Embed Size (px)
Citation preview

BJU International (1999), 83, 515–516
CASE RE PORT
Primitive neuroectodermal tumour of the adrenal glandY. MATSUOKA, Y. FUJII , T. AKASHI*, N. GOSEHI† and K. KIHARADepartments of Urology, *Pathology and †Surgery, Tokyo Medical and Dental University School of Medicine, Tokyo, Japan
cytoplasm, partially forming distinct Homer WrightCase report
rosettes (Fig. 2a). Immunohistochemical stains werepositive for MIC2 (CD99) (cytoplasmic surface membraneA 32-year-old woman presented with a 4-month history
of abdominal pain. On physical examination, a huge staining, Fig. 2b) and NSE, providing evidence of aprimitive neuroectodermal tumour (PNET). The patientfirm mass was palpable at the left epigastrium.
Laboratory studies revealed high serum LDH and neuron- underwent two courses of adjuvant chemotherapy withetoposide, ifosfamide and cisplatin. However, she died 5specific enolase (NSE) levels of 4070 U/L and 13 ng/mL
(normal range <10), respectively. CT showed a 10 cm months after surgery with progression of local recur-rence, and liver, lung and brain metastases.mass in the left retroperitoneal area, with multiple liver
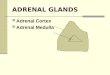
metastases. The patient underwent surgery and the largemass of the adrenal gland adherent to the surroundingtissue was removed, together with the left kidney (Fig. 1).The tumour tissue consisted of monomorphic cellswith round to oval nuclei and abundant eosinophilic
a
b
Fig. 2. a, The histological pattern of the tumour includes extensiveHomer-Wright rosette formation by monomorphic malignant small
Fig. 1. The gross specimen of the adrenal tumour and left kidney. cells. Haematoxylin and eosin, reduced from ×200. b, Intensemembrane-associated staining of tumour cells with anti-MIC2The tumour has a fibrous capsule adhering to the kidney, and its
central area is necrotic and hyalinized. antibody. Reduced from ×200.
515© 1999 BJU International

516 CASE REPORTS
Further study will reveal the true incidence of adrenalComment
PNET and its clinical characteristics.The Ewing family of tumours, consisting of classicalEwing’s sarcoma and PNET, is the second most common
Acknowledgementmalignant bone tumour in children and adolescents [1].These tumours can also occur in soft tissue, commonly
The authors gratefully acknowledge Dr Hiroyuki Oshima,in the chest wall and paraspinal region, and rarely from
Professor of Urology, Tokyo Medical and Dentalan organ [2]. Only three cases of PNET arising in the
University School of Medicine, for his helpful comments.adrenal gland have been reported, all of whom diedwithin a year of presentation [3]. The Ewing’s tumoursbelong to the group of neoplasms commonly referred to
Referencesas ‘small round cell’ tumours, including neuroblastoma,
1 Grier HE. The Ewing family of tumors. Ewing’s sarcoma andrhabdomyosarcoma and non-Hodgkin’s lymphoma [1].primitive neuroectodermal tumors. Pediat Clin North Am
DiCerentiating them is occasionally diBcult, especially in1997; 44: 991–1004
the soft-tissue variants. It is possible that PNETs in the 2 Marley EF, Liapis H, Humphrey PA et al. Primitive neuroecto-adrenal gland have been missed to date because of its dermal tumor of the kidney — another enigma: a pathologic,histological similarity to neuroblastoma. Recent molecu- immunohistochemical, and molecular diagnostic study. Amlar and genetic studies have revealed that classical J Surg Pathol 1997; 21: 354–9
3 Marina NM, Etcubanas E, Parham DM, Bowman LC, Green A.Ewing’s sarcoma and PNET are the same tumour withPeripheral primitive neuroectodermal tumor (peripheralvariable cell diCerentiation, defined by a unique charac-neuroepithelioma) in children. Cancer 1989; 64: 1952–60teristic translocation t(11;22) or its variation within the
4 Fellinger EJ, Garin CP, Triche TJ, Huvos AG, Rettigtumour cell [1]. Molecular techniques used to identifyWJ. Immunohistochemical analysis of Ewing’s sarcoma cellthis translocation have greatly improved diagnoses insurface antigen p30/32MIC2 . Am J Pathol 1991; 139: 317–25this family of tumours. Additionally, immunoreactivity
for the MIC2 gene product, a cell surface glycoprotein,is also known to be useful in distinguishing Ewing’s
Authorstumours from the other small round-cell tumours; onlyY. Matsuoka, MD, Urologist in training.Ewing’s tumours are reported to be positive for MIC2Y. Fujii, MD, StaC Urologist.[1,4]. Of the Ewing family, the PNET variant showsT. Akashi, MD, StaC Pathologist.
considerable neuroectodermal diCerentiation [1]. In theN. Goseki, MD, Assistant Professor.
present case, this diCerentiation was indicated by high K. Kihara, MD, Assistant Professor.serum levels and tumour staining of NSE, and rosette Correspondence: Dr Y. Fujii, Department of Urology, Tokyoformation. This is the first case of PNET arising in the Medical and Dental University,1-5-45, Yushima, Bunkyo-ku,adrenal gland confirmed by immunoreactivity for MIC2. Tokyo 113, Japan.
© 1999 BJU International 83, 515–516






![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://img.dokumen.tips/doc/110x75/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)