Embed Size (px)
Citation preview

aInstitute for Healthcare Delivery and Population Science, Baystate Health, Springfield, Massachusetts; bDepartment of Pediatrics, University of Massachusetts Medical School–Baystate, Springfield, Massachusetts; cSchool of Medicine, Boston University, Boston, Massachusetts; and dDivision of General Pediatrics, Boston Medical Center, Boston, Massachusetts
Dr Peacock-Chambers conceptualized and designed the study, participated in study selection, conducted the analyses, drafted the initial manuscript, and revised the manuscript; Ms Ivy participated in the study selection, data collection, and analyses, drafted sections of the initial manuscript, and reviewed and revised the manuscript; Dr Bair-Merritt conceptualized and designed the study and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
DOI: https:// doi. org/ 10. 1542/ peds. 2017- 1661
To cite: Peacock-Chambers E, Ivy K, Bair-Merritt M. Primary Care Interventions for Early Childhood Development: A Systematic Review. Pediatrics. 2017;140(6):e20171661
CONTEXT: The pediatric primary care setting offers a platform to promote positive parenting behaviors and the optimal development of young children. Many new interventions have been developed and tested in this setting over the past 2 decades.OBJECTIVE: To summarize the recent published evidence regarding the impact of primary care–based interventions on parenting behaviors and child development outcomes; to provide recommendations for incorporation of effective interventions into pediatric clinics.DATA SOURCES: A literature search of PubMed and PsycINFO was conducted from January 1, 1999, to February 14, 2017.STUDY SELECTION: Publications in which primary care–based interventions and reported outcomes regarding the child’s development or parenting behaviors associated with the promotion of optimal child development are described.DATA EXTRACTION: Forty-eight studies in which 24 interventions were described were included. Levels of evidence and specific outcome measures are reported.RESULTS: Included interventions were categorized as general developmental support, general behavioral development, or topic-specific interventions. Two interventions resulted in reductions in developmental delay, 4 improved cognitive development scores, and 6 resulted in improved behavioral intensity or reduction in behavioral problems. Interventions used a variety of theory-based behavior change strategies such as modeling, group discussion, role play, homework assignment, coaching, and video-recorded interactions. Three interventions report the cost of the intervention.LIMITATIONS: Community or home-based interventions were excluded.CONCLUSIONS: Although several interventions resulted in improved child development outcomes for children aged 0 to 3 years, comparison across studies and interventions is limited by use of different outcome measures, time of evaluation, and variability of results.
Primary Care Interventions for Early Childhood Development: A Systematic ReviewElizabeth Peacock-Chambers, MD, MSc, a, b Kathryn Ivy, BA, c Megan Bair-Merritt, MD, MSCEd
abstract
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
PEDIATRICS Volume 140, number 6, December 2017:e20171661 Review ARticle by guest on May 12, 2020www.aappublications.org/newsDownloaded from

The first 3 years of life are a critical period for child brain growth and development, with the potential to impact later social, economic, and health-related quality of life.1 Pediatric primary care, which includes health supervision and anticipatory guidance, offers an important entry point for the promotion of optimal child development in the United States because it is a universal service with frequent encounters in the first 3 years of a child’s life.2, 3 In a systematic review by Regalado and Halfon4 of publications between 1979 and 1999, the authors summarized developmental assessments, anticipatory guidance, and specific interventions used to promote development of children aged 0 to 3 years in primary care settings. They comment on the efficacy of anticipatory guidance and problem-focused counseling interventions as well as the challenges and barriers to implementing such interventions in practice. Importantly, the authors found that targeted skill-building interventions that were focused on improving parent-child interaction, 5 or specific parenting behaviors (such as book sharing, 6 coping with infant colic, 7 sleep training, 8 or non-harsh discipline9) proved to be the most effective.
New interventions to promote the optimal development of young children continue to be developed and tested. Additionally, in 2012, the American Academy of Pediatrics called for the pediatric community to “catalyze fundamental change in early childhood policy and services.” 3 This declaration underscored the need for new, more effective strategies to increase the impact of primary care on promoting optimal development for young children in the United States. Taking this statement along with the rapidly changing landscape of US pediatric primary care systems, including the rise of the medical home model10
and new models of well-child care delivery, 11 a comprehensive and current review of these interventions is needed. The authors of such a review must summarize the impact these interventions have on child development outcomes, building on a previous review focused on positive parenting outcomes.12 Furthermore, scientists and clinicians could benefit from a synthesis of available evidence-based interventions to inform areas still in need of future study. Therefore, our objective in this systematic review was to examine the interventions implemented in connection with primary care to promote optimal child development for children aged 0 to 3 years from 1999 to 2017 and to summarize the efficacy of these interventions on child and parent level outcomes.
MeThODs
search strategy
This systematic review was conducted by following the PRISMA guidelines13 to identify interventions delivered in connection with primary care setting for the promotion of optimal early development of children aged 0 to 3 years. For the purpose of this review, pediatric primary care or pediatric clinics were defined as family medicine, pediatric, or public health clinics (outside of the United States) providing preventive care to children. Interventions were defined as education, counseling, or other provider-parent engagement beyond screening for developmental delay. Parents could include nonbiological parents, grandparents, or caregivers, but henceforth we refer to these caregivers as parents. Our inclusion criteria required that English, peer-reviewed publications: (1) examined interventions for the promotion of optimal child development for children aged 0 to 3 years, (2) described delivery of the intervention within or associated with a primary care setting, and
(3) reported outcomes regarding the child’s development (cognitive, behavior, or social-emotional) or parenting behaviors associated with the promotion of optimal child development (eg, book sharing, positive discipline, or parental sensitivity using validated measures). We excluded review articles and articles that targeted children with developmental diagnoses (eg, autism, attention-deficit/hyperactivity disorder, oppositional defiant disorder) or extreme prematurity (<28 weeks’ gestation). We also excluded studies solely of parents with known substance abuse or depression because these mental health illnesses frequently require additional targeted treatment. We excluded studies that only reported outcomes regarding child sleep. Publications were considered from any country if they met the above listed criteria.
PubMed and PsycINFO were searched by E.P-C. for a selection of articles published from January 1, 1999, through February 14, 2017, using these key words: (“child development” OR “parenting”) AND (“pediatrics” OR “primary care”). In addition, we searched references of included articles and related review articles. The final list of included articles was reviewed with 2 expert child development consultants not affiliated with the study: 1 developmental behavioral pediatrician with more than 30 years of clinical and intervention development experience and a second developmental behavioral pediatrician that has written extensively about child developmental assessments and promotion in clinical settings.
study selection
Initial search terms were intentionally broad; therefore, 1 investigator (E.P-C.) screened the initial list of titles to exclude clearly irrelevant studies. Two investigators
PEACoCK-ChAMBERS et al2
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

independently screened abstracts of all potentially relevant titles (E.P-C. and K.I.) using inclusion and exclusion criteria listed above to identify studies for full text review. The investigators resolved disagreements by consensus, reviewing full-text articles and involving a third investigator as needed.
Data Abstraction and Levels of evidence
Data were abstracted from full-text articles by K.I. by using a structured form that included information on intervention delivery (content, frequency, duration, person implementing, location, specific developmental focus, and cost), study design, child age, sample size, study population, outcome measures (child or parent outcomes), and findings. Abstracted data were verified and checked for consistency by a separate abstractor (E.P-C.). Two reviewers (E.P-C. and K.I.) independently assessed the levels of evidence of the studies using a clinically relevant quality rating scheme modified from the Oxford Centre for Evidence-Based Medicine Levels of Evidence.14 Levels of evidence are classified as follows: level 1, properly powered and conducted randomized clinical trials; level 2, well-designed controlled trial without randomization, prospective comparative cohort trial; level 3, case-control studies, retrospective cohort studies; level 4, case series with or without intervention, cross-sectional study. Disagreements regarding level of evidence scores were resolved through discussion and consensus.
ResuLTs
Description of study selection
Initial searches yielded 7605 titles from all search engines. Of these, 528 abstracts (411 from PubMed and 117 from PsychInfo) were retained, with an additional 40 abstracts
identified from reference lists. After the removal of 55 duplicate articles, 513 abstracts were reviewed for inclusion and/or exclusion criteria (Fig 1). Four-hundred and twenty-five articles were excluded during abstract review, resulting in the full-text review of 88 articles. Forty articles were excluded on full-text review, yielding 48 articles in which 24 interventions were described that met all inclusion and exclusion criteria.
Intervention Description
Interventions were conducted in 12 different countries: United States, Australia, China, Holland, Canada, Norway, Turkey, Chile, Jamaica, Antigua, St. Lucia, and Iran. Interventions identified in this review could be grouped in 3 broad categories on the basis of the described intervention “focus” as
summarized in Tables 1 through 3: (1) general developmental support, such as language, social, gross and fine motor development (9 interventions, 20 studies); (2) general behavioral development, such as managing negative child behaviors through developing positive disciplinary strategies (8 interventions, 19 studies); and (3) specific developmental topics (topic specific), including infant colic and reading aloud to children (7 interventions, 9 studies). Descriptions of interventions are found in Tables 1, 2, and 3, which include the intervention components, the “dose” of the intervention, the developmental focus of the intervention, who administered the intervention, the cost when available, and the connection to primary care.
