Embed Size (px)
Citation preview

Principles of Principles of MusculoskeletalMusculoskeletalInjuriesInjuriesWiroon Laupattarakasem, M.D.Wiroon Laupattarakasem, M.D.Professor in OrthopaedicsProfessor in Orthopaedics
Faculty of MedicineFaculty of Medicine
Khon Kaen UniversityKhon Kaen University
13/12/06 Prof.Wiroon Laupattarakasem 2
Contents: Contents: Fractures and DislocationsFractures and Dislocations
■ Mechanisms of injuries■ Description or terminology■ Diagnosis■ Treatment■ Fracture healing

13/12/06 Prof.Wiroon Laupattarakasem 3
DefinitionsDefinitions■ Fracture
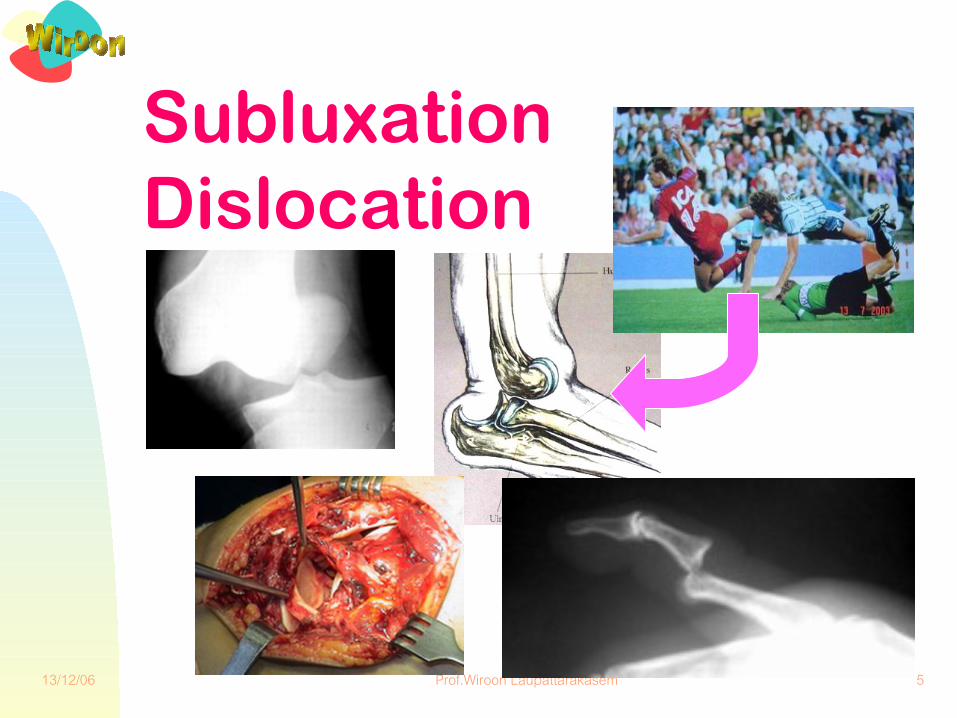
◆ Displacement of fracture fragment■ Joint injuries
◆ Dislocation (luxation) --} loss of congruency◆ Subluxation (sub+luxation)◆ Instability◆ Sprain
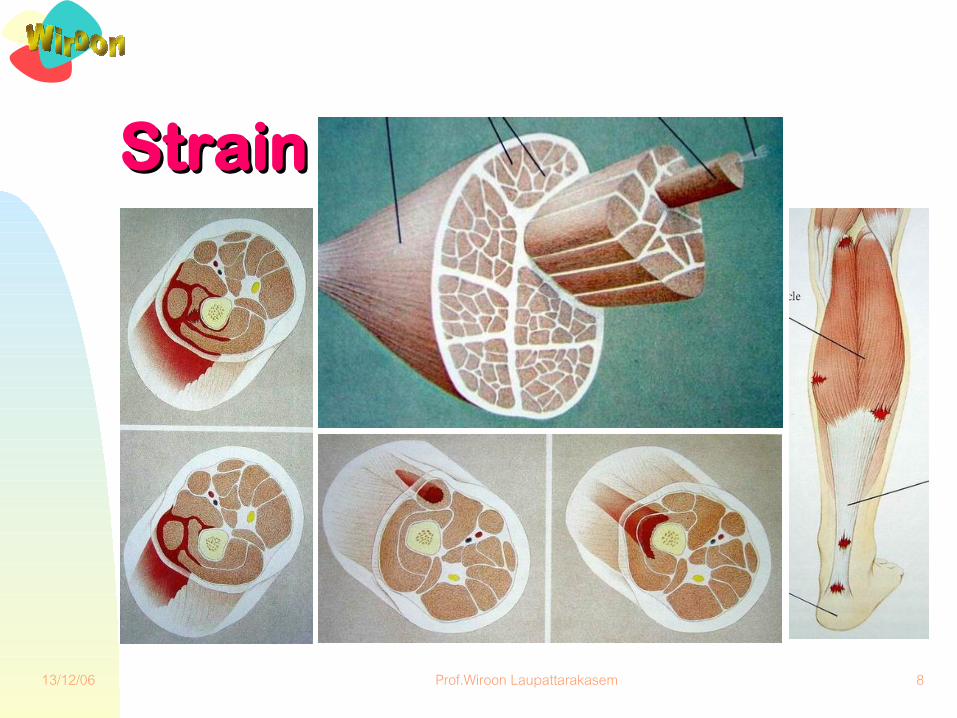
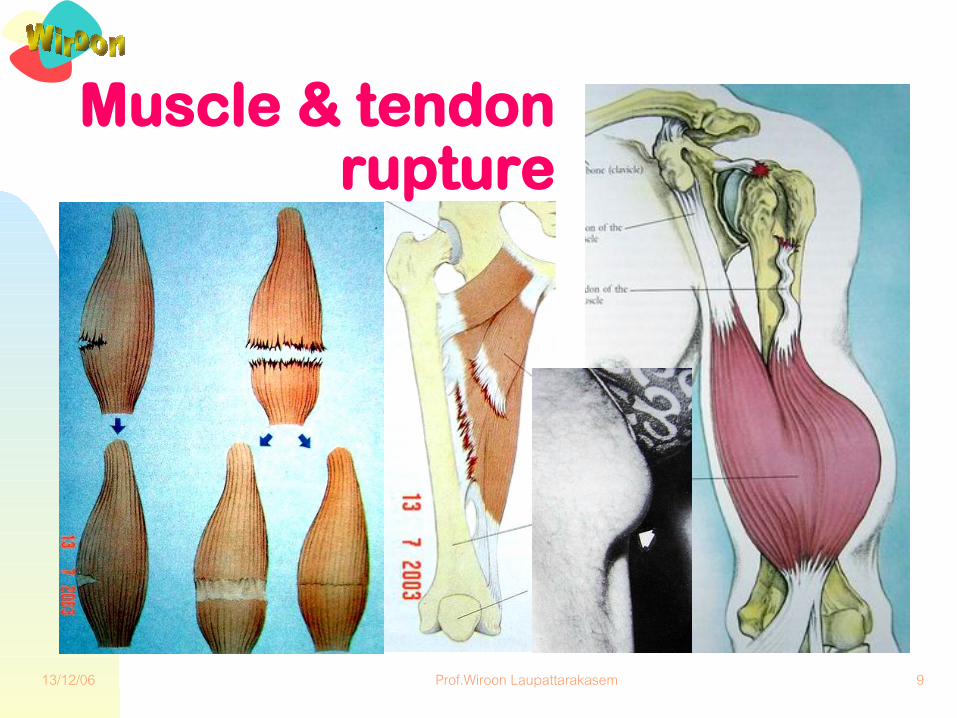
■ Muscle and tendon injuries◆ Tear or rupture◆ Strain

