Embed Size (px)
Citation preview

SPECIAL CONTRIBUTION echocardiography; ultrasound
Principles of Emergency Ultrasound and Echocardiography
Ultrasound is a form of imaging that addresses many needs in emergency medicine. It is fast, accurate, safe, noninvasive, and painless. It rapidly diagnoses immediately life-threatening conditions and reduces the num- ber of invasive or delayed diagnostic methods. However, successful imag- ing requires an understanding of ultrasonic principles. The physical princi- ples of ultrasound imaging with emphasis on its limitations and the bene- fits of emergency echocardiography are highlighted. [Plummer D: Principles of emergency ultrasound and echocardiography. Ann Emerg Med December 1989;18:1291-1297.]
I N T R O D U C T I O N Ultrasound in general and two-dimensional echocardiography (2-DE) in
particular are forms of imaging that directly address the needs of emer- gency medicine. These imaging techniques are fast, accurate, safe, nonin- vasive, and painless. They are rapidly accessible when stationed in the emergency department. The equipment is relatively inexpensive to pur- chase and maintain.
Emergency physicians can use 2-DE to test for life-threatening condi- tions, allowing for more rapid diagnosis and care of patients with critically unstable conditions such as cardiac tamponade. Furthermore, it reduces the number of dangerous and invasive procedures such as diagnostic peri- cardiocentesis and intra-arterial monitoring. Emergency physicians have shown proficiency in performing and interpreting a limited, goal-directed examination.1
An understanding of the physics of ultrasound make most of the control features and limitations of ultrasound devices almost self-explanatory. Ed- ucational and regulatory agencies that deal with ultrasound recognize the importance of this and require an extensive review of the physics of ultra- sound in their curriculum. 2 Therefore, a brief description of the physics of ultrasound followed a review of 2-DE is given.
Berman et al highlighted the importance of understanding the physical principles of ultrasound. 3 In his survey, he reported that more than 90% of practicing ultrasonographers state that a knowledge of the physical princi- ples was mandatory in order to obtain an adequate examination.
ULTRASOUND PRINCIPLES Ultrasound is a form of energy and differs from many other forms Of
energy in that it requires a medium to propagate. It cannot pass through a vacuum like electromagnetic energy. It is a nonionizing form of energy, which contributes to its safety when applied to living tissue. Ultrasound is also a form of sound and propagates in waves. Its properties are fully de- scribed by the parameters common to all waves - frequency, period, wavelength, and amplitude {Table).
Frequency describes the number of cycles per second of the wave and is measured in hertz. By definition, ultrasound is sound propagating at fre- quencies higher than 20,000 Hz, which is just above the human threshold of hearing. The frequency of diagnostic ultrasound ranges between 2.5 and 10 MHz. The wave period refers to the time required to contain one cycle of the wave. Mathematically, it is the inverse of the frequency and is ex- pressed in seconds per cycle. The wavelength refers to the spatial length
Dave Plummer, MD, FACEP Minneapolis, Minnesota
From the Department of Emergency Medicine, Hennepin County Medical Center, Minneapolis, Minnesota.
Received for publication August 3, 1989. Revision received September 1, 1989. Accepted for publication September 18, 1989.
Presented at SAEM-IRIEM Research Symposium in Fort Lauderdale, Florida, February 1989.
Address for reprints: Dave Plummer, MD, FACER Department of Emergency Medicine, Hennepin County Medical Center, Minneapolis, Minnesota 55415.
18:12 Decem ber 1989 Annals of Emergency Medicine 1291/59

ULTRASOUND & ECHOCARDIOGRAPHY Plummer
)
Acoustic Intensity Spatial Considerations
y"~ Spatial Peak
(SP)
SPATIAL
AVERAGE
INTENSITY
(SA)
T
Acoustic Intensity Temporal Considerations:
2
Temporal Peak (TP)
ulse Average (PA)
Temporal Average (TA)
Time
FIGURE 1. Graphic representation of the spatial variance of intensity of an ultrasound beam.
FIGURE 2. A c o u s t i c i n t e n s i t y graphed as a function of t ime in a pulsed ultrasound system.
required to contain one cycle of the wave. Mathematically, it is the speed of the wave divided by the frequency of the wave. The amplitude of the wave relates to the power of the wave; this is important in describing the intensity of the ultrasound beam and the beam's safety to living tis- sues.
Additional parameters describe the propagation of ultrasound through a medium - speed of propagation, im- pedance of medium, intensity of ul- trasound, and attenuation of ultra- sound beam.
