Embed Size (px)
Citation preview

Primary Surgery or Interval Debulking for AdvancedEpithelial Ovarian Cancer: Does It Matter?
Algirdas Markauskas, MD,* Ole Mogensen, MD, DMSci,* Rene dePont Christensen, PhD,Þand Pernille Tine Jensen, MD, PhD*
Objective: The aim of the present study was to investigate the surgical complexity, thepostoperative morbidity, and the survival of the women after primary debulking surgery(PDS) and neoadjuvant chemotherapy followed by interval debulking surgery (NACT-IDS)for advanced epithelial ovarian cancer.Materials and Methods: We consecutively included all patients who underwent debulkingsurgery at our institution between January 2007 and December 2012 for stages IIIc and IVofepithelial ovarian cancer.Results: Of the 332 patients included, 165 (49.7%) underwent PDS, and 167 (50.3%)had NACT-IDS. Complete intraperitoneal cytoreduction was achieved in 70.9% after PDSand in 59.9 % after NACT-IDS. Residual disease of greater than 1 cm was left in 18.5% and27.5% after PDS and NACT-IDS, respectively. Compared with NACT-IDS, PDS was as-sociated with higher surgical complexity (P G 0.001), longer operating time (P G 0.001),greater blood loss (P G 0.001), longer hospitalization (P = 0.001), and a higher rate ofmajor postoperative complications (26.7% vs 16.8%). No statistical difference in the medianoverall survival (OS) was found between the patients having complete cytoreduction andresidual disease of 1 cm or less after NACT-IDS. Furthermore, no statistical difference in themedian OS was found between the patients with macroscopic residual disease (e1 vs 91 cm)after NACT-IDS. Patients with residual disease of greater than 1 cm after PDS had a medianOS of 15 months.Conclusions: We suggest that NACT-IDSmay be a better treatment alternative for the groupof highly selected women not suitable for PDS, where expected suboptimal cytoreductiondoes not have any appreciable survival benefit and exposes them for unnecessary risks.A substantial number of women who receive either PDS or NACT-IDS have greater than1 cm of tumor tissue left after the operation. These women probably have no survival ben-efit from the operation, and future studies should focus on how to select these womenpreoperatively.
Key Words: Debulking surgery, Epithelial ovarian cancer, Surgical complexity,Postoperative morbidity, Survival
Received May 11, 2014, and in revised form July 15, 2014.Accepted for publication July 15, 2014.
(Int J Gynecol Cancer 2014;24: 1420Y1428)
ORIGINAL STUDY
1420 International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014
*Department of Gynaecology & Obstetrics, Odense UniversityHospital; and †Research Unit of General Practice, University ofSouthern Denmark, Odense, Denmark.
Address correspondence and reprint requests to AlgirdasMarkauskas, MD, Department of Gynaecology & Obstetrics,Odense University Hospital, Sdr Boulevard 29,5000 Odense C, Denmark.E-mail: [email protected].
The authors declare no conflicts of interest.
Copyright * 2014 by IGCS and ESGOISSN: 1048-891XDOI: 10.1097/IGC.0000000000000241
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

The theoretical benefits of primary cancer surgery aremultiple, including removal of resistant clones of tumor
cells, increasing the growth fraction of the tumor, maximizingthe effect of chemotherapy, reducing the risk for drug resis-tance, improving the tumor perfusion, and enhancing the im-munological competence of the patient.1,2 In epithelial ovariancancer (EOC), an inverse relationship between the size of theresidual disease after primary surgery, and overall survival (OS)was first established by Griffiths.3 The definition of ‘‘optimalcytoreduction’’ has changed over time, and the term is currentlyreserved for those with no macroscopic residual disease.4Y6
This is supported by the randomized study of the EuropeanOrganisation for Treatment and Research of Cancer and theNational Cancer Institute of Canada (EORTC-NCIC), showingthat optimal cytoreduction should be defined as total tumorresection without macroscopic residuals.7 This often demandsextensive upper abdominal surgery, which carries a high riskfor postoperative complications. Neoadjuvant chemotherapy(NACT) before cytoreductive surgery of womenwith advancedEOC (International Federation of Gynecology and Obstetrics[FIGO] stages IIIc and IV) reduces the surgical complexity andshows a tendency to decrease the postoperative morbidity andmortality.7 In addition,NACTmay increase the rate of completecytoreduction. Two recently published randomized trials com-pared primary debulking surgery (PDS) with NACTand intervaldebulking surgery (NACT-IDS) inwomenwith advancedEOC.7,8
It was demonstrated that the median OS did not differ in the2 arms, and NACT-IDS was associated with lesser postopera-tive morbidity and mortality. The studies prompted a paradigmshift in the treatment for women with advanced EOC, goingfrom primary surgery to NACT-IDS. However, it is a biologicalconcern thatNACT in the presence of a large tumor burdenmayincrease the likelihood of mutations leading to chemotherapy-resistant clones and potentially shorter progression-free sur-vival (PFS) and OS.9,10
Our center adopted the principles of advanced cytore-ductive surgery for the treatment of EOC in 2007.6 The cen-ter is population based and serves from 20% (2007Y2010) to35% (2011 and ongoing) of the Danish population. Someof the data on the present population has been included ina nationwide Danish study of Fago-Olsen et al.11 The mainpurpose of the present study is to analyze the surgical com-plexity, the postoperative morbidity, and the survival ofwomen with FIGO stages IIIc to IV EOC, treated with PDSand NACT-IDS.