13/12/06 Prof.Wiroon Laupattarakasem 4
Transverse Oblique Spiral Comminuted
FractureFracture
13/12/06 Prof.Wiroon Laupattarakasem 5
Subluxation Dislocation
13/12/06 Prof.Wiroon Laupattarakasem 6
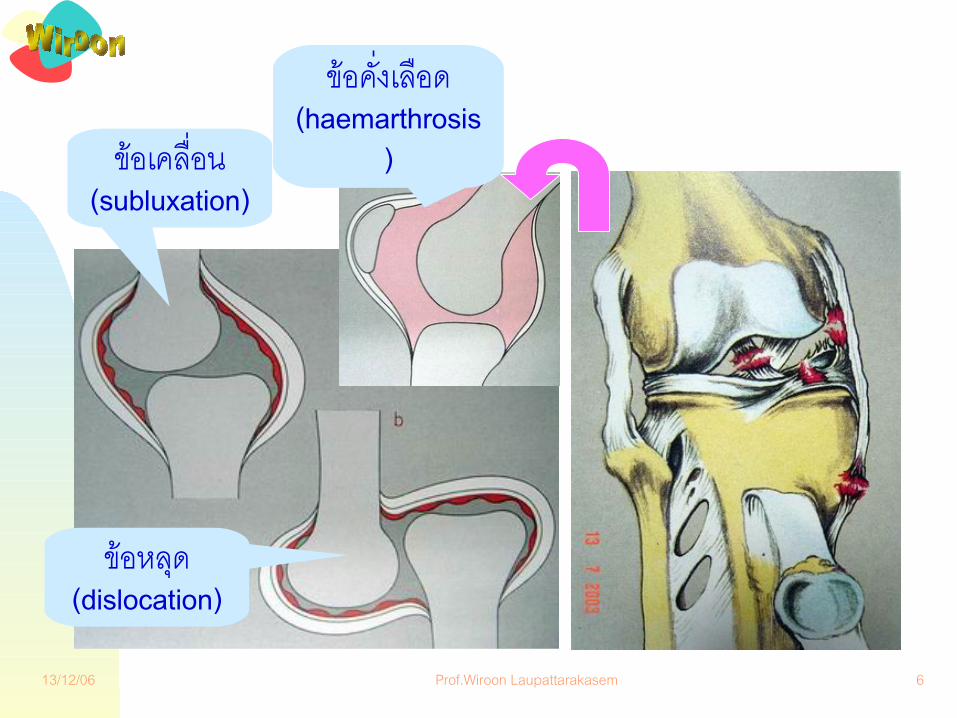
ข�อเคล!"อน (subluxation)
ข�อหล&ด (dislocation)
ข�อค("งเล!อด (haemarthrosis
)

13/12/06 Prof.Wiroon Laupattarakasem 7
Rupture of Meniscus
13/12/06 Prof.Wiroon Laupattarakasem 8
StrainStrain
13/12/06 Prof.Wiroon Laupattarakasem 9
Muscle & tendon rupture
13/12/06 Prof.Wiroon Laupattarakasem 10
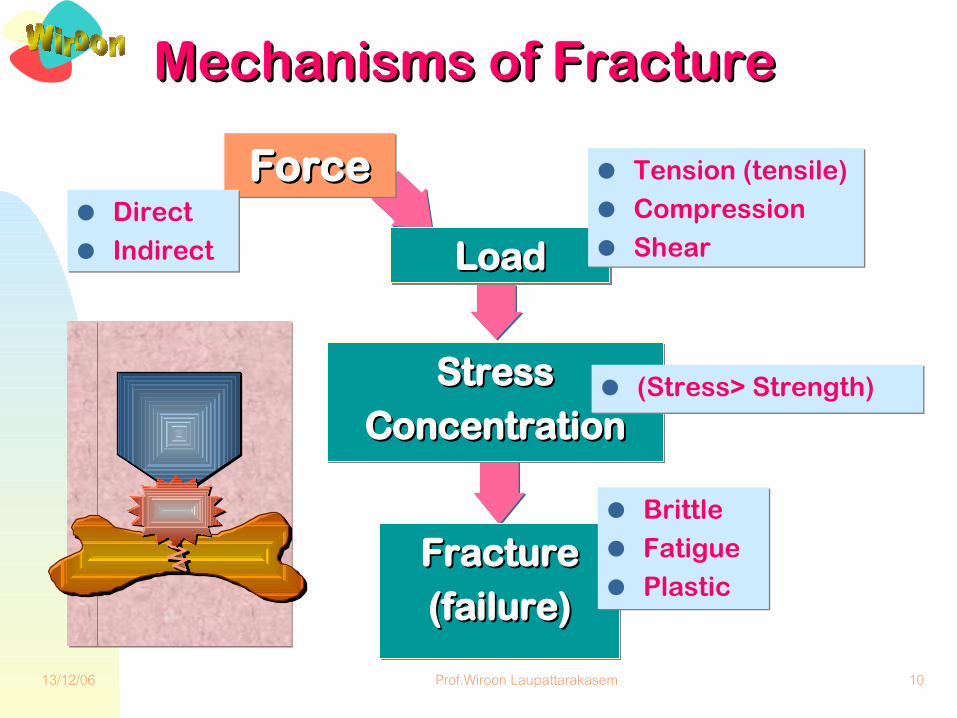
Mechanisms of FractureMechanisms of Fracture
ForceForce● Direct● Indirect
FractureFracture
(failure)(failure)
● Brittle● Fatigue● Plastic
LoadLoad
● Tension (tensile)● Compression● Shear
StressStress
ConcentrationConcentration● (Stress> Strength)
13/12/06 Prof.Wiroon Laupattarakasem 11
Fracture MechanismFracture Mechanism
by direct forces:
‘‘ ForceForce’ vs. ‘’ vs. ‘AreaArea’’ ■ Tapping fracture■ Crushed fracture■ Penetrating fracture

13/12/06 Prof.Wiroon Laupattarakasem 12
Fracture MechanismFracture Mechanism
by indirect forces■ Avulsion (tension)■ Angulation (bending)■ Rotation (torsion)■ Axial compression■ Angulation + compression■ Angulation + compression + rotation

13/12/06 Prof.Wiroon Laupattarakasem 13
Avulsion FractureAvulsion Fracturee.g., olecranon process
Triceps
13/12/06 Prof.Wiroon Laupattarakasem 14
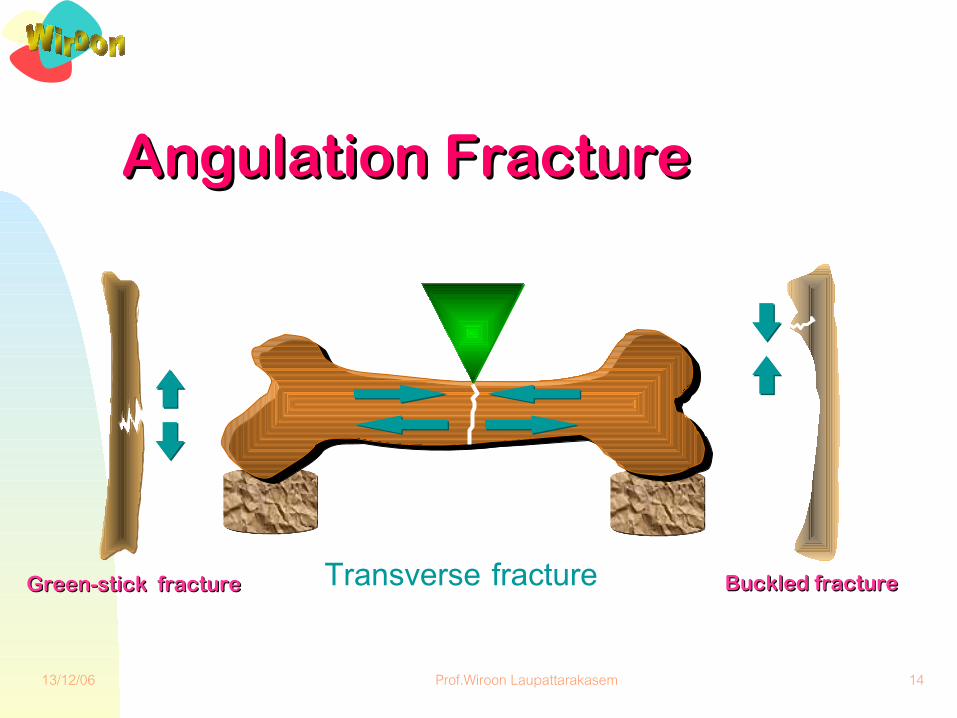
Angulation FractureAngulation Fracture
Transverse fracture Buckled fractureBuckled fractureGreen-stick fractureGreen-stick fracture
13/12/06 Prof.Wiroon Laupattarakasem 15
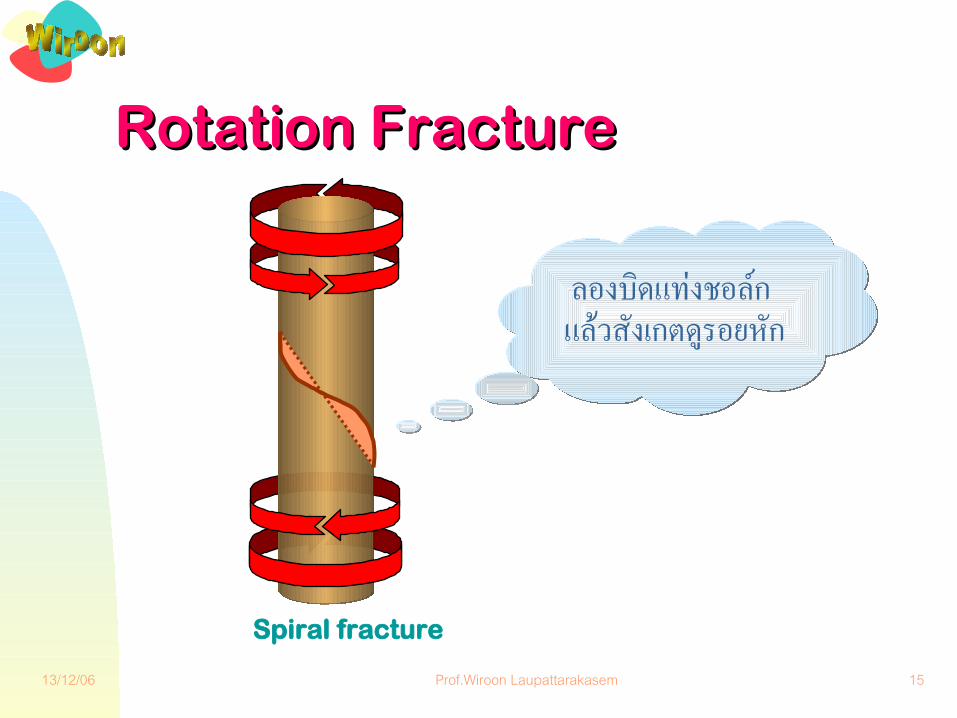
Rotation FractureRotation Fracture
Spiral fracture
ลองบ�ดแทงชอล�ก แล�วส�งเกตด�รอยห�ก