PEDIATRICS Volume 140, number 6, December 2017 3
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
FIGuRe 1Flowchart for search results through February 14, 2017.
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

General developmental interventions included the Video Interaction Project (VIP), 17 – 23 Building Blocks (BB), 19 –21, 23 Healthy Steps (HS), 24 – 28 HS plus PrePare (PP), 15, 29 Care For Development (CFD) Intervention, 16, 30 Touchpoints, 31 Play with
Our Children (POC), 32 Parenting Intervention, 33 and Sit Down and Play (SDP).34 VIP and HS were the 2 most intensive interventions involving additional meetings with child development specialists at each well-child visit from birth to age 3 years.
VIP sessions included videotaping the parent and child during a play interaction followed by review and coaching of the interaction with the specialist at a cost of $150 to $240 per child per year. BB provided a monthly newsletter and age-specific
PEACoCK-ChAMBERS et al4
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABLe 1 Summary and Description of General Developmental Support Interventions (n = 9)
Intervention Brief Description Focus Delivery
VIP Videotaping and coviewing parent-child interaction followed by discussion, developmentally age appropriate toy, and written material
Discussion of developmental concerns, review of video to identify strengths and potential areas of improvement, provide age-appropriate learning material
12 sessions, 30–45 minDelivered by: child development specialistPrimary careCost: $150–240 per child per yearPrimary care: delivered in the primary care clinic
during well-child visitsBB Age-specific newsletter mailed once
per mo with developmentally age-appropriate toy and parent-completed developmental questionnaires
Support of verbal interactions in the context of pretend play, shared reading, and daily routines
Delivered by: not applicable, materials onlyCost: $75 per child per yearPrimary care: materials sent to patients by the
primary care clinic and contacted family if questionnaires suggested possible delay
hS Meeting with developmental specialist, phone lines for questions; written material, parenting groups
Developmental, behavioral, and psychosocial aspects of care
9 enhanced well-child visits and 6 home visits in the first 3 y
Delivered by: child development specialistCost: $400–$933 per childPrimary care: delivered in the primary care clinic
during well-child visitshS + PP Meeting with developmental specialist,
phone support, and screening for risk factors (smoking, depression, domestic violence)
Education and preparation for changes in pregnancy and newborn period, identify risk in pregnant mothers
3 home visits during pregnancy and hSDelivered by: child development specialistPrimary care: hS components delivered in the
primary care clinic during well-child visitsCFD Structured interview and counseling
during an acute health visit and 1 wk follow-up visit15
Enhancement of caregiver-child interactions and home environment in resource-limited settings, introducing forms of play, communication, homemade toys, and reading aloud
2 sessions, 30 min15
Discussion based on counseling guidelines, modeling, practice with feedback, and written material16
2 sessions, 30–60 min16
Delivered by: physician or other health professionalPrimary care: delivered in clinics or by health
professionalsTouchpoints Sessions with a parent coach,
phone support, Ages and Stages Questionnaire activity-based system, video vignettes, and modeling child interactions
Strengthening of parent-health provider relationship, educate about nonharsh parent-child interactions, and increase use of community resources
Clinic and home visits from birth to 18 moDelivered by: “parent coach” (bilingual college-
educated in child development)Primary care: mentoring by social worker and nurse
from the primary care officePoC Group sessions (15 dyads per group),
home visits, and in-depth interviews for parents of children aged 0–4 y
Strengthening positive caregiver-child interaction in learning activities and play; promote comprehensive socioemotional, motor, language, and cognitive development; enhance parenting skills and knowledge; and foster networks among caregivers
Weekly group sessions, 2.5 hDelivered by: “community monitors” with support
from physicians, psychologists, and teachersPrimary care: sessions held in health center, support
from physicians, psychologists
Parenting intervention
Shown short videos (9 modules, 3 min each), discussed and encouraged mother to practice activity shown in video (∼16 min), health provider reinforced messages, gave written materials, a book, and a puzzle
Illustration of mothers doing parenting behaviors considered central to promoting child development
5 brief sessions in waiting roomsDelivered by: community health worker and nursePrimary care: delivered in the primary care clinic
during routine health maintenance visits
SDP Modeling for parents how a toy can facilitate talking or playing with their child. Parents observed and feedback provided on their interaction introducing the new toy.
Informed by social cognitive theory, promoting observational learning, resources to engage in behaviors, and concrete strategies in addition to knowledge provision
8 sessions from 2–24 mo of age, 10–15 min in waiting room
Delivered by: existing clinical staff, nonprofessionals, or volunteers
Primary care: delivered in the primary care clinic waiting room
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

toy to families at a lower cost ($75) and was studied as part of a 3-arm randomized controlled trial (RCT) with VIP. HS clinic sessions offered parents an opportunity to discuss developmental concerns with a child development specialist as well as
home visits, phone support, written material, and parenting groups. PP was an addition to HS providing 3 home visits during pregnancy. HS cost between $400 and $933 for 11 well-child visits and 2 home visits over 2.5 years. Touchpoints included
similar services (clinic and home visits, phone support) delivered from birth to 18 months of age by a “parent coach” with college-level education in child development. CFD, developed by the World Health Organization and the United Nations
PEDIATRICS Volume 140, number 6, December 2017 5
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABLe 2 Summary and Description of General Behavioral Development Interventions (n = 8)
Intervention Brief Description Focus Delivery
IY Group sessions (8–12 parents, group discussions after video vignettes, modeling, role play, and parent homework)
Nurture parenting through play, praise, rewards, limit setting, managing misbehavior
6–10 weekly group sessions, 2 hDelivered by: clinical psychologist and 1 pediatric
staff (RN, MD, LCSW, NP)Primary care: delivered at primary care clinics or
public health centersTriple P Level 1: universal parent information
strategy that provides all interested parents with access to useful information via pamphlets and electronic media
(1) enhance parental knowledge and resourcefulness; (2) promote nurturing, low-conflict environments for children; (3) promote children’s social, emotional, and intellectual competencies through positive parenting practices
Delivered by: child development specialist, psychologist, or physician
Level 2: 2 sessions in clinic, early anticipatory developmental guidance, video, and pamphlets
Primary care: delivered in primary care clinics or health centers
Level 3: 4 sessions in clinic, 30 min, for children with mild to moderate behavioral difficulties
Level 4: 8–10 sessions, 2 h, individual, group, or self-directed parent training program for children with more severe behavioral difficulties
Level 5: 12 sessions, 1–2 h, enhanced behavioral family intervention program when behavior is complicated by other sources of family distress
PCIT Compared group sessions (2–4 dyads) and homework reinforcing skills versus providing the same information in written packets
Praise for positive behavior and not giving any attention to negative behavior
4 weekly group sessions, 1.5 hDelivered by: PCIT-trained therapist and the children
with research assistantPrimary care: delivered in primary care clinic
waiting room after hoursUniversal
parenting program/toddlers without tears
Individual sessions with health care provider, handouts describing normal child development
Education regarding unreasonable expectations, harsh discipline, and nurturing parenting
3 sessions, 2 hDelivered by: health care provider and a parenting
expertPrimary care: delivered by physician separate from
usual clinic visits
Webster-Stratton
Group sessions (10 parents per group), videos, group discussion, role play, homework
Improvement of parent-child interactions, limit setting, ignoring undesired behavior, praise, reward, follow through on discipline plans
10 weekly group sessions, 2 hDelivered by: trained health visitors or nursesPrimary care: delivered at health centers
Family Foundations
Group psycho-educational sessions (5 prenatal, 4 postnatal, 8–12 couples per group)
Coparental conflict resolution, problem solving, and communication
9 group sessions, 2–3 hDelivered by: trained male and female facilitatorsPrimary care: delivered at health center
ezParent Modules on an android tablet, adapted from the Chicago parent program group sessions, includes video vignettes, knowledge questions, and interactive games
Evidence-based strategies to encourage good behavior and decrease misbehavior in children aged 2–5 y
6 modules, 1 hDelivered by: electronic devicePrimary care: delivered in large urban primary care
pediatric clinic
PriCARE Weekly group sessions (6–8 parents), includes role-play and homework
Trauma-informed positive parenting, prosocial behaviors, giving effective commands. Informed by attachment and social learning theories and based in PCIT techniques
6 weekly group sessions, 1.5 hDelivered by: 2 licensed mental health professionalsPrimary care: delivered in conference room at
primary care clinic
LCSW, Licensed Clinical Social Worker; MD, Doctor of Medicine; NP, Nurse practitioner; RN, registered nurse.
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

Children’s Fund and officially called the Care for Child Development intervention, provided a picture card and guides for clinicians to share with parents to discuss the importance of developmentally appropriate play, home-made toys, communication, and reading. POC offered group sessions by “community monitors” as well as home visits and in-depth interviews from birth to age 4 years. The Parenting Intervention and SDP were 2 brief interventions delivered in waiting rooms for 10 to 15 minutes by community health workers or paraprofessional volunteers.
General behavioral interventions included Incredible Years (IY), 35, 36 Positive Parenting Program (Triple P), 37 – 45 Parent-Child Interaction Therapy (PCIT), 46 Universal Parenting Program (also called Toddlers without Tears), 47, 48 Webster-Stratton, 49, 50 Family Foundations, 51 ezParent, 52 and PriCARE.53 Triple P was the most widely disseminated and studied program, which included 9 publications from 4 different countries. Triple P had 5 levels of intervention intensity designed to match the severity of the child’s behavioral problems (Table 2).
