Embed Size (px)
Citation preview

Priority Medicines for Europe and the World
Warren Kaplan
Richard Laing
November 2004
World Health Organization Department of Essential Drugs and Medicines Policy
WHO/EDM/PAR/2004.7

© World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. The World Health Organization does not warrant that the information contained in this publication is complete and correct and shall not be liable for any damages incurred as a result of its use. The named authors alone are responsible for the views expressed in this publication.
Contents Acknowledgements.................................................................................................................................. i Acronyms .................................................................................................................................................iii Preface.........................................................................................................................................................v
Context ...............................................................................................................................................................v The importance of prevention ........................................................................................................................vi Methods used in this Report ...........................................................................................................................vi Limitations and areas not addressed .............................................................................................................vi
Executive summary ................................................................................................................................ ix Purpose and objectives .................................................................................................................................... ix Background ....................................................................................................................................................... ix Priority‐setting ................................................................................................................................................... x Methods .............................................................................................................................................................. x Results ............................................................................................................................................................... x Cross‐cutting issues........................................................................................................................................xiv New approaches to promoting innovation .................................................................................................xiv Key conclusions ...............................................................................................................................................xv
1. Introduction..........................................................................................................................................1 1.1 Context ................................................................................................................................................. 1 1.2 Pharmaceutical gaps: a public health perspective .......................................................................... 1 1.3 The epidemiological transition and the ʺcommonality of interestʺ .............................................. 2 1.4 Conceptual framework....................................................................................................................... 2 1.5 Structure of the Project ....................................................................................................................... 3 1.6 Who is the target audience for this Report? .................................................................................... 4 1.7 Contents of the Report........................................................................................................................ 5 1.8 Areas not addressed by this study.................................................................................................... 5
2. Background to the Priority Medicines Project ...............................................................................7 2.1 Introduction ......................................................................................................................................... 7 2.2 History of pharmaceutical innovation ............................................................................................. 7 2.3 The European pharmaceutical industry in context ........................................................................ 9 2.4 Pammolli and G‐10 Reports and EU Communication ................................................................. 11 2.5 The Lisbon and Barcelona European Councils: the “3% solution”............................................. 11 2.6 Regulatory agency responses by EMEA and FDA concerning innovation............................... 12 2.7 The Framework Programmes.......................................................................................................... 13 2.8 European and Developing Countries Clinical Trials Partnership .............................................. 14 2.9 National payment systems .............................................................................................................. 15
3. Approaches to priority‐setting ........................................................................................................17 3.1 Introduction ....................................................................................................................................... 17 3.2 International approaches to priority‐setting ................................................................................. 17 3.3 Private sector prioritization methods............................................................................................. 19 3.4 Conceptual framework for the Priority Medicines Project.......................................................... 19 3.5 Providing a “menu” of complementary approaches for policy‐makers.................................... 20 3.6 Conclusion ......................................................................................................................................... 22
4. Methods used in the Priority Medicines Project .........................................................................23 4.1 Introduction ....................................................................................................................................... 23 4.2 Methodology ..................................................................................................................................... 23 4.3 Approach based on projections and trends ................................................................................... 27 4.4 Approach based on social solidarity .............................................................................................. 28 4.5 Reviewing the Preliminary List: in‐depth reviews based on the Global Forum for Health
Research approach............................................................................................................................ 28

5. Development of a Preliminary List of Priority Diseases...........................................................31 5.1 Introduction ....................................................................................................................................... 31 5.2 Demographic indicators................................................................................................................... 31 5.3 Burden of disease .............................................................................................................................. 32 5.4 EU and the world (commonality of interest)................................................................................. 34 5.5 Assessing treatment efficacy for acute and chronic high burden diseases/conditions ............ 37 5.6 Priorities based on projections and trends..................................................................................... 44 5.7 Priorities based on social solidarity ................................................................................................ 44 5.8 Summary tables................................................................................................................................. 45
6. Priority diseases and reasons for inclusion ..................................................................................47 6.1 Antibacterial drug resistance........................................................................................................... 48 6.2 Pandemic influenza .......................................................................................................................... 53 6.3 Cardiovascular disease secondary prevention.............................................................................. 57 6.4 Diabetes .............................................................................................................................................. 60 6.5 Cancer................................................................................................................................................. 62 6.6 Acute stroke....................................................................................................................................... 63 6.7 HIV/AIDS........................................................................................................................................... 64 6.8 Tuberculosis....................................................................................................................................... 66 6.9 Neglected diseases ............................................................................................................................ 68 6.10 Malaria................................................................................................................................................ 70 6.11 Alzheimer disease ............................................................................................................................. 71 6.12 Osteoarthritis ..................................................................................................................................... 73 6.13 Chronic obstructive pulmonary disease ........................................................................................ 74 6.14 Alcohol use disorders: alcoholic liver diseases ............................................................................. 76 6.15 Depression in the elderly and adolescents .................................................................................... 77 6.16 Postpartum haemorrhage and maternal mortality....................................................................... 79 6.17 Smoking cessation............................................................................................................................. 80
7. Cross‐cutting themes.........................................................................................................................87 7.1 Medicine delivery mechanisms....................................................................................................... 87 7.2 Pharmaceuticals and the elderly ..................................................................................................... 90 7.3 Pharmaceuticals and children ......................................................................................................... 91 7.4 Pharmaceuticals and women........................................................................................................... 93 7.5 Orphan diseases ................................................................................................................................ 95
8. New approaches to promoting innovation ...................................................................................99 8.1 Public‐private partnerships ........................................................................................................... 100 8.2 Determining value for innovation and setting prices ................................................................ 103 8.3 Barriers to innovation in pharmaceutical research and development ..................................... 109 8.4 Comparative effectiveness of medicines and use of “head‐to‐head” comparative trials ...... 112 8.5 Technology Platform for the Pharmaceutical Industry.............................................................. 113
9. Conclusions and recommendations .............................................................................................117 Introduction ................................................................................................................................................... 117 Major recommendations............................................................................................................................... 117 Promoting innovation through pricing and regulatory reforms............................................................. 120 Detailed recommendations .......................................................................................................................... 121 Therapeutic improvement through improved pharmaceutical delivery mechanisms ........................ 124 Special groups................................................................................................................................................ 125 Innovative responses to market deficiencies ............................................................................................. 126 Information technology and pharmaceutical innovation......................................................................... 127 Increasing patient involvement in health policy ....................................................................................... 128 Technology platform for the pharmaceutical industry ............................................................................ 129
Glossary..................................................................................................................................................131

i
Acknowledgements With the acknowledgement that consensus was not reached on all issues, the authors are indebted to the members of the Priority Medicines for Europe and the World Consultative Group for their support and advice: Mr Tom Andersen (European Investment Bank), Dr Edvard Beem (ZonMw, the Netherlands Organisation for Health Research and Development), Dr Jorge Bermudez (Fundaçao Oswaldo Cruz, National School of Public Health, Rio de Janeiro), Dr Margreet Brandsma (ZonMw), Mr Louis Currat (Global Forum for Health Research), Dr Andres de Francisco (Global Forum for Health Research), Ms Spring Gombe (Health Action International – Europe), Dr Martijn ten Ham (Ministry of Health, Welfare and Sport, the Netherlands), Dr Jan Willem Hartgerink (Ministry of Health, Welfare and Sport, the Netherlands), Professor David Henry (University of Newcastle, Australia), Ms Ellen ‘t Hoen (Médecins Sans Frontières), Ms Elisabetta El‐Karimy (ZonMW), Professor Hubert Leufkens (Utrecht Institute for Pharmaceutical Sciences), Ms Monique Middelhoff (Permanent Mission of the Kingdom of the Netherlands, Geneva), Dr Gill Samuels (Pfizer Limited), Mr Bart Wijnberg (Ministry of Health, Welfare and Sport, the Netherlands), Mr Stephen Wright (European Investment Bank). WHO participants in the Consultative Group: Dr Rafael Bengoa (Management of Noncommunicable Diseases), Dr Hans Hogerzeil (Essential Drugs and Medicines Policy), Mr Kees de Joncheere (WHO Regional Office for Europe), Dr Vladimir Lepakhin (Health Technology and Pharmaceuticals), Dr Shanthi Mendis (Chronic Diseases and Health Promotion), Dr Tikki Pang (Research Policy and Cooperation), Dr Jonathan Quick (Essential Drugs and Medicines Policy), Dr Rob Ridley (Special Programme for Research and Training in Tropical Diseases), Dr Eduardo Sabate (Management of Noncommunicable Diseases). We thank all those who wrote the background papers to this Report. The named authors alone are responsible for the content of these documents. The Reportʹs authors are grateful to the many people who reviewed previous drafts of this document and the background papers. Their comments were invaluable. However, final responsibility for the content of this Report rests with the two authors. Special thanks are due to Ms Marjolein Willemen (University of Utrecht) for her technical assistance in researching and compiling the Report and to Ms Sheila Davey for editing the text. The authors also wish to thank Ms Lisa Greenough, Mrs Kathleen Hurst and Ms Monique Renevier (WHO, Department of Essential Drugs and Medicines Policy) for their administrative support and work on the layout and production processes.

ii
WHO expresses appreciation to the Government of the Netherlands for its financial support to the study. For further information contact: Dr Richard Laing, Department of Essential Drugs and Medicines Policy, World Health Organization, 1211 Geneva 27, Switzerland. E‐mail: [email protected]. Details of all Department of Essential Drugs and Medicines Policy publications, including others in this Research Series, can be obtained from the EDM Documentation Centre. E‐mail: [email protected], fax: + 41 22 791 41 67.

iii
Acronyms ACE Angiotensin converting enzyme ACP Africa, Caribbean, Pacific AD Alzheimer disease AIDS Acquired immunodeficiency syndrome AMR Antimicrobial resistance BPCA Best Pharmaceuticals for Children Act (USA) CDC Center for Disease Control and Prevention (USA) CDER Center for Drug Evaluation and Research (USA) COHRD Commission on Health Research for Development COPD Chronic obstructive pulmonary disease CVD Cardiovascular disease DALY Disability adjusted life year DDD Defined daily dose DG Directorate General (European Union) DG SANCO Directorate General for Health and Consumer Affairs
(European Union) DNDi Drugs for Neglected Diseases initiative DNA Deoxyribonucleic acid EDCTP European and Developing Countries Clinical Trials Partnership EMEA European Medicines Agency (until May 2004 known as the
European Agency for the Evaluation of Medicinal Products) EMR Electronic medical records EU European Union EU10 New EU Member States (May 2004) EU15 EU Member States (prior to May 2004) EU25 Expanded EU (after May 2004) FDA Food and Drug Administration (USA) FDC Fixed‐dose combination FP Framework Programme GDP Gross domestic product GNI Gross national income GNIPC Gross national income per capita HAART Highly active antiretroviral therapy HIV Human immunodeficiency virus HFA Health For All HRT Hormone replacement therapy IAVI International AIDS Vaccine Initiative IDU Injecting drug user IFPMA International Federation of Pharmaceutical Manufacturers
Associations IHD Ischaemic heart disease IP Intellectual property IT Information technology

iv
IVF In‐vitro fertilization LAIV Live, attenuated influenza vaccine LRI Lower respiratory tract infection MMV Medicines for Malaria Venture MRSA Methicillin‐resistant Staphylococcus aureus NGO Nongovernmental organization NICE National Institute for Clinical Excellence (United Kingdom) NIH National Institutes of Health (USA) NME New molecular entity NNT Number needed to treat OA Osteoarthritis OAI Osteoarthritis Initiative OECD Organisation for Economic Co‐operation and Development OOPD Office of Orphan Products Development (USA) OTC Over‐the‐counter PPH Postpartum haemorrhage PPP Public‐private partnership RCT Randomized clinical trial R&D Research and development SARS Severe acute respiratory syndrome SSA Specific Support Action TB Tuberculosis t‐PA Tissue plasminogen activator UN United Nations WHA World Health Assembly WHO World Health Organization ZonMW Netherlands Organisation for Health Research and Development

Preface
v
Preface
Context
This Report on priority medicine needs for Europe and the world should be read against the backdrop of a Europe that is expanding and globalizing. The demographic changes taking place in Europe will mean that ever‐increasing numbers of people will live longer and that an increasing proportion of this elderly population will be women. These demographic changes are mirrored in most of the rest of the world and they are coupled with a rapid pace of urbanization. Many of the diseases identified in this Report are not only high burden diseases in Europe. Most countries have completed, or at least initiated, their epidemiologic transition and are faced with an aging population prone to certain cardiovascular, metabolic, joint and other chronic conditions that also afflict Europeans. Thus, there is a clear ʺcommonality of interestʺ that Europe shares with the rest of the world in this regard. This Report should also be read against the backdrop of a European health care system with a long tradition of social solidarity in which national health systems were developed to create social safety nets for all citizens. Health care costs have continued to rise throughout Europe and a variety of payment and reimbursement systems (co‐payments, reference pricing, differential pricing and others) have been developed as a means for cost containment. There is little, if any, uniformity among European countries with regard to the procedures for setting prices and reimbursement. Overall, cost controls are being achieved by setting prices at a level that may not fully reward pharmaceutical innovation and by delaying decisions about reimbursement. Little effort is made to determine ʺvalue for moneyʺ for pharmaceutical innovation. Finally, this Report should also be read against the backdrop of a European pharmaceutical industry that, in many respects, is struggling with the tension between industrial and health policy objectives. One source of tension is the apparent loss of competitiveness in the European pharmaceutical industry, highlighted by a series of recent reports that suggest that Europe is not supporting new entrepreneurship, and is losing market share and human resources to the pharmaceutical industry in the USA (see Appendix 2). Worrying trends have emerged which suggest that the time needed to bring a product to market is increasing, the number of new product launches is decreasing, and the cost of developing a new chemical entity as a medicine continues to increase. Many pharmaceutical projects in the early stages of research and development never make it through the ʺpipelineʺ, so that the translation from basic science to applied product development has become a weak link.

Priority Medicines for Europe and the World
vi
The importance of prevention
The Project has highlighted the importance of prevention wherever this is possible. For example, in 2002 measles accounted for 540 000 deaths among children under five but is largely preventable through vaccination. While having a medicine to treat measles would help individual patients, prevention through universal immunization must remain the priority for addressing this disease. Diseases such as chronic obstructive pulmonary disease, alcoholic liver disease and Type 2 diabetes can in large part be prevented by changes in behaviour and lifestyle. However, once these diseases occur, they cannot be reversed by changes in behaviour or lifestyle. For this reason, pharmaceutical research is needed to develop new products for these conditions, which account for a high disease burden in Europe.
Methods used in this Report
In this Report, three complementary methods have been used to identify “pharmaceutical gaps”, that is, those diseases of public health importance for which pharmaceutical treatments either do not exist (lack of basic scientific knowledge or market failure) or are inadequate (lack of efficacy or safety concerns or because the delivery mechanism or formulation is not appropriate for the target patient group). An evidence‐based method was used that combined: demographic information; European and global disease burden data from the World Health Organization Global Burden of Disease Database; and clinical trial data from the Cochrane Database of Systematic Reviews on the clinical efficacy of interventions used to treat these diseases/conditions. A second method was used to establish pharmaceutical gaps on the basis of information including projections of diseases and trends. Finally, in line with the established European tradition of social welfare systems, potential pharmaceutical gaps were reviewed from a perspective of social solidarity, and diseases/conditions were identified for which there is no market incentive to develop medicines. All data and background papers are found on the Project website and the accompanying CD‐ROM.i
Limitations and areas not addressed
The methods outlined above have a number of limitations. The data on global burden of disease are limited by the type and quality of the original data on mortality and morbidity. The reviews in the Cochrane Database to a large extent mirror the important chronic conditions of industrialized countries, and there is a lack of reviews of infectious, acute conditions. This evidence requires sufficient numbers of clinical trials before systematic reviews are undertaken.
i http://mednet3.who.int/prioritymeds/report/index.htm

Preface
vii
In attempting to update the three types of methods with further information on the current status of the pharmaceutical pipeline, other limitations arise. Often, data on medicine efficacy and pipelines for future medicines are difficult to obtain or interpret. The Report does not fully address underlying causes of morbidity and mortality such as tobacco use and obesity. The methodology of depending on the Global Burden of Disease Database omits these underlying conditions. Tobacco smoking is a major contributing factor to many heart and lung diseases. Obesity is a factor in many of the priority diseases we have identified, particularly cardiovascular disease, cerebrovascular disease, diabetes, cancer and osteoarthritis. Another condition that has not been addressed is osteoporosis, which in 2000 caused 3.79 million fractures in Europe. Although health promotion and disease prevention are recognized as key components of an overall strategy to deal with the priority diseases/conditions mentioned, the Report does not provide any in‐depth analysis of these. Similarly, the complex relationship between pharmaceutical research and development, innovation, intellectual property, pricing and trade is not addressed here in any comprehensive manner, as this is currently being reviewed by the WHO Commission on Intellectual Property Rights, Innovation and Public Health: (http://www.who.int/intellectualproperty/en/). This Report does not address diagnostics except for a few comments in the sections on antibacterial resistance, tuberculosis, malaria and Alzheimer disease. This would have broadened the scope of the study. In many cases, improving diagnostics may be easier to achieve than developing new medicines. A study such as this is inevitably a compromise between practicality and perfection. With more data of better quality, more time and human resources, more analyses could have been done. However, it is unlikely that the results would have been fundamentally different. This Report offers a bold vision of a Europe that can invest, innovate and cooperate to address the critical need for priority medicines for all citizens of the world.

Priority Medicines for Europe and the World
viii

Executive summary
ix
Executive summary Purpose and objectives
The purpose of the Priority Medicines for Europe and the World Project has been to study pharmaceutical innovation from a public health perspective. The objective was to prepare a public‐health‐based medicines development agenda for support by the European Union and to develop a systematic methodology for this that can be replicated. For the purposes of this Report, a public health perspective is one that is based on principles of equity, evidence and efficiency. Within the context of identifying “pharmaceutical gaps” which affect the citizens of Europe, special emphasis has been placed on identifying those research needs which are also relevant for countries in economic transition and for developing countries. This ʺcommonality of interestʺ is an important bridging aspect of the Project between Europe and the world. In many areas, public health interests and pharmaceutical industry priorities coincide. In other areas, such as neglected diseases of poor countries or orphan diseases of rich countries, the market has failed and incentives have to be created for the pharmaceutical industry to respond to these clear needs. The multiple reasons for the existence of pharmaceutical gaps were reviewed and suggestions made on a number of different approaches to create a European environment to close these gaps.
Background
Recent reviews of the pharmaceutical industry situation in Europe have suggested that Europe is lagging behind the USA in its ability to generate, organize and sustain pharmaceutical innovation. At the same time, concerns have been expressed, both at the international level and in Europe, at the lack of research to fill pharmaceutical gaps. From a public health perspective, pharmaceutical gaps can be identified as those diseases of public health importance for which pharmaceutical treatments either do not exist (lack of basic scientific knowledge or market failure) or are inadequate (lack of efficacy or safety concerns or because the delivery mechanism or formulation is not appropriate for the target patient group). Within Europe, considerable funds are expended on Framework Programmes and other Programmes which provide support for Europe‐wide research activities. Much of this support is for health‐related research which impacts the pharmaceutical industry. The focus of the Seventh Framework (2007‐2010) has yet to be decided. This Project aims to provide a basis for making the focus of the Seventh Framework “Priority Medicines for Europe and the World”.

Priority Medicines for Europe and the World
x
Priority‐setting
There are many different methods that can be used to set priorities. Essentially, they all attempt to combine an assessment of need, an estimation of the likelihood of success, the resource requirements, and the underlying values of those making the decisions. For this Project, three different approaches have been used. The first is an evidence‐based method which combines estimates of European and global burdens of disease with available information on the efficacy of existing medicines. The second method depends on prediction of likely public health trends based on past and present experience. This method prioritizes those diseases/conditions which may not have a major impact on public health at the moment but which pose a very serious threat to global public health in the future. The third method depends on values of social solidarity to identify high burden diseases for which there are currently no market incentives to develop treatments. These may be rare (“orphan”) diseases which affect people in Europe or neglected diseases which mainly affect the poor in developing countries.
Methods
The evidence‐based method used data from the World Health Organization (WHO) Global Burden of Disease Database in Geneva and Copenhagen. Data on the efficacy of existing medicines have been extracted from the Cochrane Database of Systematic Reviews and other such secondary sources. Information on predicted public health threats have been collected from WHO, the European Union (EU), the US Government and other official sources. Information on neglected and orphan diseases was collected from existing sources. Detailed background studies were commissioned using a framework developed by the Global Forum for Health Research. Drafts of this Report and the background studies have been extensively circulated for comment by experts in WHO, the EU, industry, academia and nongovernmental organizations (NGOs). Meetings were held with stakeholders to present and discuss the findings and recommendations.
Results
Demographic changes
In Europe, the population is aging, with more people — especially women — living beyond 80 years. In the new member countries of the EU, this development has been complicated by the changing dependency ratios in these countries. In developing countries there is a stark difference between Africa and other regions. In many African countries, human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) has had a substantial impact in reducing life expectancy. In most other regions, the rapid aging of the population, together with a decline in birth rates, are leading to profound changes in population structures.

Executive summary
xi
Disease patterns
One of the major results of this study relates to the ʺcommonality of interestʺ between Europe and many developing countries. The demographic and disease pattern changes taking place in Europe are also occurring in many developing countries. The striking difference was in infectious diseases, particularly neglected diseases, where the burden in Europe is low or non‐existent compared to developing countries. As a result, there are few incentives in Europe to undertake the research and development (R&D) needed to develop new medicines for these diseases. This Project has also highlighted the importance of chronic diseases in contributing to the burden of disease in developing countries. For diseases such as diabetes, cardiovascular disease (CVD), depression and cancers, therapeutic advances in Europe will benefit people in countries throughout the world. In time, diseases such as osteoarthritis and Alzheimer disease (AD) will become more prevalent in developing countries as life expectancy increases, and closing these pharmaceutical gaps will also be important. However, this focus on common benefits should not detract from the urgent need in Africa and in low‐income countries elsewhere for access to effective treatments for diseases such as tuberculosis (TB), malaria, HIV/AIDS and the many neglected diseases. Many of these countries have to contend with the continuing high burden of infectious diseases while chronic diseases increase in prevalence.
Chronic diseases
The commonality of interest between Europe and the world in relation to chronic diseases is striking. The two leading causes of death in Europe and the world are ischaemic heart disease and stroke. Over the next 20 years, the major increase in deaths from these diseases will occur in developing countries. Closing pharmaceutical gaps for chronic diseases in Europe will have major benefits if the products developed are also accessible for people in developing countries.
Acute diseases
For acute diseases, particularly infectious diseases, the burden in Europe is low. As a result, many pharmaceutical companies have abandoned research on antibiotics — a development which could have profound consequences for future generations in view of the global increase in the spread of drug‐resistant bacteria. Pandemic influenza is another major threat to global public health. The 1918‐1919 pandemic caused 40‐50 million deaths. Pandemics also occurred in 1957 and 1968. Recent outbreaks of avian influenza in Asia have signalled that the next pandemic could be similar in scale to the 1918‐1919 pandemic. Unfortunately the world is currently not prepared for such an eventuality.

Priority Medicines for Europe and the World
xii
High burden preventable diseases
Although lifestyle changes and other forms of primary prevention must be key components of any strategy to reduce the morbidity and mortality of high burden conditions (whether or not effective pharmaceuticals exist) a number of preventable high burden diseases were identified as having pharmaceutical gaps. Of these, the most important were secondary prevention of heart attack and stroke. Although secondary prevention is possible through the use of a combination of effective medicines, for a variety of reasons these medicines are often not taken. However, if the appropriate medicines were combined into a fixed‐dose combination (FDC) product, it is likely that there would be a dramatic increase in their use. This key intervention has the potential to save the lives of millions of people in Europe, particularly in conjunction with the above‐identified lifestyle changes and other approaches. Research is urgently needed on the formulation and field testing of such multidrug FDCs for this purpose. HIV/AIDS is also preventable through behavioural approaches and can also be treated, but not cured, with antiretrovirals. An effective vaccine to prevent this disease is urgently needed. Although development of a vaccine to combat HIV/AIDS is proving to be difficult, support to organizations such as the International AIDS Vaccine Initiative (IAVI) would help accelerate the vaccine R&D process. At present these activities are severely underfunded. In addition, new medicines are needed that lack cross‐resistance with existing classes of treatment. Chronic obstructive pulmonary disease (COPD) and alcoholic liver disease are two additional preventable diseases which cause substantial morbidity and mortality in Europe and the world — underlining the importance of attempting to prevent these two conditions by cessation of tobacco smoking and the prevention of alcohol abuse respectively. At present, the outlook for the discovery or development of pharmaceutical agents to effectively treat these conditions or reverse progression is poor.
High burden diseases with no curative treatments
Two high burden diseases, in Europe particularly, for which the currently available treatment is inadequate are osteoarthritis and Alzheimer disease. Both are common and increasing among the elderly, and available treatment is ineffective in reversing disease progression. A major challenge for both diseases is the absence of biomarkers which could be used to diagnose and monitor the progression of disease or the effect of treatment. Continued support is needed for basic research on these diseases. Pharmaceutical companies invest heavily in research on both of these diseases but there are major biological challenges in understanding and then reversing these progressive diseases.

Executive summary
xiii
High burden diseases with existing but inadequate therapies
Cancer and diabetes are two of the main diseases in this group. Both diseases encompass a range of different diseases, each of which may need different treatments. There are many different forms of cancer, of which some are treatable while others are not. Diabetes is divided into two types, Type 1 in which insulin therapy is required and Type 2 in which other treatments are initially possible but insulin may be needed as the disease progresses. Our analysis of research for cancer suggests that the present high level of research effort is being appropriately targeted. For diabetes, a major need for developing countries is heat‐stable insulin that could be used in a health system without the need for refrigeration. For both cancer and diabetes, comparative studies of existing treatment would be useful for prescribers, patients and reimbursement authorities. Depression is another high burden disease for which effective therapy exists for some groups of users. However, these medicines have severe and common side‐effects. The efficacy of treatments for adolescents is doubtful, and there is a need for further research on the treatment of depression among the elderly and on reducing side‐effects.
Neglected diseases and orphan diseases
There are a number of neglected diseases which primarily affect the poor in developing countries. The European and Developing Countries Clinical Trials Partnership (EDCTP) has been established to address clinical trial aspects of malaria, TB and HIV/AIDS. One of these diseases, TB, is also a serious problem in a number of new EU Member States. However, research is also needed on other neglected diseases such as trypanosomiasis (sleeping sickness), leishmaniasis and Buruli ulcer. The major gap at the moment is the lack of “translational” research, which translates basic research discoveries into products that can be tested on humans. The problem is that traditionally the EU does not support such research, and the market does not provide sufficient incentive for the pharmaceutical industry to be active in R&D of products for these diseases. As a result, the public sector must find a way to support such bridging research, possibly through support for product development public‐private partnerships (PPPs). Maternal death, often due to postpartum haemorrhage, is almost entirely limited to developing countries. One of the major contributing factors to this mortality is the absence of heat‐stable oxytocin that could be administered to the mother to prevent severe blood loss. Despite research in the early 1990s to demonstrate this stability problem, nothing has been done to develop heat‐stable oxytocin.

Priority Medicines for Europe and the World
xiv
Cross‐cutting issues
In addition to identifying priority diseases, the Project has also reviewed delivery mechanisms for existing medicines and the needs of special groups.
Delivery mechanisms
Many different systems have been devised to deliver medicines in a sustained manner, or with a delay period. While a company must provide detailed studies to demonstrate the efficacy of such products, the technology is well developed. As a result, where there is a therapeutic need, such products have been produced. However, various constraints have limited further development of such technologies for diseases of public health importance. The situation is exemplified by FDC products. Prior to the mid‐1960s, such products were very common and remain so for over‐the‐counter (OTC) products. However, due to the proliferation of irrational combinations, regulators led by the U.S. Food and Drug Administration (FDA) set a high standard for approval of prescription FDCs. In a recent development, FDC products have been recommended by the WHO Expert Committee on Selection and Use of Essential Medicines for use in the treatment of HIV/AIDS, TB and malaria. In this Report, it is recommended that two FDC products should also be evaluated for their widespread use in the secondary prevention of heart attack and stroke. There is a need for research on a number of issues relating to FDCs, including formulation, quality assurance, their effect on adherence and outcomes, and the economics of their production and use.
Special groups: the elderly, women and children
While the elderly, women and children are frequent users of medicines, they have often been excluded from clinical trials, and often the medicines available have not been produced to meet their special needs. Considerable progress has been made in the USA and in Europe in solving the problem of paediatric medicines. A similar effort is needed for medicines for the elderly, who are major consumers, and for women, whose particular needs have often been neglected by manufacturers and regulators.
New approaches to promoting innovation
Public‐private partnerships, valuing innovation, reducing barriers to innovation and comparative studies
In this Report, various approaches to promoting innovation in Europe are reviewed and research agendas proposed. Reducing regulatory barriers to innovation is a current interest of the European Medicines Agency (EMEA), the FDA and a number of other agencies. A consultative process has been established and a research agenda suggested. Regulators and

Executive summary
xv
governments should work with industry and others (including patients) to identify and remove, where possible, regulatory and reimbursement delays and barriers to innovation. Using existing flexibilities more widely may facilitate innovation for some priority products. Patient involvement and the importance of post‐marketing evaluation of new products (Phase IV studies) need further attention in the present discussions. The intention of the EU to support a research programme on the “accelerated development of new, safe and more effective medicines” is strongly supported. There is considerable scope for the use of electronic medical records (EMR) in the investigation of the relative benefits, side‐effects, and cost‐effectiveness of new medicines. Moreover, such EMR‐based studies can employ a randomization step (so‐called “randomized epidemiology”) in order to provide objective estimates of comparative effectiveness. A number of product development PPPs have emerged in the past decade. They have been established to bridge the translational research gap between basic R&D of medicines and clinical trials. They have focused on diseases where there is market failure or at least where commercial companies have limited interests. Many of the PPPs work with such commercial companies and contract out the various components of pharmaceutical development to small companies or organizations. Most of their funding has come from foundations. The EU has provided very little support for such organizations. Given adequate support, PPPs could fill a critical gap by providing products for the EDCTP to test in their clinical trials programme. Valuing innovation is a complex and difficult task undertaken by each European country’s reimbursement authorities. The uncertainty over therapeutic value and the different methods used by different national systems to value innovation and reimbursement creates a complex environment for companies to bring their product to the market. This Report proposes a model for valuing innovation that uses pharmaco‐economic methods to combine measures of efficacy with Gross National Income (GNI) per capita in order to set prices for new medicines.
Key conclusions
This study has identified the following key conclusions: • There are many chronic diseases that contribute to the disease burden in both
Europe and the world as a whole. Successful research into the development of new medicines and improved medicines needed to treat them benefits both Europe and the world.
• Antibacterial resistance and pandemic influenza are major threats to global public health which require a coordinated response appropriate for an EU Technology Platform. Increasing the uptake of influenza vaccine in European countries is an urgent first step to prepare for the inevitable influenza pandemic.

Priority Medicines for Europe and the World
xvi
• Smoking underlies many of the most common serious diseases affecting both Europe and the world. While prevention efforts must take precedence, the EU should support research on pharmaceutical methods to treat smoking cessation.
• Pharmaceutical innovation in Europe could be improved through reforms of regulatory and pricing policies. This Report recommends a programme of research focused on these areas and involving the major stakeholders.
• Therapeutics can be improved through the development of improved pharmaceutical delivery mechanisms. This would require research, for example, on FDC and heat‐stable products.
• Pharmaceutical innovation should also encompass special groups of patients such as the elderly, women and children, who have particular needs in relation to dosage forms and products.
• Where markets fail — as has occurred with tropical infectious diseases and other neglected diseases — new mechanisms are needed to promote the translation of basic research into clinically important products. While the EDCTP has been created to promote clinical research on HIV/AIDS, TB and malaria, gaps remain for other diseases. The Report recommends that the EDCTP be broadened to address other neglected diseases and that selected product development PPPs be supported to bridge the translational research gap.
• Developments in the fields of information technology (IT) and pharmaceutical innovation have created the opportunity for innovative methods to be used to compare and evaluate the performance of new medicines after their release into the market. Such an IT‐based approach would build on European strengths and could shorten the time it now takes to bring a product to market.
A number of specific research ʺgapsʺ have been identified for Antibacterial resistance, Pandemic influenza, Cardiovascular disease, Diabetes, Cancer, Acute stroke, HIV/AIDS, Tuberculosis, Neglected diseases, Malaria, Alzheimer disease, Osteoarthritis, Chronic obstructive pulmonary disease, Alcohol use disorders: alcoholic liver diseases and alcohol dependency, Depression in the elderly and adolescents, and Postpartum haemorrhage.

1. Introduction
1
1. Introduction 1.1 Context
In 2003, in preparation for its role as the President of the European Union (EU) during the second half of 2004, the Government of the Netherlands established the Priority Medicines for Europe and the World Project. The aim was to establish a public‐health‐based medicines research and development (R&D) agenda and, where necessary, to help bridge the gap between public health needs and the development priorities of the pharmaceutical industry. The Netherlands Government requested the World Health Organization (WHO) to prepare a research agenda and methodology based on public health needs and to draw up a list of priority medicinesi to be proposed for research funding by the EU as part of its Seventh Framework Programme (2007‐2010). In addition to identifying priority medicines needed for EU citizens, the aim was to identify those research needs which are also relevant for countries in economic transition and for developing countries. This “commonality of interest” is an important bridging aspect between the health needs of Europe and the world. The objective of the Project, as described in the initial proposal, was: to prepare a public health‐based medicines development agenda, for support by the EU in the short‐ (2005-2006) and medium‐term (2007-2010) future, and to develop a systematic methodology in this regard.
1.2 Pharmaceutical gaps: a public health perspective
The Project addresses pharmaceutical gaps from a public health perspective that is based on considerations of equity, evidence and efficiency. This involves considering the greatest good for the greatest number of people, promoting healthy behaviours, making use of preventive technologies and taking steps to ensure that access is assured to all who would benefit. Although the Project addresses some high burden diseases that are preventable, such as lung cancer, chronic obstructive pulmonary disease (COPD) and alcoholic liver disease, it should be underlined that any new treatment is unlikely to be a “magic bullet” and that health promotion and disease prevention will remain very high priorities for the foreseeable future.
i Priority medicines may be defined as those medicines which are needed to meet the priority health care needs of the population (“essential medicines”) but which have not yet been developed. For the purposes of this Report, a ʺpriorityʺ medicine for a priority disease is by definition also a significant improvement over already‐marketed products.
Priority Medicines for Europe and the World
2
The Project is designed to identify “pharmaceutical gaps” i.e. where treatments either do not exist or are inadequate, or where existing treatments or preventive measures are likely to become ineffective in the future, such as antimicrobial resistance or pandemic influenza. In addition, the Project aims to identify areas for improved delivery mechanisms or better formulations of existing preventive and therapeutic medicines (for example, fixed‐dose combinations (FDCs)). Particular groups, such as the elderly, women and children, who have frequently been ignored in the scientific or medicines development process, are also considered. It is encouraging to note that in the past, major pharmaceutical gaps have been closed. For example, prior to 1975, surgery for peptic ulceration was one of the most common forms of surgery. The development of a range of therapies closed this gap (see Annex to Chapter 1).
1.3 The epidemiological transition and the ʺcommonality of interestʺ
The Project focuses on different populations whose priority health needs are changing. As of 1 May 2004, the EU was enlarged from 15 countries (EU15) to 25 countries (EU25) with the addition of 10 new countries (EU10). All EU25 countries have aging populations. At the same time, countries in other parts of the world, particularly some Eastern Mediterranean and South‐East Asian countries, are rapidly moving from an era of infectious diseases to an era of chronic diseases associated with lifestyle and economic changes (e.g., changes in nutrition and physical activity leading to obesity and an increase in both diabetes and diabetes‐related diseases). As the health needs of Europe and the rest of the world overlap, a commonality of interest is emerging in the need for some priority medicines. The vast majority of cancers, cardiovascular disease (CVD), diabetes and osteoarthritis, if not already occurring, will become an increasingly high disease burden in the developing world. Over time some pharmaceutical “gaps” will close while others open up. Changing priorities may be due to pharmaceutical innovation, population changes such as aging, or behavioural changes such as smoking. Better understanding of these changes can be used to inform priority‐setting. This study also takes account of the health needs of the many African countries which are faced with the onslaught of human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) combined with the impact of other high‐burden diseases such as tuberculosis (TB) and malaria, and neglected diseases such as trypanosomiasis (sleeping sickness) (see Background Chapters 6.7, 6.8, 6.9).
1.4 Conceptual framework
The literature on priority‐setting has been reviewed to develop a conceptual framework for the Project (Chapter 3). An approach developed by the Global Forum for Health Research is particularly relevant (see Chapter 4.5) and forms the basis for some aspects of the methodology used in the Project.