The speed of ultrasound in any me- dium is a function of the density and compliance of the medium. Ultra- sound travels fastest through me- diums that are more dense or less compliant. As a result, ultrasound travels faster through solids than liq- uids or gases. When u l t r a s o u n d travels through living tissue, it en- counters a variety of tissue densities. For example, u l t r a sound t ravels slowly through fat but faster through muscle, which is denser and less compliant . The average speed of propagation through the human body is 1.54 ms. 4 This is important in de- termining the depth of a reflecting surface. When an ultrasound pulse
propagates through a medium, it gen- erates an echo when it encounters a reflecting surface. The transducer re- ceives the echo after a given time in- terval. This interval is, therefore, pro- portional to the path length of the pulse. The ul t rasound device can then display the depth of the reflect- ing surface on either a monitor or paper.
Impedance is a function of the me- dium. By definition, impedance is the speed of propagation multiplied by the medium density and is ex- pressed in rayles. A key principle is that ultrasonic reflections, or echoes, ~form at impedance boundaries. As a result, structures often can be identi- fied within an organ - for example, calcific cardiac valves in the heart or gallstones within the gallbladder.
Acoustic intensity is a difficult as- pect of ultrasound to explain and measure because the u l t rasound beam is nonuniform both spatially and temporally. The maximum in- tensity of an ultrasound beam is di- rectly in the center and defined as the spatial peak intensity (SP) (Figure 1). The spatial average intensity (SA) of the beam is the power contained within the entire beam divided by its cross-sectional area. However, diag- nostic ultrasound uses pulsed ultra- sound and is temporally nonuniform as well (Figure 2). Each short pulse precedes a long si lent period in which the t ransducer l is tens for echoes. The temporal peak intensity (TP) refers to the maximum intensity achieved during one pulse. Two other parameters calculated are the total
power in each cycle divided by the pulse duration or the cycle duration, which yields the pulse average inten- sity or the temporal average inten- sity, respectively.
These two spatial and three tempo- ral intensities combine into six sepa- rate standard intensity parameters (Figure 3) that help define and assess ultrasound safety. Potential adverse effects include tissue heating, micro- cavitation, and other poorly defined effects. Microcavitation, or the mi- croscopic disruption of medium, re- sults from extremely high-intensity ultrasound. However, the intensities generated by currently available diag- nostic ultrasound machines are safe for use in human beings. 5-7 No inde- pendently confirmed or reproducible adverse effects on living tissue exist despite decades of clinical use; there are no known injuries to human be- ings from diagnostic ultrasound.
As an ultrasound beam propagates through a tissue, it will lose power, or attenuate. This occurs as a result of three separate mechanisms. First, all mediums absorb ultrasound and convert it to heat. Second, echoes generated consume a fraction of the power of the initial beam. Finally, ul- trasound scatters in several direc- tions when propagating through a medium. The amount of attenuation is expressed in decibels. When an ul- trasound pulse encounters two re- flecting surfaces at different depths, the path length of the echo from the first reflection is less than that of the second. Therefore, the echo from the first will arrive earlier and with a
60/1292 Annals of Emergency Medicine 18:12 December 1989

Intensity Ratings
TA TP PA
SA
SP
SATA
SPTA
SATP
SPTP
SAPA
SPPA
NO REPRODUCIBLE MAMMALIAN EFFECTS HAVE BEEN INDEPENDENTLY CONFIRMED
ASPECTS OF PULSED ULTRASOUND
PULSE DURATION I I
PULSE REPETITION PERIOD I
SPL Y 4
AXIAL RESOLUTION
SPL "-., / UNRESOLVED RESOLVED
"'1 I "1 FULL ECHO
LATERAL RESOLUTION
FULL ECHO
m
PART ECHO I NO ECHO
6
greater strength than that of the sec- ond. The display then can map these two echoes appropriately in different vertical positions corresponding to depth but with a different brightness corresponding to the echo strengths. As a result, these two identical re- flecting surfaces will appear different on the display.
An important aspect of attenuation is that it increases with greater fre- quency. In living tissue, the amount of attenuation in decibels per centi- meter is 1/2 * frequency. The higher the ultrasound frequency, the faster it loses power and the less tissue penetration is possible. However, in- creased frequency improves resolu- tionso that resolution and tissue penetration are inversely related.
RESOLUTION Resolution refers to the ability of
the device to discriminate small ob- jects or defects in objects. The fre- quency of the ultrasound limits the resolution of the system.
Pulsed ul t rasound consists of a short pulse of two or three cycles of high-frequency ultrasound (Figure 4). Each cycle in the pulse has a given wavelength. The spatial pulse length (SPL) is a sum of these wavelengths. Parameters similar to those used to describe simple waves also describe the nature of repeating pulses. The pulses repeat with a given pulse repe- tition frequency (PRF), which is usu- ally 1 KHz. The pulse duration is the time required for one pulse cycle.
