Embed Size (px)
Citation preview
Practical Pointers for the Cardiometabolic Patient
Primary Care Updates Rosemont, Illinois October 15, 2013
Content Collaborator

Session 1
Session 1: Practical Pointers for the Cardiometabolic Patient Learning Objectives 1. Review evidence-based screening recommendations for diabetes, while understanding how to best employ nutritional
guidelines to better care for patients at risk for or with diabetes. 2. Discuss the cardiac risk consequences associated with CKD and establish appropriate management plans to ensure
improved health outcomes. 3. Define the differences in cardiac risk scoring and the clinical applications for your practice. 4. Assess and employ enhanced patient communication strategies designed to improve patient outcomes. 5. Discuss the importance of early clinical data on the interrelationships between circadian rhythms and metabolism. Faculty
Dr Pamela Kushner, fellow of the American Academy of Family Physicians (AAFP), received her medical degree from the University of California, Irvine College of Medicine. She is a clinical professor in family medicine at the University of California, Irvine College of Medicine. She is also a family physician in private practice in Downey, Calififornia, and a past director of the osteoporosis diagnostic center in Los Alamitos, California. Dr Kushner is the past California representative to the AAFP. She was the first female president of the Long Beach Medical Association. Widely recognized as an expert in preventive medicine, Dr Kushner has published articles in several journals. Dr Kushner is a member of several professional associations. She is also a medical board reviewer for the state of California and a trustee of Long Beach M emorial Medical Center Faculty Financial Disclosure Statement The presenting faculty reports the following:
Dr Kushner receives consulting fees from AstraZeneca and Janssen Pharmaceuticals, Inc., and nonCME activity honoraria from Bristol-Myers Squibb.
Pamela Kushner, MA, MD, FAAFP Clinical Professor Department of Family Medicine University of California at Irvine Irvine, California
1
Practical Pointers for the Cardiometabolic Patient
SPEAKERsPamela Kushner, MA, MD, FAAFP
SESSION 17:45–9:15am
Presenter Disclosure Information
►Dr Kushner receives consulting fees from AstraZeneca and Janssen Pharmaceuticals, Inc., and nonCME activity honoraria from Bristol-Myers Squibb.
The following relationships exist related to this presentation:
Off-Label/Investigational Discussion
► In accordance with pmiCME policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
Practical Pointers in the Cardio Metabolic Patient
Pamela Kushner, MA, MD, FAAFPClinical ProfessorUniversity of CaliforniaIrvine Medical Center
Learning Objectives• Apply evidence-based screening recommendations for
diabetes, while understanding how to best employ nutritional guidelines to better care for patients at risk for or with diabetes.
• Identify the cardiac risk consequences associated with CKD and establish appropriate management plans to ensure improved health outcomes.
• Define the differences in cardiac risk scoring and the clinical applications for your practice.
• Assess and employ enhanced patient communication strategies designed to improve patient outcomes.
• Discuss the importance of early clinical data on the interrelationships between sleep disruption and metabolism.
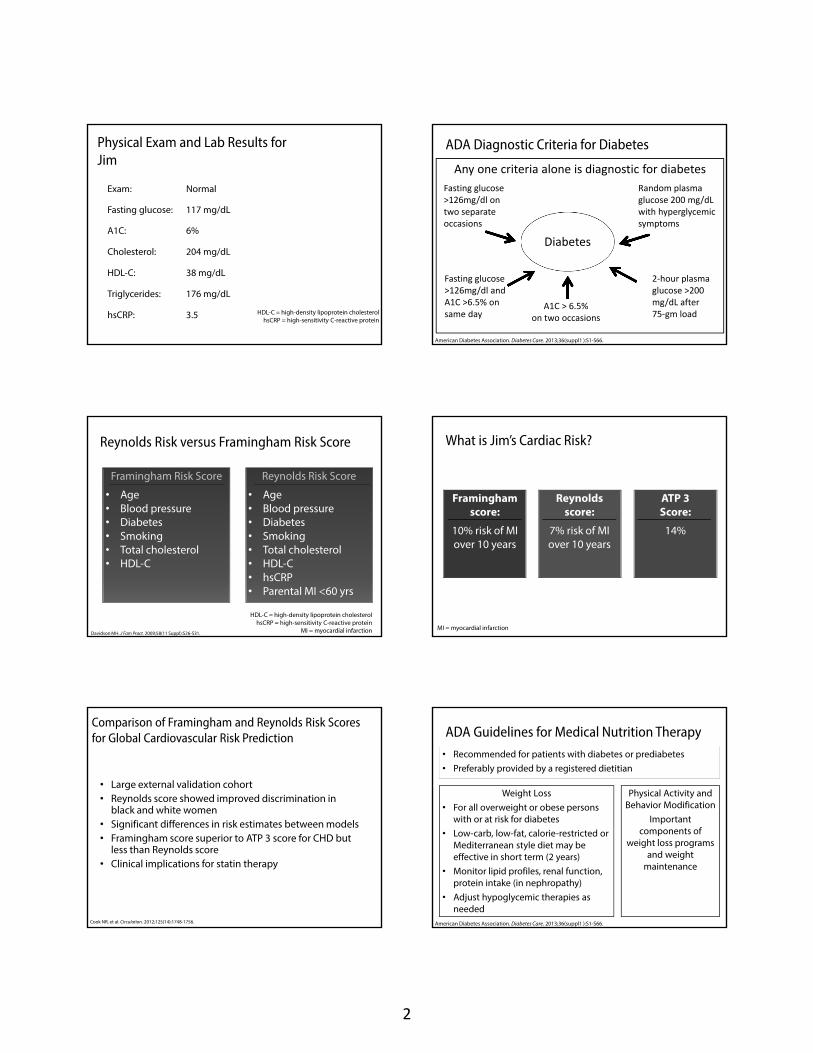
Meet Jim. Should We Test Him for Diabetes?