13/12/06 Prof.Wiroon Laupattarakasem 16
Long bone
Oblique fracture
Axial CompressionAxial Compression
13/12/06 Prof.Wiroon Laupattarakasem 17
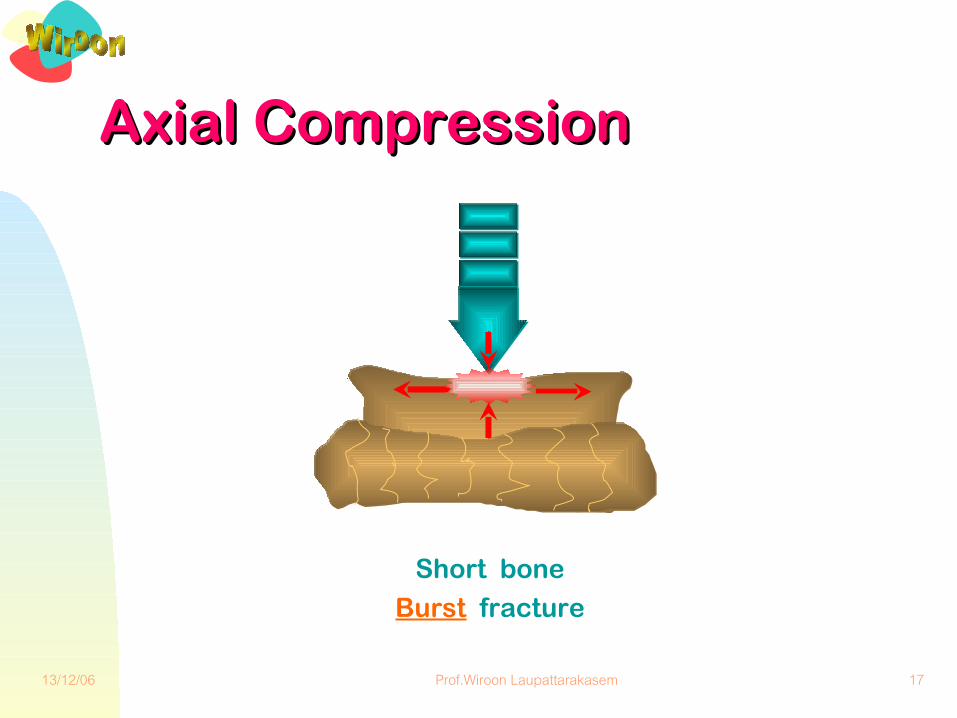
Axial CompressionAxial Compression
Short bone
Burst fracture

13/12/06 Prof.Wiroon Laupattarakasem 18
Angulation + CompressionAngulation + Compression
Butterfly
fracture
13/12/06 Prof.Wiroon Laupattarakasem 19
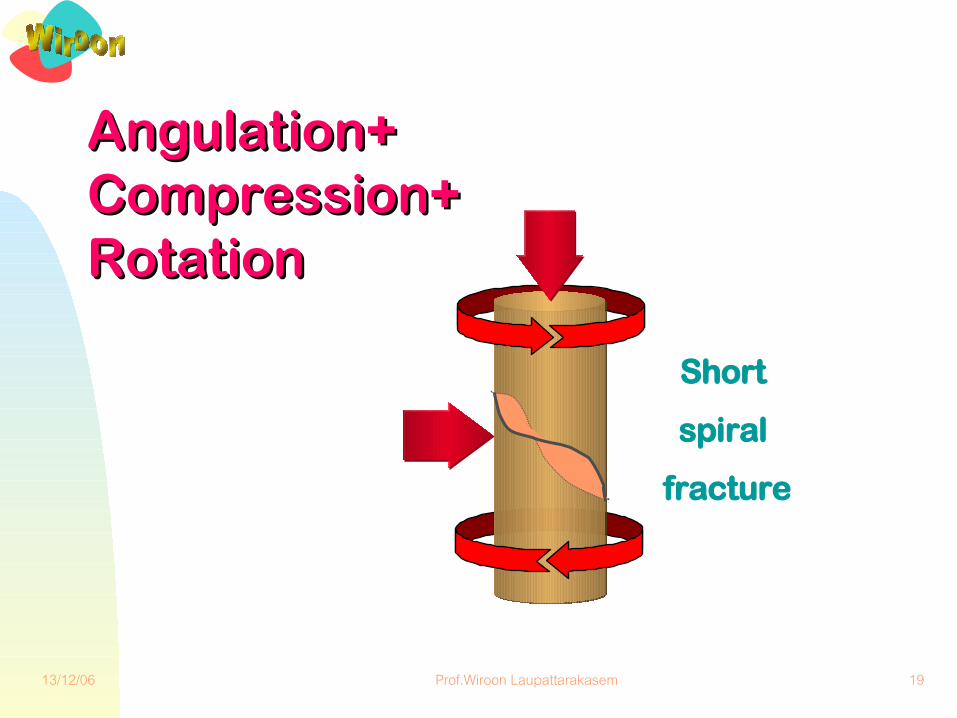
Angulation+ Angulation+ Compression+ Compression+ RotationRotation
Short
spiral
fracture

13/12/06 Prof.Wiroon Laupattarakasem 20
Common Fracture DeformitiesCommon Fracture Deformities
CompressionDistraction
RotationAngulationOverriding
Malapposition

13/12/06 Prof.Wiroon Laupattarakasem 21
Description of a Description of a Fracture DeformityFracture Deformity■ Global agreements:
◆ Always indicating deformity of the distal fragment in relation with the proximal one
◆ e.g., anterior displacement = anterior displacement “of the distal fragment”
Distal
Anterior
Not ‘anteriordislocation’ !
Proximal

13/12/06 Prof.Wiroon Laupattarakasem 22
Description of FracturesDescription of Fractures■ Fracture■ Fracture of the right femur■ Fracture of the right femoral shaft■ Oblique fracture of the right femoral shaft with
anteromedial displacement■ Type II open oblique fracture of the right
femoral shaft with anteromedial displacement
Which one tells you more definitely ?

13/12/06 Prof.Wiroon Laupattarakasem 23
Styles:Description of FracturesDescription of Fractures
➾ Fracture of the femur➾ Femoral fracture ➾ Fractured femur➾ Fracture, femur➽ Fracture femur
ใช�บอยในภาษาพ�ดแตไมถ�กหล�กตามภาษาเข"ยน

13/12/06 Prof.Wiroon Laupattarakasem 24
Description of Bone and Joint Description of Bone and Joint InjuriesInjuries■ “Fracture” / “dislocation, etc.”
◆ Adding adjective, conjunction, preposition◆ Usually describing acute conditions
● Define otherwise old fracturemal-united fractureun-united fracturerecurrent dislocation

13/12/06 Prof.Wiroon Laupattarakasem 25
Description of Bone and Joint Description of Bone and Joint InjuriesInjuries■ Described by telling
◆ Anatomy, site (e.g., side, bone, part)◆ Type, extent (e.g., open, incomplete)◆ Configuration (e.g., transverse, comminuted)◆ Deformity, ‘direction’ (e.g., displacement,
‘anterior’)◆ Eponym (Colles, Monteggia, Galeazzi)◆ Complication, cause (e.g., infected, fatigue,
pathological)

