Embed Size (px)
Citation preview

Pro’s and Pitfalls in Cardiac Imaging

ResourcesResources
• Stress echo Stress echo – Douglas et al, JACC; 2007; 50: 187-204Douglas et al, JACC; 2007; 50: 187-204
• Stress nuclearStress nuclear– Brindis et al, JACC 2005; 46: 1587-605Brindis et al, JACC 2005; 46: 1587-605 – Tool to calculate appropriateness:Tool to calculate appropriateness:http://www.skyscape.com/download/reseller.asp?format=binary&os=win&device=pc&product=spectmpi

Iglehart JK, NEJM 2009;360:1030Iglehart JK, NEJM 2009;360:1030

It’s a
Big Deal

The 3 Worst Reasons For the The 3 Worst Reasons For the Recent Growth in Imaging Recent Growth in Imaging
UseUse• Defensive medicineDefensive medicine
• Self-referralSelf-referral
• Inappropriate indicationsInappropriate indications

What is An Appropriate Imaging Study?What is An Appropriate Imaging Study?
An appropriate imaging study is one in which the An appropriate imaging study is one in which the expected incremental information, combined with expected incremental information, combined with clinical judgment, exceeds the expected negative clinical judgment, exceeds the expected negative consequences* by a sufficiently wide margin for a consequences* by a sufficiently wide margin for a specific indication that the procedure is generally specific indication that the procedure is generally considered acceptable care and a considered acceptable care and a reasonable reasonable approach for the indication.approach for the indication.
**Negative consequences include the risks of the procedure (i.e., radiation or contrast exposure) and the downstream impact of poor test performance such as delay in diagnosis (false negatives) or inappropriate diagnosis (false positives).

Modern Cardiac Imaging Facts
• Extremely powerful in revealing non-invasive information– Anatomy, patho-physiology– Therapeutic relevance to treatment
• Highly inter-disciplinary– Many stakeholders
• Very costly– Capital investment– Running costs– Sophisticated manpower– Complex interaction between “players”

Sequential Bayesian analysis of CAD probability using MPI.
Loong C Y , Anagnostopoulos C Heart 2004;90:v2-v9
©2004 by BMJ Publishing Group Ltd and British Cardiovascular Society

Pre- test Likelihood of CAD based upon age, sex, and symptoms
Pro’s and Pitfalls in Cardiac Imaging
First Rule of Testing:
Never order a test if you do not know what to do
with the results

Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Gibbons, R. J. et al. J Am Coll Cardiol 2010;55:483-495
Effect of Screening on Clinical Outcomes

Technologies That Will Be Discussed
• CXR (briefly)
• Nuclear Studies
• Echocardiography
• Computerized Tomography
• Magnetic Resonance Imaging/Angiography

CXR• Chest Pain—
– rule out dissection– pneumothorax– hemothorax – pneumonia– chamber dimensions – effusions – pulmonary vascularity– coronary aneurysm
• Cough/Dyspnea/Fever with sxs
• Cancer screening “forget it”
• Ordering and not following up “missed mass”

Gamma Camera

Role of Nuclear Cardiac Imaging
• Diagnosis of coronary artery disease,
• Evaluation of cardiac function abnormalities,
• Monitoring of patients under treatment for established cardiac disease.
• Verification of the diagnosis of acute myocardial infarction



Up to 20% of nuclear stress tests are false positives!*******
• Maybe we should re-name it “unclear” medicine– Most cardiologists do!!
• Inferior wall defects are especially common due to the overlap of the diaphragm with the heart muscle, yielding the appearance of reduced blood flow.
• Anterior defects are common in females with large breasts for the same reasons……..as well as many men!*******These numbers are under
study environments in peer reviewed interpretations

ECG Gated SPECT imaging(MUGA: multi gated acquisition)
• Simultaneous assessment of perfusion and function in a single injection, single acquisition sequence.
• Tc-99m permits evaluation of regional myocardial wall motion and wall thickening throughout the cardiac cycle
• Quantitates LV volume and EF

Indications for Pharmacologic Nuclear Perfusion Stress Imaging
• Inability to perform adequate exercise
• Left bundle branch block
• Ventricular pacemaker
• CCB’s or Beta blockers
• Evaluation of patients very early after acute MI (<3 days) or very early after stenting (<2 weeks)


Nuclear Imaging and Chest Pain

Asymptomatic


Nuclear Imaging
• Out comes data is good. Large area of ischemia, multiple ischemic locations, poor LV function, Lung uptake - bad prognosis
• Established for peri-operative ?? need
• Too sensitive for non-life threatening CAD
• High radiation exposure
• $$$$$$

Heart Scan CT calcium score

Calcium Scoring
If you know you are at high risk – How will a scan change outcomes?