MATERIALS AND METHODSAll patients with FIGO stage IIIc to IVepithelial ovarian,
fallopian tube, and primary peritoneal cancers treated at ourinstitution between January 1, 2007, and December 31, 2012,were identified. Only patients, who underwent debulking sur-gery, were included. Patientswhounderwent laparotomy beforeNACT were included in the NACT-IDS group, because weconsidered laparotomy as being diagnostic as no effort toachieve maximal cytoreduction was made. Electronic medicalfiles of the patients were used for data collection.
All patients were scheduled to receive 6 cycles ofplatinum-based chemotherapy with standard regimen being
carboplatin + paclitaxel. No patients received intraperitoneal(IP) chemotherapy as this treatment is not yet approved forgynecological malignancies in Denmark.
The decision to perform either PDS or NACT-IDSwas made at a multidisciplinary team conference and basedon the probability of complete IP cytoreduction. All pa-tients were preoperatively evaluated by magnetic resonanceimaging (MRI) and positron emission tomography and com-puted tomography (PET-CT) scans. In some cases, open lapa-roscopywas performed to exclude substantial serosal disease ofthe small bowel. Patients where complete IP cytoreductionseemed not to be achievable because of disseminated disease(tumor 9 2 cm behind porta hepatis, extensive intestinal serosaldisease, bulky lymphnodes above the level of the left renal vein)or poor general condition (combination of age 9 75Y80 years,albumin G 3.0 g/dL, American Society of AnesthesiologistsGroup [ASA] 9 2) were scheduled to NACT.12 Women withFIGO stage IV disease were treated equally to stage IIIc, andPDS was performed if complete IP cytoreduction was esti-mated to be possible, unless the patient had multiple metas-tases in the liver and/or the lungs or substantial malignantpleural effusions.
All patients were routinely evaluated clinically and byMRI scans by the same team of experts after 2 cycles ofNACT and then offered IDS after the third cycle, unless theyhad evidence of progressive disease or the general conditionof the patient still was too poor for surgery.
All operations were performed by a gynecological on-cologist. Bowel, hepatopancreatic surgery, and lymphade-nectomy above the renal vein were performed in collaborationwith experienced abdominal surgeons. Pelvic and paraaor-tic lymphadenectomy were performed if diagnosed as path-ological on imaging or if pathological bulky nodes wereidentified during surgical exploration. All patients receivedthe same postoperative care, including 24 to 48 hours ob-servation at the intensive care unit, if major peritoneal strip-ping was performed.
Surgical complexity was graded using a surgical com-plexity scoring system based upon the complexity and thenumber of surgical procedures performed,13 for example,hysterectomy + salpingo-oophorectomy giving, 1 point; omen-tectomy, 1 point; paraaortic lymphadenectomy, 1 point; pelviclymphadenectomy, 1 point; small bowel resection, 1 point; pel-vic peritoneum stripping, 1 point; abdominal peritoneum strip-ping, 1 point; large bowel resection, 2 points; splenectomy,2 points; diaphragm stripping/resection, 2 points; splenecto-my, 2 points; liver resection, 2 points; rectosigmoidectomywith anastomosis, 3 points. This gives 3 surgical complexityscore (SCS) groups: 1 (low), e3 points; 2 (intermediate), 4 to7 points; and 3 (high), Q8 points.
Postoperative complications were evaluated using theMemorial Sloan-Kettering Cancer Center surgical secondaryevents grading system14:0, no events observed within 30 days after operation1, use of oralmedications or bedside interventions to treat an event2, use of intravenous medications, total parenteral nutrition,
enteral nutrition, or blood transfusion to treat an event3, interventional radiology, therapeutic endoscopy, or opera-
tion required to treat an event
International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014 Primary Surgery or Interval Debulking
* 2014 IGCS and ESGO 1421
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

4, residual or lasting disability that requires major rehabili-tation or organ resection
5, an event that resulted in the death of the patientMajor postoperative complications were defined as grade 3
to 5 events.
