Embed Size (px)
Citation preview

203
Promising Directions for the Diagnosis and Management ofGynecological Cancers
EC KOHN1,2, GB MILLS3 and L LIOTTA1
1Laboratory of Pathology and 2Gynecologic Malignancies Faculty, Center for Cancer Research, National Cancer Institute, Bethesda, MD;3Department of Molecular Therapeutics, Division of Medicine, MD Anderson Cancer Center, Houston, TX, USA
ABSTRACT
Diagnosis and management of cancer requires tools with both high sensitivity and specificity. The minimally invasive cervical smear hasdemonstrated how a test, even one with low specificity, can change the public health profile of a cancer from a late stage deadly disease toearly diagnosis with rare tumor-related deaths. The benefit of such a test is best demonstrated by the low frequency of cervix cancer and itsgood outcome in countries where this test is readily available and used with appropriate secondary follow up. Early and specific symptoms, andidentification and prevention for high risk groups has had similar impact for endometrial cancer. Neither a robust test, nor reliable or specific earlysymptoms are available for ovarian cancer, making clinical and scientific advances in this area a critical world-wide need. Current approachestesting one protein or gene marker at a time will not address this crisis expeditiously. New sensitive, specific, accurate, and reliable technologiesthat can be implemented using high throughput mechanisms are needed at as low a cost as possible. Ideally, these technologies should be focusedon readily available patient resources, such as blood or urine, or as in the case of cervix cancer, minimally invasive informative approaches such ascervical smears. Techniques that allow data mining from a large input database overcome the slow advances of one protein–one gene investigation,and further address the multi-faceted carcinogenesis process occurring even in germ line mutation-associated malignancy. Proteomics, the studyof the cellular proteins and their activation states, has led the progress in biomarker development for ovarian and other cancers and is beingapplied to management assessment. Amenable to high throughput, internet interface, and representative of the proteome spectrum, proteomictechnology is the newest and most promising direction for translational developments in gynecologic cancers.
NEED FOR BIOMARKERS INGYNECOLOGIC MALIGNANCIES
Clinical conundrums currently facing our discipline arethe detection of ovarian cancer at a stage of developmentwhere intervention has a high likelihood of cure or longterm remission, as well as the identification of the subsetof early stage gynecologic cancer patients who are athigh risk of recurrence and death from cancer. Earlydetection of ovarian cancer has been plagued by the lackof clinically specific symptoms, poor specificity of thephysical examination, and a minimally invasive highlyspecific screening test. Like most other solid tumorswhen identified early, ovarian cancer is amenable tosurgical extirpation and, with additional chemotherapywhere indicated, can have up to a 95% five and ten yearsurvival [1]. Unfortunately, only 15–20% of patients arediagnosed with stage I ovarian cancer and of those, manyare not anticipated to have a malignancy prior to surgeryand may not receive optimal surgical evaluation [2].A biomarker that allows early detection in the absence
of a change in surgical or medical treatment may cause apopulation stage shift and lead time outcome bias as wasinitially seen with mammography and adjuvant therapyin breast cancer [3]. However, longer term follow up ofthe impact of mammography and adjuvant chemotherapyhas now been shown to cause a real benefit and increasein overall longevity. Thus, a shift of stage at diagnosis in
ovarian cancer should have a marked impact on publichealth. A shift to early detection would lend increasingimportance to a second goal for biomarker developmentfor early diagnosis. We need a reliable mechanism toidentify those patients with early stage limited diseasewho will relapse and die of disease. Again, as withother solid tumors including breast cancer, there remainsapproximately 15–25% of early stage patients who willsuccumb to disease [1]. Do these patients have a uniquemolecular subtype of cancer not discernable with currenttechnology? Newer data with cDNA microarray analysisis uncovering gene transcription signatures that suggesta new molecular subtyping may be useful in ovarianand other cancers [4,5]. We need to determine how toidentify this patient subgroup and then to tailor therapyaccordingly. This approach would limit the numberof early stage patients subjected to chemotherapy forwhom it may not have been necessary. Identificationof biomarker diagnostics for early detection and fordiscrimination of those cancers likely to recur will allowindividualization and optimization of therapy for womenwith gynecologic malignancies [6].
