Embed Size (px)
Citation preview

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 1
PROMOTING ATTENDANCE
POLICY
Under Review
Policy Extant Agreed vie Area Partnership Forum (APF) Review March 2019
Issued: 12th August 2004
National Review to be completed by Autumn 2016
Local Review 1 August 2016
Responsible Officer: Director of Human Resources on behalf of the Local Partnership Forum
Version No: 2*
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 2
PROMOTING ATTENDANCE POLICY
1. Introduction The greatest resource of Shetland NHS Board (the Board) is its staff, because it is through them that services are delivered and improved. Staff salaries are the single greatest cost to the NHS Shetland budget, and promoting attendance is crucial in the development of an efficient service, which has, at its core, the wellbeing of its staff. This document aims to give all those working in the service (managers and those being managed) clear guidance on the issues relating to promoting a healthy workplace and promoting staff health and attendance. Whilst the Board aims to secure the attendance of all staff, it is recognized that a certain level of absence due to sickness may occur and that the sensitive management of health problems and the promotion of good health contributes to the retention of these staff. The Board also recognises that there will be occasions where, after consideration, staff who cannot attend work due to their health problems may not be able to continue working. The Board’s procedures on Management of Capability and Discipline should also be referred to for guidance on the management of health problems as appropriate. In addition, the Board has complementary policies and procedures to support staff, for example Special Leave and flexible working practices, and these should also be considered when managing and promoting staff attendance.
2. Statement of Intent The Board is seeking to create and build up a working culture in which regular attendance at work is normal. This is helped by introducing:
monitoring and management procedures to identify situations where an employee’s attendance is falling below agreed standards; and
It is a question of achieving the right balance between managing absence efficiently and providing support and help to a member of staff who has health problems or is

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 3
experiencing personal difficulties. This Policy and the procedures that follow support this principle. Attendance levels provide a picture of staff well being, levels of morale and health and safety management performance. So, monitoring attendance levels is an important tool in assessing these factors and in deciding where action is needed. The importance of communication in the creation of such a working culture cannot be overestimated. Ensuring staff awareness of the importance of attendance is an essential prerequisite to everything that follows in these procedures. The objective of these procedures will only be achieved if a proactive, consistent and effective approach is adopted throughout the Board. This approach relies on:
ff, managers and staff representatives.
3. Why is this Policy necessary? The purpose of the Promoting Attendance Policy is to improve and support the health and wellbeing of staff at work and to reduce the level of sickness absence. The Policy will also encourage and enable the adoption and implementation of best practice in relation to the promotion of health and well being at work. For the year ending 31 March 2006, the sickness absence rate within NHS Scotland was estimated to be 5.23% (Source: ISD). NHS Shetland currently has a sickness absence rate of 4.23%, equating to approximately 10 working days for each employee. The target absence rate for NHS Shetland is 4% by March 2008. All staff have an eligiblity to sick leave and pay in accordance with their terms and conditions of service. There will not normally be any extension of sick pay provisions. Failure to adhere to absence reporting procedures, poor attendance or abuse of the sick leave provisions are, however, disciplinary offences and should be dealt with in accordance with the Board’s Disciplinary Procedures.
4 Aims The aim of this Policy is to help the Board make the most of attendance by reducing short and long-term absence through promoting positive attitudes to work and trying to reduce staff ill health as far as possible. However, it is important to remember that, “owing to the very nature of a ‘health-care environment’, the issues surrounding sickness absence need to be set in their own particular context.” (HEA).

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 4
The aims of the Promoting Attendance Policy are to:
possible levels of staff attendance at work;
– communicated to and understood by all staff – which makes sure that everyone is dealt with fairly and consistently;
reasonable adjustments to duties are made, or other suitable employment is offered through redeployment where necessary;
possible, offer appropriate support and help to get them back to work;
Occupational Health Service, staff support services and other specialist agencies;
redeployment is appropriate;
monitor attendance levels by setting up systems, through the Human Resources Department, which provides relevant and up-to-date information; and
by a staff representative, or colleague.
5. Putting the Promoting Attendance Policy into practice

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 5
The main principles
Board will use an approach that is consistent, fair, sympathetic and caring in nature.
rt and guidance of the Human Resources department, managers must make sure that they collect enough information on the nature and extent of the health problem in order to make a reasonable decision in each case. This involves setting up an effective communication system with staff, getting medical advice from the Occupational Health Service where necessary and seeking advice from the Human Resources Department. All information gathered will be processed in accordance with the requirements of
the Data Protection Act 1998 and the Information Commissioner’s Codes of Practice.
At all stages in this process:
contribute to possible solutions;
opportunity to be accompanied by a representative from a trade union or professional organisation or a colleague. A summary flowchart is attached as Appendix A. ;
6. Definitions used within the procedures 6.1 Sickness absence This occurs when ill health, including disability, makes a person unfit to work. It also occurs when a doctor advises an individual to stay away from work due to illness,

