Embed Size (px)
Citation preview
Professional Practice Guidelines for Professional Practice Guidelines for the Use and Interpretation of SVTs: the Use and Interpretation of SVTs:
The Time Has ComeThe Time Has Come
Jerry SweetJerry SweetMay 20, 2011May 20, 2011
London, EnglandLondon, England

PreviewPreview•• Statements of Statements of the obviousthe obvious
–– Symptom validity testing is a mature area in terms Symptom validity testing is a mature area in terms of research and practiceof research and practice
–– SVTs are uniquely SVTs are uniquely ‘‘ownedowned’’ by psychologyby psychology
–– Within neuropsychology, SVT research literature is Within neuropsychology, SVT research literature is more well developed than most other more well developed than most other clinical clinical topicstopics
–– To the extent that To the extent that somesome view SVTs as view SVTs as ““controversialcontroversial””, it , it is merely a pseudois merely a pseudo--controversy for a very small minoritycontroversy for a very small minority
•• Review what clinicians Review what clinicians ‘‘shouldshould’’ be doing be doing
•• With regard to SVTs, neuropsychologists have all With regard to SVTs, neuropsychologists have all the guidance that is needed!the guidance that is needed!
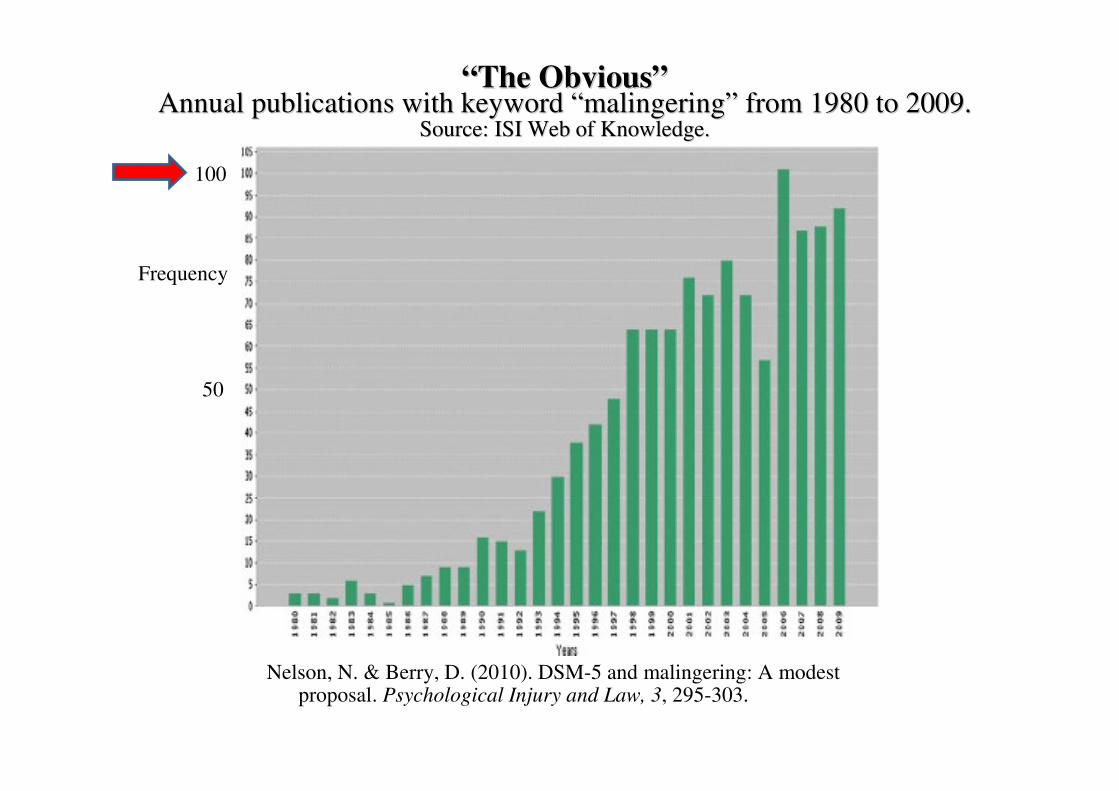
Nelson, N. & Berry, D. (2010). DSM-5 and malingering: A modestproposal. Psychological Injury and Law, 3, 295-303.
Frequency
100
50
jkl““The ObviousThe Obvious””
Annual publications with keyword Annual publications with keyword ““malingeringmalingering”” from 1980 to 2009. from 1980 to 2009. Source: ISI Web of Knowledge.Source: ISI Web of Knowledge.

““The ObviousThe Obvious””NeuropsychologyNeuropsychology’’ss Knowledge Base is Uniquely Well DevelopedKnowledge Base is Uniquely Well Developed
Medline searches of keywords in the title or keywords:Medline searches of keywords in the title or keywords:““MalingeringMalingering”” –– produced produced 2,341 results2,341 results (title or keyword)(title or keyword)
Of the 100 most recent journal articles in English: Of the 100 most recent journal articles in English:
–– 41 41 -- Neuropsychology journals Neuropsychology journals –– 28 28 -- Psychology journals Psychology journals –– 13 13 -- Medicine journalsMedicine journals–– 3 3 -- Neurology journalsNeurology journals–– 8 8 -- Psychiatry journalPsychiatry journal–– 5 5 -- Multidisciplinary journalMultidisciplinary journal–– 2 2 -- Other journal Other journal
–– 90 90 -- Articles by psychologists (1st author)Articles by psychologists (1st author)–– 4 4 -- Articles by psychiatrists (1Articles by psychiatrists (1stst author)author)–– 4 4 -- Articles by physicians (1Articles by physicians (1stst author)author)–– 2 2 -- Articles by other (1Articles by other (1stst author)author) Q
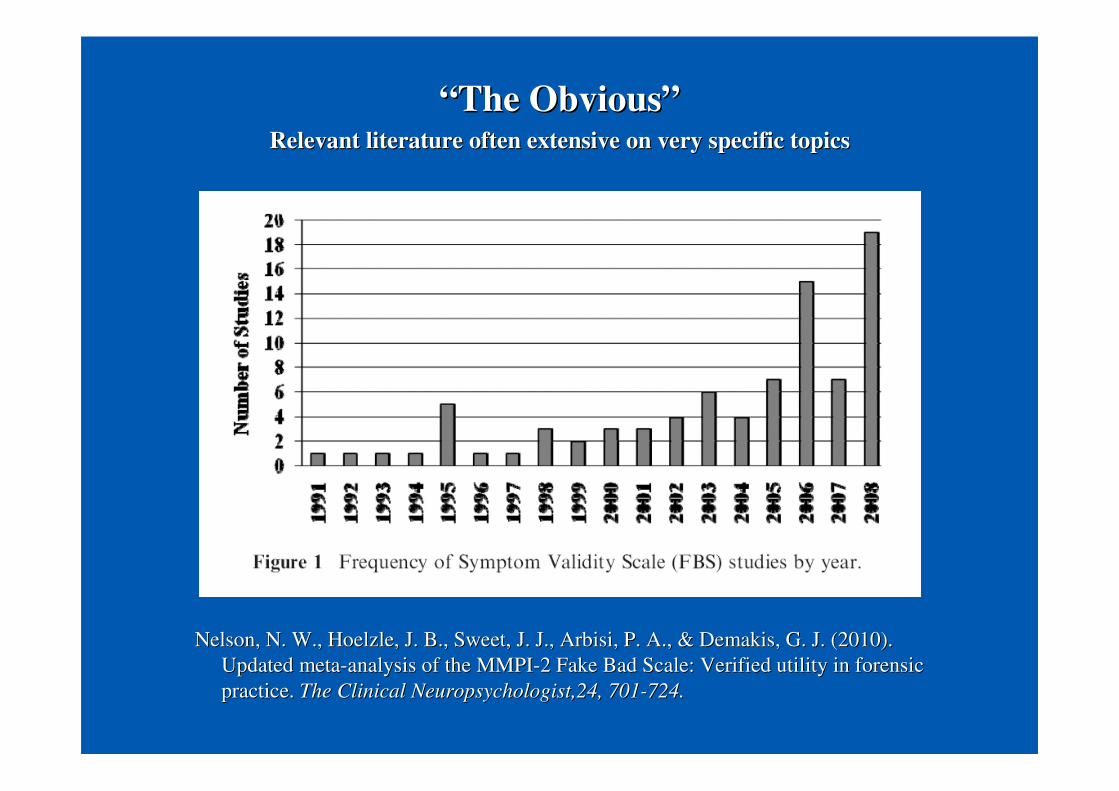
““The ObviousThe Obvious””Relevant literature often extensive on very specific topicsRelevant literature often extensive on very specific topics
Nelson, N. W., Hoelzle, J. B., Sweet, J. J., Arbisi, P. A., & DeNelson, N. W., Hoelzle, J. B., Sweet, J. J., Arbisi, P. A., & Demakis, G. J. (2010).makis, G. J. (2010).Updated metaUpdated meta--analysis of the MMPIanalysis of the MMPI--2 Fake Bad Scale: Verified utility in forensic2 Fake Bad Scale: Verified utility in forensicpractice. practice. The Clinical Neuropsychologist,24, 701The Clinical Neuropsychologist,24, 701--724. 724.
0
2
4
6
8
10
12
14
16
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Perc
enta
ges
of F
oren
sic
Top
ics
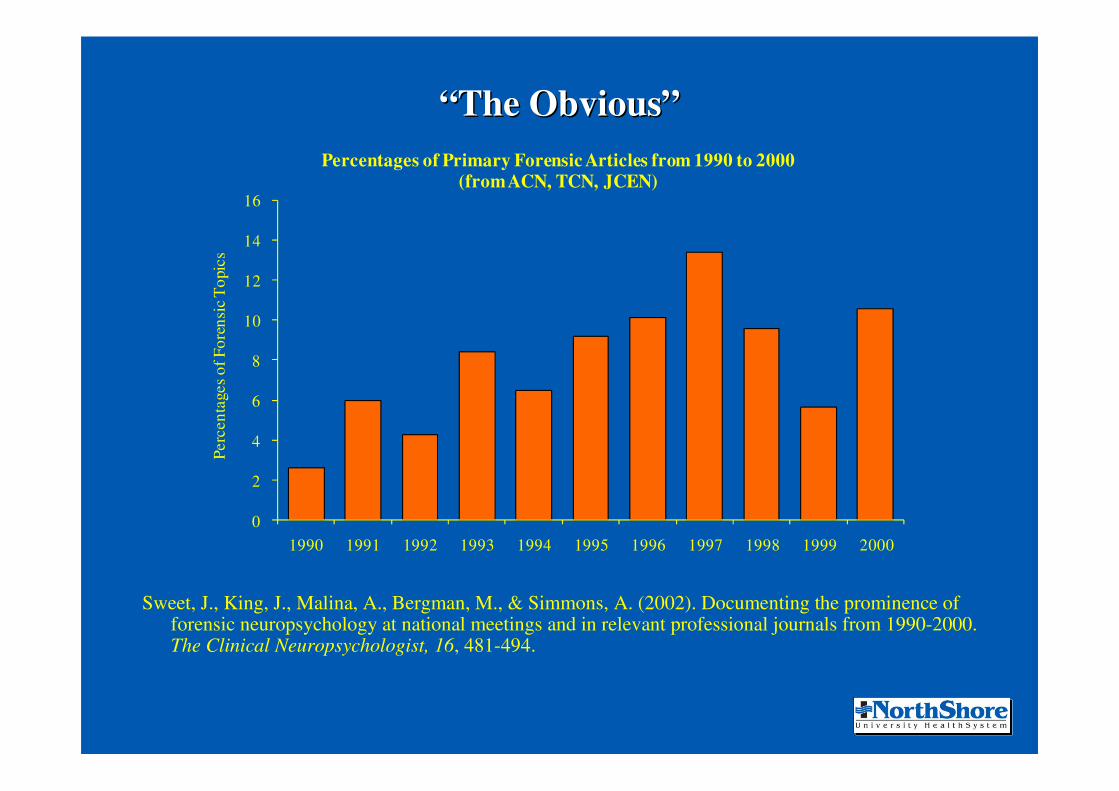
Percentages of Primary Forensic Articles from 1990 to 2000 (from ACN, TCN, JCEN)
““The ObviousThe Obvious””
Sweet, J., King, J., Malina, A., Bergman, M., & Simmons, A. (2002). Documenting the prominence of forensic neuropsychology at national meetings and in relevant professional journals from 1990-2000. The Clinical Neuropsychologist, 16, 481-494.

