Embed Size (px)
Citation preview

Pros and cons of FFR Pros and cons of FFR in multivessel in multivessel
disease: from FAME disease: from FAME to ACSto ACS
Giuseppe Biondi ZoccaiGiuseppe Biondi Zoccai
University of Modena and Reggio Emilia, Modena, University of Modena and Reggio Emilia, Modena, ItalyItaly
[email protected]@gmail.com

Learning goalsLearning goals
• Scope of the problem
• What are the implications of FAME
• What about the culprit lesion in ACS
• What about non-culprit lesions in ACS

The first coronary angioplasty The first coronary angioplasty by Andreas Gruentzigby Andreas Gruentzig

Extent of CAD in the VANWISH Extent of CAD in the VANWISH trialtrial
Kerensky et al, J Am Coll Cardiol 2002;39:1456-63
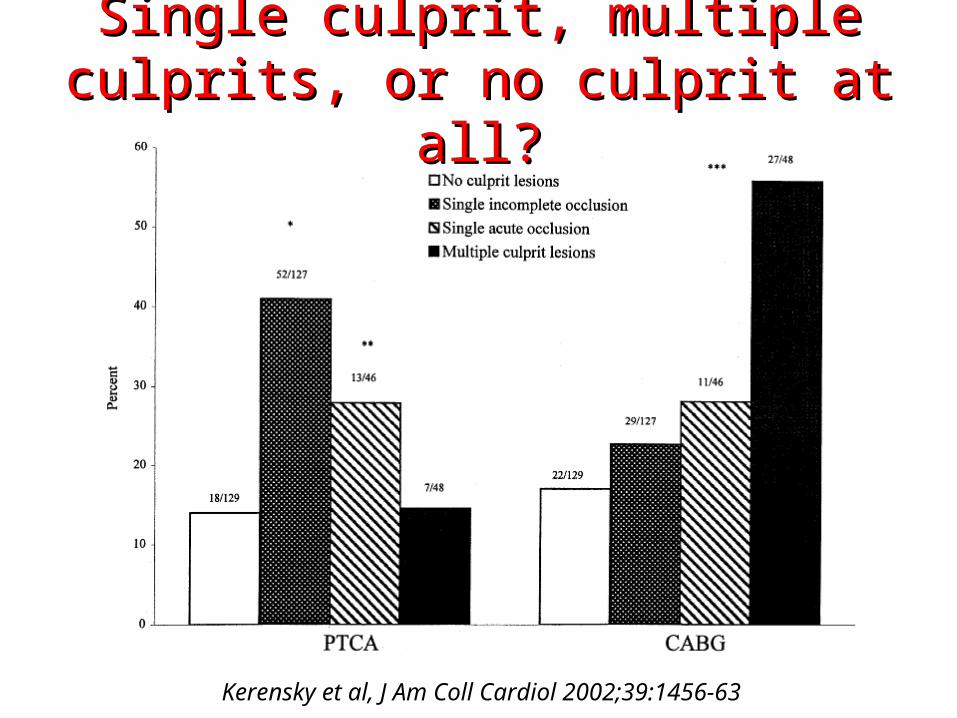
Single culprit, multiple culprits, Single culprit, multiple culprits, or no culprit at all?or no culprit at all?
Kerensky et al, J Am Coll Cardiol 2002;39:1456-63

What is most trustworthy?What is most trustworthy?
Melikian et al, J Am Coll Cardiol Intv 2010;3:307–14

Is SYNTAX no more such?Is SYNTAX no more such?
Nam et al, ACC 2011 (J Am Coll Cardiol 2011;57:E1090)
Learning goalsLearning goals
• Scope of the problem
• What are the implications of FAME
• What about the culprit lesion in ACS
• What about non-culprit lesions in ACS

Visual angiographic Visual angiographic assessment vs FFR in the FAME assessment vs FFR in the FAME
trialtrial
Tonino et al, J Am Coll Cardiol 2010;55:2816-21

FAME trialFAME trial

FAME at 2 yearsFAME at 2 years
Pijls et al, J Am Coll Cardiol 2010;55:2816-21

FAME: deferred groupFAME: deferred group
Pijls et al, J Am Coll Cardiol 2010;55:2816-21

Learning goalsLearning goals
• Scope of the problem
• What are the implications of FAME
• What about the culprit lesion in ACS
• What about non-culprit lesions in ACS