Chemotherapy was considered postponed if delayedmore than 6 weeks after the operation and abandoned if thepatient did not receive the full 6 cycles.
Patientswere followeduntil September15, 2013, or death.
Statistical AnalysisThe OS time was calculated in days from the date of
the decision making regarding treatment modality (PDS vsNACT-IDS) to death or to the date of the last follow-up. ThePFS time was calculated in months from the date of decisionmaking to the approximate date of recurrence/progressionof the disease. The Kaplan-Meier method was used to esti-mate survival. Multiple Cox regression was used to comparesurvival between the relevant groups, adjusted for suitableconfounders. To assess the differences in the baseline andthe surgical characteristics of the PDS and NACT-IDSpopulations, we used a W
2-based median test for continuousvariables, for example, age and Fischer exact test for cate-gorical variables, for example, disease stage. We chose not
to perform statistical comparison of OS and PFS betweenthe PDS and NACT-IDS groups, as patients in our retro-spective study were highly selected, that is, patients submittedto NACT-IDS had more extensive disease and/or poorergeneral condition. Software used was Stata 11.2 (StataCorp,College Station, TX).
RESULTSFour hundred seven women with advanced EOC were
identified. Seventy-five (18.4%) were excluded, as they hadno debulking surgery at any time during their treatment, eitherbecause of progressive disease during chemotherapy (n = 59,78.7%) or poor general condition (n = 16, 21.3%). Threehundred thirty-two women were included in the study ofwhom165 (49.7 %) underwent PDS and 167 (50.3 %) weretreated with NACT-IDS. Twenty-eight (16.8%) in the NACT-IDS group underwent diagnostic laparotomy before NACT.The preoperative and surgical characteristics of the studypopulation are summarized in Tables 1 and 2, respectively.
Patients submitted to PDS had more complex surgery(P G 0.001) with higher rates of diaphragmatic striping (P =0.02) and bowel resection (P = 0.005), longer operating time(P G 0.001), greater perioperative blood loss (P G 0.001), andlonger hospitalization (P = 0.001). Complete IP cytoreduc-tion was achieved in 117 (70.9%) patients of the PDS group
TABLE 1. Baseline characteristics of the patients
PDS, N = 165 NACT-IDS, N = 167 P
Age, median (range), years 65 (24Y89) 66 (28Y88) 0.814*BMI, median (range) 24.6 (15.2Y40.8) 24.8 (17.6Y42.4) 0.826*Cancer type, n (%) 0.012†
Epithelial ovarian cancer 127 (77.0) 118 (70.7)Primary peritoneal cancer 20 (12.1) 39 (23.4)Fallopian tube cancer 18 (10.9) 10 (6.0)
Histology, n (%) 0.028†Serous 151 (91.5) 162 (97.0)Mucinous 9 (5.5) 1 (0.6)Clear cell 3 (1.8) 2 (1.2)Endometrioid 1 (0.6) 1 (0.6)Carcinosarcoma 1 (0.6) 0 (0.0)Undifferentiated 0 (0.0) 1 (0.6)
FIGO stage, n (%) 0.039†IIIc 127 (77.0) 111 (66.5)IV 38 (23.0) 56 (33.5)
ASA group, n (%) 0.193†1 61 (37.0) 50 (29.9)2 87 (52.7) 105 (62.9)3 16 (9.7) 12 (7.2)4 1 (0.6) 0 (0.0)*Median test by Pearson W
2.†Fischer exact test.BMI, body mass index; FIGO, International Federation of Gynecology & Obstetrics.
Markauskas et al International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014
1422 * 2014 IGCS and ESGO
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

and 100 (59.9%) of the NACT-IDS group. The proportionof patients with stage IV disease who had complete IPcytoreduction was 28 (24%) and 39 (39%) in the PDS andNACT-IDS group, respectively. Debulking to less than or equalto 1 cm of residual disease could be achieved in 139 (84.2%)women of the PDS group and 121 (72.5%) of the NACT-IDSgroup. Residual disease of greater than 1 cm was left in 26(15.8%) women after PDS and 46 (27.5%) after NACT-IDS.
Most patients experienced no or just minor events(grades 0Y2) after debulking surgery (73.7% and 83.3% in thePDS and NACT-IDS group, respectively). However, the rateof major complications (grade 3Y5 events) was greater in thePDS group compared with NACT-IDS (44 [26.7%] vs 28[16.8%]). The major complications are given in Table 3.