• 45-year-old Hispanic male • Comes in for employee physical• Feels great and no complaints• Non-smoker • Father had type 2 diabetes• BMI = 31 kg/m2
• Blood pressure = 146/83 mmHg
USPTF says only screen asymptomatic patients if blood pressure >135/80 mmHg
ADA Recommendations for Diabetes Screening in Asymptomatic Persons
• Begin at age 45 • Screen at least every 3 years• Screen at any age and more
frequently if age >25 withat least one risk factor
Risk Factors:• First-degree relative• High-risk race• History of gestational
diabetes• PCO• HDL<35 mg/dL• TG>250 md/dL• Physical inactivity• History of CVD• Signs of insulin
resistance
2
Physical Exam and Lab Results for Jim
Exam: Normal
Fasting glucose: 117 mg/dL
A1C: 6%
Cholesterol: 204 mg/dL
HDL-C: 38 mg/dL
Triglycerides: 176 mg/dL
hsCRP: 3.5 HDL-C = high-density lipoprotein cholesterolhsCRP = high-sensitivity C-reactive protein
ADA Diagnostic Criteria for Diabetes
Diabetes
Fasting glucose >126mg/dl on two separate occasions
Random plasma glucose 200 mg/dL with hyperglycemic symptoms
2‐hour plasma glucose >200 mg/dL after 75‐gm load
A1C > 6.5%on two occasions
Fasting glucose >126mg/dl and A1C >6.5% on same day
Any one criteria alone is diagnostic for diabetes
American Diabetes Association. Diabetes Care. 2013;36(suppl1 ):S1-S66.
Reynolds Risk versus Framingham Risk Score
Davidson MH. J Fam Pract. 2009;58(11 Suppl):S26-S31.
Framingham Risk Score
• Age• Blood pressure• Diabetes• Smoking• Total cholesterol• HDL-C
Reynolds Risk Score
• Age• Blood pressure• Diabetes • Smoking • Total cholesterol• HDL-C• hsCRP• Parental MI <60 yrs
HDL-C = high-density lipoprotein cholesterolhsCRP = high-sensitivity C-reactive protein
MI = myocardial infarction
What is Jim’s Cardiac Risk?
Framingham score:
10% risk of MI over 10 years
Reynolds score:
7% risk of MI over 10 years
ATP 3 Score:
14%
MI = myocardial infarction
Comparison of Framingham and Reynolds Risk Scores for Global Cardiovascular Risk Prediction
• Large external validation cohort• Reynolds score showed improved discrimination in
black and white women• Significant differences in risk estimates between models• Framingham score superior to ATP 3 score for CHD but
less than Reynolds score• Clinical implications for statin therapy
Cook NR, et al. Circulation. 2012;125(14):1748-1756.
ADA Guidelines for Medical Nutrition Therapy
Weight Loss• For all overweight or obese persons
with or at risk for diabetes• Low-carb, low-fat, calorie-restricted or
Mediterranean style diet may be effective in short term (2 years)
• Monitor lipid profiles, renal function, protein intake (in nephropathy)
• Adjust hypoglycemic therapies as needed
Physical Activity and Behavior Modification
Important components of
weight loss programs and weight
maintenance
American Diabetes Association. Diabetes Care. 2013;36(suppl1 ):S1-S66.
