Embed Size (px)
DESCRIPTION
prob 3 gastro
Citation preview

GASTROINTESTINAL SYSTEM BLOCK PROBLEM 3
ALMIRA NABILA VALMAI405130193

LO1. Hubungan suhu dengan HR
2. Distensi dengan palpasi dalam
3. Cramp abdominal pain
4. Coated tongue
5. anatomi, histologi, fisiologi saluran cerna bawah
6. Kelainan pada pencernaan bawah

HUBUNGAN SUHU DENGAN HRLO 1

DISTENSI DENGAN PALPASI DALAMLO 2

• Deep palpation of the abdomen is performed by placing the flat of the hand on the abdominal wall and applying firm, steady pressure. It may be helpful to use two-handed palpation (Figure 93.2), particularly in evaluating a mass. Here the upper hand is used to exert pressure, while the lower hand is used to feel. One should start deep palpation in the quadrant directly opposite any area of pain and carefully examine each quadrant. At each costal margin it is helpful to have the patient inspire deeply to aid in palpation of the liver, gallbladder, and spleen.
• Entire abdomen: (6 f’s: fat, flatus, feces, fluid, fetus, fatal cancer): may be sign of obstruction Lower half: pregnancy, full bladder, ovarian tumor, uterine fibroids (common benign growths)

CRAMP ABDOMINAL PAINLO 3
• Cramping is a type of pain that comes and goes (intermittent) or that changes in position or severity. Cramping is rarely serious if it is relieved by passing gas or a stool. Many women have cramping pain with their menstrual periods. Generalized cramping pain is usually not a cause for concern unless it gets worse, lasts for longer than 24 hours, or localizes. Cramping that starts suddenly with diarrhea or other minor health problems can be quite painful but is usually not serious.

COATED TONGUELO 4

• A coated or white tongue occurs when the surface is colonised by bacteria or fungi, and dead cells become trapped between the small nodules on the tongue.

ANATOMI, HISTOLOGI, FISIOLOGI SALURAN PENCERNAAN BAWAH
LO 5


Small Intestine
• 90% of absorption occurs in the small intestine

Small Intestine
• The Jejunum – Is the middle segment of small intestine– 2.5 meters (8.2 ft) long– Is the location of most
• Chemical digestion• Nutrient absorption
– Has few plicae circulares– Small villi


Small Intestine
• The Ileum– The final segment of small intestine– 3.5 meters (11.48 ft) long – Ends at the ileocecal valve, a sphincter that
controls flow of material from the ileum into the large intestine


Small Intestine
• Intestinal Secretions– Watery intestinal juice
– 1.8 liters per day enter
intestinal lumen
– Moisten chyme
– Assist in buffering acids
– Keep digestive enzymes and
products of digestion in
solution
• Intestinal Movements– Chyme arrives in duodenum
– Weak peristaltic contractions move it slowly toward jejunum• Myenteric reflexes
• Not under CNS control
• Parasympathetic stimulation accelerates local peristalsis and segmentation

Coordination of Secretion & Absorption

Coordination of Secretion & Absorption
• Intestinal Absorption – It takes about 5 hours for materials
to pass from duodenum to end of ileum
– Movements of the mucosa increases absorptive
effectiveness• Stir and mix intestinal contents
• Constantly change environment around epithelial cells

Large Intestine
• Is horseshoe shaped
• Extends from end of ileum to anus
• Lies inferior to stomach and liver
• Frames the small intestine
• Also called large bowel
• Is about 1.5 meters (4.9 ft) long and 7.5 cm (3 in.) wide

Large Intestine Functions
– Reabsorption of water – Compaction of
intestinal contents into feces
– Absorption of important vitamins produced by bacteria
– Storage of fecal material prior to defecation

Parts of Large Intestine• The Cecum
– Is an expanded pouch – Receives material arriving
from the ileum– Stores materials and begins
compaction
• Appendix– Also called vermiform appendix
– Is a slender, hollow appendage about 9 cm (3.6 in.) long
– Is dominated by lymphoid nodules (a lymphoid organ)

