Embed Size (px)
Citation preview

JJG
Jean-Jérôme GUEX Nice (Fr), Modena (Ita)
IS CHRONIC CEREBRO SPINAL VENOUS
INSUFFICIENCY (CCSVI)
THE SOLE ETIOLOGY OF MULTIPLE
SCLEROSIS (MS) ?
Probably not,
but !

JJG
Conflicts of interest: None in this field.

JJG http://sep-diagnostic.ch/?rub=284
Relapsing Remitting= RR
80% of patients
Secondary Progressive = SP
Primary Progressive = PP
10% of patients
The most severe

JJG
EPIDEMIOLOGIC FEATURES
2.5 millions patients worldwide, the most
frequent chronic neurologic disease in young
adults
Mean age of onset 31 y
2 females Vs 1 male
Higher prevalence in whites of northern europe
ancestry

JJG
SUSPECTED ETIOLOGIES OF MS
environmental factors
Hereditary Predisposition
viral Infection :measles, Epstein-Barr, herpes zoster
Lack of vitamin D
20 genes potentially involved
Tobacco
CCSVI

JJG
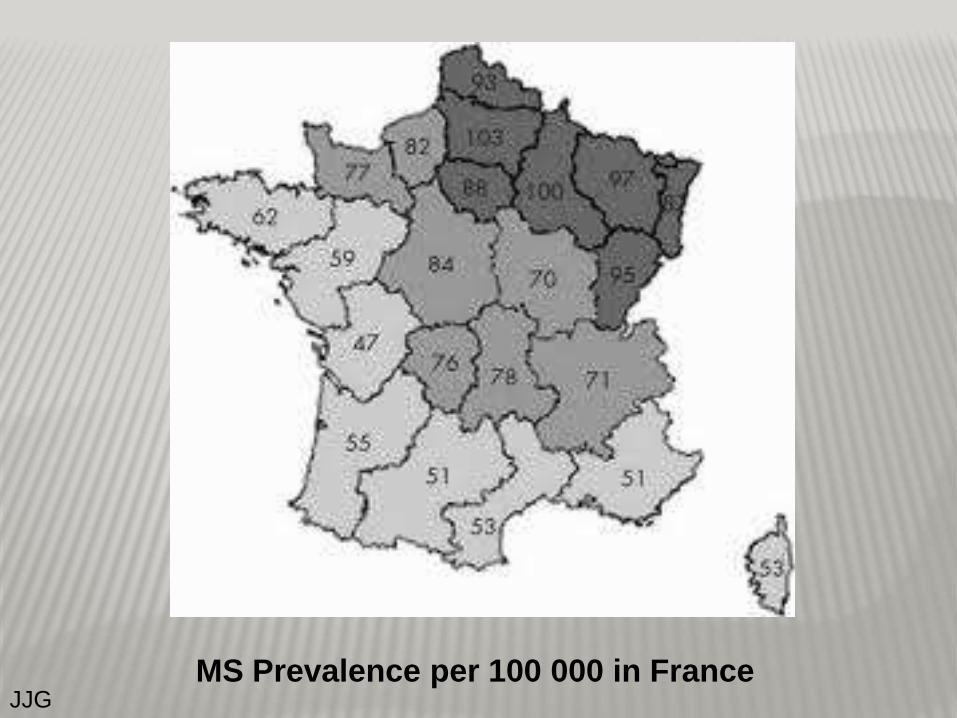
JJG MS Prevalence per 100 000 in France

JJG

JJG
MEDICAL RX (AVAILABLE IN FRANCE)
acute
Solu-Medrol IV
CIS
IFN
RR MS
IFN, Copaxone, Elsep, Tysabri
SP & PP MS
IFN, Elsep, Tysabri, & Nonspecif: azathioprine,
methotrexate, cyclophosphamide, …
JJG
In 2009, at the UIP World Meeting Monaco, Paolo Zamboni organised a session:
« CHRONIC CEREBRO SPINAL VENOUS INSUFFICIENCY and MULTIPLE
SCLEROSIS. »
He described a new pathophysiology and the « liberation treatment »
The effect on the medical community was immediate, as was the buzz on the WEB……