The SPL is the critical determinant
FIGURE 3. The six independent ex- pressions of accurate intensity.
FIGURE 4. Graphic representation of the relation between the spatial pulse length (SPL), pulse duration, and pulse repet i t ion period in a pulsed ultrasound system.
FIGURE 5. Geometric relation of spatial pulse length to axial resolu- tion.
FIGURE 6. Effect of beam width on lateral resolution. A wide beam is unable to resolve a small defect in reflecting surface.
of resolution (Figure 5). Consider the case of two reflecting surfaces sepa-
18:12 December 1989 Annals of Emergency Medicine 1293/61

ULTRASOUND & ECHOCARDIOGRAPHY Plummer
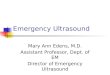
FIGURE 7. Large acute traumatic hemopericardiurn with evidence of cardiac tamponade.
rated by a distance that is less than the SPL. When the beam contacts the first ref lect ing surface, i t forms an echo and par t i a l ly t r ansmi t s to the second surface. The second reflecting surface generates a second echo. The two echoes re turn to the transducer, overlapping one another, and the ma- chine is unable to resolve a differ- ence between these two surfaces. On the o ther hand, if the d i s tance be- tween the two surfaces exceeds the SPL, the echoes gene ra t ed by each surface travel back to the t ransducer s p a t i a l l y s epa ra t ed . T h e s e echoes will arrive at different t imes, and the machine wil l resolve these two sur- faces.
The geometry of this re la t ionship dictates that the m i n i m u m axial res- olut ion is equal to SPL/2. Therefore, to improve axial resolution, the SPL must be at a m i n i m u m . Because the SPL is the sum of the wavelengths in a pulse, reducing the SPL requires ei- ther a reduct ion in the number of ul- trasound cycles or a reduct ion of the wavelength of the u l t rasound wi th in the pu l se . M o s t i n s t r u m e n t s use pulses containing only two cycles per pulse. Therefore, these i n s t r u m e n t s reduce the SPL by d e c r e a s i n g the wavelength of the u l t rasound in the pulse. However, this requires increas- ing the frequency, wh ich resul t s in faster beam a t t enua t ion . Therefore, there is an inverse relat ion be tween axial reso lu t ion and t i ssue penetra- t ion of the beam.
La te ra l r e s o l u t i o n is d e p e n d e n t only on the width of the beam. The importance of beam wid th is shown (Figure 6). C o n s i d e r the case of a wide beam scanning across a reflect- ing surface that contains a small de- fect. As the beam encounters the de- fect, there is always at least a part ial echo generated by the surface. The u l t rasound machine , therefore, does not resolve the defect. On the other hand, if a na r row b e a m scans the same surface, there wil l be a poin t at which no echo returns, and the ma- chine wil l resolve this defect.
As a result, narrowing of the beam becomes impor tant in lateral resolu- tion. His tor ical ly , u l t rasonographers used smal ler p iezoe lec t r ic e l emen t s t o achieve narrow ul t rasound beams. However, even wi th small elements,
the beam wid th even tua l ly widens. A l t h o u g h dev ices such as acous t i c lenses he lp m i n i m i z e beam widen- ing, they are unable to e l imina te it. As a r e su l t , l a t e r a l r e s o l u t i o n re- ma ined poor ly con t ro l led un t i l the in t roduct ion of the l inear phased-ar- ray (LPA) transducer. The LPA trans- d u c e r c o n s i s t s of m a n y s m a l l piezoelectr ic e lements that pulse as a group but wi th a smal l temporal dis- persion. The m a n y resu l t ing waves act through the process of reinforce- m e n t to create a s u m m a t i o n beam. T h e LPA t r a n s d u c e r c o n t r o l s t he w i d t h of the s u m m a t i o n beam by cont ro l l ing the phase differences of the i nd iv idua l e lements . Both axial and lateral resolut ion range between 3 and 5 mm. s
MODES The mode of operat ion refers to the
display characterist ics. In A-mode, a display dot moves from left to right, and an echo received by the trans- ducer causes a vert ical deflection. In B-mode, the vert ical pos i t ion of the dot is a func t ion of the t ime de lay from pulse generat ion to echo recep- tion; there is no real - t ime recording of the display in B-mode. M-mode re- fers to "mo t ion mode" and is B-mode when the ins t rument records dot po- si t ions over real t ime. Tradit ionally, M-mode devices accompl ish this by producing paper s tr ip-charts that re- cord the depths of reflecting surfaces. However , these three modes are all one -d imens iona l and diff icul t to in-
terpret. As a result, they are not often useful in the ED.