PROTEOMICS: DEFINITIONS ANDTECHNIQUES
The proteome is the array of expressed proteins. It varies
Correspondence to: Elise C. Kohn, MD, Laboratory of Pathology, Center for Cancer Research, National Cancer Institute, Bethesda, MD, USA.E-mail: [email protected]

204 EC KOHN, GB MILLS, L LIOTTA
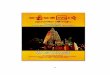
Fig. 1. Application of serum marker screen/ultrasound approach to ovarian cancer screening. Single biomarkers, such as CA125, multiplexbiomarkers, or signature comprising information of hundreds to hundreds of thousands of input points can be used as a primary screen in thediagnostic paradigm for ovarian cancer.
temporally and spatially within and between organs. Thecomplexity of this dynamic component of the bodyis further expanded through co- and post-translationalprotein modifications, activation status, and breakdownproducts. This array of variation is important. As isdemonstrated in the immune system, a very small peptideepitope may stimulate an active immune response. Thehuman genome contains only 30–35,000 genes; signalamplification occurs at the level of gene transcriptionin promoter regulation, copy number, alternative splicingand transcript stability. Further amplification occurs withprotein translation and modification coupled with proteinstability. The proteome, predicted to be between 1.5and 100 million different units, is therefore the mostbroad and actively changing representation of an organ’sfunction at any given time. The serum proteome, proteinsand protein products in circulating blood, is thus the mostcomprehensive general source of information in the bodythat can contain information regarding organ-confinedevents, and host responses. New technologies are underdevelopment for optimal mining of this data reserve andto apply it for patient benefit [7].Mass spectroscopy is a technique long used to charac-
terize and identify chemicals and proteins in the labora-tory and the clinic. Its sensitivity has increased with morecomplex machinery such that mass spectroscopy toolsnow can discriminate hundreds of thousands of signals.Mass spectroscopy can “see” changes in the snapshotof the proteome at a given time. The complexity ofthe signal can be pared down by coupling with chip-based protein capture systems to create a first level
sample fractionation. Solid phase bait chips can narrowthe selection to hydrophobic interactive proteins or thosewith selected properties, such as aliphatic or minimallycharged proteins. The spectroscopy pattern from a givensample will differ with the bait used for selectionand therefore can provide opportunities to analyze thepotential dataspace from multiple views. The resultantdatastreams must then be mined for their hidden valuesand properly applied for patient benefit.Bioinformatics has advanced dramatically in the past
decade and is now an important adjunct tool in clinicaldiagnostics. Multiple higher order analytic programs havebeen developed with which to mine the large databasesdeveloped using mass spectroscopy proteomic tools andthose emanating from genomic and transcriptomic arrayanalyses [8,9]. Decision trees have been developed,tested, and shown to offer discriminating capacity. Thesedirections of mass spectroscopy coupled with complexbioinformatics analysis are being harnessed and appliedfor clinical biomarker development [10].
PROTEOMIC BIOMARKERS OFDIAGNOSIS
The search for biomarkers of ovarian cancer diagnosisand specifically early diagnosis has been ongoing fordecades [11–16]. CA 125, the work horse of ovariancancer detection, has an unacceptably high false positiverate leading to invasive assessment and a high falsenegative rate, especially in early stage disease and lowvolume disease leading to inappropriate reassurance [17].

PROMISING DIRECTIONS FOR THE DIAGNOSIS AND MANAGEMENT OF GYNECOLOGICAL CANCERS 205
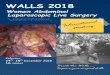
Serum proteins
Mass spectroscopy
Proteomic image
Pattern recognitionlearning algorithm
Early diseasediagnosis
Risk analysisearly
recurrence
Fig. 2. Paradigm for application of serum protein pattern diagnostics. Proteomic signature biomarker analysis, following validation in prospectivetrials, can be developed for high throughput. Blood samples can be subjected to mass spectroscopy in a central reference laboratory, datastreamssent to bioinformatics algorithms, and results received in a confidential webcentric platform.