Acute microvascular damage in Acute microvascular damage in myocardial infarctionmyocardial infarction
STEMI
Variable degree of reversible microvascular
stunning
Maximum achievable flow is less
Smaller gradient and higher FFR across any
given stenosis
With time, the microvasculature may recover, maximum achievable flow may increase, and a larger gradient with a
lower FFR may be measured across a given stenosis

Similar stenosis but different extent Similar stenosis but different extent of perfusion areaof perfusion area

• 26 col-schema fcf (figuur)26 col-schema fcf (figuur)
Poor collaterals low FFR = 0.50
100
Pd
50
An identical stenosis, but...An identical stenosis, but...
0
• 26 col-schema fcf (figuur)26 col-schema fcf (figuur)
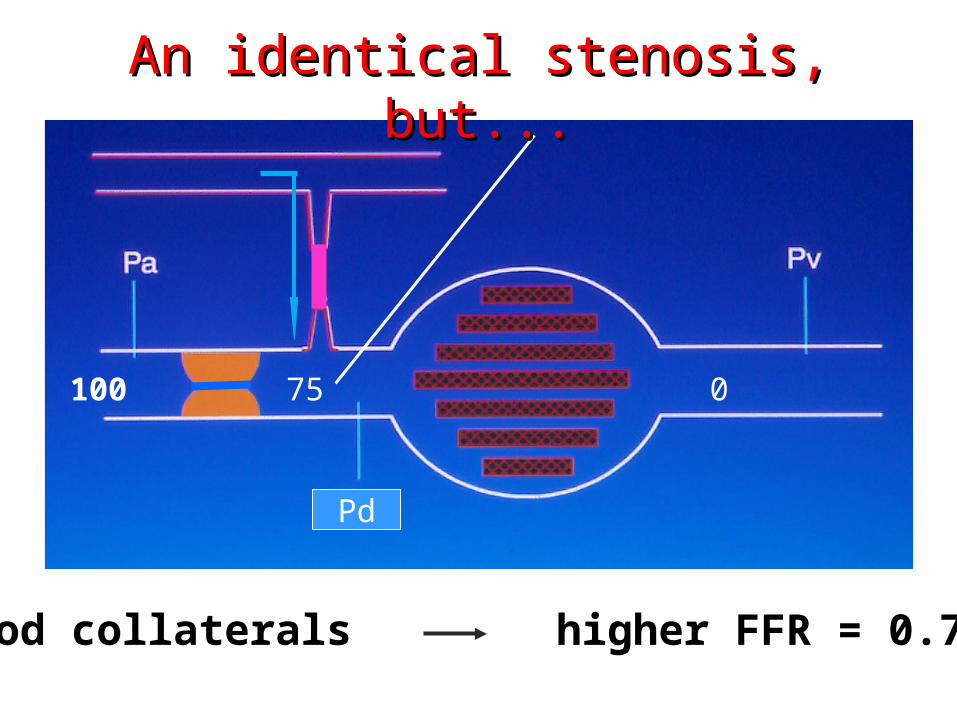
Good collaterals higher FFR = 0.75
100
Pd
75 0
An identical stenosis, but...An identical stenosis, but...

Visible collaterals on the Visible collaterals on the coronary angiogram (Rentrop) coronary angiogram (Rentrop) and fractional collateral blood and fractional collateral blood
flow Qc/Qnflow Qc/Qn

What about serial lesions?What about serial lesions?

What about severe left ventricular What about severe left ventricular hypertrophy?hypertrophy?
In severe left ventricular hypertrophy, there is an exaggerated increase of left ventricular mass in comparison to the vascular bed,
resulting in the potential for ischemia even in normal or almost normal coronary arteries
Thus, specificity may be reduced (cut-off >0.80?)However, sensitivity remains satisfactory