• Recommended for patients with diabetes or prediabetes• Preferably provided by a registered dietitian

3
Thirsty? (16 oz)
4‐oz Serving
Starbucks Cinnamon Dolce Latte
Jamba Juice Mango a go go
Calories 300 290
Carb 40 g 69 g
Fat 10 g 0 g
Protein 11 g 2 g
Fiber ― 2 g
Should We Test Jim for Kidney Disease?
NKF guidelines1
If at increased risk, should be tested with
markers and GFR
USPSTF2
Insufficient evidence to routinely screen
asymptomatic adults for CKD
GFR = glomerular filtration rateCKD = chronic kidney disease
We do an in office urine CLIA waived microalbumin dip and find…
• GFR 75 ml/min/1.73m2
• Negative urine microalbumin• Goal BP <140/90 mmHg
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
Stages of CKD
Stage Description GFR(mL/min/1.73 m2)
1 Kidney damage with normal GFR
> 90
2 Kidney damage with mild ↓ GFR
60–89
3a Moderate ↓ GFR 45–59
3b Moderate ↓ GFR 30–44
4 Severe ↓ GFR 15–29
5 Kidney failure < 15 or on dialysis
Pathogenesis of Atherosclerosis
Atherosclerosis
Cardiometabolic syndrome
Syndrome X
Insulin resistance syndrome
Dyslipidemic hypertension
syndrome
Hyperinsulinemia
Atherogenic pattern B syndrome
MESA: Multi-Ethnic Study of Atherosclerosis
• 4,364 subjects without diabetes• Impaired fasting glucose (100 to 125 mg/dl) or
insulin resistance• Insulin resistance and WHR associated with
concentric LV remodeling independent of BMI• Results support the cardiometabolic phenotype,
defined by insulin resistance and central obesity playing a critical role in LV remodeling independent of BMI
Budoff MJ, et al. J Am Coll Cardiol. 2013;61(16):1698-706.
WHR = wait-to-hip ratioLV = left ventricular BMI = body mass index

4
Meet Helen
• 55-year-old black female
• Shift worker• Presents with
GFR 51cc/min/1.73m2 down from GFR 58cc/min/1.73m2 5 months ago. Both times urine microalbumin is positive 100mg/L
• She’s here for refills and fatigue
Medical History:• Hypertension• Hyperlipidemia• Type 2 diabetes 5 years• Non-smoker• Sister had nonfatal MI
at 59
Medications:• Amlodipine 5 mg• HCTZ 50 mg• Ibuprofen 200 mg prn• Metformin 500 mg BID• Fish oil supplement
BIDGFR = glomerular filtration rateMI = myocardial infarctionHCTZ = hydrochlorothiazide
Gender and Race Differences in CKD RiskBlack race 4-fold higher risk of stage 4 CKD or ESRD
and at much younger age than whites
Women Higher risk of CKD than men
Men Higher risk of ESRD than women
Age > 65 years Increased risk of ESRD
Prevalence of CKD stage 3 or higher
≈ 13.5 million white persons≈ 1.8 million black persons
Risk of CKD stage 3 or higher
Almost 64% of US population will develop stage 3 or higher
National Chronic Kidney Disease Fact Sheet 2010. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/diabetes/pubs/pdf/kidney_factsheet.pdf.Grams, ME et al. Am J Kidney Dis. 2013. 62(2):245-252
Chronic Kidney Disease Definition
Kidney damage is defined by its pathologic abnormalities including…
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266. *Johnson CA, et al. Am Fam Physician.
Markers of damage in
blood or urine tests or imaging studies for 3 or more months
GFR less than 60 mL/min/1.73 m2 for 3 or more
months*
Structural or functional
abnormalities of the kidney,
with or without decreased GFR
GFR = glomerular filtration rate
Cardiometabolic Syndrome and Chronic Kidney Disease
• Major risk factor for:– End-stage renal disease (ESRD)– Cardiovascular (CV) disease– CV sudden death
• < 2% of CKD progresses to renal replacement therapy (RRT)
• 50% of CKD die of CAD• 10 times risk of patient with normal
microalbuminGo AS, et al. NEJM. 2004;351:1296-1305.
Keith DS. Arch Intern Med. 2004;164:659-663.
CKD is Cardiac Risk Equivalent by NKF, ADA, and AHA Guidelines
Odds Ratio for CVD
Stage 2 1.5
Stage 3 2–4
Stage 4 10
Stage 5 50
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.American Diabetes Association. Diabetes Care. 2013;36(suppl1 ):S1-S66.
What is Helen’s Risk?