Parts of Large Intestine
• The Colon– Has a larger diameter and thinner wall than small
intestine – The wall of the colon• Forms a series of pouches (haustra)
– Haustra permit expansion and elongation of colon

Parts of Colon
• Ascending Colon – Begins at superior border of cecum – Ascends along right lateral and posterior wall of peritoneal
cavity to inferior surface of the liver and bends at right colic flexure (hepatic flexure)
• Transverse Colon– Crosses abdomen from right to left; turns at left colic flexure
(splenic flexure)– Is supported by transverse mesocolon– Is separated from anterior abdominal wall by greater omentum

Parts of Colon
• The Descending Colon – Proceeds inferiorly along left side to the iliac fossa (inner
surface of left ilium)– Is retroperitoneal, firmly attached to abdominal wall
• The Sigmoid Colon – Is an S-shaped segment, about 15 cm (6 in.) long– Starts at sigmoid flexure– Lies posterior to urinary bladder– Is suspended from sigmoid mesocolon– Empties into rectum

Parts of Colon



Parts of Large Intestine• The Rectum
– Forms last 15 cm (6 in.) of digestive tract
– Is an expandable organ for temporary storage of feces
– Movement of fecal material into rectum triggers urge to defecate
• The anal canal is the last portion of the rectum– Contains small longitudinal folds called
anal columns • Anus
– Also called anal orifice– Is exit of the anal canal– Has keratinized epidermis like skin


Physiology of the Large Intestine
• Absorption in the Large Intestine– Reabsorption of water
– Reabsorption of bile salts• In the cecum
• Transported in blood to liver
– Absorption of vitamins produced by bacteria
– Absorption of organic wastes

Physiology of the Large Intestine
Three Vitamins Produced in the Large Intestine
1. Vitamin K (fat soluble):• Required by liver for synthesizing four clotting factors, including
prothrombin
2. Biotin (water soluble):• Important in glucose metabolism
3. Pantothenic acid: B5 (water soluble):
• Required in manufacture of steroid hormones and some
neurotransmitters

Physiology of the Large Intestine
• Organic Wastes
– Bacteria convert bilirubin to urobilinogens and
stercobilinogens
– Bacteria break down peptides in feces and generate• Ammonia, Indole & skatole, hydrogen sulfide
– Bacteria feed on indigestible carbohydrates (complex polysaccharides)• Produce flatus, or intestinal gas, in large intestine

Movements of the Large Intestine• Gastroileal & gastroenteric reflexes
– Move materials into cecum while you eat
– Movement from cecum to transverse colon is very slow, allowing hours for water absorption
– Peristaltic waves move material along length of colon
– Segmentation movements (haustral churning) mix contents of adjacent haustra
• Movements from transverse colon through rest of large intestine results from powerful peristaltic contractions (mass movements)
• Stimulus is distension of stomach and duodenum; relayed over intestinal nerve plexuses
• Distension of the rectal wall triggers defecation reflex– Two positive feedback loops– Both loops triggered by stretch
receptors in rectum

KELAINAN SALURAN PENCERNAAN BAWAH
LO 6

DIARRHEA
• Definition– clinically, diarrhea defined as stools that are looser and/or more
frequent than normal; or 24 h stool weight >200 g (physiological definition, less useful clinically)
• Classification– acute vs. chronic– small volume (tablespoons of stool; typical of colonic diseases)
versus large volume (>1/2 cup stool; typical of small bowel diseases)
– watery (bowel disease) vs. steatorrhea– secretory (diarrhea persists with fasting) vs. osmotic (diarrhea
stops with fasting)




ACUTE DIARRHEA• Definition
– passage offrequent unformed stools for <14 d • Etiology
– most commonly due to infections– most infections are self-limiting and resolve within 7 d
• Risk Factors – food (seafood, chicken, turkey, eggs, beef)– medications: antibiotics, laxatives– others: high risk sexual activity, infectious outbreaks, family history (IBD)
• Classification– broadly divided and classified into inflammatory and non-inflammatory diarrhea– mechanisms: stimulation of intestinal water secretion and inhibition of water
absorption (i.e. secretory problem) – in inflammatory diarrhea, organisms and cytotoxins invade mucosa, killing mucosal
cells, further perpetuating the diarrhea


