Embed Size (px)
Citation preview

Prolonged Exposure and Virtual Reality–EnhancedImaginal Exposure for PTSD following a Terrorist
Bulldozer Attack: A Case Study
Sara A Freedman, Ph.D.,1 Hunter G. Hoffman, Ph.D.,2 Azucena Garcia-Palacios, Ph.D.,3
Patrice L (Tamar) Weiss, Ph.D.,4 Sara Avitzour, MSW,1 and Naomi Josman, Ph.D.4
Abstract
In this case study, virtual reality was used to augment imaginal exposure in a protocol based on prolongedexposure. A 29-year-old male patient developed posttraumatic stress disorder after surviving a deadly terroristbulldozer attack on two civilian buses and several cars in Jerusalem; the traumas witnessed by the survivorincluded a decapitation. The crowded bus in which the patient was riding was pushed over onto its side by theterrorist, injuring, trapping, and terrifying the passengers and causing gasoline to leak. Guided by his therapist,the patient entered an immersive computer-generated virtual world to go ‘‘back’’ to the scene of the traumaticevent to help him gain access to his memories of the event, process and reduce the intensity of the emotions(fear=anger) associated with his pathological memories, and change unhealthy thought patterns. Traumaticmemories of childhood abuse and traumatic memories of the bulldozer terrorist attack were treated usingimaginal exposure while the patient was in the virtual environment BusWorld. The patient showed largeposttreatment reductions in PTSD symptoms, and his Clinician-Administered PTSD Scale (CAPS) scoresdropped from 79 pretreatment to zero immediately posttreatment, and CAPS was still at zero 6 months later.Although case studies are inconclusive by nature, these encouraging preliminary results suggest that furtherexploration of the use of virtual reality during modified prolonged exposure for PTSD is warranted. As terroristattacks increase in frequency and severity worldwide, research is needed on how to minimize the psychologicalconsequences of terrorism.
Introduction
Asubset of people who experience a terrifying and po-tentially deadly physical or emotional incident develop
chronic psychological problems such as posttraumatic stressdisorder (PTSD). The incidence of developing PTSD followingdirect exposure to a terrorist attack is as high as 37.8%.1 Peoplewith PTSD commonly have persistent thoughts, memories, ornightmares about the traumatic event; have trouble sleeping;avoid thinking about the traumatic event; feel emotionallynumb; and show social avoidance. Other common symptomsinclude recurring flashbacks, irritability, anger, rage, and hy-pervigilance. PTSD sufferers often systematically avoid mem-ories and emotions associated with the traumatic event. Foaand Kozak2 theorize that avoidance perpetuates pathologicalmemories of traumatic events and interferes with recovery.
When used to treat PTSD, the core components of exposuretherapy include having participants repeatedly self-generate,visualize, and describe their recollection of the traumaticevent (imaginal exposure) and gradually exposing them re-peatedly to fear-evoking, real-world situations or objects thatremind them of their traumatic event (in vivo exposure).3
According to Foa and Kozak,2 the most effective exposuretherapy involves eliciting a fear response as patients ac-cess their memory of the traumatic event. During therapy,while their memory of the traumatic event is activated andthey are showing a fear response, patients process theiremotions associated with the traumatic memory (e.g., viahabituation). While their memory of the traumatic event isaccessed, information incompatible with some of the patho-logical elements of memory is introduced. For example, in-stead of the erroneous belief that avoiding any thoughts
1Department of Psychiatry, Hadassah University Hospital, Jerusalem, Israel.2HITLab, Mechanical Engineering, University of Washington, Seattle, Washington.3Department of Psychology, Jaume I University, Castellon, Spain.4Department of Occupational Therapy, University of Haifa, Mount Carmel, Haifa, Israel.