JJG
J Neurol Neurosurg Psychiatry. 2009 Apr;80(4):392-9.
Chronic cerebrospinal venous insufficiency in patients with multiple sclerosis.
Zamboni P, Galeotti R, Menegatti E, Malagoni AM, Tacconi G, Dall'Ara S, Bartolomei I, Salvi F.
BACKGROUND:
The extracranial venous outflow routes in clinically defined multiple sclerosis (CDMS) have not previously
been investigated.
METHODS:
Sixty-five patients affected by CDMS, and 235 controls composed, respectively, of healthy subjects, healthy
subjects older than CDMS patients, patients affected by other neurological diseases and older controls not
affected by neurological diseases but scheduled for venography (HAV-C) blindly underwent a combined
transcranial and extracranial colour-Doppler high-resolution examination (TCCS-ECD) aimed at detecting at
least two of five parameters of anomalous venous outflow. According to the TCCS-ECD screening, patients
and HAV-C further underwent selective venography of the azygous and jugular venous system with venous
pressure measurement.
RESULTS:
CDMS and TCCS-ECD venous outflow anomalies were dramatically associated (OR 43, 95% CI 29 to 65,
p<0.0001). Subsequently, venography demonstrated in CDMS, and not in controls, the presence of multiple
severe extracranial stenosis, affecting the principal cerebrospinal venous segments; this provides a picture of
chronic cerebrospinal venous insufficiency (CCSVI) with four different patterns of distribution of stenosis and
substitute circle. Moreover, relapsing-remitting and secondary progressive courses were associated with
CCSVI patterns significantly different from those of primary progressive (p<0.0001). Finally, the pressure
gradient measured across the venous stenosies was slightly but significantly higher.
CONCLUSION:
CDMS is strongly associated with CCSVI, a scenario that has not previously been described,
characterised by abnormal venous haemodynamics determined by extracranial multiple venous
strictures of unknown origin. The location of venous obstructions plays a key role in determining the
clinical course of the disease

JJG

JJG
J Vasc Surg. 2009 Dec;50(6):1348-58.
A prospective open-label study of endovascular treatment of chronic cerebrospinal
venous insufficiency.
Zamboni P, Galeotti R, Menegatti E, Malagoni AM, Gianesini S, Bartolomei I, Mascoli F, Salvi F.
OBJECTIVE:
Chronic cerebrospinal venous insufficiency (CCSVI) is characterized by combined stenoses of the principal pathways of
extracranial venous drainage, including the internal jugular veins (IJVs) and the azygous (AZY) vein, with development of
collateral circles and insufficient drainage shown by increased mean transit time in cerebral magnetic resonance (MR) perfusion
studies. CCSVI is strongly associated with multiple sclerosis (MS). This study evaluated the safety of CCSVI endovascular
treatment and its influence on the clinical outcome of the associated MS.
METHODS:
Sixty-five consecutive patients with CCSVI, subdivided by MS clinical course into 35 with relapsing remitting (RR), 20 with
secondary progressive (SP), and 10 with primary progressive (PP) MS, underwent percutaneous transluminal angioplasty (PTA).
Mean follow-up was 18 months. Vascular outcome measures were postoperative complications, venous pressure, and patency
rate. Neurologic outcome measures were cognitive and motor function assessment, rate of MS relapse, rate of MR active
positive-enhanced gadolinium MS lesions (Gad+), and quality of life (QOL) MS questionnaire.
RESULTS:
Outpatient endovascular treatment of CCSVI was feasible, with a minor and negligible complication rate. Postoperative venous
pressure was significantly lower in the IJVs and AZY (P < .001). The risk of restenosis was higher in the IJVs compared with the
AZY (patency rate: IJV, 53%; AZY, 96%; odds ratio, 16; 95% confidence interval, 3.5-72.5; P < .0001). CCSVI endovascular
treatment significantly improved MS clinical outcome measures, especially in the RR group: the rate of relapse-free patients
changed from 27% to 50% postoperatively (P < .001) and of MR Gad+ lesions from 50% to 12% (P < .0001). The Multiple
Sclerosis Functional Composite at 1 year improved significantly in RR patients (P < .008) but not in PP or SP. Physical QOL
improved significantly in RR (P < .01) and in PP patients (P < .03), with a positive trend in SP (P < .08). Mental QOL showed
significant improvement in RR (P < .003) and in PP (P < .01), but not in SP.
CONCLUSIONS:
PTA of venous strictures in patients with CCSVI is safe, and especially in patients with RR, the clinical
course positively influenced clinical and QOL parameters of the associated MS compared with the
preoperative assessment. Restenosis rates are elevated in the IJVs but very promising in the AZY, suggesting the need to
improve endovascular techniques in the former. The results of this pilot study warrant a subsequent randomized control study.