• Investigations – stool cultures/microscopy (C&S/O&P)– C&S only tests Campylobacter, Salmonella, Shigella, E. Coli
other organisms must be ordered separately– flexible sigmoidoscopy: useful if inflammatory diarrhea
suspected – biopsies are the most useful method of distinguishing
idiopathic IBD (Crohn's disease and ulcerative colitis) from infectious colitis or acute self-limited colitis
– C. difficile toxin: indicated when recent/remote antibiotic use, hospitalization, nursing home or recent chemotherapy

• Treatment – Fluid and electrolyte replacement orally in most cases, intravenous if severe extremes of
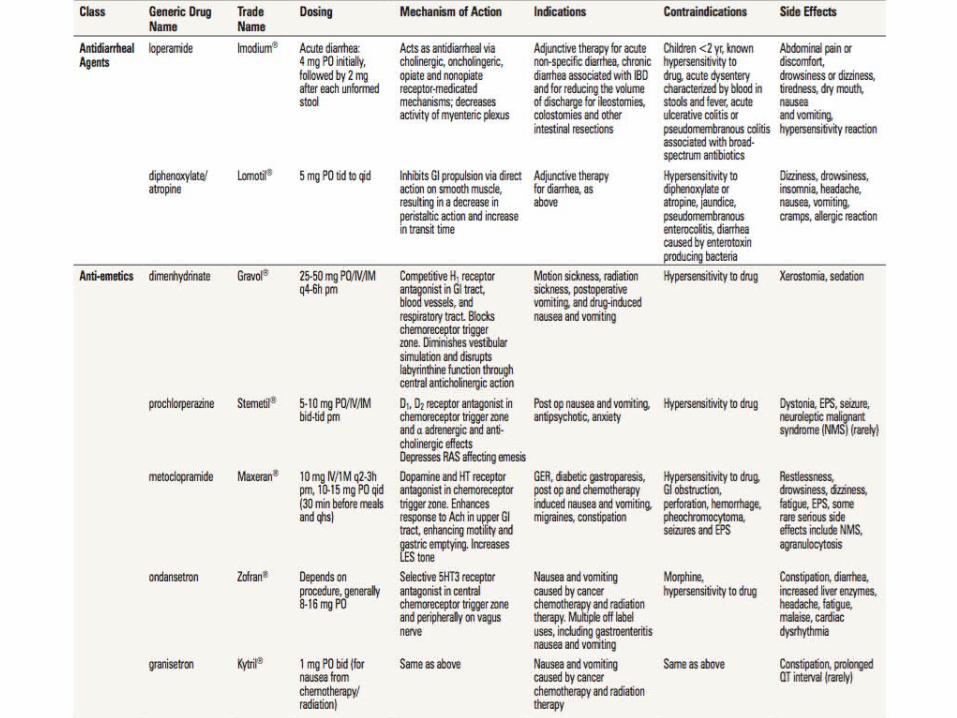
age/coma– anti-diarrheals
• antimotility agents: diphenoxylate, loperamide (Imodium®); contraindicated in mucosal inflammation – side effects: abdominal cramps, toxic megacolon
• absorbants: kaolin/pectin (Kaopectate®), methylcellulose, activated attapulgite– act by absorbing intestinal toxins/micro-organisms, or by coating intestinal mucosa– much less effective than antimotility agent
• modifiers of fluid transport: bismuth subsalicylate (Pepto-Bismol®) may be helpful – antibiotics: rarely indicated
• risks – prolonged excretion of enteric pathogen (especially Salmonella)– drug side effects (including C. difficile infection)– development of resistant strains
• indications for antimicrobial agents in acute diarrhea: – Septicemia – prolonged fever with fecal blood or leukocytes – clearly indicated: Shigella, V. cholerae, C. difficile, traveller's diarrhea (enterotoxigenic E.
coli (ETEC)), Giardia, Entamoeba histolytica, Cyclospora – situational: Salmonella, Campylobacter, Yersinia, non-enterotoxigenic E. coli– Salmonella: always treat Salmonella typhi (typhoid or enteric fever); treat other
Salmonella only if there is underlying immunodeficiency, hemolytic anemia, extremes of age, aneurysms, prosthetic valve grafts/joints, sickle cell disease

