Embed Size (px)
Citation preview

219Saudi Journal of Medicine & Medical Sciences | Vol. 2 | Issue 3 | December 2014 | 219-222
Primitive Neuroectodermal Tumor of the Kidney: Case Report in a 13 Year-Old Boy
Hamed M. El-DarawanyDepartment of Urology, King Fahd Hospital of the University, University of Dammam, Al-Khobar, Kingdom of Saudi Arabia
Correspondence: Dr. Hamed M. El-Darawany, King Fahd Hospital of the University, University of Dammam, P.O. Box 40076, Al-Khobar 31952, Kingdom of Saudi Arabia. E-mail: [email protected]
CASE REPORT
INTRODUCTION
Primitive neuroectodermal tumor (PNET) is a small, round-cell neoplasm that represents about 1% of all sarcomas. It affects cerebral and cerebellar tissues and is considered to be a neural crest derivative.[1] PNET was fi rst described by Stout in 1918.[2] In 1975, Seemayer was the fi rst to report PNET in the kidney.[3] It closely resembles Ewing’s Sarcoma and is diffi cult to be differentiated from it.[4] Renal PNET occurs more frequently during the childhood or adolescence with an aggressive behavior. It often recurs locally and metastasizes early to regional lymph nodes, lungs, liver, bone and bone marrow with poor prognosis.[5] The diagnosis of
PNET is based on a combination of electron microscopy, immunohistochemistry, chromosomal analysis, FISH, and light microscopy.[6]
CASE REPORT
This was a case report of a 13-year-old boy who was transferred to the “Emergency Room” with severe acute right loin pain for a few hours. There was no history of a similar attack or any comorbid diseases. The surgical team made a diagnosis of acute appendicitis based on the right iliac fossa pain with rebound tenderness. He was scheduled for appendectomy. Through a Mcburny incision, a normal appendix with hemoperitonium was noticed. A right paramedian incision was performed to detect the source of bleeding. A bleeding right retroperitoneal mass related to the kidney was detected. Evaluation of the retroperitoneal mass by urology team revealed an upper pole right renal mass with infi ltration of the posterior peritoneum. A biopsy was taken from the mass, bleeding was controlled and the abdomen was closed. Post-operative computed tomography (CT) scan revealed a huge mass originating from the upper
Access this article onlineQuick Response Code:
Website:www.sjmms.net
DOI:10.4103/1658-631X.142584
A B S T R A C T
A 13-year-old boy presented with acute right loin pain. Computed tomography scan showed a huge mass originating from the upper pole of the right kidney. Right radical nephrectomy was performed. Histopathological examination revealed a neuroectodermal tumor of the kidney. There was local and lymph node invasion as well as distant metastasis to the lungs, liver and bone. The patient died 18 months from the time of initial diagnosis. Nearly 94% of primitive neuroectodermal tumor shows the complete response to combined surgery, radiation and chemotherapy. However, in the presence of metastases, the 5-year survival drops to 29%.
Key words: Extra osseous, kidney, primitive neuroectodermal tumor, Wilms
ملخص البحث :
يعرض هذا التقرير حالة لصبي في الثالثة عشرة من عمره كان يعاني من ألم حاد في الخاصرة. وضحت الأشعة المقطعية كتلة كبيرة في أعلى الكلية اليمنى. تم إزالة ألكلية اليمنى. وضح الفحص المجهري ورم الأديم العصبي الظاهر. وقد وجد أن المرض تغلغل موضعياً وأصاب الغدد
اللمفاوية والرئتين والكبد والعظام. توفي المريض بعد 18 شهرًا من التشخيص المبدئي بسبب انتشار المرض في الجسم ، علمًا بأن البقاء على قيد الحياة لمدة خمس سنوات في مثل هذه الحالات لا يتجاوز 29%.