Cardiac risk equivalent of diabetes /CKD

5
Laboratory Evaluation of CKD
• Consider serum and protein electrophoresis for MM in differential
Standard: • CBC• Basic metabolic panel• Urinalysis• Serum albumin• Alkaline phosphatase• Intact PTH• Lipid profile• 25 hydroxy D• Serum phosphate• Calcium
Further evaluation when glomerulonephritides suspected:
• Hepatitis B, C• HIV• ANA• Complement
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
Imaging in CKD
• Renal sonogram• Renal radionuclide scanning may be
useful to screen for renal artery stenosis (with captopril)
• Consider retrograde pyelography if negative ultrasound and suspicion of obstruction or stones
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
Pertinent Findings
Vitals
Blood pressure 157/98 mmHg
BMI 29 kg/m2
Waist circumference
39 in
Imaging
Renal sonogram Normal
EKG Normal
Exam
HEENT Normal
Cardiorespiratory Normal
Trace peripheral edema;slightly swollen left knee
Pertinent Findings, cont.
LabsHbA1c 8.2%
Hematocrit 36
Alkaline phosphatase, uric acid, electrolytes
Normal
Vitamin D 27 ng/ml
Total cholesterol 230 mg/dL
HDL-C 40 mg/dL
LDL-C 130 mg/dL
hsCRP 4
Calcim, Intact PTH Normal
Microalbuminuria
Development: 5-10 years after onset of diabetes
Marker of: Inflammation and endothelial dysfunction, renal vascular proliferation
Risk factor for: Early cardiovascular mortality
Normal level: < 30 mg albumin/g creatinine
Testing: • Validate by repeat testing within 3-6 month if may be affected by exercise, CHF, very high glucose or blood pressure, or UTI
• Yearly in patients with diabetes or hypertension
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
Signs and Symptoms of CKD
Dialysis: 45% of CKD patients report depressive symptoms at initiation
Stage 1-3• GFR >30 cc/min• Asymptomatic
Stage 4-5Usually when electrolyte/ metabolic disturbances appear
Stage 5
Signs of metabolic acidosis:• Loss Of Lean
Body Mass• Muscle Weakness• Anemia• Peripheral Edema• Hypertension • Sleep
Disturbances
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.

6
Management Plans for CKD
• Delay the progression
• Treat the pathological manifestations of CKD
• Plan for long-term renal replacement therapy
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
Chronic Kidney Disease: Management
• BP control– Prioritize ACE inhibitors or ARBs
• Cardiovascular risk modification– Statins
• Glycemic control– Dietary modifications (salt, protein, phosphates, fat)
• Be alert for potential complications– Anemia, bone disease, electrolyte disturbances
• Co-manage with nephrology
ACE = angiotensin-converting enzymeRB=angiotensin-II receptor blockers
Hypertension Treatment
• ACE Inhibitor or ARB (nephroprotective)– Ramipril decreased progression to
nephropathy – Not tested in trials of CKD in patients >70
• Mechanism in addition to BP reduction– Decrease intraglomerular pressure– Reduce membrane permeability
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.Heart Outcomes Prevention Evaluation Study Investigators. Lancet. Jan 22 2000;355(9200):253-259.
Angiotensin Agents in CKD
• ACE or ARB can be continued if GFR decline after 4 months<30% baseline
• May need low-potassium diet (written instructions)
• May need institute loop diuretic to control BP• Goal to keep serum potassium <5.5mEq/L
Rivera JA, et al. Am Fam Physician. 2012;86(8):749-754.
Benefits and Harms of Screening, Monitoring, and Treatment for CKD Stages 1 to 3
• ACE-inhibitors and ARBs reduced ESRD versus placebo, primarily in patients with diabetes who have macroalbuminuria
• Risks for mortality, ESRD, or other clinical outcomes did not significantly differ between strict and usual blood pressure control.
Fink, H. Ann Intern Med. 2012;156(8):570-581.
ACE = angiotensin-converting enzyme ARB = angiotensin II-receptor blockerESRD = end-stage renal disease RR = relative riskCI = confidence interval
ACE-inhibitors:RR: 0.65 (95% CI, 0.49–0.88)
ARBs:RR: 0.77 (95% CI: 0.66–0.90)
Low Diastolic BP Associated with Higher Mortality in CKD
• Observational study of 650,000 US veterans• Relationship of blood pressure with mortality
in CKD follows a J-shaped curve, especially diastolic pressure
• Systolic pressure 130–159 mmHg combined with diastolic pressure 70–89 mmHg confers lowest mortality risk
Covesdy C, et al. Ann Intern Med. 2013;159(4):233-242.