JJG
©2009 Society for Vascular Surgery Published by Elsevier, Inc.

JJG
CCSVI: DUS/TCD DEFINITION
Anomalies of
cerebro-spinal drainage :
Stenoses ou occlusions
Reflux
Blocks
Observed on:
V Diameters , Surface areas
variations
Inversions, absences, blocks
reflux
Parietal, valvular Anomalies

JJG
Zamboni’s 5 DUS criteria.
2 POSITIVE CRITERIA OR MORE
- Demonstrate CCSVI
-Indicate the need for selective venogram
of IJV and Azygos.

JJG
Surface VJI
0°(lying.)
S(90°)
CSA(J2) = S(0 )- S(90 ). N >0
Postural dependency of the cerebral venous outflow
Valdueza JM. Lancet 2000;355:200-201
Example: 106-17 = + 89 (mm2)

JJG
The 5 boxes describe the 5 abnormalities included in the proposed ultrasound diagnostic Cleveland Clinic Center for Medical Art & Photography

JJG
J 1
(term.)
J2
(Thyr.)
J 3
(bif.car.)
Internal Jugular Vein
Valve
J1

JJG
IJV dilation in J1, décubitus 0 ; S= 2 cm2
CP

JJG
IJV in J2, sitting position 90 ; S= 0.03 cm2
thyroïde
CP

JJG
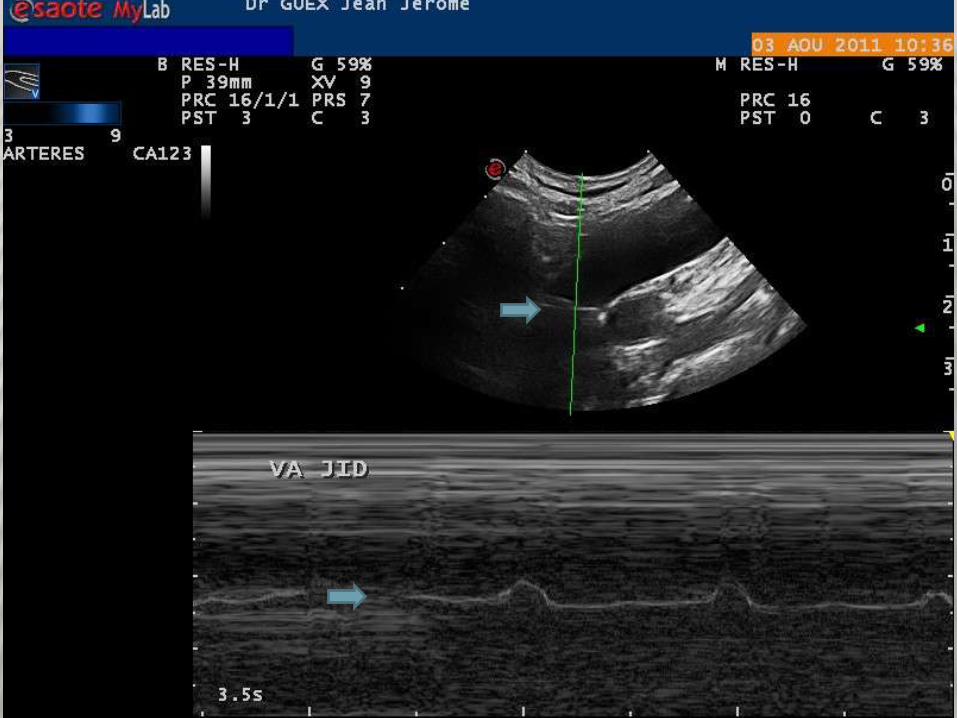
Ultrasound assessment in CCSVI. (a) Triplex scanner, longitudinal access of the
neck in chronic cerebrospinal venous insufficiency multiple sclerosis patient. In the
distal internal jugular vein, close to the junction, the flow is blocked as demonstrated
both by the absence of color and by the Doppler spectrum analysis, with the sample
completely open in the lumen and no angle correction. (b) An immobile intraluminal
defect of the defined septum (multiple arrows) almost completely obstructing the lumen
shows the cause of the hampered venous outflow.
Zamboni ©
JJG