[Downloaded free from http://www.sjmms.net on Thursday, March 03, 2016, IP: 197.163.82.182]
El-Darawany H: Primitive neuroectodermal tumor of the kidney
Saudi Journal of Medicine & Medical Sciences | Vol. 2 | Issue 3 | December 2014 220
and cords of neoplastic cells were noticed arranged around blood vessels. The cells had plumped vesicular nuclei, mild pleomorphic inconspicuous nucleoli and frequent mitoses. Some cells had clear and others had eosinophilic cytoplasm with indistinct cell borders. The lymph nodes were invaded by tumor cells. This picture was consistent with a malignant high grade round cell tumor (high monomorphic blast cell Wilms’ versus clear cell sarcoma of the kidney). The tumor was stage III, T2N1M0 tumor). Immunohistochemical staining (CD99) confi rmed sarcoma of the kidney. It had features that suggested a PNET. Due to a local and lymph node invasion, the patient was referred to Medical Oncology for chemo-radiotherapy. One year later, the patient had surgical excision of a local recurrence. It was followed by a second course of chemotherapy and radiotherapy. The patient developed local as well as distant bone, lung and liver metastases, and died 18 months from the initial diagnosis.
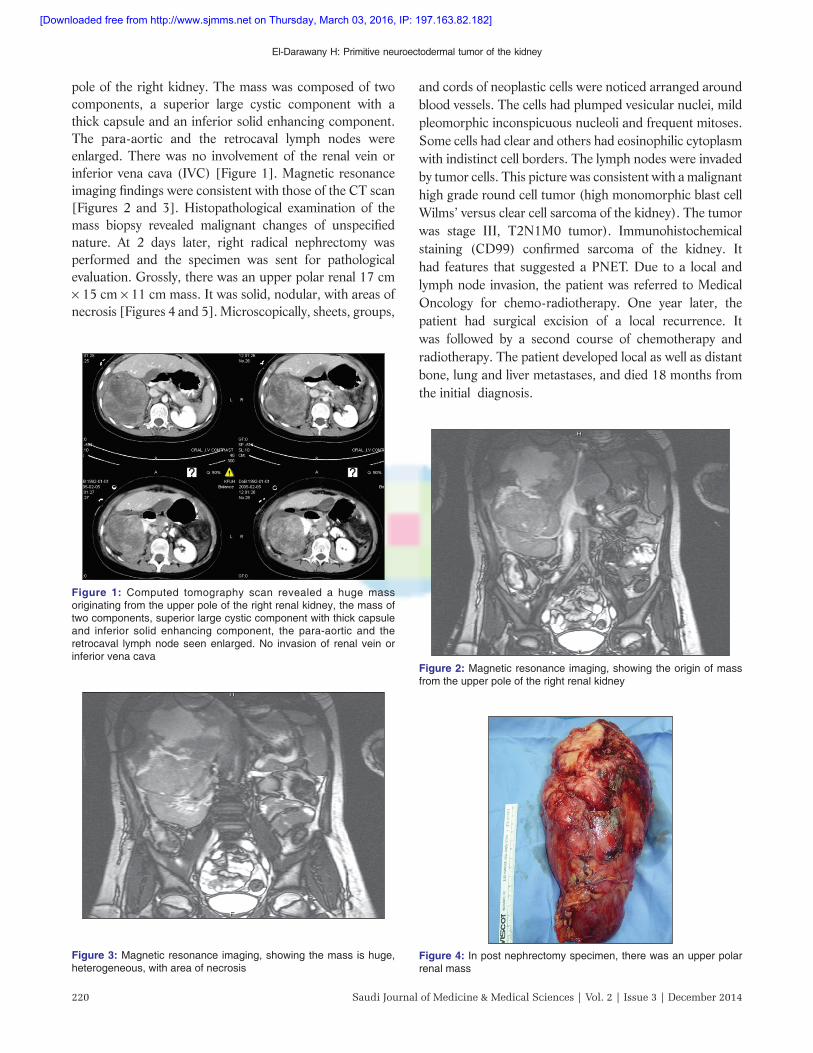
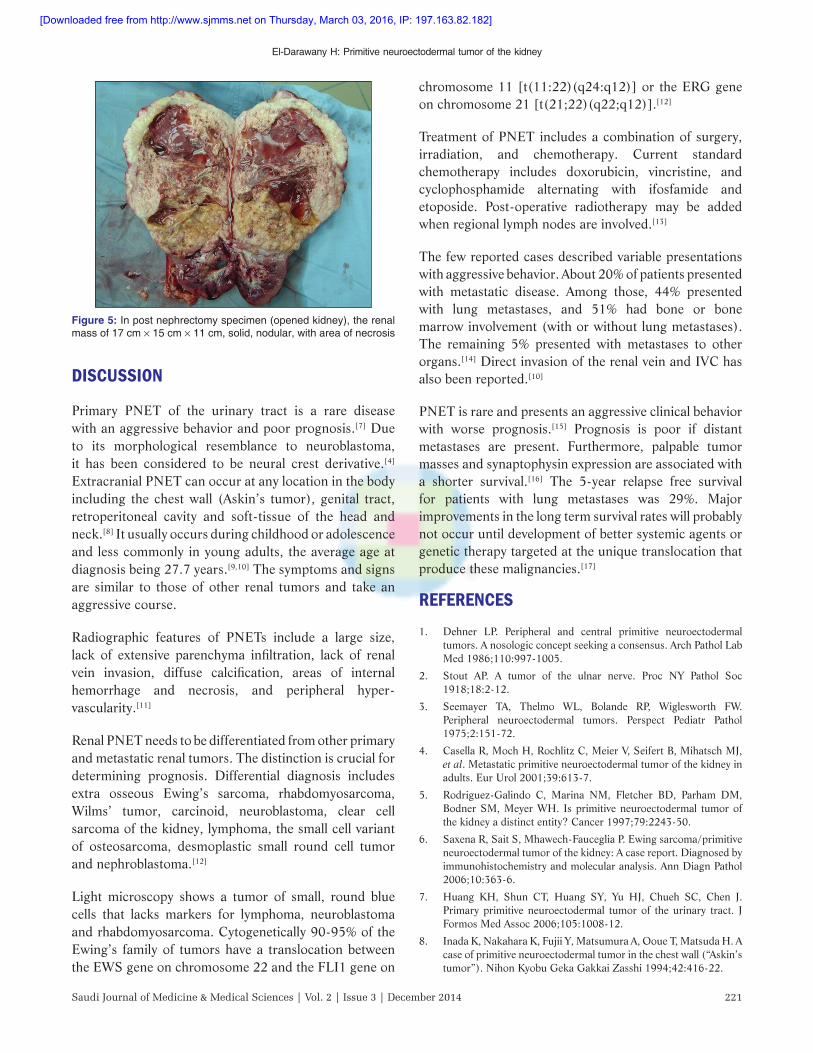
pole of the right kidney. The mass was composed of two components, a superior large cystic component with a thick capsule and an inferior solid enhancing component. The para-aortic and the retrocaval lymph nodes were enlarged. There was no involvement of the renal vein or inferior vena cava (IVC) [Figure 1]. Magnetic resonance imaging fi ndings were consistent with those of the CT scan [Figures 2 and 3]. Histopathological examination of the mass biopsy revealed malignant changes of unspecifi