With increasing Triple P levels, the total number of sessions as well as length of sessions increased. The Webster-Stratton intervention, IY, and PriCARE were among the more intensive group-based parenting programs involving ∼10 parents in 6 to 10 sessions delivered by child psychologists or pediatric staff, including role play, homework, and group discussion. PriCARE adapted a trauma-informed program called Child-Adult Relationship Enhancement54 on the basis of principles and techniques derived from PCIT for the primary care setting. PCIT and the Universal
PEACoCK-ChAMBERS et al6
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABLe 3 Summary and Description of Specific Developmental Topic Interventions (n = 7)
Intervention Brief Description Focus Delivery
Family-centered treatment (colic)
Individual sessions, developed IFTP Identification of potential causes of and responses to infant colic, develop coping mechanisms to deal with crying
3 sessions within 6 wkDelivered by: pediatrician and mental health
specialistPrimary care: delivered in the primary care clinic
BBP (colic) Booklets and video mailed to parents, optional phone call and group parenting session
Development of a tailored management plan to address infant crying
25 min video, 1 group session 1.5 hDelivered by: maternal child health nursesCost: $60Primary care: overseen by pediatrician at respective
health centersThB (colic) Video for parents describing the best
way to calm their infant on the basis of a step-wise approach beginning with feeding, then holding, changing, swaddling, side-laying, swaying, exposing to white noise, and then pacifier
Strategies to soothe crying infant 30 min videoDelivered by: multimedia videoPrimary care: delivered in community hospitals on
the newborn nursery, assume cared provided by general pediatricians
Infant massage (colic)
Mothers learned to administer infant massage during 1 session, then massaged infants once during the day and once at night before sleeping. Control group was rocked gently for 5–25 min
Infant massage for soothing 1 session, daily massage 15–20 minDelivered by: training by expert in infant massage,
massage administered by mothersPrimary care: training provided in clinic
Literacy promoting intervention (reading)
Families given an age appropriate book and written handout explaining benefits of reading to children
Child literacy and parent-child interactions
Each well-child visit from 6–18 moDelivered by: pediatric providersPrimary care: delivered in the primary care clinic
during well-child visitsRoR (reading) Reading demonstrations of age-
appropriate books, anticipatory guidance, written material, and age-appropriate book written in English
Child literacy and parent-child interactions
Each well-child visit from 6 mo to 6 yDelivered by: volunteer (demonstration) and
physician (anticipatory guidance)Primary care: delivered in the primary care clinic
waiting roomsRoR + M Modeling how parents could use a
developmentally appropriate book to engage the child in mathematics activities around specific concepts (discriminating small numbers of objects, counting, simple arithmetic, geometry, spatial thinking) by using mathematical language and written handout focused on each concept
Child literacy, parent-child interactions, and promotion of basic math skills
1 session at a well-child visitDelivered by: pediatric residentsPrimary care: delivered in the primary care clinic
BBP, Baby Business Program; IFTP, Individualized Family Treatment Plan; ThB, The happiest Baby.
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

Parenting Program required fewer sessions (3–4) ranging from 1.5 to 2.5 hours. Family Foundations included psycho-education for coparents to resolve conflicts between parents beginning prenatally. EzParent was the only behavioral intervention that was entirely delivered via an electronic device, adapting a parenting group curriculum into 6 multimedia interactive modules.
The topic-specific interventions included 4 interventions for colic (Family-Centered Treatment, 55 Baby Business Program, 56 The Happiest Baby, 57 and Infant Massage58) and 3 interventions to promote reading aloud (Literacy Promotion Intervention, 59 Reach Out and Read [ROR], 6, 60, 61 and Reach Out and Read plus Mathematics [ROR + M]62). The 4 colic interventions varied greatly in intensity from development of individualized family treatment plans designed by a pediatrician and mental health specialist (Family-Centered Treatment) to multimedia videos with optional discussion (Baby Business Program and The Happiest Baby) as well as infant massage. ROR is a well-studied program to promote child literacy during well-child visits, also previously described in Regalado and Halfon’s4 review. The authors of 2 additional studies completed after 1999 evaluated the intervention through a quality improvement evaluation across 10 states in the United States.6, 60 The authors of a third study modified the intervention to teach specific math topics.62 A literacy intervention similar to ROR evaluated the impact of reading aloud on receptive and expressive language development.59
sample Composition
The authors of the studies included in this review recruited participants from varying socioeconomic backgrounds, ethnicities, and nationalities. VIP involved primarily low-income and Spanish-speaking participants in the United States,
a large proportion of which did not receive education beyond the seventh grade. HS studies included 15 primary care sites across the United States.25 – 27 Three interventions (CFD, POC, and the Parenting Intervention) were studied solely in low- or middle-income countries. In contrast to the general developmental interventions, behavioral interventions tended to target participants on the basis of behavioral concerns rather than demographic factors. The researchers for IY, 35, 36 Webster-Stratton, 49, 50 and PriCARE53 studies enrolled children that scored above a certain threshold on behavioral assessments or whose parents reported concerns regarding their child’s behavior. Triple P tailored the intervention intensity on the basis of the severity of the child’s behavioral problems.
Levels of evidence
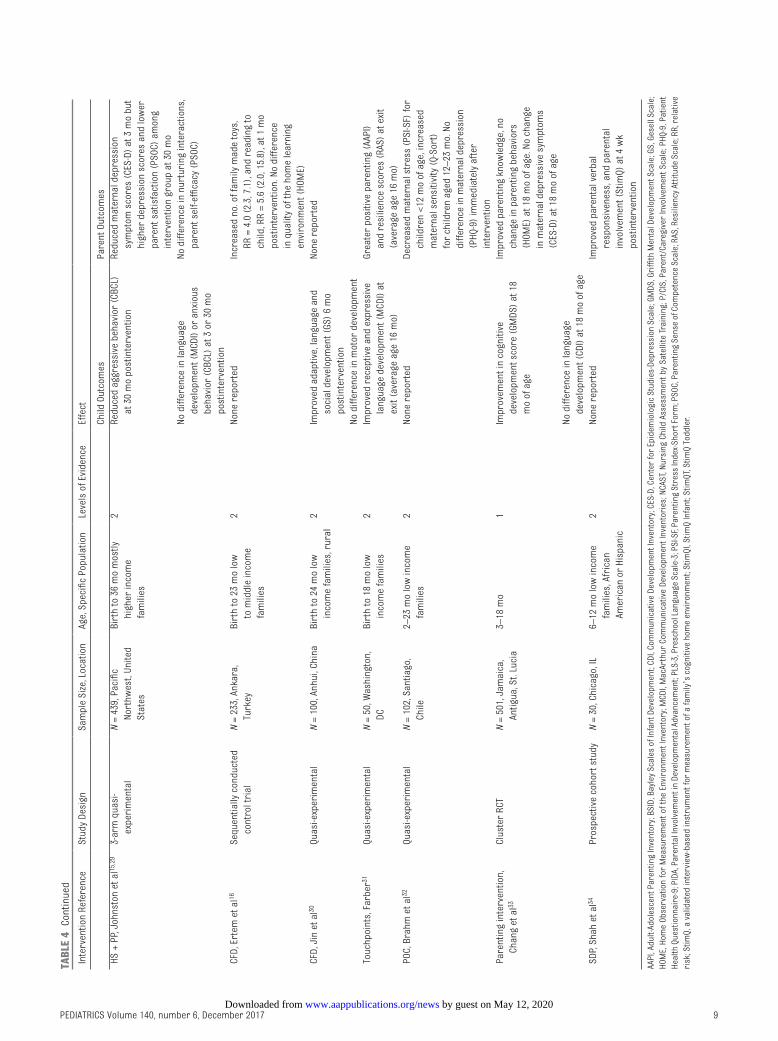
General developmental interventions were primarily conducted as quasi-experimental study designs, with the exception of the VIP and the Parenting Intervention studies in which RCTs were employed (Table 4). Sample sizes ranged from 50 at a single site31 to >3000 study participants in 10 sites.25, 26 All of the general behavioral interventions were evaluated by at least 1 RCT (Table 5). For topic-specific studies, RCT study design was employed in colic interventions, whereas observational cohorts or cross-sectional comparisons with historical controls were used in the literary studies (Table 6). All Levels of Evidence scores are reported in Tables 4 through 6.