1. Introduction
3
Figure 1.1 below (see Appendix 3.6) offers a public health perspective of the scale of unmet treatment needs. This model identifies that for some diseases effective treatments exist and are widely used (Area 1). For other diseases, effective treatments exist but obstacles to access exist (Area 2). The obstacles may be due to factors such as cost or weaknesses in the health system. The third area includes conditions for which some treatments exist but the delivery mechanism or formulation may be inappropriate for the target patient group. Area 4 encompasses those conditions for which no effective treatment is available. This project focuses on Areas 3 and 4 and not on Areas 1 and 2.
Figure 1.1: Identifying gaps (unmet therapeutic needs): a public health perspective
3
Few treatments available, better formulations and
delivery mechanisms needed
2
Treatable with existing interventions
but obstacles to access exist
1
Treatable with current mix of interventions
Untreatable with existing interventions(including incurable chronic conditions)
4
0%
0%
100%
100%
Population coverage with current mix of interventions
Combined efficacyof a mix
of allavailable
interventions
Maximum achievable coverage
Source: Adapted from the Report of the Ad Hoc Committee on Health Research Relating to Future
Intervention Options, WHO, 1996
1.5 Structure of the Project
The Project was organized in three phases. Phase 1 (August 2003 to March 2004) involved the development of a research plan, a methodology, collection of data and the production of a Preliminary List of diseases/conditions for more detailed studies. Phase 2 (April to August 2004) involved in‐depth studies of these diseases, cross‐cutting themes (delivery mechanisms, the elderly, women, children and orphan diseases) and four papers which related to innovation. The final phase (August to November 2004) involved reviews and discussion of the draft methodology and final list of research priorities prior to publication and presentation of the findings. Throughout the Project, an international project consultative group, including academics, nongovernmental organizations (NGOs), the Dutch Ministry of Health,

Priority Medicines for Europe and the World
4
representatives of the pharmaceutical industry and WHO staff, met on a regular basis to review progress. In addition, regular meetings were held in Brussels with EU Commission staff from Directorate General (DG) for Research, DG Enterprise and DG SANCO (Public Health). During the second phase of the Project, numerous meetings were held with the pharmaceutical industry, patients, NGOs and professional groups. As part of this Project, a Specific Support Action has been supported by the European Commission to identify common areas of interest in national public research funding in the areas of priority medicines. The Netherlands Organisation for Health Research and Development (ZonMw) is coordinating the inventory of national programmes and priorities and is preparing an ERA‐NET Coordination Action to be submitted in March 2005.i Draft versions of this Summary Report and the Background Report were distributed for comment on 31 August 2004, were reviewed by the Project Consultative Group in Geneva on 22‐24 September and this Report was presented to stakeholders at a meeting in Brussels on 4 October 2004. The Report will be presented for discussion at a meeting of ministries and other high‐level authorities on 18 November 2004 in the Hague, the Netherlands. The preliminary results of the ZonMw Priority Medicines Specific Support Action will also be presented on 18 November.
1.6 Who is the target audience for this Report?
This Report is addressed to different audiences. The primary audience are the EU decision‐makers – the Council, Parliament and the European Commission (notably, but not exclusively, the Directorates General for Research, Enterprise, SANCO and Development). European Member States which are responsible for funding research and paying for medicines are another focus for this Report. Another crucial group is the European Investment Bank as well as directors of research in the European pharmaceutical industry. While their priority‐setting may be strongly influenced by market forces, the reality is that these market forces, particularly in Europe, are driven by public health realities. Policy‐makers and politicians at national and regional levels may also find this Report and the background documents useful for their decision‐making. Researchers who are deciding where to put their future efforts may find the methods and conclusions useful for their decisions. Patient groups and payers (social health insurance organizations, funders and reimbursement authorities) have a common interest in identifying which research should be prioritized and encouraged.
i ZonMw Priority Medicines http://www.zonmw.nl/index.asp?s=7747 (accessed 25 September 2004).

1. Introduction
5
1.7 Contents of the Report
This Summary Report has been produced in parallel with a Background Report that contains annexes and appendices which are available on a CD‐ROM and on the WHO website (http://mednet3.who.int/prioritymeds/report/index.htm). The Report sets out the burden of disease for Europe and the world as a whole. It identifies where pharmaceutical gaps exist and outlines what can be done to fill these gaps and what measures need to be taken to promote innovation. The Report provides a broad approach to priority‐setting which uses multiple methods and involves different stakeholders. The methodology described can be adapted for use at national or regional levels. This Project can be seen as a first step to rational decision‐making for setting priorities and for promoting innovation in the pharmaceutical industry in Europe. Chapter 2 describes how innovation occurs in the pharmaceutical sector and outlines recent concerns about the decline in innovation and competitiveness in Europe. Chapter 3 briefly describes different approaches to setting priorities and the approaches selected for use in this Report. Chapter 4 covers the various methods used in the study, the preliminary results of which are described in Chapter 5. Chapter 6 focuses on the various priority diseases requiring priority medicines and provides a summary of the detailed information included in the background documents. Cross‐cutting themes related to delivery mechanisms, the special needs of the elderly, women and children, and the particular case of “orphan” diseases (which affect relatively small numbers of people) are dealt with in Chapter 7. Chapter 8 looks at issues related to promoting innovation. These issues include public‐private partnerships, determining value for innovation, barriers to innovation and issues relating to comparative studies of the effectiveness of medicines. Chapter 9 provides conclusions and recommendations for the different stakeholders. This Report includes limited references, as comprehensive documentation is provided in the background documents on the CD‐ROM or web page.
1.8 Areas not addressed by this study
This study does not address health system issues such as access or quality of care. Nor does it address gaps related to logistical or sociological barriers. In addition, it does not address conditions or risk factors which can be considered major underlying causes of morbidity or mortality such as obesity or osteoporosis. The study makes little reference to the availability of diagnostics or devices and does not address issues related to intellectual property, as this is the subject of the WHO Commission on Intellectual Property Rights, Innovation and Public Health.i However, if this study were to be repeated in other regions, it is recommended that these issues should also be addressed.
i http://www.who.int/intellectualproperty/en/

Priority Medicines for Europe and the World
6
2. Background to the Priority Medicines Project
7
2. Background to the Priority Medicines Project
2.1 Introduction
This chapter reviews the history of pharmaceutical development and highlights the recent decline in the number of new innovative products being produced. It provides a brief overview of recent reports about global competitiveness in pharmaceuticals in Europe (by Pammolli, the G‐10 group, and the European Commission) and of recent reports on pharmaceutical innovation from the European Medicines Agency (EMEA) and the U.S. Food and Drug Administration (FDA).
2.2 History of pharmaceutical innovation
This section is closely based on Background Chapter 8.3. In summary, there has been a series of waves of innovation in the pharmaceutical industry1,2 The first generation innovations (1820‐1880) were a consequence of the ʺChemical Revolutionʺ introduced by Antoine Lavoisier and the French School of Chemistry at the end of the 18th century. The development of chemical extraction and experimental methods allowed isolation and purification of ʺactive principlesʺ of medicinal plants with known medicinal properties, such as morphine, quinine, curare and belladonna. Such methods also allowed for the synthesis or isolation from plants or coal tar of simple organic chemicals with medicinal properties, such as ether, chloroform, carbolic acid and salicylic acid as an antipyretic. The second generation innovations (1880‐1930) were driven by public medical research laboratories for sera and vaccines as well as by private German, French and Swiss dye companies with increasing expertise in organic chemistry. These developments led to the establishment of the modern pharmaceutical industry. The third generation (1930‐1960) included innovations in organic and natural products chemistry leading to the isolation and synthesis of vitamins, corticosteroids, sex hormones and antibacterials. A major development during the third generation, together with an increase in the intensity of research, was the adoption of intensive marketing methods aimed at physicians, hospitals and pharmacies. Innovations of the fourth generation (1960 to about 1980) resulted from a marked shift in the scientific basis of the industry from chemistry and pharmacology to the life sciences. A well developed phased system for developing new medicines developed during this period, the so‐called ʺPhase I‐IVʺ system for clinical trials. The first stage involves basic research and translational research. This phase merges into the preclinical phase, in which animal and other studies are undertaken. In clinical Phase I studies, a limited number of human subjects are subjected to studies to determine

Priority Medicines for Europe and the World
8
dosing levels, detect very common side‐effects, assess how the body metabolizes the medicine and, in some cases, what effect the medicine has. In Phase II studies, which involve a larger number of patients, the new medicine is tested for efficacy, for possible side‐effects and to obtain more information on dosing. Phase III trials involve even more patients. In Phase III trials, new medicines are most often compared to placebos and, less frequently, to existing therapies to determine their relative effectiveness. Although further attention is paid to side‐effects, any unusual events may not be detected. Phase IV studies are undertaken after the medicine has been marketed and are primarily used to detect rare but significant side‐effects. Throughout these various phases of development there is a very high rate of attrition among candidate medicines. As a result, only a very small number of products which enter the research and development (R&D) “pipeline” eventually reach and remain on the market. The most important medicines of the 1960s and beyond were used for the treatment of chronic diseases such as diseases of the central nervous system, cardiovascular diseases and cancers. In response to the proliferation of medicines and the thalidomide crisis in 1961, governments imposed strict regulatory measures to ensure the efficacy and safety of candidate medicines. The latest wave of innovation (since 1980) is based on advances in the discovery and application of biotechnology (recombinant deoxyribonucleic acid (DNA) and monoclonal antibody methods) in the production of physiological proteins used in the therapy or diagnosis of many diseases. Figure 2.1 below, taken from the keynote paper by Achilladelis and Antonakis, shows the successive ʺwavesʺ of innovation but also clearly shows the downward trend in innovation over the last 10 years.
Figure 2.1: Pharmaceutical innovation over time
Source: Research Policy, 30, Achilladelis B, Antonakis N. The dynamics of technological innovation: the case of the pharmaceutical industry. Pages 535‐538. Copyright 2001, with permission from Elsevier (Note: ʺTTʺ is ʺtechnological trajectoryʺ and its definition can be found in the original paper. It is not relevant for the present discussion).
1920 25 30 35 40 45 50 55 60 65 70 75 80 85 1990
50
40
30
20
10
No. of innovationsAll innovationsInnovations related to TTsRadical innovations
2. Background to the Priority Medicines Project
9
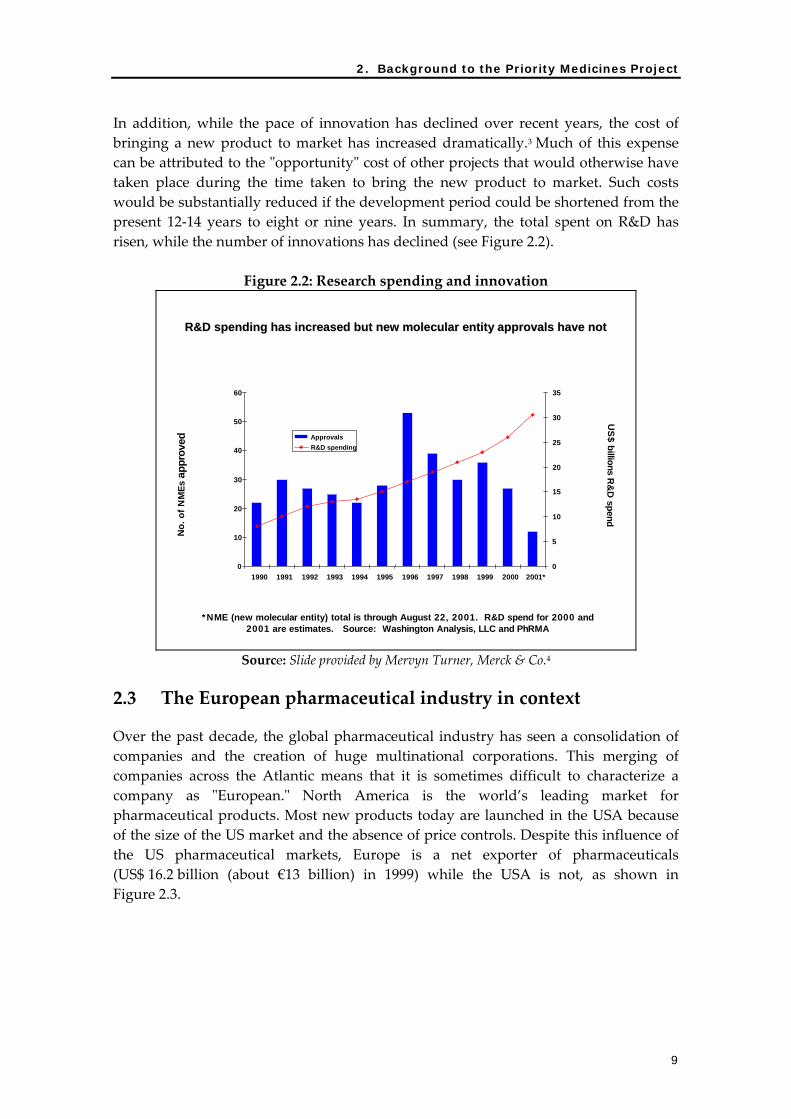
In addition, while the pace of innovation has declined over recent years, the cost of bringing a new product to market has increased dramatically.3 Much of this expense can be attributed to the ʺopportunityʺ cost of other projects that would otherwise have taken place during the time taken to bring the new product to market. Such costs would be substantially reduced if the development period could be shortened from the present 12‐14 years to eight or nine years. In summary, the total spent on R&D has risen, while the number of innovations has declined (see Figure 2.2).
Figure 2.2: Research spending and innovation
No .
of N
MEs
app
r ove
dU
S$ billions R
&D
spend
*NME (new molecular entity) total is through August 22, 2001. R&D spend for 2000 and 2001 are estimates. Source: Washington Analysis, LLC and PhRMA
R&D spending has increased but new molecular entity approvals haR&D spending has increased but new molecular entity approvals have not ve not
0
10
20
30
40
50
60
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001*0
5
10
15
20
25
30
35
ApprovalsR&D spending
Source: Slide provided by Mervyn Turner, Merck & Co.4
2.3 The European pharmaceutical industry in context
Over the past decade, the global pharmaceutical industry has seen a consolidation of companies and the creation of huge multinational corporations. This merging of companies across the Atlantic means that it is sometimes difficult to characterize a company as ʺEuropean.ʺ North America is the world’s leading market for pharmaceutical products. Most new products today are launched in the USA because of the size of the US market and the absence of price controls. Despite this influence of the US pharmaceutical markets, Europe is a net exporter of pharmaceuticals (US$ 16.2 billion (about €13 billion) in 1999) while the USA is not, as shown in Figure 2.3.

Priority Medicines for Europe and the World
10
Figure 2.3: Net pharmaceutical balance of trade by country (From: The World Medicines Situation, WHO, 2004)
Medicines in countries' international tradeExports minus imports – 1999
US$
bill
ion
Net importers Net exporters76543210-1-2-3
USAJa
pan
Canad
aBraz
il
Spain
Poland
Australi
a
Turkey
Saudi A
rabia
Greece
IndiaChina
Belgium
Denmark
France
Sweden UK
Irelan
d
German
y
Switzerl
and
Source: ITC database
After marketing costs, R&D is typically the second biggest item in the spending profile of large pharmaceutical companies (Figure 2.4).
Figure 2.4: Research spending by major pharmaceutical companies (From: The World Medicines Situation, WHO, 2004)
Valu
e in
US$
bill
ion
R&D spending by 10 major pharmaceutical companies, 2001
R&D as % salesR&D spending in US$ billion
20
15
10
5
0
Bristol M
yers
Squibb
Astraz
enec
a
Pharmad
a
Roche
Merck
Novarti
sPfiz
er
Aventis
Johnso
n & Jo
hnson
GSK
Source: Moses Z. The Pharmaceutical Industry Paradox. Reuters Business Insight, 2002

2. Background to the Priority Medicines Project
11
While the focus of this Report is on improving public sector research priority‐setting, it is important to find ways to provide incentives to encourage the pharmaceutical industry to address public health goals.
2.4 Pammolli and G‐10 Reports and EU Communication
In 2000, the EU Commission issued a report on “Global Competitiveness in Pharmaceuticals: A European Perspective” (also known as the Pammolli Report after one of its authors). Its main finding was that while large differences exist across European countries, the European pharmaceutical industry as a whole has been losing competitive advantage to the USA. Overall, the Report found that Europe was “lagging behind in its ability to generate, organize, and sustain innovation processes that are increasingly expensive and organizationally complex.” The competitiveness of the European pharmaceutical industry was reported to be inhibited by domestic and fragmented markets and research systems. Between 1990 and 2000, R&D expenditure in the USA was double the amount spent in Europe. According to the Pammolli Report, eight of the top 10 best‐selling medicines originated from the USA, compared with only one from Europe.5 Largely in response to the Pammolli Report, a high level commission of the European Union, the High Level Group on Innovation and Provision of Medicines (the “G‐10 Medicines Group”), was convened to provide a number of recommendations for public health policies and actions in the area of pharmaceuticals (“G‐10 Report”). These proposals were directed to competitiveness within the industry, pharmaceutical regulation and innovation, generic medicines and the role of patients. In July 2003, the European Commission issued a Communication entitled ʺA Stronger European‐based Pharmaceutical Industry for the Benefit of the Patient – A Call for Actionʺ, which detailed its responses to the 14 wide‐ranging recommendations set out in the G‐10 Report. The Commissionʹs report reviewed each recommendation of the G‐10 Report and discussed how the recommendations might be taken forward and what the G‐10 Group could do to facilitate the process. In making its recommendations, the Commission took account of the health issues raised by the scheduled enlargement of the EU in May 2004.
2.5 The Lisbon and Barcelona European Councils: the “3% solution”
In March 2000, the European Council in Lisbon set out a 10‐year strategic commitment to bring about economic, social and environmental renewal in the EU. The strategy included a focus on the creation of a stronger economy in order to drive job creation. At the same time, social and environmental policies were to be developed that would ensure sustainable development and social inclusion.i
i http://europa.eu.int/comm/lisbon_strategy/index_en.html

Priority Medicines for Europe and the World
12
In March 2002, the European Council in Barcelona officially called for action to increase public and private investment in research and technological development. The Council recommended that investment in medicines research in the EU (both public and private) should rise from 1.9% to 3% of Gross Domestic Product (GDP) by 2010.6 The Council recognized the value of public funding insofar as links to industry were emphasized. There were explicit proposals in the report to improve the effectiveness of public support for, and the use of public resources for research and innovation. In referring to the EU desire to improve links between public research institutions and the private sector, for example, the report said that “…such partnership offers a potentially powerful tool to make investment in research more attractive to business while also benefiting public research.” There have recently been discussions on establishing a Technology Platform for Innovative Medicines which may be a suitable mechanism to implement the Barcelona decisions (see Appendix 8.5.1).7
2.6 Regulatory agency responses by EMEA and FDA concerning innovation
In March 2004, the EMEA launched a consultation exercise on their ʺRoadmap to 2010: Preparing the Ground for the Future,ʺ a strategy to allow the EMEA to better facilitate medicines regulation in an expanded Europe, within a setting of increasing innovation and research.8 This document recognized that the legislative, institutional and scientific environment in Europe is undergoing changes brought about by the impact of new European Community legislation and by EU enlargement. In addition, the impact of an aging population, greater demand for medicines, and the increase in antibacterial resistance is forcing the EMEA to take a fresh look at its role. This EMEA document did not tackle the difficult issue of new and flexible approaches to medicine regulation. This is because in the EMEA the scientific committees, and through these the national authorities, play a role in scientific evaluation but not in medicine dossier requirements. However, the EMEA recognized the need to develop a more proactive approach to pharmaco‐vigilance and risk management strategies, as well as improving access by health care professionals and patients to information emanating from the EMEA. Also in March 2004, the U.S. Food and Drug Administration (FDA), the American counterpart of the EMEA, produced a document entitled “Innovation or Stagnation? Challenge and Opportunity on the Critical Path to New Medical Productsʺ which argued that “… applied sciences needed for medical product development have not kept pace with the tremendous advances in the basic sciences.”9 The FDA suggested that new animal or computer‐based predictive models, biomarkers for safety and effectiveness, and clinical evaluation techniques were needed to improve predictability and efficiency along the “critical path from laboratory concept to commercial product.” Significantly, the FDA emphasized the difficulty involved in ʺpredicting ultimate success with a novel candidate…ʺ at any point during the R&D development cycle. The document cited the fact that a new medicinal compound entering Phase I testing, after perhaps 10 years of

2. Background to the Priority Medicines Project
13
preclinical screening and evaluation, is still estimated to have only an 8% chance of reaching the market. The FDA document identified a need to improve the efficiency and effectiveness of the clinical trial process, including trial design, endpoints and analyses. The FDA acknowledged that ʺ… most of the tools used for toxicology and human safety testing are decades old… and may fail to predict the specific safety problem that ultimately halts development…ʺ Moreover, clinical trials may not uncover safety problems, the trials may be run with too few or with non‐representative patients. They suggested that the development of new clinical markers or surrogate endpoints for clinical effectiveness will become increasingly important. The paper emphasized the importance of research into the regulatory process, and highlighted the value that can be added to such a research agenda by the scientists working in medicine regulatory authorities and by the use of regulatory data.
2.7 The Framework Programmes
Since 1984, the European Commission (Directorate General Research) has undertaken a series of four‐year Framework Programmes (FPs). The Frameworks are intended to address:10 • “research conducted on so vast a scale that single Member States either could not provide
the necessary financial means and personnel, or could only do so with difficulty”; • “research which would obviously benefit financially from being carried out jointly, after
taking account of the additional costs inherent in all actions involving international cooperation”;
• “research which, owing to the complementary nature of work carried out at national level in a given sector, would achieve significant results in the whole of the Community for problems to which solutions call for research conducted on a vast scale, particularly in a geographic sense”;
• “research which contributes to the cohesion of the common market, and which promotes the unification of European science, and technology; as well as research which leads where necessary to the establishment of uniform laws and standards.”
Most of the research supported by the Framework Programme can be characterized as ʺpre‐competitiveʺ research. The Programme does not ʺbuild buildings or create institutionsʺ and it supports very little translational research (i.e., translation of basic research discoveries into products that can be tested on humans) or clinical research. However, some projects undertake such activities, often in cooperation with industry. The core of the Framework Programmes are the cooperation between small manufacturing entities, industry, research institutes and universities. The Seventh Framework in particular is organized around six objectives. One of these objectives is promoting collaborative research, which appears to apply to recommendations of the Priority Medicines Project.i
i See http://europa.eu.int/comm/research/future/pdf/com‐2004‐353_en.pdf

Priority Medicines for Europe and the World
14
The Fifth Framework Programme (1998‐2002) focused on age‐related diseases and disorders involving high morbidity.11 It sought to sponsor research in a number of pharmaceutical‐related areas including stroke, Alzheimer disease, degenerative joint diseases and antibacterial resistance. The Sixth Framework Programme (2002‐2006), with a focus on life sciences, genomics and biotechnology for health, has a particular line of research that is relevant to the Priority Medicines Project. One of the objectives is to confront the global emergency caused by the three major communicable diseases – HIV/AIDS, tuberculosis (TB) and malaria – through the development of effective disease interventions, particularly for use in developing countries. This line of research envisages that developing countries will be significant partners and will participate directly in specific activities within the Sixth Framework Programme. Most recently, a call has been issued for research to address key areas linked to the “bottlenecks” in medicines development and these would include regulatory aspects (see Appendix 8.3.3). The Sixth Framework Programme has a budget allocation of about €2.2 billion for the life sciences area for the four years of the Programme. This allocation can be contrasted with the USA where the National Institutes of Health (NIH) has an annual budget of about US$ 30 billion (about €24.5 billion). While the Framework Programmes are major funders of health research in Europe, it is clear that the level of funding is dwarfed by the considerable amounts which EU Member States spend on such research. The EU supports the coordination of such efforts through a range of instruments such as the Priority Medicines Specific Support Action (SSA), which was initiated under the Sixth Framework Programme’s budget for life sciences.
2.8 European and Developing Countries Clinical Trials Partnership
The EU Member States and Norway have established the European and Developing Countries Clinical Trials Partnership (EDCTP), under an Article 169 Joint Programme of Activities.12 The collaboration will result in €400 million in research funds from the EU and national programmes to support clinical trials and build clinical trials capacity in the developing world. A new legal entity has been established to allow the EDCTP to operate flexibly, without being constrained by customary ways of working in any existing organization. This new model has been identified as an example of ʺgood practiceʺ which could be duplicated in relation to other diseases or phases of medicine development. The mission of the EDCTP is to accelerate the development of new clinical interventions to fight HIV/AIDS, malaria and TB in developing countries, particularly sub‐Saharan Africa, and to generally improve the quality of research in relation to these diseases. It is not yet clear whether in the future the EDCTP will also address other neglected diseases such as trypanosomiasis (sleeping sickness) or what will be
2. Background to the Priority Medicines Project
15
done to bridge the translational and preclinical gap between basic research and clinical trials.
2.9 National payment systems
European countries have a long history of social solidarity. This tradition has meant that governments either directly or through a social security system have made provisions for pharmaceuticals to be available to all. As a result, European governments have an interest in controlling expenditures and employ a wide range of price control mechanisms. However, in the USA, where only about 60% of people have health care coverage, these kind of price control mechanisms do not exist. The USA is the only member of the Organisation for Economic Co‐operation and Development (OECD) not to use some form of control on medicine prices (see Background Paper by Jacobzone).13 This makes the USA an attractive market for the launch of new products in an environment where profits are greater than in Europe. The difficulty faced by governments in promoting a productive pharmaceutical industry while trying to control health care costs has been the focus of numerous recent reports, described above in Chapter 2.4.

Priority Medicines for Europe and the World
16
References 1 Achilladelis B. The dynamics of technological innovation: the sector of antibacterial
medicines. Research Policy 1993;22 (4):279–308.
2 Harrison PF, Lederberg J, editors. Orphans and incentives: developing technology to address emerging infections. Washington D.C.: National Academy Press; 1997. Available from: http://www.nap.edu/catalog/5948.html (accessed 2 August 2004).
3 Goozner M. The $800 million pill. Berkeley (CA): University of California Press; 2004.
4 Turner, MJ. Developing new and effective medicines. Presentation given at the Royal Institute of International Affairs. London, 13 September 2003.
5 Gambardella A, Orsenigo L, Pammolli F. Global competitiveness in pharmaceuticals: a European perspective. Enterprise Papers No.1. Luxembourg: European Commission; 2001. http://mednet3.who.int/prioritymeds/report/append/22a_apx.pdf
6 Raising EU R&D intensity: improving the effectiveness of the mix of public support mechanisms for private sector research and development. Report to the European Commission by an Independent Expert Group; 2003. Available from: http://europa.eu.int/comm/research/era/3pct
7 Technology Platform for innovative medicines ‐ aims and objectives. Brussels: European Commission. Available from: http://www.cordis.lu/lifescihealth/innomed_aims.htm (accessed 26 August 2004).
8 The European Medicines Agency road map to 2010: Preparing the ground for the future. London: European Agency for the Evaluation of Medicinal Products (EMEA); 2003. Report No.: EMEA/H/34163/03. Executive Summary available from: www.emea.eu.int/pdfs/general/ direct/directory/3416303en.pdf (accessed 2 August 2004).
9 U.S. Food and Drug Administration, Department of Health and Human Services. Innovation stagnation: challenge and opportunity on the critical path to new medical products. Rockville (USA): Food and Drug Administration; 2004. http://mednet3.who.int/prioritymeds/report/append/barr_FDA_apx1.pdf
10 Research and the European Union, Parliamentary Office of Science and Technology, Summary Report. London: Parliamentary Office of Science and Technology; 1996. Available from: http://www.parliament.uk/post/pn083.pdf (accessed 13 March 2004).
11 Fifth Framework Programme. Luxembourg: European Commission. Available from: http://www.cordis.lu/life/src/part_docs.htm (accessed 8 March 2004).
12 European and Developing Countries Clinical Trial Partnership, Joint Programme of the Action, Part A, Technical content and the overall work plan for the entire period of the Action, Annex I Part A, Final draft 13 November 2003.
13 Jacobzone S. Pharmaceutical policies in OECD countries: reconciling social and industrial goals, labour market and social policy. Occasional Papers No. 40. Paris: Organisation for Economic Co‐operation and Development; 2000. Report No.: DEELSA/ELSA/WD(2000)1. http://mednet3.who.int/prioritymeds/report/append/22d_oecd_apx.pdf
3. Approaches to priority-setting
17
3. Approaches to priority-setting 3.1 Introduction
This chapter reviews the various approaches which have been used to set priorities for health research — internationally and nationally — and explains the rationale for the choice of methods used in this Project. The key message underlined here is that all methods of priority‐setting have limitations and that different methods need to be used, depending on the different circumstances.
3.2 International approaches to priority‐setting
Since the late 1980s, there have been many attempts by various international organizations and less formal groups to develop methods for prioritizing health research (see also Annex to Chapter 3). During the 1990s, a series of commissions undertook studies aimed at priority‐setting for health or for health research. Although none of these specifically focused on pharmaceutical research, the methods used have influence the approach used in this Project. The Commission on Health Research for Development (1990) was an independent international initiative formed in 1987 with the aim of improving the health of people in developing countries through a focus on research (see Appendix 3.1). The World Development Report (1993) 1 was produced by the World Bank in conjunction with the World Health Organization (WHO). This report used a measure of the Burden of Disease and the Disability Adjusted Life Year (DALY), which have also been used in this Project (see Appendix 3.2). The Ad Hoc Committee on Health Research (1996) was established in 1994 by WHO. A major contribution of this Committee was the identification of specific high priority product development opportunities using a systematic “five‐step” process which is the basis of the conceptual model used in this project.2 More recently, other organizations have continued to build on previous efforts to establish priorities for global health research. The Global Forum for Health Research (2000)3 has created a framework (Combined Approach Matrix) (see Appendix 3.6) which brings together in a systematic manner all information (current knowledge) related to a particular disease or risk factor. The framework allows identification of common factors by looking across diseases or risk factors. Completing the matrix should highlight the “blank areas”, i.e., where there are gaps in information needed to make rational decisions. This method was updated in

Priority Medicines for Europe and the World
18
2004. The approach used in the Priority Medicines Project is based, in part, on this methodology (see Chapter 4). WHO‐IFPMA Round Table (2000‐2001) was a joint task force, comprising representatives of WHO and the International Federation of Pharmaceutical Manufacturers Associations (IFPMA), convened to establish a working list of infectious diseases and to review disease burden as a way of directing research priorities. In addition to using DALYs to measure the impact of disease, the task force also used additional criteria such as mortality, societal costs, likelihood of treatment, and future trends. They then reviewed existing interventions on the basis of availability and any limitations of medicines. The task force also reviewed current levels of industry activity for each disease. A judgement on the need for additional medicines R&D was therefore made on the basis of both the current and likely future availability of medicines and of other treatment approaches. Altogether a combination of 17 assessment criteria were used. The final results and recommendations were never published (see Appendix 3.7). The UNICEF‐UNDP‐World Bank‐WHO Special Programme for Research and Training in Tropical Diseases (TDR) prioritizes research by using an adapted version of the Global Forum’s framework for priority‐setting, expanded to include information on TDRʹs comparative advantages. This combined information is then used to define TDRʹs strategic research emphasis (see Appendix 3.4). This priority‐setting approach served as a starting point for efforts to develop an approach to a much broader range of diseases for use in the Priority Medicines Project.4 The U.S. National Institutes of Health (NIH) is the largest public funder of biomedical research in the world. In 1998, the Institute of Medicine (IOM) investigated the priority‐setting methods which the NIH uses to fund research. What is striking from the IOM report5 is the wide diversity of methods used in the different institutes which make up the NIH. The U.S. Food and Drug Administration (FDA): the U.S. drug regulatory authority has created categories of medicines, based on whether or not they demonstrate improvement over existing medicines. The USA defines a medicine as ʺPriorityʺ for regulatory purposes because it demonstrates that the product is a significant improvement over already marketed products. This may be for a new product or modification of an existing product. Such a designation facilitates the registration process.6 The European Medicines Agency (EMEA), Canada, and other regulatory agencies have similar designations. Although not intended for use in prioritizing research, in practice this designation rewards successful research.

3. Approaches to priority-setting
19
3.3 Private sector prioritization methods
Methods of prioritization in the pharmaceutical industry vary from company to company depending on their history and their strategic vision. Decisions about new medicines are generally made within a set of four different contexts: scientific opportunity, market assessment, available and required resources, and medical need. The common steps taken are to:
• Review the market place to identify unmet medical needs.
• Benchmark competitor products to understand the competitive landscape.
• Identify the market segments and patient populations a product will target.
• Identify all possible additional indications that might make the compound more valuable.
• Create a dosing and delivery profile to provide optimal dosing and delivery mechanisms.
• Understand the broad market preferences for the key characteristics of the product. The goal of market research at this point would be to find a product profile which payers are willing to pay for and which provides a sufficient return on investment (for example, is the product profile such that physicians would prescribe it at the levels needed to justify further development?).
• Assemble market research to profile key geographic markets to ensure product success.
The strength of this approach is that it clearly identifies products that the ʺmarketʺ is willing to pay for and that will ensure an adequate return on investment. Unfortunately, this approach will ignore diseases which mainly affect the poor in low‐income countries.
3.4 Conceptual framework for the Priority Medicines Project
Priority‐setting generally uses two main approaches: technical analysis, which depends on different sources of ʺevidenceʺ; and interpretive assessments, which depend on expert opinion. Both methods have strengths and weaknesses. The Project used different methods from the spectrum of possible approaches: available evidence; predictions and trends; and social solidarity. A framework for this kind of analysis has been developed by the University of Colorado and adapted for use by the United Kingdom National Institute for Clinical Excellence (NICE) (see Figure 3.1).

Priority Medicines for Europe and the World
20
Figure 3.1: A cognitive continuum framework
INTUITION
ANALYSIS
Quality ofAnalysis
Quality ofIntuition
Least precise/explicit Most precise/explicit
MODE: 7 6 5 4 3 2 1
Knowledge Generation
Decision/Policy Making
non-cognitive
judgement
clinicaljudgement
expertconsensusjudgement
descriptivemodels
casecontrolstudy
randomizedcontrolled
trial
laboratoryexperiment
non-cognitive
judgement
clinicaljudgement
expertconsensusjudgement
decisionmodels
Source: J. Dowie. In: Health Care Priority Setting. A. Oliver ed. Nuffield Trust, UK
3.5 Providing a “menu” of complementary approaches for policy‐makers
In efforts to establish priorities for pharmaceutical research, the Priority Medicines Project has used three complementary approaches. For the purposes of this Report, where adequate data are available on burden of disease and on the efficacy or lack of efficacy of treatments, an evidence‐based approach has been used (Modes 1‐2 in Figure 3.1). Where data on burden of disease or efficacy do not exist, projection or trend analysis methods have been used (Modes 4‐6 in Figure 3.1). For orphan and neglected diseases or where market failures occur, principles of social solidarity have been applied (Modes 4‐7 in Figure 3.1). See Background Chapter 3. In order to bring complementary information to this approach, we have used the framework developed by the Global Forum for Health Research to ask additional questions about the current state of diseases of interest. This involved obtaining information, in a standardized way, about the conditions identified using the evidence‐based approach: the current ʺstate of the artʺ of scientific knowledge; the medicine R&D pipelines; and the funds allocated for research on various therapeutic interventions.

3. Approaches to priority-setting
21
A. Priorities based on an evidence‐based approach (e.g., acute stroke, chronic obstructive pulmonary disease, Alzheimer disease): Modes 1 and 2 in Figure 3.1
For this approach, burden of disease analysis has been combined with assessments of the data produced by WHO and systematic reviews of randomized clinical trials undertaken by the Cochrane Reviews. Each of the burden of disease and clinical efficacy analyses has important limitations which are discussed in Chapter 4. At best, the combination of burden of disease and clinical efficacy provides a preliminary, quantitative and retrospective view of pharmaceutical gaps. This is because the Cochrane Reviews do not include reviews of newer or very old therapeutic interventions (see Background Chapter 4).
B. Priorities based on projections and trends (e.g., antimicrobial resistance, pandemic influenza): Modes 4‐7 in Figure 3.1
Looking ahead, what are the emerging diseases that could affect the EU and the world? What existing diseases or risk factors will grow in importance? The answers to these questions form the second prioritization method and are based primarily on consensus judgements and observational and clinical evidence. Although antibacterial resistance is not a disease or condition per se, its importance as a threat to global public health is expected to continue to grow. The same holds true for pandemic influenza.
C. Priorities based on social solidarity (e.g., “orphan” and neglected diseases): Modes 4‐7 in Figure 3.1
The ethical and moral aspects of priority‐setting have been selected as the third prioritization method along the continuum of Figure 3.1. Ethics and moral values are often invoked to mobilize support for various health initiatives, and theories of social justice (e.g., the fair and equitable treatment of people) have attempted to justify medicine and public health as a special ʺsocial goodʺ (see Background Chapter 3). Many European countries have a long history of social solidarity. This has been demonstrated by the creation of universal social security systems and of national health systems which are intended to ensure universal access to medical care and pharmaceuticals. In the EU and elsewhere, governments have enacted legislation to protect the interests of people suffering from rare (“orphan”) diseases. This requires society to spend substantial funds on a limited number of people who suffer from rare diseases such as Gaucher Disease. At a global level, based on principles of global solidarity, similar efforts are needed to address neglected diseases, which mainly affect the poor in low‐income countries as well as other poor populations. In response, orphan and neglected diseases have been selected as priority diseases, even though the former affect small numbers of patients and the latter affect patients living outside the EU. Special patient groups (the elderly, women and children) are also considered since these groups often lack effective medicines.

