Embed Size (px)
Citation preview


Proceeding of a workshop held in Addis Ababa, EthiopiaNovember 15th to 17th, 2001
Edited by Andy Catley and Jeffrey Mariner

Contents
Summary i
Abbreviations ii
Acknowledgements ii
Introduction 1
Session 1
Overview of the origins, principles and methods of participatory epidemiology 2
Participatory Epidemiology: Setting the Scene 2Livestock Keeping and Indigenous Knowledge in the Horn of Africa:Personal reflections on 25 years experience 6
Session 2
Issues affecting the wider use of participatory epidemiology 10
Issue 1 - Qualitative versus quantitative methods 11Issue 2 - Methodological features of participatory inquiry 13Issue 3 - Training and learning in participatory epidemiology 16
Session 3
How can participatory epidemiology assist the Pan African Programme for the Control of Epizootics? 18
Participatory Disease Modelling 18Participatory Epidemiology and Disease Surveillance 18Experiences with assisting and quantifying disease surveillance information forsmall ruminants as obtained through the Nomadic Animal Health Auxilliary System(NAHA-System) in Central Rangelands of Somalia 19Disease surveillance and community-based animal health: experience of theOperation Lifeline Sudan Southern Sector Livestock Programme 22Participatory Disease Searching 23Participatory Epidemiology in Veterinary Research and Education 26
Session 4
National PACE Programme Working Groups 27
Tasks for Working Groups 27Presentations by Working Groups 27
1. Lessons learned during the workshop 272. Ways to use Participatory Epidemiology in National PACE Programmes 283. Training needs 30
Annex 1Workshop timetable 32
Annex 2List of participants 34
Annex 3Participants’ evaluation of the workshop 37
Partic ipatory Epidemiology: Lessons Learned and Future Directions

Summary
The Pan African Programme for the Control ofEpizootics (PACE) aims to complete the finaleradication of rinderpest from Africa and improvecontrol of other epizootics diseases such ascontagious bovine pleuropneumonia and footand mouth disease. Experience has shown thatdisease control is particularly problematic inmore remote arid and semi-arid areas inhabitedby pastoralist communities. In regions such asthe Horn of Africa, logistical and resourceconstraints are compounded by insecurity and insome cases, limited government presence.
Within the PACE Programme, the Community-based Animal Health and ParticipatoryEpidemiology (CAPE) Unit supports thedevelopment of primary-level veterinary servicesin pastoral areas. The focus is on privatised,community-based delivery systems that areenabled through appropriate policies andlegislation. CAPE also aims to complementconventional livestock disease investigation andsurveillance methods through the widerapplication of “participatory epidemiology” (PE).Participatory epidemiology has evolved from theprinciples and methods of Rapid Rural Appraisaland Participatory Rural Appraisal, and providesopportunities to make best use of pastoralists’considerable indigenous knowledge on animalhealth while also encouraging communityparticipation in disease control.
However, participatory approaches and methodsare not widely used by epidemiology units withinState Veterinary Services. This workshop wasorganised by the CAPE Unit to present recentdevelopments in PE to senior veterinarians,
academics and researchers in the Horn of AfricaRegion, and explore how PE might assist nationalPACE programmes to achieve their objectives.The workshop comprised a mix of presentations,discussion and working groups on key topics,and informal networking and exchange ofexperiences and ideas.
Recent developments in the use of PE byveterinarians with pastoralist communities in theregion included studies of the reliability andvalidity of participatory methods, and thedevelopment of a disease model for rinderpestbased on field data derived from PE. Theseexperiences were useful for showing how PE canbe combined with and complement conventionalepidemiological approaches.
The main outcomes of the workshop were:• Improved understanding of the potential roles
of PE in veterinary epidemiology• Raised awareness of important methodological
issues affecting best practice of PE• Widespread support for the wider use of PE in
national PACE programmes• Interest from veterinary schools for
incorporating PE into either undergraduate orpostgraduate teaching, and research activities
• Identification of PE training needs for veterinaryand livestock workers at central and field levels
During 2002, the CAPE Unit will follow up trainingneeds in national PACE programmes and supportteaching and research on PE in veterinary schoolsand research institutes. The contents of anintroductory training course on PE were presentedand discussed during the workshop.
iPartic ipatory Epidemiology: Lessons Learned and Future Directions
AbbreviationsASF African swine fever
CAHW Community-based Animal Health Worker
CAPE Unit Community-based Animal Health and Participatory Epidemiology Unit
CBPP contagious bovine pleuropneumonia
FMD foot and mouth disease
IIED International Institute for Environment and Development
ND Newcastle disease
OAU/IBAR Organization of African Unity/Interafrican Bureau for Animal Resources
PACE Pan African Programme for the Control of Epizootics
PARC Pan African Rinderpest Campaign
PAVE Participatory Approaches to Veterinary Epidemiology Project
PDS Participatory Disease Searching
PE Participatory Epidemiology
PRA Participatory Rural Appraisal
RVF Rift Valley fever
TOT Training of Trainers
Acknowledgements
The workshop Participatory Epidemiology: Lessons Learned and Future Directions was opened by Ato BelayEjigu, Vice Minister of Agriculture, Federal Democratic Republic of Ethiopia and Woizero Hadera Gebru, Head,Animal Resource and Fisheries Development Department.The workshop was made possible by funding from the Department for International Development (DFID),United Kingdom to the CAPE Unit, PACE Programme, OAU/IBAR.
The CAPE Unit gratefully acknowledges the assistance of Dr.Sileshi Zewde, National Coordinator, PACEEthiopia and communications staff from PACE Ethiopia. CAPE also appreciates the assistance of MaximilianBaumann (Freie University of Berlin), Berhanu Bedane (PACE Programme), Bryony Jones (VSF Belgium), JohnMcDermott (International Livestock Research Institute), Micheal Thrusfield (University of Edinburgh), TonyWilsmore (University of Reading) for assisting with facilitation of working group sessions.
ii Partic ipatory Epidemiology: Lessons Learned and Future Directions
Partic ipatory Epidemiology: Lessons Learned and Future Directions 1
Introduction
Background
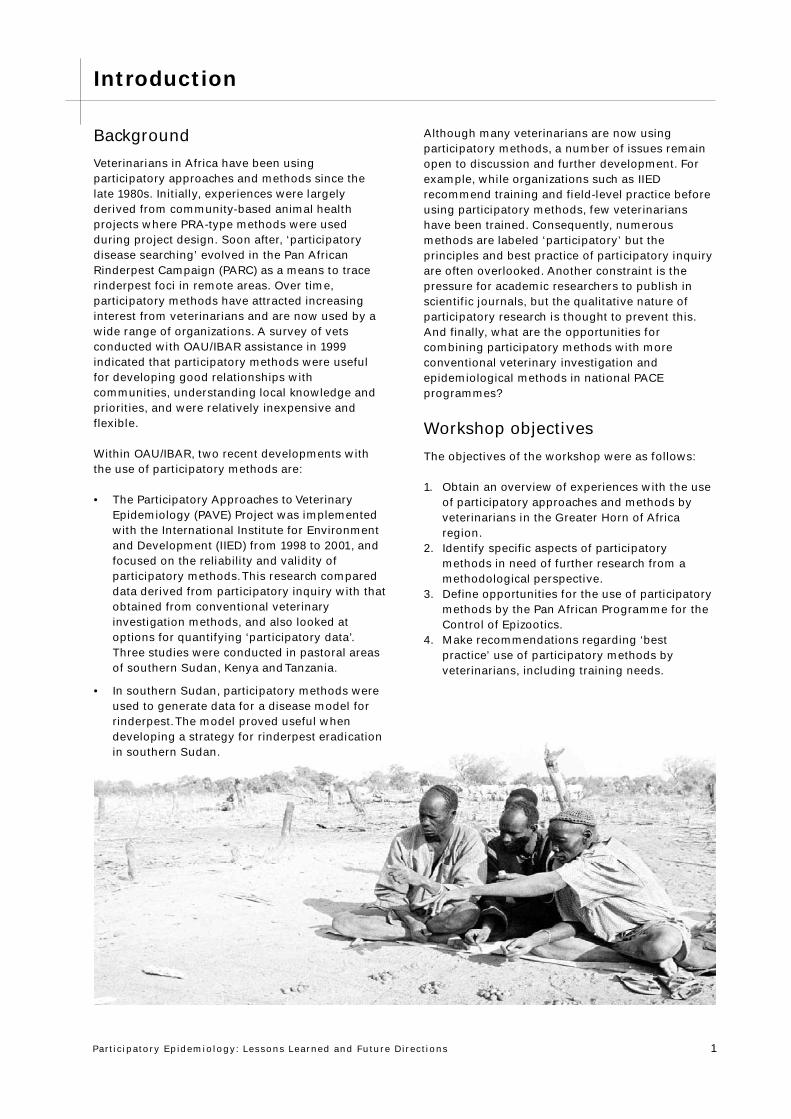
Veterinarians in Africa have been usingparticipatory approaches and methods since thelate 1980s. Initially, experiences were largelyderived from community-based animal healthprojects where PRA-type methods were usedduring project design. Soon after, ‘participatorydisease searching’ evolved in the Pan AfricanRinderpest Campaign (PARC) as a means to tracerinderpest foci in remote areas. Over time,participatory methods have attracted increasinginterest from veterinarians and are now used by awide range of organizations. A survey of vetsconducted with OAU/IBAR assistance in 1999indicated that participatory methods were usefulfor developing good relationships withcommunities, understanding local knowledge andpriorities, and were relatively inexpensive andflexible.
Within OAU/IBAR, two recent developments withthe use of participatory methods are:
• The Participatory Approaches to VeterinaryEpidemiology (PAVE) Project was implementedwith the International Institute for Environmentand Development (IIED) from 1998 to 2001, andfocused on the reliability and validity ofparticipatory methods. This research compareddata derived from participatory inquiry with thatobtained from conventional veterinaryinvestigation methods, and also looked atoptions for quantifying ‘participatory data’.Three studies were conducted in pastoral areasof southern Sudan, Kenya and Tanzania.
• In southern Sudan, participatory methods wereused to generate data for a disease model forrinderpest. The model proved useful whendeveloping a strategy for rinderpest eradicationin southern Sudan.
Although many veterinarians are now usingparticipatory methods, a number of issues remainopen to discussion and further development. Forexample, while organizations such as IIEDrecommend training and field-level practice beforeusing participatory methods, few veterinarianshave been trained. Consequently, numerousmethods are labeled ‘participatory’ but theprinciples and best practice of participatory inquiryare often overlooked. Another constraint is thepressure for academic researchers to publish inscientific journals, but the qualitative nature ofparticipatory research is thought to prevent this.And finally, what are the opportunities forcombining participatory methods with moreconventional veterinary investigation andepidemiological methods in national PACEprogrammes?
Workshop objectives
The objectives of the workshop were as follows:
1. Obtain an overview of experiences with the useof participatory approaches and methods byveterinarians in the Greater Horn of Africaregion.
2. Identify specific aspects of participatorymethods in need of further research from amethodological perspective.
3. Define opportunities for the use of participatorymethods by the Pan African Programme for theControl of Epizootics.
4. Make recommendations regarding ‘bestpractice’ use of participatory methods byveterinarians, including training needs.
Partic ipatory Epidemiology: Lessons Learned and Future Directions2
Jeffrey C. Mariner1, Andy Catley1, Darlington Akabwai1, Bryony Jones2
and Tim Leyland1
1Community-based Animal Health and Participatory Epidemiology(CAPE) Unit, Pan African Programme for the Control of Epizootics,Organization for African Unity/Interafrican Bureau for AnimalResources, PO Box 30786, 00100 Nairobi, Kenya2 Vétérinaires sans frontières - Belgium, PO Box 13986, Nairobi, Kenya
Introduction
Simply stated, participatory epidemiology is theapplication of participatory rural appraisaltechniques to the collection of epidemiologicinformation.
In the current era of globalisation, there is anincreasing demand for animal health information.Internationally, the Sanitary and Phyto-SanitaryAgreement of the Global Agreement on Tariffs andTrade established science-based methods as thebasis for livestock and livestock product tradedecision-making. Countries are now required toprovide data to substantiate their national animalhealth status relative to trade. This presents specialproblems for developing countries with remote andextensive agriculture systems. Remote andmarginalized livestock populations are under-represented in service delivery and informationsystems. As a result, these populations suffer fromthe direct lack of services and pose epidemiologicrisks to the national livestock population as awhole. The absence of current surveillanceinformation on the animal health status of remotepopulations adversely affects export trade.In the late 1980’s Tufts University developed athermostable vaccine against rinderpest and beganimplementation of a series of projects to introducethe use of the vaccine at both field and laboratorylevel as part of the OAU/IBAR Pan AfricanRinderpest Campaign (PARC). In the course of therinderpest eradication effort, the need foralternative animal health delivery systems forremote, marginalized communities becameapparent. This led to a programme of actionresearch on community-based animal healthdelivery systems that included rinderpest control ina variety of communities in East and Central Africa.Nearly simultaneously, a major community-basedanimal health programme was set in motion byTufts and Unicef to address the basic animal healthand rinderpest vaccination needs of the
communities affected by the complex emergency insouthern Sudan.
As part of the process of designing thesecommunity-based programmes, participatory ruralappraisal techniques were used to conduct needsassessments on animal health issues. The needsassessments focused on the following areas:• Animal health problems and priorities• Local veterinary knowledge and concepts
- Disease vectors, reservoirs,epidemiologic understanding
- Treatment• Appropriate interventions• Community structure, decision making and
entry points
This information was used to formulate projectsthat directly addressed the perceived needs of thecommunity through an appropriate combination ofconventional approaches, local knowledge andcommunity institutions. In the process, all thoseinvolved developed a tremendous respect for theextent of existing veterinary knowledge on thepresentation and patterns of disease. This led to theidentification of participatory epidemiology (PE) asan area of qualitative inquiry for furthermethodologic development and promotion as anappropriate technique for the rapid, effective, andeconomic collection of epidemiologic information.
Underlying concepts
Participatory approaches are founded on thephilosophy that empowering beneficiaries toidentify and overcome the challenges they arefacing is the surest route to achieving sustainabledevelopment. The basic requirements forpractitioners of participatory development are arespect for traditional knowledge, willingness tolearn, and attitude of open-mindedness. Theexperts that apply participatory methods all comewith technical educations and skills. The real valueof these educations is not in providing universalmodels for development but in providing the toolsto respond to new information in an innovative andconstructive manner.
Participatory rural appraisal (PRA) is a qualitativeintelligence gathering approach designed to rapidly
Overview of the origins, principles andmethods of participatory epidemiology
Session 1
Participatory Epidemiology: Setting the Scene
Partic ipatory Epidemiology: Lessons Learned and Future Directions 3
achieve a best-bet understanding of a situation as abasis for an action plan. It is a decision-orientedinformation collection and analysis process. Amulti-disciplinary team of experts usuallyimplements participatory rural appraisals. The PRAmethod provides a toolkit of techniques andactivities that facilitate the exchange ofinformation. The process is open-ended in that itallows the beneficiaries to provide direction to theinformation gathering process. This has beenreferred to as discovery and is based on theassumption that the appraisal team cannot andshould not assume that they can anticipate all theissues and information that is important tounderstanding the situation. The process isparticipatory since the informants actually benefitfrom the information collection process. First, thedata collection tools provide an opportunity forcommunity self-realization through bettervisualization of their life and livelihood situations.Secondly, the information obtained though PRA isinformation for action that should result ininterventions directly benefiting those whoprovided the data.
The participatory approach makes use of existingquantitative information and uses qualitativeintelligence to fill the gaps between available data.It is perhaps important to note that quantitativedata and the statistical methods used to analysequantitative data cannot establish casual relations.They merely establish the probability ofassociation between factors. It is in fact otherqualitative information that is used to determinecasual relationships and essential to the correctinterpretation of quantitative data.
In the developing world, the high cost, complexityand lack of flexibility associated with quantitativestudies has meant that the availability ofquantitative data is very limited. In fact, the veryscarcity of quantitative data implies that the datais not representative and has often meant that theinformation resulting from such studies ismisleading.
The method of sampling in PRA studies is basedon the principal of key informants rather thanrandomisation. The study actively seeksindividuals who are likely to have specializedknowledge or a uniquely informative perspectiveon the issues under study. In the case PE, thestudy team actively seeks out livestock ownersand traditional healers who are respected for theirability relative to animal health. Other types of keyinformants are traditional elders and communityleaders who are directly involved in decision-making processes and have some authority to
speak for the group. Finally, veterinaryprofessional, international experts and individualswith expert knowledge about the sociology of thegroups under study are frequently consulted.
The way qualitative data is assessed and validatedis fundamentally different from quantitative data.In the quantitative world, statistics are used tocalculate the probability that randomisedinformation and associations are valid. Validationin the qualitative approach is based on weighing ofevidence from diverse sources. This may includeinformation derived from quantitative orlaboratory-based testing. But PRA can make use ofbroader forms of experiential knowledge andinformation such as oral testimony andobservations from samples of non-random keyinformants.
The tools of participatory
epidemiology
Participatory epidemiology utilizes the PRA toolkitof methods. These methods may be grouped assecondary sources, direct observation, interviewtechniques, visualization techniques and methodsof ranking and scoring.