T w o - d i m e n s i o n a l u l t r a s o u n d , or B-scan mode, consists of many sepa- rate u l t r a sound beams opera t ing in B - m o d e m o v i n g w i t h i n a s i n g l e p lane . The s y s t e m maps r e t u r n i n g echoes in both hor izonta l and verti- cal posit ions, resul t ing in a cross-sec- t ional image. The image by vir tue of i ts t w o - d i m e n s i o n a l c h a r a c t e r s im- plifies in terpre ta t ion and is useful in the ED. Two-d imens iona l scanning requires a rapidly moving beam; this is produced by e i ther a mechan ica l o s c i l l a t i n g h e a d , a m e c h a n i c a l swi tched array, or an LPA. Mechani- cal heads are large and diff icul t to use. Many diagnost ic u l t rasound sys- tems now use LPAs for this purpose. LPA transducers are smaller, lighter, and more expens ive and produce a b e t t e r i m a g i n g c a p a c i t y t h a n me- chanical transducers.
Wi th each pulse of an LPA trans- ducer, there is a changing t empora l r e l a t i on a m o n g the i n d i v i d u a l ele- m e n t s t h a t r e s u l t s in a b e a m of s l igh t ly different d i rec t ion for each pu lse . T h e i n s t r u m e n t t h e n m a p s m a n y of the beams to a f rame and displays each frame to a screen. The display densi ty refers to the number of beams in each frame and typica l ly is 120. The display usual ly changes at a rate of 30 t imes per second. Each beam in each frame requires a mini- m u m of one pulse from the machine. Therefore, to increase ei ther the den- s i ty or rate of the display, a faster
62/1294 Annals of Emergency Medicine 18:12 December 1989

TABLE. C o m m o n t e r m s in u l t r a s o u n d
Term
Frequency
Period Wavelength
Speed Impedance
Attenuation Pulse duration
Pulse repetion frequency
Spatial pulse length
Axial resolution
Lateral resolution
Display density Display rate
Definition Values
Cycles/sec 2.5 - 10
Sec/cycle Speed/frequency
m/sec 1.54 Speed/density dB/cm 1/2. frequency
Seconds
Cycles/sec 1
Wavelength.cycles
SPL/2 3 - 5
Beam width 3 - 5 Beams/frame 120
Frames/sec 30
Units
MHz
mm/ms rayle
dB/cm
o
KHz
mm
mm
pulse rate requiring a higher pulse repetition f requency is necessary. This can be accomplished only by in- creasing the frequency of the ultra- sound. This, in turn, decreases the ability of the ultrasound to penetrate tissue. Therefore, there is an inverse relationship between display quality and tissue depth.
The amplifier is the component of the system between the pulse genera- tor and the display. It controls the gain, compensat ion, and rejection. The gain controls the overall power of the amplification of any incoming signal. Adjusting the gain adjusts the overall brightness of the display. The compensation reduces the effects of attenuation, and adjusting the com- pensation changes the brightness at selected depths. Rejection controls the threshold of echo signal dis- played. This changes the amount of noise on the display.
The main characteristics of ultra- sound, higher frequency, can be sum- marized as bet ter resolut ion, im- proved display quality, and decreased tissue penetration of the beam. Con- trols routinely avai lable on ul tra- sound machines are gain for control of amplifier power, compensation for reducing the effects of attenuation, noise suppression, depth, and fre- quency.
ED ECHOCARDIOGRAPHY With an understanding of the prin-
ciples and limitations of ultrasound, a wide var iety of l imited imaging techniques can be learned quickly. Probably the most compelling reason for emergency physicians to learn ul- t rasound techniques is to perform emergency 2-DE, by which the heart can be assessed rapidly for imme- diately l i fe-threatening conditions. Furthermore, it is a simple examina- tion to learn because there are only a few windows. Each window is either above, between, or below the ribs.
There are constraints in emergency medicine that require modification of the standard 2-DE examinat ion. For example, it is difficult to image an agitated or immobilized patient; as a result, there is no standard ex- amination. 9 The examination is an interact ive process requiring mod- ification depending on the patient 's presentation. A goal-directed exam- ination is brief and requires less than ten minutes, lo
Echocardiographic windows refer to the planes used to visualize the heart, which are subcostal, left para-" sternal, apical, right parasternal, and suprasternal notch.l l Only the first three have consistently yielded valu- able information in the ED.