Outcomes
General Developmental Support
Among the general developmental interventions, cohorts enrolled in HS and VIP experienced fewer cases of developmental delay compared with control groups at 12 months28 and 3 years, respectively.17, 18 The effects
of VIP on child development were more pronounced among children of mothers with seventh to 11th grade educations in 1 study17, 18 and for mothers with a literacy level of ninth grade or higher in a second study.19 VIP also resulted in decreased hyperactivity and externalizing behaviors.23 HS and PP resulted in a reduction in child aggressive behavior at 30 months of age measured by the Child Behavior Checklist (CBCL).15, 29 No difference in child behavior was detected with HS alone. CFD resulted in improved adaptive, language, and social development 6 months postintervention.30 Touchpoints was associated with significant improvement in child language development (expressive and receptive) measured by the MacArthur Communicative Development Inventories at 16 months of age.31 The Parenting Intervention was associated with significantly improved cognitive development (Griffith Mental Development Scale), but not specifically language development.33
Multiple studies reported significant changes in both parenting behaviors and psychological well-being. Parents enrolled in the VIP, 19 BB, 19 HS, 25, 26 CFD, 16 and SDP34 interventions engaged in educational activities (such as reading) at significantly higher levels compared with control groups. The overall quality of the home environment improved among families enrolled in VIP and BB at 6 months of age.19 HS, 24 Touchpoints, 31 and POC32 were associated with greater parental sensitivity and higher quality parent-child interactions. Parents enrolled in VIP reported significantly reduced stress and depressive symptoms compared with controls.22 One study in which HS and PP were evaluated revealed an increase in parental depressive symptoms and a decrease in parenting satisfaction among the intervention group at 30 months.15, 29
PEDIATRICS Volume 140, number 6, December 2017 7
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

PEACoCK-ChAMBERS et al8
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABL
e 4
Gene
ral D
evel
opm
enta
l Sup
port
Inte
rven
tions
: Res
ults
and
Lev
els
of E
vide
nce
Inte
rven
tion
Refe
renc
eSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion
Age,
Spe
cific
Pop
ulat
ion
Leve
ls o
f Evi
denc
eEf
fect
Child
out
com
esPa
rent
out
com
es
VIP,
Men
dels
ohn
et a
l17, 18
RCT
N =
99, N
ew Y
ork,
NY
Birt
h to
36
mo
low
in
com
e fa
mili
es,
mos
tly h
ispa
nic
1Si
gnifi
cant
ly fe
wer
cas
es o
f de
velo
pmen
tal d
elay
(BS
ID).
No
chan
ge in
lang
uage
(PL
S-3)
or
beha
vior
(CB
CL)
at 2
1 an
d 33
mo
of a
ge.
Sign
ifica
ntly
red
uced
par
entin
g st
ress
(P
SI-S
F) a
nd im
prov
ed p
aren
tal
teac
hing
(PI
DA),
no c
hang
e in
de
pres
sion
(CE
S-D)
or
the
hom
e en
viro
nmen
t (St
imQT
) at
33
mo
of
age
VIP
3-ar
m R
CTN
= 41
0, N
ew Y
ork,
NY
Birt
h to
36
mo
low
in
com
e fa
mili
es,
mos
tly h
ispa
nic
1Im
prov
ed a
tten
tion
at 2
4 m
o,
decr
ease
d hy
pera
ctiv
ity a
nd
exte
rnal
izin
g be
havi
ors
at 3
6 m
o of
age
Impr
oved
qua
lity
of th
e ho
me
envi
ronm
ent (
Stim
QI)
and
incr
ease
d tim
e sp
ent r
eadi
ng (
read
ing
diar
y)
at 6
mo
of a
geM
ende
lsoh
n et
al19
Berk
ule
et a
l20Re
duct
ion
in m
ild a
nd m
oder
ate
depr
essi
ve s
ympt
oms
(PhQ
-9)
at 6
m
o of
age
Canfi
eld
et a
l21De
crea
sed
pare
ntin
g st
ress
(PS
I-SF)
Cate
s et
al, 22
Wei
sled
er
et a
l23At
6, 2
4, a
nd 3
6 m
o
Less
har
sh d
isci
plin
e at
24
mo
of a
geBB
, Men
dels
ohn
et a
l, 19
Berk
ule
et a
l203-
arm
RCT
N =
410,
New
Yor
k, N
YBi
rth
to 3
6 m
o lo
w
inco
me
fam
ilies
, m
ostly
his
pani
c
1No
diff
eren
ce in
att
entio
n or
imita
tion
play
at 2
4 m
oIm
prov
ed q
ualit
y of
the
hom
e en
viro
nmen
t (St
imQI
) at
6 m
o of
age
Canfi
eld
et a
l, 21 W
eisl
eder
et
al23
Incr
ease
d no
. rea
ding
inst
ance
s pe
r da
y (r
eadi
ng d
iary
)Re
duct
ion
in m
ild d
epre
ssiv
e sy
mpt
oms
(PhQ
-9)
at 6
mo
of a
geNo
cha
nge
in h
arsh
dis
cipl
ine
at 2
4 m
ohS
, Cau
ghy
et a
l24RC
TN
= 37
8, S
outh
east
an
d So
uthw
est,
Unite
d St
ates
Birt
h to
36
mo
1No
diff
eren
ces
in b
ehav
ior
(CBC
L) a
t 34
–37
mo
of a
geGr
eate
r pa
rent
al s
ensi
tivity
(NC
AST)
, le
ss h
arsh
dis
cipl
ine,
and
hig
her
qual
ity p
aren
ting
inte
ract
ions
(P/
CIS)
at 3
4–37
mo.
No
diffe
renc
e in
th
e ho
me
envi
ronm
ent (
hoM
E)h S
RCT
6 si
tes,
qua
si-
expe
rim
enta
l 9 s
ites
N =
3165
, Uni
ted
Stat
esBi
rth
to 3
6 m
o2
No s
igni
fican
t diff
eren
ce in
ag
gres
sive
or
anxi
ous
beha
vior
(C
BCL)
Less
sev
ere
disc
iplin
e an
d gr
eate
r re
port
ed r
eadi
ng a
ctiv
ities
with
ch
ild a
t 62
mo.
Gre
ater
igno
ring
ch
ild m
isbe
havi
or a
t 36
mo,
but
not
at
62
mo
Min
kovi
tz e
t al25
, 26
Zuck
erm
an e
t al27
At 3
6 m
o of
age
hS, N
iede
rman
et a
l28Co
hort
N =
363,
Chi
cago
, IL
Birt
h to
36
mo
3Si
gnifi
cant
ly fe
wer
cas
es o
f de
velo
pmen
tal d
elay
(ch
art r
evie
w)
at 1
2 m
o po
stin
terv
entio
n
None
rep
orte
d
by guest on May 12, 2020www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 140, number 6, December 2017 9
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
Inte
rven
tion
Refe
renc
eSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion
Age,
Spe
cific
Pop
ulat
ion
Leve
ls o
f Evi
denc
eEf
fect
Child
out
com
esPa
rent
out
com
eshS
+ P
P, J
ohns
ton
et a
l15, 29
3-ar
m q
uasi
-ex
peri
men
tal
N =
439,
Pac
ific
Nort
hwes
t, Un
ited
Stat
es
Birt
h to
36
mo
mos
tly
high
er in
com
e fa
mili
es
2Re
duce
d ag
gres
sive
beh
avio
r (C
BCL)
at
30
mo
post
inte
rven
tion
Redu
ced
mat
erna
l dep
ress
ion
sym
ptom
sco
res
(CES
-D)
at 3
mo
but
high
er d
epre
ssio
n sc
ores
and
low
er
pare
nt s
atis
fact
ion
(PSo
C) a
mon
g in
terv
entio
n gr
oup
at 3
0 m
oNo
diff
eren
ce in
lang
uage
de
velo
pmen
t (M
CDI)
or a
nxio
us
beha
vior
(CB
CL)
at 3
or
30 m
o po
stin
terv
entio
n
No d
iffer
ence
in n
urtu
ring
inte
ract
ions
, pa
rent
sel
f-effi
cacy
(PS
oC)
CFD,
Ert
em e
t al16
Sequ
entia
lly c
ondu
cted
co
ntro
l tri
alN
= 23
3, A
nkar
a,
Turk
eyBi
rth
to 2
3 m
o lo
w
to m
iddl
e in
com
e fa
mili
es
2No
ne r
epor
ted
Incr
ease
d no
. of f
amily
mad
e to
ys,
RR =
4.0
(2.
3, 7
.1),
and
read
ing
to
child
, RR
= 5.
6 (2
.0, 1
5.8)
, at 1
mo
post
inte
rven
tion.
No
diffe
renc
e in
qua
lity
of th
e ho
me
lear
ning
en
viro
nmen
t (ho
ME)
CFD,
Jin
et a
l30Qu
asi-e
xper
imen
tal
N =
100,
Anh
ui, C
hina
Birt
h to
24
mo
low
in
com
e fa
mili
es, r
ural
2Im
prov
ed a
dapt
ive,
lang
uage
and
so
cial
dev
elop
men
t (GS
) 6
mo
post
inte
rven
tion
None
rep
orte
d
No d
iffer
ence
in m
otor
dev
elop
men
tTo
uchp
oint
s, F
arbe
r31Qu
asi-e
xper
imen
tal
N =
50, W
ashi
ngto
n,
DCBi
rth
to 1
8 m
o lo
w
inco
me
fam
ilies
2Im
prov
ed r
ecep
tive
and
expr
essi
ve
lang
uage
dev
elop
men
t (M
CDI)
at
exit
(ave
rage
age
16
mo)
Grea
ter
posi
tive
pare
ntin
g (A
API)
and
resi
lienc
e sc
ores
(RA
S) a
t exi
t (a
vera
ge a
ge 1
6 m
o)Po
C, B
rahm
et a
l32Qu
asi-e
xper
imen
tal
N =
102,
San
tiago
, Ch
ile2–
23 m
o lo
w in
com
e fa
mili
es2
None
rep
orte
dDe
crea
sed
mat
erna
l str
ess
(PSI
-SF)
for
child
ren
<12
mo
of a
ge, i
ncre
ased
m
ater
nal s
ensi
tivity
(Q-
Sort
) fo
r ch
ildre
n ag
ed 1
2–23
mo.