Priority Medicines for Europe and the World
22
3.6 Conclusion
In this Report, three complementary approaches to prioritization are used in an effort to overcome the inadequacies of any one of these approaches when used exclusively. For those decision‐makers who would like to use only evidence‐based approaches, it should be noted that absence of evidence does not necessarily mean there is no threat or need. For those who would prefer to use a consensus‐based expert opinion approach, it should be pointed out that such expert groups have often missed important developments. And while an approach based on the use of projections and trends is critical in efforts to prepare for future threats to global public health, it inevitably involves the use of judgements made on the basis of uncertain information. Finally, for those who would use social solidarity as the sole criterion for prioritization, it is important to note that there are many people, both rich and poor, from developed and developing countries, who have benefited substantially from medical advances achieved as a result of approaches based on evidence or projections and trends. They should continue to receive these benefits. In the final analysis, ALL methods must be used to achieve a balanced and optimal result. By using these three approaches, the health needs of both Europe and the world have been taken into account in addressing pharmaceutical gaps for diseases of current and future public health importance, including neglected diseases. References 1 World Bank. World Development Report 1993: Investing in Health. New York: Oxford
University Press; 1993.
2 Ad Hoc Committee on health research relating to future intervention options. Investing in health research and development. Geneva: World Health Organization; 1996. Report No.: TDR/Gen/96.1.
3 Global Forum for Health Research. Website: http://www.globalforumhealth.org (accessed 12 March 2004).
4 The UNICEF‐UNDP‐World Bank‐WHO Special Programme for Research and Training in Tropical Diseases (TDR). Geneva: World Health Organization. Website: http://www.who.int/tdr (accessed 8 March 2004).
5 National Institutes of Health. Scientific opportunities and public needs, improving priority setting and public input. Washington D.C.: National Academy Press; 1998.
6 Fast track, priority review and accelerated approval. Rockville (USA): U.S. Food and Drug Administration, Center for Drug Evaluation and Research; 2004. Available from: http://www.accessdata.fda.gov/scripts/cder/onctools/Accel.cfm (accessed 12 March 2004).

4. Methods used in the Priority Medicines Project
23
4. Methods used in the Priority Medicines Project
4.1 Introduction
This Project has combined a number of methods to produce a methodology that can be used for priority‐setting at country, regional and global levels. The method is intended to be explicit and reproducible (source data are provided on the CD‐ROM and website). This chapter provides details of the complementary approaches used: the evidence‐based approach, the predictive framework and the social solidarity approach.
Figure 4.1: Schematic of the methodology used in the Priority Medicines Project
Burden of disease rankingEU10, EU25
The world (including EU25)
Cochrane database of systematic reviews
Clinical efficacy
FINAL REPORT
Projectionsand trends
Socialsolidarity
PRELIMINARY LISTOF PRIORITY DISEASES AND
GAPS
IN DEPTH REVIEWS OF PRELIMINARY LIST OF DISEASES AND GAPS
4.2 Methodology
The method uses analyses of several different factors: demographics, burden of disease and clinical efficacy.
1. A ranking exercise was carried out using burden of disease information (disability adjusted life years (DALYs) and mortality) to generate the major disease conditions which account for the majority of the total DALY burden and the total mortality burden in both the EU25 and the rest of the world (see Tables 5.3 and 5.4 in Chapter 5).
Priority Medicines for Europe and the World
24
2. The Cochrane Database of Systematic Reviews was then used to determine in a quantitive manner whether, on balance, the pharmaceutical interventions available to treat these high burden diseases were clinically efficacious. Where the reviews revealed that a treatment gap existed, the disease/condition was included in the Preliminary List. However, since the Cochrane reviews lack information on a number of major diseases (e.g., infectious diseases, diabetes), an approach based on health‐related projections and trends was also used to further define the Preliminary List. For example, it is clear that multidrug‐resistant TB is an ongoing public health problem in Eastern Europe. And in view of the recent concern over SARS and avian influenza, pandemic influenza was also included in the Preliminary List. This approach is discussed in more detail below. Another complementary approach involved the use of criteria including social justice, social solidarity and equity to set priorities. In this way, pharmaceutical gaps were identified for orphan and neglected diseases and for special patient groups. This is discussed in more detail below and in Chapter 3. 3. The Preliminary List was then reviewed to update information on the diseases/conditions using a standard set of questions (see Chapter 4.5). Detailed reports based on these questions are included in Chapter 6 of this Report. Key aspects of the methodology are discussed in more detail below.
Burden of disease
A. Disability Adjusted Life Years (DALYs)
The major groups of diseases/conditions are defined as follows: mental health, cardiovascular, cancers, injuries, respiratory conditions, digestive conditions, musculoskeletal/rheumatoid conditions, infectious diseases, nutrition/endocrine disorders, sensory organ disorders, maternal conditions, oral conditions, urinary system conditions, and congenital anomalies. Over the past decade, WHO, the World Bank and many other organizations have used and promoted the concept of DALYs as an integrated measure of mortality and disability. The indicator combines mortality and morbidity in a single measure. One DALY can be thought of as one lost year of ‘healthy’ life and the burden of disease as a measurement of the gap between current health status and an ideal situation where everyone lives into old age free of disease and disability. Although the WHO global burden of disease methodology is not perfect, it is the best single tool available for the audience of this Report, i.e., strategic planners and decision‐makers. It provides a single summary measure of ill health, a fundamental tool for policy‐makers when considering the relative benefits of different policy options. Measuring the burden of disease using DALYs is well‐established in Europe. It can be broken down to show the relative contributions of different conditions to the overall

4. Methods used in the Priority Medicines Project
25
burden of disease, it can show the burden of disease that can be attributed to known risk factors, and can be combined with cost to assess cost‐effectiveness. In calculating DALYs, this Report uses existing data sources for the EU15, EU10, EU25 and the world, obtained from the WHO Global Burden of Disease Database.1
B. Mortality
Mortality is also used here as a measure of burden of disease as this is easy to understand. However, this measure is not able to reflect the burden of pain and suffering experienced by patients with chronic diseases such as osteoarthritis. The mortality data used here are from the WHO Global Burden of Disease Database which estimates global and regional mortality. These data have been disaggregated into broad categories and then into specific disease categories and are made available by country, sex and age group.
C. Demographics
The demographic component of this Report is based on regional and international public databases and on reviews of global and regional reports.2
Clinical efficacy
To determine pharmaceutical gaps, what is needed is a measure of the clinical efficacy of different pharmaceutical interventions. The primary data source for this is the analyses found in the Cochrane Database of Systematic Reviews. These systematic reviews, based on relevant studies from the international medical literature, are conducted by the international Cochrane Collaboration, an organization of over 7000 health professionals, researchers, scientists and consumers from approximately 80 countries. There are 50 international Cochrane review groups. These highly structured reviews summarize and synthesize results from the highest quality research studies, usually randomized, placebo‐controlled trials. The results are combined statistically. The work of the Cochrane Groups is considered the gold standard in the search for the best systematic reviews of medical evidence. However, the Cochrane Database has a number of limitations. One of the drawbacks is that these reviews are retrospective in the sense that the most recent interventions or products lacking market approval may not have sufficient numbers of patients to warrant a systematic review. Moreover, some of the interventions that are reviewed may no longer be used in clinical practice or have been superseded by other, more efficacious interventions. Another drawback is that most trials data in the Cochrane Database are placebo‐controlled trials. Where possible, decisions should be based on comparison of new interventions with current practice, not with placebos (see Chapter 8.4). What is important from a public health viewpoint is not whether a new intervention works better than “nothing”, but whether it works better than the current best available treatment. Another limitation of the Cochrane Database is the lack of data on adverse events – information which is useful in determining priorities (see Annex to Chapter 5).The randomized clinical trials in the

Priority Medicines for Europe and the World
26
database are designed to assess efficacy and only occasionally report side‐effects. Analyses of the available data on adverse events from the Cochrane Database were not used in determining priorities because only a small number of trials were involved. The difficulty faced in obtaining this data underlines the need to improve the regulatory process using Phase IV research (post‐marketing surveillance) to collect data on both adverse events and exposure to pharmaceuticals in large numbers of patients.
Relative Risk as a measure of clinical efficacy
The Cochrane system uses different statistical measures for summarizing the results of a large number of placebo‐controlled clinical trials. In order to display all of the data in a consistent way, the results from the original Cochrane tables of results have been recalculated into Relative Risk ratios. This involved the use of pooled mean estimates of the Relative Risk ratios from many trials involving the same intervention so that desired (i.e. beneficial) outcomes have ratios greater than 1. This has made it possible to display the results graphically in a way in which treatment effects better than placebo fall above the horizontal line (see Figure 4.2 below). Figure 4.2 shows the results obtained from many trials of different treatments for schizophrenia. The mean Relative Risk ratios derived from many trials for each intervention are displayed as square boxes in the vertical lines. These vertical lines represent ʺ95% confidence intervals,ʺ i.e., if the trials comprising the pooled results were repeated by resampling 100 times, in 95 of the 100 times, the true value for the mean Relative Risk ratios would fall somewhere along the vertical line.i The use of several square boxes for each intervention indicates that different dosages of the same medicine were tested. Where the square box is above the horizontal ʺ1ʺ line but the confidence interval line crosses below the horizontal ʺ1ʺ line this means that the benefits shown by the various clinical trials for the particular intervention might have occurred by chance alone. Therefore, in the statistical sense, the intervention has not been shown to have an unequivocal benefit. In the Background Chapter 5, there are a number of pages of these charts which have been used to generate a Preliminary List of priority conditions, as described below.
i Most confidence intervals involving ratios are asymmetric so the Relative Risk ratios are not in the middle of each vertical line.

4. Methods used in the Priority Medicines Project
27
Figure 4.2: Trial results for different schizophrenia treatments
Invasive bladder cancer in men(Local treatment with or without single or combination Pt therapy)
(Outcome: death)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
. . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s no
Pt t
hera
py)
Single agent Pt therapy
Pooled data
Combination Pt therapy
Pooleddata
In order to establish a preliminary list of conditions with a high burden of disease and for which there appear to be pharmaceutical gaps, the results of the many Cochrane Database meta‐analyses were reviewed and charts were then generated (as in Figure 4.2). Through the use of these charts it is possible to identify where pharmaceutical gaps exist, i.e., wherever the number of Relative Risk ratios where there is statistical benefit (confidence interval lines wholly above the horizontal line) is less than the number of ratios in which the lower end of the confidence interval line is below the ʺ1ʺ line. This is a statistically rigorous but crude overall measure as it does not take into account the absolute level of the relative risk measure, it may mix different treatments and outcomes, and depends heavily on how many meta‐analyses were performed. However, it is striking how, for some conditions, nearly all the pooled trial results consistently demonstrate efficacy (e.g. secondary treatment after myocardial infarction), while others, such as the treatment of acute stroke, consistently fail to demonstrate efficacy. An attempt was made to calculate risks of side‐effects but the data were incomplete and thus were not used to make the final preliminary assessments.
4.3 Approach based on projections and trends
The second priority‐setting approach that contributed to generating the list of high burden diseases for which there appear to be pharmaceutical gaps involved the use of health‐related projections and trends based primarily on consensus judgements and observational and clinical evidence. For example, various studies have demonstrated that multidrug‐resistant TB is an ongoing public health problem in Eastern Europe. In addition, resolutions of the World Health Assembly (WHA) and the European Parliament have identified antibacterial resistance as a serious threat to global public health. As a result, both of these have been included in the Preliminary List. Another

Priority Medicines for Europe and the World
28
example is diabetes. Although this is a disease of major global public health importance, it is poorly represented on the Cochrane database. Similarly, in view of the fact that the European and global population is aging rapidly, the Preliminary List includes some diseases/conditions that account for a high disease burden among the elderly. We have also relied on recent WHA resolutions for the inclusion of a number of additional diseases in the Preliminary List.3
4.4 Approach based on social solidarity
The final priority‐setting approach used concepts of social justice, social solidarity and equity to place on the Preliminary List certain conditions with pharmaceutical gaps, such as orphan and neglected diseases. Diseases affecting special patient groups (the elderly, women and children) are also included. The recent resolutions from the Joint EU/ACP Parliamentary Assembly have been considered in this section.4
4.5 Reviewing the Preliminary List: in‐depth reviews based on the Global Forum for Health Research approach
The diseases/conditions identified in the Preliminary List as having pharmaceutical gaps, were then rigorously reviewed by asking the following questions, based on the methods developed by the Global Forum on Health Research:
• What is the size and nature of the disease burden?
• What is the control strategy?
• Why does the disease burden persist?
• What can be learnt from past/current research into pharmaceutical interventions for this condition?
• What is the current “pipeline” of products that are to be used for this particular condition?
• What are the opportunities for research into new pharmaceutical interventions?
• What are the gaps between current research and potential research issues which could make a difference, are affordable and could be carried out in a) five years or b) in the longer term?
• For which of these gaps are there opportunities for pharmaceutical research?
Based on these specific reviews, for each condition, recommendations have been made on the steps needed to close the identified pharmaceutical gap. The methods described in this chapter are detailed in the background chapter and annexes. The original burden of disease databases and the spreadsheets of the Cochrane Database analyses are available on the CD‐ROM and website to enable review of the results and further analyses for different countries or regions.

4. Methods used in the Priority Medicines Project
29
References 1 WHO Statistical Information System (WHOLIS). Geneva: World Health Organization.
Available from: http://www.who.int/whosis/menu.cfm (accessed 12 March 2004).
2 State of world population. Making 1 billion count: investing in adolescents’ health and rights. New York: United Nations Development Programme; 2003. Press summary. Available from: http://www.unfpa.org/swp/2003/pdf/english/swp3summary_eng.pdf (accessed 8 March 2004).
3 World Health Organization. World Health Assembly announcements on Buruli ulcer and HIV/AIDS. Geneva: World Health Assembly; 2004. Report No.s: WHA57.1 and WHA57.14.
4 Africa, Caribbean, Pacific‐European Union (ACP‐EU) Joint Parliamentary Assembly Resolution on poverty‐related diseases and reproductive health in ACP States. Addis Ababa: ACP‐EU Joint Parliamentary Assembly; 2004. Report No.: ACP‐EU 3640/04/fin.

Priority Medicines for Europe and the World
30

5. Development of a Preliminary List of Priority Diseases
31
5. Development of a Preliminary List of Priority Diseases
5.1 Introduction
This chapter provides summary results of the data collected on demographic changes in Europe and the world, the burden of disease in these areas, and the results of the assessment of the efficacy of treatment for various diseases. The background chapter provides much of the data in a graphical format and readers are encouraged to refer to these charts. A few examples are provided here. Detailed tables of summary results are included in the annexes for this chapter. The purpose of the analysis reported in this chapter was to produce a summary list which would be the basis for in‐depth studies reported in Chapter 6.
5.2 Demographic indicators
Global situation
In todayʹs world of over 6 billion people, a number of demographic changes are having profound effects on global public health. Over the past 50 years, average life expectancy at birth has increased globally by almost 20 years. Another trend is an increase not only in the number but also in the proportion of the elderly in the population. As life expectancy increases, mortality and morbidity are increasingly shifting to older age groups — the majority of whom will be women. This widening of the sex differential in life expectancy was a central feature of mortality trends in developed countries in the twentieth century. Another trend is the rapid urbanization taking place around the globe. As a result of these trends, over the next 30 years, there will be a demographic shift to rapidly aging populations in large cities, particularly in Asia, Latin America and in some African countries. These demographic changes will be marked by an increase in noncommunicable diseases such as diabetes, mental conditions, cardiovascular disease (CVD) and osteoarthritis.
Europe
Between 1992 and 2000, the proportion of older people (65 years and over) in the EU15 population increased from 13% to 15%. The proportion of people 65 years and over in the EU10 is also expected to rise. The most dramatic increase in the EU15 in the future will occur in the number of very old people (aged over 80), which is expected to increase dramatically over the next 15 years. In 1900, in Europe and North America, women typically outlived men by two or three years. Today, the average gap between the sexes is about seven years, but exceeds 12 years in parts of the former Soviet Union. In 2000, average life expectancy at birth for

Priority Medicines for Europe and the World
32
the EU15 Member States was 78 years (75 for men and 81 for women). In the new EU member countries, average life expectancy is lower, at 73 years. This gender difference in life expectancy means that for some diseases like osteoarthritis, the increase in prevalence will be particularly marked in older women. Related to this change has been a shift in the dependency ratio of potential workers to pensioners, which has fallen sharply. This trend towards ever‐increasing numbers of elderly is particularly severe in Germany and Italy, each of which is projected to have only 1.1 potential workers per pensioner by 2040. In Europe, these demographic trends will have economic and social consequences in a number of areas, including health and health care systems. From the financing perspective, aging imposes a higher economic burden on fewer people. Higher costs will occur, because the cost of health care for the elderly is far more than for younger age groups.
Figure 5.1: Average life expectancy at birth in EU countries
Avg EU15
Avg EU10
Avg EU25
68
70
72
74
76
78
80
1992 1993 1994 1995 1996 1997 1998 1999 2000Years
Ave
rage
life
exp
ecta
ncy
at b
irth
Source: WHO Global Burden of Disease Database (2003)
5.3 Burden of disease
Globally, five disease groups account for 70% of the total burden of disease as measured in DALYs (see Table 5.1 and Background Chapter 4 which defines the conditions found in the disease categories of Tables 5.1 and 5.2). Infectious disease is ranked number one worldwide, with 31% of the total burden, followed by mental conditions, injuries, CVD and maternal conditions (12.9%, 12.2%, 9.3% and 8.6% respectively of total DALY burden). In contrast, the expanded EU has a slightly different mix of diseases to account for 73% of its burden of disease. These five disease groups are mental conditions, CVD, cancer, injuries and respiratory conditions (25.3%, 17.1%, 16.7%, 8. 7% and 5.9%, respectively of the total burden). While the global burden of disease per capita is about 240 DALYs per 1000 people, it is only about 130 DALYs per 1000 people in the expanded EU. The disease groups contributing to this difference are infectious diseases (13.7 times greater per capita than in the expanded

5. Development of a Preliminary List of Priority Diseases
33
EU), maternal conditions (11.94 times higher), congenital anomalies (22.8 times higher) and injuries (1.60 times higher). Table 5.1: Burden of disease (DALYs) and per capita, by condition and region, 2002
(ranked in order of importance for EU15)
Source: WHO Global Burden of Disease Database (2003)
Mortality
The global mortality rate for all diseases is 9.16 deaths per 1000 people. The five groups of diseases with the highest mortality rates are: CVD (2.63 deaths per 1000), infectious diseases (2.47 per 1000), cancer (1.17 per 1000), injuries (0.83 per 1000), and respiratory conditions (0.59 per 1000). (See Table 5.2 which is not ranked according to mortality burden).
Table 5.2: Deaths and death rates (per 1000 people) by condition and region, 2002
Source: WHO Global Burden of Disease Database (2003)
Groups
Global EU25 EU15 EU10
Total Per1.000
% Total Per1.000
% Total Per1.000
% Total Per1.000
%
Mental 191,660,642 30.8 12.9% 14,857,720 32.8 25.3% 12,379,282 32.7 26.3% 2,478,438 33.27 21.16%CVD 138,013,023 22.2 9.3% 10,088,093 22.2 17.1% 7,637,493 20.1 16.2% 2,450,599 32.90 20.92%Cancer 77,152,633 12.4 5.2% 9,839,035 21.7 16.7% 7,989,864 21.1 16.9% 1,849,172 24.82 15.78%Injuries 182,590,897 29.3 12.2% 5,099,011 11.2 8.7% 3,644,620 9.6 7.7% 1,454,392 19.52 12.41%Respiratory 55,059,995 8.9 3.7% 3,523,243 7.8 5.9% 3,167,675 8.4 6.7% 355,568 4.77 3.04%Digestive 46,300,182 7.4 3.1% 2,925,351 6.5 4.9% 2,205,780 5.8 4.7% 719,571 9.66 6.14%Musculoskeletal 28,349,766 4.6 1.9% 2,563,271 5.7 4.4% 1,994,910 5.3 4.2% 568,362 7.63 4.85%Infections 462,516,353 74.3 31.0% 2,282,694 5.0 3.9% 1,849,365 4.9 3.9% 433,329 5.82 3.70%Nutrition/End 61,520,078 9.9 4.1% 2,390,372 5.2 4.0% 2,042,736 5.4 4.3% 347,636 4.67 2.97%Sense organs 69,379,818 11.2 4.7% 2,868,843 6.3 4.9% 2,248,811 5.9 4.8% 620,032 8.32 5.29%Maternal 128,884,629 20.7 8.6% 725,905 1.6 1.2% 593,440 1.6 1.2% 132,464 1.78 1.13%Oral 7,372,021 1.2 0.5% 434,767 0.9 0.7% 343,829 0.9 0.7% 90,937 1.22 0.78%Urinary 15,213,854 2.4 1.0% 601,238 1.3 1.0% 498,616 1.3 1.0% 102,622 1.38 0.88%Congenital 27,402,428 4.4 1.9% 608,304 1.3 1.0% 496,447 1.3 1.0% 111,857 1.50 0.95%Total 1,491,416,317 239.6 100% 58,807,846 129.7 100% 47,092,868 124.2 100% 11,714, 978 157.26 100%
Groups
Global EU25 EU15 EU10
Total Per1.000
% Total Per1.000
% Total Per1.000
% Total Per1.000
%
Mental 191,660,642 30.8 12.9% 14,857,720 32.8 25.3% 12,379,282 32.7 26.3% 2,478,438 33.27 21.16%CVD 138,013,023 22.2 9.3% 10,088,093 22.2 17.1% 7,637,493 20.1 16.2% 2,450,599 32.90 20.92%Cancer 77,152,633 12.4 5.2% 9,839,035 21.7 16.7% 7,989,864 21.1 16.9% 1,849,172 24.82 15.78%Injuries 182,590,897 29.3 12.2% 5,099,011 11.2 8.7% 3,644,620 9.6 7.7% 1,454,392 19.52 12.41%Respiratory 55,059,995 8.9 3.7% 3,523,243 7.8 5.9% 3,167,675 8.4 6.7% 355,568 4.77 3.04%Digestive 46,300,182 7.4 3.1% 2,925,351 6.5 4.9% 2,205,780 5.8 4.7% 719,571 9.66 6.14%Musculoskeletal 28,349,766 4.6 1.9% 2,563,271 5.7 4.4% 1,994,910 5.3 4.2% 568,362 7.63 4.85%Infections 462,516,353 74.3 31.0% 2,282,694 5.0 3.9% 1,849,365 4.9 3.9% 433,329 5.82 3.70%Nutrition/End 61,520,078 9.9 4.1% 2,390,372 5.2 4.0% 2,042,736 5.4 4.3% 347,636 4.67 2.97%Sense organs 69,379,818 11.2 4.7% 2,868,843 6.3 4.9% 2,248,811 5.9 4.8% 620,032 8.32 5.29%Maternal 128,884,629 20.7 8.6% 725,905 1.6 1.2% 593,440 1.6 1.2% 132,464 1.78 1.13%Oral 7,372,021 1.2 0.5% 434,767 0.9 0.7% 343,829 0.9 0.7% 90,937 1.22 0.78%Urinary 15,213,854 2.4 1.0% 601,238 1.3 1.0% 498,616 1.3 1.0% 102,622 1.38 0.88%Congenital 27,402,428 4.4 1.9% 608,304 1.3 1.0% 496,447 1.3 1.0% 111,857 1.50 0.95%Total 1,491,416,317 239.6 100% 58,807,846 129.7 100% 47,092,868 124.2 100% 11,714, 978 157.26 100%
Global EU25 EU15 EU10
Deaths Rate (x000)
% Deaths Rate (x000)
% Deaths Rate (x000)
% Deaths Rate (x000)
%
Mental 1,104,861 0.18 1.94% 184,943 0.41 4.25% 172,239 0.45 4.79% 12,704 0.17 1.70%CVD 16,398,754 2.63 28.76% 1,816,431 4.00 41.78% 1,438,274 3.79 39.97% 378,157 5.08 50.53%Cancer 7,272,814 1.17 12.75% 1,177,355 2.60 27.08% 983,792 2.60 27.34% 193,563 2.60 25.86%Injuries 5,188,115 0.83 9.10% 225,887 0.50 5.20% 170,794 0.45 4.75% 55,092 0.74 7.36%Respiratory 3,696,309 0.59 6.48% 227,154 0.50 5.23% 208,522 0.55 5.79% 18,632 0.25 2.49%Digestive 1,962,517 0.32 3.44% 204,457 0.45 4.70% 167,704 0.44 4.66% 36,753 0.49 4.91%Musculoskeletal 104,873 0.02 0.18% 15,765 0.03 0.36% 15,044 0.04 0.42% 721 0.01 0.10%Infections 15,363,334 2.47 26.94% 274,716 0.61 6.32% 247,636 0.65 6.88% 27,080 0.36 3.62%Nutrition 1,705,758 0.27 2.99% 130,230 0.29 3.00% 117,781 0.31 3.27% 12,449 0.17 1.66%Sense organs 3,208 0.00 0.01% 141 0.00 0.00% 135 0.00 0.00% 6 0.00 0.00%Maternal 2,902,560 0.47 5.09% 11,650 0.03 0.27% 9,262 0.02 0.26% 2,388 0.03 0.32%Oral 1,627 0.00 0.00% 214 0.00 0.00% 196 0.00 0.01% 18 0.00 0.00%Urinary 847,168 0.14 1.49% 66,123 0.15 1.52% 57,497 0.15 1.60% 8,626 0.12 1.15%Congenital 475,387 0.08 0.83% 12,205 0.03 0.28% 9,938 0.03 0.28% 2,267 0.03 0.30%Total 57,027,285 9.16 100% 4,347,270 9.58 100% 3,598,815 9.49 100.00% 748,455 10.05 100.00%
Groups
Global EU25 EU15 EU10
Deaths Rate (x000)
% Deaths Rate (x000)
% Deaths Rate (x000)
% Deaths Rate (x000)
%
Mental 1,104,861 0.18 1.94% 184,943 0.41 4.25% 172,239 0.45 4.79% 12,704 0.17 1.70%CVD 16,398,754 2.63 28.76% 1,816,431 4.00 41.78% 1,438,274 3.79 39.97% 378,157 5.08 50.53%Cancer 7,272,814 1.17 12.75% 1,177,355 2.60 27.08% 983,792 2.60 27.34% 193,563 2.60 25.86%Injuries 5,188,115 0.83 9.10% 225,887 0.50 5.20% 170,794 0.45 4.75% 55,092 0.74 7.36%Respiratory 3,696,309 0.59 6.48% 227,154 0.50 5.23% 208,522 0.55 5.79% 18,632 0.25 2.49%Digestive 1,962,517 0.32 3.44% 204,457 0.45 4.70% 167,704 0.44 4.66% 36,753 0.49 4.91%Musculoskeletal 104,873 0.02 0.18% 15,765 0.03 0.36% 15,044 0.04 0.42% 721 0.01 0.10%Infections 15,363,334 2.47 26.94% 274,716 0.61 6.32% 247,636 0.65 6.88% 27,080 0.36 3.62%Nutrition 1,705,758 0.27 2.99% 130,230 0.29 3.00% 117,781 0.31 3.27% 12,449 0.17 1.66%Sense organs 3,208 0.00 0.01% 141 0.00 0.00% 135 0.00 0.00% 6 0.00 0.00%Maternal 2,902,560 0.47 5.09% 11,650 0.03 0.27% 9,262 0.02 0.26% 2,388 0.03 0.32%Oral 1,627 0.00 0.00% 214 0.00 0.00% 196 0.00 0.01% 18 0.00 0.00%Urinary 847,168 0.14 1.49% 66,123 0.15 1.52% 57,497 0.15 1.60% 8,626 0.12 1.15%Congenital 475,387 0.08 0.83% 12,205 0.03 0.28% 9,938 0.03 0.28% 2,267 0.03 0.30%Total 57,027,285 9.16 100% 4,347,270 9.58 100% 3,598,815 9.49 100.00% 748,455 10.05 100.00%
Groups
Priority Medicines for Europe and the World
34
Cardiovascular disease is the leading cause of death in all regions studied, accounting for more than a quarter of the deaths at the global level and over 40% in the expanded EU. Infectious disease is the second leading cause of mortality globally (26.94%) but accounts for less than 7% of disease burden in the expanded EU.
5.4 EU and the world (commonality of interest)
Globally, 20 major diseases account for nearly 60% of the total DALY burden in both the expanded EU and the rest of the world. Of these diseases, several are among the major contributors to the burden of disease both globally and in the EU25. As shown in Table 5.3, the high burden diseases common to both regions (marked in grey) are unipolar depression, ischaemic heart disease, cerebrovascular disease, chronic obstructive pulmonary disease (COPD) and “other digestive diseases”. With regard to the mortality burden (Table 5.4), unipolar depression is not a contributor but ischaemic heart disease, cerebrovascular disease and chronic obstructive pulmonary disease remain important. Various cancers, lower respiratory tract infections and diabetes are now important contributors to the commonality of interest between causes of death in the EU and the world as a whole. From Tables 5.3 and 5.4, it is very clear that smoking is a risk factor for many major preventable causes of mortality and morbidity in EU25 nations and throughout the world. For example, three of the top five causes of mortality in the expanded EU and the world (Table 5.4) are closely linked to smoking. Pharmacotherapy has a relatively small but nevertheless important role to play in the prevention of smoking‐related morbidity and mortality. However, it is important that expenditure on pharmaceutical products should not divert funds from other social and health policies designed to reduce smoking.

5. Development of a Preliminary List of Priority Diseases
35
Table 5.3: A commonality of interest (EU25 and the world) Combined DALYs for acute and chronic conditions
% DALYs % DALYsLower respiratory infections 5.8% 87,022,413 Unipolar depressive disorders 7.8% 4,562,824
HIV/AIDS 5.8% 86,072,449 Ischaemic heart disease 7.4% 4,352,119
Unipolar depressive disorders 4.5% 67,294,568 Cerebrovascular disease 5.3% 3,098,672
Diarrhoeal diseases 4.1% 61,095,069 Alcohol use disorders 4.2% 2,473,940
Ischaemic heart disease 3.9% 58,333,612 Other cardiovascular diseases 3.9% 2,265,104
Cerebrovascular disease 3.3% 49,117,639 Alzheimer and other dementias 3.5% 2,045,695
Other unintentional injuries 3.3% 48,681,728 Hearing loss, adult onset 3.4% 2,016,587
Low birth weight 3.1% 46,354,993 Trachea, bronchus, lung cancers 3.3% 1,931,408
Malaria 3.0% 44,715,596 Chronic obstructive pulmonary disease 3.0% 1,791,685
Other infectious diseases 2.7% 39,956,812 Other digestive diseases 2.8% 1,640,727
Road traffic accidents 2.6% 38,659,636 Other malignant neoplasms 2.5% 1,468,537
Tuberculosis 2.4% 35,361,041 Osteoarthritis 2.4% 1,413,905
Birth asphyxia and birth trauma 2.3% 34,482,934 Road traffic accidents 2.4% 1,406,167
Chronic obstructive pulmonary disease 1.9% 27,708,405 Other unintentional injuries 2.1% 1,225,167
Other digestive diseases 1.8% 27,354,033 Diabetes mellitus 2.0% 1,187,376
Measles 1.8% 27,057,601 Colon and rectum cancers 1.9% 1,139,030
Hearing loss, adult onset 1.7% 26,033,550 Cirrhosis of the liver 1.9% 1,112,110
Cataracts 1.7% 25,250,631 Self‐inflicted injuries 1.8% 1,087,030
Violence 1.4% 21,427,433 Breast cancer 1.7% 1,008,610
Self‐inflicted injuries 1.4% 20,835,502 Other respiratory diseases 1.7% 994,027
Total 58.5% 872,815,644 65.0% 38,220,720
Cause CauseWorld EU25
Note: Grey shading indicates diseases that are among the major contributors to disease burden both globally and in the EU25. ʺCirrhosis of the liverʺ includes alcoholic liver diseases but not liver cancer. By ʺalcohol use disordersʺ this report specifically means alcohol dependence and addiction.

Priority Medicines for Europe and the World
36
Table 5.4: A commonality of interest (EU25 and the world) Combined mortality for acute and chronic conditions
% Deaths % DeathsIschaemic heart disease 12.6% 7,168,113 Ischaemic heart disease 18.11% 787,142
Cerebrovascular disease 9.6% 5,493,698 Cerebrovascular disease 10.90% 473,892
Lower respiratory infections 6.6% 3,765,624 Other cardiovascular diseases 10.78% 468,511
HIV/AIDS 4.9% 2,821,472 Trachea, bronchus, lung cancers 5.38% 233,985
Chronic obstructive pulmonary disease 4.8% 2,745,816 Lower respiratory infections 4.01% 174,224
Other cardiovascular diseases 4.1% 2,357,038 Other malignant neoplasms 3.63% 157,730
Diarrhoeal diseases 3.1% 1,767,326 Colon and rectum cancers 3.46% 150,420
Other infectious diseases 2.9% 1,656,824 Chronic obstructive pulmonary disease 3.33% 144,879
Tuberculosis 2.8% 1,604,819 Other digestive diseases 2.51% 108,979
Low birth weight 2.2% 1,270,449 Breast cancer 2.18% 94,980
Trachea, bronchus, lung cancers 2.2% 1,238,867 Diabetes mellitus 2.18% 94,783
Malaria 2.1% 1,222,180 Alzheimer and other dementias 2.15% 93,380
Road traffic accidents 2.1% 1,191,732 Cirrhosis of the liver 1.76% 76,312
Diabetes mellitus 1.7% 986,837 Hypertensive heart disease 1.72% 74,966
Other unintentional injuries 1.6% 927,870 Prostate cancer 1.65% 71,562
Hypertensive heart disease 1.6% 906,873 Stomach cancer 1.61% 69,902
Other digestive diseases 1.6% 892,966 Other respiratory diseases 1.60% 69,762
Self‐inflicted injuries 1.5% 876,524 Self‐inflicted injuries 1.34% 58,316
Stomach cancer 1.5% 849,477 Pancreas cancer 1.33% 57,726
Cirrhosis of the liver 1.4% 783,166 Lymphomas, multiple myeloma 1.30% 56,412
Total 71.1% 40,527,670 80.90% 3,517,863
Cause CauseWorld EU25
Figure 5.2 displays the burden of disease as a percentage of the total DALY burden in each of the two regions — graphically illustrating the relative importance of selected disease/conditions in Europe and the world as a whole.

5. Development of a Preliminary List of Priority Diseases
37
Figure 5.2 A commonality of interest for Europe and the world EUROPE THE WORLD
?? ??
?? ??
* Includes bladder, breast, cervical,colon, uterine, lung liver, mouth, oesophageal, ovarian, pancreatic, prostate, stomach cancer and leukaemias, melanomas, lymphatic cancers and myelomas
** Cerebrovascular disease*** Chagas disease, dengue, leishmaniasis, lymphatic filariasis,
onchocerciasis, schistosomiasis, trypanosomiasis
10% 8% 6% 4% 2% 0 2% 4% 6% 8% 10% DALYsAntibacterial resistance
Pandemic influenza
Ischaemic heart disease
Diabetes mellitus
Cancer*
Acute stroke**
HIV/AIDS
Tuberculosis
Neglected diseases***
Malaria
Alzheimer and other dementias
Osteoarthritis
COPD
Alcohol use disorders
Unipolar depression
Maternal haemorrhage
5.5 Assessing treatment efficacy for acute and chronic high burden diseases/conditions
As described in Chapter 4, the Cochrane‐based method was used to identify a number of potential pharmaceutical gaps for the following diseases/conditions which account for a high burden of disease in the EU and the world. Smoking cessation treatments: Tricyclic antidepressant medicines, particularly nortriptyline (4 trials and 703 patients) and bupropion (16 trials and 5374 patients: see Figure 5.3) are efficacious although the clinical effects are quite modest. Bupropion leads to a near doubling of the likelihood of abstinence at 12 months, but the overall success rate was less than 20% in the treated groups. Clearly there is considerable scope for improvement (see Appendix 6.17).

Priority Medicines for Europe and the World
38
Figure 5.3
Smoking cessation(Outcome: abstinence after 6 or 12 months)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
. . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Fluoxetine
Sertraline
Paroxetine
All SSRI antidepressants
Nortriptyline
Bupropion:6 months
Bupropion:12 months
Depression in adolescents and the elderly: Depression is a common, yet under‐recognized problem in young people. Estimated prevalence ranges from 0.4% to 2.5% in primary school children, and from 0.4% to 8.3% in adolescents. Analysis of a ʺgapʺ for treating depression in children is based on nine trials (454 patients) and only for the use of tricyclic antidepressants. The burden of unipolar disease in EU25 children (0‐14 years) is about 140 000 DALYs for boys and about 135 000 DALYs for girls. The total DALY burden for all ages for the EU25 is very large (about 4.6 million DALYs). The detailed review of the epidemiology and of the present and possible future course of medicine development for depression in adolescents and the elderly in Background Chapter 6.15, supports the preliminary assessment based on the Cochrane review that better antidepressants are needed for adolescents and the elderly. Postpartum depression: Postpartum mental illness is an important and common problem which can have profound short‐ and long‐term effects on maternal morbidity, the infant/child and the family as a whole. Review of the Cochrane Database reveals only one trial involving 198 patients. Postpartum depression has been included as a potential ʺgapʺ because of its importance in the special patient populations described in Chapter 7.

5. Development of a Preliminary List of Priority Diseases
39
Figure 5.4
Depression in adults, children (Outcome: responders)
0
0.5
1
1.5
2
2.5
3
3.5
. . . . . . . . . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Progestogensfor postnataldepression
St. Johns Wort
TCAs in children and adolescentsImipramine
Fluoxetine
Sertraline
Phenelzine
Moclobemide
Amisulpride
Amineptine
Ritanserin
"Any drug"
Note: ʺTCAsʺ are tricyclic antidepressants Acute stroke: Analysis of the Cochrane reviews, and conclusion that a pharmaceutical gap exists, is based on 107 trials involving 96 531 patients. The burden of this condition in EU25 is about 3 million DALYs. From the retrospective Cochrane analysis, the vast majority of treatments for acute stroke are not statistically better than placebo. This preliminary view is corroborated by an in‐depth analysis of treatment for acute stroke (see Background Chapter 6.6).