CYBERPSYCHOLOGY, BEHAVIOR, AND SOCIAL NETWORKING
Volume 13, Number 1, 2010ª Mary Ann Liebert, Inc.DOI: 10.1089=cyber.2009.0271
95

associated with the traumatic event is their best coping strat-egy, patients may realize during therapy that gradually ap-proaching and remembering the traumatic event will reducetheir suffering in the long run. During therapy, a healthiermemory is formed containing new elements. Patients developmore accurate metamemorial assumptions and retain fewerpathological beliefs. Exposure therapy is the most empiri-cally supported intervention for PTSD4 and has a high treat-ment success rate for patients who complete treatment.Unfortunately, most people who have PTSD never seektreatment, and most people with PTSD who seek treatmentnever receive cognitive behavior therapy (CBT) involvingexposure (e.g., prolonged exposure [PE]). Although large-scale efforts to increase dissemination are underway, CBTcombined with exposure is not widely used by clinicians in thecommunity who treat patients with PTSD.5 Several differentexposure therapy protocols for treating PTSD have been de-veloped and studied. In addition to the goal of improvingoutcome of completers, increasing patient and clinician ac-ceptance and reducing treatment dropouts are importantareas for future improvement.
People with PTSD fastidiously avoid thinking about theirtraumatic event. Getting them to imagine=self-generateimages of their traumatic experience during therapy can bedifficult.2 Patients often have exaggerated worries about whatis going to happen if they allow themselves to access theirtraumatic memory (e.g., they will go crazy or have a heartattack). For some patients, pathological memories may beunusually difficult to access using imaginal exposure, limit-ing emotional processing.2 According to Foa and Kozak,2
situations that enhance fear evocation and habitation duringtherapy are expected to improve treatment outcome.
Virtual reality (VR) computer-generated simulations oftraumatic events have been proposed as a means of facili-tating a patient’s ability to visualize and remember a fear-provoking traumatic event in a gradual, controlled fashion.6,8
Instead of patients having to use great effort to self-generateimages that help them gain access to their memories oftraumatic events, the computer generates the images forthem. Guided by their therapist, patients enter an immersivecomputer-generated virtual world that helps take them backto the scene of the traumatic event. With VR, patients expe-rience gradually more realistic depictions of the terrorist at-tack they witnessed=experienced, to help them gain access totheir memories of the event, process and reduce the intensityof the emotions (fear=anger=guilt) associated with their path-ological memories (e.g., via habituation), and change un-healthy thought patterns. Graded exposure helps patientsbecome more comfortable thinking about what happenedwith much less anxiety and less avoidant of remembering thetraumatic events.
VR therapy for PTSD was first used in a case series byRothbaum et al.7 to treat combat veterans. In the first studyusing VR to treat civilian PTSD, Difede and Hoffman6 de-veloped a virtual environment that involves a graded im-mersive simulation the September 11, 2001, attack at theWorld Trade Center in Manhattan. In the first controlledstudy on VR exposure therapy for PTSD,8 nine out of the 10VR exposure therapy patients showed a reduction in PTSDsymptoms, seven patients no longer had PTSD after VR ex-posure therapy, and five who had previously failed to im-prove with traditional therapy showed 25% to 50% or more
reductions in PTSD symptoms after completing therapy.8
These gains were maintained at 6-month follow-up. In con-trast, all waiting-list control patients still had clinical PTSD atthe end of the study. Further research on VR exposure ther-apy for PTSD is warranted by these encouraging preliminaryresults, and there are a growing number of patients needingtreatment for PTSD. For example, tens of thousands of U.S.soldiers are returning from Iraq and Afghanistan with PTSD.9
As terrorist attacks increase in frequency and severity world-wide, research is needed on how to minimize the psycho-logical consequences of terrorism.4
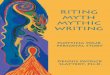
Palestinians and Israelis have both been victims of trau-matic events stemming from their violent conflict. Israelicivilians have been targeted in a number of Palestinian ter-rorist attacks. For example, in 2008, in downtown Jerusalem,a Palestinian construction worker driving a bulldozer at-tacked a woman and infant in a car, ramming the plow of hisbulldozer into the woman’s windshield, decapitating thefemale driver with his plow.10 He subsequently used hisbulldozer to lift two public transit buses loaded with civilianpassengers onto their sides, trapping the passengers inside(see Fig. 1), and went on to crush several more cars. Severalcivilians were killed, and their mutilated bodies had to beextricated from cars crushed by the bulldozer. In addition tothe fatalities, several people were injured in the attack. Anumber of survivors of that attack subsequently developedPTSD. The patient in the present case study was a passengeron one of the buses turned over in the attack. He was in gravepersonal danger and helped other passengers off the busbefore escaping himself.