7
Statin Therapy for Cardiovascular Risk Modification
Most studies show reduced CV events with statin therapy in Stage 2 and Stage 3 CKD
Treating to New Targets (TNT) study2
• Baseline GFR = 65 (Stage 2)• Statin therapy improved
renal function over 60 months
• Both groups improved, but higher dose greater than lower dose
Study of Heart and Renal Protection (SHARP)1
• Simvastatin + Ezetimibe• Improved CVD outcomes in
CKD and ESRD (GFR = 26)• Improved renal outcomes
as well in CKD
1. Baigent C, et al. Lancet. 2011;377(9784):2181–2192. 2. Shepherd J, et al. CJASN. 2007;2(6):1131-1139 .
AACE Nutritional Recommendations for Diabetic Patients
• Regular meals and snacks and
• Avoid fasting to lose weight
• Plant-based diet, high fiber low-calorie, low glycemic index
• Explain nutritional facts label
• Use mild instead of high heat cooking
• Explain three types of carbohydrates: sugars, starch, and fiber
• Specify healthful snacks
• Eat protein with low saturated fatsAACE Diabetes Resource Center . Available at: http://resources.aace.com
Haagen Dazs Vanilla Ice Cream vs Frozen Yogurt
4‐oz Serving
Ice Cream Frozen Yogurt
Calories 270 180
Cholesterol 85 mg 45 mg
Protein 4 g 8 g
Carb 20 g 31 g
Fat 17 g 2.5 g
A ACE Nutrition Guidelines Continued
Carbohydrates• 7–10 servings/day of fresh fruits, vegetables,
whole grain and other helpful carbohydrates• Lower glycemic index foods (score < 55 out of
100 may be helpful (whole oats, legumes, lentils, chickpeas, brown rice)
Fats• Specify healthy fats• No or low fat dairy products• Limit saturated fat and trans fat• No need to avoid animal protein but limit
processed meatsAACE Diabetes Resource Center . Available at: http://resources.aace.com
ADA Nutritional 2013 Guidelines for Diabetic Management
Goals:• Reduce weight by 5-10% for overweight/ obese or 15% for
Class 3 obesity• Decrease BMI 2-3 units
Limit saturated fat intake to less than 7% of total calories
Limit intake of sugar sweetened beverages
Limit alcohol intake to <1drink/day for women and <2 drinks/day for men
Increase dietary fiber to 25-50 grams/day
American Diabetes Association. Diabetes Care. 2013;36(suppl1 ):S1-S66.
ORIGIN: Omega-3 Fatty Acid Trial Conclusions
Omega-3 Effects on Death and CV Outcomes
• Did not reduce rate of primary outcome (CV death)
• Did not reduce major vascular events
• Did not reduce death from any cause or from arrhythmia
ORIGIN Trial Investigators. N Engl J Med. 2012;367:319-328.ORIGIN = Outcome Reduction with Initial Glargine Intervention
Omega-3 Effects on Lipid and Glucose Control
• Greater mean reduction in TG vs placebo
• No effect on – other lipids– plasma glucose– A1C,– BP – Heart rate

8
U.S. Preventive Services Task Force. Ann Intern Med. 2009;150(6):396-404.
USPSTF Recommendation on Aspirin for Prevention of CVD
MenAge 45-79
Years
Women Age 55-79
Years
MenAge <45
Years
WomenAge <55
Years
Men and Women Age
≥80 YearsEncourage
aspirin when benefit of
preventing MI outweighs
potential harm (GI hemorrhage)
Encourage aspirin when
benefit of preventing
stroke outweighs
potential harm (GI hemorrhage)
Do not encourageaspirin for MI prevention
No recommend-
ation
Risk Level at Which CVD Events Prevented Outweigh GI Harms
Men Women
Age 10-year CHD Risk
Age 10-year CHD Risk
45-59 ≥ 4% 55-59 ≥ 3%
60-69 ≥ 9% 60-69 ≥ 8%
70-79 ≥ 12% 70-79 ≥ 11%
Applies to adults not taking NSAIDs and who do not have GI pain or history of GI ulcers
On Further Questioning About Her Sleep…
Helen says she has significant daytime sleepiness and nocturnal gasping but no snoring.
Regulation of Circadian Behavior and Metabolism by Synthetic REV-ERB • Synchronizing rhythms of behavior and
metabolic processes is important for cardiovascular health and preventing metabolic disease
• Administration of synthetic REV-ERB ligands alters circadian behavior and the circadian pattern of core CLOCK gene expression in the hypothalamus of obese mice resulting in less fat mass and improved lipids and glycemic control
• Hypothalamus integrates nutrition and hormonal signals
Myers KA, Mrkobrada M, Simel DL. JAMA. 2013;310(7):731-741.