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 6
convalescence or the possibility of being contagious. (This is also covered in the Board’s Management of Employee Capability Procedures.)
6.2 Short-term absence Short-term absence is the period of time covered by a self-certificate (up to and including seven working days). This type of absence does not normally have a set pattern and is usually caused by minor, in most cases unconnected, ailments.
6.3 Frequent short-term absence This is where a member of staff has a number of short-term absences, which may or may not be related.
6.4 Long-term absence Long-term absence is the period of time covered by a doctor’s certificate (initially in excess of seven working days). For the purposes of this policy and procedures and the management of attendance, long-term absence within the Board will be regarded as 4 weeks continuous absence or longer. (See Appendix B)
6.5 Unauthorised absence This occurs when a member of staff’s absence:
for notifying the line manager/Board about the absence.
7. Putting the Policy and Procedures into practice 7.1 Promoting the Policy and Procedures
will have access to the Policy and procedures via the Board’s Intranet and through HR Policy and Procedures Manuals located throughout the Board. All new staff will be informed about the Policy and Procedures at the Corporate
Induction Session.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 7
The Policy and Procedures are referred to in the Staff Handbook.
procedures.
7.2 Recording and monitoring
Line managers are responsible for monitoring and recording absence data within their teams, and using the systems in place to ensure that this notified to the Payroll and Human Resources Departmens (eg, Payroll timesheets and Return to Work Interview Forms). The HR Department is responsible on behalf of the Board for collating data with regards to attendance (See Appendix D). Reasons for recording and monitoring attendance include:
Meeting the requirements of the Statutory Sick Pay provision and Occupational Sickness Allowance;
Identifying attendance patterns, and frequency and length of absences;
Helping to detect problems early, so leading to speedier management or medical responses;
Helping to decide whether the absence is a ‘capability’ or ‘disciplinary’ matter; and,
Helping to identify general issues relating to absence and health at work which can inform the implementation and development of relevant policies and procedures.
Managers must make sure that a record is made of any meetings that they have with members of staff to make clear the conversation that took place and the support that was offered.
7.3 ‘Trigger points’ It is important that managers have clear ‘trigger points’ in place for reviewing sickness absence. These ‘triggers’ include:
-term sickness absence, defined as four episodes or more than eight days’ short term sickness absence within a twelve month period
absence that is not satisfactorily explained;
absence that reaches a continuous period of 4 weeks (‘long term’ sickness
absence).
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 8
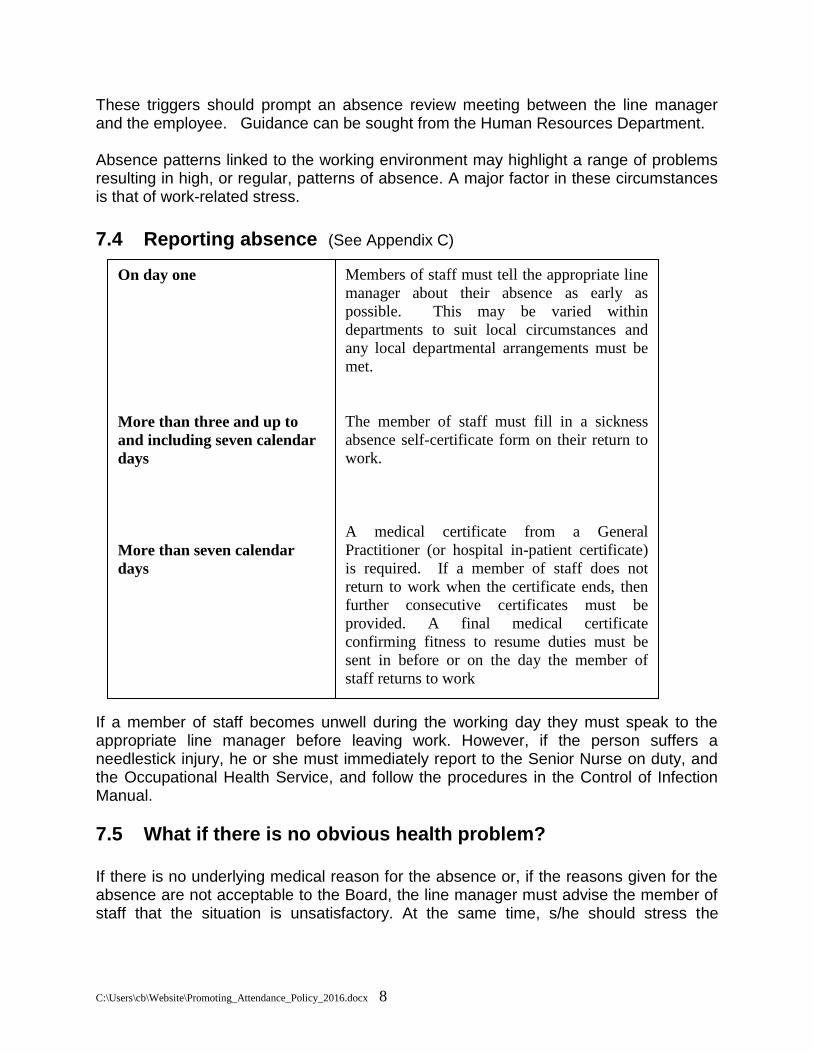
These triggers should prompt an absence review meeting between the line manager and the employee. Guidance can be sought from the Human Resources Department. Absence patterns linked to the working environment may highlight a range of problems resulting in high, or regular, patterns of absence. A major factor in these circumstances is that of work-related stress. 7.4 Reporting absence (See Appendix C) If a member of staff becomes unwell during the working day they must speak to the appropriate line manager before leaving work. However, if the person suffers a needlestick injury, he or she must immediately report to the Senior Nurse on duty, and the Occupational Health Service, and follow the procedures in the Control of Infection Manual.
7.5 What if there is no obvious health problem? If there is no underlying medical reason for the absence or, if the reasons given for the absence are not acceptable to the Board, the line manager must advise the member of staff that the situation is unsatisfactory. At the same time, s/he should stress the
On day one
More than three and up to
and including seven calendar
days
More than seven calendar
days
Members of staff must tell the appropriate line
manager about their absence as early as
possible. This may be varied within
departments to suit local circumstances and
any local departmental arrangements must be
met.
The member of staff must fill in a sickness
absence self-certificate form on their return to
work.
A medical certificate from a General
Practitioner (or hospital in-patient certificate)
is required. If a member of staff does not
return to work when the certificate ends, then
further consecutive certificates must be
provided. A final medical certificate
confirming fitness to resume duties must be
sent in before or on the day the member of
staff returns to work