13/12/06 Prof.Wiroon Laupattarakasem 26
Hair-line fractureTea-cup fracture
Green-stick fracture
Buckled fractureลองเอา
ก�#งไม�สดมาห�กด�
Incomplete Fractures
13/12/06 Prof.Wiroon Laupattarakasem 27
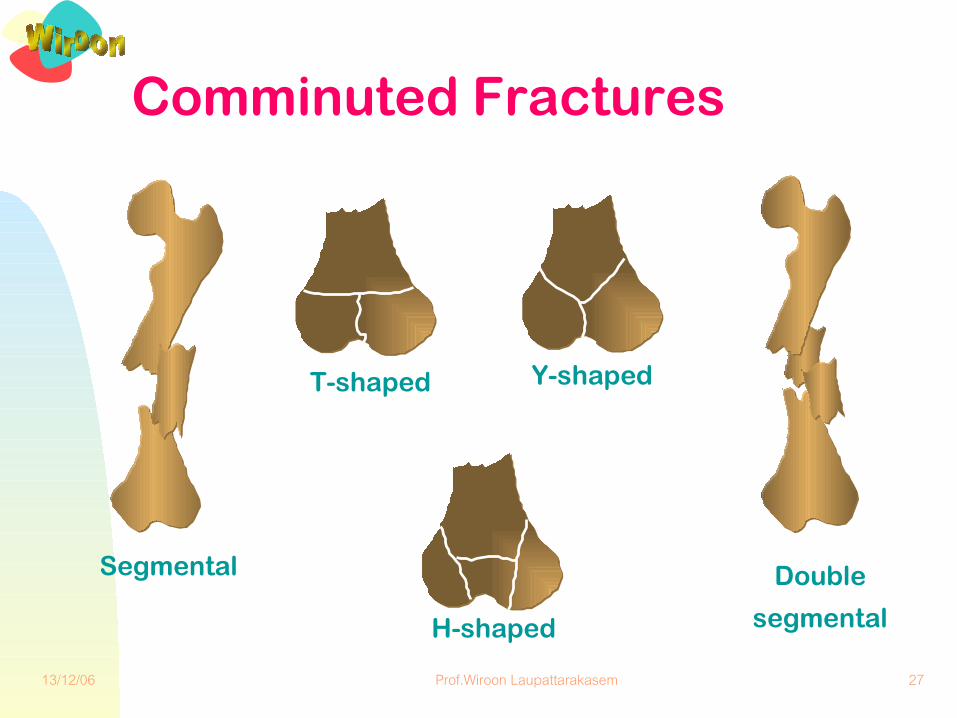
Segmental
T-shaped Y-shaped
H-shaped
Comminuted Fractures
Double
segmental
13/12/06 Prof.Wiroon Laupattarakasem 28
Description of Fractures
Example:Try your own!

13/12/06 Prof.Wiroon Laupattarakasem 29
Description of FracturesDescription of Fractures
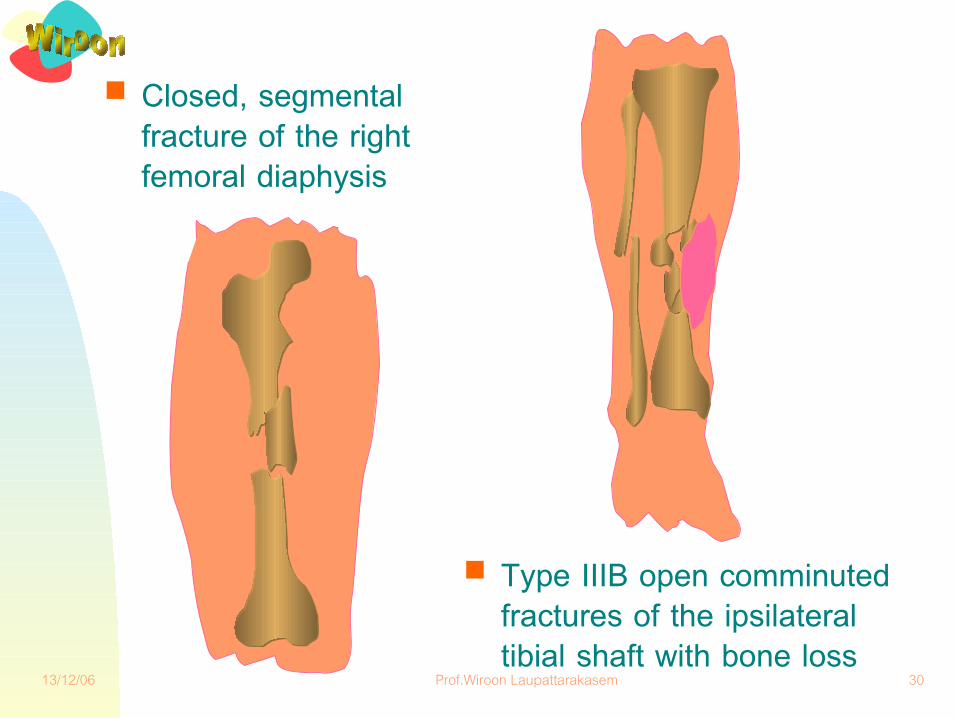
✎ Closed, segmental fracture of the right femoral diaphysis and type IIIB open comminuted fractures of the ipsilateral tibial shaft with bone loss
Example:
ลองประเม�นต�วเองด�วาเข�าใจ
ท'กค)าหร*อไม
13/12/06 Prof.Wiroon Laupattarakasem 30
■ Closed, segmental fracture of the right femoral diaphysis
■ Type IIIB open comminuted fractures of the ipsilateral tibial shaft with bone loss

13/12/06 Prof.Wiroon Laupattarakasem 31
Open fracturesOpen fractures
■ Open fracture = fracture + contamination
■ Classifications ---} prognosis◆ Type I: inside - out◆ Type II: outside - in◆ Type III: Type II + destruction
of other functional unit(s)
ไมใช Openedfracture
Type IIIA, B, C

13/12/06 Prof.Wiroon Laupattarakasem 32
Type III Open FracturesType III Open Fractures■ Shotgun fracture■ High velocity gunshot fracture■ Displaced segmental fracture■ Diaphyseal segmental bone loss■ Farm yard / highly contaminated (wound) ■ Crushed fracture from high speed vehicle■ Associated major vascular injury

13/12/06 Prof.Wiroon Laupattarakasem 33
DescribeDescribe

13/12/06 Prof.Wiroon Laupattarakasem 34

13/12/06 Prof.Wiroon Laupattarakasem 35
DiagnosisDiagnosis■ Common errors—missing and
misdiagnosing (incorrect diagnosis)?■ Tools?
◆ History taking◆ Screening test◆ Physical examination◆ Radiological examination◆ Laboratory investigation

13/12/06 Prof.Wiroon Laupattarakasem 36
DiagnosisDiagnosis
■ History taking◆ Where, when and how did it happen?◆ Which part (s) of the body is (are)
involved?◆ What treatments have been given
prior to the arrival?
ถ�าม"ป+ญหาการส*#อภาษาก�บผ��ป.วย ควรขอร�องให�ผ��น)าสง
ชวยอย�ให�ประว�ต�ด�วย

13/12/06 Prof.Wiroon Laupattarakasem 37
Screening TestsScreening Tests■ Upper extremities
◆ Active movements, shaking hands■ Ribs & sternum
◆ Chest compression – AP, bilateral◆ Cough, deep inspiration
■ Pelvis ◆ Compression – both ilia, pubis
■ Lower extremities◆ Active movements, sign-of-4
■ Spines◆ Active movements, palpation
Functional tests to detect
the evidence of injuries

13/12/06 Prof.Wiroon Laupattarakasem 38
Physical ExaminationsPhysical Examinations
■ Fracture/dislocation◆ Definite signs
● Deformity● Abnormal motion● Crepitus
เจ/บปวดเพ�#มข01นอาจเพ�#มการบาดเจ/บ