This case report presents the first results of a treatmentbased on Foa’s PE protocol11 but using VR to augment theimaginal exposure components during treatment of PTSD ina civilian survivor of the 2008 bulldozer attack.
Method
Participant
At pretreatment assessment, the patient was a 29-year-oldmiddle-class married male Israeli citizen. He had recentlysurvived the July 2008 terrorist bulldozer attack in Jerusalemand entered treatment approximately 1 month after the at-tack. He is college educated, has been employed full timesince the traumatic event, and has had no prior treatment forPTSD. His ‘‘reexperiencing’’ symptoms included nightmaresand intrusive images of the terror attack as well as nightmaresand intrusive thoughts of previous traumas. His flashbacks ofthe bulldozer attack were very vivid, including smell. Heshowed significant physiological reactivity (fight-or-flightresponse) with these intrusions. His avoidances includedtrying not to think or talk about the event, avoiding travelingon buses, avoiding the place of the attack, and avoidingpeople of Arab descent. He reported significant sleep dis-turbance, anger outbursts, difficulty concentrating, and anexaggerated startle response. Pretreatment, the patient ful-filled criteria for PTSD related to the terrorist attack as well asa major depressive disorder. According to the pretreatmentassessment, carried out with the Structured Clinical Interviewfor DSM-IV (SCID) and Clinician-Administered PTSD Scale(CAPS), the patient’s PTSD symptoms and depression hadbegun subsequent to the attack and included suicidal idea-tion, although with no concrete plans to commit suicide.
96 FREEDMAN ET AL.

Although the patient showed no psychiatric diagnoses priorto the traumatic event, he did have pretrauma subclinicalobsessive compulsive disorder (OCD), which had consider-ably worsened since the attack and now fulfilled criteria forOCD at pretreatment assessment.
Apparatus
During the VR exposure sessions, the participant wore ahead-mounted display that included separate display screensfor each eye and stereo earphones. The participant was pre-sented with a computer-generated view of Virtual IsraelBusWorld environment.12 He was able to look around thevirtual world using a mouse. Our simulation of a terrorist busbombing attack allows graded exposure wherein a therapistis able to control the severity of the scenario by pressing twofunction keys and by simply asking the participant to visu-alize various subsets of the attack while in VR. In the presentstudy, the virtual environment depicted two increasingly
distressing levels of exposure. Level 1 shows the street scenefrom an urban Israeli sidewalk, near a cafe, across the streetfrom a bus stop. At level 2, a bus appears, approaches, andstops at the bus stop. Higher levels of BusWorld (levels 3through 12), depicting suicide bus bombings of graduallyincreasing levels of severity (see Josman et al.12 for details)were available to the therapist but not needed with thepresent patient.
BusWorld was designed by our team with input fromwww.firsthand.com. Firsthand.com created the BusWorldVR software for our team, incorporating sound effects gen-erously provided by Navy Commander Russell Shilling.BusWorld was originally designed to treat PTSD patientswho had witnessed a terrorist suicide bus bomb explosion.12
Procedure
All treatments and assessments occurred in the Depart-ment of Psychiatry, Hadassah University Hospital, Jerusalem,
FIG. 1. Bulldozer used in a terrorist attack on civilians in Jerusalem (A: photo by Gil Yochanan, ynetnews.com) and thepatient’s attacked bus (B: photo by Moti Boksin, Israelinationalnews.com, � Zaka Organization; both images used withpermission).