No
diffe
renc
e in
mat
erna
l dep
ress
ion
(PhQ
-9)
imm
edia
tely
aft
er
inte
rven
tion
Pare
ntin
g in
terv
entio
n,
Chan
g et
al33
Clus
ter
RCT
N =
501,
Jam
aica
, An
tigua
, St.
Luci
a3–
18 m
o1
Impr
ovem
ent i
n co
gniti
ve
deve
lopm
ent s
core
(GM
DS)
at 1
8 m
o of
age
Impr
oved
par
entin
g kn
owle
dge,
no
chan
ge in
par
entin
g be
havi
ors
(hoM
E) a
t 18
mo
of a
ge. N
o ch
ange
in
mat
erna
l dep
ress
ive
sym
ptom
s (C
ES-D
) at
18
mo
of a
geNo
diff
eren
ce in
lang
uage
de
velo
pmen
t (CD
I) at
18
mo
of a
geSD
P, S
hah
et a
l34Pr
ospe
ctiv
e co
hort
stu
dyN
= 30
, Chi
cago
, IL
6–12
mo
low
inco
me
fam
ilies
, Afr
ican
Am
eric
an o
r hi
span
ic
2No
ne r
epor
ted
Impr
oved
par
enta
l ver
bal
resp
onsi
vene
ss, a
nd p
aren
tal
invo
lvem
ent (
Stim
Q) a
t 4 w
k po
stin
terv
entio
n
AAPI
, Adu
lt-Ad
oles
cent
Par
entin
g In
vent
ory;
BSI
D, B
ayle
y Sc
ales
of I
nfan
t Dev
elop
men
t; CD
I, Co
mm
unic
ativ
e De
velo
pmen
t Inv
ento
ry; C
ES-D
, Cen
ter
for
Epid
emio
logi
c St
udie
s-De
pres
sion
Sca
le; G
MDS
, Gri
ffith
Men
tal D
evel
opm
ent S
cale
; GS,
Ges
ell S
cale
; ho
ME,
hom
e ob
serv
atio
n fo
r M
easu
rem
ent o
f the
Env
iron
men
t Inv
ento
ry; M
CDI,
Mac
Arth
ur C
omm
unic
ativ
e De
velo
pmen
t Inv
ento
ries
; NCA
ST, N
ursi
ng C
hild
Ass
essm
ent b
y Sa
telli
te T
rain
ing;
P/C
IS, P
aren
t/Ca
regi
ver
Invo
lvem
ent S
cale
; PhQ
-9, P
atie
nt
heal
th Q
uest
ionn
aire
-9; P
IDA,
Par
enta
l Inv
olve
men
t in
Deve
lopm
enta
l Adv
ance
men
t; PL
S-3,
Pre
scho
ol L
angu
age
Scal
e-3;
PSI
-SF,
Pare
ntin
g St
ress
Inde
x-Sh
ort F
orm
; PSo
C, P
aren
ting
Sens
e of
Com
pete
nce
Scal
e; R
AS, R
esili
ency
Att
itude
Sca
le; R
R, r
elat
ive
risk
; Stim
Q, a
val
idat
ed in
terv
iew
-bas
ed in
stru
men
t for
mea
sure
men
t of a
fam
ily’s
cog
nitiv
e ho
me
envi
ronm
ent;
Stim
QI, S
timQ
Infa
nt; S
timQT
, Stim
Q To
ddle
r.
TABL
e 4
Cont
inue
d
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

PEACoCK-ChAMBERS et al10
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABL
e 5
Gene
ral B
ehav
iora
l Dev
elop
men
t Int
erve
ntio
ns: R
esul
ts a
nd L
evel
s of
Evi
denc
e
Inte
rven
tion,
Ref
eren
ceSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion
Age,
Spe
cific
Pop
ulat
ion
Leve
ls o
f Evi
denc
eEf
fect
Child
out
com
esPa
rent
out
com
es
IY, R
eedt
z et
al35
RCT
N =
186,
Tro
mso
, No
rway
2–8
y1
Decr
ease
in b
ehav
ior
inte
nsity
(E
CBI-I
S) im
med
iate
ly a
fter
in
terv
entio
n, n
o di
ffere
nce
at 1
2 m
o po
stin
terv
entio
n
Redu
ced
use
of h
arsh
dis
cipl
ine
(PPI
), im
prov
ed p
ositi
ve p
aren
ting
(PPI
), pa
rent
sat
isfa
ctio
n at
12
mo
post
inte
rven
tion
Mea
n ag
e: 3
.9 y
high
beh
avio
ral i
nten
sity
No d
iffer
ence
in p
aren
ting
self-
effic
acy
(PSo
C)IY
, Per
rin
et a
l36RC
T an
d di
rect
as
sign
men
tN
= 17
3, G
reat
er B
osto
n ar
ea, U
nite
d St
ates
2–4
y1
Redu
ced
beha
vior
pro
blem
s an
d in
tens
ity (
ECBI
-IS)
at 6
and
12
mo
post
inte
rven
tion
Redu
ced
obse
rved
neg
ativ
e pa
rent
-ch
ild in
tera
ctio
n–su
ppor
tiven
ess/
nurt
urin
g (D
PICS
-R)
and
redu
ced
self-
repo
rted
neg
ativ
e pa
rent
ing
(PS)
at 1
2 m
oPo
or s
ocia
l-em
otio
nal
deve
lopm
ent
No d
iffer
ence
in o
bser
ved
disr
uptiv
e be
havi
or (
DPIC
S-R)
No d
iffer
ence
in o
bser
ved
nega
tive
pare
ntin
g–pa
rent
neg
ativ
ity/
host
ility
(DP
ICS-
R) a
t 12
mo
post
inte
rven
tion
Trip
le P
leve
l 2 &
3,
McC
onne
ll et
al37
Quas
i-exp
erim
enta
lN
= 92
3, A
lber
ta,
Cana
daBi
rth–
11 y
, mea
n ag
e: 2
.8 y
2No
ne r
epor
ted
No s
igni
fican
t diff
eren
ce in
per
sona
l di
stre
ss o
r ch
ild r
eari
ng d
istr
ess
(PSI
-SF)
, or
fam
ily fu
nctio
ning
(N
LSCY
) at
8–1
2 w
k po
stin
terv
entio
nTr
iple
P le
vel 3
, Tur
ner
and
Sand
ers38
RCT
N =
30, B
risb
ane,
Au
stra
lia2–
6 y,
mea
n ag
e: 3
.3 y
1Re
duce
d be
havi
or p
robl
ems
(PDR
, EC
BI-P
S, h
CPC)
, int
ensi
ty (
ECBI
-IS)
at 6
mo
post
inte
rven
tion
Impr
oved
dis
cipl
ine
styl
e (P
S) a
nd
satis
fact
ion
(PSo
C) a
t 6 m
o po
stin
terv
entio
nFa
mily
req
uest
ing
advi
ceNo
diff
eren
ce in
chi
ld d
isru
ptiv
e be
havi
or (
FoS)
No d
iffer
ence
in p
aren
t sel
f-effi
cacy
(P
CoS)
, pos
itive
par
entin
g (F
oS),
mat
erna
l dep
ress
ion,
anx
iety
, or
stre
ss (
DASS
)Tr
iple
P le
vel 3
, McC
orm
ick
et a
l39RC
TN
= 10
1, S
eatt
le, W
A1.
5–12
y1
No d
iffer
ence
in c
hild
beh
avio
r (C
BCL)
at 3
mo
post
inte
rven
tion.
No d
iffer
ence
in d
isci
plin
e (C
DS),
pare
nt s
atis
fact
ion
or s
elf-e
ffica
cy
(PCo
S) a
t 3 m
o po
stin
terv
entio
nM
ean
age:
4.8
yTr
iple
P le
vel 4
, Leu
ng
et a
l40RC
TN
= 69
, hon
g Ko
ng,
Chin
a3–
7 y
1Im
prov
ed b
ehav
ior
prob
lem
s (P
DR,
ECBI
-PS)
, int
ensi
ty (
ECBI
-IS),
cond
uct,
emot
ion,
hyp
erac
tivity
, an
d pe
er in
tera
ctio
ns (
SDQ)
im
med
iate
ly a
fter
inte
rven
tion
Impr
oved
sel
f-rep
orte
d di
scip
line
styl
e (P
S), p
aren
t sat
isfa
ctio
n, s
elf-
effic
acy
(PCo
S), a
nd m
arita
l hea
lth
(RQI
) im
med
iate
ly a
fter
inte
rven
tion
Mea
n ag
e: 4
.2 y
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 140, number 6, December 2017 11
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
Inte
rven
tion,
Ref
eren
ceSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion
Age,
Spe
cific
Pop
ulat
ion
Leve
ls o
f Evi
denc
eEf
fect
Child
out
com
esPa
rent
out
com
esTr
iple
P le
vel 4
, Leu
ng
et a
l41Co
hort
stu
dyN
= 48
0, h
ong
Kong
, Ch
ina
3 y
old
low
inco
me
fam
ilies
, chi
ld b
ehav
ior
prob
lem
3Im
prov
ed b
ehav
iora
l int
ensi
ty
(ECB
I) im
med
iate
ly
post
inte
rven
tion
Impr
oved
par
enta
l sat
isfa
ctio
n,
self-
effic
acy
(PSo
C), d
ecre
ased
pa
rent
ing
stre
ss (
PSI)
and
depr
essi
on, a
nxie
ty o
r st
ress
sy
mpt
oms
(DAS
S) im
med
iate
ly
post
inte
rven
tion
Trip
le P
leve
l 4, Z
ubri
ck
et a
l42Qu
asi-e
xper
imen
tal
N =
1610
, Wes
tern
Au
stra
lia36
–48
mo
2Im
prov
ed b
ehav
ior
inte
nsity
(E
CBI-I
S) a
t 12
and
24 m
o po
stin
terv
entio
n
Impr
oved
sel
f-rep
orte
d di
scip
line
styl
e (P
S), m
enta
l hea
lth (
DASS
), pa
rent
al
confl
ict d
ue to
par
entin
g (P
PC),
and
mar
ital h
ealth
(AD
AS)
at 1
2 an
d 24
m
o po
stin
terv
entio
nM
ean
age:
45
mo
Trip
le P
leve
l 4 a
nd 5
, Sa
nder
s et
al43
, 444
arm
RCT
No
cont
rol
beyo
nd 1
5 w
kN
= 30
5, B
risb
ane,
Au
stra
lia36
–48
mo
2Im
prov
ed d
isru
ptiv
e be
havi
or (
PDR)
an
d be
havi
oral
inte
nsity
(EC
BI)
at
12 m
o an
d 3
y po
stin
terv
entio
n.