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 9
importance of regular attendance at work and reaffirming the Board’s and/or departmental standards of attendance. In cases where circumstances and investigation indicate a more serious situation, it may be necessary to formally set appropriate standards for attendance which are consistent with the Board’s underlying approach to attendance. The line manager should meet with the member of staff to let him or her know that:
sely monitored;
monitoring period there may be the need for disciplinary action.
7.6 What if the absence is caused by a work-related or personal problem? In these circumstances assistance should be offered to the member of staff to help them overcome the problem. The assistance offered would be dependent upon the nature of the problem. Help could include temporarily altering their shift pattern or, if a personal problem, granting compassionate leave (not necessarily paid leave) if this is felt necessary. In these circumstances the member of staff must continually update their line manager, who will monitor and re-assess the support mechanisms as necessary. The Human Resources Department will give advice as appropriate. Members of staff may, dependent upon the nature of the absence, be referred to the Occupational Health Service.
7.7 The importance of maintaining contact During any periods of extended sickness absence, contact between the line manager and the member of staff is particularly important. The purpose of the contact is to:
r;
when; and
f’s health. It is important that managers apply a consistent approach when reviewing individual circumstances in order to prevent staff from feeling that particular members of staff are being singled out for special treatment. Any contact made should be sensitive and not intrusive and displaying genuine concern.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 10
The method and frequency of contact will depend on the circumstances surrounding the absence and managers will discuss this with their staff member should their absence be for more than seven consecutive days. Contact in the first instance should be by telephone. In cases of long-term sickness absence, it may be more appropriate to offer meetings at the member of staff’s home or within the workplace for face-to-face reassurance. If a meeting to discuss continuing long-term sickness absence is to be held, the member of staff should be asked if they wish to be accompanied. The Human Resources Department will also attend to give advice to the manager and the member of staff. It is important that such meetings are handled sensitively and the member of staff is assured that the meeting does not represent any kind of disciplinary procedure.
8. Return to work After any period of absence a member of staff’s return to work should be acknowledged by the line manager and a Return to Work Interview held. This is an informal meeting, which is to be recorded on the Return to Work Interview form (see Appendix E) which should then be forwarded to the Human Resources Department in a sealed enveloped marked Strictly Confidential). The purpose of the meeting is to:
necessary.
At this meeting the member of staff should be given the opportunity to raise any issues they have about their absence and to get help from the Board if appropriate. This discussion may cover some or all of the following, depending on the circumstances of each case.
-certificate or provides a medical
certificate as required. Seek reassurance that the member of staff is fit to return.
discuss a referral to Occupational Health.
member of staff know, explaining what the Board considers to be a reasonable standard of attendance and what may happen if this is not met.
regularly, for example a temporary change in hours or duties and training.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 11
or unpaid leave in line with other Board Policies and Procedures if this is appropriate.
misuse should be addressed under the procedures set out in the appropriate Board policy document.
If a discussion is necessary, this should not be confrontational in any way. It should rather be an investigation into any underlying problems - medical, work-based or domestic, which may be affecting attendance. If the reasons for absence are personal or sensitive, the member of staff may prefer to talk to someone outside the immediate situation, such as Occupational Health or to seek a referral to the staff counselling service through the Occupational Health Service. Where staff work in the Community and in other circumstances where a face-to face meeting cannot be reasonably achieved by the line manager (this would include single-handed practitioners and unreasonable further disruption to the delivery of health care services) and the absence has been for less than one week in duration, the discussion may be achieved by telephone with responses being appropriately recorded. For line managers with a significant number of direct reports, it is acceptable for return to work interviews to be appropriately delegated and recorded. It is of the utmost importance that all staff are treated equally and consistently and return to work interviews are required by the Board for all absences. The issue will be one of a reasonable approach in the circumstances.
9. Referring staff to Occupational Health Service (OHS) 9.1 Self-referral Members of staff should be made aware that they can self-refer to the OHS for any health related matter particularly if it relates to, or is affecting their work. Attendance at OHS is confidential and no communication to any third party will normally result from a self-referral unless the member of staff agrees it is work related or there is a legal requirement to be met. If members of staff are experiencing difficulties at work due to additional pressures, or intimidating or unwanted behaviour, then they should discuss this with either their line manager, the Human Resources Department or a Confidential Contact.
9.2 Management referral Managers can refer a member of staff to the OHS in order to provide assistance to the member of staff on a health related matter, or to enable the OHS to provide the manager with management advice about the member of staff’s health in relation to their

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 12
work. Before such a referral can take place managers must advise their member of staff. It is essential that such a referral is not portrayed as a punishment, and that the reasons for it are fully explained to the member of staff. The reason for referral should be clearly set out in Appendix G: Request for Occupational Health Referral along with any specific issues on which the line manager wishes to receive advice. In general, the types of issues about which questions might be asked include:
whether there is an underlying medical problem that could affect performance;
Prolonged sickness absence (periods of sickness absence of more than one calendar month
Short-term sporadic absence
the prognosis and likely effect on fitness for work;
restrictions to, or adaptations needed for, work;
the need for, and nature of, a programme of support (planning a phased return to work);
recommendations for rehabilitation into work; and
ill- health retirement issues, where relevant. The Occupational Health Service will in return provide a written report to the Manager, within 5 working days; the manager will then discuss this with the member of staff. Medical details provided to the OHS are confidential and are not passed on in reports to managers; the advice given is about fitness (or otherwise) for work, and any restrictions that might be needed. Managers are positively encouraged to contact the Occupational Health Service by telephone if they have questions on the advice given or need further advice or clarity. The Occupational Health Service welcomes feedback on the service provided, as this can be taken into account at service review meetings.
10. Assessing risk The Board will fully meet its responsibilities as laid down in health and safety law. This includes, where appropriate, carrying out a risk assessment before a member of staff returns to work.
11. Phased return to work and adjustments When a member of staff is fit to return to work but cannot carry out their full range of duties either in the short or longer term, every effort should be made to give them the opportunity for an earlier return to work. This might include reducing or amending their range of duties.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 13
The Board must take any steps which it is reasonable for it to have to take to reduce or remove any substantial disadvantage which a physical feature of the premises or of the Board’s employment arrangements causes a disabled member of staff compared to a non-disabled member of staff so as not to breach the Disability Discrimination Act (1995). Any adjustments should be made following:
advice and recommendations; with the member of staff; and
Reasonable adjustments to a member of staff’s job can include:
and
fittings and design. A clear written programme, including timescales and review period, must be agreed with the line manager and member of staff before any return to work can take place. The Human Resources Department must be involved with regard to reaching agreement on any variation to contract and pay policy. The use of flexible working arrangements and family friendly policies is encouraged. Assistance is available from the Disability Employment Advisers based within Job Centres and other agencies. They can support the member of staff and the workplace with respect to carrying out needs assessments, and they can advise on any equipment and modifications that might be required for the working environment. A more detailed framework for managing a Phased Return to Work is at Appendix G.
12. Redeployment If a member of staff has been identified as unfit to return to their current post, the Board must consider transferring the member of staff to fill an existing vacancy ( Reference Disability Discrimination Act 1995). The line manager should fully discuss with the member of staff all the options available for redeployment in line with the Board’s Redeployment Policy and must involve the Human Resources Department in such discussions to ensure up-to-date and relevant knowledge of the openings available. Redeployment may mean changing career direction and must include the assessment and identification of the person’s training needs. This should be discussed with either