PE WITH VR FOR PTSD: BULLDOZER ATTACK IN ISRAEL 97

Israel, with Institutional Review Board approval. At Ha-dassah Hospital, all patients who seek medical treatment atthe emergency room following a large-scale terrorist attackare followed up afterwards by a psychologist. This patientreceived a telephone interview 4 days after the attack. Duringthe interview, he described high levels of PTSD and depres-sive symptoms. He was invited to attend a clinical assess-ment, which took place 1 month posttrauma. At thisassessment, standardized clinical interviews were carried out.The patient was asked to join the study, he signed informedconsent, and began treatment 6 weeks after the terrorist at-tack. The clinical assessments carried out pre- and posttreat-ment were conducted by an independent assessor, a trainedtherapist who was blind to what treatment the patient re-ceived (i.e., was not aware that the patient’s treatment in-volved VR). The patient was assessed using two standardizedclinical interviews: the Clinician-Administered PTSD Scale(CAPS)13 and the Structured Clinical Interview for DSM-IV(SCID-I).14 The interviews and questionnaires were repeatedat the end of treatment. In addition, the patient completedseveral self-report questionnaires. The Beck Depression In-ventory (BDI),15 Posttraumatic Symptoms Scale (PSI),15
Posttraumatic Cognitions Inventory (PTCI),17 and BriefSymptom Inventory (BSI)18 were filled out biweekly duringthe treatment.
Treatment
Because three of the imaginal exposure sessions took placewhile the participant was in VR, the treatment was not PE,which has a very strict definition. The treatment is based onPE,11 and treatment was carried out and supervised by ther-apists who have extensive knowledge and training in PE. Thetreatment was delivered during 10 individual sessions of 90minutes each conducted approximately once weekly over a12-week period. The initial session consisted of psychologicaleducation regarding PTSD symptoms as well as informa-tion regarding the VR system. The participant was taught abreathing exercise and asked to practice it as homework.During session 1, it became apparent that the trauma of theterrorist attack had resulted in reactivation of memories of
previous traumatic events. As a result, the patient’s intrusivememories and images were a mixture of all these events.According to Foa’s manualized PE protocol,19 for patientswith multiple trauma memories, the most distressing traumamemory should be treated first. For this patient, the mostdistressing memories were of childhood physical abuse hehad experienced from his father. So the therapist treated thepatient’s issues with childhood physical abuse first.
In the second session, a hierarchy for in vivo exposure wasestablished, the rationale for in vivo exposures was ex-plained, and the client and therapist together chose an ex-posure task that the client carried out for homework. Insessions 3, 4, and 5, the client carried out imaginal exposurewhile in virtual reality (i.e., imaginalþVR exposure). Therationale for imaginal exposure in VR was first explained tothe patient, and he put on the VR helmet. While in VR, thepatient was asked to tell the story of the event in first person,present tense. The therapist was able to see what the clientwas viewing in VR and was able to control the level of ex-posure. As therapy progressed, the sessions of VR withimaginal exposure addressed ‘‘hot spots’’ where the patientfocused on particularly difficult parts of his memory of thetraumatic event(s). For example, in session 3, he carried outthe imaginal exposure regarding his childhood physicalabuse while in VR BusWorld. The first level of VR BusWorldwas used. His eyes were open, and he was viewing BusWorldas he repeatedly described his childhood physical abuse to histherapist using imaginal exposure. He was fully engagedthroughout, initially reporting high ratings on the SubjectiveUnits of Distress Scale (SUDS). SUDS ratings gradually de-clined in a pattern indicating habituation. At the end of thesession, the patient reported relief and explained it was thefirst time he had ever told the story of the abuse. For home-work, he carried out further in vivo assignments and listenedto the associated audio recording of his therapy session. Atsession 4, the client reported that the previous session hadhelped. He was now no longer having intrusive memories ofhis childhood physical abuse. Imaginal exposure during VRwas now used to help him process his emotions associatedwith his pathological memories of the terrorist bulldozerattack. He was reluctant to begin, and his anxiety was very
FIG. 2. Screenshot of level 2 of BusWorld (a VR therapy software owned by the University of Washington, Seattle,www.vrpain.com).