Frequency of Forensic Articles in TCN
0
2
4
6
8
10
12
14
16
18
20
22
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Freq
uenc
y
““The ObviousThe Obvious””
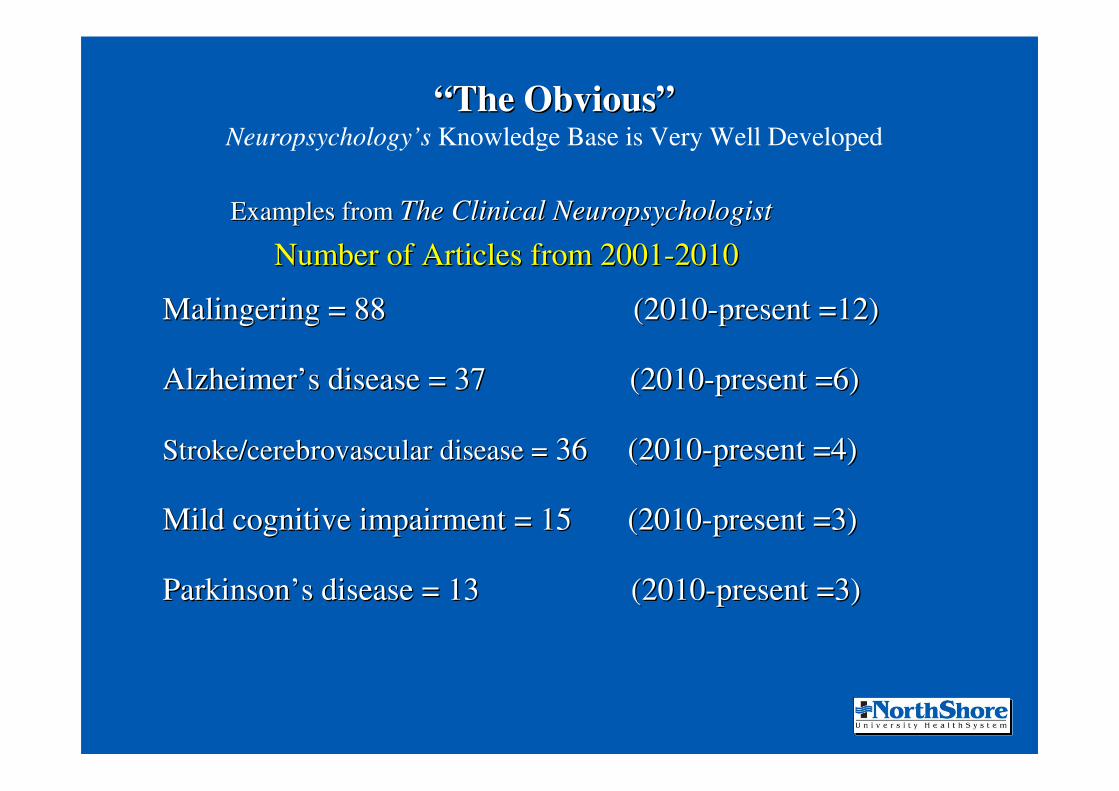
Examples from Examples from The Clinical NeuropsychologistThe Clinical Neuropsychologist
Number of Articles from 2001Number of Articles from 2001--20102010
Malingering = 88 (2010Malingering = 88 (2010--present =12)present =12)
AlzheimerAlzheimer’’s disease = 37 (2010s disease = 37 (2010--present =6)present =6)
Stroke/cerebrovascular disease =Stroke/cerebrovascular disease = 36 (201036 (2010--present =4)present =4)
Mild cognitive impairment = 15 (2010Mild cognitive impairment = 15 (2010--present =3)present =3)
ParkinsonParkinson’’s disease = 13 (2010s disease = 13 (2010--present =3)present =3)
““The ObviousThe Obvious””Neuropsychology’s Knowledge Base is Very Well Developed