No d
iffer
ence
bet
wee
n tr
eatm
ent
grou
ps
Impr
oved
par
ent c
ompe
tenc
e (P
CoS)
, di
scip
line
(PS)
, and
mar
ital c
onfli
ct
at 3
y. N
o di
ffere
nce
at 1
2 m
o po
stin
terv
entio
n
Mea
n ag
e: 4
1 m
oLo
w in
com
e fa
mili
es, h
igh
beha
vior
al in
tens
ityNo
diff
eren
ce in
dep
ress
ion,
anx
iety
, or
str
ess
(DAS
S) fo
r m
othe
rs o
r fa
ther
s at
12
mo
post
inte
rven
tion
Trip
le P
leve
l 4 a
nd 5
, Can
n et
al45
Coho
rt s
tudy
N =
589,
Mel
bour
ne,
Aust
ralia
1–15
y, m
ean
age:
4.5
y3
Impr
oved
beh
avio
ral i
nten
sity
an
d re
duce
d be
havi
or
prob
lem
s (E
CBI)
imm
edia
tely
po
stin
terv
entio
n.
Redu
ctio
n in
dys
func
tiona
l par
enta
l st
yles
(PS
), im
prov
ed p
aren
tal
satis
fact
ion
and
self-
effic
acy
(PCo
S),
impr
oved
dep
ress
ion,
anx
iety
, an
d st
ress
sym
ptom
s (D
ASS)
im
med
iate
ly p
ostin
terv
entio
nPa
rent
-chi
ld in
tera
ctio
n th
eory
, Ber
kovi
ts e
t al46
RCT
N =
30, G
aine
svill
e, F
L3–
6 y
1Im
prov
ed b
ehav
ior
inte
nsity
(EC
BI-
IS)
at 6
mo
post
inte
rven
tion
Impr
oved
sel
f-rep
orte
d co
nfide
nce
(PLo
C-SF
) an
d di
scip
line
styl
e (P
S)
at 6
mo
post
inte
rven
tion.
Univ
ersa
l par
entin
g pr
ogra
m/t
oddl
ers
with
out t
ears
, his
cock
et
al, 47
Bay
er e
t al48
Clus
ter
RCT
N =
733,
Mel
bour
ne,
Aust
ralia
8 m
o1
No d
iffer
ence
in e
xter
naliz
ing
or
inte
rnal
izin
g be
havi
ors
(CBC
L) a
t 10
, 16,
or
28 m
o of
age
Decr
ease
d un
reas
onab
le e
xpec
tatio
ns
(PBC
) at
16
and
28 m
o. D
ecre
ased
ha
rsh
disc
iplin
e (P
BC)
at 1
6 m
o, b
ut
not a
t 28
mo
of a
geNo
diff
eren
ce in
nur
turi
ng b
ehav
iors
(P
BC),
mat
erna
l dep
ress
ion,
anx
iety
, or
str
ess
(DAS
S)W
ebst
er-S
trat
ton,
Pa
tter
son
et a
l, 49
Stew
art-B
row
n et
al50
RCT
N =
116,
oxf
ord,
En
glan
d2–
8 y
1De
crea
sed
beha
vior
and
con
duct
pr
oble
ms
(SDQ
) at
6 m
o, b
ut n
ot
at 1
2 m
o po
stin
terv
entio
n. N
o di
ffere
nce
in b
ehav
ior
inte
nsity
(E
CBI-I
S), e
mot
ion,
hyp
erac
tivity
, or
pee
r in
tera
ctio
n
Redu
ctio
n in
dep
ress
ive
sym
ptom
s (G
hQ)
at 1
2 m
o po
stin
terv
entio
n
Mea
n ag
e: 4
.6 y
TABL
e 5
Cont
inue
d
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

General Behavioral Development
Four interventions resulted in decreased behavioral intensity between 2 and 24 months after the intervention: IY, 35, 36 Triple P levels 3 and 4, 38, 40 – 45 PCIT, 46 and PriCARE.53 Children engaged in the Webster-Stratton intervention exhibited fewer behavioral problems at 6 months, but this difference did not persist at the 12-month follow-up.49, 50 The Universal Parenting Program47, 48 and ezParent52 did not result in any difference in child behavior between the intervention and control groups.
A number of the behavioral interventions also affected parenting behaviors and psychological outcomes. IY resulted in improved positive parenting behaviors 12 months postintervention, 35, 36 and multiple interventions (IY, Triple P level 3 and 4, 38, 40, 42 PCIT, 46 and PriCARE53) led to reductions in the use of harsh discipline. Parental satisfaction, 35, 40, 41 self-efficacy, 40, 41, 43, 44 or confidence46 improved significantly with 3 different interventions, and marital health improved w, ith Triple P40 – 42 and Family Foundations.51 Although in most studies assessed parent mental health, only the Webster-Stratton49, 50 intervention and Family Foundations51 were associated with a reduction in depressive symptoms beyond 10 months postintervention.
Specific Developmental Topic
All 3 interventions designed to address infant colic revealed improvement in colic symptoms in short-term follow-up, but they resulted in mixed results beyond 2 months postintervention (Table 6). The Baby Business Program was also associated with lower maternal depressive symptom scores at 6 months postintervention.56 In contrast, The Happiest Baby video was associated with higher parental stress scores at 12 weeks postintervention.57
PEACoCK-ChAMBERS et al12
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
Inte
rven
tion,
Ref
eren
ceSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion
Age,
Spe
cific
Pop
ulat
ion
Leve
ls o
f Evi
denc
eEf
fect
Child
out
com
esPa
rent
out
com
esCh
ild b
ehav
ior
prob
lem
No d
iffer
ence
in to
tal m
enta
l hea
lth
scor
es (
GhQ)
or
pare
ntin
g st
ress
(P
SI)
Fam
ily F
ound
atio
n,
Fein
berg
et a
l51RC
T In
tent
ion
to T
reat
N =
399,
Uni
ted
Stat
esBi
rth
to 1
0 m
o m
iddl
e cl
ass,
mos
tly w
hite
1Im
prov
ed p
aren
t rep
orte
d so
otha
bilit
y, d
ecre
ased
nig
ht
wak
ing
at 1
0 m
o of
age
Impr
oved
pos
itive
cop
aren
ting
and
com
mun
icat
ion
(obs
erve
d),
and
qual
ity o
f mar
riag
e (Q
MI),
de
crea
sed
depr
essi
on (
CES-
D) a
nd
anxi
ety
sym
ptom
s (P
SWQ)
at 1
0 m
o of
age
ezPa
rent
, Bre
itens
tein
et
al52
RCT
N =
79, C
hica
go, I
L2–
5 y
low
-inco
me
fam
ilies
, m
ostly
Afr
ican
Am
eric
an
or L
atin
o
1No
diff
eren
ce in
chi
ld b
ehav
ior
(ECB
I) at
6 m
o po
stin
terv
entio
nNo
diff
eren
ce in
par
entin
g be
havi
or
(PQ)
, sel
f-effi
cacy
(TC
Q), o
r st
ress
(P
SI-S
F) a
t 6 m
o po
stin
terv
entio
nPr
iCAR
E, S
chill
ing
et a
l53RC
TN
= 12
0, P
hila
delp
hia,
PA
2–6
y1
Decr
ease
d be
havi
or p
robl
ems
(ECB
I) at
7 w
k po
st in
terv
entio
nIn
crea
sed
pare
ntal
em
path
y (A
API2
) an
d de
crea
sed
hars
h di
scip
line
at 7
w
k po
stin
terv
entio
nM
ean
age:
4.3
yLo
w in
com
e, c
hild
beh
avio
r pr
oble
m
AAIP
2, A
dult
Adol
esce
nt P
aren
ting
Inve
ntor
y –
2; A
DAS,
Abb
revi
ated
Dya
dic
adju
stm
ent s
cale
; CDS
, Chi
ld D
isci
plin
e Su
rvey
; CES
-D, C
ente
r fo
r Ep
idem
iolo
gic
Stud
ies-
Depr
essi
on S
cale
; DAS
S, D
epre
ssio
n-An
xiet
y-St
ress
Sca
le; D
PICS
-R, D
yadi
c Pa
rent
-Chi
ld
Inte
ract
ive
Codi
ng S
yste
m–R
evis
ed; E
CBI-I
S, E
yber
g Ch
ild B
ehav
ior
Inve
ntor
y-In
tens
ity S
cale
; ECB
I-PS,
Eyb
erg
Child
Beh
avio
r In
vent
ory-
Prob
lem
Sca
le; F
oS, F
amily
obs
erva
tion
Sche
dule
; GhQ
, Gen
eral
hea
lth Q
uest
ionn
aire
; hCP
C, h
ome
and
Com
mun
ity
Prob
lem
Che
cklis
t; NL
SCY,
Nat
iona
l Lon
gitu
dina
l Sur
vey
of C
hild
ren
and
Yout
h; P
BC, P
aren
t Be
havi
or C
heck
list;
PDR,
Par
ent
Daily
Rep
ort;
PLoC
-SF,
Pare
ntin
g Lo
cus
of C
ontr
ol S
hort
For
m; P
PC, P
aren
t Pr
oble
m C
heck
list;
PPI,
Pare
ntin
g Pr
actic
es
Inte
rvie
w; P
Q, P
aren
ting
Ques
tionn
aire
; PS,
Par
entin
g Sc
ale;
PSI
, Par
entin
g St
ress
Inde
x; P
SI-S
F, Pa
rent
ing
Stre
ss In
dex
Shor
t For
m; P
SoC,
Par
entin
g Se
nse
of C
ompe
tenc
e; P
SWQ,
Pen
n St
ate
Wor
ry Q
uest
ionn
aire
; QM
I, Qu
ality
of M
arri
age
Inde
x; R
QI,
Rela
tions
hip
Qual
ity In
dex;
SDQ
, Str
engt
h an
d Di
fficu
lty S
cale
; TCQ
, Tod
dler
Car
e Qu
estio
nnai
re.