Partic ipatory Epidemiology: Lessons Learned and Future Directions4
Secondary sources
Secondary sources refer to existing literature,reports, maps and databases on the communitiesand issues under study. All good PRA studies beginwith an inventory of secondary sources and areview of these sources.
Direct observation
The techniques of direct observation refer toobserving the environment and daily activities oflivestock owners. One of simplest starting pointsis to get out and walk through the village orcattle camp and surrounding pasture. Observethe condition of the people, livestock, housingand pasture. Note what plants are present. Try tobe present for production activities like milkingand note who is carrying-out the tasks and howthey are completed.
Semi-structured interviews
One of the main tools of participatoryepidemiology is the semi-structured interview. Insemi-structured interviews, a checklist of subjectsto be covered is used as a point of reference ratherthan a questionnaire. The interview team makesuse of open-ended questions to allow participantsthe opportunity to introduce topics and issues. Forexample, after introductions, an opening questionmight be “What are the problems with yourlivestock?” As the participants introduce topics,probing questions are asked to obtain more detailand check information for internal consistency.
Visualisation techniques
The visualisation techniques include approachessuch as map, Venn diagram, timeline and seasonalcalendar construction. Mapping usually involvesclearing an area of sand and sketching with sticksthe relative location of key resource and strategiesused by the community. This includes things suchas grazing areas, cultivation areas, water sources,salt sources, woodlands, wild foods, wildlife,habitat of insect vectors of disease, friendly andunfriendly neighbours, trade routes, seasonalmovements, and emergency movements. Usingthis approach, the appraisal team can very quicklyobtain an overview of the area and the spatialdistribution of key resources. In epidemiology, thespatial relationship between communities, theirsocial relations and movement patterns go a longway towards determining livestock contact patternsand are key to understanding the epidemiology ofinfectious disease. Timelines and seasonalcalendars are very powerful tools for describingthe temporal patterns of disease in a location.
Ranking and scoring methods
Ranking and scoring refers to a group oftechniques used to prioritise information orprovide semi-quantitative estimates of the relativesize or impact of categories as perceived by theparticipants. In ranking, the respondents are askedto place items in their order of priority. Forexample, if 5 diseases have been mentioned asproblems, the interviewer requests that they belisted in order of importance. A more systematicalternative is pair-wise ranking where therespondents are asked to identify which is themore important disease of each possiblecombination of two diseases from the list.Proportional piling is very flexible technique inwhich respondents are asked to divide 100 objectssuch as seeds or stones into piles of sizesrepresenting the relative size or importance ofdifferent categories. The number of objects in eachpile is then counted to give a score. These exercisescan be repeated in subsequent interviews and theresults analysed statistically.

Partic ipatory Epidemiology: Lessons Learned and Future Directions 5
Data validation and analysis
In the process of data collection, the use ofprobing questions is an important quality controltool to assess the internal consistency of reports.Once a body of information is obtained from aseries of interviews and data collection exercises,the information can be assessed through theprocess of triangulation. The term triangulationsimply means comparing information obtainedfrom multiple informants and multiple methodsto look for patterns. If the information suggests auniform conclusion then the interpretation isrelatively straightforward. Occasionally, differentgroups of key informants may provide conflictinginformation. The study team must then considerhow the differing perspectives of the informantsimpact the information obtained.
An important advantage of PE that provides ahigh degree of flexibility is iterative analysis. Asthe data is gathered, the study team can reviewthe information available and refine the studyhypotheses. They have the opportunity to includenew questions or data collection exercises as aresult of information discovered during the PRAprocess. A further form of analysis isparticipatory analysis. Once the study team feelsthey have a reasonable best-bet scenario thatdescribes the situation, they can present thatscenario back to the participants. The participantscan then add, subtract or clarify information inthe best-bet scenario.
Applications of participatory
epidemiology
As was mentioned in the introduction, PE was firstdeveloped as a project needs assessment tool. Ithas also found application in animal health projectmonitoring and evaluation. The techniques can beused to track changes in disease impact over timeas well as to collect the perceptions ofbeneficiaries and other stakeholders on the impactof the project, weaknesses and possible ways toimprove performance.
Perhaps more importantly, PE has importantapplications as an epidemiologic surveillance tool inits own right. Participatory epidemiology has beenadapted as a very successful method of targetedsurveillance for rinderpest. In fact, a few low costand relative sort-term PE studies have dramaticallyaltered the conventional wisdom regarding themechanisms of endemicity and spatial distributionof rinderpest in East Africa. This approach has beentermed participatory disease searching (PDS).
Participatory disease searching
In PDS, the disease search team is interested ininformation on a specific disease but takesprecautions not to communicate this interest torespondents. Questions are asked about generalanimal health concerns. If the target disease isidentified as a problem, probing questions can beasked about the target disease in combinationwith other subjects. The investigation seeks toestablish the history of the disease in acommunity and trace reports forwards andbackwards in time. Often, herders guide thedisease search team to active cases of diseasethat can then be confirmed by laboratorydiagnostic methods. An example of a form oftimeline, a bar chart illustrating rinderpestreports by from Somali herders, is presented inFigure 1. Note that Figure 1 illustrates theprincipal of triangulation. All the availableindependent reports form a coherent pattern withan inter-epidemic period of about 5 years.
Another promising application of PE is in thegeneral disease surveillance. Community-basedanimal health programmes are in place in anumber of countries and in some countries morethan one thousand community-based animalhealth workers (CAHWs) are active. Theseprogrammes are important animal healthinformation networks. Programme monitorsdebrief and re-supply CAHWs on a more or lessmonthly basis. The CAHWs are aware of majordisease outbreaks and are a source ofinformation about trends in endemic disease.Several appropriate techniques of samplecollection such as dried blood on filter paperhave been developed for both serological andgenetic analysis. At present national diseasesurveillance systems have yet to create aframework to adequately utilize this importantand sensitive source of disease information.
Efforts are now underway to combineparticipatory epidemiological approaches withmore conventional forms of analyticalepidemiology. To this end, the Community-basedAnimal Health and Participatory Epidemiology(CAPE) Unit has been supporting the use of PE asa method of collecting expert opinion for use ininfectious disease modelling. Also, studies havebeen completed by the PAVE Project to validateexisting veterinary knowledge as a form ofepidemiologic data. The results of this worksuggest that combinations of both participatoryand analytic techniques yield an extremelypowerful approach to the study of epidemiology.

Partic ipatory Epidemiology: Lessons Learned and Future Directions6
Darlington AkabwaiCommunity-based Animal Health and ParticipatoryEpidemiology (CAPE) Unit, Pan African Programme for theControl of Epizootics, Organization for African Unity/Interafrican Bureau for Animal Resources, PO Box 30786,00100 Nairobi, Kenya
This paper focuses on one aspect ofpastoralists - the ethnoveterinary knowledge(EVK) which has enabled them to scrape aliving from a climatically hostile ecosystem forages. The vehicle of survival has mainly beenlivestock keeping and the accumulatedquantum of traditional knowledge is based onthis livelihood. The paper goes on to highlightsspecific examples of EVK that pastoralists haveacquired from time immemorial andrecommends that veterinary epidemiologistsopen their attitudes in order to tap this EVKfrom pastoralists. This is particularly importantduring the last stages of rinderpest diseasecontrol and that is at the surveillance anddisease search stages.
Introduction
The Horn of Africa is home to around 20 millionpastoralists. In general, pastoralists’ areas areplaces with unique characteristics that haveproduced unique constraints among itsinhabitants (see Box opposite). It is theseconstraints that have hardened the inhabitantsof these areas to withstand the rigors of harshenvironmental conditions. When outsiderscome to the Horn they are bound to complainof the harsh climate and wonder how theinhabitants can live with their livestock quitecomfortably. In contrast, the real pastoralistfinds everything normal because he or she hasknown no other environment since childhood.They have accumulated vast traditionalknowledge and experience on the tactics ofsurvival in these environments. That is whypastoralists are experts on issues of livestockkeeping in their environments. To them,livestock keeping is the most reliable livelihoodas it offers them the most successful copingstrategies for survival. It is howeverunfortunate that most outsiders coming to thepastoral areas are not aware of the existence ofsuch EVK among pastoralists. Some veterinaryepidemiologists belong to this category.
The unique characteristics of the pastoralists areas
1. Harsh climate and rugged topography.
2. Remote, largely inaccessible by road anddistant from public-and private-sectorcentralized services.
3. Movement in search of pasture and water iskey to survival (satellite camps or kraals atAwi ; home site - Ere)
4. The pastoralists are often branded “unwillingto change” but they cannot afford the luxuryof experiments offered by the outsiders.
5. Maintain traditional structures, - pillars ofdecision-making.
6. They have complex decision makingprocesses
7. Suffer from colonial and post colonialisolation - marginalization
8. Still hanging on dependency syndrome ofhandouts and this has slowed downprivatization efforts.
9. Insecurity due to civil conflict and the deadlycross-border raids.
The weakness of veterinary
epidemiology in pastoralists areas
As noted above, many veterinary epidemiologistsare not aware that pastoralists are well equippedwith very valuable EVK and are unwilling to learnfrom these local experts. There are many reasonsfor this lack of awareness, but the most obvious isthat they have not been formally trained in theirinstitutions of learning about the pastoralists andtheir unique EVK. Worse still, they have not hadany opportunity to learn it themselves in the fieldsince most of them are not willing as pointedabove. The question is why have they not taken thetrouble to tap this knowledge among pastoralistsand yet these livestock owners are so vital in theepidemiology and the eradication of livestockdiseases in the Horn of Africa?
• One obvious reason is that most veterinaryprofessionals come from outside thepastoralists’ areas and they are therefore notkeen to come closer to the pastoralists. Theygenerally have negative attitudes towards thesepeople.
• The other reason is that veterinaryepidemiologists are trained to work with
Livestock keeping and indigenous knowledge in theHorn of Africa: Personal reflections on 25 yearsexperience

Partic ipatory Epidemiology: Lessons Learned and Future Directions 7
sedentary herds using conventional approaches.They cannot accommodate the dynamics ofpastoralists’ areas and lack the inherentflexibility required to work in such areas.
• The veterinarians cannot therefore reach thetraditional knowledge system (EVK) that isembedded in the cultural matrix of thesepeople.
• These factors have contributed to the poorperformance of veterinary service delivery inthese unique areas, thus exacerbating themarginalization of the pastoralists.
These factors will continue to impact negatively onthe surveillance stage of disease control programs.
Ethnoveterinary knowledge among
pastoralists: some examples
Wherever they exist in Africa, pastoralists have triedto devise ways of living in harmony with their harshenvironment. Broadly speaking these ways are manyand diverse, and continue to be changed with timeand with new challenges. A few examples of thesetraditional knowledge systems are given below.
Expert knowledge on range ecology
Pastoralists have learnt how to manage their fragileecosystem. Despite the fact that they have beenaccused of causing widespread overgrazing andmismanagement of their production system, theyare pleading innocence until proven guilty. This isbecause they are very knowledgeable about theirland forms, soil and pasture types, and they knowthe capacities of their wells and most of thewatering points. Knowledge about salty pastures,red or black soils found in rolling plains or at theshoulders of hills are examples of their ability toclosely observe their ecosystems. In addition,pastoralists have designed grazing patterns thattake into account the production capacity and thedynamics of their ecosystem for any given season.
One of the elements of a grazing pattern ismovement. To a pastoralist and contrary to popularbelief, nomadism is not haphazard but is acalculated response to cope up with hostilechanges in one part of the grazing areas. It is asurvival coping strategy that has developed withtime. In the final analysis they are capable ofmanaging their production system withoutdamaging it. In fact, they accuse outsiders as themain cause of environmental degradation inpastoral areas. Pastoralists have devised evenseasonal calendars for specific areas and use thestars to tell the beginning and end of a season. In
addition, stars help them to foretell the severity ofan impending drought!
Experts in obstetrics and animal reproduction
The most valued item in livestock keeping amongpastoralists is milk. Pastoralists begin talking aboutmilk the very day a cow is serviced by a bull. Theyknow the pregnancy periods of all their domesticanimals and they take care to monitor the days ofpregnancy for each cow or camel. For example, aTurkana pastoralist knows that the gestation periodfor a camel is thirteen lunar months. He knows thisfrom years of patient observation. And to makesure he does not forget when to start getting milk,each month that passes is recorded with a linedrawn on the head stool until the thirteen lunarmonths have passed and the pregnant camelcalves down.
Correcting cases of infertility
The reproductive capacity of any given animal isobserved with keenness. For instance theanoestrus cows are taken to salty pastures forgrazing. To a Turkana pastoralist, the salty grass willreplace the missing salt and minerals which couldinclude the phosphates. Pastoralists report positiveresponses as most of the cows returning fromakicuar (meaning to quench the thirst for salt)actually come back pregnant. Some pastoralistsalso perform a surgery on the clitoris of heifersthat have failed to become pregnant. When the tipof the clitoris is cut off slightly, the heifer isstimulated and eventually gets pregnant whenserved. It is not known as yet what happens but itis popular management of heifer infertility amongmost pastoralists.
Assisting calvings
All pastoralist know in one way or the other to helptheir cows to calve down. But at the same timethere are people whom each community recognizesas the experts in handling the most difficultobstetrical cases. These are often consulted using atraditional fee.
Ability to communicate clearly
Most pastoralists are good orators but in any tree-of-men (Ekitoengikiliok in Turkana; Kokwo in Pokot)there are always expert communicators that thecommunity has recognized as talented orators.These are the people who will be given theresponsibility of repeating the discussion that goeson in the tree-of-men so that everybody will get themessage clear and loud. This is a traditional skillwhich is unique to pastoralist communities andshould be taken seriously by outsiders attemptingto work with these communities.

Partic ipatory Epidemiology: Lessons Learned and Future Directions8
Knowledge about pastoralist home economics
It is the pastoral woman who is the authority whenit comes to the matters of food production in apastoralists household. She has acquired the skillsof an ant that gathers and stores during times ofplenty to be used when things go bad. For instancemost pastoralist women are skillful in drying milkduring the wet season when there is surplusproduction. That powdered milk will be fed onmainly children when the drought becomes severe.Similarly some milk is cooked into ghee for uselater. The desert fruits are also dried for the samepurpose. The Somali women are particularly wellknown for preserving camel meat into nyirinyir(minced paste). It is a delicacy for Somali men andit adds love for his wife.
Livestock disease perceptions and etymology
among pastoralists
A few examples are given to illustrate the livestockdisease perception and etymology as given byvarious pastoral groups.
Blackquarter
This is a livestock disease that is recognized andaccurately described by most pastoralists andagro-pastoralists. The Turkana pastoralists, call itlokichuma which literally means ‘piercing pain’(from akicum meaning ‘to pierce’). Thedescription was borrowed from human feelingsas the Turkana pastoralist watched, with imaginedpain, the limping of the sick cow. The Fulani ofCameroon call this disease labba meaning the‘Devil’s spear’. The Fulani believe that the lesionwhich causes the sick animal to limp came as aresult of the animal being pierced by the Devil’sspear which pierces the heavy muscles withoutphysically cutting the hide. Similarly the Afar ofEthiopia name this disease harraymude whereharra means ‘forequarter’ and mude means ‘topierce or to spear’.
Rinderpest
Rinderpest is a livestock disease that can causevery high mortality. The disease is endemic inspecific inaccessible pastoralist areas in the sub-Saharan Africa. The names given to rinderpest bythe various cattle keeping communities tell veryvivid stories that can be very effective tools forawareness creation.
The Turkana give the traditional name forrinderpest as lokiyo or loleeo. The two names werederived by the Turkana pastoralists as follows.Ngakiyo in English means ‘tears’ and lokiyodenotes a livestock disease manifested by copious
lacrimation and nasal discharges, involving verymany cattle in herd and easily spreads to otherneighboring herds in an outbreak fashion. It is thewidespread lacrimation signaling a catastrophicepisode or plague that stimulated the coinage ofthe name. The plague often involved not only cattlebut even buffalo herds. In this case, when herdersnotice emaciated buffaloes they move their cattleaway to avoid the disease. Loleeo is borrowed fromtheir neighbours, the Karamojong, where that wordmeans ‘malicious’. The Turkana use the word todescribe a unique type of pipe-stem diarrhoeawhich is watery and greenish brown.
The Fulani of Cameroon call rinderpest pettuwhich they like to a strong wind that destroys a lotof fruits when it passes through a laden mango orapple tree. The picture paints rinderpest as beingcapable of blowing through cattle herds, leavingthem dead. The Afar of Ethiopia, call rinderpestdegahabe which means ‘empty kraal’ - it comesfrom the expression geso foyas habe which means‘the kraal of cattle is empty’.
The Dinker Rek and Dinker Boor of southern Sudancall rinderpest awet or nyan tek. The word awetcomes from wet piny, which in Dinka Rek means toscatter down like a hen that scatters the sorghumgrain when it is fed in a container. The older Dinkacompared this observation to a disease, whichscatters down cattle. The Dinka Bor called it nyantek meaning ‘one calf remains’. This indicates themanner in which rinderpest kills all the cattle,leaving only one or a few animals to becomeimmune to the disease.
The Latuko of southern Sudan give to rinderpestthe name lopirit. This is derived from the wordpirit, referring to the speed at which a fluid isemitted. When the expression is used to describea disease in cattle, it refers to projectile emissionof watery faeces.
All the above people are aware of the presence ofmodern vaccines and admit that they have notreatment of their own. However, they do havesophisticated quarantine procedures, which theyput into effect during outbreaks.
Trypanosomiasis
The disease is common in many pastoral and agro-pastrol areas. The main vector being the tsetse flythough biting flies contribute by mechanicaltransmission. This protozoan disease affects alldomestic animal but the examples given here aremainly from cattle.
The Turkana of Kenya and the Toposa of southernSudan call trypanosomiasis in cattle lokipi. Thename comes from ngakipi which means ‘water’. This