Twenty-four (14.5%) in the PDS group needed re-operation to treat an event: 5 having intra-abdominal abscess,8 having wound dehiscence, 6 having bowel perforation,4 having fistula, and 1 having urinary tract leakage. In theNACT-IDS group, 15 (9%) required reoperation: 4 havingintra-abdominal abscess, 4 having wound dehiscence, 3 havingbowel perforation, 1 having bowel obstruction, and 3 havingwound infection.
Twenty-two (6.6%) patients experienced a long lastingdisability (grade 4 event) after debulking surgery, 12 (7.3%)in the PDS group and 10 (6.0%) in the NACT-IDS group, and
it was associated with surgery of high complexity in 8 (66.7%)and 6 (60%) patients, respectively. Complete cytoreductionwas achieved in 10 (83%) and 10 (100%) patients, who expe-rienced a grade 4 event after PDS and NACT-IDS, respectively.
Six (3.6%) in the PDS group died during the first30 days after the operation (grade 5 event), and only 2 (33.3%)of these women achieved complete cytoreduction. Surgeryof high complexity was performed in only 1 (16.7%) case.Four patients died because of sepsis, one had pulmonaryembolism, and one died because of deteriorating generalcondition after PDS. In the NACT-IDS group, 3 women(1.8%) died during the first 30 days after surgery and allhad complete IP cytoreduction. One patient underwent sur-gery of low complexity (33%). The causes of death werepulmonary embolism, cerebral thrombosis, and sepsis.
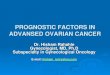
The median OS and PFS in relation to the residualdisease and type of debulking surgery are demonstratedin Figures 1 and 2, respectively.
Five (3%) patients had complete radiological and bio-chemical remission (Cancer Antigen 125 G 35 U/mL) afterNACT and all had microscopic tumor residuals only. Themedian OS of those patients was 31 months, and they had nopostoperative events after IDS.
The median delay of chemotherapy in patients, wherechemotherapy was postponed, was 7 weeks for both groups.
TABLE 2. Surgical characteristics of the patients
PDS, N = 165 NACT-IDS, N = 167 P
SCS, median (range) 6 (1Y15) 4 (1Y12) G0.001*SCS groups, n (%) G0.001†
Low SCS 16 (9.7) 65 (38.9)Intermediate SCS 80 (48.5) 62 (37.1)High SCS 69 (41.8) 40 (24.0)
Diaphragmatic surgery, n (%) 66 (40) 46 (27.5) 0.020†Bowel stoma, n (%) 78 (47.3) 53 (31.7) 0.005†Other radical procedures, n (%) 35 (21.2) 23 (13.8) 0.084†
Liver resection 5 (3.0) 3 (1.8)Cholecystectomy 1 (0.6) 4 (2.4)Pancreas resection 5 (3.0) 3 (1.8)Gastric resection 1 (0.6) 1 (0.6)Splenectomy 21 (12.7) 11 (6.6)Urinary bladder resection 2 (1.2) 1 (0.6)
Residual disease, n (%), cm 0.030†0 117 (70.9) 100 (59.9)e1 22 (13.3) 21 (12.6)91 26 (15.8) 46 (27.5)
Blood loss, median (range), mL 1440 (100Y13000) 800 (20Y6000) G0.001*Length of the operation, median (range), minutes 210 (30Y496) 150 (30Y480) G0.001*Hospitalization, median (range), days 9 (3Y54) 7 (2Y46) 0.001*
*Median test using Pearson W2.
†Fischer exact test.RD, residual disease.
International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014 Primary Surgery or Interval Debulking
* 2014 IGCS and ESGO 1423
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

The median number of chemotherapy cycles in PDS patientswhere chemotherapy was abandoned was difficult to estimate(mean value, 1.57), as 13 (56.5%) did not receive postoper-ative chemotherapy at all. Five (55.6%) NACT-IDS patientsdid not receive postoperative chemotherapy, and the remaining4 (44.4%) received a median of 4 cycles in total. Patients in theNACT-IDS group received at least 3 cycles of chemotherapybefore IDS.
A Cox regression analysis of the covariates in relationto survival for the PDS and NACT- IDS groups are givenin Table 4. When adjusted for multiple variables, residualdisease and age were significantly associated with medianOS after PDS. Residual disease of greater than 1 cm wasassociated with an almost 3-fold increased risk for death afterPDS compared with complete cytoreduction (hazard ratio[HR], 2.921; 95% confidence interval [CI], 1.643Y5.195; P =0.0003). Therewas a trend that residual disease of 1 cm or lesswas associated with worse median OS when comparedwith complete cytoreduction after PDS (HR, 1.78; 95% CI,0.98Y3.22; P = 0.0564).