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 14
the Human Resources Department or the Staff Development Manager. This may include providing training opportunities from:
Reference must be made to the Redeployment Policy before entering into discussions.
13. Ending employment and retirement Where a return to work is not feasible even though all options for reasonable adjustment or redeployment have been fully investigated and exhausted, then termination of employment on the grounds of ill health is likely to be necessary. In following this course of action the Board must demonstrate that the line manager:
ropriate
support, i.e. OHS;
le or
not practical; and fully involved the Human Resources Department. The fact that occupational sick pay is no longer being paid is not, in itself, a fair reason for dismissal. If termination of contract is the only available option, the member of staff must be invited in writing to attend a meeting to discuss the termination of their employment on grounds of incapacity due to ill-health. This meeting will be arranged and supported by the Human Resources Department who will also draft and send the letter of invitation. Such a meeting should not be a surprise to the member of staff, as significant other work will have been undertaken in this regard. The member of staff must be advised in the letter of the fact that termination is likely to be an outcome and must be offered the opportunity to be accompanied by a trade union or professional organisation representative or colleague at this meeting. The meeting will be handled in a sympathetic and understanding way, ensuring that the member of staff is given time to discuss their point of view and making certain they have a clear understanding of the outcome. It is unlikely that any new developments will be raised at this meeting.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 15
If the member staff is unable to attend a meeting, consideration should be given to meeting at the member of staff’s home (with their explicit consent). It may also be appropriate to involve OHS to ensure the least distress at this time. The Human Resources Department or nominated deputy will then write to the member of staff giving the termination date, taking into account the relevant period of notice. The letter will also set out the member of staff’s right to appeal against the decision. As the member of staff is still employed at this time, the appeal procedure will be through the Board’s Grievance Procedures.
14. Responsibilities In putting the Promoting Attendance Policy and Procedures into practice it is vital that all those involved (in other words, every member of staff) are fully aware of their role and responsibilities. The following section sets these out.
The member of staff should:
line manager
know, within the agreed procedures, about any absences and to produce medical certificates as necessary; understand the impact their absence has on the delivery of services;
et them know about their absence, length of time off and return to work date;
given for their benefit and recognise the positive support of going to these appointments; and see or talk to their line manager on return from sick leave by participating in a Return
to Work Interview.
The manager should:
way which will improve attendance levels, reduce absence costs and encourage staff to aim for high attendance levels;
individual circumstances and the member of staff’s right to confidentiality in relation to their absence;

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 16
reporting absences;
to be receptive, sympathetic and flexible in dealing with these problems, always letting staff know about the availability of any staff support services;
attendance procedures and the implications for their personal situation at all stages;
activities to prevent and reduce health problems as far as possible;
line with the Data Protection Act 1998;
hold Return to Work Interviews with their member(s) of staff upon their return and forward this paperwork to the Human Resources Department
get advice and support from the Human Resources Department, OHS, Health and Safety, the Employment Service and the Disability Employment Advisor when appropriate; and
ensure that staff involved in promoting attendance also receive training.
The staff representative should:
Partnership Constitution and Agreement; and
Human Resources should:
representatives when interpreting their obligations and the Promoting Attendance Procedures;
allow the procedures to be put into practice effectively;
throughout the Board.
The Occupational Health Service should:
problems have on the working environment; provide an advisory function to management on the implications of legislation in the
field of Health and Safety;

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 17
agencies to make sure that all relevant and appropriate information is available concerning the health of a member of staff;
volved in the earliest stages of staff absence to reduce the length of absence as far as possible and help the member of staff return to work; and
work with managers to identify and put appropriate solutions into place in the following ways:
letting managers know about any ways in which a member of staff’s medical condition might limit their ability to perform their normal duties;
advising managers on the length of time the member of staff’s ability to perform their normal duties might be limited once they have returned to work;
advising managers on the employment implications of any continuing disability, including recommendations on adjustments to their work, redeployment and legislative obligations;
advising on involving the Employment Service, and in certain circumstances disability employment advisors; and
advising the member of staff and the Board with regard to application for ill-health retrial, within the terms of the Superannuation Scheme for NHS Scotland.
15. Training The Board will provide training for all line managers in the effective and consistent application of these procedures.
16. Review The application of this Policy will be reviewed on an annual basis by the Human Resources Department on behalf of the Local Partnership Forum. Monitoring will be undertaken by the Local Partnership Forum, normally through the results of the Staff Survey and sickness absence statistics.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 18
PROMOTING ATTENDANCE FLOW CHART
Employee returns from absence
"Welcome Back"/Return to work discussion between manager and
employee
No
Is further action needed? YesContinue to monitor their
attendance & notify HR.
Is a referral to OHS
appropriate?
Continue to monitor their
absence. Does the absence
continue?
A standard is
setNo Yes
No
No further action
YesRefer to OHS.
Is other action necessary?
Ill health confirmed. Consider changes to
the empoyee's duties or hours or work
environmentYes
Set standardsNo ill health issues then consider
disciplinary action
No further action No Continue to monitor their attendance.
Does the absence continue?Yes
Consider disciplinary action No Is there a medical condition for the
absence?Yes
Consider redeploymentNo Is the employee able to return to their post? Yes
NoYes Adjustments made
to post
The person retires or the
contract ends for reasons of ill
healthPerson starts their new post Successful return to post.
Monitor and review the situation.

