Embed Size (px)
Citation preview

Procedures
Basic Format
Septoplasty
Objectives
• Assess the anatomy, physiology, and pathophysiology of the Septoplasty.
• Analyze the diagnostic and surgical interventions for a patient undergoing a _______________.
• Plan the intraoperative course for a patient undergoing_____________.
• Assemble supplies, equipment, and instrumentation needed for the procedure.

Objectives
• Choose the appropriate patient position• Identify the incision used for the procedure• Analyze the procedural steps for_____________.• Describe the care of the specimen• Discuss the postoperative considerations for a
patient undergoing _______________ .

Terms and Definitions
• Anosmia• Epistaxis• Hyperosmia• Naris (plural nares)• Nasal (Latin for nose)• Nasal Chonchae
(turbinates)• Nasal septum
• Olfactory• Paranasal sinus• Parosmia• Rhinitis • Rhino• Sinus

Definition/Purpose of Procedure• Excision and resection of the septum to correct any
deviation as a result of injury or a congenital nasal deformity; to improve the functioning capabilities of the nose—to improve breathing
• The cartilaginous or osseous portions of the septum that lie between the flaps of the mucous membrane and the perichondrium are straightened; cartilage & bony spurs may block the meatus and compress the middle turbinate on that side, resulting in an obstruction of the sinus opening
• Other names: nasal septal reconstruction (NSR), submucous resection of the septum (SMR)

Relevant A & P: External nose—lateral and anterior views

Relevant A & P: Nasal Septum & Related Structures
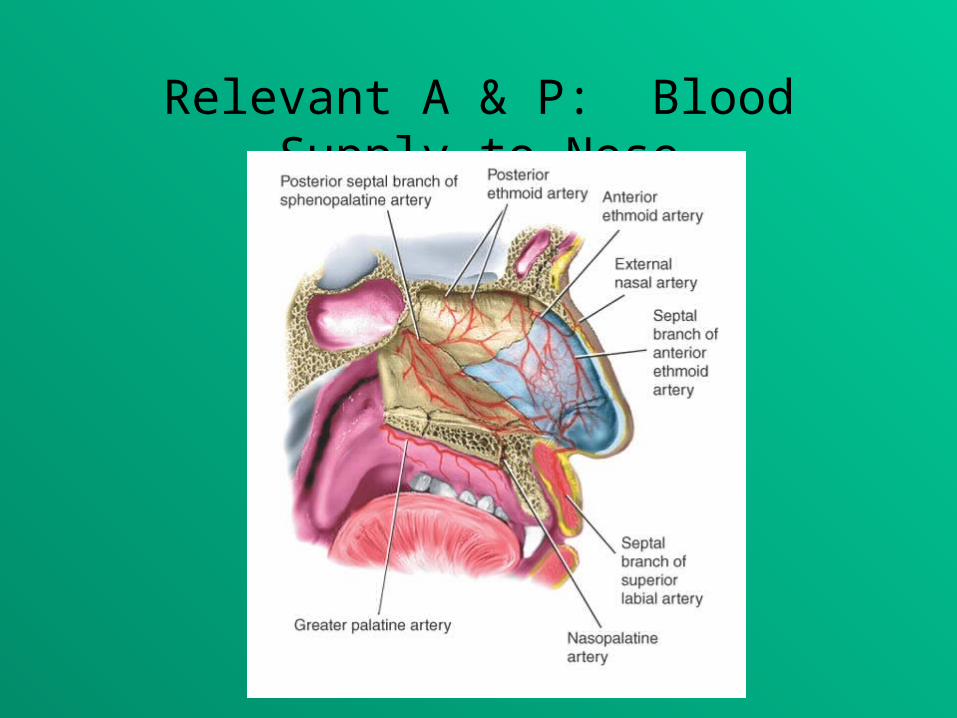
Relevant A & P: Blood Supply to Nose

Pathophysiology
Diagnostics
• Exams– Rhinoscopy: Direct vision
• Preoperative Testing

Surgical Intervention:Special Considerations
• Patient Factors– Pt should know before hand that he/she will be mouthing-
breathing postoperatively because of postop nasal packing 1-3 days post-op
– Pt should understand that application of ice will reduce swelling and brusing around eyes and nose postopertively
– If under local, keep noise to a minimum in the OR– Advise pt to remain still and to expect vibrations caused by bone
remodeling (mallet and osteotome)– Be aware of drapes on face—minimize claustrophobia and
facilitate respiration– This is a clean case—use best technique
• Room Set-up– Surgeon may prefer bed turned to 90 degrees of anesthesia for
greater access to head– Separate Mayo set up for surgeon to use for preop anesthetic and
cocaine nasal packing

Surgical Intervention: Anesthesia
• Method: Local, Regional, General– Local with IV sedation and analgesia is typical– General for the very apprehensive
• Equipment– Note that anesthesia should ensure pt eye
protection using ointment & protective eyewear

Surgical Intervention: Positioning• Position during procedure
– Supine, head tilted back
– HOB may be slightly elevated (reverse Trendelenburg)
– Pt comfort: flex hip and knees w/OR table settings or pillow under knees/lower legs
– Tuck arms to sides; use protective arm sleds and padding
• Supplies and equipment– Foam headrest or donut for head stabilization
• Special considerations: high risk areas– Ulnar nerves where arms are tucked