In the NACT-IDS group, FIGO stage IV (HR, 1.63;95% CI, 1.01Y2.65), residual disease of greater than 1 cm(HR, 1.92; 95% CI, 1.15Y3.19), and ASA score of greater
than 2 (HR, 3.36; 95% CI, 1.35Y8.35) were associated withsignificantly worse median OS.
DISCUSSIONIn the present cohort study, we have analyzed surgi-
cal complexity, postoperative morbidity, and OS of womentreated at our institution with debulking surgery for FIGOstage IIIc and IV epithelial ovarian, fallopian tube, and pri-mary peritoneal cancers.
Although most women in the PDS and NACT-IDSgroups (73.7% and 83.3%, respectively) experienced no orjust minor events after surgery, our study confirms that therisk for major complications (22%) or even death (2.7%)should not be neglected, while counseling and selecting pa-tients for surgery. The rate of major postoperative compli-cations was higher after PDS compared with NACT-IDS, andthere was a positive relationship with surgical complexity. Itis problematic to compare postsurgical morbidity betweenvarious studies because of potential reporting bias and dif-ferences in the selection of patients. Chi et al15 reported 22%of grade 3 to 5 events after upfront extensive upper abdominalsurgery for advanced EOC and a mortality rate of 1.4%. The
TABLE 3. Specification of postoperative events
PDS (N = 165), n (%) NACT-IDS (N = 167), n (%) P*
Vascular events 13 (7.9) 7 (4.2) 0.174Venous thromboembolism 7 (4.2) 4 (2.4)Cardiovascular events 6 (3.6) 1 (0.6)Cerebrovascular events 0 (0.0) 2 (1.2)
Major infections 34 (20.6) 21 (12.6) 0.055Sepsis 15 (9.1) 6 (3.6)Wound infection 2 (1.2) 8 (4.8)Intra-abdominal abscess 17 (10.3) 13 (7.8)
Bleeding/hematoma 4 (2.4) 11 (6.6) 0.110Pleural effusions 13 (7.9) 6 (3.6) 0.103Wound dehiscence 10 (6.1) 4 (2.4) 0.109Bowel perforation (overall) 6 (3.6) 3 (1.8) 0.335
Anastomotic leak 2 (1.2) 1 (0.6)Ischemia/necrosis 4 (2.4) 2 (1.2)
Bowel obstruction 2 (1.2) 2 (1.2) 1.000Urinary tract leakage 2 (1.2) 1 (0.6) 0.622Pancreatic leakage 2 (1.2) 0 (0.0) 0.246Fistula 5 (3.0) 3 (1.8) 0.500Surgical events 0.126
Grades 0Y2 121 (73.3) 139 (83.3)Grades 3Y5 44 (26.7) 28 (16.8)
Reoperation 24 (14.5) 15 (9.0) 0.127Postponed chemotherapy 21 (12.7) 9 (5.4) 0.022Abandoned chemotherapy 23 (13.9) 9 (5.4) 0.009
*Fischer exact test.
Markauskas et al International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014
1424 * 2014 IGCS and ESGO
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

overall rate of major complications after PDS at the MemorialSloan-Kettering Cancer Center was reported to 9%, and therate of grade 5 complications was 0.7%.16 The rate of majorpostoperative complications and mortality reported in a ret-rospective multicenter study of Rafii et al17 were 11.5% and0.5%, respectively, and the rate of complications was higherafter PDS compared with NACT-IDS (OR, 2.17 [1.16Y4.09]).A mortality rate of 2.5% and 0.7% for the PDS and NACT-IDS arms, respectively, was reported in the EORTC-NCICtrial, and the corresponding figures were 5.6% and 0.5% inthe CHORUS trial.7,8 However, compared with our results,the patients were younger in the EORTC-NCIC trial andthe study of Rafii et al, and the proportion of patients withFIGO stage IV disease was lower in all 3 studies citedpreviously.7,8,17
In the present study, two thirds of the postoperativePDS deaths (n = 4) occurred in patients in whom optimalcytoreduction could not be achieved and despite of surgery oflow complexity. Residual disease of greater than 1 cmwas leftin 26 women (15.8%) after attempting radical surgery at PDS.These women have not gained any survival benefit, and most
likely, they should have been referred to NACT-IDS. Selectionof patients for upfront surgery is a major issue as predic-tion of optimal debulking surgery is very difficult. Use ofopen laparoscopy together with diffusion-weighted MRIand PET-CT seem to be promising in providing addi-tional information.18 All women in our study had preopera-tive PET-CT and MRI scans, and the rate of upfront surgerywas lower compared with other centers, but the rate ofcomplete cytoreduction was high. However, 28 (16.8%)women underwent laparotomy before NACT and representfailures in preoperative triaging, as they were found withmore extensive disease than otherwise expected on imaging.In all cases, no major effort for upfront cytoreduction wasmade, only sufficient tissue material was secured for theproper histological diagnosis of malignancy, and the patientswere scheduled to NACT-IDS. So far, the optimal methodfor selecting women for PDS is lacking, and improvementsare highly warranted as operation should only be performed ifa clear survival benefit is expected (ie, complete cytoreduction).Another pending question is if some of the women who wereradically operated after NACT-IDS should have been operated
FIGURE 1. OS by residual disease and type of debulkingsurgery. RD, residual disease; [n to .], no estimation ofthe upper limit of the confidence interval for the survivalmedian, because of short observational time.