APPENDIX B
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 19
Continued certificated
sickness absence to 8
weeks minimum
Establish period of
certified absence of 4
weeks maximum
Return to full duty4-Return to full duty
3-See note Restricted Duties
2-Continued sickness absence toward expected recovery
1-Unfit to resume employment of any type** Return to restricted
duties
ACTIONS ACTIONS ACTIONS ACTIONS ACTIONS
Maintain contact with
employee
Offer support and advice
if appropriate
Monitor medical certificate
i.e. information source
* possible timespan
* diagnosis
* prognosis
* expected return
Judge potential of return to
duty usng above information
** Discuss
feasibility of
return to restricted
duties with HR
Notify following points:-
Availability of suitable post.
Reasonable adjustments.
Retraining if appropriate.
Discuss case with Head
of HR and Occupational
Health
Maintain contact with employee
Establish possible
outcomes via referral
to Occupational health
Access to Medical Records by
Occupational Health Dept if
appropriate
Report from Occupational Health
Continue monitoring of
sickness absence wih possible
referral to Occuaptional
Health if prognosis altered.
Discuss case
with HR
Discuss
options with
HHR/
Occupational
Health
Ill Health
Retirement
Ill Health
Termination
MANAGEMENT OF LONG TERM SICKNESS ABSENCE
OUTCOMES:

APPENDIX C
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 20
ABSENCE REPORTING: PROCEDURE FOR STAFF
1. It is the responsibility of all staff to ensure that every effort is made to communicate with the respective managers whilst on sick leave. All staff should ensure that they know the reporting arrangements within their work area, and whom they should contact if their manager is not available.
2. If you are unable to attend work, you must tell your manager at the earliest
opportunity before your starting time and no later than within one hour of your scheduled starting time.
3. It is your responsibility to make contact personally with your manager. Only in
exceptional circumstances where you are unable to phone personally, a relative or friend may phone on your behalf, but the responsibility remains with you. Where the manager is not available, it is essential that contact be made with an alternative senior member of staff who will be responsible for taking the information and passing it to the manager. Messages should not be left on voice mail, with the hospital switchboard or with other wards or departments.
4. Failure to make contact in time may lead to you being treated as absent, pay being stopped and may ultimately lead to disciplinary action.
5. It is important that you communicate all relevant details when making contact,
including:
The reason for absence (“sick” or “unwell” is not an adequate description); An indication of when you expect to be fit to return to work; and Details of any appointments with your GP.
6. At this stage, your manager will tell you when you should get in touch again and
when, if appropriate, a sick certificate must be submitted. 7. It is your responsibility to ensure you keep your manager informed of your
progress and, in particular, should you be unable to return when you anticipated. If you are absent immediately before leave days or days off, you must tell your manager when you will be fit to come back to work.
8. If your sickness is more than seven working days including weekends, a medical
certificate will be required from your doctor. Any subsequent certificates should be submitted timeously, ensuring all days in the absence period are covered. Failure to submit a medical certificate will result in pay being withheld.
9. If you fall ill at work or have to leave due to sickness or other reasons, you must
discuss this with your line manager or deputy before leaving.
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 21
ABSENCE MONITORING
1. Managers are responsible for collecting accurate information on both individual staff members and for their departments and for submitting that information to both the Payroll Department and the Personnel Department.
2. The manager records individual staff’s absence on an absence record form as
soon as they are informed by the individual of their absence. This should occur even where a member of staff has presented himself or herself for work and has had to go home.
3. Each individual’s absence including annual, statutory, sick, maternity and other
leave, will be recorded on the Payroll system. This information is used by the Human Resources Department to analyse absence. Managers should monitor individual staff’s absence on an ongoing basis, preferably after each period of absence to allow the manager to identify, at an early stage, areas of concern. The earlier issues are identified and discussed with the staff member, the more effective the response and action will be for both the staff member and manager.
4. Departmental absence is collated by the manager and submitted on a monthly
basis in the form of a time sheet to the Personnel Department and the Payroll Department by the 6th of each month.
5. The information collated is:
The number of available hours in the month; Number of hours lost through sickness by individual members of staff; and Number of hours lost through other absence by individual members of staff.
6. The ‘available hours’ figures should be based on the situation at the end of the
month and should include temporary staff but not bank or casual staff. Vacant posts should not be included in the figures. The ‘available hours’ should be calculated using the following formula:
Whole time equivalent x conditioned hours x 4.3
7. All sickness absence, certificated, uncertificated or self-certificated, long or short
term, should be included in the sickness absence figures. Where a member of staff has had to go home due to ill health, the part day should be included in the figures. Maternity leave should not be included in the figures for sickness absence.
8. Other absence figures should include: annual leave, public holidays, maternity
leave, training/study leave, etc. and should be clearly identified on the return. 9. Absence rates are calculated using the following calculations:
Sickness Hours in Month x 100 = percentage figure
Available hours
10. This figure will provide a consistent, simple measure against which comparisons can be made.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 22
11. The Human Resources Department will collect the absence information and the
present it to the Local Partnership Forum on a six monthly basis.
12. The Human Resources Department aims to produce the following documents on a monthly basis, once SWISS systems are in place to enable this to happen:
collated for the Board;
-by-month position.
13. It is the manager’s responsibility to investigate further the figures for their
department with support from the Human Resources Department.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 23
STATEMENT OF SICKNESS
Part 1 – STATEMENT: TO BE COMPLETED WHEN EMPLOYEE REPORTS IN SICK
Employee’s Name:
Post & Grade:
Date/Time of Notification:
Date/Time Sickness Commenced:
Anticipated Return Date:
Name of Person Receiving Notification:
Nature of Illness/Absence stated was:
Previous sickness/absence in last 12 months (not including this occurrence):
Total Number of days: ___________________
Total Number of occasions:_______________ Part 2 – STATEMENT TO BE COMPLETED WHEN EMPLOYEE RETURNS TO WORK
Duration of this period of sickness/absence From: To: No. Days:
Date of return to work interview:
Type of Certification Self Certificate Medical Certificate No Certificate
Did you seek medical guidance? Yes/No
If yes from whom? __________________
Is this episode linked to a previous Absence? Yes/No Give details:
Was absence related to an injury at work or work related accident or illness? Yes/No If yes provide Incident Report Reference:
Additional Comments / further actions:(include any requirements for adjustments/ improvements / referrals)
I certify that I have been unable to work (either with NHS Shetland or any other employer) during the period above due to sickness as stated and confirm the above information.
Employee Signature: Date:
Managers Signature: Date:
Part 3 – STATEMENT: FURTHER ACTION TAKEN
HR Department Consulted Date _________
Name________________
Advice given from Personnel Department:
Date referred to Occupational Health:
Date of Occupational Health Examination:
Date Occupational Health Report received:
Further discussion with HR Department
Advice Taken:
RETURN COMPLETED FORM TO THE OCCUPATIONAL HEALTH DEPARTMENT