However, recent data in the longitudinal series of studiesof Jacobs and coworkers and Skates has shown that therate of change of CA 125 may increase its predictivevalue [18,19]. A small but real increase in detection ofearly stage cancer has been projected. However, CA 125alone or in combination with color Doppler ultrasound isunlikely to be sufficient for the detection of early stageovarian cancer [20,21].Numerous investigators are working on biomarker dis-
covery in ovarian cancer using cell lines, tumor samples,and patient serum samples. Applied techniques includecandidate marker validation [22–24], and global unbiasedsearches using cDNA microarray screening [25,26], geneexpression patterns [5,27,28], protein screening [29,30],and proteomic pattern analysis [10,31,32]. The lackof a precursor lesion or known pre-cancer syndromecombined with the relative rarity of ovarian cancer hasmade this challenge more difficult. As approximately 1 in2500 postmenopausal women will develop ovarian cancerin their lifetime, coupled with 70% or more of patientspresenting with advanced stage disease, the detection ofearly stage disease is a “needle in a haystack” search [18].Since there is no true consensus as to the precursor cell orentity, and only recently a transgenic mouse model [33],researchers are hampered by lack of models from whichto identify individual biomarker candidates.Application of advanced bioinformatics to genomic
or proteomic datastreams from patient materials has ledto progress in discerning gene and protein signatures
of ovarian cancer [10,25,34]. The serum proteome hasthe greatest potential to provide information from organ-confined early stage disease [10,35–37]. Serum suffusesthe tumor and the tumor microenvironment and may alsobe acted upon by the tumor microenvironment. Thus,changes in protein patterns in sera can reflect the statusof distant organs. Several groups have analyzed serumsamples using mass spectroscopy coupled with differentbioinformatics techniques. All have reported the abilityto identify some pattern or collection of proteins thathave predictive potential in the experimental setting. Ourgroup led the way using surface enhanced laser desorp-tion and ionization with a genetic cluster bioinformaticsalgorithm to show that there is a discriminative patternof mass spectroscopy features discerned from plasmasamples that can differentiate between unaffected womenand those with ovarian cancer. The algorithm was trainedusing serum samples from women with all stages ofovarian cancer. It was able to recognize all stage I cancersin a separate cohort of blinded multi-stage samples [10].This addresses the first goal, to develop a biomarkerthat can identify early stage disease. The findings havebeen extended using different selection chip matricesand a more sensitive tandem mass spectroscopy systemcapable of detecting several hundred thousand features inthe low molecular weight protein/peptide range (Conradset al, manuscript submitted). Data are reproduciblewith samples from different institutions and identifysignature patterns with several features that are identified

206 EC KOHN, GB MILLS, L LIOTTA
PP
P
P
P
P
P
P
Pcytoplasm
nucleus
P
PP
P
P
PP
P
P
Tumor biopsy
Microdissection
Array protein lysates
Bioinformatics analysis
Proteomic pathway profile
Tailored therapeutics recommendations
Fig. 3. Application of molecular signature for clinical decision making. Protein expression and signal pathway activation status can be monitoredin tumor tissue by minimally invasive biopsy acquisition followed by protein lysate array analysis. Bioinformatic integration of the array datacan yield a description of the molecular profile of the cancer driving logical targeted therapeutic combinations individualized to the expressedgenetic aberrations in the patient’s tumor.
reproducibly (Petricoin and Liotta, preliminary results).Work is underway to isolate the features in order to learnmore about the tumor and its local microenvironment.The field is now charged with demonstrating robust-
ness of the lead biomarker approaches. This includesdemonstration that the assay can be translated to the com-munity serum collection standards, that results transcendbias that may occur related to the time of day, meal, med-ication, or other patient variables, that it is applicable togenetically at-risk as well as sporadic risk cancer patients,and that it can be processed in a high throughput fashionat acceptable cost. The value of these assays as monitorsof cancer recurrence need to be evaluated in prospectiverandomized trials designed to ascertain sensitivity andspecificity impact on outcomes and quality of life.