13/12/06 Prof.Wiroon Laupattarakasem 39
Physical ExaminationsPhysical Examinations■ Fracture/dislocation
◆ Relative signs● Similar to soft tissue contusion
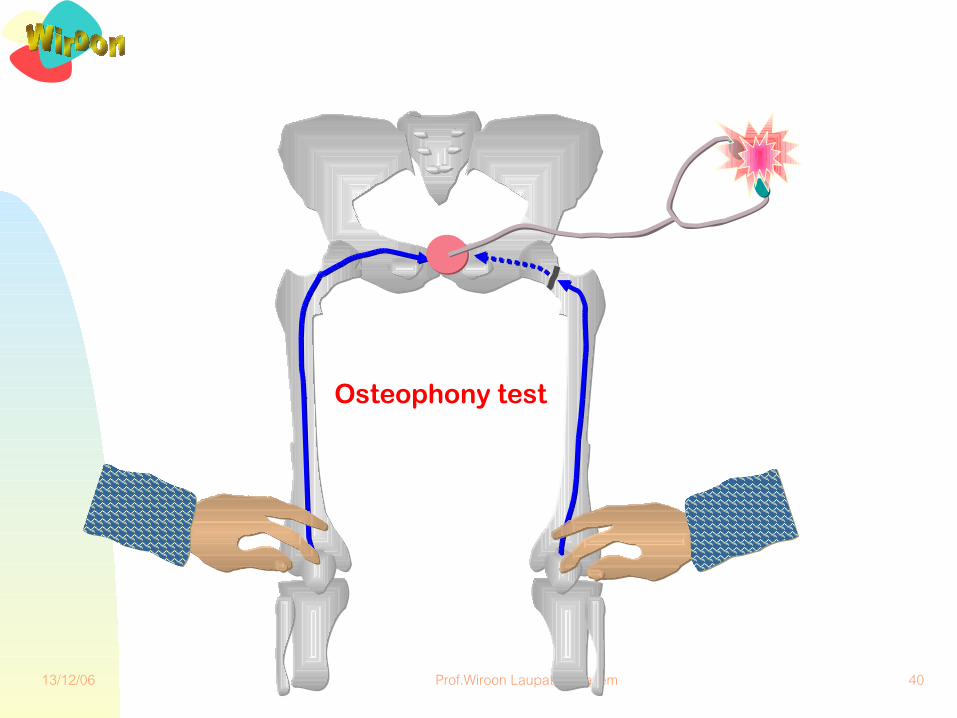
tenderness, swelling, ecchymosis● Circumferential involvement● Osteophony test● Axial compression test
เคาะกระด�กแล�วฟ+งเส"ยง
13/12/06 Prof.Wiroon Laupattarakasem 40
Osteophony test
13/12/06 Prof.Wiroon Laupattarakasem 41
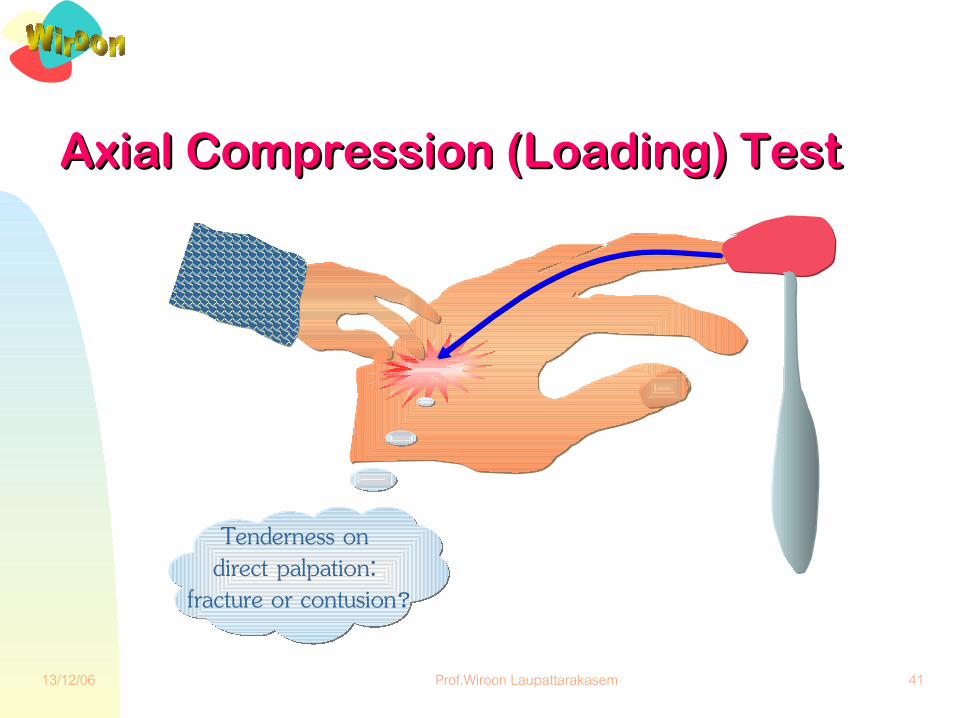
Axial Compression (Loading) TestAxial Compression (Loading) Test
Tenderness on direct palpation:
fracture or contusion?

13/12/06 Prof.Wiroon Laupattarakasem 42
Radiographic ExaminationsRadiographic Examinations■ Plain film
◆ AP, lateral, (2 obliques)◆ Special views, e.g., swimmer’s, axial
■ Computerized tomography (CT scan)■ Magnetic resonance imaging (MRI)■ Special techniques
◆ e.g., tomography, angiography, MRA

13/12/06 Prof.Wiroon Laupattarakasem 43
Roentgenographic Roentgenographic ViewsViews■ 2 views: AP, lateral; two oblique■ 2 joints: parallel bones, one displaced
fracture, e.g., Monteggia■ 2 sides: growing ossification centers■ 2 occasions: non-displaced scaphoid
fracture■ 2 media: contrast media

13/12/06 Prof.Wiroon Laupattarakasem 44

13/12/06 Prof.Wiroon Laupattarakasem 45
Axial view Axial view for the for the calcaneuscalcaneus

13/12/06 Prof.Wiroon Laupattarakasem 46
Ultimate Goals of Treatment in Orthopaedics
to restore....... FORMFORM ..........and FUNCTIONSFUNCTIONS

13/12/06 Prof.Wiroon Laupattarakasem 47
Priority Setting for Priority Setting for Trauma PatientsTrauma Patients■ To save
◆ Life◆ Limb◆ Function◆ Aesthetics
13/12/06 Prof.Wiroon Laupattarakasem 48
TreatmentTreatment■ Immediate cares
(at the injury site) for◆ A irway obstruction◆ B reathing◆ C irculatory failure: shock◆ D islocation/ fracture
SplintSplint the injured the injured parts:parts:
● Involved joints: Involved joints: one joint above one joint above and below and below
● Different types of Different types of splintsplint
● Thomas splint Thomas splint (best for LE)(best for LE)

13/12/06 Prof.Wiroon Laupattarakasem 49
Thomas Thomas SplintSplint

13/12/06 Prof.Wiroon Laupattarakasem 50
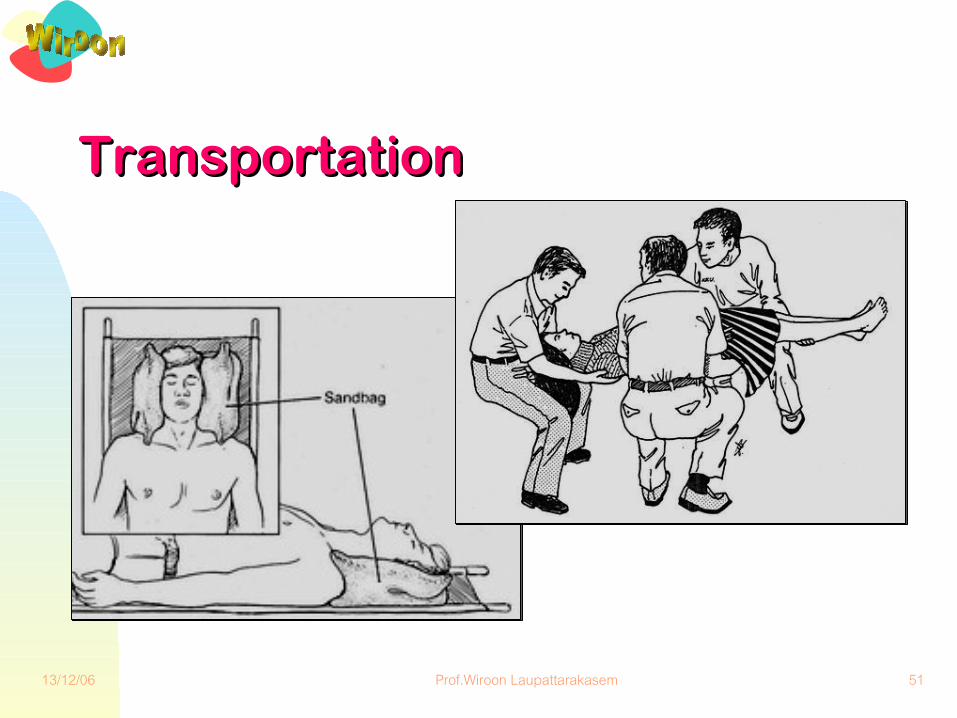
TreatmentTreatment■ Transportation
◆ In suspicion of head injury, splint the neck
◆ Move the victim only when necessary◆ Move unconscious or back-injured
patient as a log (by 3 rescuers)◆ Drive carefully to the hospital
13/12/06 Prof.Wiroon Laupattarakasem 51
TransportationTransportation