What about lesion length?What about lesion length?
Brosh et al, Am Heart J 2005;150:338-43
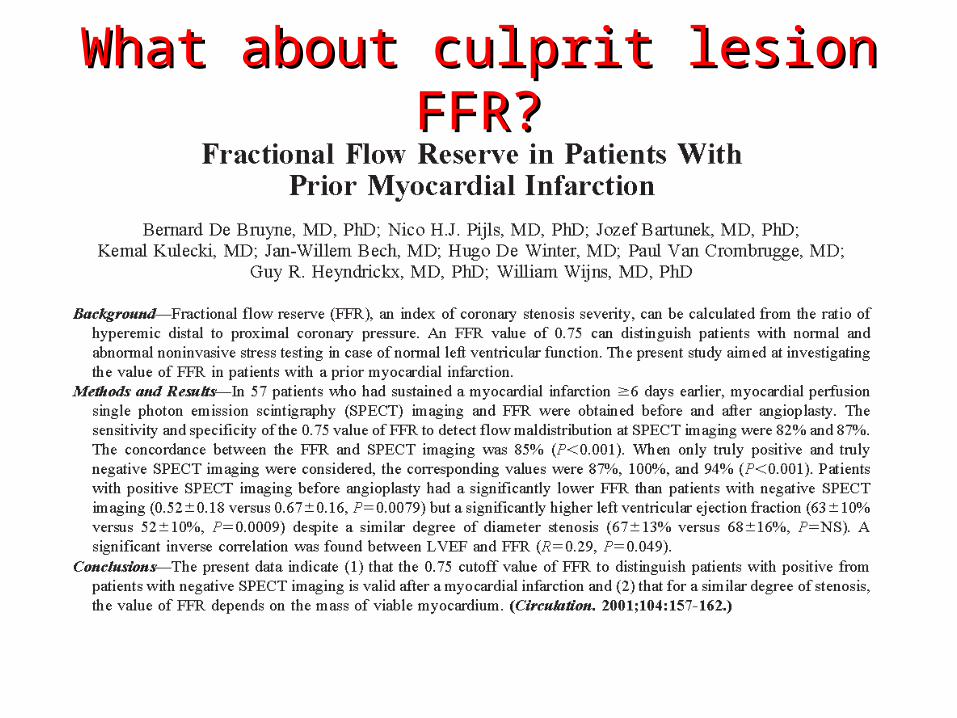
What about culprit lesion FFR?What about culprit lesion FFR?
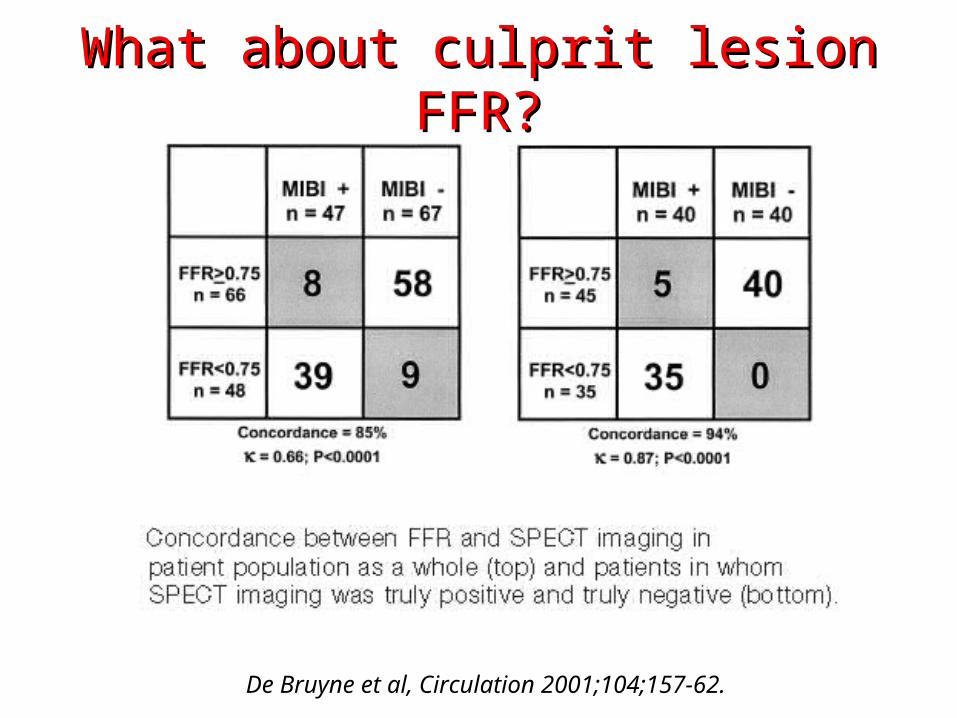
De Bruyne et al, Circulation 2001;104;157-62.
What about culprit lesion FFR?What about culprit lesion FFR?