JJG

JJG
Vertebral Vein

JJG

JJG
CEREBRAL VEINS

JJG

JJG
Zamboni P, Galeotti R. The CCSVI syndrome,
Phlebology 2010;23:269-279
The QDP® (Esaote) for detection of intracerebral reflux

JJG
Veine azygos et V. brachiocephaliques échappent à EDV/EDTC

JJG
En débubitus (EDV CE 0 )
Droite
V Jugulaires Internes:
blocage de flux J1 J2 J3 Reflux J1 J2 J3
Flux Normal J1 J2 J3
Anomalie mode B: septum anneau Valve anormale
membrane Hypoplasie autre……………………..
réseau collatéral
V Vertébrales:
flux orthograde en V2 non visualisable en V2
réseau collatéral
Gauche
V Jugulaires Internes:
blocage de flux J1 J2 J3 Reflux J1 J2 J3
Flux Normal J1 J2 J3
Anomalie mode B: septum anneau Valve anormale
membrane Hypoplasie autre……………………..
réseau collatéral
V Vertébrales:
flux orthograde en V2 non visualisable en V2
réseau collatéral

JJG
En position assise (EDV CE 90 )
Droite
V Jugulaires Internes:
blocage de flux J1 J2 J3 Reflux J1 J2 J3
Flux Normal J1 J2 J3
V Vertébrales:
flux orthograde en V2 non visualisable en V2
Collatéralité
ΔCSA positif ΔCSA negatif
Gauche
V Jugulaires Internes:
blocage de flux J1 J2 J3 Reflux J1 J2 J3
Flux Normal J1 J2 J3
V Vertébrales:
flux orthograde en V2 non visualisable en V2
Collatéralité
ΔCSA positif ΔCSA negatif
Examen Echo-Doppler Trans-Crânien (EDTC 0 )
Absence de reflux au niveau des Veines Intra Crâniennes Reflux VIC
JJG
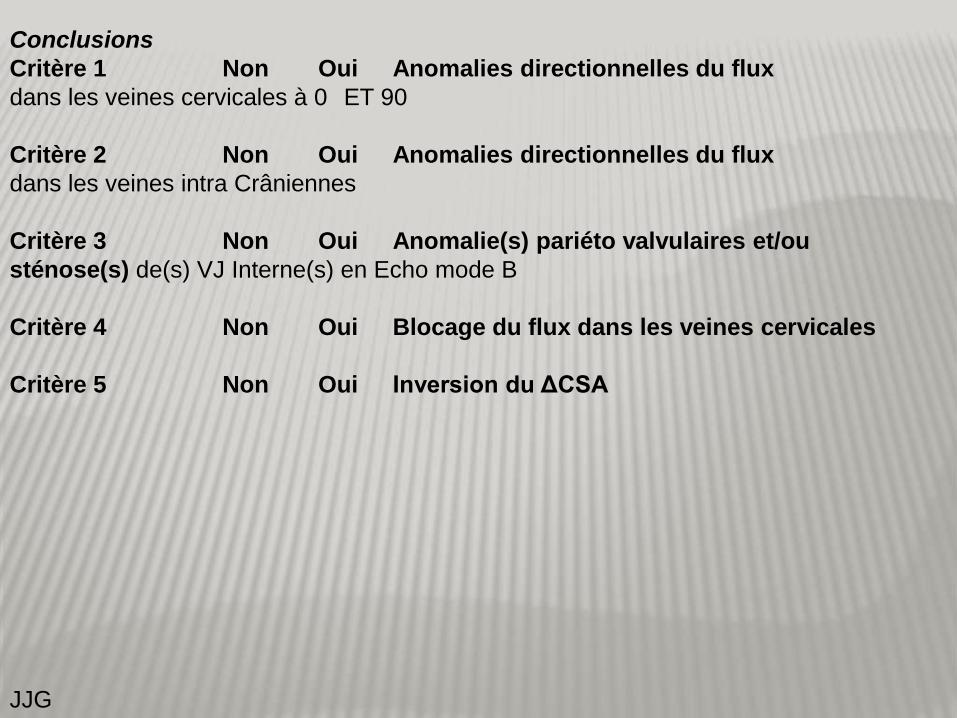
Conclusions
Critère 1 Non Oui Anomalies directionnelles du flux
dans les veines cervicales à 0 ET 90
Critère 2 Non Oui Anomalies directionnelles du flux
dans les veines intra Crâniennes
Critère 3 Non Oui Anomalie(s) pariéto valvulaires et/ou
sténose(s) de(s) VJ Interne(s) en Echo mode B
Critère 4 Non Oui Blocage du flux dans les veines cervicales
Critère 5 Non Oui Inversion du ΔCSA