98 FREEDMAN ET AL.

high (SUDS¼ 85). Once he did start, the anxiety went downsuddenly (SUDS¼ 50): the therapist felt he was disengagedand so increased BusWorld to level 2. This increased en-gagement and anxiety, and the SUDS rose to 70 and thengradually fell back to 50 in a pattern more typical of habitu-ation. Homework involved in vivo exposure by looking at areal bulldozer from a distance of 50 meters also includedlistening to the audio recording of his most recent imaginalwith VR exposure session (including what he told the thera-pist during the therapy session and what the therapist said).He was reporting high levels of anger and expressed concernthat he would act on his anger. As a result, session 5 includedCBT for anger management. In session 6, the client reportedthat listening to the audio recording of his therapy sessions(which had previously made him anxious before he habitu-ated) no longer resulted in any anxiety at all. At this point inhis recovery, most of his current anxiety was related to theincrease in OCD symptoms precipitated by the bulldozerterrorist attack. Since he had been experiencing some intru-sive memories from a third traumatic incident, from his timeas a soldier in the army, this was treated with imaginal ex-posure (without VR). In session 7, no imaginal exposure wascarried out, since he reported no more intrusive memories oranxiety. Instead, exposure was carried out by showing thepatient photographs of bus accidents, terror attacks, andterror attack victims. Extinction took place very quickly tothese images. Over the next three sessions, he continued ex-posures to bulldozer-related images, including videos. Dur-ing homework between sessions, he carried out real-lifein vivo exposures to bulldozers, including standing close to aworking bulldozer.
After the final VR with imaginal exposure session, thetherapist summarized all the progress the patient had madeduring the course of treatment and reviewed techniques hecould use after therapy was completed, (e.g., being less
avoidant of his memories of traumatic events, reducingavoidant behaviors in the real world, increasing naturallyencountered in vivo exposures). These techniques help pa-tients maintain the progress they have made and, ideally, tocontinue to reduce their PTSD symptoms over time post-treatment.
Results
The client’s SUDS ratings indicated both within-sessionand across-session habituation to anxiety at each level ofexposure. He showed no psychiatric diagnoses prior to thetraumatic event. After the attack, pretreatment, the patientfulfilled criteria for PTSD related to the terrorist attack as wellas a major depressive disorder. According to the pretreatmentassessment, carried out with the SCID and CAPS, the pa-tient’s PTSD symptoms and depression had begun subse-quent to the attack and included suicidal ideation, althoughwith no concrete plans to commit suicide. Although the pa-tient showed no psychiatric diagnoses prior to the traumaticevent, he did have subclinical OCD prior to the trauma,which had considerably worsened since the attack and nowfulfilled criteria for OCD at pretreatment assessment.
At the posttreatment assessment after his last session andat 6-month follow-up, the SCID, CAPS, and BDI showed thatthe client had fully recovered from PTSD, depression, andOCD. The self-report questionnaires also showed a significantreduction in symptom levels (see Tables 1A and 1B). Re-garding the value of his in vivo exposures, during the com-pletion of the CAPS at posttest, the patient said, ‘‘Every day Ipass by the place of the attack at least twice. I think of whathappened and continue on my way. This week, for the firsttime since the attack, I went on the same bus I took when theattack happened. I sat on the ‘unsafe’ side and said to myself‘I’m doing this and everything is all right.’ ’’ At 6-monthfollow-up, the client reported that the therapy had helpedhim in many areas of his life. He has returned to fullfunctioning and passes the site of the attack almost daily.
Discussion
In this case study, a PE-based program involving imaginalexposure augmented by VR was effective for the treatment ofPTSD. There was a large pretreatment to posttreatment re-duction of symptoms as evaluated by the CAPS, posttrau-matic stress symptoms, and Posttraumatic CognitionsInventory (PTCI; avoidance, reexperiencing, arousal, andcognitions). These gains held at 6-month follow-up. Therewas also a reduction in general psychopathology as mea-sured by the BSI and BDI. Although the level of depression
Table 1A. Pretreatment to Posttreatment
Assessment Scores
Measure Pretreatment Posttreatment
6 monthsposttreatment
follow-up
CAPS Total 79 0 0CAPS
Reexperiencing25 0 0
CAPS Avoidance 21 0 0CAPS Hyperarousal 33 0 0BDI 14 0 0BSI 100 4 15
Table 1B. Scores in Self-Report, Questionnaires at Pretreatment and Posttreatment,
at Sessions 2, 5, 10, and 12, and at 6 Months Posttreatment Follow-up
Measure Pretreatment Session 2 Session 5 Session 10 Session 12 Posttreatment 6 months posttreatment
BDI 14 12 12 2 2 0 0PSS 31 30 11 6PTCI 88 104 52 54
Note: The patient showed remission of PTSD symptoms after completing therapy.BDI, Beck Depression Inventory; PSS, posttraumatic stress symptoms; PTCI, Posttraumatic Cognition Inventory; BSI, Brief Symptom
Inventory.