The subcostal window is the pre- ferred view. This view is obtained by placing the transducer in the sub- xyphoid area and directing the plane of the beam scan toward the left shoulder. The structure closest to the
transducer is the right ventricle. The anterior per icardium appears as an echogenic interface between the right ventricle and the liver. This is the most useful view in many clinical presentations because it is most in- dependent of the patient's condition and cooperat ion. Frequently, this view is sufficient for a goal-directed emergency examination. 12 It yields information on cardiac activity, peri- cardial fluid, gross a s sessmen t of ventr icular chamber size, and con- tractility.
The left parasternal window con- sists of both long- and short-axis views. Each view requires placement of the transducer in the left second or third intercostal space. The long-axis view results by directing the plane of the scan in the long axis of the heart. The structures seen are the large left ventricle, the left a t r ium wi th the mitral valve, and the aortic outflow. The right ventricle is small and clos- est to the transducer. Obtain the left parasternal short-axis view by direct- ing the plane of the scan in the short axis of the heart. In this view, the most evident finding is the round left ventricle, the thick intraventricular sep tum, and the c re scen t - shaped right ventricle. This view also dem- onstrates the papillary muscles and mitral valve apparatus.
Obtain the apical view by placing the transducer on the point of maxi- m u m impulse (PMI) and directing the plane of the scan through the in- tercostal space. The resulting four- chamber view is useful for identifica- tion of intracardiac masses as well as the intraventricular septum and in- tra-atrial septum. The transducer is closest to the apex of the heart ; therefore, the screen displays the heart upside down. Patients who are obese, well muscled, or uncoopera- tive or have chronic obstructive pul- monary disease, or chest wall defor- mities hinder the operator's visual- ization in both the parasternal and apical windows.
The right parasternal and supra- sternal windows are technically diffi- cult v iews and not rou t ine ly per- formed in the ED.
ED echocardiography is goal di- rected. Depending on the clinical pre- sentation, examiners seek evidence for very specific abnormalities. The most common immediate goals are to determine cardiac function, to find evidence of pericardial disease, or to
18:12 December 1989 Annals of Emergency Medicine 1295/63

ULTRASOUND & ECHOCARDIOGRAPHY Plummer
look for complicat ion of trauma. Much less frequently, examiners look for evidence of pulmonary em- bolism, great vessel disease, or major structural abnormalities.
The most immediate use is to de- termine the presence of cardiac mo- t ion in clinical e lect romechanical dissociation (EMD). Identification of cardiac activity in patients in clinical EMD results in further pursuit of re- versible (noncardiac) etiologies for this condition. The absence of car- diac activity (true EMD) is a poor prognostic sign and may be useful in the early termination of resuscitation efforts. Furthermore, it aids in assess- ing mechanical capture in patients undergoing transcutaneous external cardiac pacing.
2-DE is useful for immediate eval- uation of hemodynamic status. In pa- tients with hypotension or shock, 2-DE noninvasively assesses cardiac regional and global inotropic state. Often, the finding of good global ac- tivity aids in focusing on a hypo- volemic or high-output etiology. Pa- tients in cardiogenic shock display findings on echocardiography that aid in early diagnosis and treatment. The finding of right ventricular hypo- kinesis wi th good left ventr icular function allows the careful delivery of a volume bolus before pulmonary artery catheterization. 1°,~3 Poor left ventricular activity requires an ear- lier application of cardiac inotropic agents.
2-DE is an important adjunct in di- agnosing myocardial dysfunction in the evaluation of patients with chest pain. 14-19 This is especially useful in patients with nondiagnostic chest pain, nondiagnostic ECGs, or sus- pected silent ischemia. As many as 90% of acute cardiac patients have adequate in i t ia l 2-DE examina- tions, l° Findings such as regional or global wall mot ion abnormalities, pericardial fluid, or major structural abnormality help in treatment and disposition decisions. Indications for thrombolytic therapy in the future may include acute echocardiographic findings.
2-DE is useful in detecting pericar- dial disease such as pericardial effu- sion or acute hemopericardium in emergency patients. 2-DE is faster and easier than M-mode echocar- d iography for de tec t ing and lo- calizing pericardial effusion fluid, z°
Routine 2-DE in trauma is useful.
