying electrophysiologic procedures. On the second day of testing, all 109 tilt- table tests were performed in the absence of preceding electrophysiologic studies. Vasodepressor responses oc- curred more often on the first day of testing in patients with preceding electrophysiologic procedures compared with patients studied in the absence of this procedure (6 of 16 or 38% vs 24 of 93 or 26%) although the differ- ence did not achieve statistical significance (p = 0.25). Of the 16 patients who underwent tilt-table testing after the completion of electrophysiologic studies, most (10 of 16 or 63%) did not have a vasodepressor response.
The mean number of clinical syncopal episodes was significantly higher in patients with reproducible vaso- depressor responses than in those having negative results
I290 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 JUNE 1,1993

from 2 tests (15 ? 17 vs 6 + 16, p ~0.02) (Table II). Patients with reproducible positive test results also had a significantly higher mean number of clinical syncopal events relative to patients with nonreproducible respons- es (15 k 17 vs 5 f 8, p ~0.04) (Table II). The average duration of clinical symptoms (years) was significantly longer in patients with reproducible vasodepressor re- sponses than in patients with negative results from 2 studies (14 f 14 vs 5 + 11, p <0.008) or nonreproducible vasodepressor responses (14 + 14 vs 3 f 5, p ~0.02). The elapsed time between the most recent syncopal event and the performance of tilt-table testing was not signilicantly different among the 3 groups (Table II), and did not appear to inlhtence the outcome of testing. A similar percentage of patients in each of the 3 patient subgroups reported a warning symptom, such as dizzi- ness, before their syncopal event (Table II). However, a higher percentage of patients with reproducible vasode- pressor responses experienced a prodrome compatible with vasodepressor syncope (nausea, diaphoresis, warmth, weakness) at the time of their clinical event than did patients with two negative test results (82 vs 44%, p ~0.04) (Table II), whereas differences between the for- mer patients and those with nonreproducible responses were not statistically different (82 vs 56%, p = 0.2). Stepwise logistic regression identified the mean number of syncopal events, the average duration of symptoms, and the presence of a prodrome as significant predictors of reproducible responses during repeat day testing.
Isoproterenol infusion provoked vasodepressor re- sponses in 11 of 54 patients (20%) tested. Isoproterenol produced vasodepressor responses in 7 of 45 patients (16%) with 2 preceding negative tilt tests, and 4 of 9 patients (44%) with 1 positive followed by 1 negative tilt test (p = 0.07). The mean dose of isoproterenol was higher in patients with positive results than in those with negative results (2.1 f 0.8 vs 1.6 f 0.7 pg/min, p = 0.007).
DISCUSSION The present study is the first reported attempt to
examine systematically the day-to-day reproducibility of the responses to upright tilt-table testing under stan- dardized conditions on 2 consecutive days. The princi- pal ftndings of our study are the high degree of vari- ability in the responses to upright tilt testing, and the frequent nonreproducibility of vasodepressor responses during repeat tilt testing on a second day. Results of the present study are different from those reported recently by Raviele et al6 in a similar patient population. In the latter study, repeat tilt-table tests were performed nonuniformly after a mean period of 3 days (range 1 to 13) in 14 of 15 patients with initial vasodepressor re- sponses, whereas patients with initial normal responses did not undergo repeat testing.6 Ten of 14 patients (71%) in the study by Raviele et al6 had reproducible vasode- pressor responses on a second day of testing. Our yield of reproducible responses was much lower (31%). The factors accounting for the differences in the results of the 2 studies are not clear but may be due to differences in patient selection, the time interval between tests, or the conditions under which testing was performed.