PE WITH VR FOR PTSD: BULLDOZER ATTACK IN ISRAEL 99

at pretest measured by the BDI was not clinically significant,the SCID revealed a pretreatment diagnosis of major de-pression disorder. At the end of the treatment, as well as at6-month follow-up assessment, the client no longer met cri-teria for this disorder nor for another disorder identified atpretest, OCD. Although case studies are inconclusive bynature, the strong impression of the therapists was that VRaccelerated the effect of imaginal exposure, reducing the needto repeat sessions. In this case, two difficult traumatic events(childhood physical abuse and the bulldozer attack) neededan unusually small number of imaginal exposure sessionswhile in VR to result in a large decrease in the number ofintrusive thoughts and images and a large reduction in theimpact of PTSD symptoms on the patient.
Other VR therapy worlds for treating PTSD have made useof imaginal exposure while the patient was in a virtual world:WTC World,6,8 IraqWorld,20 Virtual Vietnam,7 and VirtualIraq.21 For example, in the real September 11 attacks on theWorld Trade Center, thousands of pedestrians were on thestreets of Lower Manhattan during a Monday morning rushhour. Yet in a VR exposure therapy software depiction of theattacks,6,8 there were no pedestrians, and no police cars, firetrucks, or ambulances were visible in the virtual world. WTCWorld left it up to users to fill in missing information withtheir own individual recollection=self-generated imagery. Inshort, VR was used to provide a context, and imaginal ex-posure was used by the patients while they were in VR.However, WTC World shows simulations of the terrorist at-tack in a sequence of increasingly realistic depictions. Level 1shows a blue sky before the attack, and no planes are visible.at level 2, a plane flies by but does not attack. at level 3, aplane hits WTC building but does not explode, and no soundeffects are heard. at level 4, a plane hits WTC building withanimated explosion but no sound effects. At level 5, a planehits WTC building with animated explosion and corre-sponding sound effects; the audio and visual effects becomeprogressively severe up to level 12.
Unlike the abovementioned clinical VR therapy worldsfor PTSD, in the present use, BusWorld did not show anyterrorist attack. No suicide bomber blew up the virtual bus,no bulldozers were visible in VR, no cars were crushed, nobus was lifted over onto its side, no sounds of metal bendingwere heard, no blood or broken glass was visible, no gasolineleaked onto the sidewalk, no people (avatars) were visible,and nobody screamed in BusWorld as used by this client.These details were all left up to the client to self-generate frommemory, using imaginal exposure based on his own idio-syncratic experience=eyewitness perspective of what hap-pened during the terrorist bulldozer attack. The approachused in the current study was a hybrid between previous usesof VR exposure (involving simulations of the terrorist attacks)and previous uses of conventional imaginal exposure withno VR.
VR with imaginal exposure combines the increased emo-tional engagement of VR with the high flexibility of imaginalexposure. For example, to our knowledge, the present studyis the first attempt to use imaginal exposure with VR for atraumatic event that is, to a casual observer, completely un-related to the content of the virtual world. The patient had theillusion of being in BusWorld as he repeatedly described hischildhood physical abuse to his therapist using imaginalexposure. BusWorld triggered not only his memories of the
bulldozer attack but also his memories of childhood abuse,which were associated with the his more recent memories forthe terrorist bulldozer attack on his bus. In this client’s case,being in BusWorld helped him access his memories of hischildhood abuse. The memories of the bus attack and thememories of childhood abuse may have been in the same‘‘fear structure’’ in memory (a mental program for escapingdanger2). We speculate that one reason patients with multipletraumas are so avoidant of the most recent trauma is becausethe recent trauma memory is a doorway to other painfulmemories from previous traumas.
