Embed Size (px)
Citation preview

PROCEEDINGS OF THE GERMAN SOCIETY FOR N E U R O S U R G E R Y
M O D E R N ASPECTS OF N E U R O S U R G E R Y V O L U M E 4
I. T H E P E R I P H E R A L V I S U A L P A T H W A Y
II. P I T U I T A R Y T U M O R S
III. VARIA
P R O C E E D I N G S O F T H E 2 3 r d A N N U A L M E E T I N G H E L D I N H A M B U R G , S E P T E M B E R 2 5 - 2 7 . 1 9 7 2
Editors H. K U H L E N D A H L , Düsseldorf
M. B R O C K , Hannover D . L E VAY, Wi thyham/Sussex T. J. W E S T O N , Ferr ing/Sussex
1973
E X C E R P T A M E D I C A A M S T E R D A M A M E R I C A N E L S E V I E R C O M P A N Y , I N C . N E W Y O R K

© Excerpta Medica Foundation, 1973 All rights reserved. N o par t of this publication may be reproduced, stored in a retrieval System or transmitted, in any form or by any means , electronic, mechanical, photocopying, recording or otherwise, without permission in writing from the publisher.
International Congress Series N o . 306 ISBN Excerpta Medica 90219 0249 4 ISBN American Elsevier 0444 15104 4 Library of Congress Catalog Card N u m b e r 73-152681
Publisher Excerpta Medica 335 Jan van Galenstraat Amste rdam P.O. Box 1126
Sole Distributors for the U.S.A. and Canada American Elsevier Publishing Company , Inc. 52 Vanderbilt Avenue New York, N .Y. 10017
Printed in The Nether lands by N.V. Drukkeri j Trio, The Hague

T H E G E R M A N SOCIETY F O R N E U R O S U R G E R Y
President 1972 Hans Kuhlendahl , Düsseldorf
Vice-P resident Kur t Schürmann, Mainz
Secretary Wolf Schiefer, Erlangen
Treasurer Helmut Penzholz, Heidelberg

C O N T E N T S
H. K U H L E N D A H L : Preface vi
I. T H E P E R I P H E R A L V I S U A L P A T H W A Y A. H O P F : Anatomy of the peripheral (infrageniculate) visual pathway 3 C H . B A U M A N N : Physiology of the lower visual pathway 8 L. G E R H A R D : Neuropa thology of the peripheral visual pathway 1 0 E. A U L H O R N : Visual field defects in sellar and parasellar processes 1 6 A. H U B E R : Differential diagnosis of disc swelling 2 3 F . M A R G U T H : Symptomatology of space-occupying lesions in the area of the sella
turcica 3 2 A. N O V E R : Inflammations, vascular diseases, and arachnitis in the region of the pe
ripheral visual pathway (summary) 3 5 A. TÄNZER: The radiological diagnosis of lesions of the peripheral visual tract . . . 3 6 K . VON W I L D and H. R U F : Diagnostic problems and errors in suprasellar meningiomas 4 3 M . S A M I I : Visual disturbances caused by a low located optic chiasm 4 8 H. BRENNER and G . P E N D L : Neuro-ophthalmological non-hemorrhagic complications
of intracranial aneurysms 5 6 F . L O E W and G . K R E M E R : Operative procedures in the sellar and parasellar region
( tumors , opto-chiasmatic arachnoidit is) 6 0 R. S E I T Z : Traumat ic lesions of the optic nerve and differential diagnosis of optic nerve
a t rophy 6 8 U. MÜLLER, W. BETTAG and F . RÖMER: The operative care of t raumat ic optic lesions 7 2 N . K L U G : Penetrating orbitocerebral injuries 7 5
IL P I T U 1 T A R Y T U M O R S P . C. SCRIBA: Endocrinology of the hypotha lamus and the pituitary gland 8 3 R. F A H L B U S C H : Endocrinology of pituitary tumors 9 0 F R . E N G E L H A R D T : The influence of the hypothalamus on adenohypophyseal neoplasms 9 6 C. R. P ICKARDT, F . E R H A R D T , R. FAHLBUSCH, J. GRÜNER and P . C. SCRIBA: T h e d i a g -
nostic significance of the Stimulation of TSH secretion by administrat ion of thyro-tropin releasing hormone ( T R H ) in diseases of the hypothalamus and pituitary . . 1 0 5
U. HACHMEISTER: Ultrastructural aspects of anterior pituitary tumors 1 0 8 A. M. L A N D O L T : The oncocytoma, a new histological type of pituitary adenoma (sum
mary) 1 1 6 W. SAEGER: Light and electron microscopic studies of pituitary adenomas from patients
vii