JJG
SUMMARY ANATOMY, DUS, TCD
IJVs non parallel to Carotids.
3 different segments with different behavior.
Vertebral veins parallel to arteries.
Intracerebral veins can be investigated with TCD
Azygos not visible with DUS.
2 criteria mean CCSVI & mean need for selective
venogram and possible PTA.

JJG
DEMYELINIZATION

JJG
J Cereb Blood Flow Metab. 2009 Dec;29(12):1867-78.
Anomalous venous blood flow and iron deposition in multiple sclerosis.
Singh AV, Zamboni P.
Abstract
Multiple sclerosis (MS) is primarily an autoimmune disorder of unknown origin. This review
focuses iron overload and oxidative stress as surrounding cause that leads to immunomodulation
in chronic MS. Iron overload has been demonstrated in MS lesions, as a feature common with
other neurodegenerative disorders. However, the recent description of chronic cerebrospinal
venous insufficiency (CCSVI) associated to MS, with significant anomalies in cerebral venous
outflow hemodynamics, permit to propose a parallel with chronic venous disorders (CVDs) in the
mechanism of iron deposition. Abnormal cerebral venous reflux is peculiar to MS, and was not
found in a miscellaneous of patients affected by other neurodegenerative disorders characterized
by iron stores, such as Parkinson's, Alzheimer's, amyotrophic lateral sclerosis. Several recently
published studies support the hypothesis that MS progresses along the venous vasculature.
The peculiarity of CCSVI-related cerebral venous blood flow disturbances, together with
the histology of the perivenous spaces and recent findings from advanced magnetic
resonance imaging techniques, support the hypothesis that iron deposits in MS are a
consequence of altered cerebral venous return and chronic insufficient venous drainage.

JJG
DEMYELINATION
JJG
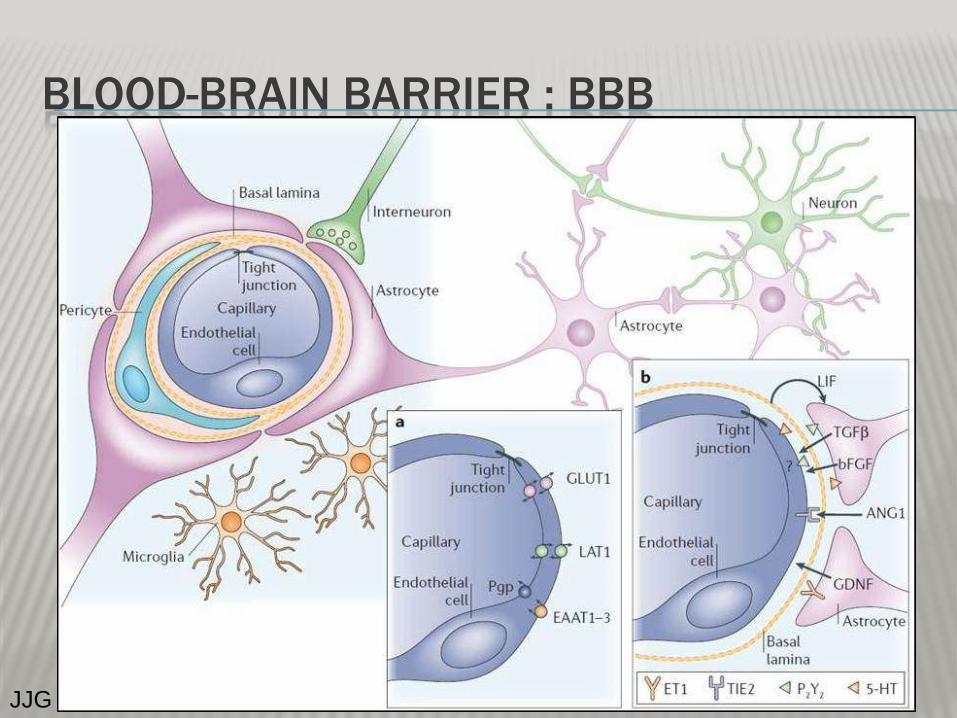
BLOOD-BRAIN BARRIER : BBB