What about culprit lesion FFR?What about culprit lesion FFR?

What about culprit lesion FFR?What about culprit lesion FFR?
Tamita et al, Catheter Cardiovasc Intervent 2002;57:452-9

What about culprit lesion FFR?What about culprit lesion FFR?
Beleslin et al, Eur Heart J 2008;29:2617-2624

What about culprit lesion FFR?What about culprit lesion FFR?

What about culprit lesion FFR?What about culprit lesion FFR?
Samady et al, J Am Coll Cardiol 2006;47:2187-93

Learning goalsLearning goals
• Scope of the problem
• What are the implications of FAME
• What about the culprit lesion in ACS
• What about non-culprit lesions in ACS
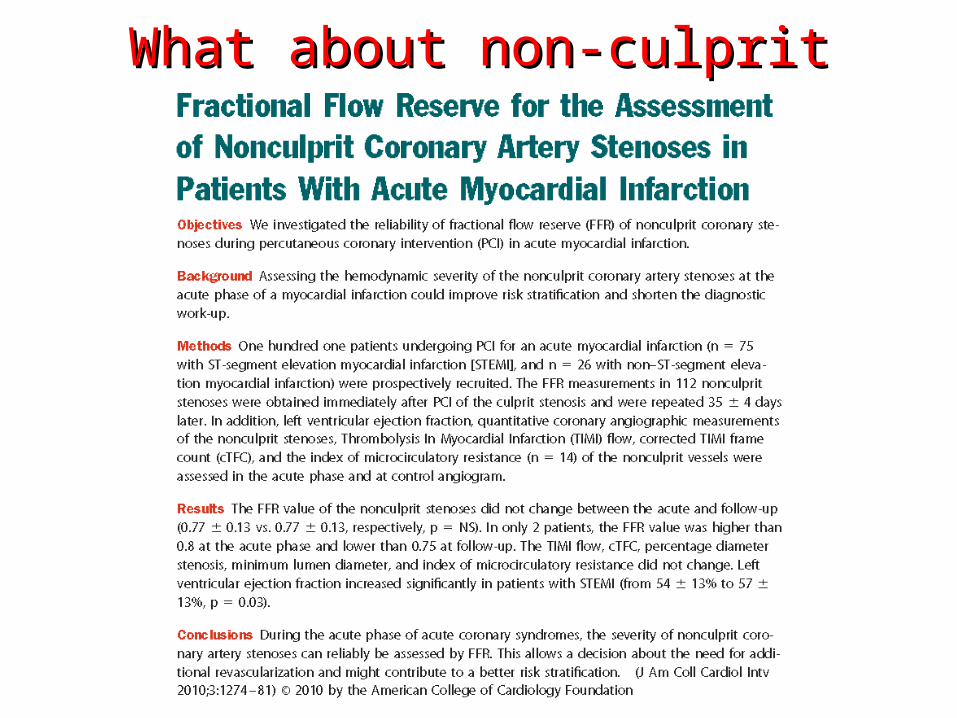
What about non-culprit lesions?What about non-culprit lesions?
What about non-culprit lesions?What about non-culprit lesions?
Ntalianis et al, Catheter Cardiovasc Intervent 2002;57:452-9