Sleep Deprivation and Sleep Apnea
CDC estimates 7%–19% of US adults not getting adequate sleep
Circadian misalignment results from:• Increased % Americans
with shift work• Frequent time zone
travel• Long work hours
Sleep apnea increases risk of:
• Hypertension• Heart attack• Stroke • Congestive heart failure• Arrhythmias• ↑ inflammatory
cytokines• ↑ accidents
Myers KA, Mrkobrada M, Simel DL. JAMA. 2013;310(7):731-741.
Sleep Apnea Clinical Score
• Hypertension (risk factor and consequence)• Nocturnal choking or gasping had highest
prediction• Snoring• Neck circumference • >15 increases likelihood• <5 less likely
Myers KA, Mrkobrada M, Simel DL. JAMA. 2013;310(7):731-741.
ACP Guidelines for Treating Sleep Apnea
• Weight loss encouraged for overweight and obese• CPAP as first-line treatment• Mandibular advancement devices for patients who
can't tolerate CPAP• No support for drug therapy currently• evidence lacking for benefits of surgery for first-
line treatment
CPAP = continuous positive airway pressureQaseem A, et al. Ann Intern Med. 2013;159:471–483.
9
Applying KDOQI to Helen
• Change to ACE or ARB• Correct vitamin D to >30• Goal BP < 130/80 mmHg• BMI < 25 goal• Lose 7%body weight• Waist circumference
< 88 cm (woman)< 102 cm (man)
• Aspirin• Increase metformin
and add another oral agent to get A1C < 7%
• Sleep study• Stop glucosamine and
NSAID• Consider PT to increase
activity
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
ADA Management Guidelines:Aspirin Therapy Aspirin 75–162 mg/day
• Primary prevention in type 1 or type 2 diabetes patients at increased CVD risk (10-year risk >10%)
• Secondary prevention in those with diabetes and history of CVD
Clopidogrel 75 mg/day)
• For patients with CVD and documented aspirin allergy
Both aspirin and clopidogrel
• Reasonable for ≤1 year after ACS
• No sufficient evidence to recommend aspirin for primary prevention in lower risk individuals (10-year risk <5%; eg, men <50 years of age or women <60 years of age without other major risk factors)
• Potential adverse effects from bleeding likely offset potential benefits• Clinical judgment recommended for patients in these age groups with
other risk factors (10-year risk 5%–10%)American Diabetes Association. Diabetes Care. 2013;36(suppl1 ):S1-S66.
Protein/Creatinine Ratio
• Most accurate way to measure protein in a spot urine
• Nephrotic ratio>3.5 (correlates to 3.5 g protein)
• Recommended by KDOQI-NKF when monitoring proteinuria in adults with CKD if albumin/creatinine ratio > 500–1000 mg/g
• Should be done within 3 months of positive albumin/creatinine dipstick of > +1
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
CKD Diagnosis in Medicare Patients, by Age, Gender, & Race
Medicare patients age 65 & older, alive & eligible for all of 2011. CKD claims as well as other diseases identified in 2011.
Adjusted odds ratio of a CKD diagnosis code in Medicare patients, by age, gender, & race, 2011
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System. U.S. Department of Health and Human Services, 2011. Available at: http://www.cdc.gov/ckd.
Probability of Urine Albumin & Creatinine Testing in Medicare Patients At Risk For CKD
• Medicare patients from the 5% sample, age 20 & older, with Parts A & B coverage in the prior year
• Patients diagnosed with CKD or ESRD during prior year are excluded.
• Tests tracked during each year.
Prob
abili
ty o
f Tes
ting
All Diabetes (no hypertension)
Diabetes & hypertensionHypertension (no diabetes)
Centers for Disease Control and Prevention. Chronic Kidney Disease Surveillance System. U.S. Department of Health and Human Services, 2011. Available at: http://www.cdc.gov/ckd.
KDOQI Treatment of CKD Pathology
Condition Treatment
Anemia Hgb <10 then treat with erythropoiesis
Hyperphosphatemia Phosphate binders and phosphate restriction (goal < 4.6 mg/dL)
Hyperparathyroidism Calcitriol or vitamin D analogs (goal >30 mg/mL)
Volume overload Loop diuretic
Metabolic acidosis Oral alkali supplementation
Ferritin Goal of 100-800 ng/mL
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease. Am J Kidney Dis. 2002 Feb;39(2 Suppl 1):S1-266.