TABL
e 5
Cont
inue
d
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 140, number 6, December 2017 13
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
TABL
e 6
Spec
ific
Deve
lopm
enta
l Top
ic In
terv
entio
ns: R
esul
ts a
nd L
evel
s of
Evi
denc
e
Inte
rven
tion,
Ref
eren
ceSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion,
Ag
eAg
e, S
peci
fic P
opul
atio
nLe
vels
of E
vide
nce
Effe
ct
Child
out
com
esPa
rent
out
com
es
Fam
ily-c
ente
red
trea
tmen
t, Sa
lisbu
ry
et a
l55
RCT
N =
62, U
nite
d St
ates
4–8
wk
1De
crea
sed
child
cry
ing
(h/d
) at
6 w
k an
d tim
e sp
ent f
eedi
ng a
t 6 a
nd 1
0 w
k po
stin
terv
entio
n
No d
iffer
ence
in m
ater
nal d
epre
ssiv
e sy
mpt
oms
(BDI
) or
str
ess
(PSI
) at
6
or 1
0 w
k po
stin
terv
entio
nIn
fant
s w
ith c
olic
, mos
tly
whi
teNo
diff
eren
ce in
tota
l h o
f sle
ep p
er d
BBP,
his
cock
et a
l56RC
TN
= 77
0, M
elbo
urne
, Au
stra
lia4–
13 w
k1
Decr
ease
d cr
ying
sev
erity
at 4
mo
of
age
and
few
er c
hang
ed fo
rmul
a at
6
mo
of a
ge. N
o di
ffere
nce
in s
leep
pr
oble
ms
or d
urat
ion
Decr
ease
d m
ater
nal d
oubt
at 4
mo
of
age,
and
dep
ress
ive
sym
ptom
s at
6
mo
of a
ge
high
inco
me
fam
ilies
No d
iffer
ence
in s
leep
qua
lity,
m
ater
nal a
nger
, saf
ety,
or
limit
sett
ing
T hB,
McR
ury
and
Zolo
tor57
RCT
N =
35, C
olum
bus,
oh
New
born
mid
dle
to h
igh
inco
me
fam
ilies
1No
diff
eren
ce in
cry
ing
(h/d
) or
sle
ep
(h/d
) at
6 o
r 12
wk
of a
geGr
eate
r pa
rent
al s
tres
s (P
SI)
in th
e in
terv
entio
n gr
oup
at 1
2 w
k of
age
Infa
nt m
assa
ge, S
heid
aei
et a
l58RC
TN
= 10
0 Ir
an<1
2 w
k1
Decr
ease
sev
erity
of c
olic
(VA
S),
dura
tion
of c
ryin
g (m
in/d
), an
d in
crea
sed
dura
tion
of s
leep
(m
in/d
) 1
wk
post
inte
rven
tion
None
rep
orte
d
Lite
racy
pro
mot
ing
inte
rven
tion,
hig
h
et a
l59
RCT
N =
205,
Uni
ted
Stat
es5–
11 m
o lo
w in
com
e,
mul
tieth
nic
fam
ilies
1In
crea
sed
rece
ptiv
e vo
cabu
lary
in
chi
ldre
n 13
–17
mo
of a
ge,
expr
essi
ve v
ocab
ular
y in
chi
ldre
n 18
–25
mo
of a
ge (
MCD
I-SF)
Incr
ease
d fr
eque
ncy
of r
eadi
ng a
t be
dtim
e (d
/wk)
at m
ean
age
of
18 m
o
RoR,
Silv
erst
ein
et a
l60Pr
e/po
st q
ualit
y im
prov
emen
tN
= 17
3, S
eatt
le, W
A5.
5 m
o–6
y4
Grea
ter
repo
rt o
f rea
ding
as
favo
rite
act
ivity
imm
edia
tely
aft
er
inte
rven
tion
Grea
ter
repo
rt o
f rea
ding
alo
ud a
s fa
vori
te a
ctiv
ity, >
10 c
hild
ren’
s bo
oks
in h
ome,
and
rea
ding
alo
ud
at le
ast o
nce
per
wk
imm
edia
tely
po
stin
terv
entio
nGr
eate
st e
ffect
for
non-
Engl
ish
spea
kers
RoR,
Nee
dlm
an e
t al6
Quas
i-exp
erim
enta
l hi
stor
ical
con
trol
sN
= 16
47, 1
0 st
ates
in
Unite
d St
ates
6–72
mo
4No
ne r
epor
ted
Grea
ter
repo
rt o
f rea
ding
alo
ud a
s fa
vori
te a
ctiv
ity, >
10 c
hild
ren’
s bo
oks
in h
ome,
and
rea
ding
alo
ud
at b
edtim
e, a
nd a
loud
≥3
per
wk
imm
edia
tely
pos
tinte
rven
tion
Grea
test
effe
ct fo
r pa
rent
s w
ith le
ss
than
a c
ompl
eted
hig
h sc
hool
ed
ucat
ion.
RoR,
Jon
es e
t al61
Quas
i-exp
erim
enta
l Pr
ospe
ctiv
e co
ntro
lled
stud
y
N =
352,
Lou
isvi
lle, K
Y2–
24 m
o2
None
rep
orte
dM
ore
likel
y to
rep
ort e
njoy
men
t in
shar
ed r
eadi
ng 2
y p
ostin
terv
entio
n
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

Three interventions in which the promotion of early literacy was evaluated had relatively consistent results. Three ROR studies revealed a significant increase in the number of parents reporting reading aloud as their favorite activity with their child or increased frequency of reading on a weekly basis in cross-sectional samples or quasi-experimental studies.6, 60, 61 These effects were stronger among non-English speaking families60 and families with less than a completed high school education.6 The ROR + M intervention resulted in greater mathematics engagement by parents as well.62 The Literacy Promoting Intervention by High et al59 was associated with increased receptive and expressive vocabulary.
DIsCussIOn
In the past 15 years, multiple new interventions have been developed and tested in connection with primary care settings with the goal of improving the developmental trajectories of young children. Twenty-four interventions are included in this review, with data from 48 studies, primarily evaluated by RCT or quasi-experimental study design. A number of these interventions were evaluated across multiple cities and countries in studies with >3000 participants.