with acromegaly correlated with the plasma level of growth hormone 117 H . HIRSCHBIEGEL and W . ISCHEBECK: Expansive extradural growth of pituitary ade-
nomas 122 H . - E . C L A R and F . RÖMER: Methods of diagnosis of parasellar processes of the base of
the skull 124 L . G E R H A R D , V. HENSELL and V. R E I N H A R D T : Dystopie pinealoblastomas 129 H . A L T E N B U R G , H . W A L D B A U R and F . W O L F : Brain scan findings in cases of sellar and
suprasellar tumors 133 R. K A U T Z K Y and D . LÜDECKE: Experiences with the transsphenoidal approach to the
hypophysis 135 W . PIOTROWSKI , H . P E N Z H O L Z and K . P ISCOL: Indications and choice of surgical
procedure for pituitary tumors 142 H . W . P I A : Transfrontal t ranssphenoidal Operation on the pituitary gland 146 T. R I E C H E R T : The combined open-stereotactic transsphenoidal Operation on tumors of
the hypophysis 148 T. SCHARPHUIS , E. H A L V E S and T H . G R U M M E : The subfrontal and transethmoidal
approach applied to hypophysectomy 150 H . R U F , K . VON W I L D and M. N E U B A U E R : Fol low-up studies on 33 craniopharyngio-
mas and 95 cases of ch romophobe and acidophil pituitary adenomas after t reatment by transfrontal Operation 152
O. G R A T Z L a n d R. F A H L B U S C H : Cryohypophysectomy in connection with t ranssphenoidal surgery of pituitary adenomas 162
H . BRENNER and F . BÖCK: Possible mechanisms explaining postoperative visual defects following extirpation of suprasellar meningiomas 165
F . M U N D I N G E R and W . BRÄUN: Stereotactic interstitial Curie therapy of pituitary a denomas : a long-term follow-up study of up to 12 years 168
K . VON W I L D , P. RÖTTGER and W . KRÜCKE: Recurrent adenoma of the adenohypophy-sis in connection with polyadenomatosis of endoerine glands, pheochromocytoma and alopecia totalis 175
H . N O W A K O W S K I : Indicat ions, therapeutic value and results of hypophysectomy. . . 180 W . K R E N K E L : Craniopharyngiomas 184 H . ZIMMERMANN, H . G . SOLBACH and W . W I E G E L M A N N : Pre- and postoperat ive hor
m o n e Substitution in pituitary tumors 191 D . LÜDECKE, H . F R A H M and H . D . FREISENHAUSEN: Pathophysiology and therapy of
diabetes insipidus after Operations in the region of the hypophysis 197 H . D . FREISENHAUSEN and H . F R A H M : New aspects of the pathogenesis and therapy of
diabetes insipidus 203
III . V A R I A R.-I . K A H L , M. SAMII and H . W I L L E B R A N D : Clinical results of perineural fascicular
neurolysis 209 H . P E N Z H O L Z : Comments on the treatment of peripheral nerve injuries with homolo-
gous nerve grafts 213 R. MÜKE: Experiences with percutaneous cervical cordotomy 215 V. G R U N E R T and M. SUNDER-PLASSMANN : In t ra luminal occlusion of carot id-eavernous
sinus fistulas using a Fogar ty catheter 219 H . W A N D T , W . GOBIET and W . J. B O C K : The advantage of frontal siting of the ventri-
cular catheter in atr ioventricular shunt Operations 225 H . W A L D B A U R , W . G R A F and S T . K U N Z E : Investigations into the passage of the b road-
spectrum penicillin, carbenicillin, into the C S F 227 W . WINKELMÜLLER and A. S P R I N G : The importance of dopamine-rich struetures in the
midbrain for vigilance, motorici ty and blood pressure regulation 231 K . ROOSEN, W . J. B O C K , B. NIEDERMEIER, J. LIESEGANG and W . G R O T E : In t raopera t ive
gas-analytical studies of the cerebral venous blood in cases of intracranial ang ioma 235 E. M A R K A K I S , M. B R O C K , G . B O C K and H . D I E T Z : Respiratory changes of brain pulsa-
viii