Heart Scan CT calcium score
• If you want to do more angiograms promote CT Ca Score
• No outcome data but may add a little to Framingham
• Treat risk factors regardless of Ca• Insurance will pay in Texas• Radiation is likely greater risk than benefit
—radiation is lower than CTA or nuke, however

CT Angiogram


Asymptomatic
If you know you are at high risk – How will a scan change outcomes?

CHD Dissection PE - Good

Symptomatic CAD


Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.
Gibbons, R. J. et al. J Am Coll Cardiol 2010;55:483-495
Prognostic Value of Coronary CTA
CT Angiography
• Less invasive than cath—technology has outpaced our knowledge as to how to use it
• Radiation is high• Renal failure and contrast nephropathy
similar to Coronary Angiography• If need intervention radiation and contrast
is doubled• $$$$$$$$$

CMR appropriate use

CMR appropriate use
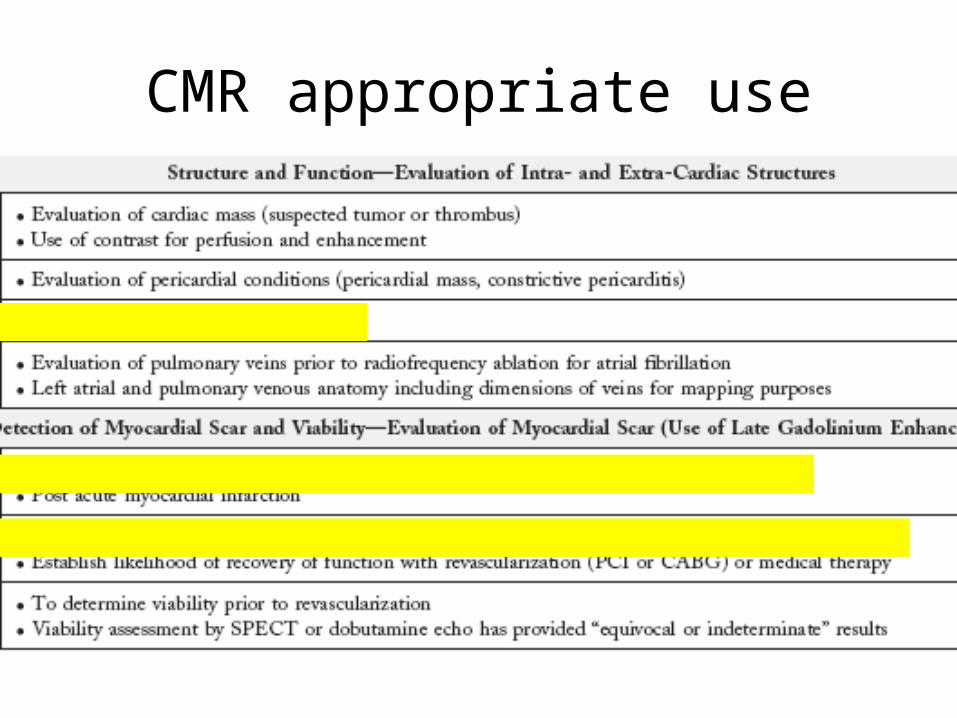
CMR appropriate use

Magnetic resonance imaging
• Public Health Advisory: Risk of Burns during MRI Scans from Transdermal Drug Patches with Metallic Backings
• Pacemakers, Defibrillators
• Tattoos (myth busters)
• Gadolinium nephrogenic systemic fibrosis (NSF) in renal insufficiency

Should I worry about radiation associated with medical testing?