13/12/06 Prof.Wiroon Laupattarakasem 52
TreatmentTreatment
■ Emergency cares (at ER/AE room) for◆ A irway obstruction◆ B reathing (bleeding)◆ C irculatory failure◆ D islocation/ fracture
● IntubationIntubation
● HaemostasisHaemostasis
● Fluid / blood Fluid / blood replacementreplacement
● SplintageSplintage
13/12/06 Prof.Wiroon Laupattarakasem 53
General principles of treatmentGeneral principles of treatment
■ Firstly do no harm■ Base treatment on an accurate diagnosis and
prognosis■ Select treatment for specific problems■ Cooperate with the laws of nature■ Be realistic and practical in treatment■ Select treatment for individual patient
13/12/06 Prof.Wiroon Laupattarakasem 54
■ Definitive treatments of fracture / dislocation◆ Reduction (manipulation)◆ Immobilization
TreatmentTreatment
Retention of reduction

13/12/06 Prof.Wiroon Laupattarakasem 55
Closed Closed VsVs Open Treatment Open Treatment
■ Joint immobilization■ Skin problems■ Socioeconomic problems■ Risks of surgery
◆ Anaesthesia◆ Blood transfusion◆ Infection

13/12/06 Prof.Wiroon Laupattarakasem 56
Definitive TreatmentsDefinitive Treatments■ Reduction
▼Closed manipulation ▼with or without fluoroscopy --} image intensifier or C-arm
▼Open (under direct vision)

13/12/06 Prof.Wiroon Laupattarakasem 57
Image Intensifier (C-arm)Image Intensifier (C-arm)

13/12/06 Prof.Wiroon Laupattarakasem 58
■ Alignment◆ how parallel is the longitudinal axes?
Overriding Angulation Rotation
Reduction -- goalsReduction -- goalsFracture deformities to be corrected :

13/12/06 Prof.Wiroon Laupattarakasem 59
■ Apposition◆ end-to-end contact◆ (side-to-side contact: bayonet)
OverridingTranslationCompression
Fracture deformities to be corrected :Reduction -- goalsReduction -- goals
13/12/06 Prof.Wiroon Laupattarakasem 60
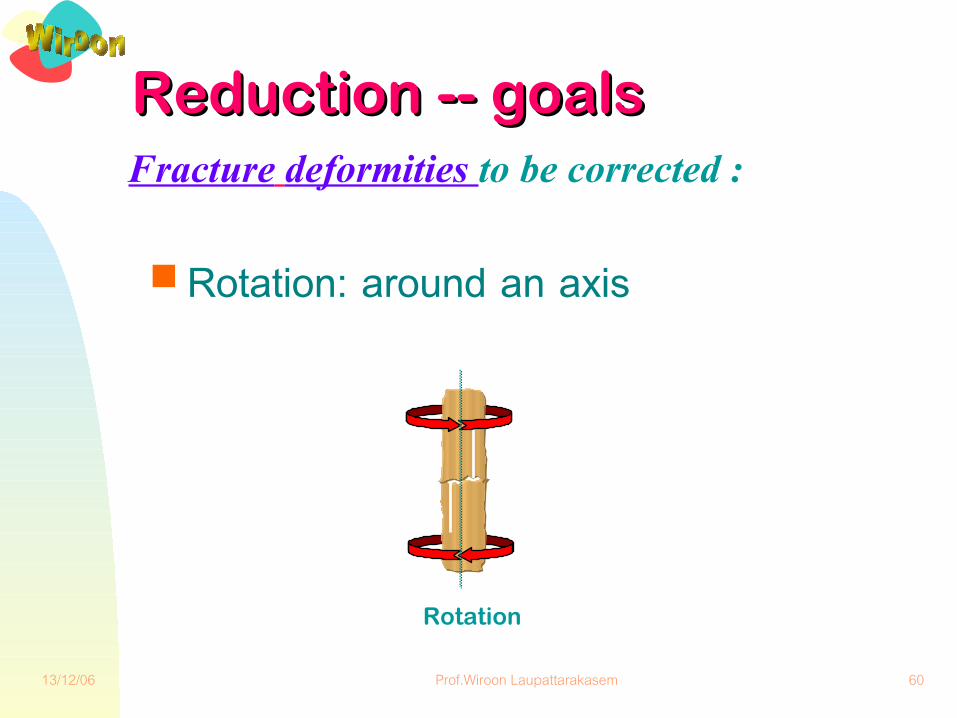
■ Rotation: around an axis
Rotation
Fracture deformities to be corrected :Reduction -- goalsReduction -- goals
13/12/06 Prof.Wiroon Laupattarakasem 61
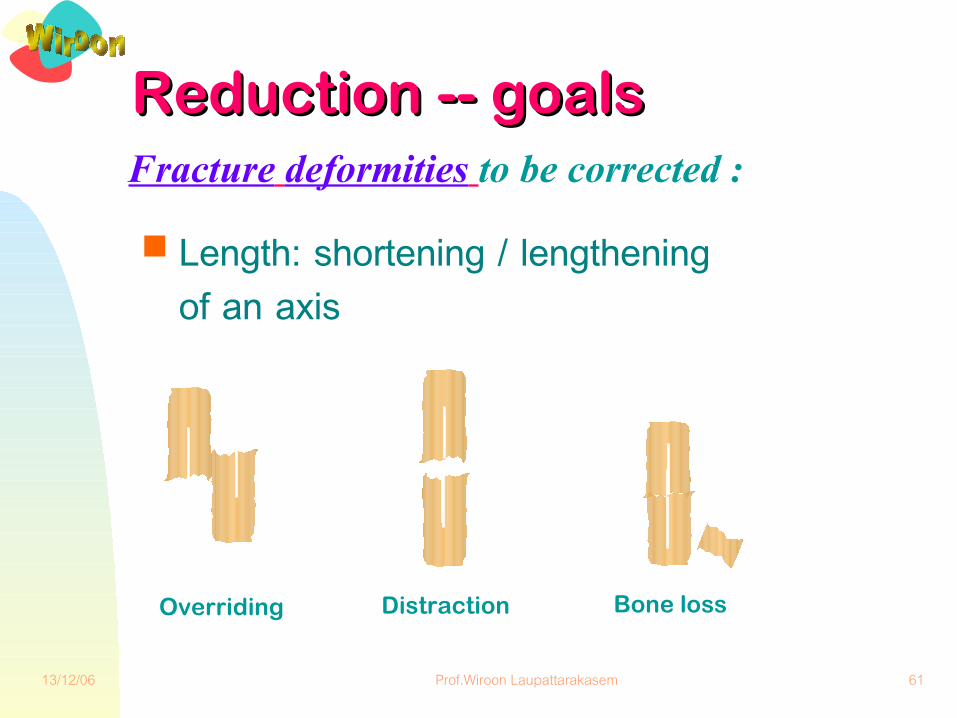
■ Length: shortening / lengthening of an axis
Fracture deformities to be corrected :Reduction -- goalsReduction -- goals
Overriding Distraction Bone loss

13/12/06 Prof.Wiroon Laupattarakasem 62
ReductionReduction
3-point effect
of deforming &
reduction forces
‘Curved’ cast
to maintain
reduction
‘Straight’ cast
results in
re-displacement
or

13/12/06 Prof.Wiroon Laupattarakasem 63
ReductionReduction
Increase
deformity
2
Apply
Traction
1
Reduce 1cortex
3
Reverse
deformity
4

13/12/06 Prof.Wiroon Laupattarakasem 64
ReductionReduction
Increase
deformity
Reduce 1
cortex
Reverse
deformity
Apply
Traction
13/12/06 Prof.Wiroon Laupattarakasem 65
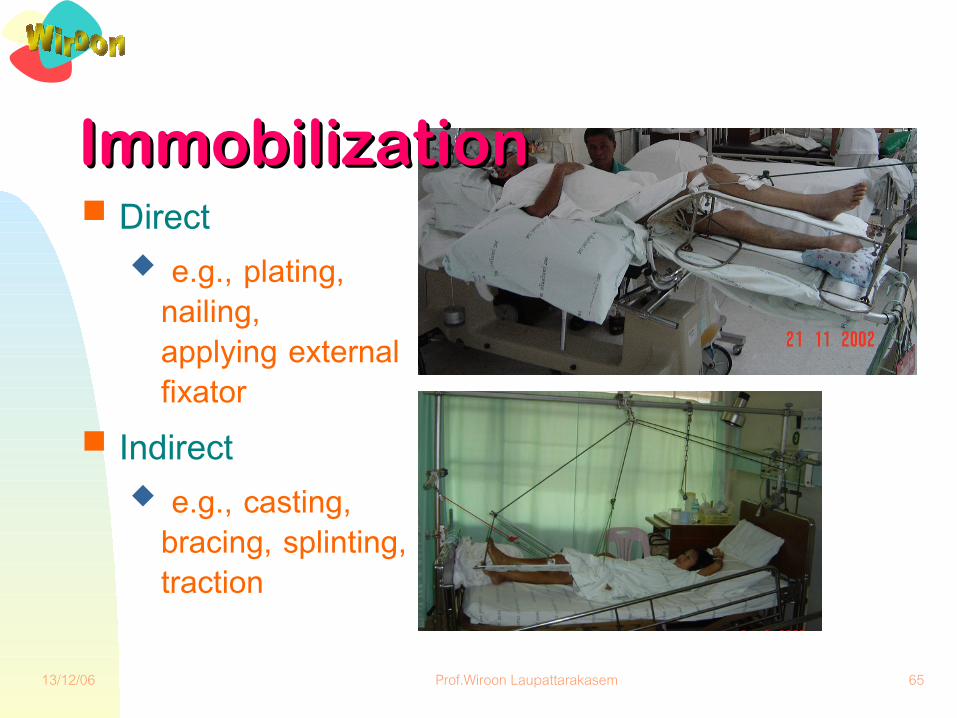
ImmobilizationImmobilization■ Direct
◆ e.g., plating, nailing,applying external fixator
■ Indirect ◆ e.g., casting,
bracing, splinting, traction