Priority Medicines for Europe and the World
40
Figure 5.5
Treatment of acute stroke(Outcome: death - any cause at end of treatment or follow up unless noted otherwise)
0
0.5
1
1.5
2
2.5
3
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Any thrombolytic
Within 3 hours
Within 6hours
Lubeluzole(excitatory amino
acidantagonist)
Pentoxifyllinetheophylline
aminophylline
Tirilazad Steroids Variousheparinfractions
Amphetamines
Variousanticoagulants
Alzheimer disease: The burden of Alzheimer disease in the EU25 is about 2 million DALYs, higher than for lung cancer. The Cochrane reviews contain 17 separate analyses involving 5540 patients. Eleven of the 17 analyses showed that therapeutic interventions are not statistically better than placebo over time periods greater than about three months. This preliminary view is supported by in‐depth analysis of Alzheimer disease (see Background Chapter 6.11).
Figure 5.6
Alzheimer disease (Various outcomes)
0
1
2
3
4
5
. . . . . . . . . . . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Tacrine
Rivastigmine (two doses)
Galantamine (dose
LOW
MEDIUMHIGH
D-cycloserine
Donepezil(for
dementia due to
Alzheimer)
Memantine
Memantine: Alzheimer + vascular dementia
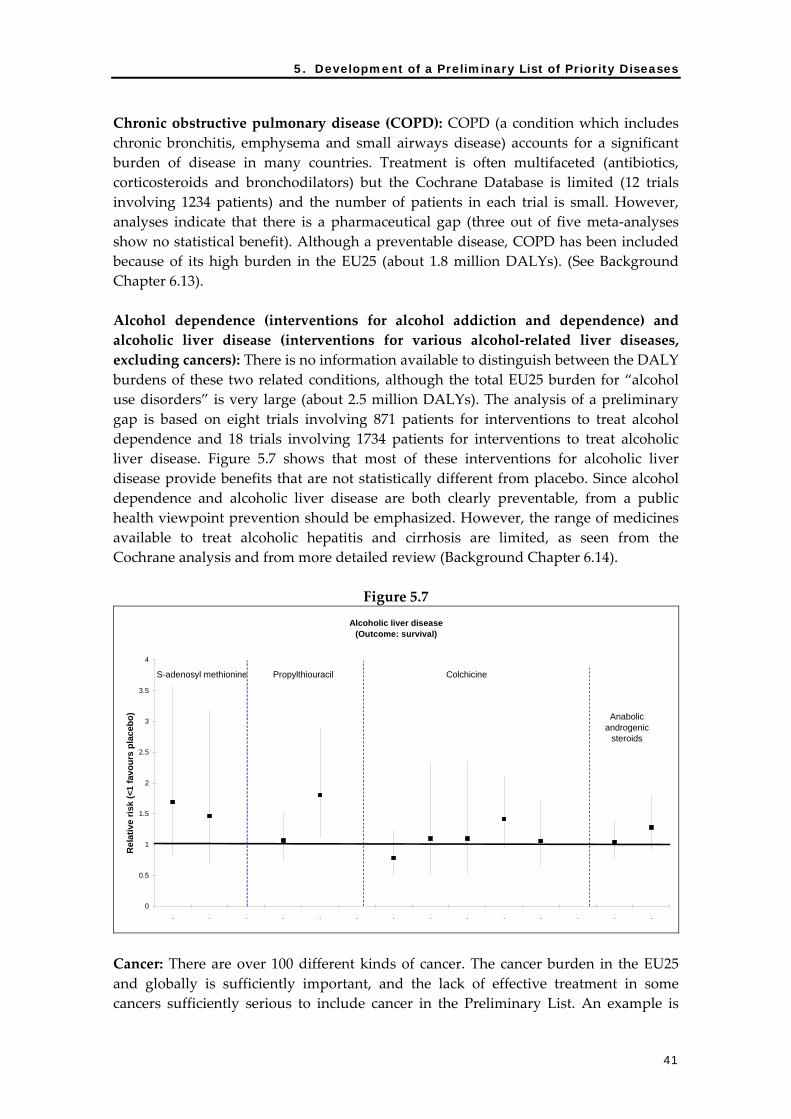
5. Development of a Preliminary List of Priority Diseases
41
Chronic obstructive pulmonary disease (COPD): COPD (a condition which includes chronic bronchitis, emphysema and small airways disease) accounts for a significant burden of disease in many countries. Treatment is often multifaceted (antibiotics, corticosteroids and bronchodilators) but the Cochrane Database is limited (12 trials involving 1234 patients) and the number of patients in each trial is small. However, analyses indicate that there is a pharmaceutical gap (three out of five meta‐analyses show no statistical benefit). Although a preventable disease, COPD has been included because of its high burden in the EU25 (about 1.8 million DALYs). (See Background Chapter 6.13). Alcohol dependence (interventions for alcohol addiction and dependence) and alcoholic liver disease (interventions for various alcohol‐related liver diseases, excluding cancers): There is no information available to distinguish between the DALY burdens of these two related conditions, although the total EU25 burden for “alcohol use disorders” is very large (about 2.5 million DALYs). The analysis of a preliminary gap is based on eight trials involving 871 patients for interventions to treat alcohol dependence and 18 trials involving 1734 patients for interventions to treat alcoholic liver disease. Figure 5.7 shows that most of these interventions for alcoholic liver disease provide benefits that are not statistically different from placebo. Since alcohol dependence and alcoholic liver disease are both clearly preventable, from a public health viewpoint prevention should be emphasized. However, the range of medicines available to treat alcoholic hepatitis and cirrhosis are limited, as seen from the Cochrane analysis and from more detailed review (Background Chapter 6.14).
Figure 5.7 Alcoholic liver disease
(Outcome: survival)
0
0.5
1
1.5
2
2.5
3
3.5
4
. . . . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
S-adenosyl methionine Propylthiouracil Colchicine
Anabolic androgenic
steroids
Cancer: There are over 100 different kinds of cancer. The cancer burden in the EU25 and globally is sufficiently important, and the lack of effective treatment in some cancers sufficiently serious to include cancer in the Preliminary List. An example is

Priority Medicines for Europe and the World
42
provided of two different platinum (Pt)‐based treatment regimens for bladder cancer (about 270 000 DALYs in the EU25) from the Cochrane Database (nine trials involving 2492 patients). Further analysis is found in Background Chapter 6.5, confirming the need to include cancer in the list of Priority Medicines.
Figure 5.8
Invasive bladder cancer in men(Local treatment with or without single or combination Pt therapy)
(Outcome: death)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
. . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s no
Pt t
hera
py)
Single agent Pt therapy
Pooled data
Combination Pt therapy
Pooleddata
Postpartum haemorrhage: This is a rare condition in Europe but a very serious problem in developing countries for women in the third stage of pregnancy. One of the main pharmacological reasons for these deaths is the absence of heat‐stable oxytocin. The global DALY burden for maternal haemorrhage is over 4.4 million DALYs. Thus, birth‐related conditions (9 of 15 analyses showing equivocal benefit), and specifically postpartum haemorrhage, are on the Preliminary List (see Background Chapter 6.16). Osteoarthritis: Osteoarthritis is a moderate burden in the EU25 (about 1.4 million DALYs) but will take on increasing importance as the population ages. Although the Cochrane Database is very weak (seven different trials involving only 471 patients), subsequent detailed analysis has revealed that pharmacological gaps include the lack of a curative therapy and the lack of a suitable biomarker for the disease (see Background Chapter 6.12). Secondary prevention of cardiovascular disease (CVD): Secondary prevention of CVD is included in the list because of recent evidence suggesting that there may be substantial public health benefits in combining in one pill low doses of several pharmaceuticals active in preventing secondary cardiovascular events (see Background Chapter 6.3).1 A large number of trials involving more than 100 000 patients have clearly demonstrated the value of antiplatelet agents (Figure 5.9) and ACE inhibitors (Figure 5.10) in preventing secondary events in patients who are at high risk of such
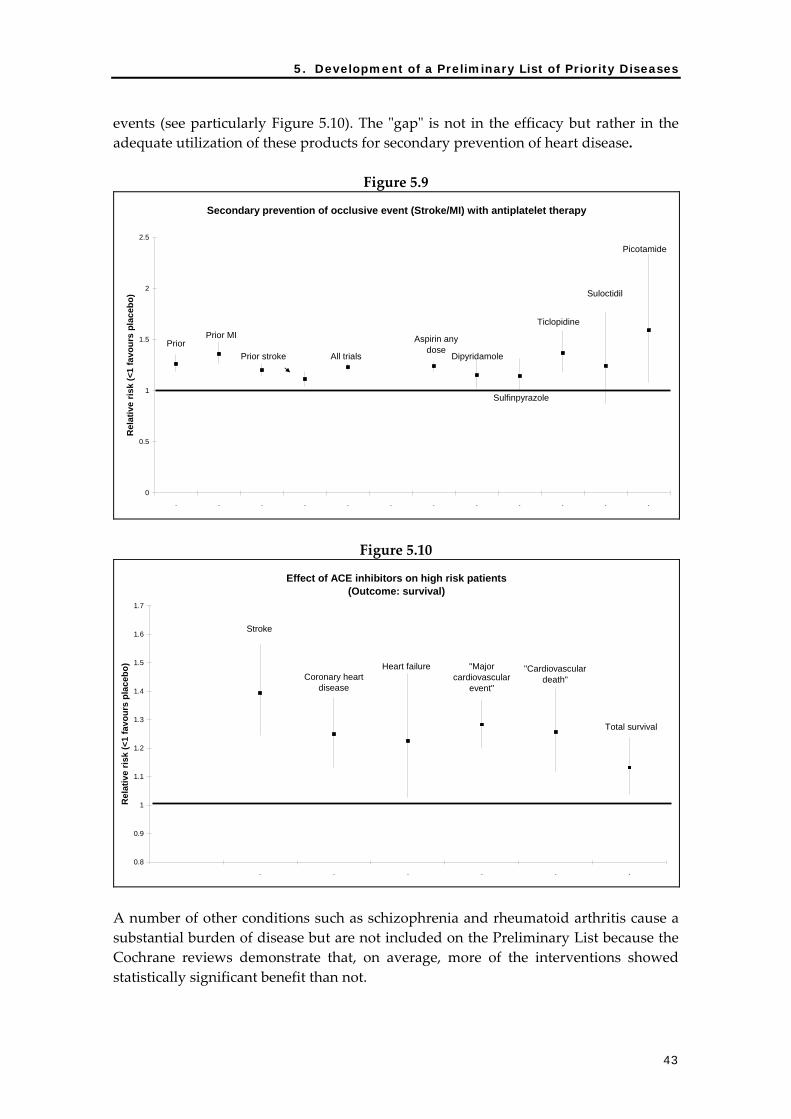
5. Development of a Preliminary List of Priority Diseases
43
events (see particularly Figure 5.10). The ʺgapʺ is not in the efficacy but rather in the adequate utilization of these products for secondary prevention of heart disease.
Figure 5.9
Secondary prevention of occlusive event (Stroke/MI) with antiplatelet therapy
0
0.5
1
1.5
2
2.5
. . . . . . . . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Prior Prior MI
Prior stroke All trials
Aspirin any dose
Dipyridamole
Sulfinpyrazole
Ticlopidine
Suloctidil
Picotamide
Figure 5.10
Effect of ACE inhibitors on high risk patients(Outcome: survival)
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
1.7
. . . . . .
Rel
ativ
e ris
k (<
1 fa
vour
s pl
aceb
o)
Stroke
Coronary heart disease
Heart failure "Major cardiovascular
event"
"Cardiovascular death"
Total survival
A number of other conditions such as schizophrenia and rheumatoid arthritis cause a substantial burden of disease but are not included on the Preliminary List because the Cochrane reviews demonstrate that, on average, more of the interventions showed statistically significant benefit than not.

Priority Medicines for Europe and the World
44
5.6 Priorities based on projections and trends
Antibacterial resistance, pandemic influenza, diabetes (Chapters 6.1, 6.2, 6.4, respectively). While the full extent of the present burden of antibacterial resistance is unknown, it has been included in the list due to its importance as a present and future global public health burden. Pandemic influenza is also included because of the enormous threat it poses to global public health. The risk of a pandemic on the scale of the 1918‐1919 pandemic, that is caused by a virus with a mortality rate equivalent to SARS, is a compelling reason to include pandemic influenza in the Preliminary List. Type 1 (insulin‐dependant) diabetes is at present neither curable nor preventable. Type 2 diabetes will be an increasing problem as the global population ages. Moreover, type 2 diabetes is now being seen in younger patients as well. Although to some extent preventable with non‐pharmacologic interventions, Type 2 diabetes is also incurable. There is a need to develop better insulins and insulin analogues to treat the disease.
5.7 Priorities based on social solidarity
This listing was based on the principles outlined in Chapters 3 and 4. It includes neglected diseases (6.9), diseases of the elderly (7.2), women (7.4), children (7.3) and orphan diseases (7.5), and the major infectious diseases with high mortality rates (HIV/AIDS, TB and malaria). (See 6.7, 6.8 and 6.10, respectively).

5. Development of a Preliminary List of Priority Diseases
45
5.8 Summary tables
On the basis of the data collected and the different criteria used, the following diseases/conditions have been identified as demonstrating pharmaceutical gaps. Their ranking here is based on the relative importance of these diseases/conditions based on the findings of this study, and on the potential for publicly funded research to have a major impact in reducing the burden of disease.
1. Infections due to antibacterial resistance 2. Pandemic influenza 3. Cardiovascular disease (secondary prevention) 4. Diabetes (Type 1 and Type 2) 5. Cancer 6. Acute stroke 7. HIV/AIDS 8. Tuberculosis 9. Neglected diseases 10. Malaria 11. Alzheimer disease 12. Osteoarthritis 13. Chronic obstructive pulmonary disease 14. Alcohol use disorders: alcoholic liver diseases and alcohol dependency 15. Depression in the elderly and adolescents 16. Postpartum haemorrhage
This Preliminary List will be discussed in more detail in Chapter 6 and the diseases are the subject of detailed in‐depth reviews in the background documents. Based on these studies specific recommendations are made for research activities related to specific aspects of the disease. Reference 1 Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. BMJ
2003;326(7404):1419‐1425.

Priority Medicines for Europe and the World
46

6. Priority diseases and reasons for inclusion
47
6. Priority diseases and reasons for inclusion
This chapter provides details of various diseases/conditions that have been reviewed in detail as part of this priority‐setting exercise. The diseases have been selected based on the preliminary exercise described in Chapters 4 and 5 and they have been ranked in order of their potential public health impact if the pharmaceutical gap remains. The first two diseases, infections due to antibacterial resistance and pandemic influenza, both pose enormous threats to global public health which will require major multisectoral responses. The next four diseases, cardiovascular disease (CVD), diabetes, cancer and acute stroke, are all chronic diseases with a clear ʺcommonality of interestʺ in both Europe and the world. Again, there are major differences in the research requirements for these diseases. The next group of diseases, HIV/AIDS, tuberculosis (TB), neglected diseases and malaria, are all infectious diseases which mainly affect people in developing countries. However the research needs vary. For HIV/AIDS, because of the number of cases occurring in developed countries, the industry invests substantially in research and development (R&D) for new treatments. For the other diseases, the major need is for translational research support to convert basic science advances into products that can be used in clinical trials by the European Developing Countries Clinical Trials Partnership (EDCTP). The next two diseases, Alzheimer and osteoarthritis, are primarily diseases of Europe where, despite major efforts by pharmaceutical companies, progress towards developing curative treatment or medicines to slow or reverse the progression of disease has been disappointing. These are diseases where basic research is needed to establish biomarkers. Two high burden diseases (chronic obstructive pulmonary disease (COPD) and alcoholic liver disease) are highlighted next. These are diseases for which treatment is inadequate but the conditions are preventable, by not smoking or by limiting alcohol intake, respectively. The last two conditions, depression in the elderly and adolescents, and postpartum haemorrhage, are included because, although effective treatment exists, the existing medicines have some limitations. Antidepressants often cause side‐effects and oxytocin, which is used to prevent postpartum haemorrhage, is not heat‐stable — making it difficult to use in developing countries, where it is needed most. This chapter should be read in conjunction with the background documents which provide additional details for all of the statements made in this Summary Report. In addition, some themes are revisited in Chapters 7 and 8.

Priority Medicines for Europe and the World
48
6.1 Antibacterial drug resistance
A. Background
The discovery of antibiotics in the mid‐twentieth century led to a revolution in the management and treatment of infectious diseases. Today, we are witnessing the emergence of drug resistance along with a decline in the discovery of new antibacterials. Both trends are due to challenges in developing new therapeutic agents and the withdrawal of some companies from the field. As a result, we are facing the possibility of a future without effective antibiotics. This would fundamentally change the way modern medicine is practised. It would jeopardize the outcome of treatment not only for common diseases like respiratory tract infections and urinary tract infections but also procedures such as transplant and joint replacement surgery, cancer and AIDS chemotherapy, which depend on the availability of effective antibiotics to treat or prevent infections. WHO has issued two World Health Assembly Resolutions on this topic and in 2001 launched a Global Strategy for the Containment of Antimicrobial Resistance.1 The European Union (EU) has also issued a number of different strategy documents.2,3,4 These documents stress the importance of concerted international action although the arguments have not been sufficiently convincing to place this issue high on the political agenda in individual countries. As responsibility for health remains predominantly national, there is a potentially significant disparity between the problems and potential solutions associated with antibacterial resistance and the institutions and mechanisms to deal with them. Both WHO and the EU have very limited powers to ensure implementation of recommendations in health matters, including containment of antibacterial resistance. Today, action is needed on many fronts: to stimulate basic and applied research and innovation of new antibacterial drugs and other treatment options in response to increased resistance; to reduce inappropriate use through the use of evidence‐based public health interventions; to improve prescribing and dispensing practices; and to conduct high‐quality surveillance of antibacterial resistance and of antibiotic consumption patterns in hospitals and the community. Resistance to antibiotics is a natural biological phenomenon. However, there is an obvious correlation between rates of use and the level of resistance, although the pace of emergence of resistance can vary from pathogen to pathogen and from medicine to medicine. Once resistance occurs, it is very difficult to reverse. Figure 6.1.1 shows the relationship (with regression line and its 95% upper and lower confidence intervals) between penicillin‐resistant pneumococci and antibiotic use as Defined Daily Dose (DDD). This development of resistance occurs at different rates.

6. Priority diseases and reasons for inclusion
49
Figure 6.1.1: Relationship between penicillin‐resistant pneumococci and outpatient antibiotic use (showing also the 95% confidence intervals)
Total antibiotic use (DDD/1000 population/day)
-
403020100
60
50
40
30
20
10
0
USA
UK
Sweden
Spain
Portugal
NorwayNetherlands
LuxembourgItaly
Ireland
Iceland
Greece
Germany
France
FinlandDenmark
Canada
BelgiumAustria
Australia
Taiwan, China
Peni
cilli
n-re
sist
ant S
. pne
umon
ia (%
)
Source: Albrich WC, Monnet DL, Harbarth S., Emerg Infect Dis 2004;10(3):514‐7
Rates of antibiotic use (penicillins as well as others) vary dramatically between countries in Europe. For example, antibiotic consumption is four times higher in France than in the Netherlands, although there is no reason to believe that the burden of infectious disease varies greatly between the two countries.5 Of particular concern is the mounting evidence from many European countries of a rapid increase in the rates of resistance to common organisms, which may result in these bacteria becoming untreatable. For example, the United Kingdom experienced an explosive increase in the level of blood culture isolates of methicillin‐resistant Staphylococcus aureus (MRSA) from less than 5% of Staphylococcus aureus infections to more than 50% within a decade.6

Priority Medicines for Europe and the World
50
Figure 6.1.2: The frequency of MRSA among blood cultures with Staphylococcus aureus in England and Wales 1992‐2002
0
5
10
15
20
25
30
35
40
45
50
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
% M
RSA
Years
Source: Health Protection Agency, UK
The health and economic impact of antibacterial resistance is profound and increasing. Failure of the initial antibiotic regimen due to resistant bacteria increases the risk of secondary complications and fatal outcome, underscoring the clinical dilemma of using broad or narrow spectrum empirical therapy and the prevailing lack of rapid diagnostic tests. Studies repeatedly show that mortality rates are twice as high in patients infected with resistant strains compared with those with non‐resistant strains, after taking into account differences in severity of illness and any underlying disease of affected patients. Estimates, which are mainly intended to give an impression of the order of magnitude of the resistance problem in Europe, indicate that MRSA nosocomial (hospital‐acquired) bacteremia is estimated to be responsible for 1277 deaths annually and an economic loss of €117 million. The annual costs of MRSA bloodstream infections alone already exceed the EU budget for antibacterial resistance research for 1999‐2002.
B. Control strategies
Control strategies encompass:
Surveillance: monitoring the evolution and effects of interventions through sound and standardized surveillance systems which track antibacterial resistance as well as the consumption of antibacterial agents.
Prevention: prevention of communicable diseases and infection control to reduce the need for antibacterial agents.

6. Priority diseases and reasons for inclusion
51
Research and product development: new approaches for prevention and treatment of infection and continued support for research into new medicines, including better models for predicting resistance to novel agents and making collections of genomic‐based targets available to interested parties to screen against their own targets.
International cooperation: an effective strategy requires close cooperation between regions and countries since these resistant organisms are ʺinternational travellers.ʺ
Although much has been done by the EU in the Fifth and Sixth Framework Programmes (FPs) to address the problem of antibacterial resistance, the present level of investment (including human and financial resources) is far too low. Within DG SANCO (the public health commission of the EU) action has been taken to implement the Community strategy against Antimicrobial Resistance. This encompasses actions in regard to surveillance, prevention, research, product development and international cooperation (see Appendix 6.1.8). Because of the currently limited size of the market for antibiotics in developed countries (due to the low incidence of infectious diseases) and the high investment costs and considerable time needed for R&D for new antibiotics, many large pharmaceutical companies have stopped investing in research in this area — as evidenced by the dramatic drop in antibacterial new molecular entities approved for use in the USA.
Figure 6.1.3: Antibacterial new molecular entities approved for use in the USA 1983‐2002
0
5
10
15
20
1983-1987 1988-1992 1993-1997 1998-2002
No.
of F
DA
app
rove
d an
tibac
teria
l NM
E
Source U.S. Food and Drug Administration, Center for Drug Evaluation and Research. New molecular entities (NMEs) reports. Available at: http://www.fda.gov/cder/rdmt/
(accessed 28 July 2004)

Priority Medicines for Europe and the World
52
This trend must be reversed by providing significant incentives to companies to invest in this area. The need for antibiotics will remain high and is anticipated to increase with an aging population, increased global infection rates, and increasing numbers of immunocompromised patients. When new drugs are developed it is of equal importance that systems are in place to secure their appropriate use in order to reduce emergence of resistance. There are several possible ways of dealing with this. There may be a need for a special regulatory regime for antibiotics in situations where a great public health need exists, e.g., to treat infections due to multidrug‐resistant microorganisms in hospitals where little or no alternative treatment is available. For example, antibiotics could be treated like cancer or AIDS medicines. This would mean that, on the basis of limited Phase II efficacy trials, products could be conditionally released under the new European Medicines Agency (EMEA) procedures. The companies that develop these products would be required to undertake detailed monitoring of efficacy, antibacterial impact and safety. Such data could be used for eventual licensing of the product for broader use. For instance, as the mortality rate for these patients with multidrug‐resistance may approach 30% or 40% and the cost of their care in intensive care units is measured in thousands of Euros per day, reimbursement authorities would need to be prepared to pay for the very substantial benefits these products would bring. Such a restricted release would prevent the widespread ʺblockbusterʺ launch that would promote resistance, while still allowing the companies to recoup the cost of their research over a longer time period. When new drugs are developed, the possibility that they could be released as a fixed‐dose combination (FDC) product to prevent the emergence of resistance should be explored (see Chapter 7.1). Promoting research into the development of rapid diagnostic tools may prevent the misuse of antibiotics by identifying at the outset in the doctorʹs office which antibiotic is needed for treatment. Thirdly, vaccines for specific infections may be a useful way to prevent the need for antibiotics. Such targeted research should be further supported by the EU Framework Programmes. The establishment of the European Centre for Disease Prevention and Control (CDC) offers a major opportunity for the establishment of an EU‐wide surveillance system that would link: antibacterial surveillance, monitoring of drug consumption, and prescribing practices with the evaluation of interventions to prevent the emergence of resistance. The proposal for a Technology Platform for the European pharmaceutical industry (see Appendix 8.5.1) is another opportunity to mobilize European industry to address this immense challenge. We live in a period when antibiotics still function. However, many first‐line medicines are rapidly losing their effectiveness. Immediate action is needed to: stimulate innovation; to reduce the misuse of antibiotics and their excessive use for veterinary and agricultural purposes; to conduct surveillance of resistance patterns in hospitals

6. Priority diseases and reasons for inclusion
53
and the community; to monitor prescription and consumption patterns at local, national, regional and global levels; and to intervene to improve prescribing and dispensing practices. If no such action is forthcoming, we will have lived through a century (1950‐2050) of antibiotics but our children and grandchildren will face a world without such therapy. This tragedy can be avoided but only with substantial coordinated investment along the lines proposed in the EU and WHO strategy documents.
6.2 Pandemic influenza
A. Background
Influenza is a viral disease which occurs annually in an epidemic form and every few decades in pandemic form. Although the first pandemics were recorded more than 1000 years ago, the most recent lethal pandemics occurred in 1918‐1919, in 1957‐1958 and in 1968. Recent outbreaks of highly pathogenic avian influenza in Asia have raised concern about the possibility that the next pandemic could be caused by a new virus strain originating from poultry but adapted to infect humans. In ʺnormalʺ epidemic years up to one million people die — most of them elderly. In the 1918‐1919, pandemic, 40‐50 million people died worldwide, mainly in the 20‐39 age group.7 To address current and future risks related to influenza, in May 2002 WHO convened a consultation of influenza experts, virologists, epidemiologists and public health officials.8 The consensus that was achieved led to the publication of the first Global Agenda on Influenza Surveillance and Control (Appendix 6.2.2). The Global Agenda was politically endorsed by the adoption of a World Health Assembly Resolution, which called on Member States ”to support research and development on improved influenza vaccines, particularly concerning their suitability for use in developing countries, in order to develop and produce an influenza vaccine formulation capable of conferring long‐lasting and broad protection against all influenza virus strains.” WHO was asked ”to search jointly with other international and national partners, including the private sector, for solutions to reduce the present global shortage of, and inequitable access to, influenza vaccines and antiviral drugs, both for epidemic and global pandemic situations.” The event that marked the beginning of European planning for the next influenza pandemic was the EU‐sponsored conference “Pandemic Preparedness in the Community” that was held in Brussels on 27 November 2001.9 In its preliminary conclusions, the conference noted: “The next pandemic is imminent. EU Member States are not prepared. Vaccine availability is not secured. Antiviral stocks do not exist and will not be available under the current market forces. In the event of a pandemic millions of people could die, economies will be affected and services (medical, civil) could collapse. Members of the public will not excuse authorities, who will be held responsible for not having put in place up‐to‐date preparedness.”

Priority Medicines for Europe and the World
54
In March 2004, the European Commission published a working document on “Community Influenza Pandemic Preparedness and Response Planning.” The document noted that ʺcurrent vaccine production capacity is not deemed to be sufficient to meet the demands of the Community in the event of a pandemic. Manufacturers’ reserve capacity is not likely to be enough to support a sudden increase in demand. Availability of vaccines or antivirals to populations most at risk may, in critical situations, be further limited by measures imposed by Member State authorities to provide maximum protection to their own population. Measures should, therefore, be considered with a view to ensuring equity of access.ʺ The Commission emphasized that international collaborative research performed during the inter‐pandemic period would be vital for preparing an effective pandemic response. These meetings and reports identified the key strategies for addressing this challenge and both WHO and the EU are now moving into the implementation phase. But the challenges are great from a biological, pharmaceutical, logistic, political and health system standpoint.
B. The disease
Influenza viruses are RNA viruses which mutate frequently, leading to new viruses which cause yearly epidemics. Influenza affects people of all ages in all parts of the world, and each year 5%‐20% of people worldwide will develop symptomatic illness.10 Epidemics of varying degrees of severity occur each winter. In industrialized countries, most deaths associated with influenza occur among the elderly. Each epidemic involves major economic costs. In recent years, in Madagascar and the Democratic Republic of the Congo, outbreaks have been extensive and case fatality rates have been 3%‐4% — rates similar to those experienced in developed countries during the 1918‐1919 pandemic. Avian influenza viruses do not normally infect species other than birds and pigs. However, in 1997, avian influenza appeared in Hong Kong and infection spread to 18 people, six of whom died. Human cases of avian influenza reappeared in 1999 and again in 2003 and early 2004. In August and September 2004, additional fatal cases of human avian influenza were reported, three of these in Viet Nam. The persistence of highly pathogenic avian influenza viruses in poultry flocks in Asian countries provides continuing opportunities for the direct infection of humans. At this stage, the avian influenza virus does not appear to have the potential for human‐to‐human transmission. However, as more humans become infected, the likelihood increases that humans might be concurrently infected with both human and avian influenza strains, leading to a new virus strain involving human‐to‐human spread of the disease. WHO and infectious disease experts throughout the world are concerned that these events could lead to a new human influenza pandemic.

6. Priority diseases and reasons for inclusion
55
C. Control strategies
There are three possible approaches to control or prevention of pandemic influenza: vaccination, antivirals and non‐medical interventions. Influenza vaccines are the mainstay of influenza prevention and control. They are immunogenic, safe, provide clinical protection and have been shown to be cost‐effective in European countries. There are four antivirals that have proven efficacy in treatment and prophylaxis of influenza A infections but they are very expensive and have limited effect. Non‐medical interventions, ranging from personal hygiene and wearing masks to use of quarantine and screening travellers, could potentially delay the transmission of the pandemic virus. However, if the pandemic strain is as infective as anticipated, these measures will not be able to prevent global spread.11
Figure 6.2.1: Rates of vaccine distribution per 1000 total population by country (EU Countries solid bars)
CanadaUnited StatesRep. of Korea
AustraliaSpain
BelgiumThe NetherlandsUnited Kingdom
GermanyNew Zealand
ItalyIcelandFranceJapan
SwitzerlandGreeceFinlandIreland
Russian Fed.HungaryPortugalSweden
DenmarkAustria
LuxembourgSlovak Republic
SloveniaNorway
ArgentinaBrazil
PolandCzech Republic
RomaniaLithuaniaBulgaria
South AfricaMexicoLatvia
TurkeyEgypt
Source: MIV Study Group
At present, nearly 300 million doses of vaccine are produced each year, mainly by European manufacturers. Despite strong recommendations as to who should receive the vaccine, uptake is often less than 20% of what would be expected (Figure 6.2.1). Even fewer ʺtreatmentsʺ of antivirals are produced. In Europe, the cost per person of vaccine varies from €15‐30, which has been shown to be cost‐effective. The antiviral

Priority Medicines for Europe and the World
56
treatments cost €30‐40 for therapy, while a four‐week course of preventive therapy costs €130‐215.12 At present, because of the low uptake of vaccine for annual use, there is limited capacity to expand production. While the present product is trivalent and the pandemic vaccine would be monovalent, there is still not enough capacity with existing facilities to meet the needs of Europe, let alone the world. It takes several years to build a factory to produce such vaccines, and vaccine development and production during a pandemic is a slow solution. In response to these limitations, some new vaccines have been developed, including an intranasal live‐attenuated influenza vaccine that can induce more effective mucosal immunity and is easy to administer. However, implementation of these vaccines has been limited. In addition, reverse genetics have been used to synthesize safe prototype vaccine strains for the annual vaccine in a quick way, even if the original strain cannot grow in eggs. However, there are concerns about access to this technique because of intellectual property issues. The EMEA has issued guidance for the rapid authorization of new vaccines in the event of a pandemic. The suggestion that the use of adjuvants would allow a lower dose of antigen in current inactivated vaccines is very attractive for the short term. However, the gap between the potential benefits of a vaccine and current uptake would be best bridged with long‐lasting, broad spectrum vaccines. Alternative vaccine delivery mechanisms, particularly the use of aerosol sprays, offer hope for a more rapid delivery mechanism. Meanwhile, further research is needed on antivirals and on the impact of other pharmaceuticals (for example, statins) on influenza in patients also taking such medicines. Pandemic influenza in the twenty‐first century could be as devastating as the 1918‐1919 epidemic was to a world recovering from the First World War. Much could be done to prepare for this potential disaster. The question is whether policy‐makers, researchers and companies will take the necessary actions before the occurrence of such an event.

6. Priority diseases and reasons for inclusion
57
2002
2020
-
10,000,000
20,000,000
30,000,000
40,000,000
Cardiovascular diseases
6.3 Cardiovascular disease secondary prevention
Cardiovascular disease (CVD) is very common and will become even more common and a serious public health problem over the next 20 years, particularly in developing countries. In Europe, there are an estimated 80 million people who have a greater than one in four, 10‐year risk of a vascular event. Already, CVD is the leading cause of death in Europe and the world (see Figure 6.3.1).
Figure 6.3.1: Deaths worldwide estimated for 2002 and projected for 2020 attributable to cardiovascular disease
The determinants of CVD that have driven this epidemic of ill health in developed and developing countries are well established. Smoking, high blood pressure, high cholesterol, diabetes and obesity are among the most important risk factors for heart attack and stroke. These risks are cumulative. Thus a smoker with high blood pressure is at greater risk than a smoker with normal blood pressure. For patients who have already had a heart attack or stroke, reducing these risk factors (irrespective of the level) will dramatically reduce the risk of a repeat heart attack or stroke. This finding means that even for surviving patients with normal blood pressure or normal cholesterol they would benefit from medicines that reduce cholesterol or blood pressure. There is evidence that lifestyle interventions, such as stopping cigarette smoking, dietary change and increasing physical activity levels in patients with established cardiovascular disease, are likely to reduce risks of recurrent vascular events. It is likely that the beneficial effects of smoking cessation, increased physical activity and dietary change will be largely independent and together they are likely to be substantial. Although the benefits of specific lifestyle changes are clear and their costs generally limited, the most efficient and cost‐effective ways of bringing about these changes in lifestyle have not been extensively investigated. With regard to smoking cessation, advice from health professionals has been shown to be effective. Although nicotine replacement therapy and antidepressant drugs have short‐term benefits in smoking cessation their long‐term effectiveness is uncertain.

Priority Medicines for Europe and the World
58
It has been clearly demonstrated that antiplatelet therapy (with a medicine like aspirin), 13 blood pressure lowering medicines (ACE inhibitors or a diuretic)14,15 and cholesterol lowering drugs (statins),16 used separately or in combination, reduce the risk of recurrent vascular events. WHO has published two recent reviews which strongly support the use of these medicines for secondary prevention (see Appendices 6.3). However, many patients with existing CVD receive substantially incomplete preventive therapy. The problem is that, for a variety of reasons, these patients are not prescribed the four different medicines they need to take. In 1999‐2000, a major survey involving about 50 leading European hospitals identified major shortfalls in the secondary preventive care provided to patients who had been admitted with ischaemic heart disease.17 Ideally, each of the treatments should have been used in all patients but well under half of all patients were receiving all the recommended treatments. Another feature of the data was that there was only very limited improvement in treatment in comparison with a comparable survey completed a few years earlier. This information reinforces the need for novel strategies that will give physicians new ways of bridging the large gaps between defined optimal care and actual clinical practice. The simple solution to this deficiency is to develop and test a fixed‐dose combination (FDC) product of these proven effective medicines. The research agenda proposed in this section is different to that of the other sections because this approach offers the greatest potential short‐ to‐medium term impact of all of the possible research activities in this Report. The evidence for the use of FDCs to improve adherence, reduce costs, improve access and equity, and reduce medication errors for TB is convincing. However, to improve the treatment of CVD, there is a need for the testing of new formulations of two different, four‐drug FDCs for the secondary prevention of heart attack and stroke (see text box on the previous page). Once such products are formulated there will be a need for clinical trials to assess the effect of these products on blood pressure, cholesterol and platelet functioning, adherence to guidelines, and the overall effect on mortality
Suggested formulation for secondary prevention of heart attack • Low‐dose antiplatelet therapy (for example
aspirin 75mg) • Full dose of a standard statin (for example
simvastatin 40mg) • Full dose of an angiotensin converting enzyme
inhibitor (for example lisinopril 10mg), and • Half dose of a beta‐blocker (for example atenolol
25mg) Suggested formulation for secondary prevention of stroke • Low‐dose antiplatelet therapy (for example
aspirin 75mg) • Full dose of a standard statin (for example
simvastatin 40mg) • Full dose of an angiotensin converting enzyme
inhibitor (for example lisinopril 10mg), and • Half dose of a diuretic (for example
hydrochlorothiazide 12.5mg)

6. Priority diseases and reasons for inclusion
59
and morbidity. These trials should be undertaken in both developed and developing countries. While the EU Framework Programmes have not supported many clinical trials, trials for these proposed FDCs should be an exception. Because the component medicines are now off‐patent, there is no incentive for innovative pharmaceutical companies to undertake such trials, and the generic companies do not generally have the capacity to do so. It is estimated that these four‐drug FDCs could reduce the risk of a second heart attack or stroke by about two‐thirds.18 If this combination proved effective, and cheap generic versions of the individual medicines were used, this would be a very cost‐effective intervention. On the basis of the background paper, it is strongly recommended that a research agenda should be established to produce and test FDC products for secondary prevention of heart attack and stroke to improve adherence and prevent mortality and morbidity.