Up to 33% of patients with penetrat- ing chest injury have clinically silent hemopericardium (Figure 7). 21 Other important findings include regional wall abnormalities, pneumopericar- dium, or intrathoracic foreign body. 22 Rarer findings include extracardiac mediast inal or intracardiac hema- toma.23, 24 2-DE visualizes both clot- ted and u n c l o t t e d hemoper i ca r - dium. 2s Only computed tomography (CT} scan and magnetic resonance imaging (MRI) rival 2-DE for the non- invasive diagnosis of hemopericar- dium. Both CT and MRI have signifi- cant limitations but are useful ad- juncts to 2-DE in ques t ionab le c a s e s . 26-28
Cardiac c o n t u s i o n f rom b lun t trauma is difficult to diagnose. ECG, nuclear imaging, and enzymatic and physical characterist ics have low specificity and sensitivity.~9, 3o Alter- natively, 2-DE provides an immedi- ate noninvasive assessment of car- diac contusion. 31,32 In consecutive patients with blunt trauma, Reid noted that 18% with previously un- suspected hemopericardium and 6% with regional wall abnormalities. 21
Selected patients receive echocar- diography to search for evidence of massive pulmonary embolus, mani- fested on echocardiography as acute cor pulmonale demonstrated by a di- lated nonhypertrophied right ventri- cle, 33 right ventricular hypokinesis, 34 paradoxic intraventr icular septum motion, 35 and, rarely, right-sided thrombus. 36-39 These abnormalities may present in patients with EMD, shock of unknown etiology, or any significant respiratory impairment. Most authors support the liberal use of 2-DE in these settings. 4°
2-DE is capable of demonstrating evidence of acute aortic dissection or rupture; this is particularly valuable because these disorders have very high mortali ty rates that increase with time to diagnosis. 41 A common finding in this event is acute hemo- pericardium, which results from ret- rograde dissection of the hematoma. Other findings include identification of an intimal tear either as a flap or double linear density42, 4g or aortic root dilation; 44 2-DE is very sensitive in the diagnosis of these disor- ders. 45-4s Rarely, 2-DE will demon- strate aortic dissection even in the presence of a normal aortography. 49 This examination is particularly im- portant in trauma patients, s°
2-DE is sensitive in the detection of certain types of major structural abnormalities, including aneurysm, pseudoaneurysm, myocardial rup- ture, and mural thrombus. These are all complications of either ischemic heart disease or chest trauma and are often seen by emergency physicians. These conditions carry an extremely high mortality rate and require early and preferably non invas ive diag- nosis, sl-53 These abnormalities may be demonstrated on patients with he- modynamic instability.
Similar abnormalities may present in patients suspected of having com- p l i c a t i o n s f r o m i n v a s i v e pro- cedures, s4 Patients demonstrating a worsening hemodynamic state after central venous catheter placement, pulmonary arterial catheterization, or t r ansvenous pacer p l acemen t should receive immediate 2-DE.
SUMMARY Since the introduction of 2-DE to
the Hennepin County Medical Cen- ter ED, 8% of the scans have been technically inadequate. Inadequate examinations most frequently result from patient agitation, positioning of the patient, obesity, or chronic ob- structive pulmonary disease. Also, concurrent procedures, such as con- trol venous line placement or peri- toneal lavage, occasionally interfere with availability of standard echo windows. Further, the equipment is large and difficult to place in prox- imity to the critically ill patient. Pos- itive examinations are always com- pleted within five minutes of arrival. Because 2-DE confirms or excludes immediately life-threatening condi- tions, the scans have contr ibuted greatly to the immediate care of the patients.
2-DE resolves difficult issues in the ED evaluation and treatment of critical patients. Emergency physi- cians have demonstrated the ability to perform and interpret this test. It has lead to the earlier finding of life- threatening conditions and has re- duced the number of invasive diag- nostics, s4 Formal determination of the impact of ED 2-DE on patient outcome requires further research.
REFERENCES 1. Mayron R, Gaudio FE, Plummet D, et al: Echocardiography performed by emergency phy- sicians: Impact on diagnosis and therapy. Ann Emerg Med 1988;17:150-154. 2. Kremkau FW: Education in the physics of di-
64/1296 Annals of Emergency Medicine 18:12 Oecember 1989

agnostic ultrasound: Is it necessary? Appl Ra- dioI 1981;10:112.
3. Berman MC: Defining the role of the so- n0grapher. Med Ultrasound 1984;8:55-60.
4. Gross SA, Johnson RL, Dunn F: Comprehen- sive compilation of empirical ultrasonic proper- ties of mammalian tissues. J Acoust Soc Am 1980;68:93-108.
5. Nyborg WL, Ziskin MC: Biological Effects of Ultrasound. New York, Churchill Livingstone, 1985.
6. Cartensen EL, Gates AH: The effects of pulsed ultrasound on the fetus. J Ultrasound Med 1984;3:145.
7. Stark CR, Orleans M, Havercamp AD, et ah Short- and long-term risks after exposure to di- agnostic ultrasound in utero. Obstet Gynecol 1984;63:194.
8. Erbel R, Rohmann S, Drexler M, et ah Im- proved diagnostic value of echocardiography in patients with infective endocarditis by transoe- sophageal approach: A prospective study. Eur Heart J 1988;9:43-S3.