10
Nephrology Referral
• Rapid deterioration in renal function:– Unexplained proteinuria >1,000 –
1,500 g/24 hr– Unable to control hypertension
• Evidence shows that referral and comanagement at Stage 4 improves morbidity and decreases mortality (GFR < 30 ml/min/1.73m2)
KDIGO 2012 Clinical Practice Guideline. Kidney International Supplements. 2013;3:112–119.
When to Consider Renal Replacement Therapy
• Presence of one or more of the following:– Hyperkalemia– Pruritus– Intractable volume overload– Inability to control blood pressure– Refractory malnutrition– Cognitive impairment
• Don’t treat just based on GFR #, although GFR usually is 5-10 cc/min/1.73m2
KDIGO 2012 Clinical Practice Guideline. Kidney International Supplements. 2013;3:112–119.
NKF Referral to Registered Dietician
• Approved under Medicare B if used in disease management
Patient Adherence: The Current Issues
≈ 1/3 to 1/2 of US patients do not adhere to prescribed medication regimens
Non adherence costs the US ≈ $100–290 billion annually
ACA aims to shift towards improved quality outcomes and efficiency…the jury is still outWho will care for the highest risk patients if payment is tied to performance analysis?
ACA=Affordable Care ActNEHI . Thinking outside the Pillbox: A System-Wide Approach to Improving Patient Medication Adherence for Chronic Disease. August 2009. http://www.nehi.net/publications/44/thinking_outside_the_pillbox_a_systemwide_approach_to_improving_patient_medication_adherence_for_chronic_disease
Adherence: Shared Decision Making and Responsibility
• Open ended questions-allow patient to talk• Try not to interrupt• Leave a sense of where the diagnosis is going but
you don't need to know the answer• Find out the patient's primary concern and