Partic ipatory Epidemiology: Lessons Learned and Future Directions 9
word describes the disease of cattle which ischaracterized by widespread oedema in the body ofthe affected animal, during the final stage of awasting condition. The carcass literally quenchesfire and releases a lot of smoke when roasted.
The Didinga and Latuko of southern Sudan calltrypanosomiasis lobi. The word lobi in the twotribal groups describes gradual loss of bodycondition of the affected cow. The disease isspread by the tsetse fly (called lolir in LatukoI andikirongit in Didinga).
The Nuer of southern Sudan call trypanosomiasisliey/guaw and they derive these two names from liymeaning stealing slowly, like something is secretlyremoving something from inside the animal whichbecomes thin. Guaw is a cattle diseasecharacterized by gradual loss of condition, periodicfever, sunken eyes, lacrimation and photophobia.Frequently these animals seek shade and have hairloss in from their tails.
In nearly all cases the pastoralists have beenexposed to modern trypanocidal drugs, such asethidium bromide. They associate the effectivenessof these modern drugs with their local terms fortrypanosomiasis , thus indicating they are correctin their diagnosis. There is some evidence that thelocal names which describe wasting diseases (e.g.in southern Sudan) may in fact be a combination ofseveral diseases such as combined infection ofliver fluke with trypanosomiasis.
Disease diagnosis and use of traditional remedies
These few examples of livestock diseaseperceptions by the pastoralists show thatpastoralists are very good in diagnosing livestockdisease entities in their traditional way. In fact,when discussing the Turkana classification oflivestock diseases Ohta (1984) stated that “Theyclassify the conspicuous uncommonness visible onthe animal”. In other words the Turkana identifywhat they believe are defining symptoms andname the disease accordingly. It is after diagnosingthat they indicate traditional remedies for thesedisease entities. All pastoral groups in sub-saharanAfrica express this ability with pride.
In both East and West Africa traditional medicationsare well known and discussed freely. For instancethe Fulani known as the WodaBee in Niger and theTaureg in Niger are skillful in vaccinating theircattle against contagious bovine pleuralpneumonia (CBPP) by placing a piece of infectedlung from a cow that has died of CBPP into a foldof slit skin on the side of the nose of cattle to bevaccinated (Stem, 1996).
Conclusions
As indicated above, pastoralists have accumulateda vast amount of traditional knowledge that hasenabled them to utilize livestock keeping as a viablelivelihood. It is now up to us to open ourselves totap this EVK in order to enrich modernepidemiology. This will entail a complete change ofattitudes on our side as professionals and a movecloser to the grassroots where the custodians of thatknowledge reside. It means we have to reseek thepeople, accept nomadism as a coping strategy forsurvival rather than viewed it as unnecessaryloitering by those people, that we become flexibleand broad minded instead of being the rigidveterinarians that we have been accused of, and thatwe should be prepared to learn the livestock diseaseperceptions of the livestock owners and the waydisease names are derived from the socio-culturalbackgrounds. This is particularly important at thelast stages of rinderpest disease control and that isat the surveillance and disease search stages.Pastoralists ability to identify and describeaccurately the livestock diseases will be a real asset.This is because this people will hardly miss a case!
Bibliography
Catley, A., Leyland, T., 2001. Community participation and thedelivery of veterinary services in Africa. PreventiveVeterinary Medicine 49, 95-113.Grandin, B., 1986. Wealth ranking in small holder communities: afield manual. ITDG Publications, London.Ohta, I., 1984. Symptoms are classified into diagnosticcategories: Turkana’s view of livestock disease. AfricanMonographs supplementary issues 3, 71-93.Katabarwa, N.M., Richards, Jr. F.O., Ndyomugenyi R., 2000. Inrural Ugandan communities the traditional kinship/clansystem is vital to the success and sustainment of the AfricanProgram for Onchocerciasis Control. Annals of Tropical Medicineand Parasitology, 94(5), 485-495.Mariner, J.C., 2001. Report of the Consultancy to Assist in theDevelopment of a Rinderpest Eradication Strategy in theWest and East Nile Ecosystems. Community-based AnimalHealth and Epidemiology (CAPE) Unit, Pan African Programme forthe Control of Epizootics (PACE), Nairobi.Oba Gufu, 1985. Perception of Environment among KenyanPastoralists: Implications for Development. Nomadic Peoples,19, 33-57Prior, J., 1994. Pastoral Development Planning. Oxfam DevelopmentGuidelines No. 9, Oxfam Publications, Oxford.Sollod, A.E., Stem, C., 1991. Appropriate animal health informationsystems for nomadic and trans-humant livestock populations inAfrica. Rev. sci. tech. Off. Int. Epiz., 10(1), 89-101.Stem, C., 1996. Ethnoveterinary Research in a LivestockDevelopment Context. In: Ethnoveterinary Research andDevelopment. (pp.193-206). McCorkle, Constance M. and EvelynMathias-Mundy eds. Intermediate Technology Publications. 1996.Stem, C., Sollod, E.A., 1994. Rapid reconnaissance in animalhealth planning for pastoral production systems. KenyaVeterinarian. 18 (2) 51-54. August 1994. Proceedings of the7th International Symposium on Veterinary Epidemiology andEconomics, Nairobi, August 1994.UNICEF, 1996, A study on the Ethno-Veterinary Knowledge ofthe Dinka and Nuer in Southern Sudan. Operation LifelineSudan - Livestock Programme. UNICEF-OLS, Nairobi.
Partic ipatory Epidemiology: Lessons Learned and Future Directions10
Andy CatleyCommunity-based Animal Health and ParticipatoryEpidemiology (CAPE) Unit, Pan African Programme for theControl of Epizootics, Organization for African Unity/Interafrican Bureau for Animal Resources, PO Box 30786,00100 Nairobi, Kenya
Introduction
This session was introduced by reference to asurvey of veterinary uses of participatory appraisalin Africa conducted in 1998-19991. The survey targeted veterinarians and used aquestionnaire to assess:
• Understanding of participatory approaches andmethods
Session 2
Issues affecting the wider use ofparticipatory epidemiology
• Veterinary uses of participatory methods• Perceptions on strengths and weaknesses of
participatory methods
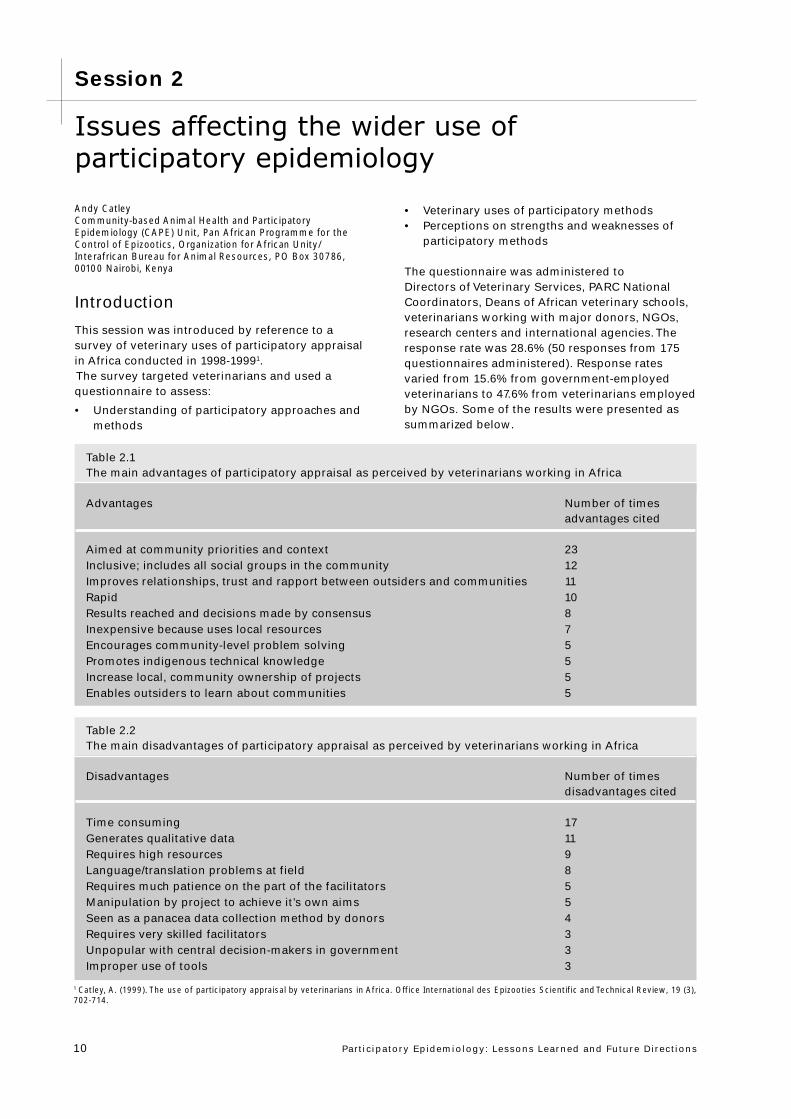
The questionnaire was administered toDirectors of Veterinary Services, PARC NationalCoordinators, Deans of African veterinary schools,veterinarians working with major donors, NGOs,research centers and international agencies. Theresponse rate was 28.6% (50 responses from 175questionnaires administered). Response ratesvaried from 15.6% from government-employedveterinarians to 47.6% from veterinarians employedby NGOs. Some of the results were presented assummarized below.
Table 2.1The main advantages of participatory appraisal as perceived by veterinarians working in Africa
Advantages Number of timesadvantages cited
Aimed at community priorities and context 23Inclusive; includes all social groups in the community 12Improves relationships, trust and rapport between outsiders and communities 11Rapid 10Results reached and decisions made by consensus 8Inexpensive because uses local resources 7Encourages community-level problem solving 5Promotes indigenous technical knowledge 5Increase local, community ownership of projects 5Enables outsiders to learn about communities 5
Table 2.2The main disadvantages of participatory appraisal as perceived by veterinarians working in Africa
Disadvantages Number of timesdisadvantages cited
Time consuming 17Generates qualitative data 11Requires high resources 9Language/translation problems at field 8Requires much patience on the part of the facilitators 5Manipulation by project to achieve it’s own aims 5Seen as a panacea data collection method by donors 4Requires very skilled facilitators 3Unpopular with central decision-makers in government 3Improper use of tools 3
1 Catley, A. (1999). The use of participatory appraisal by veterinarians in Africa. Office International des Epizooties Scientific and Technical Review, 19 (3),702-714.
Partic ipatory Epidemiology: Lessons Learned and Future Directions 11
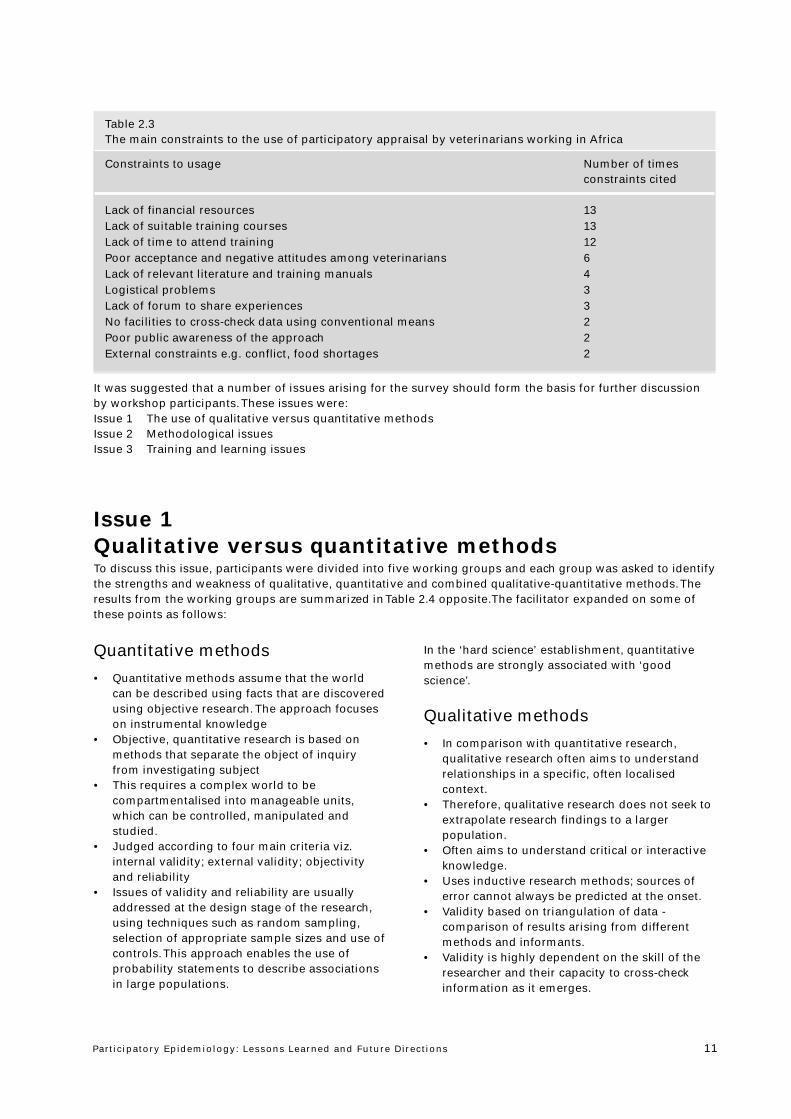
It was suggested that a number of issues arising for the survey should form the basis for further discussionby workshop participants. These issues were:Issue 1 The use of qualitative versus quantitative methodsIssue 2 Methodological issuesIssue 3 Training and learning issues
Table 2.3The main constraints to the use of participatory appraisal by veterinarians working in Africa
Constraints to usage Number of timesconstraints cited
Lack of financial resources 13Lack of suitable training courses 13Lack of time to attend training 12Poor acceptance and negative attitudes among veterinarians 6Lack of relevant literature and training manuals 4Logistical problems 3Lack of forum to share experiences 3No facilities to cross-check data using conventional means 2Poor public awareness of the approach 2External constraints e.g. conflict, food shortages 2
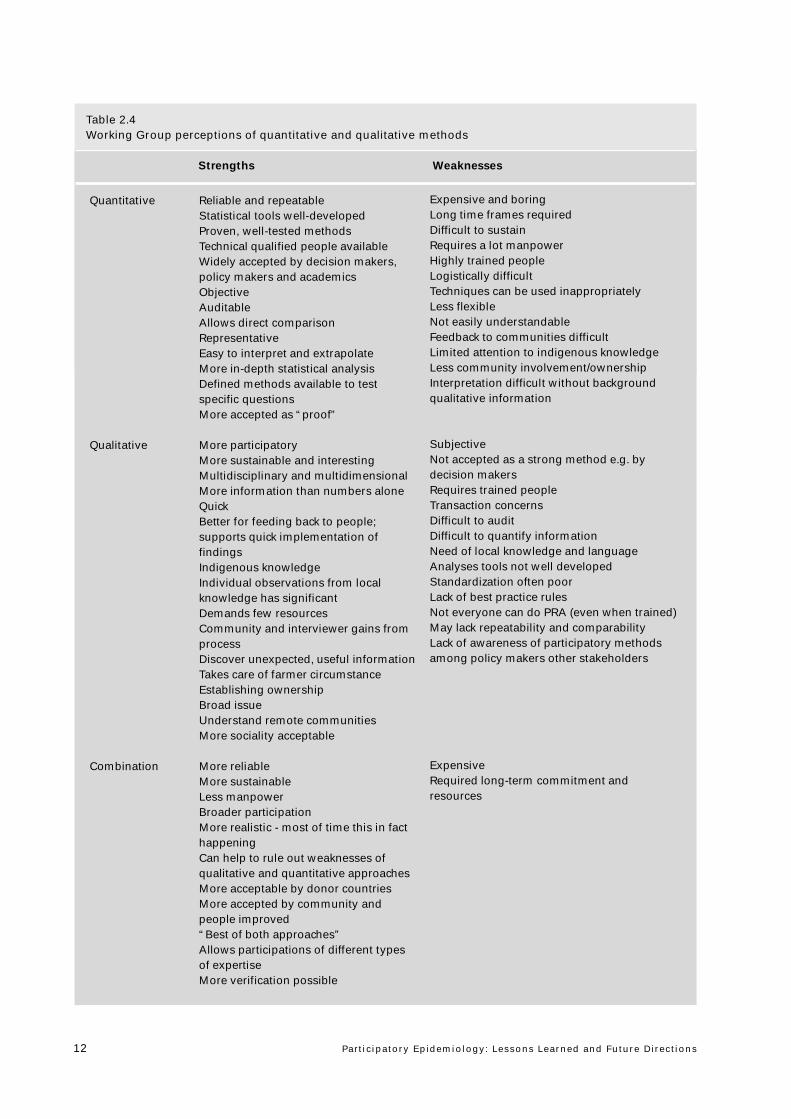
Issue 1Qualitative versus quantitative methodsTo discuss this issue, participants were divided into five working groups and each group was asked to identifythe strengths and weakness of qualitative, quantitative and combined qualitative-quantitative methods. Theresults from the working groups are summarized in Table 2.4 opposite.The facilitator expanded on some ofthese points as follows:
Quantitative methods
• Quantitative methods assume that the worldcan be described using facts that are discoveredusing objective research. The approach focuseson instrumental knowledge
• Objective, quantitative research is based onmethods that separate the object of inquiryfrom investigating subject
• This requires a complex world to becompartmentalised into manageable units,which can be controlled, manipulated andstudied.
• Judged according to four main criteria viz.internal validity; external validity; objectivityand reliability
• Issues of validity and reliability are usuallyaddressed at the design stage of the research,using techniques such as random sampling,selection of appropriate sample sizes and use ofcontrols. This approach enables the use ofprobability statements to describe associationsin large populations.
In the ‘hard science’ establishment, quantitativemethods are strongly associated with ‘goodscience’.
Qualitative methods
• In comparison with quantitative research,qualitative research often aims to understandrelationships in a specific, often localisedcontext.
• Therefore, qualitative research does not seek toextrapolate research findings to a largerpopulation.
• Often aims to understand critical or interactiveknowledge.
• Uses inductive research methods; sources oferror cannot always be predicted at the onset.
• Validity based on triangulation of data -comparison of results arising from differentmethods and informants.
• Validity is highly dependent on the skill of theresearcher and their capacity to cross-checkinformation as it emerges.
Partic ipatory Epidemiology: Lessons Learned and Future Directions12
Table 2.4Working Group perceptions of quantitative and qualitative methods
Strengths Weaknesses
Expensive and boringLong time frames requiredDifficult to sustainRequires a lot manpowerHighly trained peopleLogistically difficultTechniques can be used inappropriatelyLess flexibleNot easily understandableFeedback to communities difficultLimited attention to indigenous knowledgeLess community involvement/ownershipInterpretation difficult without backgroundqualitative information
SubjectiveNot accepted as a strong method e.g. bydecision makersRequires trained peopleTransaction concernsDifficult to auditDifficult to quantify informationNeed of local knowledge and languageAnalyses tools not well developedStandardization often poorLack of best practice rulesNot everyone can do PRA (even when trained)May lack repeatability and comparabilityLack of awareness of participatory methodsamong policy makers other stakeholders
ExpensiveRequired long-term commitment andresources
Reliable and repeatableStatistical tools well-developedProven, well-tested methodsTechnical qualified people availableWidely accepted by decision makers,policy makers and academicsObjectiveAuditableAllows direct comparisonRepresentativeEasy to interpret and extrapolateMore in-depth statistical analysisDefined methods available to testspecific questionsMore accepted as “proof”
More participatoryMore sustainable and interestingMultidisciplinary and multidimensionalMore information than numbers aloneQuickBetter for feeding back to people;supports quick implementation offindingsIndigenous knowledgeIndividual observations from localknowledge has significantDemands few resourcesCommunity and interviewer gains fromprocessDiscover unexpected, useful informationTakes care of farmer circumstanceEstablishing ownershipBroad issueUnderstand remote communitiesMore sociality acceptable
More reliableMore sustainableLess manpowerBroader participationMore realistic - most of time this in facthappeningCan help to rule out weaknesses ofqualitative and quantitative approachesMore acceptable by donor countriesMore accepted by community andpeople improved“Best of both approaches”Allows participations of different typesof expertiseMore verification possible
Quantitative
Qualitative
Combination
Partic ipatory Epidemiology: Lessons Learned and Future Directions 13
This session focused on three aspects ofparticipatory epidemiology which are commonlymisunderstood.
Confusion with questionnaires
Some workers consider the methods ofparticipatory epidemiology to be “just like aquestionnaire”. However, an important influenceon the development of participatory methods wasdissatisfaction with questionnaire surveys amongdevelopment workers. Questionnaires were oftendifficult to design and administer, and were basedon the priorities and perceptions of researchers,rather than local people. Although best-practiceguidelines for using questionnaires wereavailable, they were rarely followed. For example,pretesting of questionnaires was often overlookedand the problem of non-sampling errors wasusually ignored. Possible confusion over use oflanguage, particularly translation of technicalterms, was another issue.
In remote areas, pretesting of questionnaires canbe logistically difficult and time consuming.Similarly, after the administration ofquestionnaires and collection of data, the analysisis often conducted back in the laboratory or office.This means that if discrepancies or unusualinformation arises during the analysis, it isdifficult to verify the original data.
In part, participatory inquiry attempts to overcomesome of the problems of questionnaires. Typically,local priorities are discussed using local languageand disease terms. The overall approach is not toask standard questions to a set number of people,but to explore and analyse issues and follow-upinteresting leads. In other words, the approach isopen-ended and flexible.
Triangulation
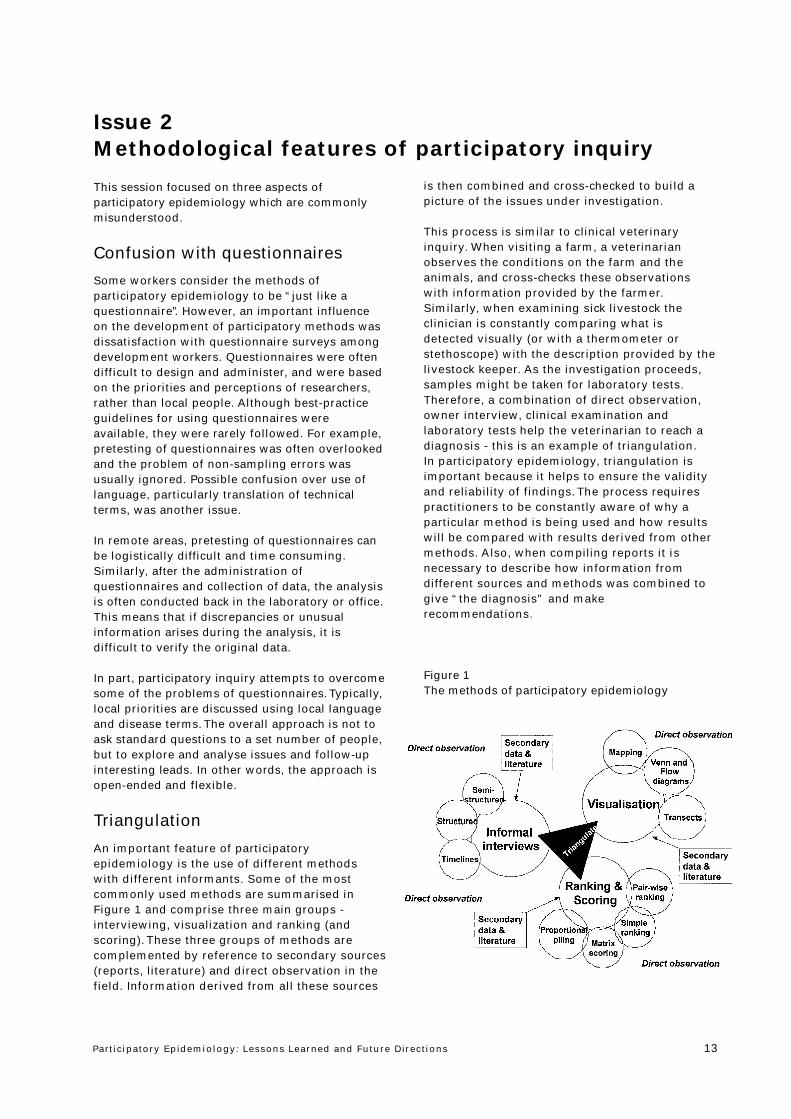
An important feature of participatoryepidemiology is the use of different methodswith different informants. Some of the mostcommonly used methods are summarised inFigure 1 and comprise three main groups -interviewing, visualization and ranking (andscoring). These three groups of methods arecomplemented by reference to secondary sources(reports, literature) and direct observation in thefield. Information derived from all these sources
is then combined and cross-checked to build apicture of the issues under investigation.
This process is similar to clinical veterinaryinquiry. When visiting a farm, a veterinarianobserves the conditions on the farm and theanimals, and cross-checks these observationswith information provided by the farmer.Similarly, when examining sick livestock theclinician is constantly comparing what isdetected visually (or with a thermometer orstethoscope) with the description provided by thelivestock keeper. As the investigation proceeds,samples might be taken for laboratory tests.Therefore, a combination of direct observation,owner interview, clinical examination andlaboratory tests help the veterinarian to reach adiagnosis - this is an example of triangulation.In participatory epidemiology, triangulation isimportant because it helps to ensure the validityand reliability of findings. The process requirespractitioners to be constantly aware of why aparticular method is being used and how resultswill be compared with results derived from othermethods. Also, when compiling reports it isnecessary to describe how information fromdifferent sources and methods was combined togive “the diagnosis” and makerecommendations.
Figure 1The methods of participatory epidemiology
Issue 2Methodological features of participatory inquiry
Partic ipatory Epidemiology: Lessons Learned and Future Directions14
“Participatory methods are
qualitative, so we can’t publish
the work”
While the qualitative nature of participatoryepidemiology is clearly a concern for manyveterinarians, it seems to be a particular problem foracademics and researchers. The perception seems tobe that unless research involves the collection ofnumerical data and presents some statisticalsummary or analysis, findings cannot be published injournals. When researchers are judged within a“publish or perish” culture, they favour conventionalmethods which are known and accepted by theirpeers and reviewers for scientific journals.
When considering this issue, two points were made:
• It is possible to describe many subjectiveopinions using numbers. For example, preferenceranking requires an informant to assign numericalranks to items or issues to demonstrate theirpreferences. In veterinary medicine, wecommonly use body condition scores tosummarise a subjective assessment of ananimal’s condition. Similarly, we can assign ranksor scores to lesions or clinical observations.
• By standardizing a ranking or scoring method,and then repeating the method, we producenumerical data that can be summarized usingcommon and simple statistical methods.
In participatory epidemiology, ranking and scoringmethods produce numerical data at an early stagein the method. Typically, within a particular surveythese methods have been used as ‘one-off’methods. For example, the results below show howone group of farmers ranked livestock diseases interms of morbidity and mortality2.
Scoring of livestock diseases in Abela Sipa,North Omo, Ethiopia
Disease Mortality Morbility
trypanosomiasis *****(5) *********(9)
anthrax ********(8) ****(4)
blackleg ********(8) ****(4)
ticks and tick-borne
disease **(2) *******(7)
internal parasites - (0) ********(8)
Note: A group of 12 male farmers were asked to score the fivemost important diseases in Abela Sipa peasant association out of
10, in terms of mortality and morbility.
Participatory methods such as proportional pilingcan be easily standardized to understand localperceptions of disease incidence.
Example
Use of proportional piling to estimate incidence of
cattle diseases in Tana River District, Kenya3
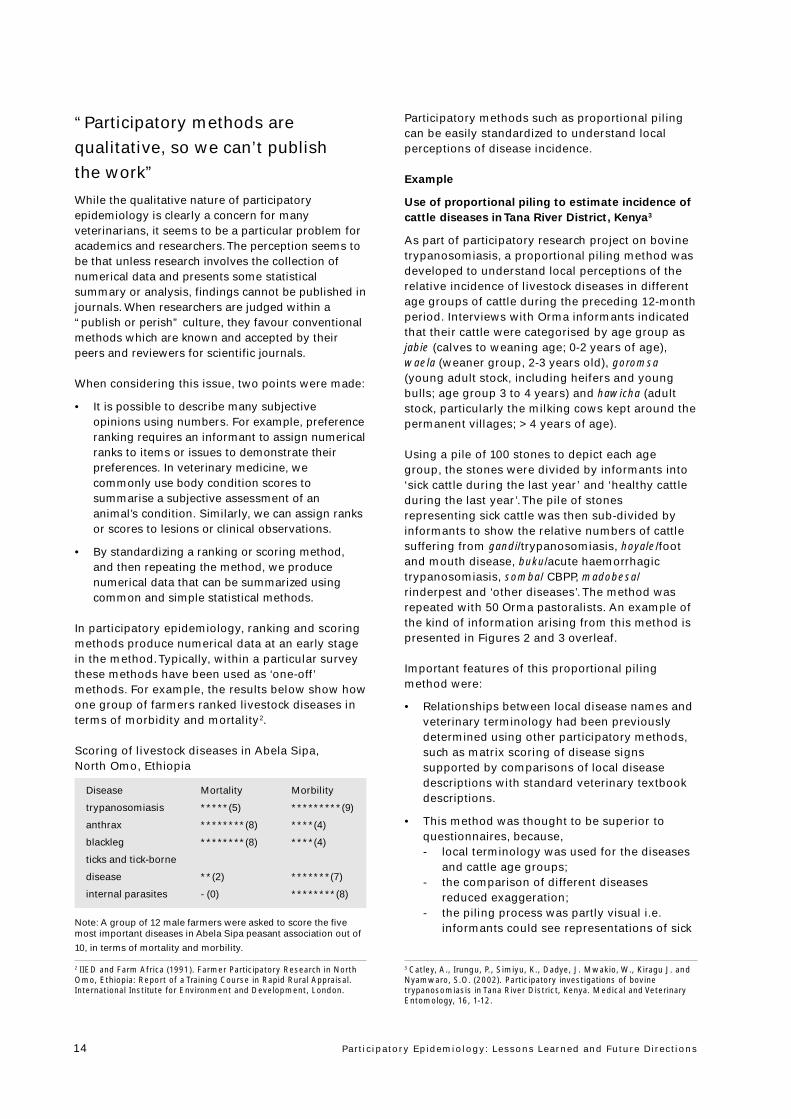
As part of participatory research project on bovinetrypanosomiasis, a proportional piling method wasdeveloped to understand local perceptions of therelative incidence of livestock diseases in differentage groups of cattle during the preceding 12-monthperiod. Interviews with Orma informants indicatedthat their cattle were categorised by age group asjabie (calves to weaning age; 0-2 years of age),waela (weaner group, 2-3 years old), goromsa(young adult stock, including heifers and youngbulls; age group 3 to 4 years) and hawicha (adultstock, particularly the milking cows kept around thepermanent villages; > 4 years of age).
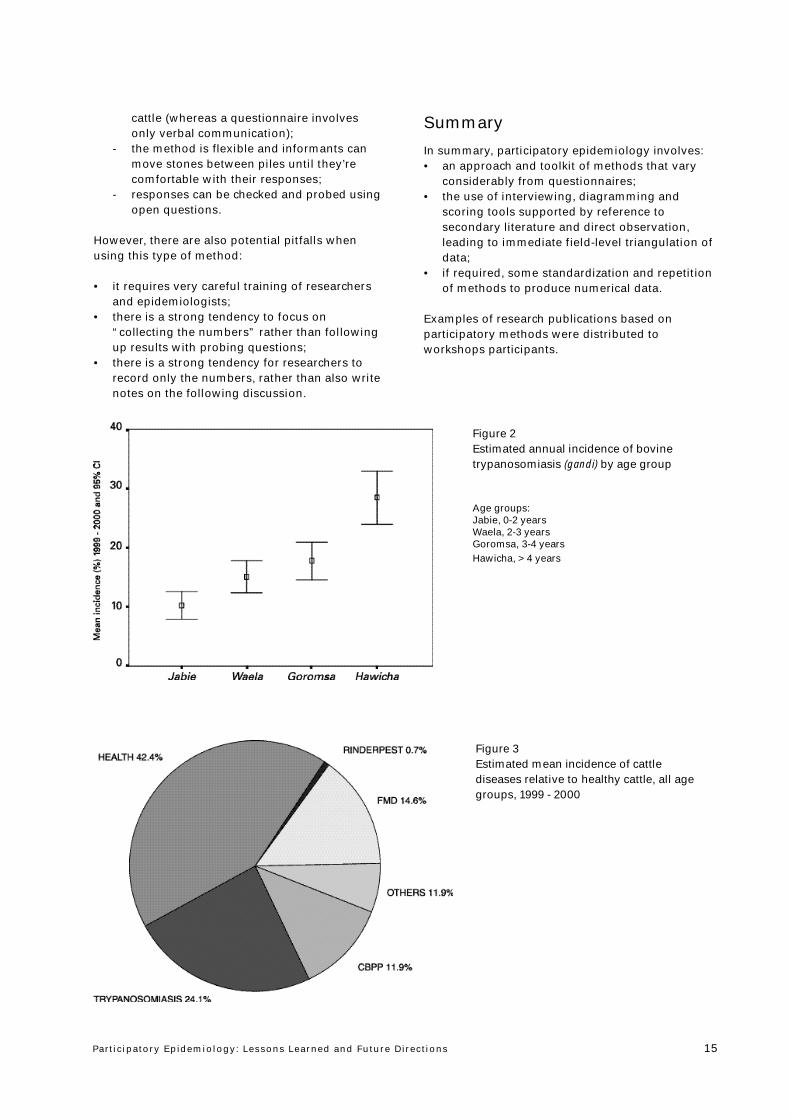
Using a pile of 100 stones to depict each agegroup, the stones were divided by informants into‘sick cattle during the last year’ and ‘healthy cattleduring the last year’. The pile of stonesrepresenting sick cattle was then sub-divided byinformants to show the relative numbers of cattlesuffering from gandi/trypanosomiasis, hoyale/footand mouth disease, buku/acute haemorrhagictrypanosomiasis, somba/ CBPP, madobesa/rinderpest and ‘other diseases’. The method wasrepeated with 50 Orma pastoralists. An example ofthe kind of information arising from this method ispresented in Figures 2 and 3 overleaf.
Important features of this proportional pilingmethod were:
• Relationships between local disease names andveterinary terminology had been previouslydetermined using other participatory methods,such as matrix scoring of disease signssupported by comparisons of local diseasedescriptions with standard veterinary textbookdescriptions.
• This method was thought to be superior toquestionnaires, because,- local terminology was used for the diseases
and cattle age groups;- the comparison of different diseases
reduced exaggeration;- the piling process was partly visual i.e.
informants could see representations of sick
2 IIED and Farm Africa (1991). Farmer Participatory Research in NorthOmo, Ethiopia: Report of a Training Course in Rapid Rural Appraisal.International Institute for Environment and Development, London.
3 Catley, A., Irungu, P., Simiyu, K., Dadye, J. Mwakio, W., Kiragu J. andNyamwaro, S.O. (2002). Participatory investigations of bovinetrypanosomiasis in Tana River District, Kenya. Medical and VeterinaryEntomology, 16, 1-12.
Partic ipatory Epidemiology: Lessons Learned and Future Directions 15
cattle (whereas a questionnaire involvesonly verbal communication);
- the method is flexible and informants canmove stones between piles until they’recomfortable with their responses;
- responses can be checked and probed usingopen questions.
However, there are also potential pitfalls whenusing this type of method:
• it requires very careful training of researchersand epidemiologists;
• there is a strong tendency to focus on“collecting the numbers” rather than followingup results with probing questions;
• there is a strong tendency for researchers torecord only the numbers, rather than also writenotes on the following discussion.
Summary
In summary, participatory epidemiology involves:• an approach and toolkit of methods that vary
considerably from questionnaires;• the use of interviewing, diagramming and
scoring tools supported by reference tosecondary literature and direct observation,leading to immediate field-level triangulation ofdata;
• if required, some standardization and repetitionof methods to produce numerical data.
Examples of research publications based onparticipatory methods were distributed toworkshops participants.
Figure 2Estimated annual incidence of bovinetrypanosomiasis (gandi) by age group
Age groups:Jabie, 0-2 yearsWaela, 2-3 yearsGoromsa, 3-4 yearsHawicha, > 4 years
Figure 3Estimated mean incidence of cattlediseases relative to healthy cattle, all agegroups, 1999 - 2000
Partic ipatory Epidemiology: Lessons Learned and Future Directions16
Training Courses
The rapid growth of RRA and PRA in developmentwork has been accompanied by the emergence ofnumerous training courses. These courses varyconsiderably in their content, trainingmethodology, duration and trainer experience.During the workshop, a training course inparticipatory epidemiology for veterinarians wasproposed based on the courses run by theInternational Institute for Environment andDevelopment and the Institute of DevelopmentStudies in the late 1980s and 1990s. These coursesincluded initial classroom-based sessions followedby field practice. The length of the courses wasaround 10 days.
Therefore, the proposed training course inparticipatory epidemiology comprised thefollowing sessions:
Outline of an Introductory Training Course in
Participatory Epidemiology
Session 1: Origins of participatory approaches and
methods
Farming Systems ResearchApplied AnthropologyAdult Education MovementAgroecosystem AnalysisRapid Rural Appraisal
Session 2: Concepts of community participation in
development
Historical background to community participationMeanings of community participationExamples of applications, uses and abuses
Session 3: “Rural Development Tourism”
Spatial bias
Temporal biasProject biasDiplomatic biasPerson biasProfessional bias
Session 4: Key features of participatory
epidemiology
Attitudes and behaviour of practitionersMixed methods- participatory and conventionalSecondary dataManaging groupsKey informantsTriangulationOptimal ignorance
Session 5: Methods - interviewing methods
Principles of informal interviewing
Use of open and probing questionsUse of checklists - written and mentalExamples from veterinary epidemiologyPractical sessions
Session 6: Visualisation methods - participatory
mapping
Priniciples of mappingTypes of maps (social, natural resource, movement etc.)Examples of maps used in epidemiologyPractical sessions
Session 7: Visualisation methods - Seasonal
Calendars
Principles and methodologiesExamples from epidemiologyPractical sessions
Session 8: Ranking and scoring methods
Principles of ranking and scoringTypes of ranking and scoringExamples from epidemiologyPractical sessions
Session 9: Summarising and analysing data
How to handle ranks and scoresStatistical tests for non parametric dataAssessing agreement between informantsMultidimensional scaling, GPA, correspondenceanalysis and other methods
Field practice: Five days in the field
This is crucial!Provides opportunity to practice methods andaddress any misunderstandingsSummarise and analyse data - in the fieldFeedback and cross-check findingsEvaluation of methodsWrite report
Who To Train?
It is often said that ‘not everyone can do PRA’. Infact, a growing body of experience in participatoryapproaches and methods in various technicalsectors shows how the attitudes and behaviour ofpractitioners is probably more important than theirknowledge about specific methods. This experienceindicates that certain types of people feel morecomfortable with PRA than others and are moresuccessful at applying the approach.
Issue 3Training and learning in participatory epidemiology