Priority Medicines for Europe and the World
60
6.4 Diabetes
The impact of diabetes and of diabetes‐related illnesses place an enormous burden on the health care systems of most countries throughout the world. It has been estimated that by the year 2025, 300 million people will have diabetes — a remarkable 5.4% of the world’s projected population. There are primarily two types of diabetes. Type 1 diabetes is an auto‐immune disease in which the pancreas can no longer produce insulin and thus the body cannot control blood sugar. The annual rate of new cases of Type 1 diabetes varies widely around the globe (see Figure 6.4.1).
Figure 6.4.1
Type 1 Diabetes (Incidence per 100000)
(year 2000)
0 10 20 30 40 50
ChinaTaiwan, China
IndonesiaJapan
ThailandJordan
BangladeshIndia
Sri LankaPoland
EgyptLithuaniaSlovenia
FranceSlovakiaGreece
Czech RepublicHungary
ItalyAustriaCyprusEstoniaBelgium
LuxembourgSpain
PortugalAustraliaGermany
NetherlandsMalta
New ZealandIreland,
DenmarkUSA
United KingdomSwedenFinland
Source: International Diabetes Federation, Diabetes Atlas, 2nd edition. (The absence of data from African and Asian countries reflects the dearth of such survey data and not necessarily the absence of diabetes in these regions). ʺAdultʺ Type 2 diabetes is a metabolic derangement in which the body gradually becomes insensitive to the action of insulin so that blood sugar control is also compromised. Overall, the prevalence of Type 2 diabetes dominates the total diabetes burden, although there is an alarming trend for juveniles to develop Type 2 diabetes. Chapter 5 mentioned the global demographic changes taking place with regard to aging and the differences in life span between genders. Data on the diabetes

6. Priority diseases and reasons for inclusion
61
burden (both Type 1 and Type 2) for Europe and the world, see Figure 6.4.2, reveal that the diabetes burden is higher for females than males for the world, for the EU15 and for the EU10.i
Figure 6.4.2: Diabetes mellitus (DALYs per 1000 by age)
EU15-MEU15-F
EU-10-MEU-10-F
W-M
W-F
0
2
4
6
8
10
12
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
Age group
DA
LYs
per 1
000
Source: WHO Global Burden of Disease Database
In the EU10, the total per capita diabetes burden shifts from men to women after the age of 60, which is about a decade earlier than in the EU15. These overall trends are expected to increase as a result of the aging of the population combined with longer female life span. The newer EU10 countries have a lower overall diabetes burden per capita. The projected increase in the prevalence of diabetes will be four times higher in the developing world than in the developed world.19 In 2025, the countries with the largest number of diabetics will be India, the Peopleʹs Republic of China and the USA. In view of the burden and associated costs of diabetes, the ongoing epidemic represents a major public health problem requiring effective control. There is a large gap between diabetes prevalence and treatment rates. It has been estimated that 30%‐50% of diabetes cases remain undiagnosed. People with Type 1 diabetes require lifelong insulin replacement and face the additional complications of
i We note that graphs of DALYs by age are commonly misinterpreted as the DALY burden at each age. DALYs actually measure incident DALYs due to new cases and new deaths at each age. For a long‐term condition like diabetes, disability‐adjusted life shown at age x may actually be lived at older ages. For short‐term conditions or conditions where death dominates, like cancer, this misinterpretation is not a problem.

Priority Medicines for Europe and the World
62
diabetes‐related diseases. At present, there is no real ability to provide effective, long‐term, tight blood sugar control through insulin replacement therapy. Moreover, insulin requires refrigeration and this creates an access problem in many developing countries. Type 2 diabetes is increasing due to urbanization and industrialization, which leads to a reduction in physical activity and consumption of a high fat diet. These lifestyle changes result in obesity, the most important risk factor for diabetes. Management of Type 2 diabetes has always centered on control of metabolism i.e., achieving a negative calorie balance and optimal intake of carbohydrates and lipids. Evidence suggests that controlling obesity and physical inactivity can prevent, or at least delay, the development of the disease in many genetically susceptible individuals. However, success in controlling these risk factors on a large scale has been limited. There are many oral agents that improve glucose control in diabetes by either improving insulin secretion or improving insulin action if diet and exercise are not working. The pharmaceutical industry considers development of effective diabetes medications as a major goal. However, there is still a need for these oral agents to act in a more efficient manner within the body (i.e., faster absorption by the body, action to control blood glucose taking place over a longer time period, fewer side‐effects, paediatric formulations). For patients requiring insulin, current methods of insulin administration cannot reproduce the body’s ability to precisely control blood glucose and other metabolic variables. Diabetes is an example of a disease with an unmet global medical need and conforms to the ʺcommonality of interestʺ principle of the Priority Medicines Project. The increases in diabetes projected over the next several decades require a global strategy for prevention, treatment and medicine development. The EU could contribute to this by creating an infrastructure to facilitate diabetes clinical trials, in particular comparative clinical “head‐to‐head” trials to compare efficacy, side‐effects and cost‐effectiveness using full pharmaco‐economic analyses. Heat‐stable insulin, available for use in developing countries lacking a regular refrigeration system would be a major public health advance.
6.5 Cancer
Cancer (a term comprising over 100 types of malignancy) is one of the major burdens of chronic disease in Europe and the world. In 2000, malignant tumours were responsible for 12% of the nearly 56 million deaths worldwide from all causes. In many countries, more than one‐quarter of all deaths are attributable to cancer. In 2000, 5.3 million men and 4.7 million women developed a malignant tumour and there were 6.2 million cancer deaths. It is predicted that cancer rates could increase by 50% to 15 million new cases in the year 2020.20 Although Europe comprises only about one‐eighth of the world’s population, it accounts for over one‐quarter of the global burden of cancer incidence. Standardized mortality rates for all cancers among all age groups in Europe reveal steady or

6. Priority diseases and reasons for inclusion
63
decreasing rates in the EU15 countries and increasing mortality rates in some, but not all, EU10 countries.21 Barring major therapeutic breakthroughs in the short term, cancers are still a major public health concern, in large part because of the preventable nature of some of the most common cancers.22 Of these, tobacco consumption remains the most important avoidable cancer risk. In the twentieth century, approximately 100 million people worldwide died from tobacco‐associated diseases (cancer, chronic obstructive lung disease, heart disease and stroke). The pharmaceutical industry has invested heavily in finding new pharmaceutical treatment options for cancer, and analysis of cancer medicines in clinical development suggests that its present level of effort is appropriate, based on the relative burden of different cancer types. Yet, despite this major input by the private sector, many cancers are still resistant to treatment and the struggle to find effective medicines is ongoing. Europe does not at present match the private or public funding levels of the USA with regard to cancer therapeutic research and development. It is recommended that the EU should expand its capacity (infrastructure and human resources) and strengthen coordination to conduct comparative Phase II/III clinical trials and continue to invest in basic research into cancer biology. The EU should continue to pursue excellence in cancer research within the existing financing structures. There is a need for an increase in the level of basic research into cancer biology. Global funding for cancer research appears overwhelmingly to be concentrated in the USA. For Europe, improving the efficiency of the cancer R&D process is important.
6.6 Acute stroke
Acute stroke is caused by either a sudden reduction in the blood supply to the brain or by a haemorrhage. It is the third leading cause of disability and death (as DALYs) in Europe after depression and ischaemic heart disease (IHD). Worldwide, stroke is the fifth leading cause of disability and death. Ten per cent of the 55 million deaths that occur every year worldwide are due to stroke.23 Despite improvements in stroke care, treatment of the long‐term effects remains one of the major problems. Fifty to seventy per cent of those who survive an ischaemic stroke will recover functional independence three months after onset, but 20% will require institutional care. The United Kingdom spends 6% of its national health budget on stroke care, twice as much as is spent on ischaemic heart disease.

Priority Medicines for Europe and the World
64
Table 6.6.1: Leading cause of deaths worldwide and in Europe (2002, percentage of total deaths)
Global EU25
EU15
EU10
IHD (12.57%) IHD (18.11%) IHD (16.79%) IHD (24.45%) Stroke (9.63%) Stroke (10.90%) Other CVD (10.78%) Stroke (13.19%) LRI (6.60%) Other CVD (10.78%) Stroke (10.42%) Other CVD (10.77%) HIV/AIDS (4.95%) Trachea, bronchus, lung
cancers (5.38%) Trachea, bronchus, lung cancers (5.31%)
Trachea, bronchus, lung cancers (5.73%)
COPD (4.81%) LRI (4.01%) LRI (4.46%) Other cancer (3.96%)
Source: WHO, Evidence, Information and Policy, 2003 Note: LRI = lower respiratory tract infections, COPD = chronic obstructive pulmonary disease, CVD = cardiovcascular disease, IHD = ischaemic heart disease The current treatment of acute stroke is unsatisfactory. Aspirin and intravenous recombinant t‐PA have been shown to be effective and their use approved by regulatory agencies. However, the effectiveness of these agents is limited and they are associated with an increased risk of intracranial haemorrhage. Over the past 30 years, surprisingly low levels of resources have been devoted to R&D of medicines for acute stroke. There is an urgent need to develop new medicines for the treatment of stroke, particularly in the field of neuroprotection. In the late 1980s and 1990s a number of companies invested heavily in stroke research but the resultant failure of costly, large‐scale clinical trials of neuroprotectants has made companies wary of research in this area. Major improvements are also needed in the chain of care; in the ability of relatives to identify an attack (public education); the prompt referral to an accident and emergency facility (mobile units); accurate diagnosis (imaging and stroke physicians); access to efficacious early therapeutic options such as thrombolytic treatment (protocols and specialized units); and referral to dedicated rehabilitation services (‘intermediate care’ stroke rehabilitation units). 24 , 25 It is also important to expand stroke prevention programmes focusing on education and vigorous risk factor management.
6.7 HIV/AIDS
By the end of 2003, over 40 million people worldwide were living with HIV/AIDS. Some regions are more affected by HIV/AIDS than others. The severity of the epidemic in sub‐Saharan Africa is well known. Elsewhere, in the Russian Federation, the profound social and economic upheaval which took place in the former Soviet Union in the 1990s has resulted in an upsurge in HIV infections. By the end of 2001, an estimated 1 million people were HIV‐positive, compared with only 30 000 at the start of 1995. Eastern Europe and Central Asia are among the regions with the fastest growing HIV rates.26 However, in Central and Western Europe, epidemics that began in the late 1980s have remained at low levels and do not appear to be expanding.

6. Priority diseases and reasons for inclusion
65
Although the European burden of HIV/AIDS is not matched by the HIV/AIDS epidemic in the rest of the world, the extent to which epidemics that began 20 years ago are still continuing in Europe (i.e. Eastern Europe), the Russian Federation and Central Asia shows a clear commonality of interest for policy‐makers.27 The commercial market for antiviral therapeutics in developed countries will ensure that for the immediate future there will be no shortage of private research funding into new HIV/AIDS therapeutics. The pipeline of potential antiviral products is large and dynamic, since the absolute numbers of products in the R&D pipeline can change from year to year as programmes are introduced and removed for various reasons.28 New targets of mechanism of action, such as fusion inhibitors and integrase inhibitors, remain active research areas. Despite this R&D activity, pharmaceutical gaps remain. No treatment is curative. Efficacy is not optimal for the present repertoire of antiviral medicines. Because the HIV genome mutates very rapidly during the course of an infection, resistance to antivirals is common. Moreover, the long‐term, adverse events of present regimens can sometimes be fatal. Adherence to treatment is difficult and the use of FDCs proposed here is a likely solution to this on a global level (see Chapter 7.1), although the fact remains that many patients are without any treatment options. Special needs remain for formulations and regimens for children and for pregnant women. FDCs of first‐line antiretrovirals are available and inexpensive for developing countries, even though access to such treatments has been slow. There is a need for second‐line FDC products. Meanwhile, on the most optimistic estimates, it is unlikely that an effective HIV vaccine will be available for at least five to ten years.29 The private sector has already invested heavily in addressing HIV/AIDS, with the USA investing the most (both financial and human resources). However, recent efforts in the EU’s Sixth Framework Programme are encouraging. From a public health viewpoint, the EU can fill treatment ʺgapsʺ by putting effort into targeting affected populations, especially women, injecting drug users (IDUs), children, adolescents and older adults. The EU should also support comparative studies of different AIDS treatment regimens. In addition, mechanisms should be sought to provide support for AIDS vaccine development. New medicines are still needed to deal with highly resistant virus or to prevent cross‐resistance to existing classes of treatment. The EU should promote innovative mechanisms to fund an integrated programme specifically directed to study FDC medicines with a view to developing and assessing acceptable formulations, and to evaluate their impact on AIDS treatment outcomes.

Priority Medicines for Europe and the World
66
6.8 Tuberculosis
Tuberculosis (TB) is a major and growing threat to public health for Europe and the world, with new epidemiological challenges. The EU25 now has a TB burden of more than 50 000 new cases per year (see Figure 6.8.1). Of these, about 10% are infected with bacteria that are already resistant to one or more of the existing medicines.30 Globally, TB control is now threatened by an upsurge in patients who are co‐infected with HIV/TB, who are straining current TB treatment and control approaches to the limit. Controlling TB with the existing tools is a cumbersome, expensive and sometimes unsuccessful task. There are no cheap, rapid, reliable diagnostics for screening for drug‐resistant TB. Moreover, the current first‐line TB diagnostic test picks up only 50% of patients with active TB. To make matters worse, medicine therapies are resource‐intensive and expensive, particularly in European settings, requiring six to eight months of therapy. Therapies for resistant TB are even longer, up to two years, and have high failure rates. All the current TB medicines were developed between 1940 and 1970, and there has since been a marked downturn in industry interest. There is no reliable vaccine to prevent TB in adults.31 Although new tools and approaches are being developed in all areas – including basic research, medicines, diagnostics and vaccines – progress is being delayed by lack of targeted funding and support. The EU now provides less than 5% of global funding for development of new TB tools. The U.S. Federal Government provides a high throughput and an in vitro screening facility to stimulate research on TB. No such service exists in Europe for any product of public health significance.

6. Priority diseases and reasons for inclusion
67
Figure 6.8.1: TB incidence in the expanded European Union
Austria Belgium Czech Republic
Denmark Estonia
Finland France
Germany Greece
Hungary Ireland
Italy Latvia
Lithuania Luxembourg
Malta Netherlands
Norway Poland
Portugal Slovakia Slovenia
Spain Sweden
United Kingdom
0 10 20 30 40 50 60 70 80 90TB Incidence per 100000
Source: European HFA Database 2003
The landscape of R&D for these new tools has also changed dramatically, with their development now being driven by public‐private partnerships (PPPs) and funded by philanthropists. Only three major pharmaceutical companies remain active in TB medicines discovery. Current EU funding for R&D of new TB tools does not always reflect these new epidemiological and pharmaceutical realities. EU funding is insufficient (around €7 million per year under the Fifth Framework Programme) and is not well targeted at the PPPs, smaller industry and academic groups, which are now the most active in TB research and development.32 The EU should support research on diagnostics, vaccines and pharmaceutical translational research being undertaken by PPPs and by small and medium‐sized enterprises to address this serious public health problem. Every encouragement should be given to the few large pharmaceutical companies still active in this field so they can contribute new pharmaceutical products for the planned clinical trials of the EDCTP.

Priority Medicines for Europe and the World
68
6.9 Neglected diseases
Neglected diseases, such as trypanosomiasis (sleeping sickness), Buruli ulcer and Chagas disease, cause enormous suffering and death, mostly among the poor in the poorest regions of the world. Neglected diseases are common, are fatal or disabling, and they have no suitable treatments. They affect populations that are large but have little or no purchasing power.33 Over 200 million people are estimated to be at risk for visceral leishmaniasis, over 100 million at risk for Chagas disease, and over 60 million people are at risk of developing trypanosomiasis in Africa. Some of these diseases, such as trypanosomiasis, are returning to levels not seen for 75 years (See Figure 6.9.1). Figure 6.9.1: Trypanosomiasis incidence in Central Africa
Sour
ce: W
HO
200
1So
urce
: WH
O 2
001
Source: WHO 2001
A great deal of basic research has been undertaken on the biology of these diseases. A few new medicines have been developed, but most of the medicines being used are “old” and often dangerous. For example, one of the medicines used for the treatment of trypanosomiasis is toxic and kills 5% of patients.34 Some diseases such as Buruli ulcer have no pharmaceutical treatment and depend on extensive surgery (see photo).
Disfiguring lesion caused by Buruli ulcer
Pho
to: A
rmed
For
ces
Inst
itute
of P
atho
logy
Pho
to: A
rmed
For
ces
Inst
itute
of P
atho
logy

6. Priority diseases and reasons for inclusion
69
There is a major need for appropriate treatments, vaccines and diagnostics for such diseases, a need that is not being addressed by the pharmaceutical industry because of the likely low return on investment.35 As a result, scientific advances into the nature of the diseases are not being translated into medical advances for patients. The R&D pipeline remains virtually empty. EU countries have for many decades demonstrated social solidarity for their citizens — ensuring universal access to medical services and medicines. Similarly, global solidarity demands that the EU support research on these neglected diseases. In 2004, the Joint Parliamentary Assembly of the EU‐Africa, Caribbean, Pacific (ACP) countries called on the European Commission to demonstrate this solidarity and ʺto include the most neglected diseases, such as sleeping sickness, Chagas disease and leishmaniasis, among its priorities and to ensure that effective, appropriate, easy‐to‐use medicines are developed and placed on the market in the developing countries at an affordable price”.36 A concerted and sustained response to the problem of neglected diseases is more than just a moral imperative, it also contributes to growing economic and social stability in traditionally neglected or exploited regions of the world, and will ultimately benefit Europe through supportive development in ACP‐countries. To this end, it is recommended that the EU should: • Mobilize and sustain adequate funding for neglected diseases.
• Encourage translational research to transform the results of basic research into useful medical applications, adapted to the needs of patients affected by neglected diseases.
• Expand the activities of the EDCTP to include other neglected diseases as well as other phases of clinical development (Phase I, Phase IV).
• Create a Centre for Preclinical Research to bridge the continuing gap between the development of promising medicine leads and their move into clinical trials. This Centre should complement the activities of the EDCTP.
• Develop mechanisms to provide direct support for public‐private partnerships to develop medicines and vaccines for diseases where there is no commercial market.

Priority Medicines for Europe and the World
70
6.10 Malaria
A. Background
Malaria accounts for over one million deaths and up to 500 million cases a year.37 Nearly 90% of cases and deaths occur in Africa. About 70% of these deaths occur in young children. Pregnant women are particularly vulnerable to malaria — placing both mother and child at risk. The economic consequences of malaria in Africa are enormous. Malaria accounts for an estimated US$12 billion (about €9.8 billion) per year in lost Gross Domestic Product (GDP) and a loss of 45 million years of productive life due to deaths and disability.38 The number of malaria cases imported into Europe is increasing and deaths occur due to a lack of recognition of the disease and sometimes because of poor medical management.
B. Control strategies
The control strategy for malaria involves controlling the mosquito vector and providing effective curative treatment to infected individuals. Vector control can include the use of insecticide‐impregnated bednets, indoor residual household spraying, and environmental and biological management. The success of these measures is heavily dependent on ecological factors such as rainfall and temperature. In many tropical environments it is extremely difficult to eradicate the vector. There is no vaccine to date and those currently in development are not expected to be available for some time. Moreover, they may not be highly effective. The EU provides support for malaria vaccine development, for which a long‐term commitment is necessary. Effective case management requires accurate diagnosis and correct treatment with effective medicines. Antimalarials such as chloroquine and sulfadoxine pyrimethamine have proven to be useful in the control of malaria but widespread resistance make these medicines useless in many areas. Newer treatments such as artemisinin‐based combination therapies are far more expensive, costing 10 to 20 times as much as the old medicines. New affordable, safe and effective medicines are urgently needed to roll back malaria. These new products should be aimed at treating young children and pregnant women. The pharmaceutical industry has largely disengaged from innovative drug R&D in tropical diseases due to the lack of market incentives. Despite its frequency and severity, malaria can be seen as a “neglected disease”(see Chapter 6.9). There have been major advances in basic science in areas such as genetics and molecular biology which allow a better understanding of the parasite and identification of possible medicine target sites.39 Yet despite the advances in basic scientific knowledge, only a few new medicines have been developed, because a funding gap exists between basic science and translational research geared toward discovery and development of new medicines.

6. Priority diseases and reasons for inclusion
71
The creation of PPPs such as the Medicines for Malaria Venture (MMV) provides a new approach to innovative medicines discovery and development (see Chapter 8.1). In a few years of operation, assisted by contributions of the private sector and with a total expenditure of about US$50 million (about €40 million), MMV has built the largest antimalarial medicines portfolio since World War II. Expenditures will increase significantly as many medicines reach clinical trial phases. Collaboration with the EDCTP will help support the cost of clinical studies and thus facilitate rapid progress. MMV estimates that at least US$30‐50 million will be required annually to maintain and expand its portfolio.40 Despite all efforts taken to reduce the attrition rate of newly discovered compounds, the lack of better tools to screen for safety, particularly with respect to reproductive and developmental toxicity, means that many promising compounds may be discarded at a late stage of development. Academic scientists, industry and regulators need to team up to translate basic research into applied sciences which will lead to the development of more cost‐efficient experimental models for medicines discovery and development. Creation and funding of new partnerships toward applied sciences for medicines R&D are needed for the development of new medicines that will meet public health needs (see Chapter 8.3). Recent basic science discoveries have created promising opportunities for medicines development but funding for translational and preclinical research must be provided to bring these medicines to patients. As in the case of other neglected diseases, the EU needs to find a mechanism to fund this translational and preclinical research.
6.11 Alzheimer disease
Alzheimer disease (AD) is a neuro‐degenerative disease of the brain that causes changes in brain function. AD usually affects people over the age of 65 years, with a progressive decline in memory, thinking, language and learning capacity.41 Age is the strongest predictor for the development and progression of AD and with the rapidly aging population of European society, AD clearly poses a major health problem. An estimated 5%‐10% of the population aged 65 years and over and 40% of the population more than 85 years of age are likely to be affected by AD. There are currently no specific tests that can positively confirm a diagnosis of AD. Definitive changes found in the brain of affected AD patients are microscopic and can be seen only when a sample of brain tissue is removed and examined, usually on autopsy. Figure 6.11.1 plots the burden of disease for AD for the different EU and world regions as a fraction of all DALYs (both acute and chronic conditions) for different age groups. AD increases to a remarkable almost 20% of the total disease burden (both acute and chronic) among 80 + women in the EU15.

Priority Medicines for Europe and the World
72
Figure 6.11.1: Alzheimer as percentage of all DALYs (by age group)
EU15-F
EU10-M
EU10-F
World-F
World-M
F0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
5-14 15-29 30-44 45-59 60-69 70-79 80+
EU15-M
Age group
Perc
enta
ge o
f all
DAL
Ys
Source: WHO Global Burden of Disease Database
AD is a good example of a condition with one or more pharmaceutical gaps, as the presently available interventions are not effective in long‐term restoration of cognition. Indeed, at present, there is no cure for AD, nor any pharmacologic therapy that can delay its onset or affect the pathophysiology of the illness. The current pharmacologic therapy for AD provides symptomatic relief for only a short period of time, and several interventions are not statistically better than placebo. While there is already considerable research in this area, continued efforts in this field are still required. This includes developing medicines that would slow progression, halt, or prevent AD from occurring.42 Additionally, challenges for clinical services include early diagnosis and intervening early with the most appropriate and effective medicine. Furthermore, validated therapeutic targets need to be identified, and better animal research models are needed which reflect the disease. There are several barriers to closing the obvious pharmaceutical gaps with regard to AD. For example, efforts are needed to identify new therapeutic targets and develop better diagnoses. A key research goal should be the development and evaluation of new instruments that are sensitive, reliable and valid for detecting changes in normal aging and early AD. In addition, there is a need for increased multidisciplinary collaboration, especially in the areas of basic scientific research for AD. Neurobiologists, clinicians and medical chemists need to work together. To this end, there is a need for funding and for guidelines to assist scientists in preclinical medicine development.
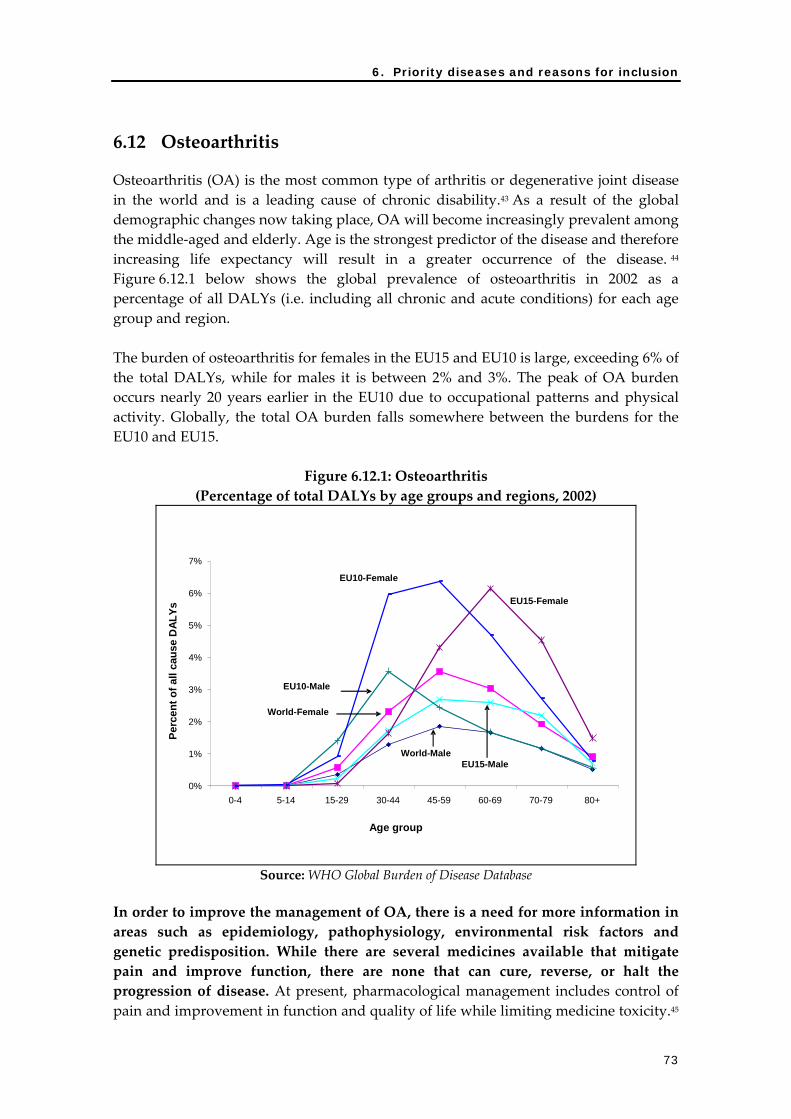
6. Priority diseases and reasons for inclusion
73
6.12 Osteoarthritis
Osteoarthritis (OA) is the most common type of arthritis or degenerative joint disease in the world and is a leading cause of chronic disability.43 As a result of the global demographic changes now taking place, OA will become increasingly prevalent among the middle‐aged and elderly. Age is the strongest predictor of the disease and therefore increasing life expectancy will result in a greater occurrence of the disease. 44 Figure 6.12.1 below shows the global prevalence of osteoarthritis in 2002 as a percentage of all DALYs (i.e. including all chronic and acute conditions) for each age group and region. The burden of osteoarthritis for females in the EU15 and EU10 is large, exceeding 6% of the total DALYs, while for males it is between 2% and 3%. The peak of OA burden occurs nearly 20 years earlier in the EU10 due to occupational patterns and physical activity. Globally, the total OA burden falls somewhere between the burdens for the EU10 and EU15.
Figure 6.12.1: Osteoarthritis (Percentage of total DALYs by age groups and regions, 2002)
Age group
Perc
ent o
f all
caus
e D
ALYs
0%
1%
2%
3%
4%
5%
6%
7%
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
EU10-Female
EU15-Female
EU10-Male
World-Female
World-MaleEU15-Male
Source: WHO Global Burden of Disease Database
In order to improve the management of OA, there is a need for more information in areas such as epidemiology, pathophysiology, environmental risk factors and genetic predisposition. While there are several medicines available that mitigate pain and improve function, there are none that can cure, reverse, or halt the progression of disease. At present, pharmacological management includes control of pain and improvement in function and quality of life while limiting medicine toxicity.45

Priority Medicines for Europe and the World
74
Osteoarthritis is often considered a ʺsilentʺ disease because it is only when the disease is advanced that the symptoms of pain are noticeable. Research into new diagnostics, biomarkers and imaging technology will be important and useful for the management of OA. Biomarkers are an essential area of research in OA and arthritis as a whole, since they will help the medical community to determine who is likely to get arthritis, the severity and progression of disease, and the response to medicines. There are a number of medicines under development for symptomatic and disease modification, and several studies are also evaluating alternative therapies. There are also several products on the market whose clinical effectiveness and long‐term safety still need to be determined. A US‐based public‐private partnership called the Osteoarthritis Initiative (OAI) is a useful model for EU efforts. The aim of this partnership, involving the National Institutes of Health (NIH) and four major pharmaceutical companies, is to discover biological markers related to the progression of OA. The OAI will collect data over the next five to seven years on individuals at high risk for the development of OA. This data will be used for the development of potential new OA treatments. A database on OA will be maintained which will include evaluation data, radiological images and a biospecimen repository. All the data will be public. It is recommended that the EU should initiate a similar entity or partner with the OAI directly. A broader approach could be considered in which data would also be gathered on the detailed epidemiology, natural history and outcomes of present combined therapies.
6.13 Chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD) is a complex disease characterized by progressive and partly irreversible airway obstruction and chronic lung inflammation. In 1997, COPD was ranked as the sixth leading cause of death and the twelfth leading cause of morbidity worldwide.46 In 2000, WHO estimated that COPD was the fourth leading cause of death worldwide, with 2.74 million deaths in 2000. By the year 2020, COPD is expected to be the third leading cause of death and the fifth leading cause of disability. This substantial increase in the global burden of COPD projected over the next 20 years reflects, in large part, the increasing use of tobacco worldwide and the changing age structure of populations in developing countries.47 COPD is the only major chronic disease with an increasing mortality rate – a disparity all the more striking amid the dramatic decline in deaths from coronary artery disease, stroke and other cardiovascular disorders.48

6. Priority diseases and reasons for inclusion
75
Figure 6.13.1 shows the per capita COPD DALY burden for age groups in various regions. The per capita burden in males is higher than in females for all regions. The per capita burden in the EU15 is at least twice that in the EU10.
Figure 6.13.1: COPD (DALYs per 1000 persons in age group)
0
5
10
15
20
25
30
35
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
World-M
World-F
EU15-M
EU10-M
EU15-F
EU10-F
Age group
DAL
Yspe
r 100
0
Source: WHO Global Burden of Disease Database
Since the major risk factor for COPD is tobacco smoking, COPD is a largely preventable disease, and a decrease in smoking would lead to a decline in COPD prevalence. However, there is a low level of public awareness about COPD. This situation is broadly similar to other preventable chronic conditions such as alcoholic liver disease (see Background Chapter 6.14) where the relatively limited success of primary and secondary prevention of alcohol consumption is unfortunately coupled with the view that alcohol‐induced liver disease is largely self‐inflicted. Traditional pharmaceutical treatments for COPD are useful in symptomatic control but do not prevent progression of the disease. Current therapies address the symptoms and range from bronchodilators and corticosteroids to oxygen. There are no effective cures and there is no single diagnostic test for COPD. In particular, no effective COPD‐specific, comprehensive anti‐inflammatory therapy currently exists. In view of the scale of the human and economic costs, better management of lung diseases should become a high priority for all European countries. It is recommended that the existing infrastructure of the Sixth Framework Programme Global Allergy and Asthma European Network should be expanded to create an EU‐wide consortium to study COPD.

Priority Medicines for Europe and the World
76
Since the outlook is poor in the short and medium term for development of emerging new therapies to treat lung inflammation or reverse COPD, the overriding imperative in developing countries and in the expanded EU should be to reduce the prevalence and incidence of smoking.
6.14 Alcohol use disorders: alcoholic liver diseases
In developed countries, alcohol is one of the 10 leading causes of disease and injury. Worldwide, in 2000, alcohol caused about 3% of all deaths (1.8 million) and about 4% of all DALYs (58.3 million). 49 Alcoholic liver disease (defined here as including alcoholic hepatitis and liver cirrhosis) is the most common cause of cirrhosis in the Western world.50 Liver fibrosis caused by alcohol abuse and its end stage, cirrhosis, are major health care problems which are difficult to treat. These conditions would be included in the WHO Global Burden of Disease categorization as ʺcirrhosis of the liverʺ. Figure 6.14.1 shows the burden of alcoholic use disorders as a percentage of the total DALY burden (all acute and chronic conditions) across various age groups and European regions. The WHO Global Burden of Disease includes only the direct burden of the mental disorder of alcohol use, addiction and dependence in this category. In Europe, this burden peaks between the ages 15‐44 at a remarkable 14%‐18% of all DALYs for men of this age group, much higher than the percentage burden for men worldwide. The burden for European women in this age group is much less but is generally in the range of the global values. Across all age groups and both sexes, the EU15 countries have higher percentage disease burdens for alcoholic use disorders than the EU10 countries.
Figure 6.14.1: Alcoholic use disorders (percent of all DALYs by age group)
EU15-M
EU10-M
EU15-F
EU10-F
World-M
World-W
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
Age group
Perc
enta
ge o
f all
DAL
Ys
Source: WHO Global Burden of Disease Database

6. Priority diseases and reasons for inclusion
77
The burden of liver cirrhosis as a percentage of the total DALY burden (all acute and chronic conditions) across various age group and regions peaks between the ages 45‐59 at about 4%‐5% of all DALYs for men in Europe. The burden for European women in this age group is much less but is generally in the range of the global values. Over all age groups and both sexes in the age range of interest, the EU10 countries have higher liver cirrhosis disease burdens than the EU15 countries, a situation reversed from that of alcohol use disorders. The peak in distribution of liver cirrhosis is about 20 years later than that for alcohol use disorders. There is a large gap between basic and applied research into alcoholic liver diseases. Despite the high burden of disease and the many potential biological targets for anti‐fibrotic therapies, there are very few medicines currently in clinical trials specifically directed to reverse, inhibit, or otherwise ameliorate the fibrosis and tissue destruction associated with alcoholic liver diseases. There is little private sector funding directed to alcoholic liver diseases and public sector funding may also be insufficient, especially when compared to the enormous economic and social burdens of alcoholic liver diseases. In principle, all alcoholic liver diseases are preventable with appropriate public health responses regarding behavioural and lifestyle change, including pharmaceutical approaches to combat alcohol addiction. However, progress in developing specific pharmaceutical interventions for alcoholic liver diseases has been hampered by poor understanding of the pathogenesis of these diseases. There is a need for better understanding of the underlying disease pathobiology and better translation between the potential targets for anti‐fibrotic treatments and the medicine development process. Effective anti‐fibrotic treatments are urgently needed.
6.15 Depression in the elderly and adolescents
Depression is a common mental disorder that is characterized by depressed mood and/or loss of interest. In 2002, depression accounted for 4.5% of the global burden and 7.6% of the European burden of disease. Depression affects 3%–15% of the general population. Suicide is one of the major causes of adolescent deaths. The percentage of the elderly affected by depression ranges from 2.5% to 53%, depending on the setting.51 The suicide rate in the elderly is greater than that for any other segment of the population.52 Globally, the age and sex distribution of depression is striking, with female depression being far more common in the 15‐60 age groups, with no significant differences between various regions (see Figure 6.15.1). Children under the age of 14 of both sexes are equally affected. However, among adolescents, the burden is higher in girls.

Priority Medicines for Europe and the World
78
Figure 6.15.1: Burden of depression (DALYs/1000)
EU25-M
EU25-F
EU15-M
EU15-F
EU-10-M
EU-10-F
W-M
W-F
0
5
10
15
20
25
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
Age group
DAL
Yspe
r 100
0
Source: WHO Global Burden of Disease Database
The biology of depression and its treatments are poorly understood, especially in adolescents and in the elderly who have been systematically excluded from studies. Antidepressants have been reported as highly efficacious in adults but they have high levels of side‐effects.53 Lack of efficacy data and a growing number of medicine‐related suicides preclude their use in young people. In a global market worth US$16.6 billion (€13.5 billion) annually, with 7.6% annual growth, the research on antidepressants is intensive, accounting for approximately 16‐20% of annual sales revenues (US$3.2‐5.6 billion or €2.6‐4.5 billion).
Recommendations for a publicly funded research agenda include:
• improving our understanding of the biology of depression and its treatments
• including adolescents, women and the elderly in basic research studies and in clinical trials of both new and existing medicines, to improve efficacy
• initiating comparative studies of existing therapies as suggested in Chapter 8.4
• encouraging comparative research to improve the effectiveness of models of care for mental health within different national health systems.