In the current study, VR was used by the therapist to helpkeep the client emotionally engaged during therapy. Forexample, in one instance when the therapist felt the patienthad disengaged, the therapist increased the level of VR(i.e., had a public bus pull up to the Israeli bus stop), leadingto an increase in the patient’s emotional engagement. Mostpeople who experience a traumatic event show high PTSDsymptoms initially but show spontaneous symptom reduc-tion with no therapy and do not end up with chronic PTSD. Inone of the few studies on the topic, Rothbaum et al.22 showedthat starting 4 weeks after the traumatic event, PTSD patientsshowed little or no spontaneous improvement without ther-apy. Thus, it is unlikely that the patient’s progress in thecurrent case study is due to spontaneous improvement.
Other patients from the same bulldozer terrorist attack inJerusalem who developed PTSD were treated by the sametherapist as in the present study, using PE without VR. Thosereceiving PE with no VR also showed a significant reductionin symptoms. However, with conventional PE, the imaginalexposure took longer, with at least six imaginal exposuresessions. Whether VR improves outcomes or increases thespeed at which exposure takes effect, or whether patientsprogress just as far and quickly with Foa’s PE with no VR, areimportant topics for future research using randomized con-trolled trials. The contribution (if any) of VR to outcome is animportant research topic.
Difede et al.8 included five patients who had failed to re-spond to PE with no VR. All five of these patients subse-quently showed at least 25% to 50% or more reductions inPTSD symptoms after completing CBT with imaginal expo-sure augmented by immersive VR. Future research is neededon whether refractory patients who fail to respond to con-ventional therapy can still benefit from VR exposure therapy.
This report involves a case study, and the substantiallimitations of this methodology are well known.23 Althoughcase studies are a good vehicle for presenting innovativetechniques, evidence for effectiveness requires convergingresults from larger, more generalizable, carefully controlledstudies.
Although CBT involving exposure is the most empiricallysupported intervention for PTSD,4 most people who havePTSD never seek treatment, and most people with PTSD whoseek treatment never receive CBT involving exposure (e.g.,PE). Although large-scale efforts to increase dissemination areunder way, CBT with exposure is not widely used by clini-cians in the community who treat patients with PTSD.5 VRhas potential to increase the proportion of patient with PTSDwilling to seek treatment. Researchers speculate that VR (es-pecially VR with D-cycloserine fear extinction learning en-hancer20) may reduce the number of therapy sessions patientsneed to complete treatment. Surveys show that people with
100 FREEDMAN ET AL.

PTSD and other anxiety disorders report being unusuallyreceptive to seeking therapy that involves VR.24,25
The present results showed for the first time that a modi-fied PE protocol using VR to facilitate the imaginal exposurewas effective for treating PTSD stemming from a terroristattack in Israel. VR helped the patient remember and habit-uate to his memory of the traumatic event and helped himstop avoiding his memory. Although preliminary, these re-sults suggest that this topic is worthy of further research.
Disclosure Statement
No competing financial interests exist. An abstract de-scribing the attached results was presented at CyberTherapy14, Lake Maggiore Italy, June 2009. Clinical Trials numberNCT00474305.
References
1. Shalev AY, Freedman S. PTSD following terrorist attacks: aprospective evaluation. American Journal of Psychiatry 2005;162:1188–91.
2. Foa EB, Kozack MJ. Emotional processing of fear: exposure tocorrective information. Psychological Bulletin 1986; 99:20–35.
3. Nacasch N, Foa EB, Fostick L, et al. Prolonged exposuretherapy for chronic combat-related PTSD: a case report offive veterans. CNS Spectrums 2007; 12:690–5.
4. Foa EB, Cahill SP, Boscarino JA, et al. Social, psychological,and psychiatric interventions following terrorist attacks:recommendations for practice and research. Neuropsycho-pharmacology 2005; 30:1806–17.
5. Becker CB, Zayfert C, Anderson E. A survey of psycholo-gists’ attitudes towards and utilization of exposure therapyfor PTSD. Behavior Research & Therapy 2004; 42:277–92.