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 24
APPENDIX F REQUEST FOR OCCUPATIONAL HEALTH REFERRAL
REFERRING MANAGER DETAILS
From:
Department:
Managers Post Title:
Line Manager (if diff from above) Tele No:
Who and where report to be addressed to: E-mail:
Date referred:
EMPLOYEE DETAILS
TITLE: Mr/Mrs/Miss/Ms/Dr/Other …………… (Please circle one)
Forename (s)
Surname:
Address:
Telephone No: (Home)
Mobile No:
DOB:
Job Title:
Place of
Work:
Hours of
Work:
Date
Appointed:
GP Details: (Name, Address)
OCCUPATIONAL HEALTH REFERRAL DETAILS
PLEASE NOTE A REFERRAL MAY NOT BE ABLE TO TAKE PLACE UNTIL YOU HAVE DISCUSSED THE REFERRAL WITH THE EMPLOYEE
1. Has any discussion taken place with the employee about their referral?
YES/NO (Delete as applicable) Please provide explanation/information if answered NO
2. Is employee currently on sick leave? YES /NO
3. If yes, what date did sick leave commence? _________________ If no, go to Q5
4. When does the current Medical Certificate run out? ___________________________________ What is the condition stated on the Medical Certificate? _________________________________

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 25
5. Describe briefly reason for appointment:
Please tick the following questions you would like the Occupational Health assessment to address: √
What is the employee’s current state of fitness to work?
If absent, what is the estimated return to work date?
Is there an underlying medical cause for frequent short-term sickness absence and, if so, is this
likely to continue?
What is the impact of the medical condition on the employee’s ability to undertake their
occupation?
Are there any duties the employee will be unfit to perform?
Are there any work modifications which would alleviate the condition or facilitate rehabilitation?
If a medical condition exists, is it likely to be made worse by work?
Is the medical condition work-related?
Is the employee on medication that would affect their ability to drive or undertake their
occupation?
Are ill-health retirement criteria likely to be met?
Has the employee any health condition or disability which could impair their ability to effectively
undertake the tasks in their role?
Any other questions or relevant background information?
If restriction to duties are required, how long might these be in place for?
Is the individual permanently unfit?
Please ensure that you have completed all relevant sections of this form then sign below and send in a sealed envelope marked as Confidential to the Occupational Health Department, Brevik House: Referring Managers Signature: __________________________________________ Print Name: ___________________________ Date: _____________________ Employees Signature: __________________________________________________
Print Name: ___________________________ Date: _____________________ To assist with your referral it would be helpful if you could enclose a copy of the following:- Job Description for employee Hazard Form for employee
Please give details sickness absence details for last 2 years
Any further details/questions can be attached as a separate sheet if required.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 26
Appendix G Phased Return to Work
1.0 Introduction 1.1 The purpose of a Phased Return to Work is to establish a temporary facility to restore the ability of an individual to work, thereby supporting them to maintain their skills and confidence.
1.2 The programme, including the timescale and review period, must be agreed between the H.R. advisor, manager/supervisor, Occupational Health Service, the employee and, if applicable, their representative. It is strongly recommended that the employee contributes to and remains actively involved throughout the process. 1.3 The principle of the programme is to provide the employee with the opportunity to begin a Phased Return to Work on a reduced workload with appropriately limited responsibilities and over an agreed time period build workload and responsibilities back to pre-absence levels in a managed, linear fashion. 1.4 The programme not only caters for the needs of the employee in question but also reduces potential financial burden on the organisation if the absence is being covered by bank/temporary staff and/or other staff in the department/area of work if the extra workload created by the absence is being shared. Managers should encourage a Phased Return to Work as an investment in an efficient and effective team.
2.0 The Benefits of a Phased Return to Work
2.1 A Phased Return to Work provides a mechanism which enables employees to return to work at an early date, with the ultimate aim of attaining full fitness to work. The benefits to the individual, their team and the organisation are as follows: Benefits to the Individual
The retention of competence, motivation, skill, peer and workplace interaction;
An enhancement of self esteem and self development;
The prevention of social stigma, isolation, and loss of confidence;
Improvements to well-being.
Benefits to the Work Team
The provision of support to colleagues;
The setting of a standard of fairness to all;
A contribution to workload;
The return to the workplace of a skilled and valued individual.
Benefits to the Organisation
A demonstration that the organisation values employees;
A mutually agreed return to duty at an early date;
The development of an enabling culture;
An effective use of resources.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 27
3.0 Return to Work Process
3.1 A collaborative approach is essential for this process to be effective. Liaison between some/all of the following people can be expected:
Employee;
Manager/supervisor;
Department Manager;
Occupational Health Services staff;
GP;
Human Resources advisor;
Employee's representative;
Other appropriate specialists. 3.2 While arrangements made to facilitate the Phased Return to Work are of a confidential nature, the operational requirements of the process may dictate the sharing of specific information, in confidence, with certain parties.