TABLE II Relation Between Clinical Findings and Test Outcomes
Group Results
A B C -/- +/- +I+
No. of patients 73 25 11
Age (year) 56k21 52k21 49 f 28
Men/women 33140 19125 714 Syncopal events 65 16 5~8 15 2 7*t
Warning symptom (%) 71 76 82
Prodrome (%I 44 56 82t Duration of symptoms (years) 5F 11 325 14 f 149/l
Elapsed time (days) between 43 + 72 28 f. 46 40 2 32
last syncopal event and first
tilt test
*p co.04 8 versus C; tp <O.OZ A versus C; $p co.04 A versus C; §p co.008 A versus C; lip < 0.01 B versus C.
I
The variability of the responses on different test days is not unexpected, since clinically, these responses are also random and unpredictable in nature. The substrate for vasodepressor syncope and its potential provocation by tilt-table testing may also be stronger or weaker on a given day of testing, thus accounting for the nonrepro- ducible test results. The observation that the vast major- ity of patients (76%) with nonreproducible vasodepres- sor responses had an initial positive and subsequent neg- ative study, rather than the opposite outcome, suggests that the day-to-day variability of these responses may not solely be a random occurrence. In some patients, a “conditioning” effect may possibly accure from expo- sure to the initial tilt test, which then inlluences the out- come of a subsequent study performed in close succes- sion. Because vasodepressor responses appear neurally mediated, input from higher brain centers to vasomotor centers may well modulate these reflexes and account for this phenomenon. I3314 In some cases an additional stimulus such as isoproterenol may be necessary to un- cover latent responses. However, even isoproterenol may fail to produce consistent responses as shown by our ob- servation that only a minority of our patients (4 of 9) with a positive followed by a negative response devel- oped a vasodepressor response during isoproterenol infusion. The observation that a small percentage (8%) of patients had an initial negative and subsequent posi- tive tilt-table test, also suggests that a single test may not be sufficient for excluding this diagnosis. The pre- cise physiology of these responses remains to be eluci- dated, and the maneuvers necessary to provoke respons- es consistently in susceptible patients have yet to be delined. The nonreproducibility of vasodepressor re- sponses on different days most patients tested also has important implications in patients who undergo repeat testing after receiving therapy. To interpret repeat test results correctly after institution of therapy, the baseline reproducibility of these responses must be established. Day-to-day variability of these responses appears to occur more often than realized, and may account for the benefits ascribed to drug therapy in many patients. Our data suggest that proposed therapeutic interventions for vasodepressor syncope can only reliably be evaluated in
TILT-TABLE TESTING 1291

patients with reproducible responses whether sponta- 1. Kenny RA, Ingram A, Bayliss 1. Sutton. Head-up tilt: a useful test for invwi-
neous or induced by tilt-table testing. gating unexplained syncopc. lancft 1986: I: 1.152.-1355.
There are several potential limitations to this study. 2. Fitqxtick A, llwdorakis G. Travill C, Sutton R. Incidence of malignant uw.
The population studied was a selected group of patients vagal syndrome in 332 syncopal patients: rwdts of c.ardiac pacing. Br Ileur! J
19s9:ht:97. referred to a cardiac arrhythmia center, and may not rep- 3. Rtzpabick A, Sutton R. Tilting towards a diagnosis in recutrent unexplained
resent unselected patients with unexplained syncope. A syncope. /mref 1989: I :6.58-6&l.
small number of patients (14%) underwent their first tilt- 4. Strashxg B. Rechavia E. Sagie A. Kusniec J. Mager A, Sclamvsky S. Agmom J. The head-up tilt table test in patients with syncope of unknown origin. Am Heart
table test after electrophysiologic testing, while the set- J 198~, ,8:923-927.