13/12/06 Prof.Wiroon Laupattarakasem 66
External Fixators

13/12/06 Prof.Wiroon Laupattarakasem 67
Internal FixationsInternal Fixations■ Plate■ Screw■ Nail, rod■ Pin, wire
◆ Kirschner ◆ Steinmann
■ Wire ◆ cerclage

13/12/06 Prof.Wiroon Laupattarakasem 68
Plate
Screw
Cerclage wire
Nail, rod
Pin, wire -Kirschner -Steinmann
Implants

13/12/06 Prof.Wiroon Laupattarakasem 69
Treatment of Open Fractures

13/12/06 Prof.Wiroon Laupattarakasem 70
Treatment of Open FracturesTreatment of Open Fractures■ Aims
◆ Preventing wound infection▼ Remove devitalized tissues▼ Preserve survived tissues▼ Apply appropriate antibiotics
◆ Fracture reduction and stabilization ---> mostly using external fixator
DebridementDebridement
อานเพ�#มเต�ม
13/12/06 Prof.Wiroon Laupattarakasem 71
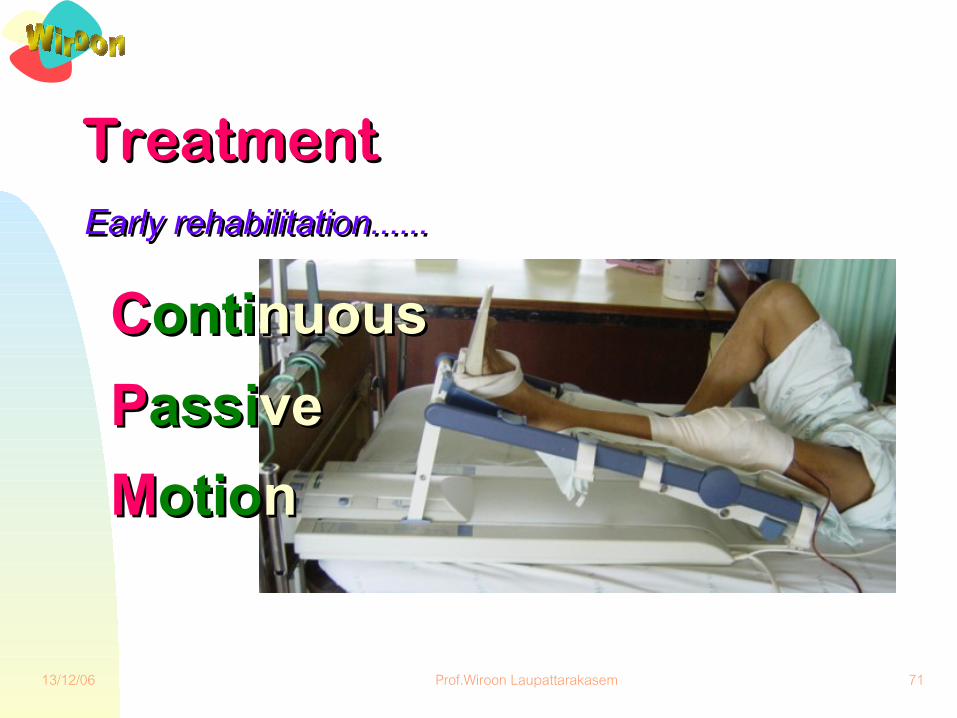
TreatmentTreatment Early rehabilitation......Early rehabilitation......
CContiontinuousnuous PPassiassiveve MMotiootionn

13/12/06 Prof.Wiroon Laupattarakasem 72
■ Conclusions◗ Recognition◗ Relief of pain◗ Reduction of fracture◗ Retention of reduction◗ Rehabilitation◗ Reconstruction
TreatmentTreatment

Specific Methods Specific Methods of Treatment for of Treatment for Closed FracturesClosed Fractures
13/12/06 Prof.Wiroon Laupattarakasem 74
■ No reduction and immobilization■ Non-weight bearing, arm sling, leave alone■ Non- or minimally displaced, stable fracture
◆ fibular # alone, rib #◆ metacarpal #, metatarsal #◆ clavicular # in small children◆ impacted # of humeral neck◆ compression # of vertebra without neuro. deficit
■ Needs close follow-up
Protection aloneProtection alone

13/12/06 Prof.Wiroon Laupattarakasem 75
No reduction--} external splintingNo reduction--} external splinting
■ Partially displaced, stable under axial load ■ Other deforming forces (angulation, rotation)
can be neutralized (stabilized) by cast molding or splinting
◆ tibia and/or fibula (cast)◆ radius and/or ulna (cast)◆ humerus (sugar tong slab)◆ small bones of hand and foot (buddy splint)

13/12/06 Prof.Wiroon Laupattarakasem 76
Closed reduction --} external imm.Closed reduction --} external imm.
■ Displaced fractures, but reduction can be obtained and maintained by closed methods
■ Fractures that do not require rigid immobilization
■ Closed reduction by◆ manipulation◆ gravity or positioning
e.g., flexion compression # of the spines◆ traction: temporary, continuous
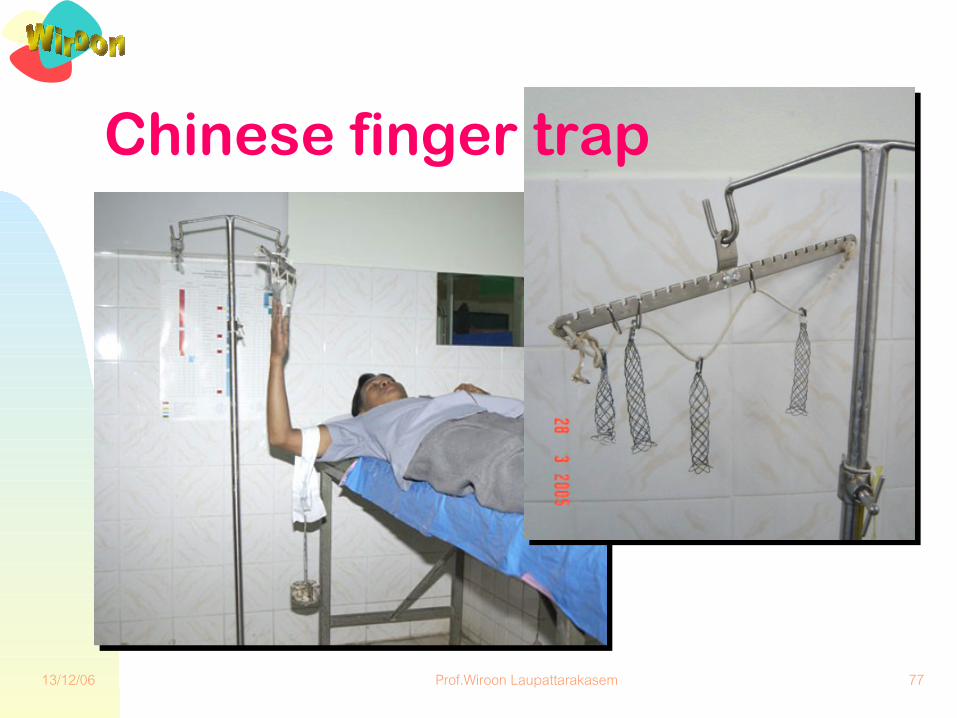
13/12/06 Prof.Wiroon Laupattarakasem 77
Chinese finger trap
13/12/06 Prof.Wiroon Laupattarakasem 78
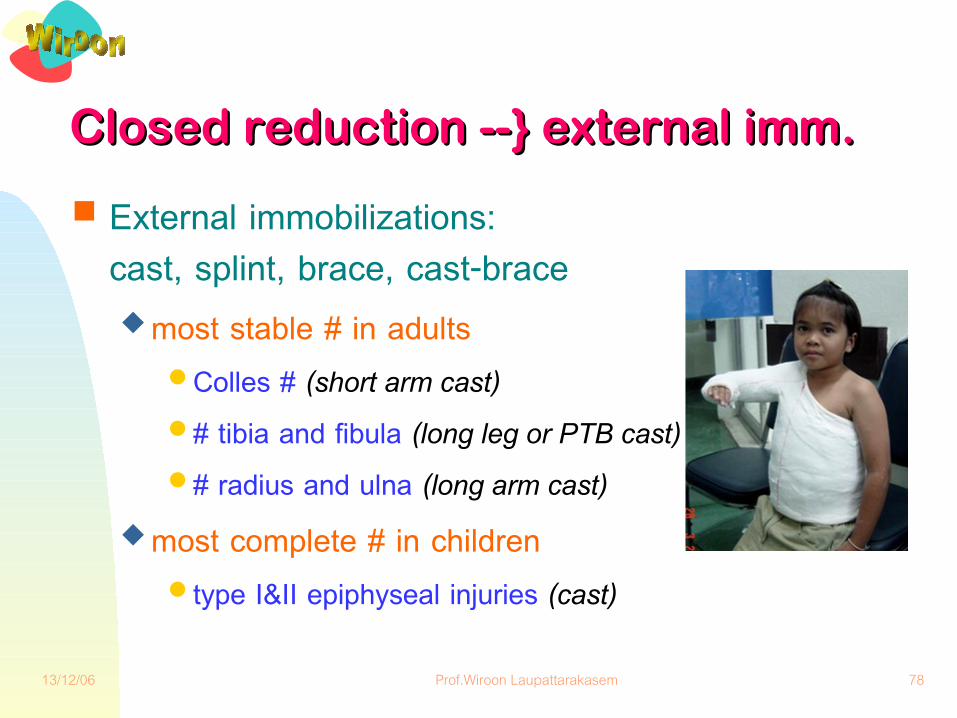
Closed reduction --} external imm.Closed reduction --} external imm.
■ External immobilizations: cast, splint, brace, cast-brace
◆ most stable # in adults● Colles # (short arm cast)● # tibia and fibula (long leg or PTB cast)● # radius and ulna (long arm cast)
◆ most complete # in children ● type I&II epiphyseal injuries (cast)