Partic ipatory Epidemiology: Lessons Learned and Future Directions 17
In order to prompt discussion on the characteristicsof a ‘good participatory epidemiologist’, JeffreyMariner introduced participants to the BriggsMyers Personality Type. This system helps tocharacterise people by personality type and is usedby various organizations to assign tasks to staffwith particular attributes.
At its most basic level, the Briggs Myers uses thefollowing characteristics:
Extrovert (E) Introvert (I)Sensing (S) intuition (N)Thinking (T) Feeling (F)Judging (J) Perceiving (P)
These characteristics are explored through a seriesof questions:
1. Where do you direct your energy?
- To the outer world of activity, and spoken words?- To the inner world of thought and emotions?
Characterisitics associated with extrovert versesintrovert people are as follows:
Extroversion Introversion
Social PrivateExpressive QuietMany FewBroad DeepInteraction ConcentrationOutward InwardAction before thought Thought before action
2. How do you process information?
- In the form of known facts and familiar terms?- In the form of possibilities or new potential?
Sensing Intuition
Facts PatternsExperience NoveltyPresent FuturePracticality AspirationEnjoyment DevelopmentRealism IdealismUsing Changing
3. How do you make decisions?
- On the basis of logic and objectiveconsiderations?
- On the basis of personal values?
Thinking Feeling
Analysing SympathisingObjective SubjectiveLogical PersonalCriticism AppreciationOnlooker ParticipantDecides on principle Decides using valuesLong term view Immediate view
4. How do you prefer to organise your life?
- In a structured way, making decisions andknowing where you stand?
- In a flexible way, discovering life as you goalong?
Judgement Perception
Close OpenDecide ExploreStructure MeanderOrganise InquireFirmness FlexibilityControl Spontaneity
Although there wasn’t enough time during theworkshop for a thorough discussion on thispersonality test, the key point was that differentpeople have different characteristics andbehaviours. For epidemiologists, some people areinstinctively more at ease when dealing withobjective data and ‘black and white’ situationswhereas other people seek to understand greyareas and can cope easily with uncertainty.Similarly, some researchers prefer the structure ofa pre-ordered learning process but others preferopen-ended inquiry and like to respond to newinformation as it arises.
Recognition of these kinds of attributes togetherwith communication skills can assist seniormanagers to identify staff who are most likely tobenefit from training in PE and apply theapproaches and methods effectively in the field.Such people are usually natural and relaxedcommunicators, observant of local customs andnorms, and respectful of other people’s views.