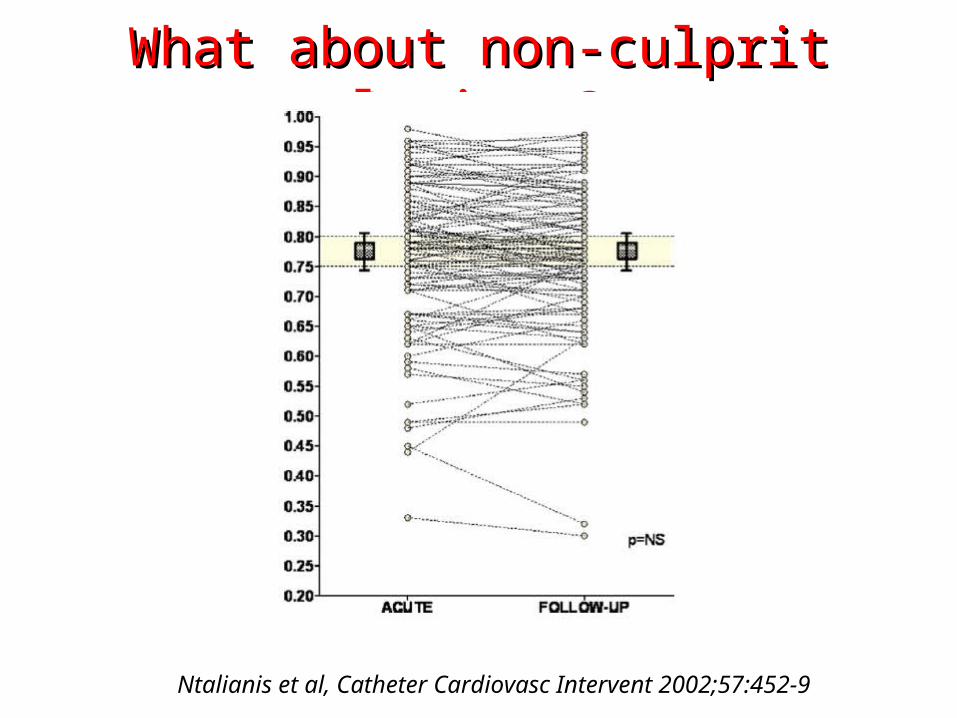
What about non-culprit lesions?What about non-culprit lesions?
Ntalianis et al, Catheter Cardiovasc Intervent 2002;57:452-9

Is it worthwhile?Is it worthwhile?

Take home messagesTake home messages

Take home messagesTake home messages
• FFR has been proved safe and effective in several settings, including 2 RCTs with clinically relevant end-point (DEFER and FAME)
• ACS do benefit from FFR as well as all others, with the notable exception of acute/subacute culprit lesions
• The upcoming FAME 2 trial will hopefully further support FFR, and provide us another argument against (or better on top of) medical therapy for CAD
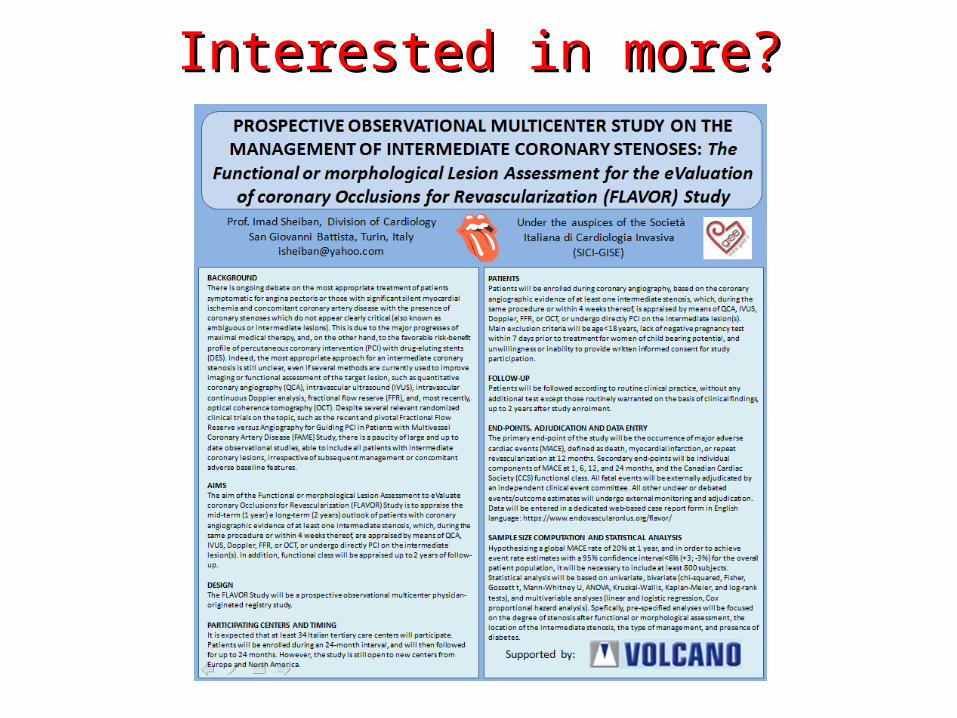
Interested in more?Interested in more?

Thank you for your attention
For any correspondence: [email protected]
For these and further slides on these topics feel free to visit the metcardio.org website:
http://www.metcardio.org/slides.html





