FIGURE 2. PFS by residual disease and type of debulkingsurgery. RD, residual disease; [n to .], no estimation ofthe upper limit of the confidence interval for the survivalmedian, because of short observational time.
International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014 Primary Surgery or Interval Debulking
* 2014 IGCS and ESGO 1425
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

upfront? It remains speculative if the survival of these womenwould have improved if complete cytoreduction on PDS couldhave been achieved. A meta-analysis by Bristow and Chi10
showed that each cycle of chemotherapy delivered before sur-gery decreased median survival by 4.1 months. However, thestudies of Vergote et al7 and Kehoe et al8 clearly showed nosurvival benefit of PDS versus NACT-IDS in their populationsof patients with advanced EOC.
A higher percentage of women having residual diseaseof greater than 1 cm after NACT-IDS can partly be explainedby that this subgroup also included women who were tech-nically debulkable to less than or equal to 1-cm residualdisease but were expected surgical effort to achieve it wasjudged too risky in relation to the extent of the disease, thegeneral condition of the patient, and the expected survivalbenefit from incomplete cytoreduction. The rate of upfrontcytoreduction to 1 cm or less varies widely among in-stitutions, but different surgical groups have suggested thatmore than 75% should be acceptable.19 Cytoreduction to 1 cmor less was achieved in 78% in our study. The high rates ofcomplete IP cytoreduction in our study (Q60% in both groups)can be attributed to the strict selection of the patients fordebulking surgery (especially PDS) combined with will andskills of the gyne-oncological surgical team. However, we hada lower median OS compared with a study of Chi et al,16
reporting a median OS of 50 months for all women (FIGOstages IIIc-IV) treated with PDS and 78 months for thewomen without residual disease. The difference in the sur-vival between the 2 studies may partly be explained by anolder population and a higher proportion of stage IV diseasein our study.16A direct comparison of the results regarding OSfrom our retrospective study with data from the 2 randomizedtrials7,8 should be interpreted with caution.
The Gynecologic Oncology Group study, GOG 172,showed that IP chemotherapy improves survival of the womenwith stage III disease having less than or equal to 1-cm
residual tumor after PDS by approximately 17 months.20 Thistreatment is currently not recognized in Denmark, and it re-mains speculative whether addition of IP chemotherapywould have translated into more superior OS in the presentpopulation. Data on the use of IP chemotherapy after NACT-IDS are still limited, as the results of larger prospective studiesare pending.21
We chose not to perform statistical comparison of thesurvival between the PDS and NACT-IDS groups, becausethe groups were highly selected on the extent of the diseaseand/or the general condition of the patients. However, thedifference in the median OS between the subgroups withcomplete IP cytoreduction (51.7 vs 33.3 months after PDSand NACT-IDS, respectively) does raise some speculations.The NACT-IDS group had lower rates of postoperativecomplications and higher rates of completion of chemother-apy. Similar results were found in a study by Fago-Olsenet al,11 which showed better OS in patients after complete IPcytoreduction after PDS compared with NACT-IDS (55.5 vs36.7 months) and increased risk for death after 2 years offollow-up after NACT-IDS. The difference in the survivalobserved in the present study could be explained by moreextensive disease among patients referred to NACT-IDScompared with PDS, for example, 39% versus 24% withstage IV having complete IP cytoreduction in our study.Vergote et al7 have confirmed that complete resection of allmacroscopic diseases during debulking surgery is the singlemost important prognostic factor in advanced EOC. There-fore, it remains unclear why significantly higher rates ofcomplete cytoreduction (19% vs 51%) and lower morbidityafter NACT-IDS do not translate into more superior OS in thestudy of Vergote et al.7 We speculate that some patients whorelapse shortly after complete cytoreduction after NACT-IDSmay have unidentified macroscopic disease left. This point ofview is supported by the observation from our study that themedian OS of women achieving complete cytoreduction after
TABLE 4. Multivariate Cox regression analysis showing HRs and CIs for OS after PDS and IDS
PDS NACT-IDS
Variables HR 95% CI P HR 95% CI P
Age 1.02 1.00Y1.05 0.0438 1.02 0.99Y1.05 0.1488BMI 0.99 0.94Y1.04 0.6993 0.99 0.94Y1.04 0.7201ASA = 1 1 Y Y 1 Y YASA e 2 0.74 0.43Y1.29 0.2882 1.38 0.80Y2.40 0.2496ASA 9 2 1.19 0.51Y2.78 0.6908 3.36 1.35Y8.35 0.0092Stage IIIc 1 Y Y 1 Y YStage IV 0.93 0.51Y1.72 0.8294 1.63 1.01Y2.65 0.0478RD = 0 cm 1 Y Y 1 Y YRD e 1 cm 1.78 0.98Y3.22 0.0564 0.93 0.41Y2.10 0.8626RD 9 1 cm 2.92 1.64Y5.19 0.0003 1.92 1.15Y3.19 0.0119Observations 165 167
BMI, body mass index; RD, residual disease.