ed nature. At 2 days later, right radical nephrectomy was performed and the specimen was sent for pathological evaluation. Grossly, there was an upper polar renal 17 cm × 15 cm × 11 cm mass. It was solid, nodular, with areas of necrosis [Figures 4 and 5]. Microscopically, sheets, groups,
Figure 1: Computed tomography scan revealed a huge mass originating from the upper pole of the right renal kidney, the mass of two components, superior large cystic component with thick capsule and inferior solid enhancing component, the para-aortic and the retrocaval lymph node seen enlarged. No invasion of renal vein or inferior vena cava
Figure 2: Magnetic resonance imaging, showing the origin of mass from the upper pole of the right renal kidney
Figure 3: Magnetic resonance imaging, showing the mass is huge, heterogeneous, with area of necrosis
Figure 4: In post nephrectomy specimen, there was an upper polar renal mass
[Downloaded free from http://www.sjmms.net on Thursday, March 03, 2016, IP: 197.163.82.182]
El-Darawany H: Primitive neuroectodermal tumor of the kidney
221Saudi Journal of Medicine & Medical Sciences | Vol. 2 | Issue 3 | December 2014
DISCUSSION
Primary PNET of the urinary tract is a rare disease with an aggressive behavior and poor prognosis.[7] Due to its morphological res emblance to neuroblastoma, it has been considered to be neural crest derivative.[4] Extracranial PNET can occur at any location in the body including the chest wall (Askin’s tumor), genital tract, retroperitoneal cavity and soft-tissue of the head and neck.[8] It usually occurs during childhood or adolescence and less commonly in young adults, the average age at diagnosis being 27.7 years.[9,10] The symptoms and signs are similar to those of other renal tumors and take an aggressive course.