Partic ipatory Epidemiology: Lessons Learned and Future Directions18
Participatory DiseaseModellingJeffrey C. Mariner1, John McDermott2, Andy Catley1 and PeterRoeder3
1Community-based Animal Health and ParticipatoryEpidemiology (CAPE) Unit, Pan African Programme for theControl of Epizootics, Organization for African Unity/Interafrican Bureau for Animal Resources, PO Box 30786,00100 Nairobi, Kenya2International Livestock Research Institute, PO Box 30709,Nairobi, Kenya3Emergency Prevention System for Tranboundary Animal andPlants Pests and Diseases (EMPRES), Animal Health Service,Animal Production and Health Division, Food and AgricultureOrganization, Viale delle Terme di Caracalla, 00100 Rome. Italy.
Infectious disease modelling relies uponquantitative data and expert opinion to makeparameter estimates. In conventional diseasemodelling experts include epidemiologists andmicrobiologists. This paper describes a state-transition model of rinderpest transmissiondynamics in East Africa. The model differs fromprevious rinderpest models and disease models ingeneral in that the knowledge of the owners of thelivestock populations being modelled is utilized asexpert opinion to derive parameter estimates andvalidate the model.
Participatory epidemiologic tools were utilized toestimate population demographics, rinderpestmortality rates, population contact structure andinter-epidemic periods. Published laboratoryinoculation data was used to estimate latency andinfectious period. The basic reproductive numberwas derived from serologic data obtained duringperiods of endemic stability. The estimates ofbasic reproductive number and infectious periodwere in turn used to estimate effective contactrates. The model was validated by comparing thepredicted epidemic curves with historicinformation provided by farmers on the actualtemporal patterns of outbreaks in two differentendemic scenarios.
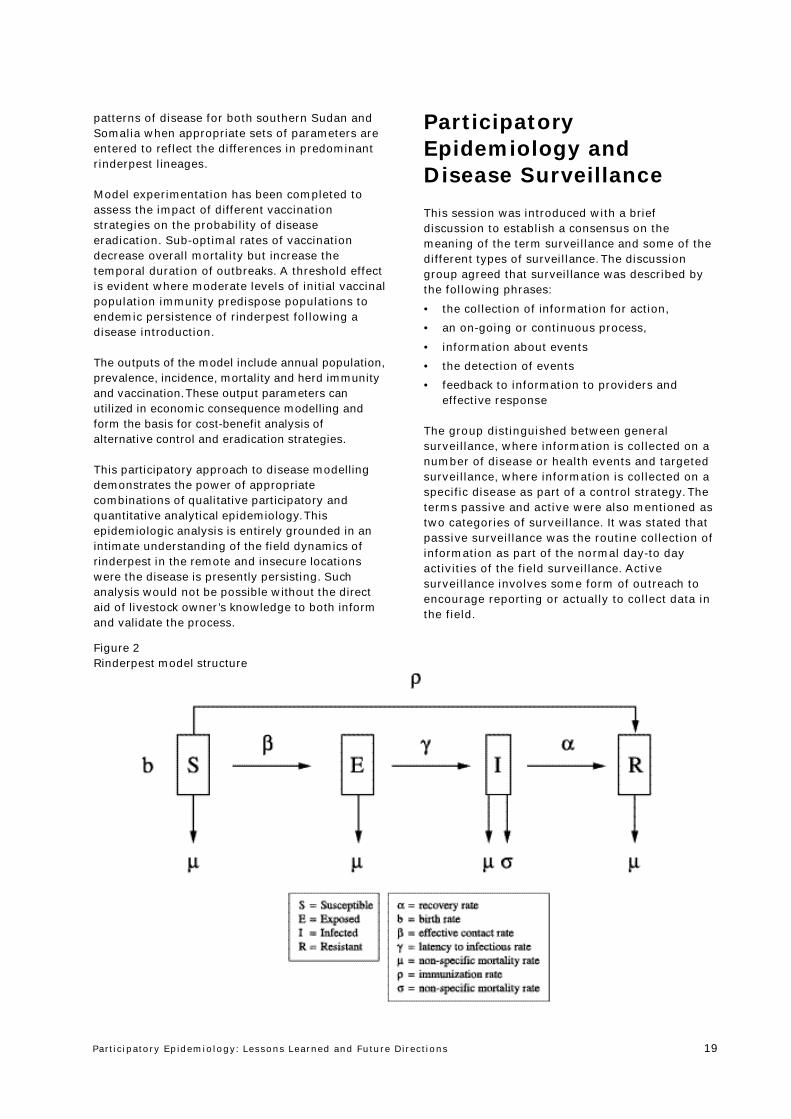
The model is a simple, open population SEIR statetransition model that incorporates stochasticelements when transmission levels are low.The structure of the model is presented in Figure1. The model incorporates vaccination as either acontinuous or a seasonally pulsed process.
Rinderpest is southern Sudan is caused bymoderately virulent rinderpest virus from Africanlineage 1. In Somali, a mild form of rinderpest dueto Africa lineage 2 is believed to be present.The model successfully reproduces the endemic
How can participatory epidemiology assistPACE?
Session 3
Figure 1Temporal distribution of herder reports of rinderpest in Somali ethnic areas of East Africa: 1980-1996
Partic ipatory Epidemiology: Lessons Learned and Future Directions 19
patterns of disease for both southern Sudan andSomalia when appropriate sets of parameters areentered to reflect the differences in predominantrinderpest lineages.
Model experimentation has been completed toassess the impact of different vaccinationstrategies on the probability of diseaseeradication. Sub-optimal rates of vaccinationdecrease overall mortality but increase thetemporal duration of outbreaks. A threshold effectis evident where moderate levels of initial vaccinalpopulation immunity predispose populations toendemic persistence of rinderpest following adisease introduction.
The outputs of the model include annual population,prevalence, incidence, mortality and herd immunityand vaccination. These output parameters canutilized in economic consequence modelling andform the basis for cost-benefit analysis ofalternative control and eradication strategies.
This participatory approach to disease modellingdemonstrates the power of appropriatecombinations of qualitative participatory andquantitative analytical epidemiology. Thisepidemiologic analysis is entirely grounded in anintimate understanding of the field dynamics ofrinderpest in the remote and insecure locationswere the disease is presently persisting. Suchanalysis would not be possible without the directaid of livestock owner’s knowledge to both informand validate the process.
ParticipatoryEpidemiology andDisease Surveillance
This session was introduced with a briefdiscussion to establish a consensus on themeaning of the term surveillance and some of thedifferent types of surveillance. The discussiongroup agreed that surveillance was described bythe following phrases:
• the collection of information for action,
• an on-going or continuous process,
• information about events
• the detection of events
• feedback to information to providers andeffective response
The group distinguished between generalsurveillance, where information is collected on anumber of disease or health events and targetedsurveillance, where information is collected on aspecific disease as part of a control strategy. Theterms passive and active were also mentioned astwo categories of surveillance. It was stated thatpassive surveillance was the routine collection ofinformation as part of the normal day-to dayactivities of the field surveillance. Activesurveillance involves some form of outreach toencourage reporting or actually to collect data inthe field.
Figure 2Rinderpest model structure

Partic ipatory Epidemiology: Lessons Learned and Future Directions20
After presentations on general and targeteddisease surveillance, a discussion was heldwhere participants stressed the importance ofcommunity-based animal health networks asinformation resources for national diseasesurveillance networks. It was noted that CAHWnetworks have been implemented bygovernment, projects and NGOs. The debatecentered on how best to incorporate CAHWnetworks into the surveillance system.Government veterinarians expressed theirfrustration at the lack of communication betweenveterinary services (VS) and project and NGO-based animal health programmes. It was notedthat many projects and NGOs had madeconcerted efforts to involve veterinary services,but in the absence of a policy framework andoperating system, it was difficult for CAHWnetworks to access the national systems.
The following points were made:• CAHWs are farmers and have the right to
make disease reports.• Monthly monitoring of CAHWs is an important
animal health information resource.• A communication gap exists between farmers
and veterinary services.• VS have no stated policy on the use of CAHW
networks as information resources.• VS have not put in place a system to collect
animal health information from CAHWnetworks.
• NGOs are usually registered and involve localVS staff in training and monitoring activitiesat the NGOs expense.
• Higher levels of the veterinary service areoften not aware of the activities of their fieldveterinarians in CAHW networks as theveterinary service do not have systems inplace to monitor and coordinate NGO andproject-based animal health activities.
• Effective feedback of summarized informationto data providers (CAHW monitors, CAHWs,and livestock owners) is key to the sustainedsuccess of any programme.
It was the consensus of the discussion that allstakeholder were willing and motivated to worktowards integration of community animal healthinto the national service delivery andsurveillance systems. It was agreed thatstakeholder workshops should be held to renewdialogue on the basis of mutual respect betweenthe VS, projects, NGOs, profession and livestockowners. The objective should be to establish apositive and productive framework for animalhealth information exchange.
Experiences with assessing and
quantifying disease surveillance
information for small ruminants as
obtained through the Nomadic
Animal Health Auxiliary System(NAHA-System) in the Central
Rangelands of SomaliaMaximilian P.O.Baumann1,2, Ahmed M. Hassan2, Hagi A. Nuux2
1Department of International Animal Health, Faculty of VeterinaryMedicine, Freie Universität Berlin, Königsweg 67, D-14163 Berlin,Germany 2 Formerly: GTZ Veterinary Component, Central RangelandDevelopment Project (CRDP), Beledweyne, Somalia
Disease surveillance data were collected during 4visits to 21 Nomadic Animals Health Auxiliaries(NAHA) from 7 villages/degaans4 (Halgan, JameecoMuktar, Bulo Burti, Biyo Neef, Aboorey, Maxas,Maqokorey) in Bulo Burti (B/B) district of HiraanRegion from February 1987 to April 1988 usingcustomized data recording sheets.
In an attempt to identify the disease situation asencountered and reported by the NAHAs and toquantify such disease information the followinganalytical steps were taken:First, the common Somali terms used for smallruminant diseases and symptoms in the studydistrict were noted and congruency with scientificterminology determined.
Then, the occurrence of a disease/symptom wasexpressed by the number of animals treated/affected (numerator) and the number of flocksharbouring animals treated/affected (denominator)to calculated the average number of animalsaffected in a flock affected. As flock sizes varywithin the district the average flock sizes of 163 inB/B district was used as denominator (and thefactor 100 included) to calculate the percentageaverage animals affected in an average flock. Thisflock disease index (FDI) served as a measure toquantify a disease as an individual animal problemor a flock problem, and, thus broken down into thefollowing categories, i.e. >0 - 5%, >5 - 10%, >10 -20%, >20 -30%, >30 - 40%, >40 - 50% and >50%.
For the disease data reported differentiation wasmade between the active involvement of the NAHAi.e. inspection and/or treatment of diseasedanimals, and his role as mediator for diseaseintelligence evolving from his pastoral community.
4 The traditionally managed communal grazing area of about 1000 to3000 km2