CHRONIC DIARRHEA• Definition
– passage of frequent unformed stool for >14 d– differential is similar to that of acute diarrhea, except that the majority of cases are non-
infectious
• Etiology I Classification

• Investigations– Guided by history– stool analysis for: C. difficile toxin, C&S, O&P ± fecal fat, WBC– blood for: CBC, chemistry, CRP, TSH, celiac serology (anti-tTG, protein electrophoresis)– colonoscopy and ileoscopy with biopsy– Small bowel biopsy– upper GI endoscopy with duodenal biopsy– wireless small bowel endoscopy capsule (last resort - very costly)– rial of lactose free diet
• may delay diagnosis of IBD and celiac disease

Maldigestion & malabsorbtion
• Definition – maldigestion: inability to break down large
molecules in the lumen of the intestine into their component small molecules
– malabsorption: inability to transport molecules across the intestinal mucosa to the circulation
– malassimilation: encompasses both maldigestion and malabsorption

• Etiology• Maldigestion
– inadequate mixing of food with enzymes (e.g. post-gastrectomy)– pancreatic exocrine deficiency– primary diseases of the pancreas (e.g. cystic fibrosis, pancreatitis, cancer)– Bile salt deficiency
• terminal ileal disease (impaired recycling), bacterial overgrowth (deconjugation ofbile salts), rarely liver disease (cholestatic)
– specific enzyme deficiencies (e.g. lactase)• Malabsorption
– inadequate absorptive surface– immunologic or allergic injury (e.g. celiac disease)
• infections/infestations (e.g. Whipple's disease, giardiasis)• infiltration (e.g. lymphoma, amyloidosis)• fibrosis (e.g. systemic sclerosis, radiation enteritis)• bowel resection • extensive Crohn's disease
• drug-induced– cholestyramine, ethanol, neomycin, tetracycline and other antibiotics
• Endocrine – e.g. diabetes (complex pathogenesis)
• Clinical Features– Symptoms usually vague unless disease is severe– weight loss, diarrhea, steatorrhea, weakness,
fatigue– manifestations of malabsorption/deficiency


• Investigations– 72 h stool collection (weight, fat content)– serum carotene, folate, Ca2+, Mg2+, vitamin B12, albumin,
ferritin, serum iron solution, INR/PTT– stool fat globules on fecal smear stained with Sudan (rarely
used)– other tests specific for etiology (e.g. CT scan/MRI to
visualize pancreas)– trial of therapy with pancreatic enzymes
• Treatment – dependent on underlying etiology


Celiac Disease (Gluten Enteropathy /Sprue)
• Definition – abnormal small intestine mucosa due to intestinal reaction to gliadin, a component of gluten
• Etiology – only autoimmune disease in which antigen (a.-gliadin) is recognized – associated with other autoimmune diseases, especially thyroid disease – gluten, a protein in cereal grains, broken down to gliadin, is toxic factor – HLA-DQ2 (chromosome 6) found in 80-90% of patients compared with 20% in general – population; also associated with HLA-DQ8
• Epidemiology – more common in women– family history: 15% of first-degree relatives– may present any time from infancy (when cereals introduced) to elderly– peak presentation in infancy
• Clinical Features – classically: diarrhea, weight loss, anemia, symptoms ofvitamin/mineral deficiency, failure to thrive; now
more commonly bloating, gas, iron deficiency – improves with gluten-free diet, deteriorates when gluten reintroduced – disease is usually most severe in proximal bowel – • thus iron, calcium and folic acid deficiency more common than vitamin B12 deficiency – gluten enteropathy may be associated with dermatitis herpetiformis skin eruption, epilepsy, – myopathy, depression, paranoia, infertility, bone fractures/metabolic bone disease