tions after experimental increase of intracranial pressure 2 3 9 J. HAMER and E. ALBERTI : The eflfect of increased intracranial pressure on the venous
pressure in the sagittal sinus of the dog 2 4 4 E. W E I G E L I N : Discussion of paper by Hamer and Alberti 2 4 9 S T . K U N Z E and W . SCHIEFER: Central ventriculography with water-soluble, resorbable
contrast media - experimental and clinical investigations 2 5 1 N . NAKAYAMA and S . W E N D E : Value of magnification technique in angular venography 2 5 7 F. RÖMER, J . LIESEGANG and R . W I N H E L L E R : A comparison of various methods for
localizing the level of cervical disc hernias 2 6 1 Index of authors 2 6 4
ix

E N D O C R I N O L O G Y O F T H E H Y P O T H A L A M U S A N D T H E P I T U I T A R Y G L A N D *
P E T E R C. SCRIBA IL Medizinische Klinik der Universität München, Munich, Federal Republic of Ge rmany
At present, the endocrinology of the hypothalamus and the pituitary gland has two main aspects with respect to tumors of this region: (1) the Observation of endocrine Symptoms per-mits the diagnosis of a tumor at an early stage, and (2) hormonal overproduction or defi-ciency must be evaluated, since therapy by ablative or substitutive measures is of considerable impor tance for the well-being and life expectancy of these patients.
P A T H O P H Y S I O L O G I C A L C O N S I D E R A T I O N S T h e rapidly growing information about the hormones of the hypothalamus and pituitary gland hasrecently been reviewed ina t ex tbook of pathophysiology (Scriba et al., 1972). Today , the blood levels of the hormones of the human anterior pituitary (Table I) are determined radioimmunologically. Determination of the levels of growth hormone ( G H ) and of the glycoproteohormones TSH, LH and FSH is most commonly carried out by endocrinologists. T h e structures of the human glycoproteohormones are not yet fully analyzed; their subunits a and ß (Table I) are just gaining at tention as pathogenic factors and for diagnostic questions, whereas the human pituitary Proteohormones , except for prolactin, have been synthesized.
Since the posterior pituitary is the subject of further Communicat ions during this Conference, it may be permitted just to ment ion briefly the functional Separation of the secretion of anti-diuretic hormone ( A D H ) and thirst. Table II gives a summary of dissociated and combined disturbances of A D H secretion and thirst.
In recent years the concept of hypothalamic hypophyseotropic hormones has been introduced into clinical endocrinology. In Table III the releasing and inhibiting factors so far known are reported, together with the structures of 4 of these factors. Synthetic T R H (thyrotropin releasing hormone) and L H - R H (LH releasing hormone) have recently been employed for diagnostic and therapeutic purposes.
The secretion of the hypophyseotropic hormones is itself influenced by hypothalamic catecholamines (neurotransmitters) . Kamber i et al. (1971) have shown by in vitro and in vivo experiments that dopamine stimulates LH secretion in rats via increased L H - R H secretion. In man L-dopa must be used since L-dopa, in contrast to dopamine , can cross the blood-brain barrier and serves as a precursor for dopamine and norepinephrine. Intravenous injection of L-dopa in patients does not increase the LH levels, as expected from animal experiments (Souvatzoglou et al., 1973). There is, however, a marked increment in growth hormone levels, presumably due to increased secretion of hypothalamic G R F after giving L-dopa intra-venously. On the other hand, prolactin levels are diminished by L-dopa (Malarkey et al. , 1971), apparently because of increased secretion of prolactin inhibiting factor (PIF) . With PIF deficiency increased prolactin secretion is observed (Turkington et al., 1971), as neuro-surgeons are well aware from the galactorrhea that follows pituitary stalk section.
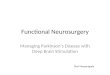
In Figure 1 a scheme is given of the vertical functional relations between the groups of * Supported by the Deutsche Forschungsgemeinschaft (SFB 51).
83