6. Priority diseases and reasons for inclusion
79
6.16 Postpartum haemorrhage and maternal mortality
Postpartum haemorrhage (PPH) remains a major cause of maternal mortality and morbidity worldwide. Approximately half a million women die annually from causes related to pregnancy and childbirth. At least a quarter of these deaths are a result of postpartum haemorrhage.54 Figure 6.16.1 shows the age distribution of haemorrhage burden (as a percentage of all female mortality) for various WHO regions. The highest mortality rate due to maternal haemorrhage is in the WHO Eastern Mediterranean Region, where it accounts for almost 8% of all female deaths.
Figure 6.16.1: Female haemorrhage mortality (as percentage of all female mortality by WHO region and global)
AFRO
WPRO
World
AMRO
EMRO
EURO
SEARO
0%
1%
2%
3%
4%
5%
6%
7%
8%
0-4 5-14 15-29 30-44 45-59 60-69 70-79 80+
Age group
Fem
ale
haem
orrh
age
mor
talit
y
Source: WHO Global Burden of Disease Database
To prevent and manage PPH, several systems need to be functioning in concert: trained birth attendants, emergency transport systems, availability of blood transfusions, essential obstetrical care and availability of effective oxytocic medicines. Administering intravenous oxytocin immediately after childbirth is the single most important intervention used to prevent PPH.55 However, the requirement for injection of oxytocin by trained staff and the fact that oxytocin requires refrigeration before use, prevents this life‐saving medicine being more widely used in developing countries, where 99% of maternal deaths occur. WHO supported a series of laboratory and field studies in 1993 and 1994 which demonstrated that oxytocin and other oxytocic drugs lost potency under field

Priority Medicines for Europe and the World
80
conditions.56 Unfortunately there has been no follow up to these studies. Thus an opportunity exists for research on and development of heat‐stable oxytocin that can be delivered through simple injection devices.
6.17 Smoking cessation
Tobacco causes nearly five million deaths per year. One in five deaths among males and one in 20 deaths among females is due to tobacco use, and by 2030, the number of tobacco‐related deaths will rise to 10 million per year. During the twenty‐first century, we are likely to see 1 billion tobacco deaths, most of them in developing countries and most of them avoidable. Numerous studies from high‐income countries, and a growing number from low‐ and middle income countries, provide strong evidence that a range of primary and secondary prevention policies can reduce smoking uptake and continuation. The prevalence of tobacco use worldwide is estimated at 29%, and is rising.57 The global rate of tobacco use is significantly higher for men (47%) than women (12%).58 In Denmark, Germany and Sweden today, record levels of women aged 14 to 19 years now smoke, even though national rates are declining. In some Asian countries, smoking among women aged 18 to 24 years has also increased. The number of women smokers is likely to triple over the next generation.58 The prevalence of smoking among young people is also increasing. Data from the Global Youth Tobacco Survey show that one out of five children in the world smokes his or her first cigarette by the age of ten. The prevalence of tobacco use among schoolchildren aged 13 to 15 years varies greatly throughout the world, from 10% to as high as 60%.59 Tobacco use is a known or probable cause of more than thirty‐five specific diseases including chronic diseases such as cancers, cardiovascular disease and respiratory disease.60,61
Smoking cessation therapies and programmes
There is overwhelming evidence of the health benefits, effectiveness and cost‐effectiveness of stopping smoking and of treatment for tobacco dependence, a disorder recognized by the 10th version of WHO’s International Classification of Diseases.62 Unfortunately, smoking cessation is rarely seen as a public health priority and is not necessarily approached as a key tobacco control strategy in governmental and institutional work plans. Short low‐intensity interventions that focus on education and increasing motivation to stop smoking produce a low but measurable success rate, and have a higher potential for population impact. Most smokers that have stopped smoking in Western countries have done so without any therapies or even doctor’s advice.61 In contrast, multi‐session, high‐intensity treatments targeting nicotine‐dependent smokers requiring individual treatment are characterized by a higher success rate, but reach only a small fraction of the population. Pharmacological treatments with proven efficacy, including nicotine replacement therapies (NRT) and bupropion, have become much more widely available in recent years in high‐income

6. Priority diseases and reasons for inclusion
81
countries63 (see Figure 5.3). The evidence base for both the effectiveness and cost‐effectiveness of clinical smoking cessation interventions is strong in Europe and the USA.64 ,65 The evidence is strong and consistent that pharmaceutical treatments significantly improve the likelihood of stopping, with success rates two to three times higher than those when no pharmaceutical treatments are used.66 Despite the proven efficacy of these products there are many obstacles to access. These include restrictions which make nicotine replacement products prescription‐only or pharmacy‐only products or not reimbursable by health authorities.
A number of new products are in clinical trial phases of product development. However, very limited public funds are invested in these research activities. The WHO Framework Convention on Tobacco Control emphasizes that the more comprehensive the package of measures used against tobacco, the greater the impact. Treatment of the addicted tobacco smokers is one of the measures needed. Encouraging the development of more effective pharmaceutical products to aid smoking cessation would be an effective use of public funds.

Priority Medicines for Europe and the World
82
References 1 WHO global strategy for containment of antimicrobial resistance. Geneva: World
Health Organization; 2001. Available from: http://www.who.int/entity/csr/resources/publications/drugresist/en/EGlobal_Strat.pdf
2 European Commission, Directorate General for Research. Antimicrobial resistance research in the quality of life programme. Luxembourg: Office for Official Publications of the European Communities; 2003. Available from: http://europa.eu.int/comm/research/quality‐of‐life/pdf/qol_antimicrobialfinal.pdf (accessed 31 July 2004).
3 EU‐issued Recommendations on the prudent use of antimicrobial agents in human medicine. Proposal for a Council recommendation, Comm. 2001, 333, Vol. II. Brussels: Council of the European Union; 2001.
4 Council Resolution of 8 June 1999 on antibiotic resistance. A strategy against the microbial threat. Official J Europ Communities 1999;41(C195):1–3.
5 European Surveillance of Antimicrobial Consumption (ESAC). Website: http://www.ua.ac.be/esac/
6 Salgado CD, Farr BM, Calfee DP. Community‐acquired methicillin‐resistant Staphylococcus aureus: a meta‐analysis of prevalence and risk factors. Clin Infect Dis 2003;36(2):131‐139.
7 Communicable diseases 2002. Global defence against the infectious disease threat. Geneva: World Health Organzation;2003. (WHO/CDS/2003.15).
8 Global agenda on influenza surveillance and control. Geneva: World Health Organization; 2003. Available from: http://www.who.int/csr/disease/influenza/csrinfluenzaglobalagenda/en/.
9 Commission working document on community influenza pandemic preparedness and response planning. Brussels: European Commission; 2004.
10 Nicholson KG, Wood JM, Zambon M. Influenza. Lancet 2003;362(9397):1733‐45.
11 WHO guidelines on the use of vaccines and antivirals during influenza pandemics. Geneva: World Health Organization; 2004. Report No.: WHO/CDS/CSR/RMD/2004.8.
12 Scuffham PA, West PA. Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine 2002;20(19‐20):2562‐2578.
13 Antithrombotic Trialistsʹ Collaboration. Collaborative meta‐analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction and stroke in high risk patients. BMJ 2002;324(7329):71‐86.
14 Heart Outcomes Prevention Evaluation (HOPE) Study Investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO‐HOPE substudy. Lancet 2000;355(9200):253‐259.
15 PROGRESS Collaborative Group. Randomised trial of a perindopril‐based blood pressure lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001; 358(9287):1033‐1041.
16 Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high‐risk individuals: a randomized

6. Priority diseases and reasons for inclusion
83
placebo‐controlled trial. Lancet 2002;360(9326):7‐22.
17 Wood D, EUROASPIRE I and II Group. Clinical reality of coronary prevention guidelines: a comparison of EUROASPIRE I and II in nine countries. Lancet 2001;357(9261):996‐1001.
18 Wald N, Law M. A strategy to reduce cardiovascular disease by more than 80%. BMJ 2003;326(7404):1419‐1425.
19 IDF. Diabetes atlas. 2nd ed. Brussels: International Diabetes Federation; 2003.
20 World cancer report 2003. Geneva: World Health Organization, International Agency for Research on Cancer; 2003 Available from: http://www.iarc.fr/WCR
21 Bray F, Sankila R, Ferlay J, Parkin DM. Estimates of cancer incidence and mortality in Europe in 1995. Eur J Cancer 2002;38(1):99‐166.
22 National Cancer Control Programmes: Policies and management guidelines. Geneva: World Health Organization; 1995.
23 WHO burden of diseases and injury (Dataset‐2002). Geneva: World Health Organization; 2003.
24 Adams HP Jr, Adams RJ, Brott T, del Zoppo GJ, Furlan A, Goldstein LB et al. Guidelines for the early management of patients with ischemic stroke: A scientific statement from the Stroke Council of the American Stroke Association. Stroke 2003;34(4):1056‐83.
25 Fisher M. The ischemic penumbra: identification, evolution and treatment concepts. Cerebrovasc Dis 2004;17:Suppl 1‐6.
26 AIDS epidemic update. Geneva: UNAIDS/World Health Organization; 2003. Available from: http://www.unaids.org (accessed 20 May 2004).
27 Fleck F. Eastern Europe and Russia face worldʹs fastest growing HIV epidemic. BMJ 2004;328(7438):486.
28 Becker SL New targets, new drugs, failed trials and the need for more information. Posit Aware 2004;15(1):12‐13.
29 Klausner RD, Fauci AS, Corey L, Nabel GJ, Gayle H, Berkeley S, et al. The need for a global HIV vaccine enterprise. Science 2003;300(5628):2036‐2039.
30 Anti‐TB drug resistance in the world. Report no. 2. Prevalence and trends. Geneva: World Health Organization; 2000. Report No.: WHO/CDS/TB/2000.278.
31 O’Brien R, Nunn P. The need for new drugs against tuberculosis. Am J Respir Crit Care Med 2001;163(5):1055‐1058.
32 EC European research area fact sheet: EU‐funded research in the fight against tuberculosis. Available from: http://europa.eu.int/comm/research/press/2003/pr2403en.html (accessed 3 March 2004).
33 Depoortere E, Legros D, Torreele E. Developing a needs‐based and rational approach to identify neglected diseases and select R&D projects that could maximally impact treatment options. Paris: Médecins Sans Frontières, Drugs for Neglected Diseases Working Group; 2001.
34 Sleeping sickness or human African trypanosomiasis. MSF fact sheet. Brussels:

Priority Medicines for Europe and the World
84
Médecins Sans Frontières; 2004. Available from: http://www.accessmed‐msf.org/documents/ssfactsheet.pdf
35 Trouiller P, Olliaro P, Torreele E, Orbinski J, Laing R, Ford N. Drug development for neglected diseases: a deficient market and a public‐health policy failure. Lancet 2002;359(9324):2188‐2194.
36 ACP‐EU Joint Parliamentary Assembly Resolution on poverty‐related diseases and reproductive health in ACP States. Addis Ababa: ACP‐EU Joint Parliamentary Assembly; 2004. Report No.: ACP‐EU 3640/04/fin.
37 Breman JG, Egan A, Keusch GT. The intolerable burden of malaria: a new look at the numbers. Am J Trop Med Hyg 2001;64(1‐2 Suppl.):IV‐VII.
38 Arrow KJ, Panosian C, editors. Saving lives, buying time. Institute of Medicine of the US National Academies of Science (IOM); 2004:1‐326.
39 Global Malaria Control Strategy. Report of a WHO Study Group on the Implementation of the Global Plan of Action for Malaria Control 1993–2000. Geneva: World Health Organization; 1993. (WHO Technical Report Series, No. 839).
40 Annual report 2003. Geneva: Medicines for Malaria Venture; 2003. Available from: http://www.mmv.org/filesupld/184.pdf
41 Mental health. Alzheimer’s disease. Brazzaville: World Health Organization Regional Office for Africa; 2002. Available from: www.afro.who.int/mentalhealth/related_disease/alzheimer_disease.html (accessed 4 March 2004).
42 Bullock R. New drugs for Alzheimer’s disease and other dementias. Br J Psychiatry 2002;180:135‐139.
43 Arthritis Foundation. Website: http://www.arthritis.org/conditions (accessed 11 February 2004).
44 Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ, 2003;81(9):646‐656.
45 Hochberg MC, McAlindon T, Felson DT. Osteoarthritis: new insights. Part 2: Treatment approaches. Ann Intern Med 2000;133(9):26‐729.
46 Murray CJ, Lopez AD. Global morality, disability and the contribution of risk factors: global burden of disease study. Lancet 1997;349(9063):1436–1442.
47 Aıt‐Khaled N, Enarson D, Bousquet J. Chronic respiratory diseases in developing countries: the burden and strategies for prevention and management. Bull World Health Organ 2001;79(10):971–979.
48 Mannino DM. Chronic obstructive pulmonary disease: definition and epidemiology. Respir Care 2003;48(12):1185‐1191.
49 Rehm J, Broome R, Monteiro M, Gmel G, Graham K, Rehn N, et al. Alcohol as a risk factor for global Burden of Disease. Eur Addict Res 2003;9(4):157–164.
50 Rehn, N, Room, R, Edwards, G. Alcohol in the European Region – consumption, harm and policies. Copenhagen: World Health Organization Regional Office for Europe; 2001.
51 Birrer RB. Depression and aging too often do mix. Postgrad Med 1998;104(3):143‐149.

6. Priority diseases and reasons for inclusion
85
52 Harwood DM, Hawton K, Hope T, Jacoby R. Suicide in older people: mode of death,
demographic factors, and medical contact before death. Int J Geriatr Psychiatry 2000;15(8):736‐743.
53 Antidepressants, side effects comparisons. Drug Digest; 2004. Website: http://www.drugdigest.org (accessed 10 July 2004).
54 Mousa HA, Walkinshaw S. Major postpartum hemorrhage. Curr Opin Obstet Gynecol 2001;13(6):595‐603.
55 Prendiville WJ, Harding JE, Elbourne DR, Stirrat GM. The Bristol third stage trial: active versus physiological management of third stage of labour. BMJ 1988;297(6659):1295‐1300.
56 Hogerzeil HV, Walker GJA, De Goeje MJ. Stability of injectable oxytocics in topical climates. Geneva: World Health Organization; 1993. Document No.: WHO/DAP/93.6. Available from: http://whqlibdoc.who.int/hq/1993/WHO_DAP_93.6.pdf
57 Jha P, Chaloupka FJ, eds. Tobacco control in developing countries. Oxford: Oxford University Press; 2000.
58 Samet J. Yoon SY. Women and the tobacco epidemic. Geneva: World Health Organization; 2001.
59 The Global Youth Tobacco Survey Collaborative Group (US Centers for Disease Control and Prevention; World Health Organization, the Canadian Public Health Association, and the U.S. National Cancer Institute). Tobacco use among youth: a cross country comparison. Tobacco Control 2002;11:252‐270.
60 U.S. Department of Health and Human Services. The health benefits of smoking cessation: a report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Centers for Disease Control, Office on Smoking and Health; 1990.
61 Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr. Mortality from smoking in developed countries 1950‐2000. Indirect estimation from National Vital Statistics. Oxford: Oxford University Press; 1994.
62 International statistical classification of diseases and related health problems, 10th ed. Geneva: World Health Organization; 1994.
63 U.S. Department of Health and Human Services. Reducing tobacco use: a report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, Office on Smoking and Health, 2000. http://www.cdc.gov/tobacco/sgr_tobacco_use.htm (accessed 3 May 2002).
64 Fiore MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and dependence. Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, 2000.
65 Lancaster T, Stead L, Snowden A, et al. Cochrane Tobacco Addiction Group. In: The Cochrane Library, Issue 2, 2002. http://www.dphpc.ox.ac.uk/cochranetobacco/ (accessed 20 May 2002.
66 Raw M, McNeil A, West R. Smoking cessation: evidence‐based recommendations for the healthcare system. BMJ 1999; 318:182‐85.

Priority Medicines for Europe and the World
86

7. Cross-cutting themes
87
7. Cross-cutting themes This chapter covers a number of issues which apply to all diseases and therapeutic strategies. The themes include medicine delivery mechanisms and the particular needs of special groups. The section on delivery mechanisms focuses on an example of where translational research is needed in order to make use of proven medicine delivery technologies to meet patient needs, namely the development and use of fixed‐dose combination (FDC) preparations. At the outset, it should be noted that, strictly speaking, FDCs are not a delivery device (such as transdermal patches and sustained release spheres) to be used in situations where delivery of a medicine is a problem that needs to be overcome. However, FDCs can the improve the delivery of medicines to patients by improving adherence to therapy. Special groups include the elderly, women and children. Each of these groups have particular pharmaceutical needs due to their changing physiology, the spectrum of diseases they face, and the fact that they have been neglected during the pharmaceutical development process. While similar issues exist for these groups, other particular needs can also be identified. Orphan diseases are a complex and heterogeneous mosaic of an estimated 5000‐8000 conditions, and for many of them no appropriate medical interventions exist because the cost of bringing a product to the market would not be compensated by the expected sales. Although since 1999 the EU has implemented an array of regulatory incentives in order to promote the development of orphan drugs, there remain various gaps both on the level of basic research and in the translational studies that are needed to bring conceptual knowledge of disease processes to the development of new therapeutics.
7.1 Medicine delivery mechanisms
Medicines have to be administered to the patient via different medicine delivery mechanisms in order to achieve maximum clinical benefit. The most common delivery mechanisms are tablets or capsules for oral delivery, suppositories for rectal delivery, and injections if the parenteral route is chosen. Over recent decades, the biomedical industry has developed a range of sustained release devices (such as patches for transdermal drug delivery and intranasal formulations), many of which rely on medicines diffusing or dissolving from a matrix or other structure that contains the medication.1 However, constraints on both private and public sector funding have limited further development of such technologies for diseases of public health importance. A review of the existing state of the art of medicine delivery mechanisms leads to two main conclusions.

Priority Medicines for Europe and the World
88
Firstly, there is a wide range of existing evidence‐based, very often off‐patent, technologies that are heavily underutilized. Such technologies could be used to improve the “patient‐friendly” performance of a number of existing medicines, the use of medicines in paediatrics and geriatrics, and other areas where individualized time‐dosing of medicines is required, e.g., patients with impaired liver or kidney functions, or patients with compromised immune systems. Safety concerns increasingly drive the need for targeting potent, but very toxic, medicines (e.g., cytostatics, antivirals and certain antifungals) to their site of action in the body, instead of exposing the whole body to the medicine. It is recommended that the EU invest in translational research programmes to bring proven medicine delivery technologies to those areas where currently available systems fail (e.g., HIV therapies for children; medicine targeting in cancer therapy; and therapies for chronic diseases in the elderly). Secondly, the advent of new biotechnology‐derived protein/DNA‐based medicines and existing proteins, such as insulin or oxytocin, have created a need for investments in better delivery technologies.2 New stabilization concepts (e.g., heat‐resistant insulin or oxytocin) and other “all‐weather” drug delivery mechanisms are a major need. Moreover, most current protein/DNA‐based medicines need to be administered to the patient via the parenteral route (i.e., injection, infusion). There is also a great need to develop alternative, needle‐free delivery mechanisms that are better adapted to patient needs. Finally, many therapies based on biologicals, including gene therapies and vaccines, need targeted delivery mechanisms to reach specific sites on the cell, inside the cell or inside the cell nucleus. The biotechnology industry is making impressive progress in these areas and public funding should be directed to maintaining academic and basic research and training of future scientists (see Background Chapter 7.1). A key example of the first conclusion, i.e., the need to stimulate translational research in order to develop proven medicine delivery technologies to meet patient needs, are FDCs. FDCs can be defined as two or more medicines in a single formulation, each drug having an independent mode of action, the combination of which creates a synergistic, additive or complementary effect. “Free” combinations can be defined as two or more drugs in separate formulations, each usually taken at the same time. Indeed, combination therapy, in whatever form, may be essential in the treatment of hypertension and other cardiovascular conditions,3 as well as for major infectious diseases such as HIV/AIDS, TB and malaria, and for the prevention of antibacterial resistance. FDCs have the potential to simplify treatment regimens and improve compliance in patients using polypharmacy. However, with few exceptions, the pharmaceutical industry has generally been wary of FDCs as an innovative delivery mechanism, particularly for antibacterials, following the extensive review of combination products as part of a study carried out by the Food and Drug Administration in the USA in the 1960s and beyond.4 For decades, virtually all clinical guidelines, the teaching of health professionals, and the regulatory environment have been resolutely opposed to the

7. Cross-cutting themes
89
concept of combining multiple biologically active compounds into a single tablet or capsule. The only exception to this stance has been for proven combinations (e.g., contraceptives based on estrogen‐prostagen combinations; combinations of enzyme inhibitors with antibiotics or Parkinson therapies; and combined potassium‐sparing diuretics). This opposition to the use of FDCs has been largely fuelled by the fear of overuse of medicines and the limited possibilities for patient‐specific individualization of therapy. However, there are some indications that the pendulum is now starting to swing back towards more support for the use of FDCs. A recent meeting at WHO (see Background Chapter 7.1) addressed the main issues related to FDCs for the treatment of HIV/AIDS, TB and malaria. Another sign is the recent paper by Wald et al. (see Background Chapter 6.3), proposing the widespread use of a cardiovascular ʺpolypill.ʺ In this Report, Chapter 6.3 recommends the evaluation of two different FDCs for the secondary prevention of heart attack and stroke respectively. However, the use of such FDCs for primary prevention of heart attack and stroke is not endorsed. Specially designed clinical trials and epidemiological, social and behavioural studies can test the potential for FDCs to inhibit or even prevent antibacterial resistance, to secondarily prevent cardiovascular disease, and to improve patient compliance for a variety of medication taken over prolonged periods. Although there are pharmacological, regulatory and intellectual property/legal barriers to the widespread use of FDCs, these barriers can be overcome with a comprehensive strategy and cooperation between and among the private and public sectors. It is recommended that an FDC research agenda should be established to answer the following questions: • In view of the clear public health need for FDCs, what are the clinically
desirable combinations?
• What is the actual evidence to support the rationales for use of FDCs? For instance, while decreasing overall antibiotic use may reverse bacterial resistance in human populations, the use of combination therapy may not necessarily have the same effect. It is thus critical to know whether the use of FDCs will prevent the appearance of drug resistance and/or reverse existing rates of drug resistance at both the individual and population levels. Although it is likely to be difficult to measure changes in ongoing antibacterial resistance in field situations, well thought out epidemiological studies should be undertaken to provide evidence as to whether FDCs slow or eliminate antibacterial resistance.
• Are the legal and intellectual property barriers to increased FDC access more apparent than real? Research should be directed to finding creative ways of managing multiple ownership issues of FDCs and increasing access for both research and clinical purposes.5
• What are the “real world” formulation and quality assurance issues?

Priority Medicines for Europe and the World
90
• Can there be standardized regulatory requirements for “combination” products? Should synergy be required for combinations or is this too high a hurdle?
It is recommended that the European Union should sponsor one or more FDC Centres of Excellence which would act as “clearing houses” for information about FDC therapy, coordinate field studies of FDCs and assemble and maintain the best evidence on their development, as well as on regulatory and legal issues.
7.2 Pharmaceuticals and the elderly
The number of elderly people is increasing throughout the world. By the year 2020, 25% of the global population will be aged 60 or over. In Europe, this proportion will be even greater.6 The increased frailty of the elderly, the increasing prevalence of diseases (including co‐morbidities) that affect them and the large numbers of medicines used per patient have a major impact on health systems. The elderly are particularly susceptible to cardiovascular diseases, Alzheimer disease, Parkinson disease, chronic obstructive pulmonary disease (COPD), depression and musculoskeletal disorders, including osteoarthritis. The aging of the society brings several specific problems. The rate of adverse reactions to medicines in elderly patients is higher than for other patient groups in society, possibly because of increased used of medicines, co‐morbidity and the risk of medicine‐medicine and medicine‐disease interactions. However, most of the adverse reactions to medicines appear to be preventable if appropriate systems are in place to avoid medicine‐related problems. 7 The altered body functions in the elderly (e.g., changing body composition and liver metabolism) may require adapted dosages and very often there is a need for alternative treatment options specifically tailored to the elderly.8 In addition to the use of multiple medicines — very often the result of co‐morbidities in the elderly — underuse of evidence‐based medication is another important, but not well‐recognized problem. Ample data show frequent occurrence of underuse of medicines among the elderly, leading to unnecessary deterioration in health. Underuse is caused by a variety of factors, ranging from poor access to health care to practical problems with formulations (for example, difficulties in opening medication containers). To improve adherence, to prevent underuse, and to provide the best possible care, there is a special need to develop adapted formulations for medications especially for use by the elderly. The pharmaceutical industry is investing heavily in research on specific diseases which are prevalent among the elderly (Alzheimer disease, Parkinson disease and others). For national governments and international institutions like the EU, it does not seem efficient to support this type of large‐scale research through the investment of limited public money.

7. Cross-cutting themes
91
One area deserving of support is in basic research in the field of aging. If there were an accurate understanding of the process of aging, it would be easier to understand the pathophysiology and epidemiology of diseases which are prevalent among the elderly. Despite the guidance of the European Medicines Agency (EMEA) (1995),9 the elderly are still unjustifiably excluded from clinical trials. Laws and guidelines should be developed which include obligations towards the participation of the elderly. The EU and national governments could improve the knowledge of medicine effects in the elderly, thereby providing more accurate health care and preventing medication errors. Cooperation between the pharmaceutical industry and governments is warranted. Appropriate dosing is the key to successful medicines development and dosing in the elderly is one Achilles heel of medicines innovation. By developing special formulations for the elderly, adherence can be improved and taking medications will be a less discomforting experience. Adverse reactions to medicines and medication errors occur frequently in the elderly and most of these events are preventable. A system should be provided which can monitor the different therapies a patient is taking. In this way, adverse reactions to medicines and other medication errors could be prevented — thereby lowering health care costs, reducing hospital admissions and increasing quality of life. Although such monitoring systems are expensive, national government support (financial or practical) may make it easier for health services to introduce them. Over the past decade, awareness of the impact of the growing numbers of elderly has increased. The aging society has been one of the Key Actions of the Fifth Framework Programme of the European Union. As stated in the Fifth Framework Programme, basic research is needed to enhance the quality of life of the elderly, and to keep them independent as long as possible, thereby reducing the burden on public health systems. If the underlying processes of aging and of the age‐dependent disorders are known, it will be easier to develop therapies and to keep the elderly as healthy as possible.
7.3 Pharmaceuticals and children
Children are subject to many of the same diseases as adults and are often treated with the same medicines. However, many of the medicines used in children are either not licensed for this age group or are prescribed outside the terms of the medicine licence (‘off‐label’). Unlicensed medicine use in children ranges from 25% to 50% and off‐label medicine use ranges from 15% to 40%. 10 , 11 Where the medicine licence contains statements such as “no evidence for use in children”, this does not necessarily mean that the medicine is unsafe for use in children, but clearly indicates the absence of data for its use in this patient group. Doses for children are often merely adjusted for their smaller weight. However, there are many other differences in children that can affect how medicines act in the body. Children not only differ in pharmacokinetic and pharmacodynamic aspects, but also in

Priority Medicines for Europe and the World
92
adherence to therapy and other factors that influence the effectiveness of medicine use. Despite this, prescriptions for children are often not based on sound scientific evidence. Because of the lack of paediatric licensing, there are only a few paediatric formulations and adult dosages have to be converted to the appropriate paediatric dosage. However, unlicensed and off‐label medicine use increases the risk of miscalculating doses and induces a higher rate of adverse reactions to medicines.12 Moreover, the intake of adult medicines is not a very pleasant experience for children. New or adapted formulations for children may improve administration and as a result improve patient adherence to therapy (e.g. paediatric HIV therapy). In addition to the research gaps on paediatric dosing and formulations, there are three other important considerations related to medicine use in children:
Data needed for effective and safe use of medicines in children and adolescents cannot be linearly abstracted from adult data. Unlicensed and off‐label use of medicines in children are essentially regulatory observations; these observations should lead to specific paediatric clinical and pharmaceutical follow‐up.
There is increasing recognition that certain paediatric morbidities are specific to childhood (e.g., neonatal respiratory problems, paediatric cancers); other condi‐tions require more specific medicine formulations and/or dosing schemes.
Certain childhood morbidities are very often ʹearly signaturesʹ for severe and chronic adult diseases (e.g., wheezing/childhood asthma and chronic respiratory diseases later in life, childhood obesity and diabetes/cardiovascular problems, paediatric mental problems and severe adult psychiatric morbidities). Accurate diagnosis and treatment at an early age are essential prevention strategies in order to reduce adult disease burden.
Therefore, specific research is needed on the use of medicines in children. However, there are several obstacles to this. First, when medication is used unlicensed or off‐label, there are no data available on effectiveness, safety, dosage or toxicity. Second, some diseases only occur in children (for example, certain forms of leukaemia, juvenile arthritis) and medicines for treatment must be investigated in children. Conducting paediatric trials is difficult, not only because the patient population is low, but because of ethical issues relating to the use of placebos and legal issues relating to liability. Third, pharmaceutical companies do not often perform paediatric studies on medicines which they intended to market primarily to adults, mainly because — despite various governmental incentives — these medicines would provide little additional revenue from use in children. There seems to be little incentive for medicine sponsors to conduct paediatric research on off‐patent medicines — a category which includes many of the medicines which are widely used in children but which lack paediatric information in their labelling.

7. Cross-cutting themes
93
There is a very important interaction between the regulatory environment and paediatric medicines research in the USA and Europe. The U.S. FDA has developed a number of initiatives to obtain more information on paediatric use of medical products. The Paediatric Labeling Rule in 1994 resulted in The Best Pharmaceuticals for Children Act (BPCA) in 2002.13 This law provides an additional six monthsʹ market exclusivity for companies that are willing to test their medication voluntarily in children. There are also important European initiatives commissioned by the EMEA. A European guideline on paediatric clinical trials has been in force since July 2002 and a Directive on Good Clinical Practice was adopted that takes into account some specific concerns on performing clinical trials in children. However, these European initiatives do not have the force of law and merely encourage the pharmaceutical industry to investigate the use of medicines in children. Thus, the US pharmaceutical industry has more incentive to conduct paediatric medicine studies than does the industry in Europe. To reduce this gap, the European Commission‐Enterprise Directorate has proposed a European Legislative Initiative called ‘Better Medicines for Children’ which would provide regulations to: provide incentives for research; introduce a period of data protection; create a specific fund that could be used to finance paediatric research; create legal requirements for paediatric clinical trials; create a central database on off‐label uses; and, among other initiatives, create a pan‐European network of clinical excellence for the performance of paediatric studies.14 To improve medicines development for children, there is a need to invest more in basic paediatric research, to improve the participation of children in clinical trials, and to reverse the underfunding of research on children‐specific medicine formulations. There is also a need for more information on the safety and efficacy of medication use in children, especially for mental disorders, which account for a high burden of disease (for example, depression, anxiety disorders). On 29 September 2004, the European Commission published a proposal for the regulation of medicines for children. The key elements of this proposal include creation of a new expert committee within the EMEA, a requirement for data on the use of medicines in children at the time of marketing authorization, a six‐month patent extension for paediatric use, increased safety monitoring, an EU inventory of therapeutic needs of children, and the provision of free scientific advice by the EMEA to the industry.i
7.4 Pharmaceuticals and women
Although women are the most frequent users of medicines, little is known about many aspects of women’s interaction with medicines and there are research gaps on important ‘female’ health issues, including breast cancer, reproduction control, female subfertility, pregnancy and lactation, and menopausal conditions (including hormone therapy). Several studies have shown that there may be differences in the effects of
i See http://pharmacos.eudra.org/F2/Paediatrics/docs/Paeds%20press%20release%2029%20Sept.pdf

Priority Medicines for Europe and the World
94
medicines in women and men.15,16 Measuring the pharmacokinetics of medicines in women of different ages and body weight would provide much‐needed information for prescribers. Since the 1960s, millions of women have taken hormonal contraception either orally (“the pill”), by injection (as a depot preparation) or as an implant. The rate of use varies by geographical area and by age.17 Nearly 40% of women who take oral contraceptives do so for more than five years. Following safety concerns about the use of such medicines for long periods, the hormonal content has been reduced over time to improve safety while at the same time preventing pregnancy. The impact of hormonal fertility control has been dramatic, with declines in fertility occurring in nearly all countries. This has had a substantial impact on the age structure of populations. While most women have access to hormonal contraception, uptake varies greatly, with rates as low as 2% in Cameroon.18 As women increasingly get married at older ages and defer having children, the prevalence of female subfertility has increased. However, subfertility treatment is still sub‐optimal. The success rate of IVF is about 25% per cycle and the technique is associated with side‐effects and an increase in the risk of complications and multiple births. Multiple births are associated with an increase in morbidity, mortality and disability. An additional concern is the lack of knowledge about the effects of medicines during pregnancy. Since the thalidomide crisis in the early 1960s, concern remains about the use of medicines in pregnancy. 19 It is estimated that about 62%‐80% of pregnant women take at least one medicine during pregnancy. Although women reduce the use of medicines once they know they are pregnant, there is a risk of exposure in the period between conception and the detection of pregnancy. Meanwhile, as more women take medicines for chronic conditions, it becomes inevitable that women will take medicines during pregnancy and while lactating. For most medicines, there are no certainties about their possible effects on the developing foetus or nearly born child. Since hardly any medication today is tested in humans in pregnancy or during lactation, this leads to the use of unproven, off‐label medicines at these times. There is a continuing need to collect data on all possible exposures and outcomes and to analyse this information. The use of post‐reproductive hormone replacement therapy (HRT), which varies from 0% to 42% among women in 20 countries,18 entails both risks and benefits. While long‐term HRT use has been found to be associated with prevention of chronic diseases (osteoporosis, some cancers), the use of HRT may also increase the risks of several cancers and cardiovascular disease. A large part of the problems associated with female interactions with medicines is due to a lack of basic knowledge about the effects of hormones, changing physiology in pregnancy or during lactation, and the causes of subfertility. In the past, womenʹs health has often been neglected. For a long time, women were excluded from clinical
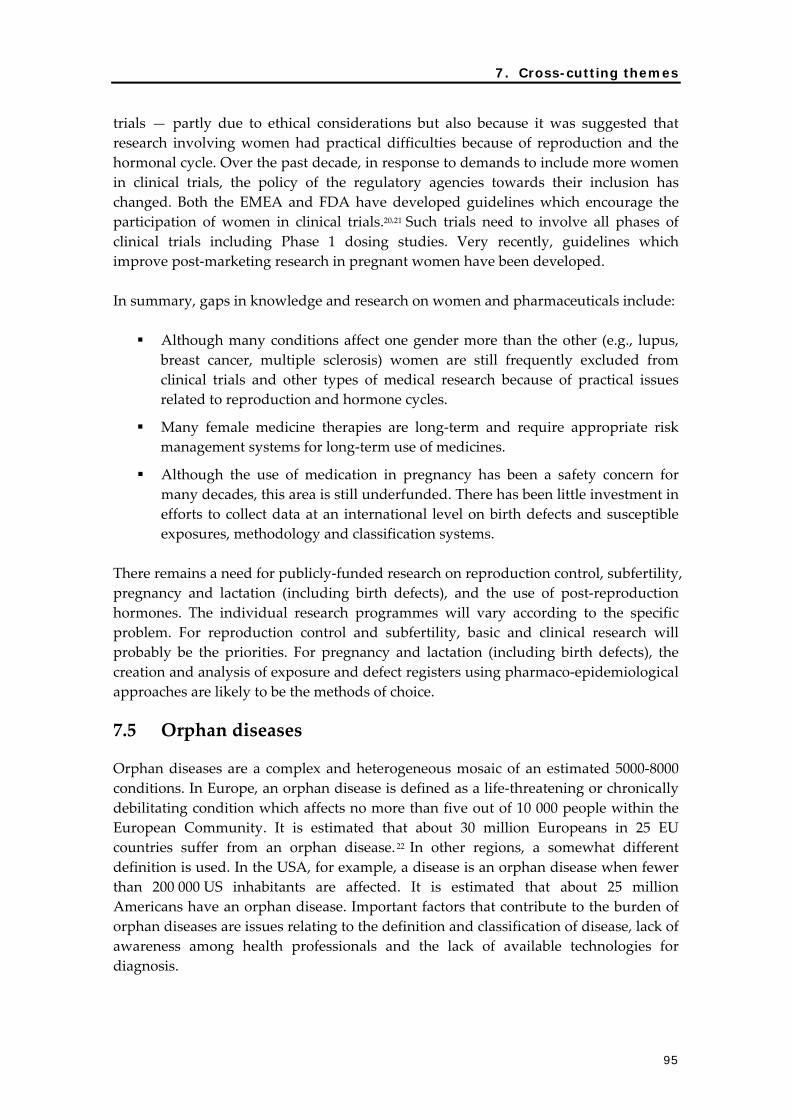
7. Cross-cutting themes
95
trials — partly due to ethical considerations but also because it was suggested that research involving women had practical difficulties because of reproduction and the hormonal cycle. Over the past decade, in response to demands to include more women in clinical trials, the policy of the regulatory agencies towards their inclusion has changed. Both the EMEA and FDA have developed guidelines which encourage the participation of women in clinical trials.20,21 Such trials need to involve all phases of clinical trials including Phase 1 dosing studies. Very recently, guidelines which improve post‐marketing research in pregnant women have been developed. In summary, gaps in knowledge and research on women and pharmaceuticals include:
Although many conditions affect one gender more than the other (e.g., lupus, breast cancer, multiple sclerosis) women are still frequently excluded from clinical trials and other types of medical research because of practical issues related to reproduction and hormone cycles.
Many female medicine therapies are long‐term and require appropriate risk management systems for long‐term use of medicines.
Although the use of medication in pregnancy has been a safety concern for many decades, this area is still underfunded. There has been little investment in efforts to collect data at an international level on birth defects and susceptible exposures, methodology and classification systems.
There remains a need for publicly‐funded research on reproduction control, subfertility, pregnancy and lactation (including birth defects), and the use of post‐reproduction hormones. The individual research programmes will vary according to the specific problem. For reproduction control and subfertility, basic and clinical research will probably be the priorities. For pregnancy and lactation (including birth defects), the creation and analysis of exposure and defect registers using pharmaco‐epidemiological approaches are likely to be the methods of choice.
7.5 Orphan diseases
Orphan diseases are a complex and heterogeneous mosaic of an estimated 5000‐8000 conditions. In Europe, an orphan disease is defined as a life‐threatening or chronically debilitating condition which affects no more than five out of 10 000 people within the European Community. It is estimated that about 30 million Europeans in 25 EU countries suffer from an orphan disease.22 In other regions, a somewhat different definition is used. In the USA, for example, a disease is an orphan disease when fewer than 200 000 US inhabitants are affected. It is estimated that about 25 million Americans have an orphan disease. Important factors that contribute to the burden of orphan diseases are issues relating to the definition and classification of disease, lack of awareness among health professionals and the lack of available technologies for diagnosis.