Partic ipatory Epidemiology: Lessons Learned and Future Directions 21
Reporting periods for each visit were the precedingmonths whereby the following calender-wiseclassification for the four different climaticseasons Gu (long rainy season) from March 22 toJune 21, Hagaa (short dry season) from June 22to September 21, Dayr (short rainy season) fromSeptember 22 to December 21, and Jilaal (longdry season) from December 22 to March 21, wasapplied. Within the district villages/degaans weregrouped into ecological sub-zones, i.e. “Inland”(Maxas, Maqokorey, Aboorey and Nooleye) and“Riverine” (Bulo Burti, Biyo Neef, JameecoMuktar, Halgan). The age of treated/affectedanimals was classified according to age groups(0 -1 year, 1.1 - 2 years, over 2 years).
The case fatality rate of a disease was assessedby asking the following question: “If 10 animalsare affected by the disease, how many will diewithout treatment ?” and expressed in percent.To enable differential diagnosis and to allow for amore detailed disease description the immunestatus (after recovery) of the animals wasinquired and recorded as immune (= yes = morethan 50% of the animals affected) or not-immune(= no = less than 50% of the animals affected).The effectiveness of the drugs applied did alsoenter the data collection.
The existing confusion for different locally usedSomali terms for single diseases, diseasesyndromes or gross symptoms in sheep andgoats, even at the village/degaan level, could bedemonstrated. For instance, the vernacular termsSambab (literally: lung) and Agmar are consideredto stand for pneumonia, which again was oftensynonymous for CCPP.
To deepen the understanding of certain diseasesor disease complexes of small ruminants such asQanje (literally: lymph node), but also termed asTu or Riimiye in some villages/degaan, oral reportsgiven by the NAHAs on symptoms and post-mortem findings were listed and broken down byvillage/degaan.
Flock disease indices for ecological sub-zonesdemonstrated and quantified the importance ofSambab in all villages/degaan of B/B district witha marked higher FDI in the “Inland” degaan ofMaxas, where Qanje also seemed to play aprominent role.
Endoparasites and cases of diarrhoea appearedwith higher “prevalences” in the ecological sub-zone characterised as “Inland” than in the“Riverine” sub-zone. A disease such as FMD insmall ruminants seemed to be restricted to
individual villages/degaan, e.g. being endemic inAboorey and, thus, not causing serious losses.
Sambab, the most prominent disease in B/Bdistrict, is a dry season disease; over 80% of thecases reported and treated by NAHAs occurred inthe dry seasons Jilaal and Hagaa. The FDI inroughly half of the cases ranged between 5% and10%. However, in a single flock up to 60% of theanimals were found affected. Sambab case fatalityrates showed a wide range believed to be likelydue to different pneumonia-causing agents andstrains. In all cases reported and treated sheepand goats over 2 years of age were attacked.Young stock (less or equal to 1 year) playedobviously a minor role. The full effectiveness ofthe antibiotic Oxytetracyclin could bedemonstrated.
A coincidence of anthelmintic treatments askedfor by flock owners with wet and humid climaticconditions leading to a rise in endoparasites ofsheep and goats could be shown. In half of theflocks 5% to 10% of the animals were consideredto deserve anthelmintic treatment by the NAHAs.However, a good numer of anthelmintics sold toand administered by the flock owners themselvesreflected the demand for appropriate andeffective anthelminthics.
In order not to loose potential informationobservations regarding diarrhoea, though low innumber, were recorded separately. A trend oflikely occurrence of diarrhoea - a symptom, not adisease itself - in dry seasons was apparent.
For the first time livestock disease surveillancedata obtained through veterinary auxiliaries froma primary animal health care delivery system inCentral Somalia, the Nomadic Animal HealthAuxiliary System, are demonstrated.
It has to be considered that the reports of diseasetreatments and patterns were provided orally bythe local NAHAs and then transferred onto thedata recording forms of the CRDP/GTZ VeterinaryComponent. Thus, figures generated should not betaken as absolute, but rather illustrating themagnitude of a condition. Figures are furtherconfounded by the willingness for veterinaryattention emerged from the decision of thelivestock herder that treatment of a diseasedanimal in his/her flock is economically justifiedand, thus, unalterable. Therefore, the methodologyapplied served as a tool to primarily exhibit trendsin disease patterns and to provide additional dataon yet not well defined disease complexes such asQanje in small ruminants.

Partic ipatory Epidemiology: Lessons Learned and Future Directions22
Disease Surveillance and
Community-based Animal Health:
Experience of the Operation
Lifeline Sudan Southern Sector
Livestock ProgrammeBryony JonesVétérinaires sans frontières - Belgium, PO Box 13986, Nairobi,Kenya
The OLS Southern Sector Livestock Programme hasapproximately 1000 CAHWs who have received twoweeks basic training in disease diagnosis,treatment and vaccination. In addition there areapproximately 150 supervisors who have beentrained for 4-9 months in animal health, andapproximately 35 field veterinarians employed byNGOs/FAO.
Routine information on cases treated is recorded byCAHWs on a pictorial monitoring form.Approximately once a month, each CAHW reports tohis/her supervisor to report on medicine usage,collection of revenue and treatments carried out. Theinformation in the pictorial form is summarized ontoa summary form. This is submitted to the fieldveterinarian. The NGO extracts any data they requirefrom the form and then all forms are submitted toFAO for entry into a centralised database.
Vaccination is usually carried out as teams ofCAHWs. Vaccinations carried out are recorded by a
literate member of the team on a dailyvaccination form. These are submitted to thesupervisor who passes them to the NGO forsubmission to the FAO database.
In addition, CAHWs report any outbreaks thathave been reported to them by livestock keepers,or any outbreaks observed during their routinework. The CAHWs give an oral report to thesupervisor of history and clinical observations.The supervisor will then follow up by visiting theoutbreak and carrying out a basic investigation;history, clinical examination, post mortemexamination (if possible) and collect samples(some but not all supervisors have sampling kitsand are able to collect and submit samples). Thesupervisor then fills in an outbreak report form.This is sent to an FAO vet in Lokichokio who isthe focal point for outbreak information. Thesupervisor also reports to the field veterinarianand if he/she is in the area, they will also followup and verify the findings for the supervisor andcollect samples if not already done. If theoutbreak is urgent or severe, then outbreakinformation is sent by radio message. FAO willthen follow up the report, either by asking forfurther information, providing appropriatemedicines or vaccines, or by visiting to carry outfurther investigations.
Treatment, vaccination and outbreak informationis collated into a summary report that is reportedback to NGOs and field supervisors eitherquarterly or during livestock co-ordinationmeetings. Data is used by NGOs and FAO incompiling reports to donors.
Future plans in the context of the final stages ofrinderpest eradication:
- outbreak reporting - to continue with theexisting system but to provide training andfield support to improve the quality ofinvestigations, reports and follow up,
- active surveillance - CAHWs to be looking forrinderpest-like disease and talking with cattleowners about possible rinderpest, supervisorsto be carrying out clinical surveillance andinterviewing livestock keepers during routinecattle camp visits, and in markets, supervisorsalso to be involved in sero-surveillancecollecting an agreed number of samples intheir area for an agreed payment,
- RP Project field staff to carry out participatorydisease searching in areas of possible RPendemicity, or as part of outbreak rumourinvestigation.
Partic ipatory Epidemiology: Lessons Learned and Future Directions 23
Participatory DiseaseSearchingBerhanu Admassu and Jeffrey MarinerCommunity-based Animal Health and Participatory Epidemiology(CAPE) Unit, Pan African Programme for the Control of Epizootics,Organization for African Unity/Interafrican Bureau for AnimalResources, PO Box 30786, 00100 Nairobi, Kenya
IntroductionParticipatory Disease Searching (PDS) as part ofparticipatory epidemiology is enablingveterinarians to collect information on specificdisease situations. This paper describes PDS asrelated to rinderpest.
The specific methods and processes that are mostuseful for PDS are:• Open-ended questions• Probing• Time-lines• Triangulation (cross-checking of reports and
data from different sources)• Use of key informants• Mapping• Clinical observation and transects
What is the problem?We have to define the problem as precisely aspossible. For example, in the case of rinderpestcontrol PDS can be conducted to:• Ascertain rinderpest status• Establish the last date of a rinderpest outbreak• Reveal recent stomatitis-enteritis (S-E)
outbreaks for investigation purposes• Collect baseline data for sero-surveillance
Preparations for PDS
• Rinderpest is a disease that depends on themixing of livestock for survival.
• There are no known carrier states or examples ofchronic infection.
• The virus survives through the continuousoccurrence of new acute cases in susceptibleanimals.
• Thus, the virus must continuously find newsusceptible animals for survival.
• A safe, effective and inexpensive vaccine existsthat has been successfully applied in most areaswhere veterinary service delivery is reliable.
These factors suggest, and indeed experience hasshown, that remote, marginalized pastoralcommunities, where livestock contact rates are highand vaccination is sporadic, are often the reservoir forthe endemic persistence of rinderpest (Mariner, 1996).
As a first step, an inventory of remote cultures andcommunities should be made and secondary sourcesof information should be obtained and researched.
In PRA, one often looks at ‘proxy indicators’ inregard to sensitive subjects for which it may bedifficult to obtain unbiased direct information.Remoteness, insecurity, and lack of services canserve as proxy indicators for the likely presence ofinfectious disease when prioritising search areas atthe national level.
It is especially important to avoid ‘tarmac’ oraccess bias in regard to rinderpest searching.As with any disease investigations, the appraisalteam should carry all necessary sampling materialsin case a SE outbreak is encountered.
PRA checklist for a Participatory Rinderpest Disease Search
1. Introduce the appraisal team as an animal health appraisal.2. Identify the respondents and establish if they cattle owners.3. Establish their main herding locations (mapping).
Items 1 to 3 introduce the subject and establish the identity of the participantsItems 4 to 6 are an expanding enquiry into animal health problems.
4. What are the current cattle disease problems in their herd? If tearing or diarrhoea is mentioned, explore thesesyndromes in detail. This item investigates what animal health problems the respondents are personally andpresently facing.
5. What are the current cattle disease problems in the area? This item inquires into what animal health problemsthe immediate community is presently facing.
6. Historically, what are the most important disease problems of cattle? This item inquires into the most significantanimal health problems the community has faced regardless of time.Invariably rinderpest is mentioned in the response to this question if the cattle owners have experiencedoutbreaks in the last two decades. Frequently it will be the first disease mentioned.
7. Have they personally seen rinderpest in their lifetimes? What does it look like?8. When was the last time their cattle where affected by rinderpest? Where did it occur? Where did it come from?
As warranted, further probing questions can be added to cross-check reports made in other interviews, further definecattle movements which may affect the epidemiology of the disease, or to contrast current outbreaks with previousoutbreaks in regard to the severity of disease.

Partic ipatory Epidemiology: Lessons Learned and Future Directions24
Interviewing as a tool for PDS
One of the objectives of PDS is usually to gathercomplete information about all disease situationsin the village livestock. Ideally, all owners of therelevant livestock species in the village shouldattend the interview. The best people to have at theinterview are those that know the animals best. Aswith other types of disease searches:
The interviewer should be careful not tocommunicate their specific interest in rinderpest tothe respondents. If possible avoid travel in vehiclesused in rinderpest control activities or withindividuals locally known to be specialized inrinderpest control. The interview should beintroduced as a general study of animal healthissues in cattle or a similarly broad theme.
Disease names
The choice of words is particularly important whendiscussing particular disease. The appraisal teamwill often think about diseases as particular entities,each with a particular separate cause. On the otherhand, think more in terms of disease syndromes.When an animal behaves in a particular way, andshows particular signs, then it is thought of as aparticular disease. This disease syndrome may havea unique local name, or the technical name of aparticular disease may be used. The tendency oflivestock owners to talk about disease syndromesbased on patterns of clinical signs, rather thanspecific diseases should be kept in mind during theinterview. Mistakes can be avoided by payingattention to a few points.
Don’t use the technical name for a disease whenasking about that disease. If you know the localname, and understand what disease or diseases ittruly represents, then use that name. In somesituations, the clinical signs and behavior of thedisease in the population are distinctive enough tobe sure that the name given by owners does refer toa single disease. In others, it is not so simple.The eliciting process of all known cattle diseasenames should be in the language of the community.This works particularly well with a small group asthe stories and ideas of one important often sparkthe mind of another. However, there are severalbiases that should be avoided.
Seasonality: livestock owners are most likely tomention diseases of the current season. After thoseare elicited, ask specifically for diseases mostprevalent in other seasons and /or year round.
Severity of disease: livestock owners are mostlikely to give the names of the most serious (i.e.
fatal) diseases so make sure that chronic diseasesand those which are not fatal, but may lead toproduction losses, are also recorded.
Incidence of disease: it is useful to ask the groupwhether there are diseases that appear onlyperiodically otherwise one might miss majorepidemics that sweep through an area, or conditionsthat appear only in unusual climatic circumstances.
Persistent questioning
One rule of collecting information throughinterviews is that you should never be satisfiedwith the first answer. When a question is asked,there is the danger that the answer could bewrong, either for the reasons listed previously, orelse because the experience of the personanswering doesn’t represent the experience of thewhole village.
It is a good idea, therefore to check and recheckevery answer that is received. Asking the samequestion in several different ways, to severaldifferent people, does this. Each time, the questionfocuses on some different aspects of the problem,and each answer is compared. If there is someinconsistency, then discussions started to try toresolve it and come up with a consensus.
Topics for probing
Probing on specific subjects can provide very usefulinsights into community knowledge on diseaseepidemiology, pathology and diagnostic processes.Often it is best to reserve these probing sessions forespecially knowledgeable key informants. These areusually more senior members of the communityrespected and consulted by the community for theirlivestock knowledge.
Diarrhoeal disease:
In a subset of interviews, the community should beprobed about the different terms used to describediarrhoeal disease. Points to be investigated are:What terms are used to signify diarrhoea in general?Are different types of diarrhoea distinguished (i.e.bloody vs. non-bloody, acute vs. chronic, etc.)What specific diseases do they associate withdiarrhoea?What indicators are used to differentiate betweendifferent diarrhoeal diseases?
Disease concepts and methods of rinderpest
transmission:
It is useful to attempt to understand local conceptsregarding the cause of disease and methods oftransmission. In regard to rinderpest, pastoralists