Markauskas et al International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014
1426 * 2014 IGCS and ESGO
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

NACT-IDS did not differ statistically significant from thosehaving residual disease of 1 cm or less (33.3 vs 28 months;HR, 0.93; P = 0.8626). It has recently been demonstrated thatcarcinomatous areas have a benign visual appearance moreoften after NACT than at PDS and chemotherapy-inducedfibrosis may hide vital tumor elements in otherwise obviousfibrotic tissue.22 This may lead to insufficient surgery andoverestimation of NACT-IDS women with ‘‘no macroscopicresiduals’’ and questions whether macroscopic tumor clear-ance during IDS is rather illusionary and may not be com-parable with the same definition as during PDS. Furthermore,a special attention must be paid to the women in the NACT-IDS population, where lacking statistical difference in themedian OS between the subgroups having macroscopicresidual disease (e1 vs 91 cm) may point toward ‘‘all ornothing’’ solution.
The strength of the present study is its population-basednature, avoiding someof the bias thatmayoccur in institutional-based investigations. No heterogeneity is present regardingthe choice of treatment modalities as all decisions were madeby the same team of experts at multidisciplinary team confer-ences. A review of the Electronic Patient Files from our insti-tution allowed inclusion of all cases meeting the inclusioncriteria aswell as a precise registrationof surgical characteristicsand postoperative events. Our study is limited by its retro-spective nature and relatively short follow-up. Patients treatedwith chemotherapy alone are not represented in our data, as themain inclusion criterion was debulking surgery.
Within the limits of our study, we suggest that NACT-IDS may be a better treatment alternative for the group ofhighly selected women where complete IP cytoreductioncannot be expected upfront, as suboptimal PDS does nothave any appreciable survival benefit and exposes the patientsfor unnecessary postoperative complications. The NACT-IDSis, until further evidence is presented, in our center consid-ered as a possibility of decreasing surgical complexity andpostoperative morbidity without compromising survival fora carefully selected group of women in whom alternativesurgical outcome otherwise would be suboptimal tumor re-section. Complete IP cytoreduction should be aimed in allcases of debulking surgery. A substantial number of womenwho receive either PDS or NACT-IDS have greater than 1 cmof tumor tissue left after the operation. These women prob-ably have no survival benefit from the operation, and fu-ture studies should focus on how to select these womenpreoperatively.
REFERENCES1. Bookman MA, Young RC. Principles of chemotherapy in
gynecologic cancer. In: Hoskins WJ, Perez CA, Young RC, eds.Principles and Practice of Gynaecologic Oncology.Philadelphia, PA: Lippincott Williams & Wilkins;2000:404Y407.
2. De Vita VT. The relationship between tumor mass and resistanceto chemotherapy. Implications for surgical adjuvant treatmentof cancer. Cancer. 1983;51:1209Y1220.
3. Griffiths CT. Surgical resection of tumor bulk in the primarytreatment of ovarian cancer. Natl Cancer Inst Monogr.1978;42:131Y136.
4. Chi DS, Eisenhauer EL, Lang J, et al. What is the optimal goalof primary cytoreductive surgery for bulky stage IIIc epithelialovarian carcinoma (EOC)? Gynecol Oncol. 2006;103:559Y564.
5. Stuart GC, Kitchener H, Bacon M, et al. 2010 GynecologicCancer Inter Group (GCIG) consensus statement on clinicaltrials in ovarian cancer: report from the Fourth OvarianCancer Consensus Conference participants of 4th OvarianCancer Consensus Conference (OCCC), GynecologicCancer Intergroup. Int J Gynecol Cancer. 2011;21:750Y755.