TABLE I Human anterior pituitary hormones
Symbol Name Molecular Amino acids Carbohy- Biological assay Normal* plasma values Plasma half-life weight drate Biological Radioimmuno-
(%> assay assay a. Proteohormones: ACTH Adrenocortico- 4600 39 — Corticosterone 0-5 LtU/ml < 1-50 pg/ml Exogenous
t ropb hormone, secretion into (9 a.m.) (8-10 a.m.) 5-13 min; corticotropin theadrenal vein
of hypophysecto-mized rats
endogenous longer
ß-MSH Melanocytesti-mulating hormone 2700 22 — Pigmentation of
frog skin ? 20-110 pg/ml 7
HGH = Human growth 21500 190 — Epiphyseal ? < 1-5 ng/ml Endogenous STH hormone =
somatotropin cartilage of tibia, hypophys-ectomized rats
50 min
HPr Prolactin 22550 (ovine) 198 — Pigeon crop 7 20-37 ng/ml 30 min
h. Glycoproteohormones: * * * TSH Thyroid 25000 a 96 15 131I-secretion 166 LtU / m l 0.6-4.2 Exogenous 68
stimulating (bovine) ß 113 of mouse thyroid ? fxU/ml min;endogenous hormone 90-130 min FSH Follicle 32000 7 15 Augmentation of — 4 mIU/ml** Initial phase 4 hrs stimulating (ovine) HCG effect on
Initial phase 4 hrs hormone rat ovaries
LH = Luteinizing 30000 a 96 18 Ascorbic acid — 13 mIU/ml** Initial phase ICSH hormone =
interstitial cell stimulating hormone
(ovine) ß 120 depletion, ovaries 1-2 hrs
* Normal plasma values depend on the deflnition of normal conditions: hour of the day, nutrition, age, sex and other factors have substantial influence?. ** Values for normal young men in mlU IRP-2-HMG/ml serum; cyclic patterns are observed in women. *** Glycoproteohormones have two chemically different subunits (M ~ 15000). Recombination experiments revealed that TSH-a, FSH-a and LH-a may be substituted; therefore the ß subunits determine biological and immunological specificity. The amino acid sequences of LH-a, LH-ß (ovine), of TSH-a, TSH-ß(bovine) and the structure of the carbohydrate units of HCG-a and HCG-ß are published; the carbohydrate units of the glycoproteohormones are linked to aspartic acid. (From Scriba et al., 1972.)