JJG
BUT THIS IS NOT NEW
Arch Pathol Lab Med. 1984 Sep;108(9):755-6.
Iron deposits and multiple sclerosis.
Walton JC, Kaufmann JC.
Abstract
A recent publication described autopsy samples from five brains in which positive staining for iron was
observed as surrounding demyelinated plaques. Because this has not been previously reported, autopsy
material from 13 patients who were being followed up at the Multiple Sclerosis (MS) Clinic, University
Hospital, The University of Western Ontario, London, Ontario, was reviewed. A total of 32 paraffin-embedded
blocks containing demyelinated plaques of varying age were sectioned and stained using a standard acid
ferrocyanide technique (Peris' test) for iron. Microscopic examination failed to detect the presence of
significant positive staining either within or surrounding the areas of demyelination. Positive
histochemical staining for iron identifies hemosiderin, the presence of which suggests either
iron overload or remote hemorrhage. Support for these two processes in the pathogenesis of MS could not
be provided from our material.

JJG
BMC Med. 2011 Mar 7;9:22.
Hypoperfusion of brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple sclerosis: a cross-sectional
preliminary report.
Zamboni P, Menegatti E, Weinstock-Guttman B, Dwyer MG, Schirda CV, Malagoni AM, Hojnacki
D, Kennedy C, Carl E, Bergsland N, Magnano C, Bartolomei I, Salvi F, Zivadinov R.
Abstract
BACKGROUND:
Several studies have reported hypoperfusion of the brain parenchyma in multiple sclerosis (MS) patients. We hypothesized a
possible relationship between abnormal perfusion in MS and hampered venous outflow at the extracranial level, a condition
possibly associated with MS and known as chronic cerebrospinal venous insufficiency (CCSVI).
METHODS:
We investigated the relationship between CCSVI and cerebral perfusion in 16 CCSVI MS patients and 8 age- and sex-matched
healthy controls. Subjects were scanned in a 3-T scanner using dynamic susceptibility, contrast-enhanced, perfusion-weighted
imaging. Cerebral blood flow (CBF), cerebral blood volume (CBV) and mean transit time (MTT) were measured in the gray matter
(GM), white matter (WM) and the subcortical GM (SGM). The severity of CCSVI was assessed according to the venous
hemodynamic insufficiency severity score (VHISS) on the basis of the number of venous segments exhibiting flow abnormalities.
RESULTS:
There was a significant association between increased VHISS and decreased CBF in the majority of examined regions of the
brain parenchyma in MS patients. The most robust correlations were observed for GM and WM (r = -0.70 to -0.71, P < 0.002 and
P corrected = 0.022), and for the putamen, thalamus, pulvinar nucleus of thalamus, globus pallidus and hippocampus (r = -0.59 to
-0.71, P < 0.01 and P corrected < 0.05). No results for correlation between VHISS and CBV or MTT survived multiple comparison
correction.
CONCLUSIONS:
This pilot study is the first to report a significant relationship between the severity of CCSVI and
hypoperfusion in the brain parenchyma. These preliminary findings should be confirmed in a larger
cohort of MS patients to ensure that they generalize to the MS population as a whole. Reduced
perfusion could contribute to the known mechanisms of virtual hypoxia in degenerated axons.

JJG
Perfusion MRI study. Cerebral blood flow
- A: CBF in a 33-year-old, RR CCSVI-MS patient with a venous hemodynamic
insufficiency severity score (VHISS) of 5.
-B: CBF in a 38-year-old, RR CCSVI-MS patient with a VHISS of 12. The dark areas
indicate lower CBF in the patient with higher VHISS.
CAUSE OR CONSEQUENCE??
Zamboni ©

JJG
DISCUSSION: IMPORTANCE OF CCSVI
DUS criteria of CCSVI discussed and disputable (Thapar et al. Phlebology 2011 )
Operator dependant
Machine dependant (QDP Esaote®)
Less specific than described ?
CCSVI not very popular among Neurologists…
What is the role of industry ?
Importance of the WEB ?