6. Zivanovic O, Aldini A, Carlson JW, et al. Advancedcytoreductive surgery: American perspective. Gynecol Oncol.2009;114:S3YS9.
7. Vergote I, Trope CG, Amant FA, et al. Neoadjuvantchemotherapy or primary surgery in stage IIIcYIV ovariancancer. N Engl J Med. 2010;363:943Y953.
8. Kehoe S, Hook J, Nankivell M, et al. Chemotherapy orupfront surgery for newly diagnosed advanced ovarian cancer:Results from the MRC CHORUS trial. Paper presented at: 2013American Society of Clinical Oncology Annual Meeting;May 2013; Chicago, IL.
9. Goldie JH, Coldman AJ. A mathematic model for relating thedrug sensitivity of tumors to their spontaneous mutation rate.Cancer Treat Rep. 1979;63:1727Y1733.
10. Bristow RE, Chi DS. Platinum-based neoadjuvantchemotherapy and interval surgical cytoreduction for advancedovarian cancer: a meta-analysis. Gynecol Oncol. 2006;103:1070Y1076.
11. Fago-Olsen CL, Ottesen B, Kehlet H, et al. Does neoadjuvantchemotherapy impair long-term survival for ovarian cancerpatients? A nationwide Danish study.Gynecol Oncol. 2014;132:292Y298.
12. Aletti GD, Eisenhauer EL, Santillan A, et al. Identificationof patient groups at highest risk from traditional approachto ovarian cancer treatment. Gynecol Oncol. 2011;120:23Y28.
13. Aletti GD, Santillan A, Eisenhauer EL, et al. A new frontier forquality of care in gynaecologic oncology surgery: multiinstitutional assessment of short-term outcomes for ovariancancer using a risk-adjusted model. Gynecol Oncol.2007;107:99Y106.
14. Martin RCII, Brennan MF, Jaques DP. Quality of complicationreporting in the surgical literature. Ann Surg. 2002;235:803Y813.
15. Chi DS, Zivanovic O, Levinson KL, et al. The incidence ofmajor complications after the performance of extensive upperabdomen surgical procedures during primary cytoreductionof advanced ovarian, tubal, and peritoneal carcinomas.Gynecol Oncol. 2010;119:38Y42.
16. Chi D, Musa F, Dao F, et al. An analysis of patients withbulky advanced stage ovarian, tubal and peritoneal carcinomatreated with primary debulking surgery (PDS) during anidentical time period as the randomized EORTC-NCIC trialof primary debulking surgery vs neoadjuvant chemotherapy(NACT). Gynecol Oncol. 2012;124:10Y14.
17. Rafii A, Stoeckle E, Jean-Laurent M, et al. Multi-centerevaluation of post-operative morbidity and mortality afteroptimal cytoreductive surgery for advanced ovarian cancer.PLoS One. 2012;7:e39415.
18. Fagotti A, Ferrandina G, Fanfani F, et al. Prospective validationof a laparoscopic predictive model for optimal cytoreduction
International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014 Primary Surgery or Interval Debulking
* 2014 IGCS and ESGO 1427
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.

in advanced ovarian carcinoma. Am J Obstet Gynecol.2008;199:642Y646.
19. Bristow RE, Eisenhauer EL, Santillan A, et al. Delaying theprimary surgical effort for advanced ovarian cancer: a systematicreview of neo-adjuvant chemotherapy and intervalcytoreduction. Gynecol Oncol. 2007;104:480Y490.
20. Armstrong D, Bundy B, Wenzel L, et al. Phase iii randomizedtrial of intravenous cisplatin and paclitaxel versus an intensiveregimen of intravenous paclitaxel, intraperitoneal cisplatin, andintraperitoneal paclitaxel in stage iii ovarian cancer: a
Gynecologic Oncology Group study. N Engl J Med.2006;354:34Y43.
21. Mackay HJ, Provencheur D, Heywood M, et al. Phase II/IIIstudy of intraperitoneal chemotherapy after Neoadjuvantchemotherapy for ovarian cancer: ncic ctgov.21. Curr Oncol.2011;18:84Y90.
22. Hynninen J, Lavonius M, Oksa S, et al. Is perioperative visualestimation of intra-abdominal tumor spread reliable in ovariancancer surgery after neoadjuvant chemotherapy? GynecolOncol. 2013;128:229Y232.
Markauskas et al International Journal of Gynecological Cancer & Volume 24, Number 8, October 2014
1428 * 2014 IGCS and ESGO
Copyright © 2014 by IGCS and ESGO. Unauthorized reproduction of this article is prohibited.