ENDOCRINOLOGY OF HYPOTHALAMUS AND PITUITARY GLAND
TABLE II Disorders of ADH secretion and thirst
ADH secretion Thirst Clinical manifestations
Absent even after induction of hyper-natremia by water deprivation
Normal Classic diabetes insipidus (polyuria and polydipsia)
Elevation of 'osmotic threshold' for ADH release
Normal 'Diabetes insipidus', urinary osmolality increases only after marked hypernatremia
Normal Decreased or absent Adipsia, hypernatremia without polyuria Elevation
of 'osmotic threshold1 for ADH release
Decreased or absent Hypernatremia, Syndrome of hypodipsia and ADH-reset
Absent even in presence of hypernatremia
Decreased or absent Severe hypernatremia without polyuria, adipsia
Normal Increased, decreased osmotic threshold for thirst
Primary polydipsia, psychogenic polydipsia has to be differentiated
Inappropriately increased Normal Hyponatremia SIADH, Syndrome of inapprop-riate ADH secretion (Schwartz-Bartter)
(After Mahoney and Goodman, 1968.)
TABLE III Hypophyseotropic hormones* - 'releasing factors'
Hypophyseotropic hormone Structure
C R F Corticotropin releasing factor MSH-RF = MSH releasing factor MIF = MSH inhibiting factor Pro-Leu-Gly-NH, G R F GH releasing factor Val-His-Leu-Ser-Ala-Glu-Glu-Lys-Glu-Ala? GIF GH inhibiting factor PRF = Prolactin releasing factor PIF = Prolactin inhibiting factor T R F Thyrotropin releasing factor pyro-Glu-His-Pro-NH2 LRF LH releasing factor pyro-Glu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-
GIy-NH8 FRF FSH releasing factor * Instead of the abbreviation RF (releasing factor) RH may be used, e.g. TRH = thyrotropin
releasing hormone. (From Scriba et al., 1972.)
85

P. C. SCRIBA
HYPOTHALAMUS:
ANTERIOR PITUITARY:
PERIPHERAL GLAND:
NEURAL OR HUMORAL (CATECHOLAMINES) STIMULI,
DRU6S
HYPOPHYSEOTROPIC H0RM0NE= RELEASING FACTOR
ANTERIOR PITUITARY HORMONE= GLANDOTROPIC HORMONE
PERIPHERAL HORMONE
-STIMULATION —-INHIBITION
BLOOD: PLASMA PROTEIN-BOUND HORMONE
MODIFYING FACTORS
BIOLOGICAL EFFECT METABOLISM
Fig. /. Regulation of anterior pituitary hormone secretion. (From Scriba et al., 1972.)
hormones briefly discussed above. Hypothalamic catecholamines and hypophyseotropic hormones , together with the glandotropic hormones of the anter ior pituitary, regulate the secretion of the peripheral target glands. The free, non-protein bound , i .e.biologicallyactive, component of the hormones of the peripheral target glands is the parameter regulated by the glandotropic hormones A C T H , TSH and gonadot ropins . Measurable alterations in the vertical hormonal axes serve for the regulation of the free peripheral hormones .
Tumors of the hypothalamic-pitui tary region may lead to a deficiency in hypophyseotropic hormones, with consequent hypopitui tar ism, or alternatively may directly produce a deficient secretion of pituitary hormones with secondary insufficiency of the target glands (Fig. 1). In contrast to these forms of hypopituitarism in cases of inactive tumors , ho rmona l over-production is found in hormonally active tumors: thus, the growth ho rmone excess of a pituitary adenoma causes acromegaly, while hamar tomas of the tuber cinereum may produce pubertas praecox by increased L H - R H secretion.
86