BIOMARKERS REPRESENT HOST ANDTUMOR EVENTS
Investigation of the serum proteome or circulatingDNA or RNA moieties for biomarker determination is
logical. Aside from the ease of obtaining the patientmaterials, blood products have the highest likelihoodof representing changes going on in organ confineddisease. However, that does not guarantee that thesignature obtained is from the tumor cells themselves.It is more likely that any signature identified reflectsthe local microenvironment occurring during and afterepithelial cell transformation [38]. Changes in the stromaand the local stroma/hyperplasia interface can precedeneoplasia. This has been shown in prostate and ovariancancer, amongst others [39–41]. Thus, incorporation ofcohorts of women with preneoplastic lesions, CIN incervix cancer, UIN and atypical uterine hyperplasia forendometrial cancer, and benign lesions that may havesome relevance to ovarian cancer are important in anybiomarker development program.
TOOLS FOR MONITORING MOLECULARTHERAPEUTIC INTERVENTIONS
Early diagnosis is an imperative in ovarian cancer and

PROMISING DIRECTIONS FOR THE DIAGNOSIS AND MANAGEMENT OF GYNECOLOGICAL CANCERS 207
a mechanism to discriminate those early stage diseasepatients destined to have recurrent and fatal disease isneeded for all gynecologic cancers. In concert with thelatter is the need for surrogate markers of response.CA125 is helpful in monitoring patients for whom it hasbeen elevated [11,42]. However, CA125 may not increasewith serial tumor recurrences or its magnitude of changemay decrease such that it ceases to be a reliable marker.The increased use of molecularly targeted therapeuticsand the further dissection of the mechanisms of actionof cytostatic agents is providing new likely surrogateendpoint targets for response monitoring. Proteomictechnologies have been developed and/or adapted forsurrogate marker analysis, and if validated in prospectivetrials, may advance our predictive abilities. The conceptof proteomic pattern signatures for disease recurrenceprediction has been applied to clinical trial. It is not yetknown if a general signature pattern of recurrence canbe developed or if patterns validated for screening willserve a dual duty in recurrence detection.Evaluation of genomic, genetic, and proteomic disease-
or treatment-specific events can be tested in relationshipto treatment outcome. The finding that c-kit mutationpositive gastrointestinal stromal tumor patients are morelikely to have a response to STI-571 (Gleevec) therapyis an example of this approach [43,44]. This is beingtested for epidermal growth factor receptor inhibitorsin ovarian and other cancers. Currently, these eventsmust be evaluated in the tumor tissue directly. Sincethat requires an invasive procedure, it is important todevelop techniques to glean the most information fromthis limited clinical sample. We and others have createdprotein microarrays allowing micro-format analysis ofselected and specific proteins [7,45,46]. This approachis amenable to high throughput analysis and serialanalysis in a quantitative fashion. Further, it is amenableto microdissection to interrogate tumor and stromaseparately, if needed. Repetitive printing of the tumor cellor stromal cell lysate array maximizes internal controlsand potential to replicate results. Arrays are subjectedto immunostaining, much like immunohistochemistry,and then applied to a reader. Quantitative results aregleaned and can be analyzed against treatment outcomeor other clinical variables of interest [7]. A criticism ofthe technique, also a criticism of the tissue array, is thatonly a microcosm of the tumor is being sampled. A truerepresentation of the tumor may not be present if thereis marked heterogeneity.Many investigators have recognized that immediately
proximate signaling events, such as the presence of thetarget receptor or of its activated state, may not be the
best biomarkers for comparison of molecular surrogatemarker results to patient outcome. Downstream eventsregulated by the molecular target and other interactivepathways, converging on a final cell survival or invasionpathway, may be more reliable surrogates of response.For example, regulation of the activation status of Aktreproducibly correlates with patient response to therapyin a small subset of patients receiving Herceptin treat-ment (Liotta, preliminary results). Thus, the proteomictools under development have the potential to providehigh throughput focused molecular dissection of thecancer and its response to therapy. These approachesmay rapidly become commonly used, robust methods ofclinical patient assessment.