Examples from Examples from Archives of Clinical NeuropsychologyArchives of Clinical Neuropsychology
Number of Articles from 2001Number of Articles from 2001--20102010
Malingering = 81 (2010Malingering = 81 (2010--present =12)present =12)
AlzheimerAlzheimer’’s disease = 58 (2010s disease = 58 (2010--present =10)present =10)
Stroke/cerebrovascular disease =Stroke/cerebrovascular disease = 29 (201029 (2010--present =2)present =2)
Mild cognitive impairment = 24 (2010Mild cognitive impairment = 24 (2010--present =7)present =7)
ParkinsonParkinson’’s disease = 17 (2010s disease = 17 (2010--present =2)present =2)
““The ObviousThe Obvious””Neuropsychology’s Knowledge Base is Very Well Developed
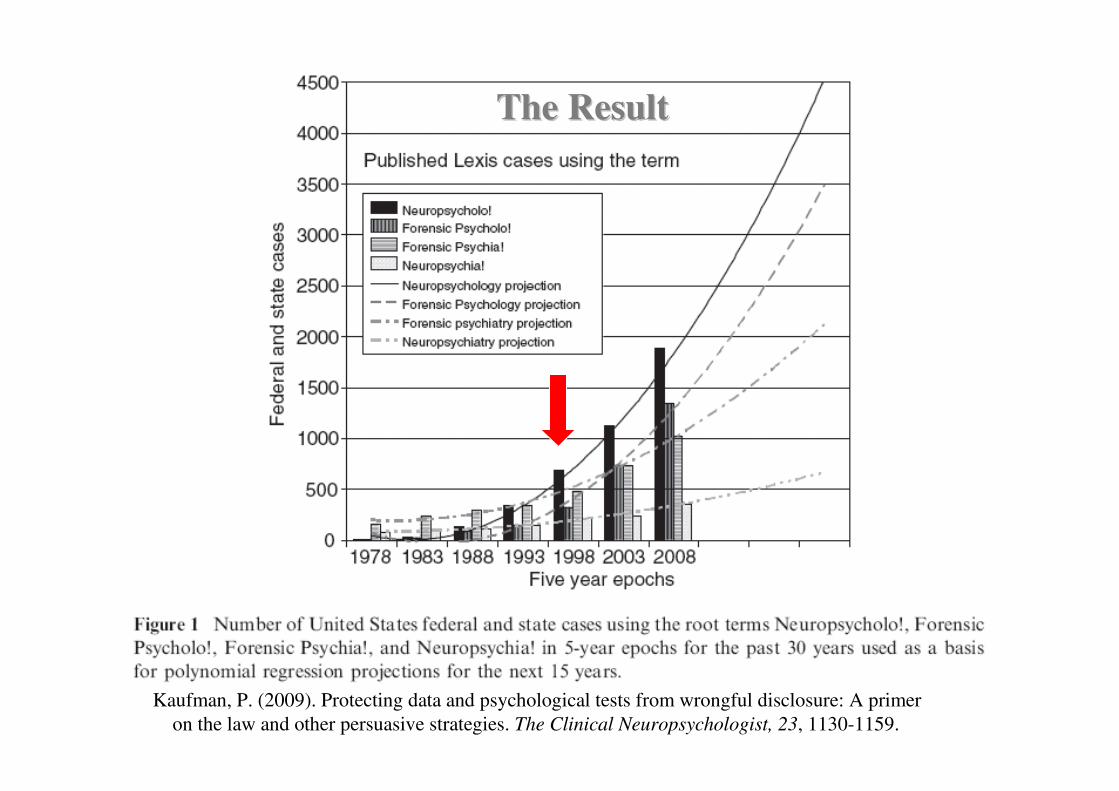
Kaufman, P. (2009). Protecting data and psychological tests from wrongful disclosure: A primeron the law and other persuasive strategies. The Clinical Neuropsychologist, 23, 1130-1159.
The ResultThe Result
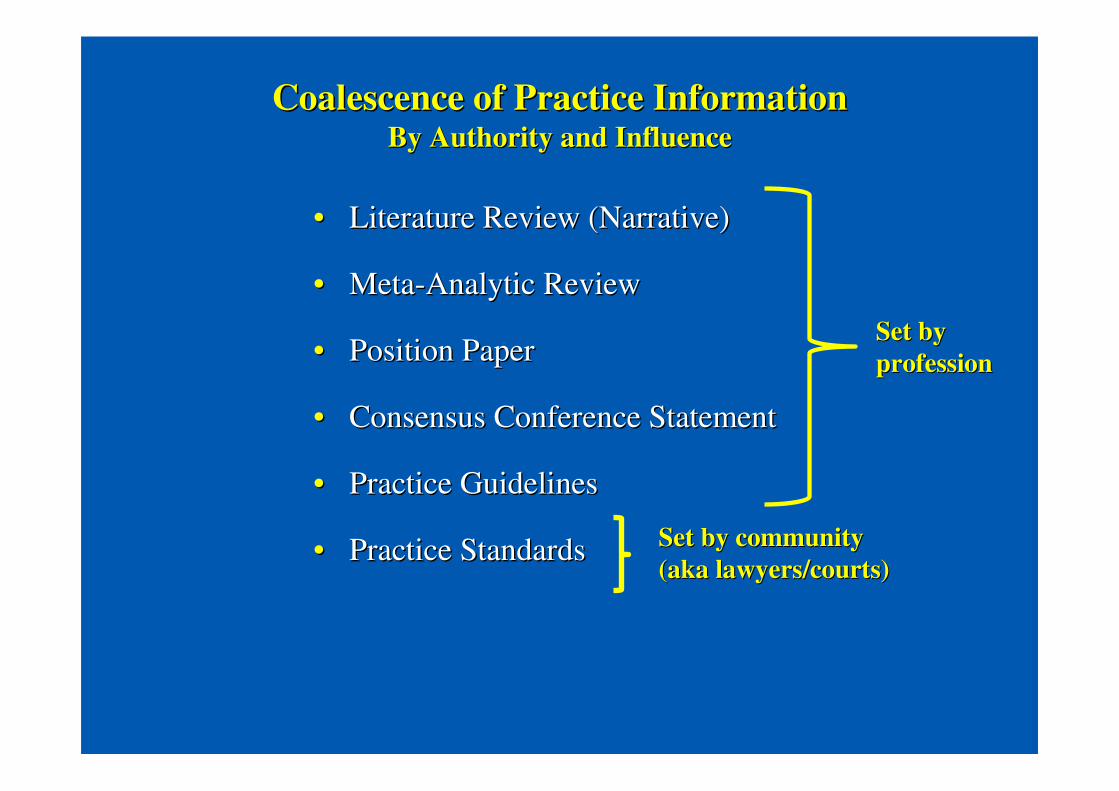
Coalescence of Practice InformationCoalescence of Practice InformationBy Authority and InfluenceBy Authority and Influence
•• Literature Review (Narrative)Literature Review (Narrative)
•• MetaMeta--Analytic ReviewAnalytic Review
•• Position PaperPosition Paper
•• Consensus Conference StatementConsensus Conference Statement
•• Practice GuidelinesPractice Guidelines
•• Practice StandardsPractice Standards
Set by Set by professionprofession
Set by communitySet by community(aka lawyers/courts)(aka lawyers/courts)

•• Moreso than most other topics Moreso than most other topics –– Limited to psych and neuropsych journals, run some Limited to psych and neuropsych journals, run some
searches with malingering or SVT or Effort versus other searches with malingering or SVT or Effort versus other common topics: total and in 2010common topics: total and in 2010
•• Unparalleled in Other DisciplinesUnparalleled in Other Disciplines–– Run searches in med journals looking for MD authors on Run searches in med journals looking for MD authors on
malingering or SVT or Effort versus in psych and malingering or SVT or Effort versus in psych and neuropsych journals with PhD authorsneuropsych journals with PhD authors
–– The comparison of difficulty finding presenters for a The comparison of difficulty finding presenters for a multidisciplinary panelmultidisciplinary panel
““The ObviousThe Obvious””The Knowledge Base is Very Well DevelopedThe Knowledge Base is Very Well Developed
Literature Reviews: SVTs and MalingeringLiterature Reviews: SVTs and MalingeringAronoff, G. Mandel, Genovese, E., Maitz, E., Dorto, A., Klimek, Aronoff, G. Mandel, Genovese, E., Maitz, E., Dorto, A., Klimek, E., & Staats, T. (2007). E., & Staats, T. (2007).
Evaluating malingering in contested injury or illness. Evaluating malingering in contested injury or illness. Pain Practice, 7,Pain Practice, 7, 178178--204. 204.
Bianchini, K.J., Mathias, C.W., & Greve, K.W. Bianchini, K.J., Mathias, C.W., & Greve, K.W. (2001). Symptom validity testing: A critical (2001). Symptom validity testing: A critical review. review. The Clinical Neuropsychologist, 15, The Clinical Neuropsychologist, 15, 1919--45.45.
Binder, L.M. & Rohling, M.L. (1996). Binder, L.M. & Rohling, M.L. (1996). Money matters: A metaMoney matters: A meta--analytic review of the effects analytic review of the effects of financial incentives on recovery after closedof financial incentives on recovery after closed--head injury. head injury. American Journal of American Journal of Psychiatry, 153Psychiatry, 153, 7, 7--10.10.
Etcoff, L.M., & Kampfer, K.M. (1996). Etcoff, L.M., & Kampfer, K.M. (1996). Practical guidelines in the use of symptom validity Practical guidelines in the use of symptom validity and other psychological tests to measure malingering and symptomand other psychological tests to measure malingering and symptom exaggeration in exaggeration in traumatic brain injury cases. traumatic brain injury cases. Psychology Review, 6Psychology Review, 6, 171, 171--201.201.
Guriel, J., & Fremouw (2003). Assessing malingered posttraumaticGuriel, J., & Fremouw (2003). Assessing malingered posttraumatic stress disorder: A critical stress disorder: A critical review. review. Clinical Psychology Review, 23Clinical Psychology Review, 23, 881, 881--904. 904.
Haines, M.E. & Norris, M.P. (1995). Detecting the malingering ofHaines, M.E. & Norris, M.P. (1995). Detecting the malingering of cognitive deficits: An cognitive deficits: An update. update. Neuropsychology Review, 5,Neuropsychology Review, 5, 125125--148.148.
Hall, R.C.W., & Hall, R.C.W. (2006). Malingering of PTSD: ForensHall, R.C.W., & Hall, R.C.W. (2006). Malingering of PTSD: Forensic and diagnostic ic and diagnostic considerations, characteristics of malingerers and clinical presconsiderations, characteristics of malingerers and clinical presentations. entations. General General Hospital Psychiatry, 28Hospital Psychiatry, 28, 525, 525--535.535.
Iverson, G.L. & Binder, L.M. Iverson, G.L. & Binder, L.M. (2000). Detecting exaggeration and malingering in (2000). Detecting exaggeration and malingering in neuropsychological assessment. neuropsychological assessment. Journal of Head Trauma Rehabilitation, 15,Journal of Head Trauma Rehabilitation, 15, 829829--858.858.
Lynch, W.J. (2004). Determination of effort level, exaggeration,Lynch, W.J. (2004). Determination of effort level, exaggeration, and malingering in and malingering in neurocognitive assessment. neurocognitive assessment. Journal of Head Trauma Rehabilitation, 19Journal of Head Trauma Rehabilitation, 19, 277, 277--283.283.