9. Pearlman AS, Gardin JM, Martin RP, et ah Guidelines for optimal physician training in echocardiography: Recommendat ions of the American Society of Echocardiography Com- mittee for Physician Training in Echocardiogra- phy. Am J Cardiol 1987;60:1.
10. Schwarz KQ, Meltzer RS: Experience round- ing with a hand-held two-dimensional cardiac ultrasound device. A m J Cardiol 1988~62: 157-159. 11. Henry WL, Demaria A, Gramiak R, et ah Report of the American Society of Echocar- diography, Commit tee on Nomenclature and Standards in Two-Dimensional Echocardiogra- phy. Circulation 1980;62:212-217.
12. Nasser FN, Giuliani BR: Clinical Two-di- mensional Echocardiography. Chicago, Year- Book Medical Publishers, 1983, p 8.
13. Dobrac M, Morgan CD, Gilbert BW: Com- plicated acute myocardial infarction: The im- portance of two dimensional echocardiography. Am [ Cardiol 1979;43:387.
14. Heger JJ, Weyman AE, Warm LS, et ah Cross-sectional echocardiography in acute myo- cardial infarction: Detection and localization of regional left ventricular asynergy. Circulation 1979;60:531.
15. Weiss JL, Bulkley BH, Hutchins JM, et ah Two-dimensional echocardiographic recognition of myocardial injury in man: Comparison with pos tmor tem studies . Circulation 1981;63: 401-408.
16. Horowitz RS, Morganroth J, Parrotto C, et al: Immediate diagnosis of acute myocardial in- farction by two-dimensional echocardiography. Circulation 1982;65:323.
17. Horowitz RS, Morganroth J: Immediate de- tection of early high-risk patients with acute myocardial infarction using two-dimensional echocardiographic evaluation of left ventrieular regional wall motion abnormalities. Am Heart J 1982;103:814-822. 18. Gibson RS, Bishop HL, Stamm RB, et ah Value of early two-dimensional echocardiogra- phy in patients with acute myocardial infarc- tion. Am J Cardiol 1982;49:1110.
19. Kloner RA, Parisi AF: Acute myocardial in- farction: Diagnostic and prognostic applications of two-dimensional echocardiography. Circula-
tion 1987;75:521.
20. Martin RP, Rakowski H, French J~ et ah Lo- calization of pericardial effusion with wide an- gle phased array echocardiography. Am f Car- diol 1978;42:904-912.
21. Reid CL, Kawanishi DT, Rahimtoola SH, et ah Chest trauma: Evaluation by two-dimen- sional echocardiography. A m Heart [ 1987; 113:971-976.
22. Whye D, Barish R, Almquist T, et al: Echo- cardiographic diagnosis of acute pericardial effu- sion in penetrating chest trauma. Am J Emerg Med 1988;6:21-23.
23. Schabelman SE, Ferdinand K, Poler M: Echocardiographic findings in a patient with tamponade due to anterior mediastinal hema- toma. South Med f 1983;76:1309-1311.
24. Berkery W, Hare C, Warner RA, et ah Non- penetrating traumatic rupture of the tricuspid valve: Formation of ventricular septal aneurysm and subsequent septal necrosis: Recognition by two-dimensional Doppler echocardiography. Chest 1987;91:778-780.
25. Lopez SJ, Garcia F, Coma C, et al: Identi- fication of blood in the pericardial cavity in dogs by two-dimensional echocardiography. Am J Cardiol 1984~53:1194-1197.
26. Yousem D, Traill TT, Wheeler PS, et ah Il- lustrative cases in pericardial effusion misdetec- tion: Correlation of echocardiography and CT. Cardiovasc Intervent Radio1 1987;10:162-167.
27. Isner IM, Carter BL, Bankoff MS, et ah Computed tomography in the diagnosis of peri- cardial heart disease. Ann Intern Med 1982;97: 473-479.
28. Sechtem U, Tscholakoff D, Higgins CB: MRI of the a b n o r m a l pe r i ca rd ium. A m f Roentgenol 1986;147:245-252.
29. Potkin RT, Werner JA, Trobaugh GB, et ah Evaluation of noninvasive techniques in sus- pected cardiac contusion. Circulation 1982;66: 627.
30. Lindenbaum GA, Carroll SF, Block EF, et ah Value of creatine phosphokinase isoenzyme de- te rminat ions in the diagnosis of myocardial contusion. Ann Emerg Med 1988;17:885-889.
31. Miller FA Jr, Seward JB, Gersh BI, et al: Two-dimensional echocardiographic findings in ca rd iac t r a u m a . A m J Cardiol 1982;50: 1022-1027.