JJG
Cavo-spinal phlebography in myelopathies. Stenoses of internal jugular
and azygos veins, venous compressions and thromboses
by H Leriche, M L Aubin, J Aboulker
Acta radiologica Supplementum (1976)
Volume: 347, Pages: 415-417
“Increased intraspinal venous pressure, resulting according to ABOULKER in
numerous spastic paraplegias and quadriplegias is due to multiple venous
abnormalities demonstrated by cavo-spinal phlebography. The most frequent
are stenoses of the internal jugular veins, the left renal, the left iliac veins, the
azygos veins and compressions of the innominate venous trunks. These
abnormalities cause a permanent stasis in the intraspinal plexuses through
excessive supply or insufficient drainage. Out of 80 patients, 60 per cent had
at least 2 abnormalities, 38 per cent at least 3 abnormalities.”
They already carried out PTAs with coronary catheters. However, they had
bad outcomes….
JJG
Studies contradicting Zamboni’s research, (Doepp, Baracchini, Wattjes,
Mayer, etc … ), are limited to small cohorts(20-30 subjects) and their
methodology is not appropriate.
Mayer CA et al: The perfect crime? CCSVI not leaving a trace in MS. J Neurol Neurosurg Psychiatry
2011;82:436-440
Baracchini C. et al. No Evidence of Chronic Cerebrospinal Venous Insufficiency at Multiple Sclerosis
Onset. Ann Neurol 2011;69:90–99
Doepp F et al. No Cerebrocervical Venous Congestion inPatients with Multiple Sclerosis Ann
Neurol2010;68:173–183
Wattjes mp et al, No association of abnormal cranial venous drainage with multiple sclerosis: a magnetic
resonance venography and flow-quantification study. J Neurol Neurosurg Psychiatry 2011;82:429-435.
Zivadinov’s study of 499 subjects finds the same trend as Zamboni’s
differences in figures may be explained by technology and protocol
differences (QDP).

JJG
0
10
20
30
40
50
60
MS CIS OND HEALTHY
Série1
Pourcentages de sujets présentant une CCSVI
MS = multiple sclerosis
CIS = Clinically Isolated Syndrome
OND = Other Neurologic Diseases
From Zivadinov

JJG
BACKGROUND: Chronic cerebrospinal venous insufficiency (CCSVI) was recently described in patients with
multiple sclerosis (MS). A subject is considered CCSVI positive if ≥2 venous hemodynamic (VH) criteria are
fulfilled.
OBJECTIVE: To determine prevalence of CCSVI in a large cohort of patients with MS, clinically isolated
syndrome (CIS), other neurologic diseases (OND), and healthy controls (HC), using specific proposed echo-
color Doppler (ECD) criteria.
METHODS: Transcranial and extracranial ECD were carried out in 499 enrolled subjects (289 MS, 163 HC, 26
OND, 21 CIS). Prevalence rates for CCSVI were calculated in 3 ways: first, using only the subjects for whom
diagnosis was certain (i.e., borderline subjects were excluded); secondly, including the borderline subjects in the
"no CCSVI" group; and finally, taking into account subjects who presented any of the VH criteria.
RESULTS: CCSVI prevalence with borderline cases included in the "no CCSVI" group was 56.1% in MS, 42.3%
in OND, 38.1% in CIS, and 22.7% in HC (p < 0.001). The CCSVI prevalence figures were 62.5% for MS, 45.8%
for OND, 42.1% for CIS, and 25.5% for HC when borderline cases were excluded (p < 0.001). The prevalence of
one or more positive VH criteria was the highest in MS (81.3%), followed by CIS (76.2%), OND (65.4%), and HC
(55.2%) (p < 0.001). CCSVI prevalence was higher in patients with progressive than in nonprogressive MS (p =
0.004).
CONCLUSIONS: Our findings are consistent with an increased prevalence of
CCSVI in MS but with modest sensitivity/specificity. Our findings point against
CCSVI having a primary causative role in the development of MS.
Zivadinov R, Marr K, Cutter G, Ramanathan M, Benedict RH, Kennedy C, Elfadil M, Yeh AE, Reuther J, Brooks C,
Hunt K, Andrews M, Carl E, Dwyer MG, Hojnacki D, Weinstock-Guttman B.
Prevalence, sensitivity, and specificity of chronic cerebrospinal venous insufficiency in MS.
Neurology. 2011 Jul 12;77(2):138-44