• Investigations – small bowel mucosal biopsy (usually duodenum) is usually diagnostic:
• villous atrophy and crypt hyperplasia• increased number of plasma cells and lymphocytes in lamina propria• increased intraepitheliallymphocytes• similar pathology in: small bowel overgrowth, Crohn's, lymphoma, Giardia, HIV
– consider CT enterography to visualize small bowel to rule out lymphoma– evidence of malabsorption (localized or generalized)
• Steatorrhea • low levels of ferritin/iron saturation, Ca2+ , Fe, albumin, cholesterol, carotene,
B12 absorption– improvement with a gluten-free diet; should not be started before anti-tTG
and biopsy– serological tests
• serum anti-tTG antibody, IgA, is 90-98% sensitive, 94-97% specific• IgA deficient patients have false-negative anti-tTG
– +thus measure serum IgA concomitantly (via serum protein electrophoresis)– fecal fat >7% over 72 h

• Treatment – Dietary counselling
• gluten free diet: avoid barley, rye, wheat– oats allowed if not contaminated by other grains
• rice and corn flour are acceptable• iron, folate supplementation (with supplementation of other vitamins as needed)
– if disappointing response to diet, consider:• incorrect diagnosis • non-adherence to gluten-free diet • unsuspected concurrent disease (e.g. microscopic colitis, pancreatic insufficiency) • development ofintestinal (enteropathy-associated T-cell) lymphoma (abdominal pain, weight
loss, palpable mass) • development ofdiffuse intestinal ulceration, characterized by aberrant intraepithelial T-cell
population (precursor to lymphoma)
• Prognosis – associated with increased risk oflymphoma, carcinoma (e.g. small bowel and colon)– risk of malignancy may be lowered by dietary gluten restriction




Gastroenteritis
Definition • Gastroenteritis is an
inflammation of the lining of the intestines caused by a virus, bacteria or parasites.
Etiology • Virus• Bacteria• Parasites
Source: https://www.nlm.nih.gov/medlineplus/gastroenteritis.html

Virus
• The most common cause of gastroenteritis.• They infect enterocytes in the villous epithelium
of the small bowel. • The result is transudation of fluid and salts into
the intestinal lumen; • Sometimes, malabsorption of carbohydrates
worsens symptoms by causing osmotic diarrhea.
• Diarrhea is mostly watery.

Viruses
• Four categories of viruses cause most gastroenteritis:Rotavirus and norovirus cause the majority of viral gastroenteritis, followed by astrovirus and enteric adenovirus.1. Rotavirus is the most common cause of sporadic, severe, dehydrating diarrhea in young children (peak incidence, 3 to 15 mo).• Rotavirus is highly contagious; most infections occur by the
fecal-oral route.• Adults may be infected after close contact with an infected
infant. The illness in adults is generally mild. Incubation is 1 to 3 days.

Viruses2. Norovirus most commonly infects older children and adults. Infections occur year-round. Norovirus is the principal cause of sporadic viral gastroenteritis in adults and of epidemic viral gastroenteritis in all age groups; large waterborne and food-borne outbreaks occur. Person-to-person transmission also occurs because the virus is highly contagious. Incubation is 24 to 48 h.3. Astrovirus can infect people of all ages but usually infects infants and young children. Infection is most common in winter. Transmission is by the fecal-oral route. Incubation is 3 to 4 days.4. Adenoviruses are the 4th most common cause of childhood viral gastroenteritis. Infections occur year-round, with a slight increase in summer. Children < 2 yr are primarily affected. Transmission is by the fecal-oral route. Incubation is 3 to 10 days.• In immunocompromised patients, additional viruses (eg, cytomegalovirus,
enterovirus) can cause gastroenteritis.


Escherichia coli
• this is a common problem for travelers to countries with poor sanitation. Infection is caused by drinking contaminated water or eating contaminated raw fruits and vegetables.
Campylobacter• the bacteria are found in animal
feces. Infection is caused by, for example, consuming contaminated food or water, eating undercooked meat (especially chicken), and not washing your hands after handling infected animals.
• Azithromycin (500 mg orally one time a day for 3 days) should be first line Rx therapy for symptoms lasting >7days, otherwise self-limited symptomatic therapy recommended.
Bacteria