Literature Reviews: SVTs and Malingering (cont.)Literature Reviews: SVTs and Malingering (cont.)Miller, W., & Miller, E. Miller, W., & Miller, E. (1992). Malingering and neuropsychological assessment. (1992). Malingering and neuropsychological assessment. Physical Physical
Medicine and Rehabilitation, 6, Medicine and Rehabilitation, 6, 547547--563.563.
Nies, K., & Sweet, J. (1994). Neuropsychological assessment and Nies, K., & Sweet, J. (1994). Neuropsychological assessment and malingering: A critical review of malingering: A critical review of past and present strategies. past and present strategies. Archives of Clinical NeuropsychologyArchives of Clinical Neuropsychology, , 99, 501, 501--552.552.
Rohling, M. (2004, Summer/Fall). Who do they think they are kiddRohling, M. (2004, Summer/Fall). Who do they think they are kidding: A review of the use of ing: A review of the use of symptom validity tests with children. symptom validity tests with children. Newsletter 40 (Division of Clinical Neuropsychology), Newsletter 40 (Division of Clinical Neuropsychology), 2222, 1 & 21, 1 & 21--26. 26.
Rogers, R., Harrell, E., & Liff, C. (1993). Feigning neuropsychoRogers, R., Harrell, E., & Liff, C. (1993). Feigning neuropsychological impairment: A critical logical impairment: A critical review of methodological and clinical considerations. review of methodological and clinical considerations. Clinical Psychology Review, 13Clinical Psychology Review, 13, 255, 255--274.274.
Rogers, R., & Payne, J. (2006) Damages and rewards: Assessment oRogers, R., & Payne, J. (2006) Damages and rewards: Assessment of malingered disorders in f malingered disorders in compensation cases. compensation cases. Behavioral Sciences and the Law, 24Behavioral Sciences and the Law, 24, 1, 1––14. 14.
Sharland, M., & Gfeller, J. (2007). A survey of neuropsychologisSharland, M., & Gfeller, J. (2007). A survey of neuropsychologiststs’’ beliefs and practices with beliefs and practices with respect to the assessment of effort. respect to the assessment of effort. Archives of Clinical Neuropsychology, 22Archives of Clinical Neuropsychology, 22, 213, 213--224.224.
Slick, D., Sherman, E., & Iverson, G. (1999). Diagnostic criteriSlick, D., Sherman, E., & Iverson, G. (1999). Diagnostic criteria for malingered neurocognitive a for malingered neurocognitive dysfunction: Proposed standards for clinical practice and reseadysfunction: Proposed standards for clinical practice and research. rch. The Clinical The Clinical Neuropsychologist, 13, Neuropsychologist, 13, 545545--561.561.
Slick, D., Tan, J., Strauss, E., & Hultsch, D. (2004). DetectingSlick, D., Tan, J., Strauss, E., & Hultsch, D. (2004). Detecting malingering: A survey of expertsmalingering: A survey of experts’’practices. practices. Archives of Clinical Neuropsychology, 19Archives of Clinical Neuropsychology, 19, 465, 465--473.473.
Vanderploeg, R. & Curtiss, G. (2000). Vanderploeg, R. & Curtiss, G. (2000). Neuropsychological validity and malingering assessment: A Neuropsychological validity and malingering assessment: A critical review and discussion. critical review and discussion. Brain Injury Source,Brain Injury Source, 4,4, 1414--16 & 4316 & 43--45.45.