validate• Review the history―don't just check it off• Partnership of good Dr. and a good patient• Shared responsibility and decision-making
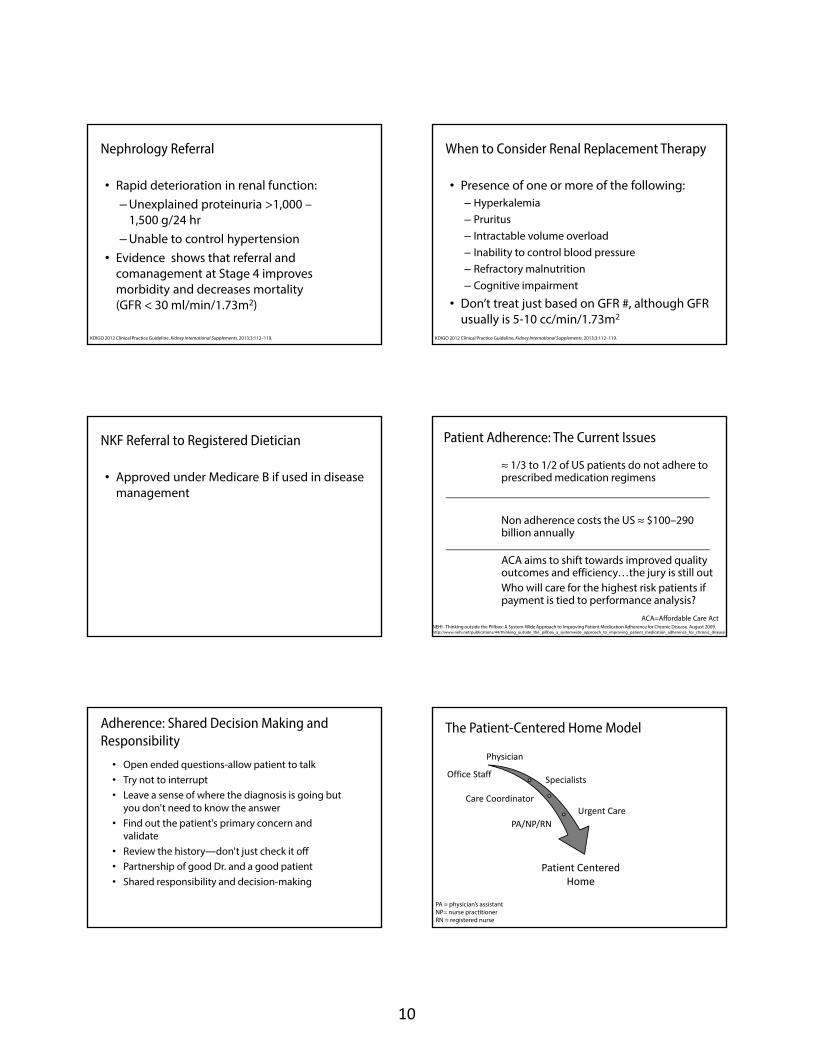
Physician
Specialists
Care Coordinator
Urgent Care
PA/NP/RN
Office Staff
Patient Centered Home
The Patient-Centered Home Model
PA = physician’s assistantNP= nurse practitionerRN = registered nurse
11
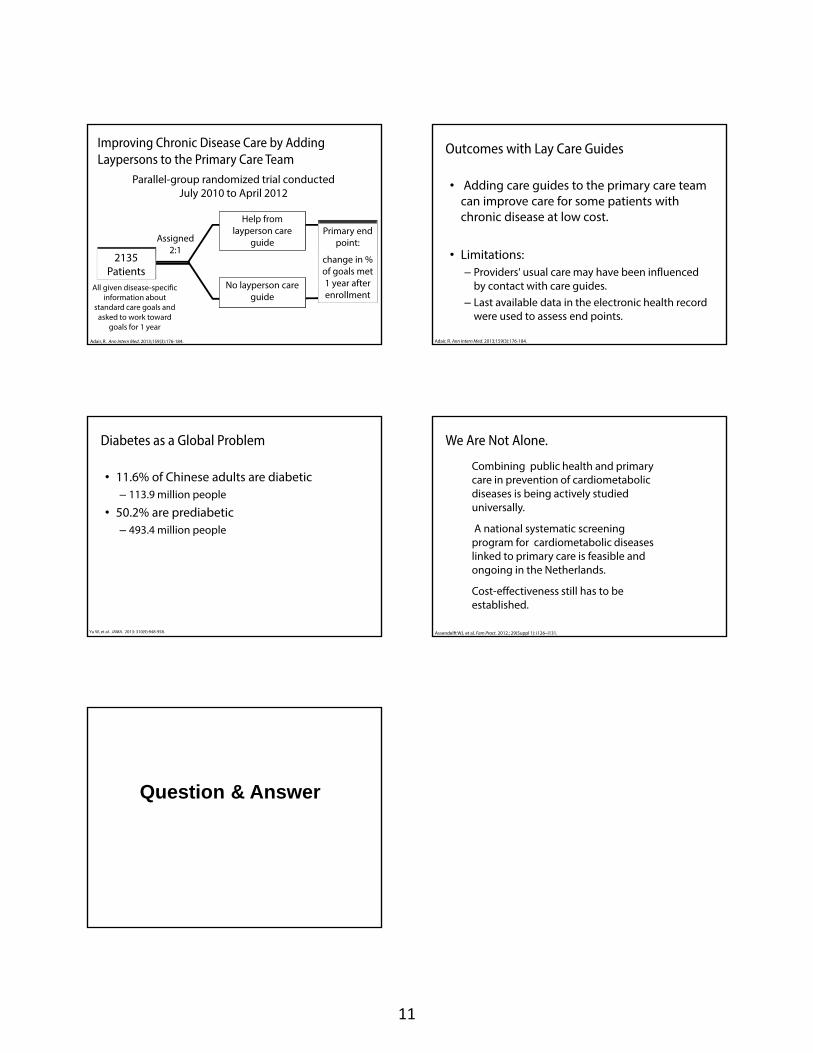
Improving Chronic Disease Care by Adding Laypersons to the Primary Care Team
Parallel-group randomized trial conducted July 2010 to April 2012
Adair, R. Ann Intern Med. 2013;159(3):176-184.
2135 Patients
Primary end point:
change in % of goals met 1 year after enrollment
Help from layperson care
guide
No layperson care guide
Assigned 2:1
All given disease-specific information about
standard care goals and asked to work toward
goals for 1 year
Outcomes with Lay Care Guides
• Adding care guides to the primary care team can improve care for some patients with chronic disease at low cost.
• Limitations:– Providers' usual care may have been influenced
by contact with care guides. – Last available data in the electronic health record
were used to assess end points.
Adair, R. Ann Intern Med. 2013;159(3):176-184.
Diabetes as a Global Problem
• 11.6% of Chinese adults are diabetic– 113.9 million people
• 50.2% are prediabetic– 493.4 million people
Yu W, et al. JAMA. 2013: 310(9):948-958.
We Are Not Alone.
Combining public health and primary care in prevention of cardiometabolic diseases is being actively studied universally.
A national systematic screening program for cardiometabolic diseases linked to primary care is feasible and ongoing in the Netherlands.
Cost-effectiveness still has to be established.
Assendelft WJ, et al. Fam Pract. 2012.; 29(Suppl 1): i126–i131.
Question & Answer