ENDOCRINOLOGY OF HYPOTHALAMUS AND PITUITARY GLAND D I A G N O S T I C I M P L I C A T I O N S O F TESTS F O R H Y P O T H A L A M I C
A N D P I T U I T A R Y F U N C T I O N This section briefly reviews the information which neurosurgeons may obta in from examina-tion of hypotha lamic and pituitary function. Table IV summarizes horizontally the site of action and vertically the effective scope of the endocrinological methods .
In clinically evident hypopituitarism the determination of basal levels of pituitary and target gland ho rmones will not always reveal subnormal values. This is for methodological reasons, since the analytical procedures do not always permit a distinction between the wide normal ranges of controls and the lowered values of these patients. Thus, in cases of complete or incomplete 'panhypopi tu i ta r i sm\ normal or subnormal basal hormone levels may be found. Therefore, as a general endocrinological rule, Stimulation tests are employed for the diagnosis of insufficiency states and suppression tests for hormonal overproduction states.
St imulat ion tests are available for the examinat ion of disorders of the hypothalamic-pituitary region. These act on the site of the hypothalamus and o n the anterior pituitary. The technical problems of all these tests have recently been discussed at length in the endocr inological tex tbook of Labhar t (1971) and will not be dealt with here. As a first example the Insulin hypoglycemia fest (Table IV) will be mentioned, in which the control person reacts with an increased secretion of growth hormone . This test is of particular value in the diagnosis of pituitary insufficiency, as discussed by Fahlbusch during this meeting (pp. 90-95). The same procedure, the insulin hypoglycemia test, also provides a means to test the CRF-ACTH-cortisol axis and to assess the ability of a patient to tolerate stressful situations.
A decreased response to this test may be due to an insufficiency at one or more of the levels mentioned, namely hypothalamus, adenohypophysis or adrenal gland. In this case lysin-vasopressin is used as a cort icotropin releasing factor ( C R F ) for further eludication. A positive response to lysin-vasopressin, i.e. increase of radioimmunologically determined A C T H levels or of Cortisol levels, reveals intact cort icotropic function of the adenohypophys i s and locates the disorder in the suprasellar region. Lysin-vasopressin may also be used for the differential diagnosis of Cushing's Syndrome, since no response is found in cases caused by adrenal tumors in contrast to cases of hypothalamic-hypophyseal origin (Scriba et al., 1972). The CRF-ACTH-cor t i so l axis is, however, only of limited value for the diff'erentiation between hypothalamic and hypophyseal disorders, since only a small proport ion of patients with tumors in the hypothalamic-hypophyseal region have secondary adrenal insufficiency.
In the next axis (Table IV) synthetic T R H is used for the Stimulation of TSH secretion by the adenohypophysis . This test provides information about the suprasellar extension of pituitary tumors (Pickardt et al., This Volume, pp . 105-107). However, n o means yet exist for specifically st imulating the secretion of endogenous T R H , as anti thyroidal drugs - and other inhibitors as well, e.g. Metopirone (Table IV) - act on the adenohypophysis and the hypothalamus simultaneously. Synthetic L H - R H has recently been employed to st imulate the secretion of both gonadotropins (LH, FSH) at the pituitary level, whereas Clomifene apparently acts via increased secretion of hypothalamic endogenous L H - R H . The Clomifene Stimulation test has , however, the disadvantage of a lag time of some days (Souvatzoglou, personal communica-tion).
After these considerations we have briefly to come back to the tests for secretion of the directly acting adenohypophyseal hormones G H and prolactin. In addit ion to the insulin hypoglycemia test (La.) it is possible to st imulate growth hormone secretion at the hypothalamic level using intravenous L-dopa injection (Souvatzoglou et al., 1973), which at the same time lowers the prolactin levels (La. ) . Since T R H stimulates the secretion of prolactin as well as of T S H , the former hormone may be checked at both the hypothalamic and the adenohypophyseal level.
The aims of endocrinological examination of patients with hypopituitarism may be summa-rized as follows: 1. Detection of hormonal deficiencies and estimation of the necessary substitutive therapy. 2. Assessment of stress tolerance. 3. Differentiation of hypothalamic and adenohypophyseal hypopituitarism. 4. Differentiation of primary and secondary insufficiency of target glands. 5. Stimulation tests at the hypothalamic and hypophyseal levels may in addit ion provide
87