Radiographic features of PNETs include a large size, lack of extensive parenchyma infi ltration, lack of renal vein invasion, diffuse calcifi cation, areas of internal hemorrhage and necrosis, and peripheral hyper-vascularity.[11]
Renal PNET needs to be differentiated from other primary and metastatic renal tumors. The distinction is crucial for determining prognosis. Differential diagnosis includes extra osseous Ewing’s sarcoma, rhabdomyosarcoma, Wilms’ tumor, carcinoid, neuroblastoma, clear cell sarcoma of the kidney, lymphoma, the small cell variant of osteosarcoma, desmoplastic small round cell tumor and nephroblastoma.[12]
Light microscopy shows a tumor of small, round blue cells that lacks markers for lymphoma, neuroblastoma and rhabdomyosarcoma. Cytogenetically 90-95% of the Ewing’s family of tumors have a translocation between the EWS gene on chromosome 22 and the FLI1 gene on
chromosome 11 [t(11:22)(q24:q12)] or the ERG gene on chromosome 21 [t(21;22)(q22;q12)].[12]
Treatment of PNET includes a combination of surgery, irradiation, and chemotherapy. Current standard chemotherapy includes doxorubicin, vincristine, and cyclophosphamide alternating with ifosfamide and etoposide. Post-operative radiotherapy may be added when regional lymph nodes are involved.[13]
The few reported cases described variable presentations with aggressive behavior. About 20% of patients presented with metastatic disease. Among those, 44% presented with lung metastases, and 51% had bone or bone marrow involv ement (with or without lung metastases). The remaining 5% presented with metastases to other organs.[14] Direct invasion of the renal vein and IVC has also been reported.[10]
PNET is rare and presents an aggressive clinical behavior with worse prognosis.[15] Prognosis is poor if distant metastases are present. Furthermore, palpable tumor masses and synaptophysin expression are associated with a shorter survival.[16] The 5-year relapse free survival for patients with lung metastases was 29%. Major improvements in the long term survival rates will probably not occur until development of better systemic agents or genetic therapy targeted at the unique translocation that produce these malignancies.[17]
REFERENCES1. Dehner LP. Peripheral and central primitive neuroectodermal
tumors. A nosologic concept seeking a consensus. Arch Pathol Lab Med 1986;110:997-1005.
2. Stout AP. A tumor of the ulnar nerve. Proc NY Pathol Soc 1918;18:2-12.
3. Seemayer TA, Thelmo WL, Bolande RP, Wiglesworth FW. Peripheral neuroectodermal tumors. Perspect Pediatr Pathol 1975;2:151-72.
4. Casella R, Moch H, Rochlitz C, Meier V, Seifert B, Mihatsch MJ, et al. Metastatic primitive neuroectodermal tumor of the kidney in adults. Eur Urol 2001;39:613-7.
5. Rodriguez-Galind o C, Marina NM, Fletcher BD, Parham DM, Bodner SM, Meyer WH. Is primitive neuroectodermal tumor of the kidney a distinct entity? Cancer 1997;79:2243-50.