6. Difede J, Hoffman H. Virtual reality exposure therapy forWorld Trade Center posttraumatic stress disorder: a casereport. CyberPsychology & Behavior 2002; 5:529–35.
7. Rothbaum BO, Hodges L, Ready D, et al. Virtual realityexposure therapy for Vietnam veterans with posttraumaticstress disorder. Journal of Clinical Psychiatry 2001; 62:617–22.
8. Difede J, Cukor J, Jayasinghe N, et al. Virtual reality expo-sure therapy for the treatment of posttraumatic stress dis-order following September 11, 2001. Journal of ClinicalPsychiatry 2007; 68:1639–47.
9. Hoge CW, Castro CA, Messer SC, et al. Combat duty in Iraqand Afghanistan, mental health problems, and barriers tocare. New England Journal of Medicine 2004; 351:13–22.
10. Jerusalem bulldozer attack. http:==en.wikipedia.org=wiki=Jerusalem_bulldozer_attack (accessed Nov. 27, 2009).
11. Foa EB, Rothbaum BO. (1998) Treating the trauma of rape.New York Guilford.
12. Josman N, Reisberg A, Weiss PL, et al. BusWorld: an analogpilot test of a virtual environment designed to treat post-
traumatic stress disorder originating from a terrorist suicidebomb attack. CyberPsychology & Behavior 2008; 11:775–7.
13. Blake DD, Weather FW, Nagy LM, et al. (1998) Clinician-administered PTSD scale for DSM-IV. Boston: National Centerfor PTSD, Behavioral Science Division.
14. First MB, Spitzer RL, Gibbon M, et al. (1995) Structuredclinical interview for DSM-IV axis I disorders–research version.New York: New York State Psychiatric Institute.
15. Beck AT, Ward CH, Mendelson M, et al. An inventory formeasuring depression. Archives of General Psychiatry 1961;4:561–71.
16. Foa EB, Riggs DS, Dancu CV, et al. Reliability and validity ofa brief instrument for assessing post-traumatic stress disor-der. Journal of Traumatic Stress 1993; 6:459–73.
17. Foa EB, Ehlers A, Clark DM, et al. The PosttraumaticCognitions Inventory (PTCI): development and validation.Psychological Assessment 1999; 11:303–14.
18. Derogatis LR, Melisaratos N. The Brief Symptom Inventory:an introductory report. Psychological Medicine 1983; 13:595–605.
19. Foa EB, Hembree EA, Dancu CV. (2002). Prolonged exposure(PE) manual revised version. Philadelphia: University ofPennsylvania.
20. Gaylord K, Hoffman HG, Maiers A, et al. VR exposuretherapyþD-cycloserine (DCS) for treating PTSD in patientswith combat-related burn injuries. Frontiers in Neuro-engineering. Conference Abstract: Annual CyberTherapy &CyberPsychology 2009 conference. DOI: 10.3389=conf.neuro.14.2009.06.034.
21. Gerardi M, Rothbaum BO, Ressler K, et al. Virtual realityexposure therapy using a virtual Iraq: case report. Journal ofTraumatic Stress 2008; 21:209–13.
22. Rothbaum BO, Foa EB, Riggs DS, et al. A prospective ex-amination of post-traumatic stress disorder in rape victims.Journal of Traumatic Stress 1992; 5:455–75.
23. Campbell DT, Stanley JC. (1963) Experimental and quasi-experimental designs for research. Boston: Houghton Mifflin.
24. Garcia-Palacios A, Botella C, Hoffman H, et al. Comparingacceptance and refusal rates of virtual reality exposure vs.in vivo exposure by patients with specific phobias. Cyber-Psychology & Behavior 2007; 10:722–4.
25. Wilson JA, Onorati K, Mishkind M, et al. Soldier attitudesabout technology-based approaches to mental health care.CyberPsychology & Behavior 2008; 11:767–9.
Address correspondence to:Dr. Hunter G. Hoffman
HITLab, Mechanical EngineeringUniversity of Washington
Box 352142Seattle, WA 98195
E-mail: [email protected]
PE WITH VR FOR PTSD: BULLDOZER ATTACK IN ISRAEL 101