13/12/06 Prof.Wiroon Laupattarakasem 79
Closed reduction --} direct fixationClosed reduction --} direct fixation
■ Closed reduction: ◆ manipulation, traction + image intensifier
■ Closed internal fixation:◆ pin, wire (supracondylar humeral #) ◆ canulated screw (femoral neck)◆ nail, rod + locking screw (tibia, femur)
■ ‘External fixator’ application

13/12/06 Prof.Wiroon Laupattarakasem 80
Open reduction --} direct fixationOpen reduction --} direct fixation■ A closed fracture that closed reduction cannot be
obtained and/or subsequently maintained■ Open fracture, after sufficient debridement■ Stable or rigid fixation can be obtained by internal
fixation (osteosynthesis) ◆ plate, screws ◆ intramedullary nail or rod (other modified designs)◆ tension band wiring
■ ‘External fixator’ application

13/12/06 Prof.Wiroon Laupattarakasem 81
Excision of a fracture fragment --} Excision of a fracture fragment --} + endoprosthesis replacement+ endoprosthesis replacement
■ Excisional arthroplasty■ High incidence of avascular necrosis, nonunion,
posttraumatic osteoarthritis ◆ femoral neck # in an elderly or being osteoporotic◆ comminuted radial head # in young adults◆ comminuted humeral head # (4-part #)◆ severe comminuted # of the patella

13/12/06 Prof.Wiroon Laupattarakasem 82
LigamentotaxisLigamentotaxis■ Severe comminuted fractures of the joint not
feasible for open reduction and fixation ◆ severe comminuted # of distal radius
■ Distraction of the ligaments and capsule to hold the fracture fragments together as reduction
◆ using external fixator and encourage early motion

13/12/06 Prof.Wiroon Laupattarakasem 83
Ligamentotaxis
13/12/06 Prof.Wiroon Laupattarakasem 84
Bag-of-bone technique
■ Severely comminuted fractures of cancellous bone not feasible for open reduction and fixation
◆ severely comminuted calcaneal #■ Manipulative molding of the fragments as an
reduction■ Encourage non-weight bearing ambulation /
motion

13/12/06 Prof.Wiroon Laupattarakasem 85
If the only tool you have is If the only tool you have is
a a hammerhammer, you tend to see , you tend to see
every problem as a every problem as a nailnailAbraham MaslowAbraham Maslow

13/12/06 Prof.Wiroon Laupattarakasem 86
Fracture HealingFracture Healing■ Regeneration, no scar■ Form Vs function: Wolff’s law■ 3 major phases:
◆ Inflammation◆ Repair: bone / cartilage /
fibrosis● External bridging callus● Medullary callus
◆ Remodeling● Creeping substitution
■ Clinical union◆ Motion◆ Tenderness / pain
■ Roentgenographic union
◆ No fracture line◆ Fully remodeled

13/12/06 Prof.Wiroon Laupattarakasem 87
Result:Result:◆ Restoration of Restoration of
original tissueoriginal tissue◆ Scar tissueScar tissue◆ Excessive repairExcessive repair◆ Failure of healingFailure of healing
Healing:Healing:◆ InflammationInflammation◆ RepairRepair◆ RemodelingRemodeling
Cell Cell matrix matrix damagedamage
TraumaTrauma
InjuryInjury◆ TypeType◆ IntensityIntensity◆ ExtentExtent◆ DurationDuration
PatientPatient◆ AgeAge◆ MetabolicMetabolic◆ Disease Disease ◆ MedicationMedication
TreatmentTreatment◆ AppositionApposition◆ StabilizationStabilization◆ LoadingLoading◆ MotionMotion
Tissue typeTissue type◆ BoneBone◆ CartilageCartilage◆ Fibrous tissueFibrous tissue◆ MuscleMuscle

13/12/06 Prof.Wiroon Laupattarakasem 88
InflammationInflammation
10%10%
RepairRepair
40%40%
RemodelingRemodeling
70%70%
Time
Inte
nsity
of r
espo
nse
13/12/06 Prof.Wiroon Laupattarakasem 89
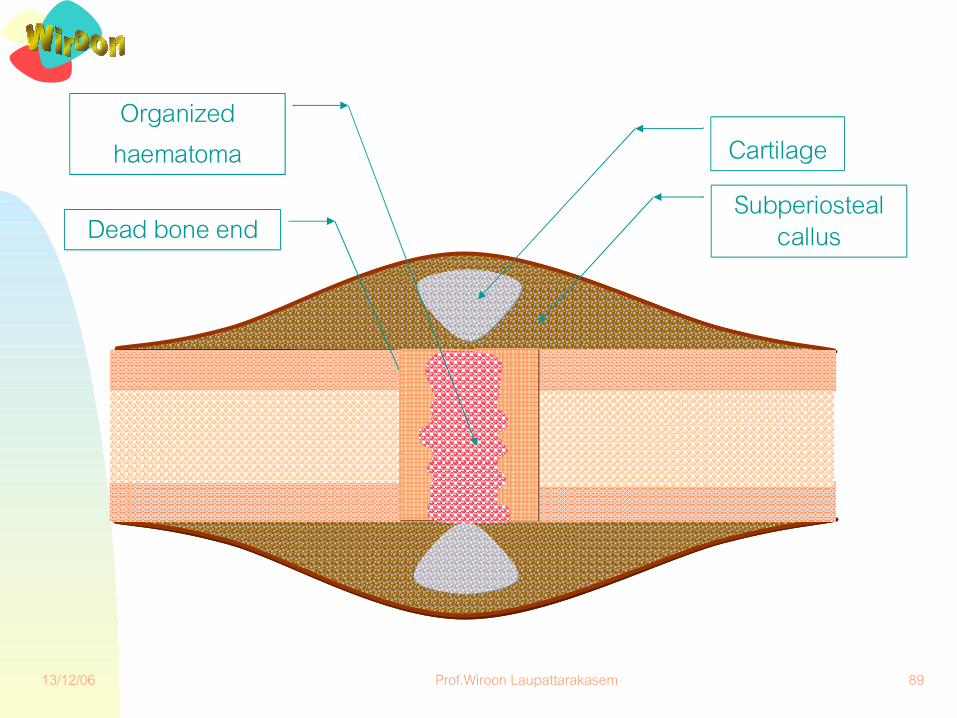
Subperiostealcallus
Cartilage
Dead bone end
Organizedhaematoma

13/12/06 Prof.Wiroon Laupattarakasem 90
Externalbridging
callus
Medullarycallus

13/12/06 Prof.Wiroon Laupattarakasem 91
Thank you Thank you for your for your
attentionattention





