Surgical Intervention: Skin Prep
• Method of hair removal: N/A• Anatomic perimeters: face—avoid solution from
getting in or near eyes and ears; do not prep interior of nose
• Solution options: may use betadine paint –avoid hibiclens at mucous membranes; may not ask for prep

Surgical Intervention: Draping/Incision• Types of drapes
– Usually turban-type head wrap or 3 towels arranged triangularly
• Order of draping– Remove paper strips from disposable drapes with adhesive
edges– Place bar drape across pt forehead & allow remainder of
drape to fall toward floor covering the head of OR table– Place U-drape on upper lip. Bring edges of U lateral to the
nose and eyes. Extend the rest to cover pt’s body
• Special considerations• State/Describe incision
– Intranasal incision into mucous membrane and perichondrium

Surgical Intervention: Supplies
• General– Head and Neck (ENT) pack; suction tubing, ESU pencil, raytex, 4
pk hand towels, needle magnet, syringe for cleaning suction
• Specific– Suture & Blades: Fine (4-0) absorbable (atraumatic); # 15 x 2– Medications on Mayo stand: Lidocaine w/epi 1: 100, 00 usually
for injection to nares (also have available on back table); Cocaine (1 sm bottle) for nasal packing
– Catheters & Drains– Packing & Nasal splints: may use Iodoform or Vaseline or
Xeroform gauze packing in addition to plastic nasal splint material (plastic or Silastic) post-op. May be manufacturer’s kit.
– 2x2’s and ¼” hypoallergenic tape
Surgical Intervention: Instruments
• General
• Specific (see following slides)

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Instruments

Surgical Intervention: Equipment
• General
• Specific– Operating headlight

Surgical Intervention: Procedure Steps• An incision is made
internally on one side of the nasal septum. After the mucous membrane is elevated away from the bone, obstructive parts of bone and cartilage are removed, and plastic surgery is performed as necessary. Then the mucous membrane is returned to its original position.

Surgical Intervention: Procedure Steps
• Before the surgical scrub, the surgeon will place cocaine-soaked cottonoids into the nares and inject of local anesthetic (usually lidocaine w/epinephrine)* STSR will set up medicine cup, cottonoids, speculum and bayonet
forceps on Mayo for surgeon to pack the nose. The circulator will pour the 4% Cocaine and count cottonoids with the STSR and ensure 27 g.local/needle and Luer-lock syringe is available
• Surgeon opens nostril w/speculum, incises the mucoperichondrium w/nasal knife, then deepens the incision w/ fine, sharp dissecting scissors. * Provide surgeon w/nasal speculum of appropriate size. Have cottle
clamp available to aid incision process. Use # 15 blade on a #7
handle for incision.

Surgical Intervention: Procedure Steps• For retraction, small skin hooks are placed• Surgeon elevates the mucoperichondrium from the septal
cartilage using a fine (Freer) elevator, & removes any spurs from the septum or nasal bone w/nasal/septum cutting forceps (punch, ronguer, or cutting forceps)* Provide suction as needed. Most likely, the sharp end of the Freer
elevator will be used.* Have chisel (or gouge) & mallet available. STSR may be asked to
“tap” the chisel held by the surgeon w/ the mallet. This may not be considered within your scope of practice at your facility—find out before hand.
* Have bayonet or Takahashi forceps available to extract tissue remnants. Surgeon may reinsert bone and cartilage to refashion the nasal cavity and to strengthen weakened areas (keep moist w/NS on the back table in a small basin)

Surgical Intervention: Procedure Steps• With the mucochondrium fully elevated, the surgeon
removes the septal cartilage w/ a nasal forcep. Examines septal tissue & reshapes as needed w/scissors, rasp, or special bone crusher that flattens cartilage.
• Surgeon replaces the septal cartilage within the nose.
• Hemostasis is achieved.
* Have suction, hemostatic agents, &/or ESU pencil available.
• Surgeon closes the incision w/suture &/or hold cartilage in place with packing material (petroleum gauze & nasal splints)
*Have splint material ready—surgeon may cut to fit the patient using Heavy scissors. It may be sutured in place.

Surgical Intervention: Procedure Steps
• Dressing may include external splints and “mustache dressing”
• Secretions are removed from pharynx to reduce risk of aspiration * provide Wieder retractor and Yankauer tip.
• For Turbinectomy

Counts
• Initial: Sponges and sharps (raytex and cottonoids)
• First closing
• Final closing– Sponges– Sharps

Dressing, Casting, Immobilizers, Etc.
• Types & sizes– Mustache dressing –have 2x2’s available and ¼” silk
or micropore tape
– External Splint of surgeon’s preference (eg. Denver splint kit)
• Type of tape or method of securing—least irritating to skin
• Have ice pack available (can make using 2 gloves tied together w/crushed ice)
Specimen & Care
• Identified as nasal cartilage
• Handled: routine in formalin

Postoperative Care
• Destination– PACU– Outpatient Discharge
• Expected prognosis (Good)– Full restoration of nasal function– Return to normal activities about 7 days

Postoperative Care
• Potential complications– Hemorrhage– Infection– Other: Damage to….perforate septum, cause
weakened septum which could lead to future deformity
• Surgical wound classification: II

Resources
• Alexander’s pp. 759-762
• MAVCC Unit 7 OBJ 7, 8, 9, 10, 11
• STST pp. 601-612
• Fuller pp. 616-621
• Goldman p. 443-444; 406-409

Case Studies in Text
Case Studies in STSR Study Guide