’ ond tilt test in these patients was performed in the
6. Abi-Senm F. Maloney J, Fouad-Tarui FM, Castle LW. The usefulness of head- up tilt tecting and hcmodynamic investigation in the work-up of syncope of unknown
absence of electrophysiologic testing. Although the tie- origin. PACE lYX8:I I: 1202-1204.
quency of vasodepressor responses was higher among 6. Raviele A, Gasparini G, DiPede F, D&e P, Bonw A, Piccolo E. Uwfulncs
patients tested before, rather than after electrophysio- of head-up till ICFI in evaluating patients with syncope of unknown origin and neg- ative elcctmphy~iologic study. Am J Cordial lY9(thS:l322--1327.
logic testing (38 vs 26%), the difference was not statisti- 7. Gmhh BP, Tcmesy-Armos P, Hahn II, Elliott L. Utility of uptight tilt-table tcst-
tally significant (p = 0.25). Therefore, vascular instru- ing in the evaluation and management of syncopc of unknown origin. Ant J McJd 1991$x%-IO.
mentation need not be invoked to account for the dis- 8. Fitzpauick AP. Thecxlorakis G, Vardaq P, Sutton R. Metbadology of head-up
cordant responses observed in the present study. In tilt testing in patients with unexplamcd synwpe. J Am Co/l Cordwl 1991: 17: 125. 130.
agreement with earlier observations,15 however, our data 9. Sm JS, Anderson AJ, Sheikh SII. Avitall B, Tchou PJ, Troup PJ, Gilbert CJ,
suggest caution in interpreting tilt-table test results after Akhtx M, Jazayeri M. Unexplained syncopc evaluated by electmphy~iologic stud-
vascular instrumentation has been performed.15-t7 A fur- ies and head-up tilt teaing. Ann lntrrn Mcd 1991:114:1013--1019. 1 0.
ther potential limitation was that not all patients with a Milstein S, Hwtikofer J. Laser J, Gomick C, Benditt DG. Disopymmidc rwer-
sal of induced hypotension-hradycardia in neurally muiiatcd syncope. Cirmlarion
negative second tilt test received isoproterenol. Isopro- l987;76(suppl IV):IV-175.
terenol was not routinely given to all patients, was il. Milstein S, Buetikofcr J. Dunnigan A. Benditt DG. Gomick C, Reycs WJ. Use- fulnar of disopymmide for prevention of uptight tilt-induced hypotension-brady-
avoided in patients with significant left ventricular out- cardia. Am J Cardin/ 1~6S:l33%1.344,
flow tract obstruction, and was administered on a case- l2. Wallin RG. Sundlof G. Sympathetic outflow to muaclcs during vasovagal syn-
by-case basis to patients with ischemic heart disease. cope J Auron Nem Sysr 1982;6:287 -291. lb Abboud F.M. Ventricular syncge. N En,ql J Med 3989:320:39!&392.
Also, the mean dose of isoproterenol used in the present 14. Wallin BG. Sundlof G. Sympathetic outflow to muscles during vasovagal syn-
study was below that used by some investigators,“-tx cope. J Aumn New $5, 1982:6:287-291.
and was lower in patients with negative rather than pos- 16. Stevens PM. Cardiovaxulat dynamxs during orthortasis and the influence of vascular instrumentation. Am J Cardiol 1066: 17121 l-218.
itive outcomes during infusion. However, isoproterenol 16. Almquirt A. Goldentxrg fF’. Milstein S. Chen MY, Chen X, Hansen R. Gor-
did not influence the baseline reproducibility of these nick C, Henditt D. Provocation of bradycardia and hypotension by i.sopmterenol and upright posture in patient.\ with unexplained syncope. N Engl J Mcd 1989:320:
responses, since it was only administered after the sec- 346-351.
ond test. Finally, it remains possible that if repeat tests 17. Chen MY, Goldenbeg IF, Milstcm S. Hwtikofer J, Almquist A, Lewr J. Bcn-
were more widely separated in time, or perhaps per- ditt DG. Cardiac electrophysiologic and hemcdynamic correlates of neurally mcdi- ated syncope. Am J Cardio/ 1989;63:6&72.
formed at random, results may have been more repro- 16. Waxman MB, Yao L, Cameron DA. Wald RW. Roseman J. Isopmtercnol
ducible. induction of vasodepresor-type reaction in vawdepresor-prone persons. Am J Car- dial 1989:63:5%65.
I.292 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 JUNE 1, 1993