Salmonella• Bacteria are found in animal feces. • Infection is caused by consuming food
that is contaminated with animal feces
• 8-48 hours incubation• Fever with chills• Nausea and vomiting• Cramping and abdominal pain• Diarrhea often grossly bloody 3-5
days• Tx if not self-limited: Trimethoprim-
sulfamethoxazole, ampicillin, ciprofloxin
Shigella• Fever with chills• Abdominal cramps• Diarrhea often with blood and mucus• Headache, malaise• Direct person-to-person spread• Tx Trimethoprim-sulfamethoxazole,
ciprofloxin, levofloxacin, ampicillin• Increasing resistance to antibiotics
noted• Azithromycin, 500 mg orally on day 1
and 250 mg orally one time a day for 4 days, may be an effective alternative treatment for resistant strains

Cholera • History of travel to endemic areas• Vibrio cholerae• Ingestion in contaminated food• Massive diarrhea-nonbloody,
liquid, gray, “rice water diarrhea”, No odor
• Dehydration occurs quickly• Vaccine available but short-lived• Tx with hydration and antibiotics
– Tetracycline, ampicillin, azithromycin, trimethoprim-sulfamethoxazole, fluoroquinolones
Clostridium difficile• Clostridium difficile • 20% chance after completing broad
spectrum antibiotic• The A and B toxins produced by C.
difficile can cause severe diarrhea, pseudomembranous colitis, or toxic megacolon.
• High risk pts: nursing home residents and employees, hospitalized pts and employees
• metronidazole (250 mg orally four times a day or 500 mg orally three times a day for 10 days)

Cryptosporidium infection• Cryptosporidium parvum causes
watery diarrhea sometimes accompanied by abdominal cramps, nausea, and vomiting.
Entamoeba • Entamoeba
histolytica (amebiasis) is a common cause of subacute bloody diarrhea in the developing world
Parasites

• Giardia infection can be transmitted through water, food, and person-to-person contact.
• Watery yellow, sometimes foul-smelling diarrhea that may alternate with soft, greasy stools, fatigue, abdominal cramps and bloating, nausea, weight loss
• Infections usually clear up within six weeks. But you may have recurrent episodes or have intestinal problems long after the parasites are gone.
• Several drugs are generally effective against giardia parasites, but not everyone responds to them. – Tinidazole 2 g orally as a single dose– Metronidazole (Flagyl) 250mg po tid x 5d
Giardia

Noninfectious causes of diarrhea include
– inflammatory bowel disease, – irritable bowel syndrome, – ischemic bowel disease, – partial small bowel obstruction, – pelvic abscess in the rectosigmoid area,– fecal impaction, – and the ingestion of poorly absorbable sugars,
such as lactulose and acute alcohol ingestion.

Sign & Symptomps Diagnose
Source: http://www.ece.ncsu.edu/imaging/MedImg/SIMS/GE2_1.html
• Based on symptoms• Physical exam• The presence of similar
cases in your community• A rapid stool test
Source: http://www.mayoclinic.org/diseases-conditions/viral-gastroenteritis/basics/tests-diagnosis/con-20019350