32. Markiewicz W, Best LA, Burstein S, et ah Echocard iograph ic eva lua t i on after b lun t t r auma of the chest . Int J Cardiol 1985;8: 269-274.
33. Come PC: Echocardiographic recognition of pulmonary arterial disease and determination of its cause. Am J Med 1988;84:384-394.
34. Kasper W, Meinertz T, Henkel B, et ah Echocardiographic findings in patients with proved pu lmona ry embol i sm. A m Heart J 1986;112:1284-1290.
35. Vardan S, Mookherjee S, Smulyan HS, et al: Bchocardiography in pulmonary embolism. Jpn Heart J 1983;24:67-78.
36. Saner HE, Asinger RW, Daniel JA, et ah Two-dimensional echocardiographic detection of right-sided cardiac intracavitary thromboem- bolus with pulmonary embolism. J Am Coll Cardiol 1984;4:1294-1301.
37. Di Carlo LA, Schiller NB, Herfkens RL, et ah Noninvasive detection of proximal pulmo-
Annals of Emergency Medicine
nary artery thrombosis by two-dimensional echocardiography and computerized tomogra- phy. Arn Heart J 1982;104:879-881.
38. Farfel Z, Shechter M, Vered Z, et ah Review of echocardiographically diagnosed right heart en t rapment of pulmonary emboli- in- transi t with emphasis on management. Am Heart [ 1987;113:171-178.
39. Chakko S, Richards F: Right-sided cardiac thrombi and pulmonary embolism. Am f Car- diol 1987;S9:195-196.
40. Goldhaber SZ: Optimal strategy for diag- nosis and treatment of pulmonary embolism due to right atrial thrombus. Mayo Clin Proc 1988;63:1261-1264.
41. Wheat MW: Acute dissecting aneurysms of the aorta: Diagnosis and treatment - 1979. Am Heart I 1980;99:373-387.
42. Roudaut RP, Billes MA, Gosse P, et ah Ac- curacy of M-mode and two-dimensional echo- cardiography in the diagnosis of aortic dissec- tion: An experience with 128 cases. C1in Car- diol 1988;1:553-562.
43. Nanda NC, Gramiak R, Shah PM: Diag- nosis of aortic root dissection by echocardiogra- phy. Circulation 1975;48:11-17.
44. DeMaria AN, Bommer W, Neumann A, et ah Identification and localization of aneurysms of the ascending aorta by cross-sectional echo- cardiography. Circulation 1979;59:755-761.
45. Dubourg O, Delorme G, Gueret P, et al: Di- agnosis of acute aortic dissection by echocar- diography. Arch Mal Coeur 1988;81:21-25.
46. Roudaut R, Billes MA, Gateau P, et al: Diag- nosis of dissecting aortic aneurysm by two di- mensional echocardiography: Experience with 58 patients. Ultrasound Med Biol 1983;(suppl 2):325-330.
47. Diehl JT, Kaiser LR, Howard RJ, et al: Two- dimensional echocardiography for diagnosing acute ascending aortic dissection. Can J Surg 1985;28:345-347.
48. McLeod AA, Monaghan MJ, Richardson PJ, et ah Diagnosis of acute aortic dissection by M-mode and cross-sectional echocardiography: A five-year experience. Eur Heart J 1983; 4:196-202.
49. Metz D, Chabert JP, Beruben E, et al: Aortic dissection with normal aortography and x-ray computed tomography: A diagnostic trap not to be ignored. Ann Cardiol 1988;37:187-190.
50. yon Doenhoff LJ, Nanda NC: Chronic trau- matic thoracic aneurysm: Demonst ra t ion by two-dimensional echocardiography. [ Cardiol 1984;54:692-693.
51. Gueron M, Wanderman KL, Hirsch M, et ah Pseudoaneurysm of the left ventricle after myo- cardial infarction: A curable form of myocardial rupture. [ Thorac Cardiovasc Surg 1975;69:736.
52. Yoshikiro MA, Ortiz J, Nanda NC: Left ven- tricular pseudoaneurysm due to penetrating in- jury of the chest: An echocardiographic diag- nosis. Am Heart J 1988;115:1134-1136.
53. Pijls NHJ, Fast JH, van der Meet JJ, et ah Biventricular free wall rupture with extracar- diac left-to-right shunt after myocardial infarc- tion. Am Heart J 1988;115:186-189.
54. Iliceto S, Antonelli G, Sorino M, et ah Two- dimensional echocardiographic recognition of complications of cardiac invasive procedures. Am f Cardiol 1984;53:846-848.
18:12 December 1989 1297/65