3.3 In line with the Promoting Attendance section of the Managing Health at Work PIN Guideline, the employee who is absent from work due to ill health will have the opportunity to meet with their manager/supervisor after a defined time. At this stage referral to the Occupational Health Service will be made if appropriate (see Paragraph 9.2 of the Promoting Attendance Policy). This referral should include previous sickness absence records. If the employee is deemed an appropriate candidate for a phased return, and is in agreement to participate in the procedure, liaison with relevant parties and key activities must take place. Specifically this will include:
Occupational Health Services assessment of the employee's capabilities and limitations;
The manager/supervisor identifying appropriate work opportunities e.g. job modification or alternative duties which may extend beyond the employee 's normal work base;
Collaboration between the appropriate staff to match the employee's ability to the available options;
Communication between appropriate staff of clear, agreed and achievable goals with a return to full duties expected within an agreed timescale;
Creation and implementation of a Phased Return to Work Programme unique to each occasion with agreed frequency of monitoring as deemed appropriate for that employee. The manager/supervisor is required to formally review the employee’s progress no less than weekly, in the first instance, with Occupational Health formally reviewing after two weeks, unless requested otherwise by the manager/supervisor. This review should take the form of a face to face meeting;
As part of the joint review, ongoing evaluation of the effectiveness of the programme will take place, with modifications made as appropriate;
The manager/supervisor has a duty of care (as defined in Health and Safety at Work legislation) to ensure that the employee or their colleagues or any other parties are

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 28
not placed under any undue risk to their health and safety during the Phased Return to Work Programme;
The manager must keep records of the agreed Phased Return to Work including any revised Risk Assessments.
4.0 Responsibilities
4.1 The manager/supervisor has a responsibility to:
Ensure the employee is jointly involved throughout the process;
Carry out a Risk Assessment and ensure it is updated where appropriate;
Advise the Occupational Health Service on the availability of job modification or alternative duties. Where these are not available due to organisational needs it may be deemed that a Phased Return to Work is not possible;
Ensure duties, workload are clearly identified and expectations understood;
Ensure any adjustments made to the Phased Return to Work Programme prior to signing are in keeping with the principles of the initiative.
Agree and sign the Phased Return to Work Programme
Counsel the employee to seek advice from either the Occupational Health Service or the Human Resources Department if in doubt regarding the Phased Return to Work Programme.
4.2 The employee has a responsibility to:
If required identify and involve an appropriate representative from the outset of the programme (e.g. union rep, friend, colleague)
Contribute to the Risk Assessment
Bring to the manager's/supervisor's attention any issues or concerns regarding the programme which may affect its success.
Agree and sign the Phased Return to Work Programme
4.3 The Occupational Health Advisor has a responsibility to:
Liaise with the employees’ manager/supervisor or department manager to identify and agree appropriate work opportunities e.g. job modification or alternative duties prior to drawing up the Phased Return to Work Programme;
Draw up the Phased Return to Work Programme. (See attachment 1.);
Ensure the programme is clearly understood;
Advise the line manager where a Phased Return to Work is not possible. This may require the individual to be redeployed.
4.4 The HR Advisor has a responsibility to:
Provide clear guidance on terms and conditions of the Phased Return to Work Programme.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 29
5.0 The Programme 5.1 The Phased Return to Work Programme is linked to absence management. In implementing this procedure, managers/supervisors should embrace the ethos of Employee Friendly Policies and should consider the following as part of the programme:
Reduced hours;
Alteration to shift pattern/days;
Modified duties;
Buddy system/mentor/supernumerary status;
Temporary relocation/role;
Release to allow attendance for treatment/therapies;
Team approach to rehabilitation.
5.2 The duration of the programme should be appropriate to the severity of the illness/injury which caused the absence and its impact on the individual. Allowances should be made for individual variances. A time period of 2 to 4 weeks would be considered normal but may be extended in exceptional circumstances as identified in section 1.2 above.
6.0 Risk Assessment 6.1 In considering the rehabilitative duties the manager/supervisor must consider the health and safety of not only the employee who is returning to work but also that of other employees and affected parties. Assistance with Risk Assessment is available from the Occupational Health service.
7.0 Terms & Conditions 7.1 As stated in Section 5.2 the duration of the programme should be appropriate to the severity of the illness/injury. A time period of 2 to 4 weeks would be considered the normal maximum period for a PRTW. If the employee has not successfully reintegrated into their full contractual hours and duties by this time, the OHS should be asked about the likelihood of future recovery including anything that may be hindering recovery. At this point, a more permanent arrangement may be considered i.e. redeployment to a more suitable job, permanent reduction of hours, job share etc. If, from the outset, it is obvious that a longer PRTW will be required (e.g. serious back injury returning to manual labour type task) then the group (as identified in Section 1.2 - OHS, employee, line manager, HR and, where appropriate, Trade Union representative) should define this during the initial meeting to decide the PRTW programme. This will reduce the need to meet every 4 weeks if/when not required. By definition more complex cases such as the example given will require ongoing, close monitoring. Responsibility for this rests with the line manager, backed up by the OHS however the full group may be required to reconvene and reconsider the case.
8.0 Pay