SUMMARY
The science of cancer biology, cancer detection, preven-tion and treatment has advanced at a lightening pace.New technology has been married to clinical practiceto identify and test new approaches to cancer detectionand for optimization of patient care. The excitementof these advances must, as always, be tempered bycautious review of the supporting data, appropriateness ofuse, and careful interpretation of results. Application ofgenomics, genetics, and proteomics to clinical diagnosis,prognostication, treatment, and triage is in our immediatefuture. Clinical trials of new tools need to be done withadequate design and power to allow us to adopt effectivenew technologies as quickly as feasible, while discardinginadequate alternatives. Recognition of the importance ofthe translational scientist in the clinical trials and clinicaltreatment venues is necessary. We cannot make importantadvances quickly or safely without developing teams forpatient recruitment, trial execution, careful data analysis,and dissemination of new tests. Use of these newtechnologies for early diagnosis of gynecologic cancers,identification of high risk or low risk patient subsetsfor triage to appropriate treatment, and new mechanismsfor reliable surrogate markers of response will advancemedical and surgical gynecologic oncology into the newcentury and provide the best clinical and scientific carefor our patients. This will permit attainment of the goalof individualized molecular medicine and with ensuringimprovement in outcome.
REFERENCES
[1] Ozols RF, Rubin SC, Thomas GM, Robboy SJ. Epithelial ovariancancer, p. 981−1058. Philadelphia: Lippincott Williams andWilkins, 2000.

208 EC KOHN, GB MILLS, L LIOTTA
[2] Barnholtz-Sloan JS, Schwartz AG, Qureshi F, Jacques S, Malone J,Munkarah AR. Ovarian Cancer: Changes in patterns at diagnosisand relative survival over the last three decades. American Journalof Obstetrics and Gynecology, 2003; in press.
[3] Etzioni R, Urban N, Ramsey S, McIntosh MW, Schwartz S, ReidB, et al. The case for early detection. Nature Reviews Cancer,2003;3:1−10.
[4] Singer G, Oldt R, Cohen Y, Wang BG, Sidransky D, Kurman RJ,et al. Mutations in BRAF and KRAS characterize the developmentof low-grade ovarian serous carcinoma. Journal of the NationalCancer Institute, 2003;95:484−486.
[5] Zorn KK, Awtrey CS, Gardner GJ, Barrett JC, Boyd J, Birrer JJ.Gene expression profiles of serous, endometrioid, and clear cellsubtypes of ovarian and endometrial cancer. Proceedings AACR,2003;44:1388A.
[6] Liotta LA, Kohn EC, Petricoin EF. Clinical proteomics:personalized molecular medicine. JAMA, 2001;286:2211−2214.
[7] Petricoin EF, Zoon KC, Kohn EC, Barrett JC, Liotta LA. Clinicalproteomics: translating benchside promise into bedside reality. NatRev Drug Discov, 2002;1:683−95.
[8] Schaid DJ, Buetow K, Weeks DE, Wijsman E, Guo SW, Ott J, et al.Discovery of cancer susceptibility genes: study designs, analyticapproaches, and trends in technology. J Natl Cancer Inst Monogr,1999;26:1−16.
[9] Strausberg RL, Greenhut S, Grouse LH, Schaefer CF, Buetow KH.In silico analysis of cancer through the Cancer Genome AnatomyProject. Trends Cell Biol, 2001;11:S66−71.
[10] Petricoin EF, Ardekani AM, Hitt BA, Levine PJ, Fusaro VA,Steinberg SM, et al. Use of proteomic patterns in serum to identifyovarian cancer. Lancet, 2002;359:572−7.
[11] Bast RC, Jr., Klug TL, St John E, Jenison E, Niloff JM, LazarusH, et al. A radioimmunoassay using a monoclonal antibody tomonitor the course of epithelial ovarian cancer. N Engl J Med,1983;309:883−7.
[12] Skates SJ, Xu FJ, Yu YH, Sjovall K, Einhorn N, Chang Y, et al.Toward an optimal algorithm for ovarian cancer screening withlongitudinal tumor markers. Cancer, 1995;76:2004−10.