17 CXR


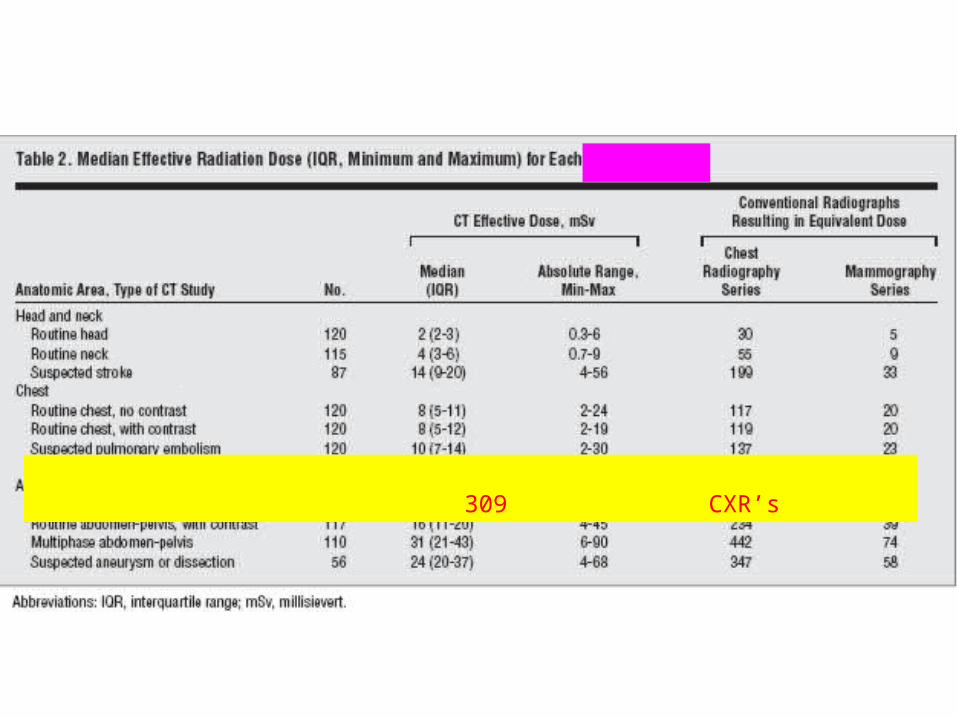
309 CXR’s

200 CXR’s
CT calcium score 20 – 262 CXR’s median 57 CXR’s
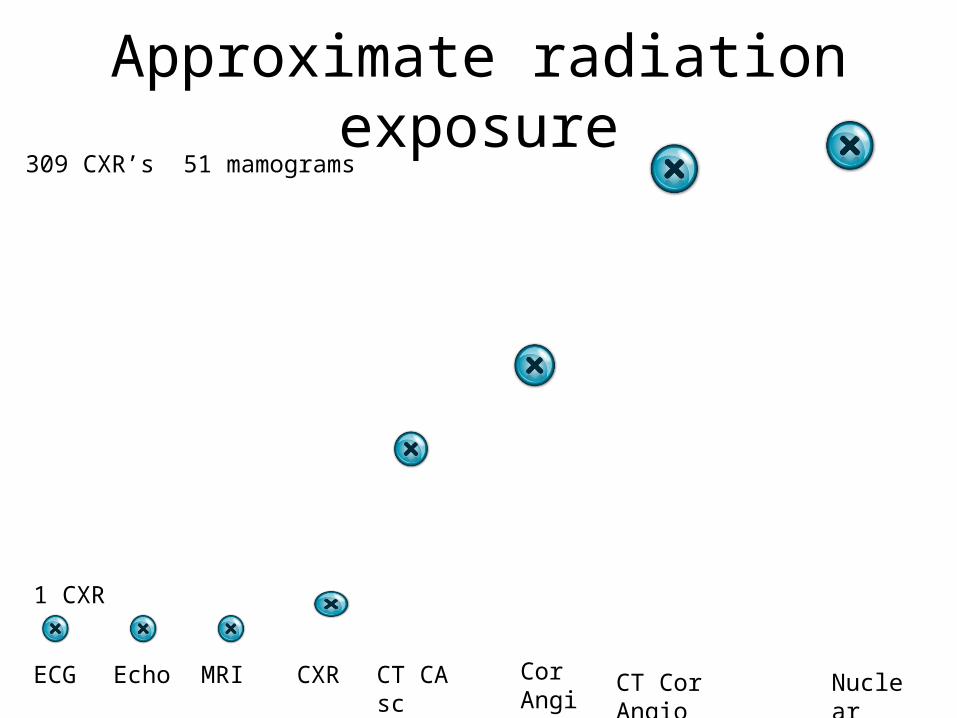
Approximate radiation exposure
ECG Echo MRI CXR NuclearCor Angio
CT Cor Angio
309 CXR’s 51 mamograms
1 CXR
CT CA sc

48% 2006
15% 1987
YOUR CHILDRENYOUR CHILDREN
SHOULD PLAN SHOULD PLAN
TO BETO BE
HEMOTOLOGY/HEMOTOLOGY/
ONCOLOGYONCOLOGY
DOCTORS!!!DOCTORS!!!

Echocardiography

Echo
• Echo is safe – no radiation• Information can change therapy• Good correlate to physical exam• Outcome data is good - sudden death,
CAD prognosis, Heart failure prognosis• It will do more in the future• It is such a good test the government will
make reimbursement zero $’s and hope you use the test anyway at your cost.