Priority Medicines for Europe and the World
96
For many orphan diseases, no appropriate medical interventions exist because the cost of bringing a product to the market would not be compensated by the expected sales. In 1999, the EU approved a legislative framework to provide incentives to develop medicinal products for orphan diseases. In the USA, this kind of legislation has been in place since 1983 when the US Orphan Drug Act was introduced.23 Since its inception, this legislation has been very successful in bringing more than 230 medicinal products for orphan diseases to the market, thereby facilitating treatment for an estimated 11 million patients in the USA, with even greater numbers being approved internationally. Experiences so far with the development of medicines for orphan diseases underline the need for a subtle and creative interplay between research, regulatory issues and market incentives. Although the EU has implemented regulatory incentives to promote the development of medicines for orphan diseases, there is a need to bridge the gap between conceptual knowledge of disease processes and the development of efficacious, safe and affordable therapeutics. In summary, various gaps related to the development of treatment for rare diseases can be identified:
• There is still a great need for a basic molecular understanding of the diseases and identification of possible pharmacological targets in many of the rare mono‐ and polygenic disorders.
• In view of the rarity of these diseases, it is recommended that public money should be used to fund basic research. EU Framework Programmes may be a good instrument for funding this research, provided that the appropriate tools for research in rare diseases are defined.
• Although genomic and proteomic technologies provide useful clues for both diagnosis and treatment of rare diseases, there is a serious gap in clinical evaluation.
• There is a lack of long‐term epidemiology data on both medicine safety and effectiveness and on the course of the disease.
• For several groups of rare diseases, fundamental research has already been done, but the next step into translational research is too difficult. For these cases, a funding programme like the Office of Orphan Products Development (OOPD) Grant Program in the USA could stimulate this research and cooperation between universities and the pharmaceutical industry.24
• A public database of clinical trials on rare diseases is needed.
• Large, multidisciplinary networks should be funded between all interested parties by facilitating European networks of medical experts, reference centres and patients groups for orphan diseases. This infrastructure is necessary for performance of clinical trials for rare diseases and subsequent monitoring of the new products.

7. Cross-cutting themes
97
References 1 Urquhart J. Controlled drug delivery: therapeutic and pharmacological aspects. J Intern
Med 2000;248(5):357‐376.
2 Crommelin DJA, Storm G, Verrijk R, de Leede L, Jiskoot W, Hennink WE. Shifting paradigms: biopharmaceuticals versus low molecular weight drugs. Int J Pharmaceutics 2003, 266;(1‐2):3‐16.
3 Wald N, Law M. A strategy to reduce cardiovascular disease by more than 80%. BMJ 2003;326:1419‐1425.
4 Bazell RJ. Drug efficacy study: FDA yields on fixed combinations. Science 1971;172(987):1013‐1015.
5 Clark J, Piccolo J, Stanton B, Tyson K. Patents pools: a solution to the problem of access in biotechnology patents? Available from: http://www.uspto.gov/web/offices/pac/dapp/opla/patentpool.pdf (accessed 10 January 2002.
6 Population database. New York: United Nations, Department of Economic and Social Affairs, Population Division; 2002. Available from: http://www.un.org/esa/population/unpop.htm (accessed 15 May 2004).
7 Thomas EJ, Brennan TA. Incidence and types of preventable adverse events in elderly patients: population‐based review of medical records. BMJ 2000;320(7237):741‐744.
8 Mangoni AA, Jackson SH. Age‐related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol 2004;57(1):6‐14.
9 Note for guidance on studies of support special populations: geriatrics. London: European Agency for the Evaluation of Medicinal Products (EMEA); 1995. Report No.: CPMP/ICH/379/95.
10 ʹt Jong GW, Vulto AG, de Hoog M, Schimmel KJM, Tibboel D, van den Anker JN. A survey of the use of off‐label and unlicensed drugs in a Dutch childrenʹs hospital. Pediatrics 2001;108(5):1089‐1093.
11 Conroy S, Choonara I, Impicciatore P, Mohn A, Arnell H, Rane A, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. BMJ 2000;320(7227):79‐82.
12 ʹt Jong GW. Unlicensed and off‐label drug use in children [dissertation]. Rotterdam: Erasmus University; 2002.
13 U.S. Best Pharmaceuticals for Children Act, 2001. Website: http://www.fda.gov/opacom/laws/pharmkids/contents.html (accessed 21 September 2004).
14 Ceci A, Felisi M, Catapano M, Baiardi P, Cipollina L, Ravera S, et al. Medicines for children licensed by the European Agency for the Evaluation of Medicinal Products. Eur J Clin Pharmacol 2002;58(8):495‐500.
15 Dominick KL, Ahern FM, Gold CH, Heller DA. Gender differences in NSAID use among older adults with osteoarthritis. Ann Pharmacother 2003;37(11):1566‐1571.
16 Isacson D, Bingefors K. Epidemiology of analgesic use: a gender perspective.

Priority Medicines for Europe and the World
98
Eur J Anaesthesiol Suppl 2002;26:5‐15.
17 Lundberg V, Tolonen H, Stegmayr B, Kuulasmaa K, Asplund K, WHO MONICA Project. Use of oral contraceptives and hormone replacement therapy in the WHO MONICA project. Maturitas 2004;48(1):39‐49.
18 World fertility report 2003. New York: United Nations, Department of Economic and Social Affairs, Population Division; 2004. Report No.: ESA/P/WP.189.
19 Diggle GE. Thalidomide: 40 years on. Int J Clin Pract 2001;55(9):627‐631.
20 General considerations for clinical trials. London: The European Agency for the Evaluation of Medicinal Products (EMEA); 1997. Report No.: CPMP/ICH/291/95.
21 Milestones in womenʹs health. Rockville (USA): Food and Drug Administration; 2001. Available from: http://www.fda.gov/womens/milesbro.html (accessed 8 July 2004).
22 What is a rare disease? Paris: European Organization for Rare Diseases (EURORDIS); 2004. Available from: http://www.eurordis.org/article.php3?id_article=252 (accessed August 31, 2004).
23 Orphan Drug Act. Public Law, 97‐141. Website: http://www.fda.gov/orphan/oda (accessed 31 August 2004).
24 Report on the first 3‐year mandate of the Committee for Orphan Medicinal Products (COMP). (April 2000‐April 2003). London: European Agency for the Evaluation of Medicinal Products (EMEA); 2003. Available from: www.emea.eu.int/pdfs/human/COMP/91180en.pdf

8. New approaches to promoting innovation
99
8. New approaches to promoting innovation
This chapter addresses current concerns about potential barriers to pharmaceutical innovation in Europe. A pharmaceutical gap can occur when market forces fail to meet public health needs. This is the situation with neglected diseases such as TB, malaria, trypanosomiasis (sleeping sickness) and other tropical infectious diseases. One response to this problem has been the establishment of public‐private partnerships (PPPs) for product development. These relatively new organizations are seen to be part of the solution to filling the translational research gap. Section 8.1 reviews the current outlook for PPPs and suggests what needs to be done to ensure their success. Reimbursement authorities set the prices that are paid by health authorities in Europe. The five major European pharmaceutical markets (France, Germany, Italy, Spain and the UK) retain unique approaches to setting reimbursement prices on pharmaceuticals. Country‐specific systems based on differing sets of authorities, negotiation processes, and fundamental principles (including pharmaco‐economics) complicate the approval of pharmaceutical prices in these countries. The process of setting prices is unpredictable and leads to uncertainty for the innovating companies. Section 8.2 outlines one of several possible solutions to this: a system in which prices would be set on the basis of the clinical efficacy of the products and the per capita Gross National Income (GNI). Section 8.3 reviews potential barriers to innovation and suggests solutions to overcoming these barriers. A consensus appears to be developing between regulators (including both the European Medicines Agency (EMEA) and the U.S. Food and Drug Administration (FDA)) and the pharmaceutical industry, and academics as to the nature of the problem and the possible solutions. Section 8.4 addresses the comparative effectiveness of medicines and the need for “head‐to‐head” comparative trials. This trend of moving away from placebo‐controlled trials is occurring for ethical and practical reasons. Regulators and reimbursement authorities are demanding such information to help them make difficult decisions. Alternative approaches to generating such information from large databases are discussed in this section. Finally, Section 8.5 highlights a proposal for an EU Technical Platform for Innovative Medicines designed to enhance and accelerate the medicines development process (see Appendix 8.5.1).
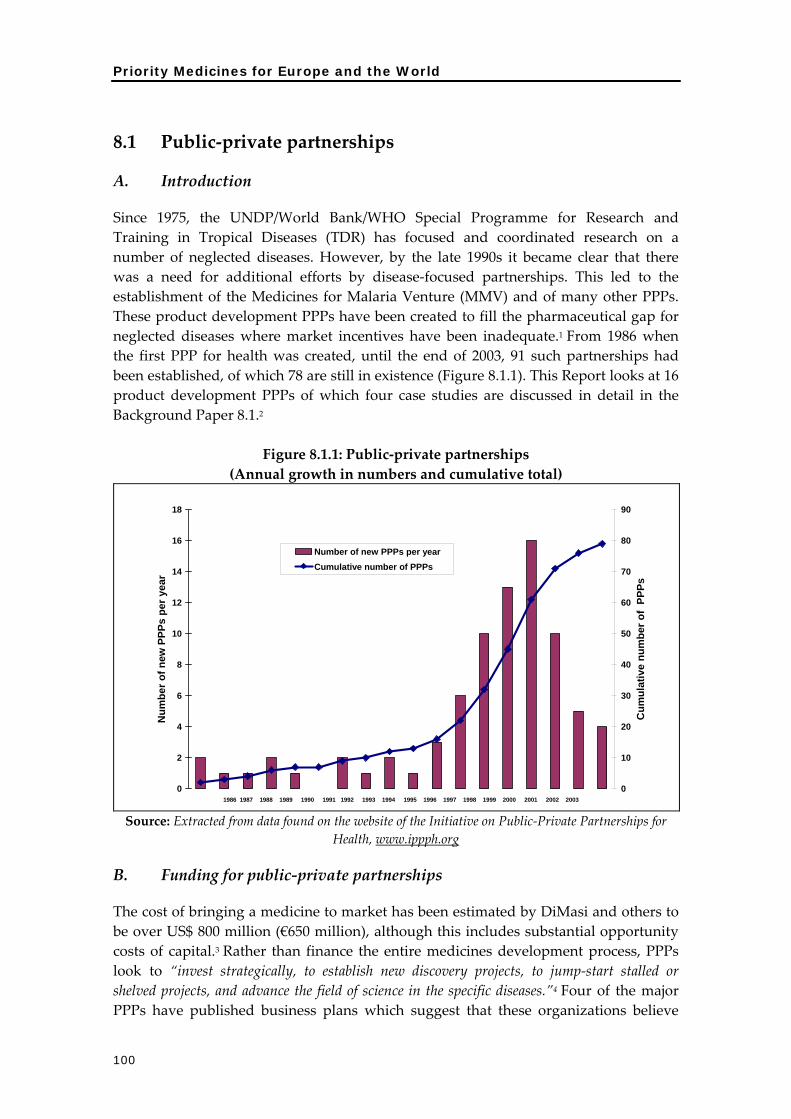
Priority Medicines for Europe and the World
100
8.1 Public‐private partnerships
A. Introduction
Since 1975, the UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR) has focused and coordinated research on a number of neglected diseases. However, by the late 1990s it became clear that there was a need for additional efforts by disease‐focused partnerships. This led to the establishment of the Medicines for Malaria Venture (MMV) and of many other PPPs. These product development PPPs have been created to fill the pharmaceutical gap for neglected diseases where market incentives have been inadequate.1 From 1986 when the first PPP for health was created, until the end of 2003, 91 such partnerships had been established, of which 78 are still in existence (Figure 8.1.1). This Report looks at 16 product development PPPs of which four case studies are discussed in detail in the Background Paper 8.1.2
Figure 8.1.1: Public‐private partnerships (Annual growth in numbers and cumulative total)
0
2
4
6
8
10
12
14
16
18
Num
ber o
f new
PPP
s pe
r yea
r
0
10
20
30
40
50
60
70
80
90
Cum
ulat
ive
num
ber o
f PP
Ps
Number of new PPPs per yearCumulative number of PPPs
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
Source: Extracted from data found on the website of the Initiative on Public‐Private Partnerships for Health, www.ippph.org
B. Funding for public‐private partnerships
The cost of bringing a medicine to market has been estimated by DiMasi and others to be over US$ 800 million (€650 million), although this includes substantial opportunity costs of capital.3 Rather than finance the entire medicines development process, PPPs look to “invest strategically, to establish new discovery projects, to jump‐start stalled or shelved projects, and advance the field of science in the specific diseases.”4 Four of the major PPPs have published business plans which suggest that these organizations believe

8. New approaches to promoting innovation
101
that they can produce medicines at considerably lower costs than those estimated by DiMasi et al., using industry data (See Table 8.1.1 below). Much of these reduced costs are expected to arise from in‐kind donations from the pharmaceutical industry or other institutions. Table 8.1.1 includes information on the International AIDS Vaccine Initiative (IAVI). However, this PPP must be considered as a special case since the processes followed for developing and testing a vaccine are very different to those involved in developing a medicine.
Table 8.1.1: Summary of product development costs (millions of US$)
by stage of the process MMV TB
Alliance Drugs for Neglected Diseases Initiative (DNDi)
IAVI Study by DiMasi et al.
study
Total discovery and preclinical
8.33 18.6 16.2 20.0 26.0
Phase I 1.58 0.6 7.0 15.2 Phase II 1.15 3.4 23.5 Phase III 9.5 22.6 30.0 86.3 Total clinical 12.23 26.6 24.2 37.0 125.0 Other 1.5 8.0 50.0 5.2
Source: Table 8.1.3 Background Document The product development PPPs have reported their pledged and required funding up to 2007, as shown in Table 8.1.2. This demonstrates a substantial shortfall in committed funds.
Table 8.1.2: Summary of funding pledged and funding needed for product development (US$ millions)
Cumulative funding pledged to
2007
PPP estimate of cumulative required resources to 2007
Implied shortfall
IAVI 174 1036 862
TB ALLIANCE 35.75 249 213
DNDi 0 255 255
MMV 97 152 83
TOTAL 306.75 1692 1413
Source: Table 8.1.5 Background Document

Priority Medicines for Europe and the World
102
At present, the vast majority of funding for product development PPPs has been provided by major philanthropic organizations such as the Bill and Melinda Gates Foundation and the Rockefeller Foundation. European governments and the USA are the second largest group of donors. Multilateral donors such as the EU, UN organizations and the World Bank have provided relatively small amounts. The international NGO Médecins Sans Frontières, has provided a five‐year grant to establish and fund the new Drugs for Neglected Diseases Initiative (DNDi). Private sector organizations, including the major pharmaceutical companies, have made financial and in‐kind donations. However, at present there appears to be a substantial shortfall in the available funding. Until now, the EU and Member States have not provided substantial direct funding or other support to PPPs.
C. Outlook for public‐private partnerships
Product development PPPs are an innovative approach to addressing the global health care crisis in developing countries. The preventable loss of life and disability suffered by people in poor countries can no longer be ignored by countries that have sufficient funding and the human resources, technology and skills required to discover and develop medicines for orphan and neglected diseases. A review of the funding requirements and sources for the existing PPPs clearly demonstrates that the major funding source for PPPs are private foundations and governments. There is a lack of direct funding and support from the EU for PPPs. As a result, opportunities are lost within the EU by failing to participate in the work done by PPPs. New discoveries in basic science, R&D of medicines and technology in support of this research, as well as other valuable benefits are not being achieved. Elsewhere, academic institutions and private sector entities in the USA, the UK and other countries have benefitted from their support of PPPs. Such benefits could occur throughout Europe if the European Union provided support for PPPs. An additional concern (see Background Chapter 8.1) is that the EU funding process is not “user‐friendly” and may actively discourage PPPs. Modifications to the current application process are needed. The EU has acknowledged the importance of neglected diseases in the Sixth Framework Programme by supporting funding for projects related to these diseases. However, at present the EU does not have a mechanism to support translational and preclinical research by PPPs. The establishment in 2003 of the European and Developing Countries Clinical Trials Partnership (EDCTP) is a substantial commitment by the EU to building capacity for the clinical trial phase of the medicines development process. The EDCTP is geared to provide services for the clinical Phases II and III of the medicines development process, and by its very existence assumes that there are sufficient chemical entities to be tested. However, the pipelines for TB and malaria medicines, as well as medicines for very neglected diseases, are far from robust. Much financial and technical support is needed to bring entities from the research and development (R&D) stage to the point where

8. New approaches to promoting innovation
103
clinical trials are needed. If the chemical entities are not available to be tested in clinical trials, the EDCTP will be underutilized. One other important European initiative to be mentioned in the context of finding new innovative approaches in drug discovery and development where public and private activities meet, is the New Safe Medicines Faster Initiative of the European Federation for Pharmaceutical Sciences (EUFEPS). This initiative has brought together a variety of industrial, academic and regulatory groups in the pharmaceutical sciences in Europe in order to carry out more research into better models for PPIs that could be applied to all stages of the drug development process, and to fuel other programmes to address the pressing need for new drugs.
D. Conclusions
The health needs of developing countries are an issue of global public health importance that calls for the full commitment and involvement of all governments. The private sector cannot be expected to provide solutions for which it will not receive a return commensurate with its investment. PPPs have done an impressive job of raising the level of awareness of the health disparities between developed and developing countries. They marshal financial and non‐financial support among the private sector for the development of products to address these diseases. Innovative and creative systems and processes for medicines development have been introduced outside the traditional for‐profit pharmaceutical model. It remains to be seen whether this innovative approach to medicines development will succeed. Product development PPPs have to contend with the risks inherent in the costly and time‐consuming process of medicines development. While PPPs are optimistic that sufficient funding will be available as medicine candidates move through each stage of the development process, it remains to be seen whether the optimism is justified. The role to date of the EU in supporting PPPs is modest. The establishment of the EDCTP supports the clinical trials process but assumes that sufficient new chemical entities exist in the pipeline to test in clinical trials. However, the pipeline for neglected diseases is far from robust, with the possible exception of HIV/AIDS medicines. It is recommended that the EU should support the translational and preclinical phases of R&D for medicines to treat neglected diseases.
8.2 Determining value for innovation and setting prices
A. Introduction
This section of the Report is concerned with the valuation of future medicines. It shows how governments in countries of variable wealth can encourage innovation through the appropriate pricing of new medicines and by having national reimbursement authorities proactively commit to rewarding genuine medical advances. The price that

Priority Medicines for Europe and the World
104
payers are willing to pay for new medicines has a direct effect on which medicines are produced by innovator companies. In Europe, all governments control prices in different ways. For companies, this final critical stage remains unpredictable. They do not know how long it will take for a decision, what the final price will be and whether additional information or studies will be required. The process itself is often referred to as a ʺblack box.ʺ5 This results in an unpredictable lottery for companies who have brought a product to market through a series of regulatory hurdles and still do not know what the final reimbursed price will be. One possible solution would be for reimbursement agencies and manufacturers to agree on the principles of valuation of future medicines in order to provide predictability for the process. By rewarding clinical performance and linking prices to national income levels, governments and insurers can encourage manufacturers to invest in the discovery of innovative medicines that address priority health care needs.
B. The international market for pharmaceutical products
The international market in which new medicines are developed has strict rules about intellectual property protection, quality, safety and efficacy.6 There is a high degree of harmonization of medicines regulation but not of national pricing policies, which are likely to be based on local factors, together with an overriding desire to contain costs.5 The initial discovery process for new medicines is demanding and involves a high failure rate.7 Companies, when they do produce a marketable product, aim to recoup the costs of all their failures and to meet expectations for high profits. The payers, which in European countries are primarily insurance organizations or reimbursement authorities, are primarily interested in controlling costs while maintaining access. While there is acceptance of the need to improve access to essential medicines in low‐income countries, the same urgency is not apparent for middle‐income countries, which often pay the same (or higher) prices as the richest and most developed nations.8 In effect, these countries are being asked to shoulder a high proportion of medicine development costs in relation to their ability to pay. Under the present system, they can only cope with this situation by limiting access, as there has been little prospect of differential pricing for middle‐income countries.
C. Differential pricing
Differential pricing occurs internationally for many products and is supported by both the World Trade Organization (WTO) and WHO in the case of essential medicines.9 Differential pricing is possible with pharmaceutical products because the marginal cost of manufacture is often much less than the average selling price. A number of pharmaceutical companies have made effective use of differential pricing for products such as vaccines, oral contraceptives, antimalarials and insulin. 10 In low‐income countries, these products sell for a fraction of the price in developed countries. Differential pricing of medicines has a wider application across low‐ and middle‐ and perhaps even high‐income countries, which vary substantially in their national measures of wealth. Applied properly, differential pricing should ensure that the

8. New approaches to promoting innovation
105
opportunity cost of purchasing medicines and investing in pharmaceutical R&D (through medicine purchasing and subsidization) is roughly equivalent across countries of variable wealth. 11 While improving the affordability of medicines in different countries, it is also a mechanism for maximizing the profit of manufacturers.12 Economic theory indicates that where the true marginal costs of a product are low, price discrimination will increase the total revenue of a company, so long as parallel trade can be minimized.12 A number of technical solutions have been proposed to limit pharmaceutical parallel trade, such as unique presentation and country‐specific labelling and packaging measures. 13 These are made possible by the regulatory requirements imposed on pharmaceutical manufacturers.
D. Spreading the burden of medicine development costs
Medicine development costs are high and companies have come to expect a relatively high rate of return to compensate for the R&D costs that are incurred early in the development cycle. However, it is unfair to expect these costs to be spread equally across countries of variable wealth. It is inevitable that high‐income countries will bear the majority of medicine development costs in an absolute sense. However, departments and agencies with responsibility for purchasing and subsidization of medicines view their activities as controlling budgets rather than promoting innovation for new medicines. As a consequence, they have developed a range of tools that are designed to limit their costs but not to encourage innovation. Budget control initiatives that have become popular include limited lists, generic substitution, reference pricing and the use of cost‐effectiveness analysis.5 However, it is a challenge for the new EU member countries to use these methods, as their funding base is relatively small and pharmaceutical companies appear reluctant to negotiate differential prices, even though the national income levels of these countries may be closer to low‐income countries than the highly developed industrialized nations.
E. Valuing new medicines
Pharmaco‐economics can act as a guide to pharmaceutical manufacturers by indicating at what price they can expect to sell future products and what prices payers should be prepared to pay. The guiding principles are to reward genuine innovation, while at the same time ensuring that new medicines remain affordable in countries of variable wealth. It is possible to combine the principles of pharmaco‐economic analysis and differential pricing to value future medicines. This approach indicates the extent to which low‐ and middle‐income countries should be expected to contribute to R&D through the prices they pay. A background paper outlines an extension of a published method in which cost‐effectiveness analysis is combined with a measure of national wealth to generate indicative prices at which a medicine might be considered to be cost‐effective.11 (See Appendix 8.2). The methodology is extended to demonstrate how manufacturers and governments can estimate how much countries should pay for future medicines that will offer significant new clinical benefits.

Priority Medicines for Europe and the World
106
F. Methods
This approach to valuing future medicines employs the established tools of evidence‐based medicine and clinical economics, and incorporates a measure of national wealth (in the form of Gross National Income (GNI) per capita). The World Bank has suggested that health care interventions may be considered cost‐effective if they buy a year of healthy life for less than the national average per capita GNI.14 The proposed approach described here estimates the benefit and monetary value of a new hypothetical medicine or regimen. The hypothetical medicine regimen and existing treatments are valued by comparison with a situation in which no effective treatment is available to treat the condition. These illustrate what price (through differential pricing) might be anticipated by manufacturers of new medicines that represent advances in the treatment of the two conditions of interest: depression and HIV/AIDS.
G. Results
HIV/AIDS treatment Using this method, the indicative ‘value for money’ price for the hypothetical new medicine regimen in Mali (per capita GNI 2003 US$290) is US$285 annually. By contrast, in the UK (per capita GNI 2003 US$28,350) the indicative price is US$27,847 annually. These results reveal the wide variations in prices of effective medicines that are justified by measures of performance and international variations in income. Figure 8.2.1: Indicative prices (on the vertical axis) in US$/annum of highly active
antiretrovirals (HAART) and a new hypothetical regimen in countries of variable wealth
0
5000
10000
15000
20000
25000
30000
267
294
441
487
607
763
855
993
1214
1637
1959
2125
2401
2557
2566
3477
3744
4921
6199
1088
1
1262
0
1562
7
1983
1
2278
3
2322
5
2607
6
Per capita GNI $US
Indi
cativ
e pr
ice
$US
Indicative price existing treatment Indicative price new drug
200 500 1000 2000 2500 5000 15000 20000 25000
United Kingdom
FranceItaly
Spain
Latvia
Slovenia
Czech Republic
Russian Fed.KazakhstanPhilippines
GeorgiaIndiaMali
200 500 1000 2000 2500 5000 15000 20000 25000

8. New approaches to promoting innovation
107
H. Indicative prices for a theoretical new medicine to treat depression
Depression is a major cause of lost DALYs but in some respects is more difficult than HIV/AIDS to characterize in a model because of the difficulty in quantifying ʺbenefit.ʺ In this model, a modest improvement in efficacy with a hypothetical new medicine is estimated in terms of days free of depression. Using this method the indicative ‘value for money’ price for the antidepressant in Mali (per capita GNI 2003 US$290) would be US$57 annually in contrast to the UK (per capita GNI 2003 US$28,350) where the indicative price would be US$5,614 annually. These prices may appear high but it must be remembered that these exercises are illustrative and the indicative price is very dependent on the assumed level of efficacy and the fraction of GNI per capita that is used in the threshold analysis.
Figure 8.2.2: Indicative prices (on the vertical axis) in US$/annum of existing
antidepressant treatment and a hypothetical new medicine with greater efficacy
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
0 5 10 15 20 25 30
Per capita GNI $US thousands
Indi
cativ
e pr
ice
$US
United Kingdom
France
Italy
Singapore
Spain
GreeceSloveniaCzech Republic
LatviaIndiaMali
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
0 5 10 15 20 25 30
United Kingdom
France
Italy
Singapore
Spain
GreeceSloveniaCzech Republic
LatviaIndiaMali
Indicative price existing treatment Indicative price new drug
I. Conclusion
These examples show that it is possible to incorporate measures of clinical performance and national wealth in determining indicative prices for pharmaceuticals. However, this does not mean that the indicative price is necessarily the ‘right’ price, the lowest possible price or an affordable price. There is also no guarantee that manufacturers will be interested in manufacturing products on this basis. However, this type of exercise can provide a framework by which reimbursement authorities can systematically ʺvalue innovation.ʺ For example, each country payment authority could proactively announce that they would be willing to pay Euros XXX per year for a new medicine that would prevent the pain and disability of osteoarthritis and reduce the need for joint replacement surgery by 30%.

Priority Medicines for Europe and the World
108
The realization of a more predictable system that encourages medicines development and achieves affordability of access in countries of variable wealth requires reconsideration of current policies towards parallel trade. Parallel imports tend to favour high‐income countries, which can benefit from the prices paid in lower‐income countries. It is recognized that this suggested solution is controversial since any inhibition of parallel trade conflicts with European law. This highlights the need for a wide debate on these issues. In the Background Chapter 8.2, a strong pharmaco‐economic case is made that reimbursement and insurance authorities could proactively determine what price they would be willing to pay for a new product, based in part on the clinical efficacy of the new medicines. The pricing would relate to efficacy and GNI per capita. This would then mean that medicines in Europe would be priced according to their clinical value and the ability of countries to pay. We would propose that such a model be developed. If correctly used, this proactive pricing scheme would mean that the parallel market in pharmaceuticals would need to be prevented. While Europe is meant to be a common market, in reality, because national authorities set medicine prices, pharmaceuticals cannot be considered to be ʺproducts moving freely in international trade.ʺ Since pharmaceuticals are also regulated by national medicine regulatory authorities, it would be perfectly possible to segment the pharmaceutical market so that pricing was set on the basis of national income and therapeutic efficacy. If rewarding innovation is one of the intended effects of reimbursement policies then setting prices related to the level of clinical efficacy and the national wealth as measured by GNI per capita would be a logical and transparent approach. Many reviewers have commented on this proposal. Some have said that the model is ʺtheoretically interestingʺ but impractical. Others have suggested that there is such a strong commitment to the ideal of a European common market that any restrictions on parallel trade would be unacceptable. Others have commented that technical requirements for such an approach would be impossible to undertake proactively. Such a variety of responses suggests that this topic should be researched and debated.
J. Postscript
After this chapter was written, the issue of determining value for innovation and setting prices was raised at the European Parliament in October 2004 during the confirmation hearings for commissioners designate. The Commissioner designate for Enterprise and Industry, Günter Verheugen, was asked what, in his view, would be the greatest challenges in the field of medicinal products over the next five years.15 In his response, Mr Verheugen said (bold added for emphasis):
ʺIndustrial policy in the pharmaceuticals sector aims to maintain a balance that will guarantee a high level of protection for public health while promoting the competitiveness and dynamism of the pharmaceutical industry – including the biotechnology sector – in order to ensure that the pharmaceuticals sector in

8. New approaches to promoting innovation
109
Europe makes a significant contribution to the achievement of the Lisbon objectives. The sector is important as a source of high‐quality jobs, an investor in R&D, and a significant positive contributor to the EU’s trade balance. This position is being eroded, however, since the sector in Europe is losing ground to its competitors at world level.ʺ ʺAs for the economic aspects of medicinal products, the Commission could, following deliberations on pricing and reimbursement methods, play a part in developing alternative approaches aimed at promoting innovation and making it financially rewarding. Similarly, questions concerning national procedures for determining the therapeutic value of new medicinal products must also be tackled. The Commission will also have to ensure that it has a means of regularly evaluating the impact of these measures. Following an initiative by the high‐level group on innovation and provision of medicines (G10 Medicines), the Commission has developed competitiveness indicators, which will be updated annually and form the basis for a report to Parliament and the Council of Ministers. Other initiatives will concern information aspects with a view to placing the patient at the centre of policy on medicinal products.ʺ ʺThe chief legislative challenges will be to introduce the measures needed to permit the correct and efficient application of the new legislation on medicinal products adopted by the European Parliament and the Council in March 2004. There will be other initiatives to complete this legislative framework, particularly in the field of paediatric medicinal products and in connection with new types of treatment.ʺ
This response to a specific question would tend to indicate that pricing and reimbursement issues in relation to promoting innovation may be open for discussion.
8.3 Barriers to innovation in pharmaceutical research and development
The impetus for this Project arose from the various reports issued between 2000 and 2003 (Appendix 2). Coincidentally, three papers were published in March 2004 by the EMEA and FDA (Appendix 8.3) and by Michael Rawlins in Nature (Appendix 8.3.4). In addition, a paper prepared by individuals working in the pharmaceutical industry was prepared for this Report (Annex 8.3). These papers all maintained that the present costs and time spent in developing new medicines were unsustainable. The authors suggested similar but slightly different solutions to the main barriers with the EMEA, FDA and Rawlins papers focusing on regulatory obstacles, while the industry paper was broader. In recent years, the cost16 and duration of medicines development have increased and this has been coupled with low output of innovative medicines from the pharmaceutical pipeline.17 Recent estimates suggest that it costs nearly US$ 1 billion for

Priority Medicines for Europe and the World
110
each new chemical entity and takes 10 to 15 years on average from discovery to market authorization. While there may be many projects in early development stages, the fact remains that little of this potential innovation is being translated into market approvals. For some diseases, there remains an inadequate understanding of basic science, and potential targets for medicines development have not been identified.
Regulatory barriers
All authors agreed that every aspect of the regulatory process should be re‐examined and that the evidence base for regulatory practices should be critically analysed using modern methodologies. In particular, this includes preclinical regulatory ʺrituals.ʺ For clinical research, there is a suggestion from Rawlins that alternatives to randomized controlled trials should be investigated. Under some circumstances, he suggests, historical controls could be utilized and alternative analytical statistical techniques using Bayesian statistics could be used to analyse data. A key recommendation of all the authors is the need to improve communication between industry, physicians and regulators in the regulatory process. What is particularly striking about the EMEA, Rawlins and FDA papers are two significant omissions. Apart from the industry paper, none of the three regulatory papers mention any role for patients in the regulatory process. They are referred to as beneficiaries of the process but never as contributors to the decision‐making. This is surprising as patients have been very influential in the rapid authorization of AIDS medicines and in the orphan drug movement. It is not clear how patients could be most effectively involved in promoting innovation and removing barriers but this is clearly an area for research. The second striking omission is the absence of any discussion of post‐marketing surveillance as a critical component of the overall process. The FDA diagram of the stages of the medicine development process omits Phase IV from its description of all of the steps in medicine development (see Figure 8.3.1 in Background Chapter 8.3).
Medicines development process
Preclinical studies: Most of the tools used for toxicology and human safety testing are decades old and may fail to predict the specific safety problem that ultimately halts development or that requires post authorization withdrawal. Each aspect of preclinical safety studies (pharmacological ‘screening’ for unintended effects; pharmacokinetic investigations in species used for toxicology testing; single‐ and repeat‐dose toxicity testing; and special toxicology testing (such as mutagenicity) has not been rigorously tested by a robust analysis of its predictive power. The FDA has suggested that scientists working within regulatory agencies have a wealth of application data available to undertake such a critical review.

8. New approaches to promoting innovation
111
More generally, there are too few analytic tools (e.g., analytical devices, assay systems, surrogate markers and cell culture methods) to assist in providing medicine safety and effectiveness studies more quickly, with more certainty, and at lower cost. Key enabling technologies involving the use of animals and the use of human tissue in biomedical research are subject to complex regulation. Any increase in complexity of regulation or indeed blocking of access to these technologies by public opinion pressures has the potential to seriously disrupt basic and applied biomedical research. Clinical development: Regulatory authorities are becoming more risk‐averse. This lack of flexibility only entrenches the existing regulatory requirements and perceptions, and often results in the need for expanded studies to quantify potential adverse events. Many requirements of medicines regulatory authorities are based on the opinion of experts, rather than on a robust body of evidence to support the continuing inclusion of each measure as a regulatory requirement. Randomized, controlled, blinded, parallel‐group clinical trials are not the only possible approach to investigating the safety and efficacy of a new medicine. It may be that new methodological research to critically evaluate alternative approaches, including actual experiments comparing novel and traditional (RCT) designs, will find that medicines development can be made more efficient without sacrificing safety and efficacy. Such alternative approaches have been successfully used for high risk diseases such as cancer or AIDS where accepting results from limited size studies combined with post‐authorization monitoring have allowed products to come to market far more quickly than by conventional approaches. The role of patient groups in the AIDS example cannot be underestimated. Indeed, patients and patients’ organizations could be equal stakeholders participating in decision‐making processes that occur in all aspects of pharmaceutical innovation including: clinical trials design; regulatory processes; treatment guidelines; marketing and pricing of medications. There is often poor communication between the industry, physicians, and regulators during medicines development. This results in requests for additional data and regulatory questions following submission, and in turn these requests lead to increasing unpredictability of outcomes and delays in the marketing authorization process. Payers do not interact with the industry at an early enough stage in the development process. Post‐marketing studies: In the four papers mentioned above, none deals with the important role of post‐marketing surveillance. In practice, there is relatively scant attention paid to Phase IV post‐marketing studies or systems. Computer‐based registries of patients and their clinical outcomes do not presently have sufficient data on both incidence of exposure to the medicine and of adverse events in long‐term, post‐marketing studies of the risks and benefits of medicines. European countries with their national reimbursement systems are in a strong position to develop such integrated systems while preserving patient confidentiality.

Priority Medicines for Europe and the World
112
Reimbursement mechanisms: A lack of predictability about the timing and level of reimbursement decisions leads to uncertainty among stakeholders. In Europe, each national reimbursement system is primarily responsible for cost containment. This is achieved by setting prices at a level that may not fully reward innovation and sometimes by delaying decisions about reimbursement. These problems lead to companies choosing to launch their products in the USA which, at present, has no such single national system or government‐based price control system. Within its Sixth Framework Programme, the European Commission has recently called for research proposals that include new approaches for accelerated development of new, safe and more effective medicines. Bottlenecks and barriers in the current medicines development process are to be identified and solutions elaborated to overcome them. The project is expected to involve a range of stakeholders, such as academia, clinicians, patient organizations, large and small industry, regulatory and ethics specialists (Appendix 8.3.3). As part of this call for proposals, it is recommended that the EU should create and support a broad research agenda, so that every requirement within the medicines development process, whether clinical or preclinical, is questioned for its regulatory relevance, costing and predictive value. The involvement of the EMEA and the various European national regulatory agencies and their scientists appears to be critical to the success of this key initiative.
8.4 Comparative effectiveness of medicines and use of “head‐to‐head” comparative trials
Prescription medicines can be very expensive and their cost may prevent access for everyone, although governments of most developed countries have subsidy systems to achieve equity of access to pharmaceuticals. Nevertheless, for most of these medications, we know little about whether or not a given medication is better value for the money than alternatives. This knowledge gap exists because most medicine regulatory authorities do not examine ʺvalue for moneyʺ. However, cost‐effectiveness is very important and many countries do incorporate some sort of economic evidence into their reimbursement schemes (Background Chapter 8.2).18 The effectiveness of a medicine beyond comparison to a placebo is not often ascertained because such a scientific evaluation is often only possible with new trials. In contrast, a comparative benefit or “non‐inferiority” trial occurs when a new medicine is tested against a standard treatment with similar efficacy, and the trial must be designed to show that the standard therapy (control) has some benefit and that the new treatment is equivalent to, or not worse than, the standard therapy.19 Active comparator studies are needed because a product cannot be evaluated and approved if efficacy is less than an existing standard therapy. Regulators do require such trials to be undertaken when existing therapies are well established and it would be unethical to conduct a placebo controlled trial.