TABLE IV Site of action and effective scope of endocrinological methods for the investigation of hypothalamic and pituitary disorders
1. Basal hormone levels Determination of (glandotropic) anterior pituitary hormones Determination of peripheral hormones
2. Stimulation tests Stimulation of the axis hypothalamus-pituitary-peripheral gland Withdrawal of peripheral hormones = Stimulation of hypothalamus-pituitary Stimulation of the anterior pituitary with hypophyseotropic hormones Stimulation of peripheral glands with glandotropic hormones 3. Suppression tests Hypothalamus-pituitary
ACTH TSH Cortisol Thyroxine, (circadian rhythm!) triiodothyronine
LH, FSH Testosterone, estrogens, progesterone
Clomifene
Growth hormone Prolactin
Insulin — Clomifene Insulin, hypo- Phenothiazine f hypoglycemia glycemia, arginine, L-dopa \
L-dopa Metopirone Antithyroid drugs (Anti-androgen) — —
Lysin-vasopressin TRH (as CRF)
ACTH Stimulation test
TSH Stimulation test
LH-RH
HCG Stimulation test
TRH
Dexamethasone T3 suppression test — Oral glucose tolerance test (Ergot-alkaloids)
(From Scriba et al., 1972.)

ENDOCRINOLOGY OF HYPOTHALAMUS AND PITUITARY GLAND information about the suprasellar extension of pituitary tumors .
Finally, suppression tests must briefly be mentioned (Table IV), as these are used in cases with hormonal overproduction (Fahlbusch, This Volume, pp . 90-95). Oral glucose tolerance tests suppress growth hormone secretion in normals and in chemical diabetes. In view of the multi-plicity of factors that st imulate growth ho rmone secretion (Scriba et al., 1972), and taking borderline cases into account , the G H suppression test by oral glucose loading is of impor tance in the diagnosis of acromegaly. Absent or paradoxical G H responses to the tests (oral glucose tolerance, arginine tolerance, insulin hypoglycemia) demonst ra te the functional au tonomy of growth hormone producing adenomata of the adenohypophysis . In general, these tests are of particular importance for the assessment of the success of therapeutic measures in cases of hormonally active tumors .
R E F E R E N C E S KAMBERI, I. A., MICAL, R. S. and PORTER, J. C. ( 1 9 7 1 ) : Hypophysial portal vessel infusion: in vivo
demonstration of LRF, FRF and PIF in pituitary stalk plasma. Endocrinology, 89, 1042 . LABHART, A. ( 1 9 7 1 ) : Klinik der inneren Sekretion, 2nd ed. Springer, Berlin-Heidelberg-New York. MAHONEY, J. H. and GOODMAN, A. D . ( 1 9 6 8 ) : Hypernatremia due to hypodipsia and elevated
threshold for Vasopressin release. Effects of treatment with hydrochlorothiazide, chlorpropamide and tolbutamide. New Engl. J. Med., 279, 1 1 9 1 .
MALARKEY, W . B., JACOBS, L. S. and DAUGHADAY, W . H. ( 1 9 7 1 ) : Levodopa suppression of prolactin in nonpuerperal galactorrhea. New Engl. J. Med., 285, 1 1 6 0 .
SCRIBA, P. C , VON WERDER, K . and SCHWARZ, K. (Eds) ( 1 9 7 3 ) : Hypothalamus und Hypophyse. In: Klinische Pathophysiologie, 2nd ed., p. 2 6 6 . Editor: W . Siegenthaler. Thieme, Stuttgart.
SOUVATZOGLOU, A., VON WERDER, K. and BOTTERMANN, P. ( 1 9 7 3 ) : The effect of intravenous L-dopa on GH and LH-levels in man. Acta endocr. (KbhJ, 73, 259.
TURKINGTON, R. W . , UNDERWOOD, L. E. and VAN WIK, J. J. ( 1 9 7 1 ) : Elevated serum prolactin levels after pituitary-stalk section in man. New Engl. J. Med., 285, 7 0 7 .
89