Types of Echo
• Transthoracic
• Transesophageal
• Stress- exercise and Dobutamine
2- and 3- D

Echo assessment Allows the assessment of:• Left ventricular size and function, including
regional wall motion abnormalities• Right ventricular size and function • Atrial abnormalities• The heart valves – Mitral, Aortic, Tricuspid and
Pulmonary (stenosis, regurgitation etc)• Intracardiac pressures• Lung pressures
http://www.asecho.org

Indications for Echo• MI/Chest pain• Murmurs• Heart Failure—right and
left/systolic AND diastolic• Pericardial
Diseases/Effusion• Endocarditis /
Myocarditis• Aortic diseases• Pulmonary Hypertension
• Dysrhythmias• Syncope• Dyspnea• Congenital Heart
Disease• Chemotherapy Toxicity• Stroke• Shock• Hypertension• Tumors/Masses

Stress Echo
• Similar appropriateness to RNI
• No radiation risk
• Less sensitive but more specific
• Technical limitation (patient, site, interpreters)
• $$ cheaper and getting cheaper
• Review on inappropriate use
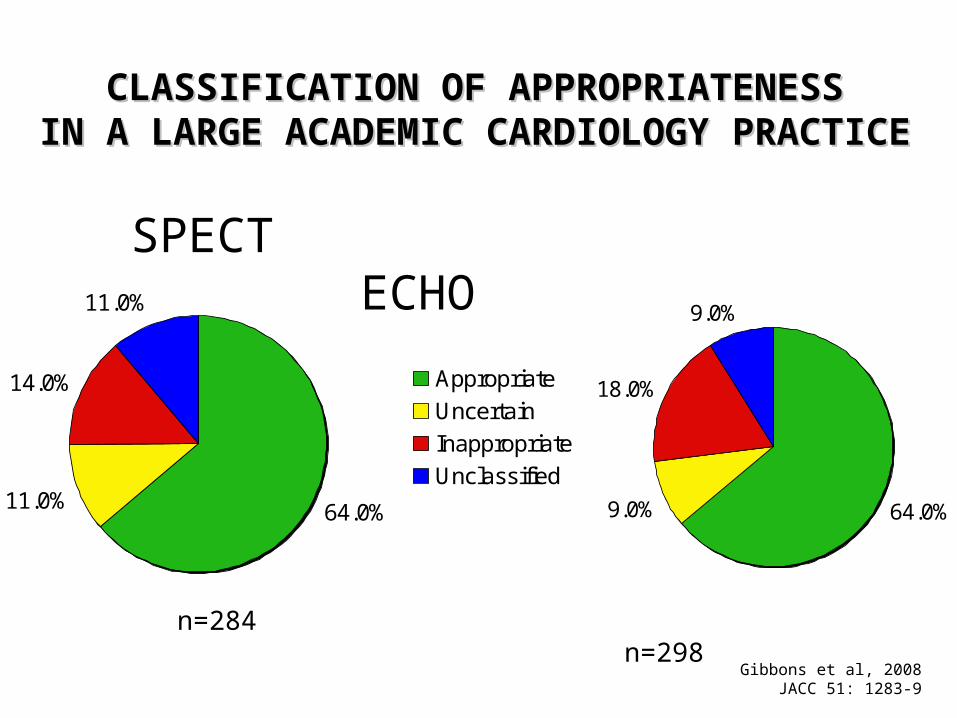
CLASSIFICATION OF APPROPRIATENESSCLASSIFICATION OF APPROPRIATENESSIN A LARGE ACADEMIC CARDIOLOGY PRACTICEIN A LARGE ACADEMIC CARDIOLOGY PRACTICE
64.0%11.0%
14.0%
11.0%
Appropriate
Uncertain
Inappropriate
Unclassified64.0%9.0%
18.0%
9.0%
SPECT ECHO
Gibbons et al, 2008JACC 51: 1283-9
n=284 n=298

Inappropriate Imaging IndicationsInappropriate Imaging IndicationsStress Echo and NuclearStress Echo and Nuclear
• Asymptomatic, low riskAsymptomatic, low risk 48% 48%• Pre-op, intermediate risk surgeryPre-op, intermediate risk surgery
able to exerciseable to exercise 17% 17%• Symptomatic, low pre-test probability,Symptomatic, low pre-test probability,
able to exerciseable to exercise 13% 13%• Pre-op, low risk surgeryPre-op, low risk surgery 10% 10%
Mayo Clinic, Gibbons et al, 2008
JACC 51:1283-89.

Conclusion
• Radiation is a serious threat
• We’re likely ordering too many imaging studies– Use the appropriateness criteria from the
ACC/AHA
• Never order a test unless you have a plan for the results

A CHEERFUL HEART IS GOOD MEDICINE– PROVERBS 17:22





