Partic ipatory Epidemiology: Lessons Learned and Future Directions 25
can often accurately describe risk factors andtypes of contact that lead to transmission.Knowledge in these areas varies significantlybetween communities and it is important not tomake assumptions.
Mapping
Rinderpest is a disease that depends on cattlecontact and movement for its survival. Mapping ofcattle movement and determination of inter-community contact is a very important activity inregard to understanding local rinderpest ecology.
In order to initiate a mapping exercise, respondentsshould be asked to specify their primary grazingsites by season. Depending on the complexity of thebio-climatic system, it may be worth constructing aseasonal calendar as a companion exercise. Often,pastoralists will specify location names that are notevident on modern maps. These initial questionsoften turn to a discussion of just exactly wherethese key resource sites are which naturally leads tothe sketching of maps on the ground.
A broad area about an arm and a half reach shouldbe cleared and smoothed. Usually, participants willnaturally gather round and equip themselves withthe necessary tools: normally sticks and otherobjections to assist in drawing and act as landmarks. The participants should first be asked toindicate key landmarks such rivers, market towns,major wells or watering sites. Then the grazing sitescan be indicated. In addition to normal grazing sites,emergency-grazing areas used in time of drought orinsecurity should be indicated. For rinderpestepidemiology, the data on movement, mixing(contact) and trade will be the most significant.These will be key factors in subsequent risk analysisand in disease control strategy design. Movementand contact data relative to the presence of the viruswill determine where and when vaccination orsurveillance is appropriate.
Clinical observation, sample
collection and transects
Before or after an interview, it is always useful towalk the camp, herd and adjacent environment.In rinderpest disease searching, tearing is a signthat can be detected at a distance. If you arewalking the herd prior to the interview and notetearing, it is best not to call attention to the sign.Proper clinical exams should be carried out afterthe interview. The only exception is when thelivestock are on the move and you run the risk oflosing the opportunity.
Analysis of results
Participatory disease searching is somewhatdifferent from other types of PRA. Most PRAinterviews start at a general level and work towardsspecifics. The interview technique used in PDScasts an ever-broadening net until the respondentsvolunteer rinderpest as a problem. At this point theinterview begins to focus down on EVK regardingrinderpest. This could happen at any of three levels:current personal experience, current personalobservation or in the past. Part of the process ofjudging the quality and significance of reportsrelates to when the respondent introduces thesubject of rinderpest.
As described previously, reports of rinderpest orother SE events should be categorized, tabulatedand examined for trends or unifying factors. Theexistence of the stomatitis-enteritis outbreakdefinition and guidelines for comprehensiverinderpest surveillance assists in the analysis ofrinderpest PDS results.
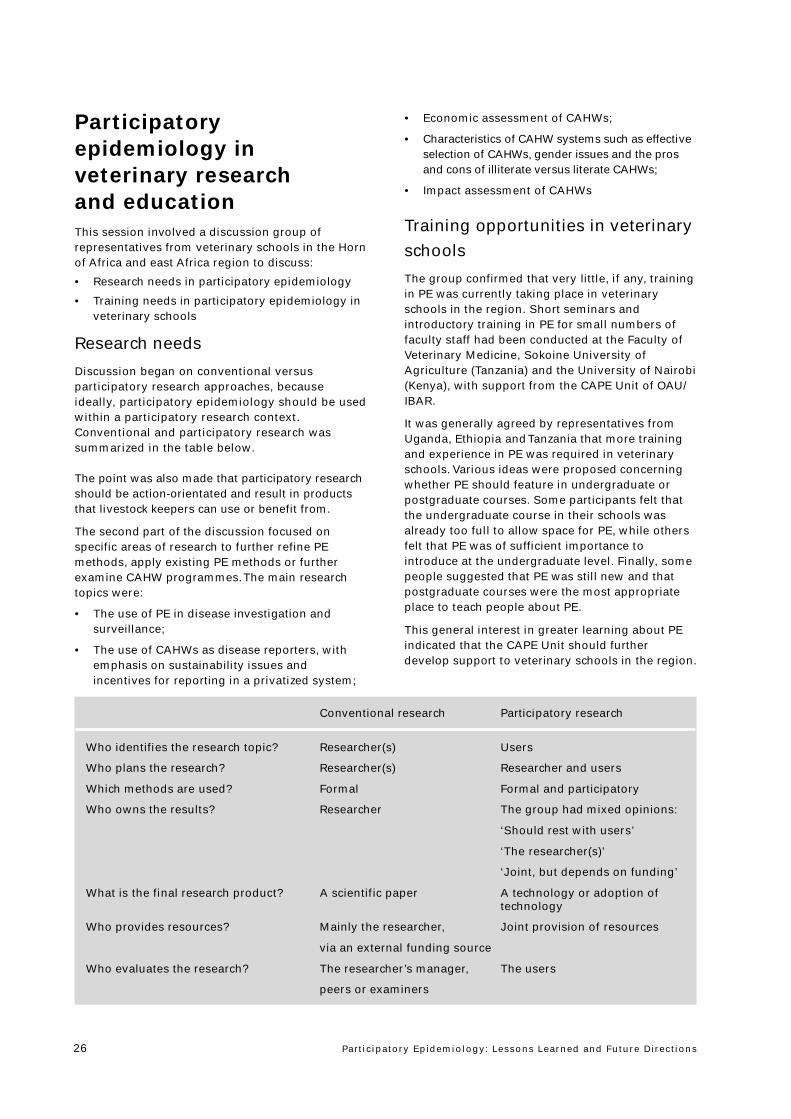
Partic ipatory Epidemiology: Lessons Learned and Future Directions26
Participatoryepidemiology inveterinary researchand educationThis session involved a discussion group ofrepresentatives from veterinary schools in the Hornof Africa and east Africa region to discuss:
• Research needs in participatory epidemiology
• Training needs in participatory epidemiology inveterinary schools
Research needs
Discussion began on conventional versusparticipatory research approaches, becauseideally, participatory epidemiology should be usedwithin a participatory research context.Conventional and participatory research wassummarized in the table below.
The point was also made that participatory researchshould be action-orientated and result in productsthat livestock keepers can use or benefit from.
The second part of the discussion focused onspecific areas of research to further refine PEmethods, apply existing PE methods or furtherexamine CAHW programmes. The main researchtopics were:
• The use of PE in disease investigation andsurveillance;
• The use of CAHWs as disease reporters, withemphasis on sustainability issues andincentives for reporting in a privatized system;
• Economic assessment of CAHWs;
• Characteristics of CAHW systems such as effectiveselection of CAHWs, gender issues and the prosand cons of illiterate versus literate CAHWs;
• Impact assessment of CAHWs
Training opportunities in veterinary
schools
The group confirmed that very little, if any, trainingin PE was currently taking place in veterinaryschools in the region. Short seminars andintroductory training in PE for small numbers offaculty staff had been conducted at the Faculty ofVeterinary Medicine, Sokoine University ofAgriculture (Tanzania) and the University of Nairobi(Kenya), with support from the CAPE Unit of OAU/IBAR.
It was generally agreed by representatives fromUganda, Ethiopia and Tanzania that more trainingand experience in PE was required in veterinaryschools. Various ideas were proposed concerningwhether PE should feature in undergraduate orpostgraduate courses. Some participants felt thatthe undergraduate course in their schools wasalready too full to allow space for PE, while othersfelt that PE was of sufficient importance tointroduce at the undergraduate level. Finally, somepeople suggested that PE was still new and thatpostgraduate courses were the most appropriateplace to teach people about PE.
This general interest in greater learning about PEindicated that the CAPE Unit should furtherdevelop support to veterinary schools in the region.
Conventional research Participatory research
Who identifies the research topic? Researcher(s) Users
Who plans the research? Researcher(s) Researcher and users
Which methods are used? Formal Formal and participatory
Who owns the results? Researcher The group had mixed opinions:
‘Should rest with users’
‘The researcher(s)’
‘Joint, but depends on funding’
What is the final research product? A scientific paper A technology or adoption oftechnology
Who provides resources? Mainly the researcher, Joint provision of resources
via an external funding source
Who evaluates the research? The researcher’s manager, The users
peers or examiners
Partic ipatory Epidemiology: Lessons Learned and Future Directions 27
Tasks for WorkingGroups
During this session, participants were divided intoworking groups representing National PACEProgrammes from Ethiopia, Kenya, Somalia, Sudan,Tanzania and Uganda. Each working group wasrequested to complete the tasks described below.
Presentations byWorking Groups1. Lessons learned during theworkshop
PACE Ethiopia
• Created more awareness on PE• Methods used and constraints in PE• Involving local communities in information
gathering way of using indigenous knowledge• CAHWs as collectors of data to be integrated
into national animal health informationsystems.
• Ways to integrate PE results in conventionalresearch, i.e.- Training needs in PE- Incorporation of PE in research and learning
institutes
PACE Tanzania
• Scope and potential application of PE in diseasesurveillance
• Participatory tools can be used to suit particularsituations (flexible and adjustable)
• Better results/findings can be obtained by theuse of both quantitative and qualitativemethods of investigation
• Results from PE can be used in contemporaryepidemiological techniques, modelling and riskassessment
• Indigenous knowledge can be captured,appreciated and used effectively; cultural andnomenclature differences need to take on board
• Appreciation of the involvement and ownershipby stakeholders and target groups
• Often a lack of common understanding aboutwhat PE is, what it can do and best practice andapplication
PACE Uganda
• PE can help tap the available local knowledgepastoral areas
• PE can complement the existing surveillancesystems
• PE can generate baseline data that can help totarget surveillance and research
• PE is associated with projects and NGOs - howsustainable are these?
• PE implies ownership, learning empowermentthe local communities
Session 4
National PACE Programme Working Groups
1. As a working group, what are the main “lessonslearned” from the presentations and discussiongroups during the workshop. List these lessonsand rank them in order of importance.
2. By reference to the objectives of:• National PACE Programmes• CAPE Unit• Veterinary schools and research centres,identify specific ways to use participatoryepidemiology to add value to PACE.
Ideas arising from discussion so far include,• Use of participatory epidemiology to improve
understanding of epizootic diseases in pastoralareas
• Testing of community-based surveillancesystems
• Participatory impact assessment of CAHWservices
• Further development and testing of PEmethods and approaches
The working group may identify other needs inaddition to this list.
Please be specific. Try to make specific proposalsbased on your knowledge of existing diseasecontrol priorities and presence of CAHW or otherservices on the ground. Which diseases should welook at in which areas? Who are the key playerswho should be involved? What are the deadlinesfor completing the work?
3. Identify training/educational needs for the variousplayers involved in testing and applying PE inpastoral areas.
Outline a training plan which specifies who shouldbe trained (which people in which institutions?)and when (what are the deadlines by whichtraining should have taken place?).
Partic ipatory Epidemiology: Lessons Learned and Future Directions28
• There is a need to integrate the PE into theNational Surveillance Network
• Need to co-ordinate PE activities at district andnational levels
• Need to train personnel in personnel at alllevels in PE methods
PACE Sudan
• Potential for getting information from CAHW• How valid - does it fit in the system• Comparison between different methodologies PE• Exchange of ideas and practices• Respect, recognize and make use of indigenous
knowledge to be incorporated into researchactivities
PACE Kenya
• Use of PE improves the understanding ofepizootic diseases in pastoral areas.
• Empowers communities to identify and solvetheir own problems
• PE is not structured questionnaire• Combined qualitative and quantitative is “best
practice”• Useful in testing community-based surveillance
systems• Participatory impact assessment of CAHW
services• Need for further development and testing of PE
methods
PACE Somalia
• To combine PACE Methods with conventionalepidemiology methods
• PE methods useful for validation of certaininformation, models, concepts
• PE methods useful for descriptive epidemiology(disease alert, pattern, livestock movement)
• Useful for first steps in an area to assess thehealth situation (if a disease problem existsbetter than disease is mild or endemic)
2. Ways to use participatory
epidemiology in National PACE
Programmes
The common themes in National PACE Programmeobjectives are:
1. Final eradication of rinderpest
2. Strengthening national epidemiology capacity
3. Control of major epizootics
4. Improved veterinary service delivery andprivatization
PACE Ethiopia
Participatory epidemiology can assist theprogramme by:• Providing information from remote areas• Passive surveillance by making use of CAHWs
through an established system• Active surveillance using PE methodsThis will lead to:• Better understanding of disease• Refining strategies• Early warning and early reaction
Specific activities
• Inventory and assessment of CAHWprogrammes
• Establish linkages and improve informationflow between CAHW/NGOs and governmentveterinary services
• Introduce PE into CAHW projects (widen scopeto reporting)
• Standardisation of information• Monitoring and evaluation• Collect indigenous knowledge• Incorporate into teaching and researchCAPE can act as an initiator and facilitator of theseactivities
PACE Tanzania
In PACE Tanzania, CAHWs are considered under theobjective ‘Improvement of the Delivery ofVeterinary Services’. So far, PE as a tool was notbeen included in the implementation/activities inthe PACE Tanzania Global Plan. However, PE can beused to add value to PACE. For example, PE has arole in:1. Strengthening veterinary services - in disease
surveillance and delivery of animal healthservices
2. Privatisation of veterinary service delivery by:- Establishment of links between private vets,
other animal health service providers- Fostering the involvement of private vets in
epidemio-surveillance3. Rinderpest eradication - clinical surveillance
Partic ipatory Epidemiology: Lessons Learned and Future Directions 29
4. CBPP control and the control of other epizootics(FMD, ND, RVF, ASF). PE can assist:- Surveillance- Control of livestock movements and
improved participation/response invaccination campaigns
- Fostering and sensitisationOverall, PE can enhance livestock owners’participation and ownership of disease controlprogrammes
CAPE can provide technical and logistical supportin areas involving PE. The Animal Health Services-Coordination Programme is responsible forimproved delivery of animal health services. Thisincludes expansion and proper use of CAHWsunder the supervision of vets in pastoral areas.
Specific proposals for immediate application of PE1. Rinderpest surveillance - support to clinical
surveillance (Dec. 2001- July 2002)2. African swine fever - involving livestock
keepers, raising awareness and improvingsurveillance and control
3. CBPP - surveillance; impact assessment of CBPP(vaccination versus control)
4. Newcastle disease - socio-economic studies
Various activities include research centres such asthe Animal Diseases Research Institute (ADRI) andveterinary investigations centers.
Also need to consider veterinary training institutes- CAPE to support curriculum development toinclude PE in undergraduate and postgraduatetraining:• Short course - for epidemiologist/field officers
(by December 2002)• Training of trainers (by April 2002)
Key Players:- Livestock keepers - associations, groups- Livestock field officers- Livestock traders- Private veterinarians- DVDS- VICs and ADRI- DVS (Epidemiology Unit)- University/SUA
PACE Uganda
1. Integrate and co-ordinate PE with othersurveillance and other epidemiologicaltools for RDP, CBPP, CCPP, OOR, FMD, ASF, LSD,RVF, rabies and other diseases. Players includeMAAIF, National Agricultural ResearchOrganizations, Faculty of Veterinary Medicine andprivate veterinary practices; timeframe - 6 months.
2. Train ‘trainers of trainers’ in PE.3. CAPE facilitates a PE investigation into “Mixed
infection syndrome; March 2002.4. DVOs and MAAIF conduct continuous
monitoring and evaluation of community-basedsurveillance system in Karamoja region.
5. Further development of PE methods in the PACEdistricts.
6. PE methods will shed light on endemic diseasesand syndromes.
PACE Sudan
General roles for PE include:1. Disease surveillance2. Disease control3. Strengthening veterinary services4. Disease diagnosis5. Research - centers include:
- 11 regional vet labs in the regions- 3 vet schools- veterinary training center (KRT).
Use of PE through CAHWs, local leaders andlivestock owners. Activity already practiced in N.Kordofan and Darfur on-going. In the southernsector through FAO, PE is used in the South to findRP outbreaks in infected zones to complementPACE programmes. PE also used duringvaccination teams.
PACE Kenya
Roles for PE can be categorized according to threemain programmes or players:
A. In the PACE Kenya Programme1. Envisage PE to improve epidemio-surveillance
network through disease surveillance andreporting. Specfically,- Rinderpest eradication process- Improve the control of other epizootics:
CBPP, FMD, RVF, LSD- Strengthen private - public sector linkages indelivery of animal health services
2. Will help in the understanding the socio-economics of major epizootics and thereforeshape/refine their control strategiesOur priority areas are the pastoral areas (Zone II& III) and the key players are public vets, NGOsand CAHWs, and private vets. Timeframe -duration of PACE and beyond.
B. In the CAPE Unit1. Streamlining the delivery of vet services in
pastoral areas2. Streamlining data collection in pastoral areas3. Linkages within the region
C. Veterinary Schools and Research Institutes1. Introduce PE in training curriculum
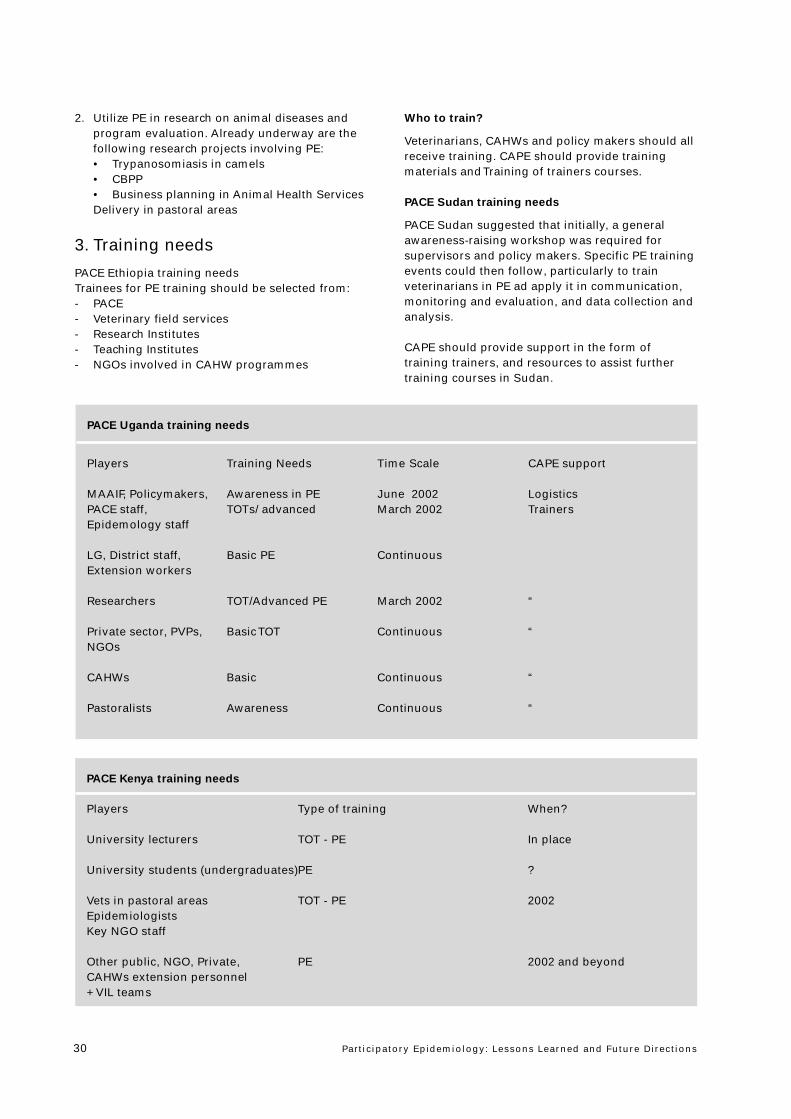
Partic ipatory Epidemiology: Lessons Learned and Future Directions30
2. Utilize PE in research on animal diseases andprogram evaluation. Already underway are thefollowing research projects involving PE:• Trypanosomiasis in camels• CBPP• Business planning in Animal Health ServicesDelivery in pastoral areas
3. Training needs
PACE Ethiopia training needsTrainees for PE training should be selected from:- PACE- Veterinary field services- Research Institutes- Teaching Institutes- NGOs involved in CAHW programmes
Who to train?
Veterinarians, CAHWs and policy makers should allreceive training. CAPE should provide trainingmaterials and Training of trainers courses.
PACE Sudan training needs
PACE Sudan suggested that initially, a generalawareness-raising workshop was required forsupervisors and policy makers. Specific PE trainingevents could then follow, particularly to trainveterinarians in PE ad apply it in communication,monitoring and evaluation, and data collection andanalysis.
CAPE should provide support in the form oftraining trainers, and resources to assist furthertraining courses in Sudan.
PACE Uganda training needs
Players Training Needs Time Scale CAPE support
MAAIF, Policymakers, Awareness in PE June 2002 LogisticsPACE staff, TOTs/ advanced March 2002 TrainersEpidemology staff
LG, District staff, Basic PE ContinuousExtension workers
Researchers TOT/Advanced PE March 2002 “
Private sector, PVPs, Basic TOT Continuous “NGOs
CAHWs Basic Continuous “
Pastoralists Awareness Continuous “
PACE Kenya training needs
Players Type of training When?
University lecturers TOT - PE In place
University students (undergraduates)PE ?
Vets in pastoral areas TOT - PE 2002EpidemiologistsKey NGO staff
Other public, NGO, Private, PE 2002 and beyondCAHWs extension personnel+ VIL teams