[13] Jacobs IJ, Skates SJ, MacDonald N, Menon U, Rosenthal AN,Davies AP, et al. Screening for ovarian cancer: a pilot randomisedcontrolled trial. Lancet, 1999;353:1207−10.
[14] Zhang Z, Barnhill SD, Zhang H, Xu F, Yu Y, Jacobs I, et al.Combination of multiple serum markers using an artificial neuralnetwork to improve specificity in discriminating malignant frombenign pelvic masses. Gynecol Oncol, 1999;73:56−61.
[15] Crump C, McIntosh MW, Urban N, Anderson G, Karlan BY.Ovarian cancer tumor marker behavior in asymptomatic healthywomen: implications for screening. Cancer Epidemiol BiomarkersPrev, 2000;9:1107−1111.
[16] Chang HW, Lee SM, Goodman SN, Singer G, Cho SK, SokollLJ, et al. Assessment of plasma DNA levels, allelic imbalance,and CA 125 as diagnostic tests for cancer. J Natl Cancer Inst,2002;94:1697−1703.
[17] Bell R, Petticrew M, Sheldon T. The performance of screeningtests for ovarian cancer: results of a systematic review. Br J ObstGynaecol, 1998;105:1136−1147.
[18] Menon U, Jacobs IJ. Recent developments in ovarian cancerscreening. Curr Opin Obstet Gynecol, 2000;12:39−42.
[19] Skates SJ. Screening for ovarian cancer-risk, education, worry:path to appropriate use? Gynecol Oncol, 2002;85:1−2.
[20] Menon U, Talaat A, Rosenthal AN, Macdonald ND, Jeyerajah AR,Skates SJ, et al. Performance of ultrasound as a second line test to
serum CA125 in ovarian cancer screening. Br J Obst Gynaecol,2000;107:165−169.
[21] Cohen LS, Escobar PF, Scharm C, Glimco B, Fishman DA.Three-dimensional power Doppler ultrasound improves thediagnostic accuracy for ovarian cancer prediction. Gynecol Oncol,2001;82:40−8.
[22] Diamandis EP, Scorilas A, Fracchioli S, Van Gramberen M, DeBruijn H, Henrik A, et al. Human kallikrein 6 (hK6): a newpotential serum biomarker for diagnosis and prognosis of ovariancarcinoma. Journal of Clinical Oncology, 2003;21:1035−1043.
[23] Shayesteh L, Lu Y, Kuo WL, Baldocchi R, Godfery T, Collins C,et al. PIK3CA is implicated as an oncogene in ovarian cancer.Nature Gen, 1999;21:99−102.
[24] Kim JH, Skates SJ, Uede T, Wong, K-kKK, Schorge JO, FeltmateCM, et al. Osteopontin as a potential diagnostic biomarker forovarian cancer. JAMA, 2002;287:1671−1679.
[25] Jazaeri AA, Lu K, Schmandt R, Harris CP, Rao PH, Sotiriou C,et al. Molecular determinants of tumor differentiation in papillaryserous ovarian carcinoma. Mol Carcinog, 2003;36:53−59.
[26] Mok SC, Chao J, Skates S, Wong K, Yiu GK, Muto MG,et al. Prostasin, a potential serum marker for ovarian cancer:identification through microarray technology. J Natl Cancer Inst,2001;93:1458−1464.
[27] Brown Jones M, Blanchette JO, Kuznetsov VA, Raffeld M, SerreroG, Liotta LA, et al. The granulin-epithelin precursor is a growthfactor for epithelial ovarian cancer: Identification through cDNAlibrary analysis. Clin Can Res, 2003;9:44−51.
[28] Bayani J, Brenton JD, Macgregor PF, Beheshti B, Albert M,Nallainathan D, et al. Parallel analysis of sporadic primaryovarian carcinomas by spectral karyotyping, comparativegenomic hybridization, and expression microarrays. Cancer Res,2002;62:3466−3476.
[29] Jones MB, Krutzsch H, Shu H, Zhao Y, Liotta LA, Kohn EC,et al. Proteomic analysis and identification of new biomarkersand therapeutic targets for invasive ovarian cancer. Proteomics,2002;2:76−84.