6. Saxena R, Sait S, Mhawech-Fauceglia P. Ewing sarcoma/primitive neuroectodermal tumor of the kidney: A case report. Diagnosed by immunohistochemistry and molecular analysis. Ann Diagn Pathol 2006;10:363-6.
7. Huang KH, Shun CT, Huang SY, Yu HJ, Chueh SC, Chen J. Primary primitive neuroectodermal tumor of the urinary tract. J Formos Med Assoc 2006;105:1008-12.
8. Inada K, Nakahara K, Fujii Y, Matsumura A, Ooue T, Matsuda H. A case of primitive neuroectodermal tumor in the chest wall (“Askin’s tumor”). Nihon Kyobu Geka Gakkai Zasshi 1994;42:416-22.
Figure 5: In post nephrectomy specimen (opened kidney), the renal mass of 17 cm × 15 cm × 11 cm, solid, nodular, with area of necrosis
[Downloaded free from http://www.sjmms.net on Thursday, March 03, 2016, IP: 197.163.82.182]

El-Darawany H: Primitive neuroectodermal tumor of the kidney
Saudi Journal of Medicine & Medical Sciences | Vol. 2 | Issue 3 | December 2014 222
9. Thyavihally YB, Tongaonkar HB, Gupta S, Kurkure PA, Amare P, Muckaden MA, et al. Primitive neuroectodermal tumor of the kidney: A single institute series of 16 patients. Urology 2008;71:292-6.
10. Huang J, Zhang J, Dong B, Chen Y, Kong W, Liu Q, et al. Primitive neuroectodermal tumor of the kidney: A single-institute series of six patients from China. Urol Int 2013;90:174-8.
11. Maccioni F, Della Rocca C, Salvi PF, Manicone AM, Ascarelli A, Longo F, et al. Malignant peripheral neuroectodermal tumor (MPNET) of the kidney. Abdom Imaging 2000;25:103-6.
12. Gonlusen G, Ergin M, Paydas S, Bolat FA. Primitive neuroectodermal tumor of the kidney: A rare entity. Int Urol Nephrol 2001;33:449-51.
13. Hakky TS, Gonzalvo AA, Lockhart JL, Rodriguez AR. Primary Ewing sarcoma of the kidney: A symptomatic presentation and review of the literature. Ther Adv Urol 2013;5:153-9.
14. Cotterill SJ, Ahrens S, Paulussen M, Jürgens HF, Voûte PA, Gadner H, et al. Prognostic factors in Ewing’s tumor of bone:
How to cite this article: El-Darawany HM. Primitive neuroectodermal tumor of the kidney: case report in! a 13 year-old boy. Saudi J Med Med Sci 2014;2:219-22.
Source of Support: Nil. Confl ict of Interest: None declared.
Analysis of 975 patients from the European Intergroup Cooperative Ewing’s Sarcoma Study Group. J Clin Oncol 2000;18:3108-14.
15. Sun C, Du Z, Tong S, Xu K, Ding W, Sun J, et al. Primitive neuroectodermal tumor of the kidney: Case report and review of literature. World J Surg Oncol 2012;10:279.
16. Ellinger J, Bastian PJ, Hauser S, Biermann K, Müller SC. Primitive neuroectodermal tumor: Rare, highly aggressive differential diagnosis in urologic malignancies. Urology 2006;68:257-62.
17. Marcus RB Jr. Ewing’s sarcoma. In: Edward CH, editor. Text Book of Principles and Practice of Radiation Oncology. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2002. p. 2277-82.
Announcement
Android AppA free application to browse and search the journal’s content is now available for Android based mobiles and devices. The application provides “Table of Contents” of the latest issues, which are stored on the device for future offline browsing. Internet connection is required to access the back issues and search facility. The application is compatible with all the versions of Android. The application can be downloaded from https://market.android.com/details?id=comm.app.medknow. For suggestions and comments do write back to us.
[Downloaded free from http://www.sjmms.net on Thursday, March 03, 2016, IP: 197.163.82.182]





