Partic ipatory Epidemiology: Lessons Learned and Future Directions 31
It was suggested that general awareness trainingwas also required to familiarise policy makers andfarmers.
The role of the CAPE Unit in training was provisionof expertise, technical back-stopping and funding.
PACE Somalia training needs
In PACE Somalia, PE training needs included staffin the Somalia Livestock Professional Forum(SLPF), National Coordination Unit, ZonalCoordination Units (4) and Zonal ProfessionalAssociations. Private veterinarians under contractto PACE Somalia should also be trained.
PACE Tanzania training needs
Players Training Needs Time Scale CAPE support
Training institutes/ Training of trainers - April 2002 Financial resourcesveterinary schools in new developments for establishment of
of PE; in-depth short course programmeCurriculum development
Research institutes/ Basic training in PE April 2002 Financial otherZonal- disease (short course) resourcesinvestigation centers Advanced training in PE e.g. Trainers
Research methodologies
National Epidemiology Basic and advanced April 2002 Financial otherUnit/Epidemiologists training in PE resources
e.g. Trainers
VICs - zonal vet. Basic training in PE Dec. 2002 FinancialResearch officers Training material
DVOs Basic training in PE April 2003 “
Private vets and Basic training and July 2003 “Livestock Field practice of PEOfficers (LFOs)in the field
CAHWs On-the- job training Continuous “
Livestock farmers Awareness raising Continuous “on-farm
Policy makers Awareness raising July 2002 “
Partic ipatory Epidemiology: Lessons Learned and Future Directions32
Annex 1Workshop timetable
Day 1
Thursday 15th November
8.30 - 9.00am Registration of participants
9.00 - 9.30am WelcomeBackground and objectives of the workshop
9.30 - 10.00am Opening speech by Ato Belay Ejigu Vice Minister, Ministry of Agriculture
10.00 - 10.30am Coffee break
10.30 - 11.30am Presentation “Participatory Epidemiology: Setting the Scene”
11.30 - 12.30am Presentation “Livestock keeping and indigenous knowledge in the Horn of Africa:Personal reflections on 25 years experience”
12.30 - 2.00pm Lunch
2.00 - 3.00pm Issues affecting the wider use of participatory epidemiologyIssue 1. Qualitative verses quantitative methods
3.00 - 3.30pm Tea break
3.30 - 4.30pm Issues affecting the wider use of participatory epidemiologyIssue 2. Methodological issues
4.30 - 4.45pm Summary of Day 1
Day 2
Friday 16th November
9.00 - 11.00am Working Groups by country
9.00 - 10.00am Issues affecting the wider use of participatory epidemiologyIssue 3. Training and practiceSession “The Ideal Qualities of a Participatory Epidemiologist”
10.00 - 10.30am Coffee break
10.30 - 11.00am Where can Participatory Epidemiology fit into PACE? - Introduction
11.00 - 12.30am Improving epizootic disease control using combined participatory and modellingapproaches
12.30 - 2.00pm LunchGroup 1 Group 2Mainly of interest to PACE Mainly of interest to researchersepidemiologists involved and academicsin epizootic disease control
2.00 - 3.00pm Participatory epidemiology Use of participatory approachesand disease surveillance and methods in community-basedanimal health services
3.00 - 3.15pm Tea break Tea break
3.15 - 3.45pm Participatory epidemiology and Participatory epidemiology anddisease surveillance (continued) research: Experiences andopportunities
3.45 - 4.45pm Participatory Disease Searching Participatory epidemiology andveterinary education
4.45 - 5.00pm Summary of Day 2
Partic ipatory Epidemiology: Lessons Learned and Future Directions 33
Day 3
Saturday 17th November
9.00 - 11.00am Working Groups by country- Identify opportunities for using PE to complement national PACE Programmes- Describe specific activities in terms of disease problems to be addressed, priority
geographical areas and key players to be involved in each activity- Identify training needs related to the above. Who should be trained, how should
they be trained?- Outline a work plan for incorporating PE-related activities into each national PACE
programme.
11.00 - 11.30am Coffee break
11.30 - 12.00am Group presentations - PACE Ethiopia
12.00 - 12.30am Group presentations - PACE Somalia
12.30 - 2.00pm Lunch
2.00 - 2.30pm Group presentations - PACE Tanzania
2.30 - 3.00pm Group presentations - PACE Kenya
3.00 - 3.15pm Tea break
3.15 - 3.45pm Group presentations - PACE Uganda
3.45 - 4.15pm Group presentations - Sudan
4.15 - 5.00pm Outstanding issues, Workshop evaluation and close
Partic ipatory Epidemiology: Lessons Learned and Future Directions34
Annex 2List of participants
Mekonnen Hailemariam
Faculty of Veterinary Medicine
Addis Ababa University
Addis Ababa
Ethiopia
Solomon Nega
Ministry of Agriculture
Addis Ababa
Ethiopia
B.M. Mugenyo
Veterinary Services Department Kenya
Kenya
Abdullatif Mohamud Abdi
Somali Livestock Professional Forum
Somalia
Stefano Tempia
PACE Somalia
Nairobi, Kenya
Tesfaye Alemu
Oromia Regional Agricultural Bureau
Ethiopia
Bitew Getinet
Amhara Region Agricultural Bureau
Ethiopia
Bekele Batiso
Bedele PACE Coordinator
Bedele
Ethiopia
A.K. Karugah
Veterinary Service Department Kenya
Kenya
Solomon Mekuria
Awassa PACE Coordinator
Awassa
Ethiopia
Gijs Van’t Klooster
FAO
Ethiopia
Darlington Akabwai
CAPE Unit
Kenya
Tambi Emmanuel
OAU-IBAR-PACE
Economic Unit
Nairobi
Kenya
Ahmed Hussein Abdel Rahman
Veterinary Research Corporation
Sudan
Ali Mohamed Gedi
Somali Livestock Professionals Forum
Somalia
William Amanfu
FAO Rome
Italy
Kaleb Bassa
PACE Communication
Ministry of Agriculture
Addis Ababa
Ethiopia
Beshahwred Shiferaw
PACE Harar Coordinator
Ethiopia
Bryony Jones
VSF Belgium
Sudan
G.W. Nasinyama
Faculty of Veterinary Medicine
Makerere University
Uganda
Dessalegn Sida
Addis Ababa PACE coordinator
Ethiopia
Osman Sorkatti
PACE Headquarters
Sudan
Tariku Sintaro
PACE Ethiopia
Ethiopia
Yirgalem G/meske
EARO (NAHRC- Sebeta)
Ethiopia
Gavin Thomson
OAU/IBAR
PACE Programme
Kenya
Partic ipatory Epidemiology: Lessons Learned and Future Directions 35
B.E Lema
Animal Disease Research Institute,
Ministry of Water and Livestock Development
Tanzania
Hanan Yousif M.A
PACE Epidemology Unit
Sudan
Solomon Tibebu
PACE Ethiopia
National Coordinator Office
Ethiopia
Dr. Mohammed M. Bahari
National PACE Programme Coordination
Ministry of Water and Livestock Development
Department of Veterinary Services
Tanzania
Habiba S.H. Hamid
OAU/IBAR/PACE/CAPE Unit
Somalia
Dawit Abebe
FAO
Addis Ababa
Ethiopia
Francis F. Sudi
Ministry of Water and Livestock Development
PACE Program
Department of Veterinary Services
Tanzania
Daynachew Sahele
PACE Ethiopia
Bahr Dar Coordination Office
Ethiopia
Yohannes Afework
Ministry of Agriculture
Ethiopia
Girma Abeto
PACE Ethiopia
Kombolcha Branch
Ethiopia
Yilkal Asfaw
Faculty of Veterinary Medime,
Addis Ababa University
Ethiopia
Michael Thrusfield
University of Edinburgh
UK
Sileshi Zewdie
PACE - Coordinator
Ministry of Agriculture
Ethiopia
Professor M.M. Kagiko
University of Nairobi
Faculty of Veterinary Medicine
Kenya
Enquebaher Kassaye
Mekelle Regional Veterinary Laboratory
Ethiopia
Maximilian Baumaun
Freie University of Berlin
Germany
Tony Wilsmore
VEERU
University of Reading
UK
Dickens Malangh Chibeu
PACE Epidemiology Unit
Kenya
Mukiibi Muka
LIRI
Uganda
Sharadhuli I. Kimera
Sokoine University
Faculty of Veterinary Medicine
Tanzania
Gebretsadik Berhe
PACE Ethiopia
Mekele Branch Coordinator
Ethiopia
Kebede W/Giorgis
Tigray Region
Ministry of Agriculture
Ethiopia
Kisa Juma Ngeiyna
Veterinary Department
Kenya
F.K. Wandaka
Department of Veterinary Services
Ministry of Agriculture & Rural Development
Kenya
Partic ipatory Epidemiology: Lessons Learned and Future Directions36
John McDermott
International Livestock Research Institute
Nairobi
Kenya
Gerard Laval
International Livestock Research Institute
Addis Ababa
Ethiopia
Kassaye Hadgu
FAO
Addis Ababa
Ethiopia
Chris Rutebarika
PACE Uganda
Uganda
Noelima Nantima
PACE Epidemiology
Uganda
Berhanu Bedane
PACE - OAU/IBAR
Nairobi
Kenya
Kisa Juma Ngeiywa
Kenya Veterinary Department
Kabete
Kenya
Sileshi Zewdie
PACE - Ethiopia Coordinator
Ethiopia
Ali Adam Tahir
Extension Training and Pastoral Development
Sudan
Gezu Bekele
FARM-Africa ADDP
Ethiopia
Yirgalem G/Meskel
National Animal Health Research Center (EARO)
Sebeta
Ethiopia
Girma Abeto
PACE - Ethiopia
Kombolcha Branch Coordinator
Ethiopia
Dessalegn Sida
PACE - Ethiopia
Addis Ababa Branch Coordinator
Ethiopia
Bitew Getinet
Amhara Region
Ethiopia
Yohannes Afework
Ministry of Agriculture
Ethiopia
Yilkal Asfaw
Faculty of Veterinary Medicine
Ethiopia
Bekele Batiso
PACE-Ethiopia
Bedele Branch Coordinator
Ethiopia
Beshahwred Shiferaw
PACE - Ethiopia
Harar Branch Coordinator
Ethiopia
Kebede W/Giorgis
Tigray Region
Ministry of Agriculture
Ethiopia
Enquebaher Kassaye
Mekelle Regional Veteinary Laboratory
Northern Ethiopia
Ethiopia
Salome Kairu Wanyorke
Veterinary Department
Ministry of Agriculture
Kenya
Hanan Yousif M.A
PACE - Sudan
Sudan
Lulseged Belay
BOA, Veterinarian
Afar
Ethiopia
Solomon Tibebu
PACE - Ethiopia
Emergency Unit
Ministry of Agriculture
Ethiopia
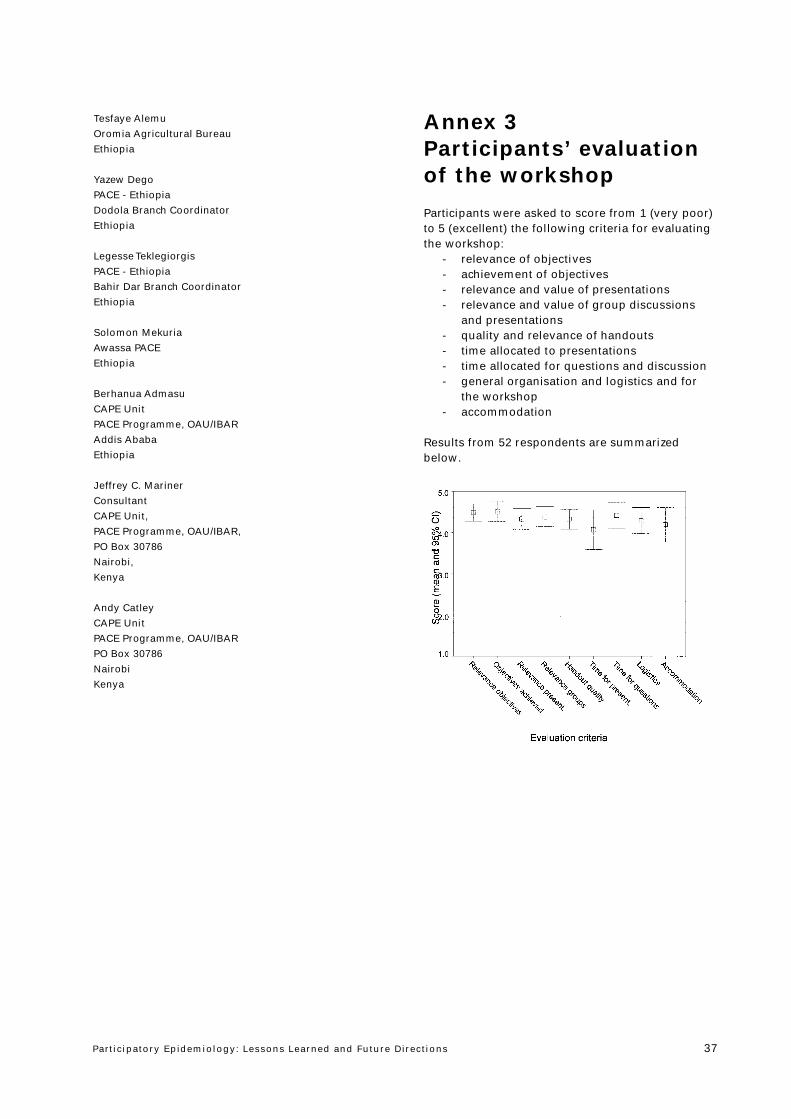
Partic ipatory Epidemiology: Lessons Learned and Future Directions 37
Tesfaye Alemu
Oromia Agricultural Bureau
Ethiopia
Yazew Dego
PACE - Ethiopia
Dodola Branch Coordinator
Ethiopia
Legesse Teklegiorgis
PACE - Ethiopia
Bahir Dar Branch Coordinator
Ethiopia
Solomon Mekuria
Awassa PACE
Ethiopia
Berhanua Admasu
CAPE Unit
PACE Programme, OAU/IBAR
Addis Ababa
Ethiopia
Jeffrey C. Mariner
Consultant
CAPE Unit,
PACE Programme, OAU/IBAR,
PO Box 30786
Nairobi,
Kenya
Andy Catley
CAPE Unit
PACE Programme, OAU/IBAR
PO Box 30786
Nairobi
Kenya
Annex 3Participants’ evaluationof the workshop
Participants were asked to score from 1 (very poor)to 5 (excellent) the following criteria for evaluatingthe workshop:
- relevance of objectives- achievement of objectives- relevance and value of presentations- relevance and value of group discussions
and presentations- quality and relevance of handouts- time allocated to presentations- time allocated for questions and discussion- general organisation and logistics and for
the workshop- accommodation
Results from 52 respondents are summarizedbelow.
PAN AFRICAN PROGRAMME FORTHE CONTROL OF EPIZOOTICSORGANIZATION OF AFRICAN UNITY (OAU) INTER-AFRICAN BUREAU FOR ANIMAL RESOURCES (IBAR)
COMMUNITY-BASED ANIMAL HEALTH &PARTICIPATORY EPIDEMIOLOGY UNIT (CAPE)PO Box 30786 Nairobi, KenyaTel: (254-2) 226447/334550/240591Fax: (254-2) 253680/226565