[30] Welsh JB, Sapinoso LM, Kern SG, Brown DA, Liu T, BauskinAR, et al. Largescale delineation of secreted protein biomarkersoverexpressed in cancer tissue and serum. Proc Natl Acad SciUSA, 2003;100:3410−3415.
[31] Daly MB, Ozols RF. The search for predictive patterns inovarian cancer: proteomics meets bioinformatics. Cancer Cell,2002;1:111−2.
[32] Rai AJ, Zhang Z, Rosenzweig J, Shih I, Pham T, Fung ET, etal. Proteomic approaches to tumor marker discovery. Arch PatholLab Med, 2002;126:1518−1526.
[33] Connolly DC, Bao R, Nikitin AY, Stephens KC, Poole TW, Hua X,et al. Female mice chimeric for expression of the simian virus40 TAg under control of the MISIIR promoter develop epithelialovarian cancer. Cancer Res, 2003;63:1389−1397.
[34] Schwartz DR, Kardia SL, Shedden KA, Kuick R, MichailidisG, Taylor JM, et al. Gene expression in ovarian cancer reflectsboth morphology and biological behavior, distinguishing clearcell from other poor-prognosis ovarian carcinomas. Cancer Res,2002;62:4722−4729.
[35] Seliger B, Kellner R. Design of proteome-based studies incombination with serology for the identification of biomarkersand novel targets. Proteomics, 2002;2:1641−51.
[36] Li J, Zhang Z, Rosenzweig J, Wang YY, Chan DW. Proteomics andbioinformatics approaches for identification of serum biomarkersto detect breast cancer. Clin Chem, 2002;48:1296−1304.

PROMISING DIRECTIONS FOR THE DIAGNOSIS AND MANAGEMENT OF GYNECOLOGICAL CANCERS 209
[37] Anderson NL, Anderson NG. The human plasma proteome:history, character, and diagnostic prospects. Mol Cell Proteomics,2002;1:845−67.
[38] Liotta LA, Kohn EC. The microenvironment of the tumour-hostinterface. Nature, 2001;411:375−9.
[39] Li Y, Liu W, Hayward SW, Cunha G, Baskin LS.Plasticity of the urothelial phenotype: Effects of gastro-intestinal mesenchyme/stroma and implications for urinary tractreconstruction. Differentiation, 2000;66:126−135.
[40] Aboseif S, El-Sakka A, Young P, Cunha G. Mesenchymalreprogramming of adult human epithlelial differentiation.Differentiation, 1999;65:113−118.
[41] Gilead A, Neeman M. Dynamic remodeling of the vascularbed precedes tumor growth: MLS ovarian carcinoma spheroidsimplanted in nude mice. Neoplasia, 1999;1:226−230.
[42] Whitehouse C, Solomon E. Current status of the molecularcharacterization of the ovarian cancer antigen CA125 and
implications for its use in clinical screening. Gynecol Oncol,2003;88:S152−157.
[43] Heinrich MC, Blanke CD, Druker BJ, Corless CL. Inhibitionof KIT tyrosine kinase activity: a novel molecular approachto the treatment of KIT-positive malignancies. J Clin Oncol,2002;20:1692−1703.
[44] Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P,Demetri G. Management of malignant gastrointestinal stromaltumours. Lancet Oncol, 2002;3:655−664.
[45] MacBeath G, Schreiber SL. Printing proteins as microar-rays for high-throughput function determination. Science,2000;289:1760−1763.
[46] Paweletz CP, Charboneau L, Bichsel VE, Simone NL, Chen T,Gillespie JW, et al. Reverse phase protein microarrayswhich capture disease progression show activation of pro-survival pathways at the cancer invasion front. Oncogene,2001;20:1981−9.










![Epidemiology of Ovarian Cancer: Risk Factors and PreventionOvarian Cancer (OC) is a global health crisis and one of the deadly gynecological cancers among women worldwide [1]. Despite](https://img.dokumen.tips/doc/110x75/5e96ed02b573f005ce5939f4/epidemiology-of-ovarian-cancer-risk-factors-and-prevention-ovarian-cancer-oc.jpg)