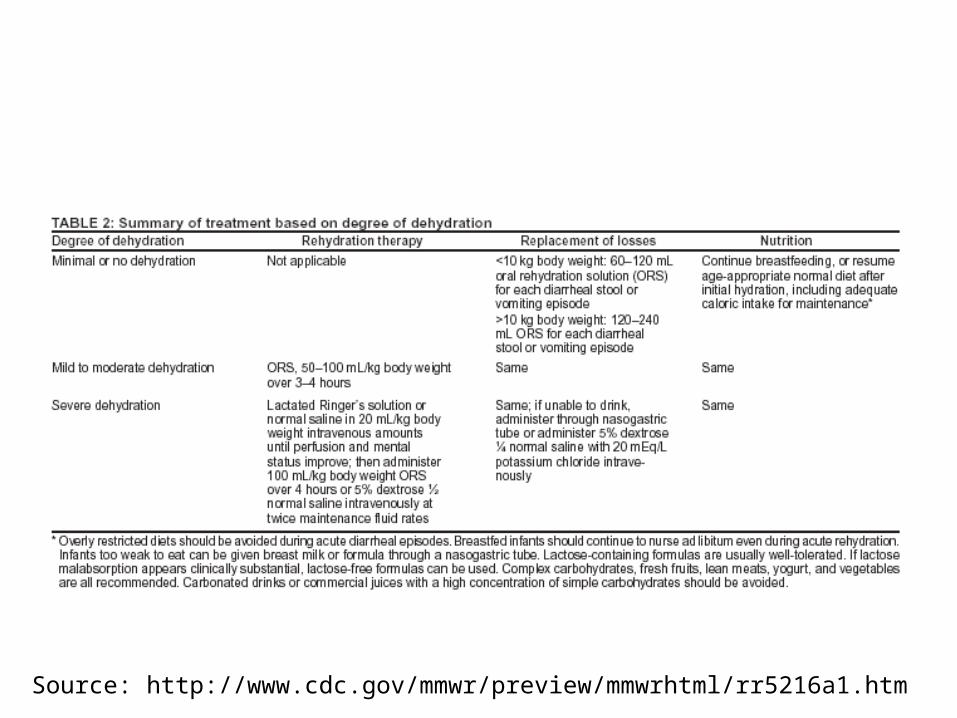
Complication
• Dehydration: the condition that results from excessive loss of body water (Dorland)
Source: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5216a1.htm
Source: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5216a1.htm

Prevention
Source: http://www.cdc.gov/healthywater/pdf/global/programs/Globaldiarrhea508c.pdf

Typhoid & Paratyphoid fever
• Typhoid fever is a disease caused by the bacteria Salmonella Typhi
• Paratyphoid fever is caused by Salmonella Paratyphi
Source: http://www.health.nt.gov.au/library/scripts/objectifyMedia.aspx?file=pdf/76/18.pdf&siteID=1&str_title=Typhoid%20and%20paratyphoid%20fever.pdf


Sign & Symptomps • Early symptoms include fever, general ill-feeling,
and abdominal pain. High fever (103°F, or 39.5°C) or higher and severe diarrhea occur as the disease gets worse.
• Some people with typhoid fever develop a rash called "rose spots," which are small red spots on the abdomen and chest.
• Abdominal tenderness• Agitation• Bloody stools• Chills• Confusion• Difficulty paying attention (attention deficit)• Delirium• Fluctuating mood• Hallucinations• Nosebleeds• Severe fatigue• Slow, sluggish, lethargic feeling• Weakness
Diagnose• A complete blood count (CBC) will show
a high number of white blood cells.• A blood culture during the first week of
the fever can show S. typhi bacteria.• Other tests that can help diagnose this
condition include:• ELISA urine test to look for the bacteria
that cause Typhoid fever• Fluorescent antibody study to look for
substances that are specific to Typhoid bacteria
• Platelet count (platelet count may be low)
• Stool culture
Source: https://www.nlm.nih.gov/medlineplus/ency/article/001332.htm

Prognosis • Symptoms usually improve in
2 to 4 weeks with treatment. The outcome is likely to be good with early treatment, but becomes poor if complications develop.
• Symptoms may return if the treatment has not completely cured the infection.
Complications• Intestinal hemorrhage
(severe GI bleeding)• Intestinal perforation• Kidney failure• Peritonitis
Source: https://www.nlm.nih.gov/medlineplus/ency/article/001332.htm
Treatment • Antibiotic therapy is the only
effective treatment for typhoid fever.
• Commonly prescribed antibiotics– Ciprofloxacin (Cipro). In the United
States, doctors often prescribe this for nonpregnant adults.
– Ceftriaxone (Rocephin). This injectable antibiotic is an alternative for people who may not be candidates for ciprofloxacin, such as children.
Prevention • A vaccine is recommended for travel
outside of the U.S. to places where there is typhoid fever. The Centers for Disease Control and Prevention website has information about where typhoid fever is common. Ask your health care provider if you should bring electrolyte packets in case you get sick.
• When traveling, drink only boiled or bottled water and eat well-cooked food.
• Water treatment, waste disposal, and protecting the food supply from contamination are important public health measures. Carriers of typhoid must not be allowed to work as food handlers.
Source: https://www.nlm.nih.gov/medlineplus/ency/article/001332.htm





