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 30
8.1 An employee, who returns to work as part of a PRTW programme, will receive the same pay they would be entitled to under their relevant Sick Pay Scheme. However, since the employee in question will not be deemed to be “sick”, the pay will not be regarded as “sick pay” and the employee need not submit doctor’s certificates to be able to receive their pay during the PRTW programme. For example: If the employee is receiving full sick pay, they would receive the same pay they would be entitled to under the relevant Sick Pay Scheme from the date of commencement in the PRTW programme, regardless of the hours they were working as part of this. Should the employee be on half-pay, but increase their hours during the PRTW beyond half hours, they will be paid for the hours that they work. Should the employee have exhausted occupational sick pay, they will be paid in accordance with actual hours worked throughout the phased return to work period and return t o full pay when contractual hours are resumed. 8.2 The employee will be permitted to off set any accrued annual leave entitlement, against adjustments to hours, in order to reach the equivalent of their contractual hours and achieve full pay, during the phased return to work period. 8.3 A phased return to work agreement is aimed at facilitating an employee’s return to work during long-term absence by providing reasonable adjustments to promote attendance. Occupational Health will provide guidance of what adjustments might be appropriate in order to achieve this. This may be a reduction/change in hours or responsibilities. If an employee has been signed back, or deemed fit to return to work by their GP, the Line Manager through consultation with the staff member will decide the required adjustments to enable the return to work. 8.4 The employee has the opportunity at any time during the phased return to work period to suggest changes to the adjustments agreed through discussion with their Line Manager. The Line Manager may seek confirmation of the change via Occupational Health if they are not in agreement with the employee or they deem necessary.

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 31
NHS SHETLAND
Phased Return to Work Proforma. Name:……………………………………………………………..Date: Department: Role: Relevant restrictions: Time: Agreed working hours.
Mon Tue Wed Thu Fri Sat Sun
Week 1
Week 2
Week 3
Week 4
Duties: Agreed changes and/or restrictions to normal duties. ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… ………………………………………………………………………………………………………………. Other: Any other relevant information. ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………….

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 32
Signed as understood and agreed: Employee:……………………………………………………………………Date………………………. Manager/supervisor…………………………………………………………Date………………………. Occupational Health ………………………………………………………..Date……………………….

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 33
Date Due For Review/Next Review December 2009
Person Responsible For Arranging Review Director of Human Resources
Person Responsible For Publishing Results Of Impact Assessment Director of Human Resouces
Results Due To Be Published YES (Inranet and Internet)
Person Responsible For Arranging Monitoring
Signed Lorraine Hall
DATE 12 January 2007
Organisation Shetland NHS Board
Person Responsible
Department
Name Of Policy Or Function Has the policy or function been assessed for relevance to the General Duty under the Race Relations (Amendment) Act 2000?
Timescale For Impact Assessment Due Date 12 January 2007
Policy New Function Existing (Revised)
Associated Policies Or Functions:
Shetland NHS Board
NHS Scotland Partner Organisations

C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 34
Rapid Impact Checklist: Summary Sheet
Positive Impacts (Note the groups affected)
All staff groups: aiding staff to return to work sooner with support and a positive infrastructure, give clear guidelines for staff and managers about their rights and responsibilites, consistent and evenly and equally ensuring no discrimination, organisational effectiveness improves, process enables higher communication aiding motivation and moral.
Negative Impacts (Note the groups affected)
Additional Information and Evidence Required Consultation conducted
Recommendations Policy/Function amended to stop or reduce adverse effects
From the outcome of the RIC, has a full EQIA process been recommended? If not, why not?
No adverse negative impacts

APPENDIX C
C:\Users\cb\Website\Promoting_Attendance_Policy_2016.docx 35
SEHD/NHSScotland PFPI/Fair for All Equality and Diversity Impact Assessment - Rapid Impact Checklist
Which groups of the population do you think will be affected by this proposal? Other groups: 1. Volunteers
minority ethnic people (incl. gypsy/travellers, refugees & asylum seekers)
women and men
people in religious/faith groups
disabled people
older people, children and young people
lesbian, gay, bisexual and transgender people
people of low income
people with mental health problems
homeless people
people involved in criminal justice system
staff
2. Workers
N.B. The word proposal is used below as shorthand for any policy, procedure, strategy or proposal that might be assessed.
What positive and negative impacts do you think there may be?
Which groups will be affected by these impacts? What impact will the proposal have on lifestyles? For example, will the changes affect: Diet and nutrition? Exercise and physical activity? Substance use: tobacco, alcohol or drugs? Risk taking behaviour? Education and learning, or skills?
Staff Positive impact on keeping staff in work and re-training.
Will the proposal have any impact on the social environment? Things that might be affected include Social status Employment (paid or unpaid) Social/family support Stress Income
Social Status Phased return to work. Positive impact on health and working lives as phased retunr to work plus favourable opportunities. Employment Dependent on circumstances of staff. Redeployement opportunities offered. Income Dependent on individual choices.
Will the proposal have any impact on Discrimination? Equality of opportunity? Relations between groups?
Positive outcome due to standardised process all staff respected equally.
Will the proposal have an impact on the physical environment? For example, will there be impacts on: Living conditions? Working conditions? Pollution or climate change? Accidental injuries or public safety? Transmission of infectious disease?
Positive working condition (potentially if amendements/changes.adaptations to workplace have to happen?
Will the proposal affect access to and experience of services? For example, Health care Transport Social services Housing services Education