JJG
ASSOCIATION BETWEEN CHRONIC CEREBROSPINAL VENOUS
INSUFFICIENCY AND MULTIPLE SCLEROSIS: A META-ANALYSIS.
Laupacis A, Lillie E, Dueck A, Straus S, Perrier L, Burton JM, Aviv
R, Thorpe K, Feasby T, Spears J.
CMAJ. 2011 NOV 8;183(16) 1203-12
O.R. 13.5 (2.6-71.4)
13.5 fold risk of having a CCSVI when suffering
from MS
CCSVI is found in 70% of MS patients
Vs 20% of controls Zamboni says.
(ACP Nov 2011)

JJG
DISCUSSION : ETIOLOGY
CCSVI is involved somewhere in MS, certainly a
predisposing factor, maybe an aetiology
The actual cause of MS (sole ?) may be
different (auto-immune / viral/ other ?)
CCSVI may be involved also in transverse
Myelitis, Migraines ?
None of the epidemiological data is
contradictory with CCSVI
JJG
DISCUSSION: ETIOLOGY
Dolic K et al. (Buffalo/ Zivadinov’s team)
recently published (PLoS ONE November 2011)
that risk factors for CCSVI are similar to MS risk
factors. These observations deserve further
analysis.
JJG
DISCUSSION: SAFETY ISSUES
Efficacy of PTA on QoL, clinical signs and MRI is
observed
No dedicated/appropriate stents are available so far
Safety: Mandato (Albany, USA)
231 patients MS had a PTA +/- stent. 97% without
secondary effect. To compare with medical rx: Natalizumab
(Tysabri) 8 deaths from progressive multifocal
leukoencephalopathy.
INDICATION
Society of Interventional Radiology Statement:
« (…)preliminary research is very promising and supports
studies aimed at understanding the role of CCSVI in MS
(…) »

JJG
CONCLUSIONS 1
Paolo ZAMBONI and his team
- Have updated ancient observations (H Leriche, M L
Aubin, J Aboulker. 1976)
- Have modelized CCSVI
- Have identified a pathophysiological mechanism
responsible for cellular lesions of MS
- Have described DUS and TCD diagnosis of CCSVI in MS
- Have updated indications of selective venogram and/or
PTA of IJVs and Azygos in patients with CCSVI and MS.

JJG
CONCLUSIONS 2
DUS and TCD diagnosis of CCSVI must be carried out
only by trained physicians and/or RV Techs.
The protocol has been recently defined and refined
(Zamboni et al. Int Angiol 2011; 30(6): 571-597)
MRV does not seem to be a valuable alternate option
for diagnosis (Simka)

JJG
CONCLUSIONS 3
Results of RCTs are expected and needed, comparison
with SHAM interventions, although recommended by
the NICE, is (for us) ethically disputable.
The so called « liberation treatment » is a
compassionate treatment which is less dangerous,
offers better results, has less side effects, and a lower
cost than most specific drugs.
The CCSVI mechanism may not explain the whole MS
but it has helped improving the situation of a number
of patients !

JJG
BREAKING NEWS:
Multiple sclerosis: a chronic infective
cerebrospinal venulitis? P K Thibault
Published online on 12 January 2012 Phlebology, doi:
10.1258/phleb.2011.011068 (…) hypothesis that the pathogenesis of the venous disease could be initiated
by a respiratory infective agent such as Chlamydophila pneumonia,
which causes a specific chronic persistent venulitis affecting the cerebrospinal
venous system. Secondary spread of the agent would initially be via the lymphatic
system to specifically involve the azygos, internal jugular and vertebral veins. The
hypothesis proposes mechanisms by which an infective venous vasculitis could
result in the specific neural damage, metabolic, immunological and vascular effects
observed in MS.

JJG





