8. New approaches to promoting innovation
113
To estimate comparative benefit between two medicines, large trials are needed, since there are often small differences between treatment outcomes when comparing the interventions.20 The industry is acting rationally in its reluctance to undertake routine comparative studies in the late stages of medicine development (i.e., Phase III) as these are both time‐consuming and expensive, although some registration authorities require this kind of study. More perhaps to the interests of the shareholders, the discovery that a new product, which has yet to establish a market, is no better than an older and cheaper one could have unfortunate commercial consequences.21 There are at least two alternatives to having either the industry or the government pay for comparative clinical trials. In one approach, private insurers and the government would set aside some fraction of their annual medicines spending to endow a new institute to provide an independent source of reputable research into comparative effectiveness and cost. Another approach relies on electronic prescription and medical databases to conduct Phase IV and/or pharmaco‐epidemiologic studies in place of randomized, controlled, comparative clinical trials. The European Commission is presently discussing so‐called “e‐prescribing” and other information technology (IT) approaches as part of its interest in the information society.22 The EU has a great comparative advantage over the USA in this, as this kind of electronic linkage of prescribers and medical records is still fragmented in the USA. The European Commission supports the use of an action plan on ʺelectronic healthʺ, addressing the crucial role of new technologies and new ways of delivering health care in improving access to, quality and effectiveness of care. This approach should be used as a way of creating post‐marketing ʺrandomized epidemiologyʺ studies to better understand comparative effectiveness and cost‐effectiveness.
8.5 Technology Platform for the Pharmaceutical Industry
Within the EU Commission there has been discussion of a Technology Platform created under the provisions on Treaty Article 171. A Technology Platform is expected to unite stakeholders around a common vision and approach for the development of the technologies and the mobilization of the necessary critical mass of research and innovation effort. The overall objective of the proposed Technology Platform for Innovative Medicines would be to enhance and accelerate the development process of medicines. This would be achieved by stimulating cooperation in R&D, in particular through reinforced PPPs, while at the same time strengthening the European science base and fostering economic growth in the pharmaceutical and biotechnology industry and fostering support for small and medium‐sized enterprises. Technology Platforms have been rarely used in the EUʹs history. Antibacterial resistance and pandemic influenza — the two priority diseases/conditions identified in this Report — may be suitable priorities around which to build a common strategy for the European pharmaceutical and biotechnology industry. Both of these pose a major

Priority Medicines for Europe and the World
114
threat to global public health. Addressing them successfully would require the involvement of every country in the EU. Individuals, doctors and pharmacists, national ministries, professional associations, universities, research institutions, regulators and the pharmaceutical industry would all have to work together to address the common threat. The proposed Technology Platform for Innovative Medicines could mobilize human and financial resources across all sectors to address these two critical problems, while promoting innovation in the European pharmaceutical industry.

8. New approaches to promoting innovation
115
References 1 Orbinski J. Market enticements are not enough. Bull World Health Organ 2001;79(8):776.
2 Kettler H, Towse A. Public private partnerships. Geneva: Commission on Macroeconomics and Health (CMH), World Health Organization; 2001. Report No.: WG2:21.
3 DiMasi, J, Hansen, R, Grabowski H. The price of innovation: new estimates of drug development costs. J Health Econ 2003;22:151‐185.
4 Kettler HE, Marjanovic S. Engaging biotechnology companies in the development of innovative solutions for diseases of poverty. Nat Rev Drug Discov 2004;3(2):171‐176.
5 Jacobzone S. Pharmaceutical policies in OECD countries: reconciling social and industrial goals, labour market and social policy ‐ Occasional Papers No. 40. Paris: Organisation for Economic Co‐operation and Development; 2000. Report No.: DEELSA/ELSA/WD(2000)1.
6 International Committee on Harmonization. Website: http://www.ich.org
7 Scherer FM. The pharmaceutical industry – prices and progress. N Engl J Med 2004;351(9):927‐932.
8 Freemantle N, Behmane D, de Joncheere K. Pricing and reimbursement of pharmaceuticals in the Baltic States. Lancet 2001;358(9278): 260.
9 World Health Organization and World Trade Organization Secretariats. Workshop on differential pricing and financing of essential drugs. April 8–11, 2001, Høsbjør, Norway. Geneva: World Health Organization; 2001. Available from: http://www.who.int/medicines/library/edm_general/who‐wtohosbjor/hosbjorexe‐eng.pdf
10 Creese A. Differential pricing and access to medicines: issues and options. Available from: http://www.who.int/medicines/organization/par/briefing/11diffpricing.ppt
11 Lopert R, Lang DL, Hill SR, Henry DA. Differential drug pricing – a role for cost‐effectiveness analysis? Lancet 2002;359(9323):2105‐2107.
12 Hammer PJ. Differential pricing of essential AIDS drugs: markets politics and public health. J Int Econ Law 2002;5(4):883‐912.
13 Mossialos E, Dukes G. Affordably priced new drugs for poor populations: approaches for a global solution. J Risk Saf Med 2001;16(1):1‐28.
14 Health, immunization and economic growth, vaccines are cost‐effective: a summary of recent research. Geneva: Global Alliance for Vaccines and Vaccination; 2000. Available from: http://www.vaccinealliance.org/txt/home/ General_Information/Immunization_informa/Economic_Impact/vacc_cost.php.
15 European Parliament Hearings. Answers to questionnaire for Commissioner Designate Mr Günter Verheugen (Enterprise and Industry) Part B – Specific questions. 2004. Available from: http://www.europarl.eu.int/hearings/commission/2004_comm/pdf/speca_verheugen_en.pdf
16 DiMasi JA, Hansen RW, Grabowski HG. The price of innovation: new estimates of drug development costs. J Health Econ 2003;22(2):151‐185.

Priority Medicines for Europe and the World
116
17 Aspden P, editor. Medical innovation in the changing healthcare marketplace:
Conference summary. Washington, D.C.: National Academy Press; 2002. Available from: http://www.nap.edu/catalog/10358.html (accessed 2 August 2004).
18 Birkett DJ, Mitchell AS, McManus P. A cost‐effectiveness approach to drug subsidy and pricing. Health Aff 2001;20(3):104‐114.
19 Rothman KJ. Placebo mania. BMJ 1996; 313(7048):3‐4.
20 Henry D, Hill S. Comparing treatments. BMJ 1995;310(6990):1279.
21 Davis BR et al. ALLHAT: setting the record straight. Ann Intern Med 2004;141(1);39‐46.
22 Communication from the Commission to the Council, the European Parliament, the Economic and Social Committee and the Committee of the Regions, eEurope 2005: an information society for all. Brussels: European Commission; 2002. Available from: http://europa.eu.int/information_society/eeurope/2002/news_library/documents/eeurope2005/eeurope2005_en.pdf (accessed 2 July 2004).

9. Conclusions and recommendations
117
9. Conclusions and recommendations
Introduction
The Priority Medicines for Europe and the World Project was established to determine priority needs for pharmaceutical innovation from a public health perspective and to make policy and research recommendations on these needs. Within this public health context, a key objective throughout has been the need to identify common areas of interest between Europe and the world as a whole, particularly in the area of discovering and developing new and improved medicines to combat diseases/conditions which pose a current or future threat to public health. At present, pharmaceutical research and development (R&D) is based on a market driven incentive system relying primarily on patents and protected pricing as a prime financing mechanism. As a result, the research agenda is driven towards areas that represent market prospects and leaves certain health needs unaddressed. This Report suggests approaches that can be used to fill the gaps that result from the current system. Since Europe can and should play a global leadership role in public health, the overall recommendations of this Report extend well beyond the specific needs of European citizens. This public health approach is consistent with Europe’s long tradition of social solidarity in which national health systems were established to create social safety nets for all citizens. In many developing countries, the poor are already increasingly affected by the chronic diseases that are widespread in Europe, including cardiovascular disease, diabetes, smoking‐related diseases and mental diseases such as depression. The recommendations presented in this Report are the outcome of a priority‐setting exercise involving multiple stakeholders. This exercise used three different prioritization methods. In similar exercises in future, it is recommended that multiple stakeholders should again be involved and that a combination of prioritization methods reflecting different perspectives be used to achieve a similar balanced and optimal result.
Major recommendations
This Report has tried to identify the ʺmain stakeholdersʺ for further action. However, in highlighting specific DGs, this does not exclude other branches of the Commission and certainly not EU Member States. Indeed, it is in this spirit of hoped‐for cooperation among many stakeholders that the bold vision of this Project must be realized.

Priority Medicines for Europe and the World
118
Antibacterial resistance
Antibacterial resistance is a major long‐term threat to public health both in Europe and worldwide. There is a risk that future generations will not be able to rely on the life‐saving benefits of antibacterials presently enjoyed. Control strategies are needed which encompass: Research and product development: New approaches are required for the prevention and treatment of bacterial infections, and support should be continued for research into new medicines. Economic incentives will be needed to address the kind of ʺmarket failureʺ which has arisen in Europe, where antibacterials are widely used and are relatively inexpensive. This contributes to the development of antibacterial resistance while providing insufficient financial return for manufacturers to invest in the development of new antibacterials. Patients, the public and industry all share a common interest in addressing this market failure.
• EU regulatory authorities should allow limited release of new products for the treatment of proven drug‐resistant organisms together with “value‐based ” pricing as this can provide a different kind of incentive for the industry to develop them (Member States, EMEA).
• The EU should promote research into the development of rapid diagnostic tools as this would help prevent the misuse of antibacterials by identifying at the outset which antibacterial is needed for treatment (DG Research, Member States).
• Targeted research into vaccines for specific infections may be a useful way to prevent the need for antibacterials and should be further supported by the EU Framework Programmes (DG Research, DG SANCO, Member States).
Surveillance: Effective surveillance of both antibacterial resistance and the use of antibacterial agents should be undertaken in Europe and worldwide.
• The new European Centre for Disease Control and Prevention should coordinate an EU‐wide surveillance system that would link antibacterial surveillance, monitoring of medicines use, and prescribing practices with the evaluation of interventions to prevent the emergence of antibacterial resistance. These interventions must include comprehensive education of medical students, doctors, and other health professionals and the public in the appropriate uses of antibacterials and the dangers associated with their misuse and overuse (DG SANCO).
Prevention: Prevention of communicable diseases and infection control is required to reduce the need for antibacterial agents (DG SANCO, Member States).

9. Conclusions and recommendations
119
International cooperation: Close cooperation between regions and countries is required because drug‐resistant organisms are ʺinternational travellersʺ (Member States, DG SANCO, DG Trade).
While these recommendations focus on antibacterial drugs, including those used to treat TB medicines, there is also a need to address the broader problem of antimicrobial resistance. In particular, resistance to antimalarials and HIV medicines is a major and growing problem in some countries. A similar combination of surveillance, prevention, R&D, and international cooperation will be required to address this threat.
Pandemic influenza
Pandemic influenza in the 21st century could be as devastating as the 1918‐1919 epidemic was to a world recovering from the First World War. However, much could and must be done to prepare for this potential disaster. Making effective plans to address the inevitable influenza pandemic will also help countries prepare systems to deal with other threats, such as bioterrorism. Action needed includes efforts to:
Support research on better short‐ and long‐term vaccines, adjuvants (chemicals which increase the effectiveness of vaccines) and delivery mechanisms, and on new and improved antiviral agents. This includes analysis of incentives to manufacturers, as development of new anti‐influenza medicines is at present not economically attractive (DG Research, DG SANCO).
Ensure an increase in the uptake of existing vaccines in order to stimulate the market, build production capacity and provide annual immunity for all European citizens. Such a high level of immunity may reduce the severity of the pandemic and benefit European citizens (Member States, DG SANCO).
Continue surveillance systems in Europe through the new European Centre for Disease Control and Prevention, and define the burden of disease in high‐risk groups, including the elderly, pregnant women and children (DG SANCO).
Conduct multi‐country trials to better define the role of antiviral agents in reducing disease transmission, severe illness and mortality. (DG Research)
Investigate through multi‐country epidemiological studies the role of other existing medicines in reducing (co)morbidity and mortality (DG Research).
Address liability, safety and regulatory issues associated with the production of a new vaccine under pandemic emergency situations (EMEA).
Investigate the establishment of national stockpiles of antiviral agents to manage outbreaks (Member States).

Priority Medicines for Europe and the World
120
Smoking and smoking cessation
In formulating the overall recommendations for this Report, consideration was given to the overwhelming evidence regarding the burdens of respiratory and cardiovascular disease that are attributable to smoking. Rates of smoking are particularly high in the new EU Member States as well as in many transitional and developing countries. While recognizing that the most effective response is the development and implementation of comprehensive and vigorous anti‐smoking policies, to be pursued throughout Europe and the world, the Report also notes the evidence regarding the variable efficacy of some pharmacological aids to smoking cessation (e.g., nicotine replacement treatments and antidepressants). Some of these treatments have modest efficacy and some have limiting side‐effects.
• The EU could make a considerable contribution in this field by encouraging the development and testing of new compounds for treatment of smoking cessation (DG Research).
Promoting innovation through pricing and regulatory reforms
Efforts to shorten the medicine development process without compromising patient safety would greatly assist in promoting pharmaceutical innovation.
• The EU should create and support a broad research agenda through which the EMEA, the national regulatory authorities, scientists, industry and the public would critically review the regulatory requirements within the medicine development process – both clinical and preclinical ‐ for their relevance, costing, and predictive value (DG Research and EMEA).
Health authorities are responsible for medicines reimbursement decisions that aim to ensure quality treatment for all patients, while reconciling this with budgetary constraints. This Report recognizes that novel approaches need to be reviewed against the background of the EU common market and the EU G‐10 initiative.
• Health and reimbursement authorities and manufacturers should agree on general principles for the valuation of future medicines (Member States and DG Research).
• The EU Commission and national authorities should support a research agenda
on the various methods of rewarding clinical performance and linking prices to national income levels. The Report maintains that these will help encourage industry to invest in the discovery of innovative medicines that address priority health care needs (DG Research).

9. Conclusions and recommendations
121
To support the development of pharmaceutical innovation, there is a need to establish a more attractive basic research environment and to create long‐term financial incentives for researchers in an effort to encourage high‐quality research in basic biomedical research.
• The EU and Member States should support the further strengthening of capacity in preclinical research to bridge the continuing gap that exists for various neglected diseases between the development of promising medicine leads and their entry into clinical trials (DG Enterprise, Member States).
• The EU should continue to support the existing translational research on diagnostics, vaccines and pharmaceuticals that is presently being undertaken by small and medium‐sized enterprises (DG Enterprise).
Detailed recommendations
List of priority diseases/conditions requiring priority medicines
The following diseases/conditions have been identified by the priority‐setting exercise in this Report. The first three items on this Preliminary List are discussed above. The remaining conditions are discussed in sections on specific conditions (ʺPharmaceutical gapsʺ) and other sections that are based on broader issues.
Infections due to antibacterial resistance Pandemic influenza Smoking cessation Cardiovascular disease (secondary prevention) Diabetes Cancer Acute stroke HIV/AIDS Tuberculosis Neglected diseases Malaria Alzheimer disease Osteoarthritis Chronic obstructive pulmonary disease Alcohol use disorders: alcoholic liver diseases and alcohol dependency Depression in the elderly and adolescents Postpartum haemorrhage

Priority Medicines for Europe and the World
122
Pharmaceutical gaps
The methodology of the Report is designed to identify pharmaceutical gaps, that is, those diseases of public health importance for which pharmaceutical treatments either do not exist (lack of basic scientific knowledge or market failure) or are inadequate (lack of efficacy or safety concerns or because the delivery mechanism or formulation is not appropriate for the target patient group). For some diseases, the biology is well understood and there are many people willing and able to pay for medicines. For these diseases, there are likely to be a range of highly effective medicines available. Peptic ulcer, cardiovascular disease, HIV infections, diabetes and depression in adults are in this category. For other diseases, there is a strong demand and willingness to pay, but effective medicines are not available because the biology is not well understood. This category includes diseases such as Alzheimer disease, osteoarthritis, certain cancers, depression in the elderly and children, and acute stroke. Another category of diseases are those where the biology is well understood but there is a limited market for the products. This category includes malaria, tuberculosis, trypanosomiasis and leishmaniasis. A fourth group of diseases are those where the biology is complex and there is a limited willingness to pay for the new medicine. This group includes orphan diseases and some neglected diseases such as Buruli ulcer. It also includes a number of preventable diseases such as chronic obstructive pulmonary disease (COPD) and alcoholic liver disease — diseases which suffer from a public perception that because they are avoidable by changes in behaviour and lifestyle they are less worthy of support. Although this categorization has limitations, it is a useful indicator of future investment needs. Where the market is strong and the problem is poor understanding of the basic biology, investment in basic research and in facilitating innovation by the pharmaceutical industry will be needed. Where the biology is well understood but the market is weak, public support for translational research — possibly through product development public‐private partnerships (PPPs) and other not‐for‐profit product development initiatives — will be the preferred solution. Where the biology is not well understood and there is also a weak market, then biological research can be supported while market incentives are created for the pharmaceutical industry, through reducing barriers to innovation and through improving reimbursement rewards. Cardiovascular disease (secondary prevention): In general, there is an absence of ʺuser‐friendlyʺ formulations to ensure that high‐risk patients receive optimal therapy. The Report recommends research on all aspects of the development of fixed‐dose combinations (FDCs) for such patients (DG SANCO, DG Research, EMEA).
9. Conclusions and recommendations
123
Diabetes: The pharmaceutical industry considers development of effective diabetes medications as a major goal, but there is still a need for oral agents to act in a more efficient manner within the body (i.e., faster absorption by the body, action to control blood glucose over a longer time period, fewer side‐effects, paediatric formulations). The EU should create an infrastructure to facilitate diabetes clinical trials, in particular comparative clinical “head‐to‐head” trials to compare efficacy, side‐effects and cost‐effectiveness using full pharmaco‐economic analyses (DG Research, DG SANCO). Cancer: Both the public sector and the pharmaceutical industry have invested heavily in finding new pharmaceutical treatment options for cancer. However, many cancers are still resistant to treatment and the search for effective medicines is ongoing. The EU should expand its capacity (infrastructure and human resources) and strengthen coordination to conduct comparative Phase II/III clinical trials and continue to invest in basic research into cancer biology (DG Research). Acute stroke: A major basic and clinical research effort is required as the current treatment of acute stroke is unsatisfactory. Most agents are not effective and they are associated with an increased risk of adverse events (DG Research, DG SANCO). Tuberculosis: Diagnosing TB with the existing tools is a cumbersome, expensive and sometimes unsuccessful task. The EU should support research on diagnostics and vaccines as well as the pharmaceutical translational research presently being undertaken by product development PPPs and by small and medium‐sized enterprises. Gaps in the regulatory process for new TB medicines can be addressed by joint negotiation of a global standard for regulatory approval of new TB medicines, institution of an automatic fast‐track process for new TB medicines, and regulatory approval of surrogate markers (when available) to support medicine registration (DG Enterprise, EMEA, DG Research). Depression in the elderly and adolescents: The biology of depression and its treatments are poorly understood in these groups. Antidepressants have been reported as efficacious in adults but they have high levels of side‐effects. Lack of efficacy data and a growing number of medicine‐related suicides preclude their use in young people. Recommendations for a publicly funded research agenda include efforts to improve the understanding of the biology of depression and its treatments and to initiate comparative studies of existing therapies (DG Research, EMEA, DG SANCO). Osteoarthritis: Public funding of research into new diagnostics, biomarkers and imaging technology is needed for the management of this debilitating condition. Biomarkers are an essential area of research since they will help the medical community to determine who is likely to get arthritis, the severity and progression of disease, and the response to medicines (DG Research).

Priority Medicines for Europe and the World
124
Alzheimer disease: Public funds must be directed toward finding more sensitive, reliable and valid instruments for detecting changes in normal aging and the onset of early Alzheimer disease. Surrogate markers are needed as therapeutic endpoints remain a major barrier in the clinical development of efficacious medicines to treat this disease (DG Research, Member States). Chronic obstructive pulmonary disease (COPD): The overriding imperative in developing countries and in the expanded EU should be to reduce the prevalence and incidence of smoking. The outlook is poor in the short‐ and medium‐term for development of new therapies to treat lung inflammation or reverse COPD. A major need is for translational research to convert basic science advances into products that can be used in clinical trials. It is recommended that the existing infrastructure of the Sixth Framework Programme Global Allergy and Asthma European Network should be expanded to create an EU‐wide consortium to study COPD (DG Research, DG SANCO). Alcoholic liver disease: All alcoholic liver diseases are preventable with appropriate public health responses involving behavioural and lifestyle changes, including pharmaceutical approaches to combat alcohol addiction. As in the case of COPD, the outlook is poor in the short‐ and medium‐term for development of new therapies to treat liver fibrosis and other diseases/conditions related to alcohol abuse. The major need is for translational research support to convert basic science advances into products that can be used in clinical trials (DG Research, DG SANCO).
Therapeutic improvement through improved pharmaceutical delivery mechanisms
Two main conclusions arise from a review of the existing state of the art of medicine delivery mechanisms: first, there is a wide range of existing off‐patent technologies that are underutilized; second, the advent of new biotechnology‐derived protein/DNA‐based medicines requires investment in better delivery technologies, particularly those that can withstand extremes of climate.
Fixed‐dose combination products
Fixed‐dose combinations (FDCs) could provide an important approach to the management of both chronic and acute diseases. Their application needs to be carefully analysed, taking into account the past problems associated with FDCs.
• Three areas of research needed for product formulation are: the possible use of a cardiovascular FDC for the secondary prevention of heart attack and stroke; the use of FDCs of antiretroviral medicines for the treatment of HIV/AIDS in adults, pregnant women and children; and the development of FDCs of second‐line TB medicines for the treatment of multidrug‐resistant TB (DG Research, DG Enterprise).

9. Conclusions and recommendations
125
• Although there are pharmacological, regulatory and intellectual property/legal barriers to the widespread use of FDCs, these barriers can be overcome with a comprehensive strategy and cooperation between and among the private and public sectors (DG SANCO, DG Enterprise, EMEA).
• It is recommended that the EU sponsor one or more FDC Centres of Excellence which would act as “clearing houses” for information about FDC therapy, coordinate field studies of FDCs, and assemble and maintain the best evidence on their development, as well as on regulatory and legal issues (DG Research).
Heat‐stable formulations
Heat‐stable formulations are required so that medicines used in hot and humid conditions maintain their required potency.
• Research is needed to develop a heat‐stable insulin, available for use in developing countries which lack a regular system of refrigeration. This would be a major public health advance, and would also provide important advantages for European patients who travel, even within Europe (DG SANCO, DG Enterprise, DG Research).
• In order to reduce postpartum haemorrhage and maternal mortality throughout the world, the development of a heat‐stable oxytocin that can be delivered through simple injection devices would lead to important public health gains (DG Enterprise, DG Research).
Special groups
The elderly
Medicines development for the elderly must also be improved. The altered body functions in the elderly (e.g. changing body composition and liver metabolism) may require adapted dosages. Appropriate dosing is the key to successful medicines development and dosing in the elderly is one Achilles heel of medicines innovation.
• Specifically, there is a need for public funding to provide therapeutic formulations tailored to the special needs of the elderly in order to improve adherence, prevent the underuse of medicines and provide the best possible care (DG Research, EMEA).
Women
Women suffer from some common conditions more frequently than men, but women are often still excluded from clinical trials and other types of medical research.
• Public‐funded research is needed on the treatment of conditions or diseases
uniquely affecting women.

Priority Medicines for Europe and the World
126
• The individual research programmes will vary according to the specific problem. For reproduction control and subfertility, basic and clinical research will probably be the priorities. For pregnancy and lactation (including birth defects), the creation and analysis of exposure and defect registers using pharmaco‐epidemiological approaches are likely to be the methods of choice.
Children
To improve medicines development for children, there is a need to invest more in basic paediatric research, to increase the participation of children in clinical trials, and to reverse the underfunding of research on children‐specific medicine formulations. There is also a need for more information on the safety and efficacy of medication use in children, especially for mental disorders, which account for a high burden of disease (for example, depression, anxiety disorders).
• Specifically, there is an urgent need to develop paediatric formulations of antiretroviral medicines, including FDCs for children (DG Research, EMEA).
Neglected diseases
A clear case has been made in this Report that the EU should support research to address neglected diseases appearing in developing countries. To this end, it is recommended that the EU should: • Mobilize and sustain adequate funding for neglected diseases.
• Encourage translational research to transform the results of basic research into useful medical applications, adapted to the needs of patients affected by neglected diseases.
• Expand the activities of the EDCTP to include other neglected diseases as well as other phases of clinical development (Phase I, Phase IV).
• Create a Centre for Preclinical Research to bridge the continuing gap between the development of promising medicine leads and their move into clinical trials. This Centre should complement the activities of the EDCTP.
• Develop mechanisms to provide direct support for PPPs to develop drugs and vaccines for diseases where there is no commercial market.
Innovative responses to market deficiencies
Product development initiatives provide an innovative approach to the critical need for new interventions to combat examples of market failure, such as development of medicines for infectious diseases in developing countries. There are many PPPs but it remains to be seen whether this innovative approach will succeed in bringing products to market. The EU has displayed strategic leadership with the establishment in 2003 of the European and Developing Countries Clinical Trials partnership (EDCTP), focused on clinical trials for the medicines development process for HIV/AIDS, TB and malaria.

9. Conclusions and recommendations
127
However the pipelines for medicines for TB, malaria and neglected diseases are far from robust. If the chemical entities are not available to be tested in clinical trials, the EDCTP will be underutilized. To date, the role of the EU in supporting product development PPPs has been modest. This Report recommends that the EU develop a leadership strategy and accompanying funding to provide selective support for translational and preclinical phases of R&D for medicines to treat various neglected infectious diseases.
• The EU research funding process is not always “user‐friendly” and may actively discourage applications from PPPs. Modifications to the current application process are needed (DG Research).
• Innovative funding mechanisms should be promoted to encourage additional investigators to undertake multidisciplinary research on microbicides for the prevention of HIV transmission (DG Research).
Information technology and pharmaceutical innovation
When new medicines enter the market, often little is known about their effectiveness and safety beyond comparison to a placebo. Moreover, knowledge of adverse effects is usually limited to what has been detected in small, short‐term trials and in pre‐marketing toxicology studies. As a result, uncertainty about the relative cost‐effectiveness of new and existing medicines hampers re‐imbursement decisions by insurers. Estimates of the comparative efficiency and safety of new medicines require extremely large and expensive trials which may delay the entry of new products. Traditional forms of post‐marketing surveillance have concentrated on the detection of uncommon severe adverse reactions and provide little information on other important aspects of medicine performance. To help bridge this gap, there is considerable scope for the use of electronic medical records (EMRs) captured in automated databases, in the investigation of the relative benefits, side‐effects and cost‐effectiveness of new medicines. Studies of tens of thousands of recipients of new and older medicines, with routine collection of major outcomes, can be conducted relatively cheaply using existing databases. Studies can be strictly observational or can employ a randomization step (randomized epidemiology) in order to provide unbiased estimates of comparative effectiveness and safety. As the results of these studies have implications for reimbursement decisions, governments and insurers should consider sharing their costs with pharmaceutical manufacturers. If agreement can be reached on the conduct and funding of such randomized epidemiological studies, it may be possible to reduce pre‐marketing regulatory requirements and speed up the market entry of new medicines. The introduction of EMRs has a range of other attractions including improvements in quality of care and in the efficiency of the operation of health systems. Electronic

Priority Medicines for Europe and the World
128
prescription and medical databases can be used to conduct Phase IV and other such pharmaco‐epidemiologic studies. The European Commission is presently discussing so‐called “e‐prescribing” and other information technology (IT) approaches as part of its interest in the information society, although such an effort will require clarification and adjudication of outstanding issues relating to data privacy. The European Union has a clear competitive advantage in ʺe‐prescribingʺ which should be exploited as a matter of urgency. In response to these challenges the Report makes the following recommendation:
• Private insurers and governments should set aside a proportion of their annual budget for medicines in order to endow an organization which could provide an independent source of research into the comparative effectiveness and cost of medicines. This is particularly needed in the case of off‐patent (generic) medicines where the industry sponsor is unlikely to invest in such strategies for post‐marketing follow‐up (Reimbursement authorities).
• A research programme should be established by the EU to use electronic prescription and medical databases to conduct Phase IV and/or pharmaco‐epidemiologic studies on comparative effectiveness. Results of these studies have implications for reimbursement decisions. Governments and insurers should consider sharing their results with pharmaceutical manufacturers (DG SANCO).
• If agreement can be reached on the conduct and funding of randomized epidemiological studies, it may be possible to reduce pre‐marketing regulatory requirements and speed up the market entry of new medicines (EMEA).
• The full realization of the potential of EMR in monitoring medicine‐related adverse effects and other health outcomes requires a significant commitment of resources, perhaps through inclusion in a technology platform (DG Research).
Increasing patient involvement in health policy
Since the public and patients are directly affected by the policies and practices that inform pharmaceutical innovation, policy‐making must reflect an approach that includes public and patient involvement. The publicʹs involvement must include, but not be limited to: providing advice on the harmonization of trial processes and confidentiality/informed consent protections for trial participants in Europe; providing input into the design and improvement of research for individual medications; membership of ethics committees; reviewing and setting medicines regulations; advising and disseminating information and encouraging involvement in clinical trials; providing insight into the design of treatment guidelines and reimbursement decisions.
• The EU should use public funds to support suitable structures to allow patient
feedback on these policies at the national and regional level (DG SANCO, DG Research).

9. Conclusions and recommendations
129
Technology Platform for the Pharmaceutical Industry
ʺTechnology Platformsʺ can be created under the provisions of Treaty Article 171. A technology platform is intended to unite stakeholders around a common vision and approach for the development of technologies and the mobilization of the necessary critical mass needed for research and innovation efforts. The mission of the proposed Sixth Framework Technology Platform for Innovative Medicines would be to enhance and accelerate the development process of medicines, in part through reinforced product development PPPs and increased support for small and medium‐sized enterprises. Antibacterial resistance and pandemic influenza — the focus of two major recommendations identified in this Report — may be suitable priorities around which to build a common strategy for the European pharmaceutical and biotechnology industry. Both of these pose a major threat to global public health. Addressing them successfully would require the involvement of every country in the EU. Individuals, doctors and pharmacists, national ministries, professional associations, universities, research institutions, regulators and the pharmaceutical industry would all have to work together to address the common threat.
• This Report recognizes that other Seventh Framework Programme actions can be used to address the issues of pandemic influenza and antibacterial resistance. However, the proposed Technology Platform for Innovative Medicines could mobilize sufficient human and financial resources across all sectors to address antibacterial resistance and pandemic influenza, while promoting innovation in the European pharmaceutical industry.
• The Platform should adopt equitable access principles to ensure that people in developing countries will have access to the fruits of the innovations through, for example, reasonable pricing clauses or open access licences that would allow low‐cost producers to offer the products in low‐income countries.

Priority Medicines for Europe and the World
130

Glossary
131
Glossary ACE‐inhibitors: Angiotensin‐Converting Enzyme inhibitors block the action of the angiotensin‐converting enzyme, dilating the blood vessels and resulting in lower blood pressure. Adherence to treatment (also compliance): the extent to which a patient takes his/her medication according to the prescribed schedule (also referred to as compliance). Antiplatelet agents: antiplatelets are used to prevent the formation of blood clots in arteries by decreasing the tendency of platelets to stick together. Biomarker: a cellular or molecular indicator of exposure, health effects, or susceptibility. Biomarkers can be used to measure internal dose, biologically effective dose, early biological response, altered structure or function, susceptibility. Biotechnology: the industrial application of biological processes, particularly recombinant DNA technology and genetic engineering. Burden of disease: refers to the overall impact of diseases and injuries at the individual level, or at the societal level or to the economic costs of diseases. Clinical research: patient‐oriented research conducted with human subjects or on material of human origin involving interaction with human subjects in order to discover what causes human disease, and how it can be prevented and treated. Clinical research can include: mechanisms of human disease; therapeutic interventions; and clinical trials; or development of new technologies. Epidemiologic and behavioural studies, and outcomes research and health services research can also be part of clinical research. Commonality of interest: (as used in this Report) those research needs which are not only relevant for the citizens of the EU, but also for countries in economic transition and for developing countries. Dependency ratio: proportion of children and old people in a population in comparison to all others, i.e., the proportion of economically inactive to economically active. Differential pricing: the sale of the same good to different buyers at different prices, with the aim of improving the affordability of medicines while at the same time generating revenue for the pharmaceutical industry. Disability adjusted life years (DALYs): are used to help measure the burden of disease and the effectiveness of health interventions. The DALY is a health gap measure, which combines information on the ʹyears of life lostʹ and ʹyears lived with disabilityʹ.

Priority Medicines for Europe and the World
132
Drug formulation: the composition of a dosage form, including the characteristics of its raw materials and the operations required to process it. Effectiveness: a measure of the extent to which a specific intervention, procedure, regimen or service, when deployed in the field in routine circumstances, does what it is intended to do for a specified population; a measure of the extent to which a health care intervention fulfils its objectives. To be distinguished from efficacy. Efficacy: the ability of a drug to produce the purported effect as determined by clinical trials. Fibrosis: liver fibrosis and cirrhosis (clinically distinct conditions but, unless specifically mentioned, they are used interchangeably in this Report) represent a continuous disease spectrum characterized by an increase in total liver collagen and other matrix proteins which disrupt the architecture of the liver and impair liver function. Fibrosis results from sustained wound healing in the liver in response to chronic or iterative injury.
Fixed‐dose combinations: two or more drugs combined in one pill or capsule, in specific dosages, to facilitate correct drug intake. Genomics: the study of the genome (the sum total of the genetic material present in a particular organism) and its action. Generic drug: a pharmaceutical product usually intended to be interchangeable with the innovator product, which is usually manufactured without a licence from the innovator company and marketed after the expiry of patent or other exclusivity rights. Generic drugs are marketed either under a non‐proprietary or approved name rather than a proprietary or brand name. Gross national income: Gross national income (GNI) (formerly gross national product, or GNP) is the sum of gross value added by all resident producers plus any product taxes (less subsidies) that are not included in the valuation of output plus net receipts of income from abroad. Ischaemic heart disease: this is caused by narrowing of the coronary arteries, which supply blood to the muscle of the heart. Lack of oxygenated blood for more than a short period causes ischaemia, or muscle cell death. Marginal costs (of a product trade): the additional cost incurred in producing one more unit of a product. Medicine use: the process of diagnosis, prescribing, labelling, packaging and dispensing, and of adherence to medicine treatment by patients.

Glossary
133
Meta‐analysis: a statistical synthesis of the data from comparable studies, leading to a quantitative summary of the pooled results. The aim is to integrate the findings, pool the data, and identify the overall trends of results. Morbidity: Any departure, subjective or objective, from a state of physiological or psychological well‐being. Mortality rate: An estimate of the portion of a population that dies during a specified period. Mutagenicity: the degree or measure of the ability to cause mutation. Neglected diseases: Diseases which are seriously disabling or life‐threatening but for which treatment options are inadequate or do not exist and the drug marketing potential is insufficient to readily attract a private sector response. Nosocomial (hospital‐acquired) bacteraemia: an infection originating in a hospital facility, occurring in a patient in whom the infection was not present or incubating at the time of admission. Orphan diseases: rare diseases, including those of genetic origin, are life‐threatening or chronically debilitating diseases which are of such low prevalence that special combined efforts are needed to address them. Pandemic: a widespread disease outbreak affecting the population of an extensive area of the world. Parallel imports: these are products imported into a country without the authorization of the right holder in that country, which have been put on the market in another country by that person or with his/her consent. Pharmaco‐epidemiology: the study of the use and effects of medicines in large numbers of people. Pharmaco‐economics: the application of the economic framework to the study of medicines use and effectiveness. Pharmacokinetics: the study of the rate of drug‐action, particularly with respect to the variation of drug concentrations in tissues with time, and the absorption, metabolism and excretion of drugs and metabolites Placebo: an inert medication or procedure i.e., one having no pharmacological effect, but that is intended to give patients the perception that they are receiving treatment of their complaint.

Priority Medicines for Europe and the World
134
Post‐marketing surveillance: a procedure implemented after a medicine has been licensed for public use, designed to provide information on the actual use of the medicine for a given indication and on the occurrence of side‐effects, adverse effects, etc. Prescribing: the act of determining what medication the patient should have and the correct dosage and duration of treatment. Primary prevention: action taken to avoid or remove the cause of a health problem in an individual or a population before it arises. Includes health promotion and specific protection. Priority medicines: those medicines which are needed to meet the priority health care needs of the population (“essential medicines”) but which have not yet been developed. In this Report, a ʺpriorityʺ medicine for a priority disease is by definition also a significant improvement over already‐marketed products. Relative risk: a measure of the incidence of a condition in those exposed to a particular factor in relation to the incidence of that condition in those not so exposed. Randomized clinical trial: an experiment in which subjects in a population are randomly allocated into groups, usually called study and control groups, to receive or not to receive an experimental preventive or therapeutic procedure, manoeuvre or intervention. The results are assessed by rigorous comparison of rates of diseases, death, recovery or other appropriate outcome in the study and control groups. Reverse genetics: in molecular genetics, the identification of genes purely on the basis of their position in the genome with no knowledge of the gene product. RNA virus: the ribonucleic acid (RNA) virus either uses RNA as its genetic material, or its genetic material passes through an RNA intermediate during replication. Secondary prevention: action taken to detect a health problem at an early stage in an individual or a population, so facilitating cure, or reducing or preventing it spreading or reducing or preventing its long‐term effects. Statins: inhibitors of HMG‐CoA reductase, an enzyme which is involved in cholesterol synthesis, especially in the liver. Inhibition of this enzyme causes a reduction in the low‐density lipoprotein in the blood. Translational research: the conversion of basic research advances into products that can be tested on humans. Sources: WHO, UNAIDS, Last JM, ed. A Dictionary of Epidemiology, 2001, National Institutes of Health, World Bank.





