MetaMeta--Analytic Reviews: SVTs and MalingeringAnalytic Reviews: SVTs and MalingeringBaer, R. Wetter, M., & Berry, D. (1992). Detection of underreporBaer, R. Wetter, M., & Berry, D. (1992). Detection of underreporting of psychopathology on the ting of psychopathology on the
MMPI: A metaMMPI: A meta--analysis. analysis. Clinical Psychology Review, 12Clinical Psychology Review, 12, 509, 509--525. 525. Berry, D., Baer, R., & Harris, M. (1991). Detection of malingeBerry, D., Baer, R., & Harris, M. (1991). Detection of malingering on the MMPI: A metaring on the MMPI: A meta--analysis. analysis.
Clinical Psychology ReviewClinical Psychology Review, , 1111, 585, 585--598.598.Binder, L. & Rohling, M. (1996). Binder, L. & Rohling, M. (1996). Money matters: A metaMoney matters: A meta--analytic review of the effects of financial analytic review of the effects of financial
incentives on recovery after closedincentives on recovery after closed--head injury. head injury. American Journal of Psychiatry, 153American Journal of Psychiatry, 153, 7, 7--10.10.Green, D. & Rosenfeld, B. (2011). Evaluating the gold standard: Green, D. & Rosenfeld, B. (2011). Evaluating the gold standard: A review and metaA review and meta--analysis of the analysis of the
Structured Interview of Reported Symptoms.Structured Interview of Reported Symptoms. Psychological Assessment, 23,Psychological Assessment, 23, 9595--107. 107. Hawes, S. & Boccaccini, M. (2009). Detection of overreporting ofHawes, S. & Boccaccini, M. (2009). Detection of overreporting of psychopathology on the psychopathology on the
Personality Assessment Inventory: A metaPersonality Assessment Inventory: A meta--analytic review. analytic review. Psychological Assessment, 21Psychological Assessment, 21, 112, 112--124. 124.
Jasinski, L., Berry, D., Shandera, A., & Clark, J. (2011). Use oJasinski, L., Berry, D., Shandera, A., & Clark, J. (2011). Use of the Wechsler Adult Intelligence f the Wechsler Adult Intelligence Scale Digit Span subtest for malingering detection: A metaScale Digit Span subtest for malingering detection: A meta--analytic review.analytic review. Journal of Clinical Journal of Clinical and Experimental Neuropsychology, 33and Experimental Neuropsychology, 33, 300, 300--314. 314.
Nelson, N., Sweet, J., & Demakis, G. (2006). MetaNelson, N., Sweet, J., & Demakis, G. (2006). Meta--analysis of the MMPIanalysis of the MMPI--2 Fake Bad Scale: Utility 2 Fake Bad Scale: Utility in forensic practice. in forensic practice. The Clinical Neuropsychologist, 20The Clinical Neuropsychologist, 20, 39, 39--58.58.
Nelson, N., Hoelzle, J., Sweet, J., Arbisi, P., & Demakis, G. (2Nelson, N., Hoelzle, J., Sweet, J., Arbisi, P., & Demakis, G. (2010). Updated meta010). Updated meta--analysis of the analysis of the MMPIMMPI--2 Symptom Validity Scale (FBS): Verified utility in forensic pra2 Symptom Validity Scale (FBS): Verified utility in forensic practice.ctice. The Clinical The Clinical Neuropsychologist, 24Neuropsychologist, 24, 701, 701--724. 724.
Reznek, L. (2005). The Rey 15Reznek, L. (2005). The Rey 15--item memory test for malingering: A metaitem memory test for malingering: A meta--analysis. analysis. Brain Injury,19,Brain Injury,19,539539--543. 543.
Rogers, R., Sewell, K., Martin, M., & Vitacco, M. (2003). DetectRogers, R., Sewell, K., Martin, M., & Vitacco, M. (2003). Detection of feigned mental disorders: A ion of feigned mental disorders: A metameta--analysis of the MMPIanalysis of the MMPI--2 and malingering. 2 and malingering. AssessmentAssessment, , 1010, 160, 160--177.177.
Vickery, C., Berry, D., Inman, T., Harris, M., & Orey, S. (2001)Vickery, C., Berry, D., Inman, T., Harris, M., & Orey, S. (2001). Detection of inadequate effort on . Detection of inadequate effort on neuropsychological testing: A metaneuropsychological testing: A meta--analytic review of selected procedures. analytic review of selected procedures. Archives of Clinical Archives of Clinical NeuropsychologyNeuropsychology, , 16,16, 4545--73.73.
Book Chapter Reviews: SVTs and MalingeringBook Chapter Reviews: SVTs and MalingeringBinder, L. (1992). Deception and malingering. In A. Puente & R. Binder, L. (1992). Deception and malingering. In A. Puente & R. McCaffrey (Eds.) McCaffrey (Eds.)
Handbook of neuropsychological assessment: A biopsychosocial perHandbook of neuropsychological assessment: A biopsychosocial perspective. New York: spective. New York: Plenum.Plenum.
Hayes, J., Hilsabeck, R., & Gouvier, W.D. (1999). Malingering tHayes, J., Hilsabeck, R., & Gouvier, W.D. (1999). Malingering traumatic brain injury: raumatic brain injury: Current issues and caveats in assessment and classification. InCurrent issues and caveats in assessment and classification. In N. Varney & R. Roberts, N. Varney & R. Roberts, (Eds.) (Eds.) The evaluation and treatment of mild traumatic brain injury.The evaluation and treatment of mild traumatic brain injury. Mahwah, NJ: Mahwah, NJ: Lawrence Erlbaum.Lawrence Erlbaum.
Larrabee, G. (2005). Assessment of malingering. In G. Larrabee (Larrabee, G. (2005). Assessment of malingering. In G. Larrabee (Ed.), Ed.), Forensic Forensic neuropsychology: A scientific approachneuropsychology: A scientific approach (pp. 115(pp. 115--158). New York: Oxford University 158). New York: Oxford University Press. Press.
Larrabee, G., Greiffenstein, M., Greve, K., & Bianchini, K. (200Larrabee, G., Greiffenstein, M., Greve, K., & Bianchini, K. (2007). Refining diagnostic 7). Refining diagnostic criteria for malingering. In G. Larrabee (Ed.), criteria for malingering. In G. Larrabee (Ed.), Assessment of malingered Assessment of malingered neuropsychological deficitsneuropsychological deficits (pp. 334(pp. 334--371). New York: Oxford University Press.371). New York: Oxford University Press.
Millis, S. (2004). Evaluation of malingered neurocognitive disorMillis, S. (2004). Evaluation of malingered neurocognitive disorders. In M. Rizzo & P. ders. In M. Rizzo & P. Esslinger (Eds.), Esslinger (Eds.), Principles and practice of behavioral neurology and neuropsycholPrinciples and practice of behavioral neurology and neuropsychologyogy(pp. 1077(pp. 1077--1089). Philadelphia: W. B. Saunders.1089). Philadelphia: W. B. Saunders.
Millis, S. & Putnam, S. (1996). Detection of malingering in posMillis, S. & Putnam, S. (1996). Detection of malingering in postconcussive syndrome. M. tconcussive syndrome. M. Rizzo & D. Tranel (Eds.),Rizzo & D. Tranel (Eds.), Head Injury and Postconcussive Syndrome Head Injury and Postconcussive Syndrome (pp. 481(pp. 481--498). New 498). New York: Churchill Livingstone.York: Churchill Livingstone.
Sweet, J. (1999). Malingering: Differential diagnosis. In J. SweSweet, J. (1999). Malingering: Differential diagnosis. In J. Sweet (Ed.) et (Ed.) Forensic Forensic neuropsychology: Fundamentals and practiceneuropsychology: Fundamentals and practice. New York: Psychology Press.. New York: Psychology Press.

Books on SVTs and MalingeringBooks on SVTs and Malingering
Boone, K.B. (2007). Boone, K.B. (2007). Assessment of feigned cognitive impairment: A Assessment of feigned cognitive impairment: A Neuropsychological Perspective. Neuropsychological Perspective. New York: Guilford.New York: Guilford.
Larrabee, G.J. (Ed.) (2007). Larrabee, G.J. (Ed.) (2007). Assessment of malingered neuropsychological deficits. Assessment of malingered neuropsychological deficits. New York: Oxford University Press.New York: Oxford University Press.
McCann, J.T. (1998). McCann, J.T. (1998). Malingering and deception in adolescents: Assessing Malingering and deception in adolescents: Assessing credibility in clinical and forensic settings. credibility in clinical and forensic settings. American Psychological Association.American Psychological Association.
Morgan, J.E. and Sweet, J.J. (2009). Morgan, J.E. and Sweet, J.J. (2009). Neuropsychology of malingering casebook. Neuropsychology of malingering casebook. New York: Psychology Press.New York: Psychology Press.
Reynolds, C.R. (Ed.) (1998). Reynolds, C.R. (Ed.) (1998). Detection of malingering during head injury litigationDetection of malingering during head injury litigation. . New York: Plenum Press.New York: Plenum Press.
Rogers, R. (Ed.) (2008). Rogers, R. (Ed.) (2008). Clinical assessment of malingering and deception (3rd Clinical assessment of malingering and deception (3rd Edition).Edition). New York: Guilford.New York: Guilford.

Books on SVTs and MalingeringBooks on SVTs and Malingering
**Boone, K.B. (2007). Boone, K.B. (2007). Assessment of feigned cognitive impairment: A Assessment of feigned cognitive impairment: A Neuropsychological Perspective. Neuropsychological Perspective. New York: Guilford.New York: Guilford.
**Larrabee, G.J. (Ed.) (2007). Larrabee, G.J. (Ed.) (2007). Assessment of malingered neuropsychological deficits. Assessment of malingered neuropsychological deficits. New York: Oxford University Press.New York: Oxford University Press.
McCann, J.T. (1998). McCann, J.T. (1998). Malingering and deception in adolescents: Assessing Malingering and deception in adolescents: Assessing credibility in clinical and forensic settings. credibility in clinical and forensic settings. American Psychological Association.American Psychological Association.
**Morgan, J.E. and Sweet, J.J. (2009). Morgan, J.E. and Sweet, J.J. (2009). Neuropsychology of malingering casebook. Neuropsychology of malingering casebook. New York: Psychology Press.New York: Psychology Press.
**Reynolds, C.R. (Ed.) (1998). Reynolds, C.R. (Ed.) (1998). Detection of malingering during head injury Detection of malingering during head injury litigationlitigation. New York: Plenum Press.. New York: Plenum Press.
Rogers, R. (Ed.) (2008). Rogers, R. (Ed.) (2008). Clinical assessment of malingering and deception (3rd Clinical assessment of malingering and deception (3rd Edition).Edition). New York: Guilford.New York: Guilford.
Position PapersPosition Papers
Useful general document, but no guidance on assessing response bUseful general document, but no guidance on assessing response biasias
Position PapersPosition Papers
““In summary, the assessment of symptom validity is an essential pIn summary, the assessment of symptom validity is an essential part of a art of a neuropsychological evaluation. The clinician should be prepared neuropsychological evaluation. The clinician should be prepared to justify a to justify a decision not to assess symptom validity as part of a neuropsychodecision not to assess symptom validity as part of a neuropsychological logical evaluationevaluation…”…”……The following are common methods for assessing symptom validity The following are common methods for assessing symptom validity (Larrabee, 2003; Reynolds, 1998; Slick, Sherman, & Iverson, 1999(Larrabee, 2003; Reynolds, 1998; Slick, Sherman, & Iverson, 1999; Sweet, ; Sweet, 1999).1999).
3.1. 3.1. ConsistencyConsistency (interviews, observations, tests)(interviews, observations, tests)
3.2. 3.2. Performance on neurocognitive tests Performance on neurocognitive tests (invalidity, inconsistencies (invalidity, inconsistencies
with known brain function, observed behavior, reliable collaterawith known brain function, observed behavior, reliable collaterals, ls,
documented background)documented background)
3.3. 3.3. Performance on psychological testsPerformance on psychological tests
3.4. 3.4. Symptom validity tests Symptom validity tests
3.5. Forced3.5. Forced--choice testschoice tests
Position PapersPosition PapersNAN Position Paper on Symptom Validity AssessmentNAN Position Paper on Symptom Validity Assessment

5.1. Procedures5.1. Procedures(a) Remain abreast of trends in the symptom validity assessment (a) Remain abreast of trends in the symptom validity assessment literature.literature.
(b) Approach the assessment of symptom validity proactively.(b) Approach the assessment of symptom validity proactively.
(c) Assess whether cognitive, psychiatric, and/or behavioral sym(c) Assess whether cognitive, psychiatric, and/or behavioral symptoms are ptoms are embellished.embellished.
(d) Use a multi(d) Use a multi--method approach. A distinction is made between a multimethod approach. A distinction is made between a multi--method method approach and a multiapproach and a multi--test approach. Whereas the administration of multiple test approach. Whereas the administration of multiple tests may or may not contribute incrementally to the validity oftests may or may not contribute incrementally to the validity of the clinical the clinical determination, the use of multiple methods that extend beyond tedetermination, the use of multiple methods that extend beyond testing is likely sting is likely to contribute to such validity.to contribute to such validity.
(e) Inform the examinee at the outset of the evaluation and as n(e) Inform the examinee at the outset of the evaluation and as needed during the eeded during the evaluation that good effort and honesty will be required (the exevaluation that good effort and honesty will be required (the examiner may aminer may inform the examinee that such factors will be directly assessed)inform the examinee that such factors will be directly assessed)..
(f) Use SVTs with the most appropriate psychometric properties, (f) Use SVTs with the most appropriate psychometric properties, given the given the characteristics of the examinee and setting.characteristics of the examinee and setting.
(g) Disperse SVTs or measures with symptom validity indicators t(g) Disperse SVTs or measures with symptom validity indicators throughout the hroughout the evaluation, with administration of at least one SVT early in theevaluation, with administration of at least one SVT early in the evaluation evaluation process.process.
(h) Report the results of symptom validity assessment.(h) Report the results of symptom validity assessment.
Position PapersPosition PapersNAN Position Paper on Symptom Validity AssessmentNAN Position Paper on Symptom Validity Assessment
Consensus StatementConsensus Statement

American Academy of Clinical Neuropsychology American Academy of Clinical Neuropsychology Consensus ConferenceConsensus Conference
Neuropsychological Assessment of Effort, Neuropsychological Assessment of Effort, Response Bias, and MalingeringResponse Bias, and Malingering
Boston, June 2008Boston, June 2008

What is a consensus conference?What is a consensus conference?
•• A meeting of individuals with a high level of A meeting of individuals with a high level of expertise on a subject, who strive to identify areas expertise on a subject, who strive to identify areas of agreement that can be made public for the of agreement that can be made public for the purpose of guiding others within the profession.purpose of guiding others within the profession.
•• Not common in psychology or neuropsychology, Not common in psychology or neuropsychology, but common among medical specialties and but common among medical specialties and interdisciplinary groups that share common interdisciplinary groups that share common interests that are deemed interests that are deemed ““importantimportant””, especially , especially when controversial topics need resolution. when controversial topics need resolution.

What is a consensus conference statement?What is a consensus conference statement?
As a product of recognized experts, it is:As a product of recognized experts, it is:
a.a. DifferentDifferent from a narrative from a narrative literatureliterature reviewreview, though perhaps , though perhaps relying on relevant published reviews of the literature,relying on relevant published reviews of the literature,
b.b. DifferentDifferent from a from a metameta--analysisanalysis of prior published studies, of prior published studies, though perhaps relying on relevant metathough perhaps relying on relevant meta--analytic (or analytic (or quantitative) reviews,quantitative) reviews,
c.c. DifferentDifferent from a typical from a typical position statementposition statement by an by an organization, which is often on a very specific point that organization, which is often on a very specific point that may or may not be informed by scientific investigation may or may not be informed by scientific investigation (e.g., ethics complaints during forensic proceedings, (e.g., ethics complaints during forensic proceedings, neuropsychologists are allowed to use testing assistants) neuropsychologists are allowed to use testing assistants) and is created by a smaller group, such as a standing and is created by a smaller group, such as a standing committee.committee.
What is a consensus conference statement?What is a consensus conference statement?
d.d. DifferentDifferent from from practice standardspractice standards, which , which ““are are mandatory and may be accompanied by an enforcement mandatory and may be accompanied by an enforcement mechanism.mechanism.”” (APA, 2005 from (APA, 2005 from Determination and Documentation Determination and Documentation of the Need for Practice Guidelinesof the Need for Practice Guidelines) )
e.e. Practice guidelinesPractice guidelines and consensus conferenceand consensus conferencestatements statements shareshare: : �� making suggestions or recommendations of making suggestions or recommendations of ““specific specific
professional behavior, endeavor, or conductprofessional behavior, endeavor, or conduct”” (APA. 2005)(APA. 2005)
�� being aspirational, not mandatorybeing aspirational, not mandatory
�� goal of assisting practitioners to deliver high quality servicesgoal of assisting practitioners to deliver high quality services
�� not viewed as a means of identifying a group or specialty area not viewed as a means of identifying a group or specialty area and not excluding practitioners from practicing in a particular and not excluding practitioners from practicing in a particular areaarea

Research Evidenceand
Scientific Issues
Consensus ConferenceNeuropsychological Assessment
of Effort, Response Bias, and Malingering
Definitions and
Differential Diagnosis
AbilityIssues
PsychologicalIssues
A Single Integrated Consensus Statement
SomaticIssues
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering
•• Definitional and Conceptual IssuesDefinitional and Conceptual Issues–– The term The term secondary gain secondary gain is not synonymous with malingering and is not synonymous with malingering and
is best limited a description of the context of evaluationis best limited a description of the context of evaluation
–– The term malingering is descriptive; though considered a The term malingering is descriptive; though considered a diagnosis, it does not identify a clinical disorderdiagnosis, it does not identify a clinical disorder
–– Failure on effort measures is not synonymous with malingeringFailure on effort measures is not synonymous with malingering
•• Ability IssuesAbility Issues–– Evidence indicates clinicians Evidence indicates clinicians cancan diagnose malingeringdiagnose malingering
–– Published diagnostic approaches (e.g., Slick criteria) are bettePublished diagnostic approaches (e.g., Slick criteria) are better r than APA DSMthan APA DSM--IVIV--TR diagnostic criteria for malingeringTR diagnostic criteria for malingering
–– Invalid presentations are: (1) not fully explained by brain Invalid presentations are: (1) not fully explained by brain dysfunction, (2) not reasonably attributable to moderator (e.g.,dysfunction, (2) not reasonably attributable to moderator (e.g.,education) or confounding variables (e.g., fatigue), and education) or confounding variables (e.g., fatigue), and significantly worse than or different in degree or pattern from significantly worse than or different in degree or pattern from performance standards known to reflect genuine disorderperformance standards known to reflect genuine disorder

•• Ability Issues (continued)Ability Issues (continued)
–– In general, neuropsychologists routinely encourage optimal efforIn general, neuropsychologists routinely encourage optimal effort. t. –– Use of psychometric indicators is the most valid approach to Use of psychometric indicators is the most valid approach to
identifying neuropsychological response validity.identifying neuropsychological response validity.–– StandStand--alone & embedded validity indicators should both be usedalone & embedded validity indicators should both be used–– SelfSelf--reported symptoms are best evaluated with instruments that reported symptoms are best evaluated with instruments that
contain proven validity measures. When these indicate invalid contain proven validity measures. When these indicate invalid responding, instruments without validity measures should not be responding, instruments without validity measures should not be interpreted.interpreted.
–– When in a clinical evaluation, clinicians should be mindful of tWhen in a clinical evaluation, clinicians should be mindful of the he possibility of future litigation and act accordingly.possibility of future litigation and act accordingly.
–– Substantial discrepancy between test results and known disorder Substantial discrepancy between test results and known disorder effects should raise concern regarding insufficient effort, respeffects should raise concern regarding insufficient effort, response onse bias, and malingering.bias, and malingering.
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering
•• Ability Issues (continued)Ability Issues (continued)
–– As the number and extent of findings indicate presence or As the number and extent of findings indicate presence or absence of response bias increase, confidence regarding validityabsence of response bias increase, confidence regarding validityconclusions is strengthened.conclusions is strengthened.
–– When a psychological disorder When a psychological disorder andand ability deficits are claimed, ability deficits are claimed, clinicians should administer measures that can evaluate responseclinicians should administer measures that can evaluate responsebias related to both.bias related to both.
–– Serial evaluations can be particularly helpful in discriminatingSerial evaluations can be particularly helpful in discriminatinggenuine injury from unrealistic performances or variable selfgenuine injury from unrealistic performances or variable self--report of deficits and disabilities that reflect variable effortreport of deficits and disabilities that reflect variable effortand/or response bias.and/or response bias.
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering

•• Somatic IssuesSomatic Issues–– When assessing the possibility of nonWhen assessing the possibility of non--credible somatic credible somatic
presentation, clinicians should use multiple wellpresentation, clinicians should use multiple well--validated validated measures covering self report, performance, and symptom measures covering self report, performance, and symptom validity.validity.
–– To keep false positives low, which is important, carefully rule To keep false positives low, which is important, carefully rule out plausible alternative explanations. The veracity of self out plausible alternative explanations. The veracity of self report considers actuarial data as an aid to clinical judgment.report considers actuarial data as an aid to clinical judgment.
–– The completeness and accuracy of historical information is The completeness and accuracy of historical information is important in evaluating the validity of somatic complaints.important in evaluating the validity of somatic complaints.
–– Clinicians should keep current with relevant literature that Clinicians should keep current with relevant literature that addresses nonaddresses non--credible somatic presentation.credible somatic presentation.
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering
•• Psychological IssuesPsychological Issues–– SelfSelf--reported psychological symptoms may be biased, false, or reported psychological symptoms may be biased, false, or
incomplete; proactive assessment must evaluate these possibilitiincomplete; proactive assessment must evaluate these possibilities.es.
–– Clinicians should utilize multiple SVTs throughout the evaluatioClinicians should utilize multiple SVTs throughout the evaluation.n.
–– Clinicians should be familiar with base rates of mental disorderClinicians should be familiar with base rates of mental disorders s and emotional symptoms in the general population.and emotional symptoms in the general population.
–– CoCo--occurrence of genuine psychopathology and occurrence of genuine psychopathology and feigned/exaggerated symptoms is common in litigants; important tfeigned/exaggerated symptoms is common in litigants; important to o delineate the relative presence of each.delineate the relative presence of each.
–– Clinicians should use best available, current methodologies and Clinicians should use best available, current methodologies and instruments.instruments.
–– Clinicians should be current consumers of the relevant scientifiClinicians should be current consumers of the relevant scientific c literature.literature.
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering
With all three areas (Ability, Somatic, Psychological), With all three areas (Ability, Somatic, Psychological), consider cultural and ethnic differences as appropriate consider cultural and ethnic differences as appropriate to individual case. Demographic variables should also to individual case. Demographic variables should also be considered. Gender is not a factor in general, but be considered. Gender is not a factor in general, but with a subset of measures (e.g., strength) gender may with a subset of measures (e.g., strength) gender may need to be considered. need to be considered.
AACN Consensus Conference on AACN Consensus Conference on Effort, Response Bias, and Malingering Effort, Response Bias, and Malingering

The Prominence of GuidelinesThe Prominence of Guidelines
National Guideline Clearing House website National Guideline Clearing House website http://www.guideline.gov/http://www.guideline.gov/
NGC is a public resource for evidenceNGC is a public resource for evidence--based clinical practice based clinical practice guidelines. Under auspices of the guidelines. Under auspices of the
What are Guidelines?What are Guidelines?American Medical Association American Medical Association
Practice parameters or guidelines should:Practice parameters or guidelines should:1) be developed by or in conjunction with physician 1) be developed by or in conjunction with physician
organizations, organizations,
2) explicitly describe the methodology and process used in 2) explicitly describe the methodology and process used in their development, their development,
3) assist practitioner and patient decisions about appropriate 3) assist practitioner and patient decisions about appropriate health care for specific clinical circumstances, health care for specific clinical circumstances,
4) be based on current professional knowledge and reviewed 4) be based on current professional knowledge and reviewed and revised at regular intervals, and and revised at regular intervals, and
5) be widely disseminated. 5) be widely disseminated.
What are Guidelines?What are Guidelines?Institute of MedicineInstitute of Medicine
Practice guidelines are systematically developed statements to Practice guidelines are systematically developed statements to assist practitioners and patients in making decisions about assist practitioners and patients in making decisions about appropriate health care for specific clinical circumstances.appropriate health care for specific clinical circumstances.
Attributes or criteria desired in the finished product:Attributes or criteria desired in the finished product:1) validity, based on the strength of the evidence, expert 1) validity, based on the strength of the evidence, expert
judgment, and estimates of health and cost outcomes judgment, and estimates of health and cost outcomes compared with alternative practices; compared with alternative practices;
2) reliability and reproducibility; 2) reliability and reproducibility;
3) clinical applicability and flexibility; 3) clinical applicability and flexibility;
4) clarity; 4) clarity;
5) attention to multidisciplinary concerns; 5) attention to multidisciplinary concerns;
6) timely updates; and 6) timely updates; and
7) documentation. 7) documentation.

Infectious Diseases Society of America Infectious Diseases Society of America Perspective on GuidelinesPerspective on Guidelines
Guidelines cannot always account for individual Guidelines cannot always account for individual variation among patients.variation among patients.
Guidelines are not intended to supplant physicianGuidelines are not intended to supplant physicianjudgment with respect to particular patients or judgment with respect to particular patients or special clinical situations. special clinical situations.
Adherence to IDSA guidelines is voluntary, with theAdherence to IDSA guidelines is voluntary, with theultimate determination regarding their applicationultimate determination regarding their applicationto be made by the physician in the light of eachto be made by the physician in the light of eachpatientpatient’’s individual circumstances.s individual circumstances.
What are Guidelines?What are Guidelines?American Psychological Association American Psychological Association
Policy on Creating GuidelinesPolicy on Creating Guidelines
GuidelinesGuidelines are statements that suggest or recommend are statements that suggest or recommend specific professional behavior, endeavor, or conduct specific professional behavior, endeavor, or conduct for psychologists. for psychologists.
Primary purpose of Primary purpose of practice guidelinespractice guidelines is to assist the is to assist the practitioner in the provision of high quality practitioner in the provision of high quality psychological services by providing wellpsychological services by providing well--supported supported practical guidance and education in a particular practical guidance and education in a particular practice area. practice area.
Practice guidelines also Practice guidelines also ““inform psychologists, the inform psychologists, the public, and other interested parties regarding desirable public, and other interested parties regarding desirable professional practicesprofessional practices””..
•• Guidelines are aspirational in intent, not mandatory.Guidelines are aspirational in intent, not mandatory.
•• Guidelines may not be applicable to every Guidelines may not be applicable to every professional and clinical situation. professional and clinical situation.
•• Not definitive and not intended to take precedence Not definitive and not intended to take precedence over the judgment of psychologists. over the judgment of psychologists.
•• Consist of recommendations to professionals Consist of recommendations to professionals concerning their conduct and the issues to be concerning their conduct and the issues to be considered in particular areas of psychological considered in particular areas of psychological practice.practice.
What are Guidelines?What are Guidelines?American Psychological Association American Psychological Association
Policy on Creating GuidelinesPolicy on Creating Guidelines

Examples of Recent APA GuidelinesExamples of Recent APA Guidelines
•• Guidelines for Child Custody Evaluations In Family Guidelines for Child Custody Evaluations In Family Law Proceedings (2010)Law Proceedings (2010)
•• Guidelines for the Practice of Parenting Coordination Guidelines for the Practice of Parenting Coordination (2011)(2011)
•• Guidelines for the Evaluation of Dementia and AgeGuidelines for the Evaluation of Dementia and Age--Related Cognitive Change (2011)Related Cognitive Change (2011)
•• Guidelines for Assessment of and Intervention with Guidelines for Assessment of and Intervention with Persons with Disabilities (2011)Persons with Disabilities (2011)
AACN Practice GuidelinesAACN Practice Guidelines
AACN Practice GuidelinesAACN Practice Guidelines
E. Assessment of Motivation and EffortE. Assessment of Motivation and EffortA growing literature suggests that the assessment of motivation A growing literature suggests that the assessment of motivation and effort isand effort iscritical when conducting a neuropsychological evaluation (Bush &critical when conducting a neuropsychological evaluation (Bush & NAN Policy &NAN Policy &Planning Committee, 2005b). This area has received the greatest Planning Committee, 2005b). This area has received the greatest emphasis in forensicemphasis in forensicassessment, in which symptom magnification, impression managemenassessment, in which symptom magnification, impression management, or even feigningt, or even feigningof impairment can occur (Mittenberg, Patton, Canyock, & Condit, of impairment can occur (Mittenberg, Patton, Canyock, & Condit, 2002). However,2002). However,the assessment of effort and motivation is important in any clinthe assessment of effort and motivation is important in any clinical setting, asical setting, asa patienta patient’’s effort may be compromised even in the absence of any potentials effort may be compromised even in the absence of any potential or activeor activelitigation, compensation, or financial incentives. Approaches folitigation, compensation, or financial incentives. Approaches for assessing motivationr assessing motivationand effort include: behavioral observations from interview or teand effort include: behavioral observations from interview or testing of behaviors suchsting of behaviors suchas avoidance, resistance, hostility, and lack of cooperation; exas avoidance, resistance, hostility, and lack of cooperation; examination of the patternamination of the patternof performance among traditional neuropsychological measures; idof performance among traditional neuropsychological measures; identification ofentification ofunexpected or unusually slow and=or impaired levels of performanunexpected or unusually slow and=or impaired levels of performance; identificationce; identificationof cognitive profiles that do not fit with known patterns typicaof cognitive profiles that do not fit with known patterns typical of brain disorders;l of brain disorders;and consideration of suspect performance on objective measures oand consideration of suspect performance on objective measures of effort. Cliniciansf effort. Cliniciansutilize multiple indicators of effort, including tasks and paradutilize multiple indicators of effort, including tasks and paradigms validated for thisigms validated for thispurpose, to ensure that decisions regarding adequacy of effort apurpose, to ensure that decisions regarding adequacy of effort are based on convergingre based on convergingevidence from several sources, rather than depending on a singleevidence from several sources, rather than depending on a single measure or method.measure or method.

E. Assessment of Motivation and EffortE. Assessment of Motivation and Effort
A growing literature suggests that A growing literature suggests that the assessment of the assessment of motivation and effort is critical when conducting a motivation and effort is critical when conducting a neuropsychological evaluation neuropsychological evaluation (Bush & NAN Policy & (Bush & NAN Policy & Planning Committee, 2005b). Planning Committee, 2005b).
AACN Practice GuidelinesAACN Practice Guidelines
E. Assessment of Motivation and EffortE. Assessment of Motivation and Effort
Approaches for assessing motivation and effort include: Approaches for assessing motivation and effort include: behavioral observations from interview or testing of behavioral observations from interview or testing of behaviors such as avoidance, resistance, hostility, and behaviors such as avoidance, resistance, hostility, and lack of cooperation; examination of the pattern of lack of cooperation; examination of the pattern of performance among traditional neuropsychological performance among traditional neuropsychological measures; identification of unexpected or unusually measures; identification of unexpected or unusually slow and/or impaired levels of performance; slow and/or impaired levels of performance; identification of cognitive profiles that do not fit with identification of cognitive profiles that do not fit with known patterns typical of brain disorders; and known patterns typical of brain disorders; and consideration of suspect performance on objective consideration of suspect performance on objective measures of effortmeasures of effort..
AACN Practice GuidelinesAACN Practice Guidelines

E. Assessment of Motivation and EffortE. Assessment of Motivation and Effort
Clinicians utilize multiple indicators of effortClinicians utilize multiple indicators of effort, including , including tasks and paradigms validated for this purpose, to ensure tasks and paradigms validated for this purpose, to ensure that decisions regarding adequacy of effort are based on that decisions regarding adequacy of effort are based on converging evidence from several sources, converging evidence from several sources, rather than rather than depending on a single measure or method.depending on a single measure or method.
AACN Practice GuidelinesAACN Practice Guidelines
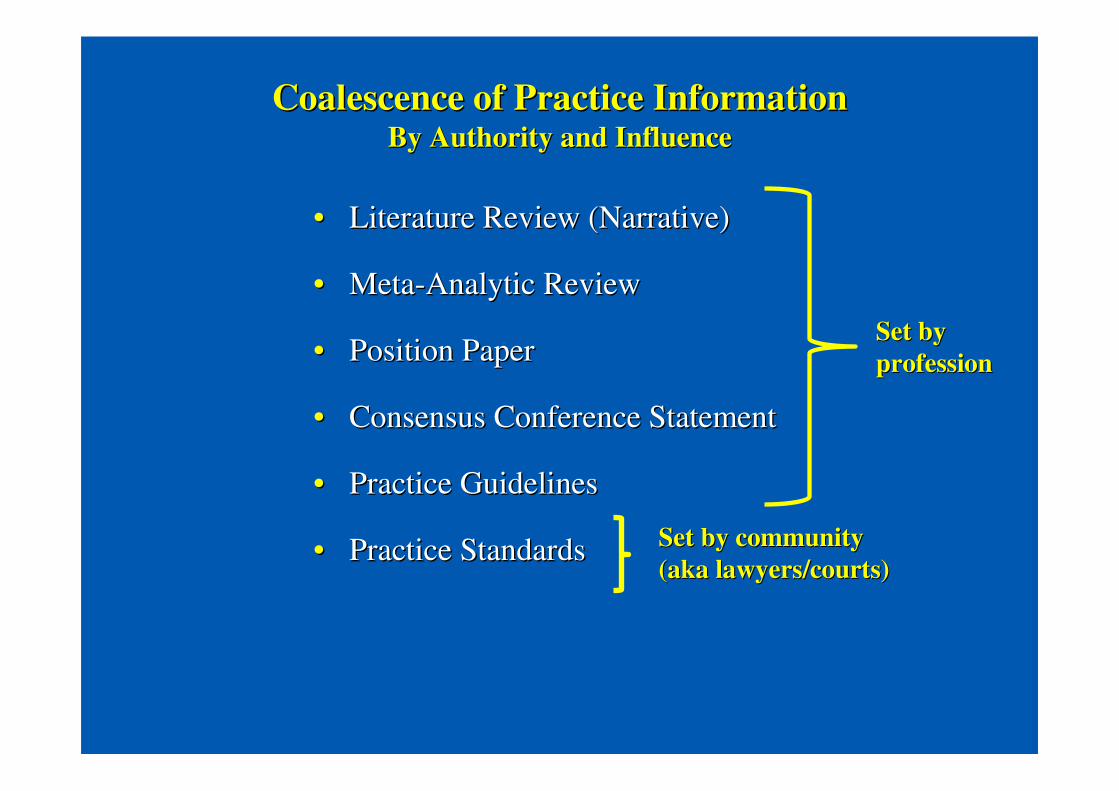
Coalescence of Practice InformationCoalescence of Practice InformationBy Authority and InfluenceBy Authority and Influence
•• Literature Review (Narrative)Literature Review (Narrative)
•• MetaMeta--Analytic ReviewAnalytic Review
•• Position PaperPosition Paper
•• Consensus Conference StatementConsensus Conference Statement
•• Practice GuidelinesPractice Guidelines
•• Practice StandardsPractice Standards
Set by Set by professionprofession
Set by communitySet by community(aka lawyers/courts)(aka lawyers/courts)
If you are not on board yetIf you are not on board yet……
Are you waiting for the knowledge base to mature?Are you waiting for the knowledge base to mature?
Are you waiting for sufficient choices of methods?Are you waiting for sufficient choices of methods?
Are you waiting for professional guidance from experts?Are you waiting for professional guidance from experts?
Are you waiting for mainstream professional Are you waiting for mainstream professional organizations to weigh in?organizations to weigh in?
What What areare you waiting for? Godot?you waiting for? Godot?
Waiting for GodotWaiting for Godot……(Wikipedia)(Wikipedia)……follows two days in the follows two days in the lives of a pair of men who divert themselves while they wait lives of a pair of men who divert themselves while they wait expectantly and in vain for someone named Godot to arrive. expectantly and in vain for someone named Godot to arrive. They claim him as an acquaintance but in fact hardly know They claim him as an acquaintance but in fact hardly know him, admitting that they would not recognise him were they to him, admitting that they would not recognise him were they to see him. To occupy themselves, they eat, sleep, converse, see him. To occupy themselves, they eat, sleep, converse, argue, sing, play games, exercise, swap hats, and contemplate argue, sing, play games, exercise, swap hats, and contemplate suicide suicide –– anything anything ““to hold the terrible silence at bay.to hold the terrible silence at bay.””
16.16. Effort and Malingering Will be Asked About in Effort and Malingering Will be Asked About in AllAll Adversarial Adversarial Cases; Deal With This ProspectivelyCases; Deal With This Prospectively
a.a. Alternatively, when the time comes, Alternatively, when the time comes, admit under oathadmit under oath loud loud and clear for everyone to hear that you are:and clear for everyone to hear that you are:
RIDICULOUSLY UNINFORMED,RIDICULOUSLY UNINFORMED,
OUTRAGEOUSLY NAOUTRAGEOUSLY NAÏÏVE,VE,
OROR OBVIOUSLY BIASED!!!OBVIOUSLY BIASED!!!b.b. Reality is anyone not evaluating for effort and response Reality is anyone not evaluating for effort and response
validity is going against the strongly stated published practicevalidity is going against the strongly stated published practicerecommendations of numerous forensic experts and can be recommendations of numerous forensic experts and can be impeached easily for saying impeached easily for saying ‘‘it isnit isn’’t sot so’’..
Points of Consensus for Neuropsychologists
To view extensive forensic bibliography, go to URL:To view extensive forensic bibliography, go to URL:
www.sweetmalingeringrefs.webstarts.comwww.sweetmalingeringrefs.webstarts.com

Evanston HospitalEvanston Hospital Glenbrook HospitalGlenbrook Hospital
Highland Park HospitalHighland Park Hospital Skokie HospitalSkokie Hospital





