The evolution of interventions to promote development of young children in primary care settings is evident when comparing our findings to those of the systematic review by Regalado and Halfon4 in 2001. As documented in the previous review, educational interventions were focused on positive parent-child interactions and improved parental knowledge about child development but did not change parenting behavior or child development outcomes.63 – 65 In contrast, 2 interventions explicitly designed to improve parental confidence and
PEACoCK-ChAMBERS et al14
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
Inte
rven
tion,
Ref
eren
ceSt
udy
Desi
gnSa
mpl
e Si
ze, L
ocat
ion,
Ag
eAg
e, S
peci
fic P
opul
atio
nLe
vels
of E
vide
nce
Effe
ct
Child
out
com
esPa
rent
out
com
esLo
w in
com
e fa
mili
es,
mos
tly A
fric
an
Amer
ican
R oR
+ M
, Jon
es e
t al62
Coho
rt s
tudy
N =
72, S
outh
ern
Unite
d St
ates
12–3
6 m
o3
None
rep
orte
dIn
crea
sed
read
ing
activ
ities
rel
ated
to
mat
h (c
ount
ing,
sha
pes,
num
bers
, ad
ditio
n/su
btra
ctio
n, a
nd p
ositi
on),
mat
hem
atic
s en
gage
men
t sco
re a
t 3
wk
post
inte
rven
tion
Low
inco
me
fam
ilies
, m
ostly
Afr
ican
Am
eric
an
BBP,
Bab
y Bu
sine
ss P
rogr
am; B
DI, B
eck
Depr
essi
on In
vent
ory;
MCD
I-SF,
Mac
Arth
ur C
omm
unic
atio
n an
d De
velo
pmen
t Inv
ento
ries
– S
hort
For
m; P
SI, P
aren
ting
Stre
ss In
dex;
ThB
, The
hap
pies
t Bab
y; V
AS, V
isua
l Ana
log
Scal
e.
TABL
e 6
Cont
inue
d
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

competence through skill building66 and coaching5 enhanced the quality of parent-child interactions in small trials (<50 participants).
The interventions summarized in this review continued this trajectory of incorporating new strategies to enhance parental skill building and parent-child interactions supported by behavior change theory.67, 68 These strategies included vicarious learning from peers, role play, homework, feedback through coaching, videotaped observation, and identification of parenting strengths. In some studies, the parental factors that could explain mechanisms of action were measured and included parental resilience, 31 satisfaction, 15, 35, 38 – 40, 45 self- efficacy, 15, 35, 38 – 40, 45, 46, 52 and stress.17, 18, 32, 38, 44, 45, 52 The authors of studies of behavioral interventions also frequently explored the impact on parental mental health as a potential mediating factor.42, 47 –51
The primary challenge in synthesizing and drawing firm conclusions about the efficacy or effectiveness of specific interventions, however, lies in the heterogeneity of outcome measures and reported findings. Among the general developmental studies, a different child outcome measure was used in almost every study, and 3 studies16, 32, 34 had no child outcome measures as part of the evaluation, making comparisons across these studies difficult. Even among studies of the same interventions, the results varied in terms of the time when evaluations occurred and the specific outcome measures that demonstrated improvement (eg, prevention of developmental delay versus behavior problems in VIP and HS studies).18, 23, 26, 28 The behavioral development studies were more consistent in their use of the CBCL or Eyberg Child Behavior Inventory (ECBI) as outcome measures of child behavioral problems.
Greater consensus on which child outcomes are most important from a clinical perspective and which validated tools are optimal for assessment of these outcomes is needed, particularly for general developmental interventions. Other specialties, such as mental health, face similar challenges69 and may serve as examples for future standardization of quality and outcome measures.70, 71 With respect to general developmental outcomes, measures of language development may be particularly important given the disparities that exist in this developmental domain72, 73 and the association with later academic achievement.74, 75 Studies with longer follow-up periods, such as studies of home visiting or preschool programs, 76, 77 may help identify measures in early childhood that predict long-term health and academic success. The behavioral development studies showed more consistent impact on the clinically relevant measures of behavioral intensity and behavior problems.
Although the factors related to the mechanism of action of interventions were assessed in many studies, the variability of results limits our ability to understand precisely why some interventions work over others, who benefits from interventions, and what may be the common pathway by which different interventions impact the same outcomes. This basic understanding is necessary to inform future policy and services.3 The collection of VIP studies provides an example research strategy to thoroughly study an intervention. The studies identified families that benefited most (on the basis of education level), 18 potential mechanism of action (mediators including responsive parenting and maternal depression), 20 and explored clinically significant outcomes such as language, harsh discipline, and social emotional development.21, 23
In addition to examining the individual mechanism of action of the interventions, researchers for future studies should attempt to identify key components that may be common across multiple interventions. Drawing again from the mental health literature, the examination of key components should include intervention content as well as factors that impact the process of intervention delivery (eg, participant and provider attitudes, specific types of interactions, and provider approach to influencing behavior change).78 Common elements of evidence-based psychologic treatments for adult anxiety and depression, for example, include altering cognitive appraisal, modifying emotion-driven behavior, preventing emotional avoidance, 79 as well as demonstrations of warmth and empathy, clear explanations, focused discussion on practical concerns, and well-organized sessions.78 Identification of common key components of developmental interventions could have implications for the feasibility of dissemination of these interventions into community settings where the majority of children receive primary care.
Several notable gaps in the literature limit the feasibility of replicating individual interventions in community settings. First, the cost of many of the identified interventions is not well described. VIP and HS reported relatively low costs compared with programs such as home visiting or Early Head Start, although both required a child development specialist.20, 26, 27 The descriptions of trainings are similarly limited. Most of the interventions were delivered by child development specialists or health care professionals that likely bring additional skills and knowledge to interactions with parents. Access to child development specialists is limited in rural settings; thus, understanding the specific skills
PEDIATRICS Volume 140, number 6, December 2017 15
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

needed to conduct the intervention is critical. Chang et al33 provided an example of a detailed description of paraprofessionals training that could be used in resource-limited settings.
Implications
Although multiple studies showed positive change in a number of different child development and parental outcomes, the heterogeneity of results limit the clear distinction between effective and noneffective interventions. To identify the services and policies that will optimally promote the development of young children, we need a clear understanding of the end point we are collectively trying to achieve. We need greater consensus on the best measures of these outcomes, and we need to understand why interventions work and who benefits most. When considering implementation of these interventions in community settings, health professionals must consider the availability and expertise of their staff and the cost of training and implementation. Examples of highly targeted interventions delivered by paraprofessionals may provide some direction for future dissemination strategies.33, 34
Limitations
This review has several limitations. Only articles published in English were reviewed. In addition, the inclusion criteria requiring a connection to primary care limited the focus to US populations and countries with similar health systems. Initially, we considered
limiting our review to studies conducted in the United States given the significant differences between health care systems around the world. Ultimately, we sought to include international studies because multiple interventions were studied in the United States and internationally, and interventions designed for settings with varying levels of resource allocation may also be relevant to lower-resource or rural settings in the United States. Our review may have missed eligible studies for various reasons. Although our search terms were intentionally broad, other terms used to describe similar interventions may have resulted in missed studies. Additional studies may have been missed or excluded because of ambiguity with respect to the age of children enrolled or the connection to primary care. Interventions conducted without a connection to primary care were excluded even if other primary care–based studies of the same intervention were included. We also excluded studies targeting specific populations such as extremely premature infants and parents with diagnosed depression or substance abuse disorders because these populations frequently require targeted therapies or treatment with medication. Finally, the Levels of Evidence system used to summarize and compare the study designs across interventions is not a definitive indicator of the quality of the study because it does not assess bias related to blinding, instrument validation, or observer versus self-report measures. The decision to use this system was based on feasibility
given the variety of study designs used and the variability of reported factors that impact study quality.
COnCLusIOns
Several interventions delivered in primary care settings can positively impact developmental and behavioral trajectories of children aged 0 to 3 years. These interventions involve the child’s parents and frequently a team of health professionals. Common measures of child development outcomes are needed to compare efficacy across studies. Further exploration of why certain interventions work and who benefits from interventions could inform future policy to make these services more widely available.
ABBRevIATIOns
BB: Building BlocksCBCL: Child Behavior ChecklistCFD: Care for DevelopmentECBI: Eyberg Child Behavior
InventoryHS: Healthy StepsIY: Incredible YearsPCIT: Parent-Child Interaction
TherapyPOC: Play with Our ChildrenPP: PrePareRCT: randomized controlled trialROR: Reach Out and ReadROR + M: Reach Out and Read
plus MathematicsSDP: Sit Down and PlayTriple P: Positive Parenting
ProgramVIP: Video Interaction Project
PEACoCK-ChAMBERS et al16
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
Accepted for publication Sep 11, 2017
Address correspondence to Elizabeth Peacock-Chambers, MD, MSc, Department of Pediatrics, Baystate Medical Center, 3601 Main St, Springfield, MA 01199. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
FInAnCIAL DIsCLOsuRe: The authors have indicated they have no financial relationships relevant to this article to disclose.
FunDInG: Supported by a health Resources and Services Administration T32 grant hP10028 (I09940000730) from June 2014 to June 2015.
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

ReFeRenCes
1. Shonkoff JP, Garner AS; Committee on Psychosocial Aspects of Child and Family health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. The lifelong effects of early childhood adversity and toxic stress. Pediatrics. 2012;129(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 129/ 1/ e232
2. hagan JF, Shaw JS, Duncan PM. Bright Futures: Guidelines for Health Supervision of Infants, Children and Adolescents, 4th ed.. Elk Grove Village, IL: American Academy of Pediatrics; 2017
3. Garner AS, Shonkoff JP; Committee on Psychosocial Aspects of Child and Family health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics. Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics. 2012;129(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 129/ 1/ e224
4. Regalado M, halfon N. Primary care services promoting optimal child development from birth to age 3 years: review of the literature. Arch Pediatr Adolesc Med. 2001;155(12):1311–1322
5. Bristor MW, helfer RE, Coy KB. Effects of perinatal coaching on mother-infant interaction. Am J Dis Child. 1984;138(3):254–257
6. Needlman R, Toker Kh, Dreyer BP, Klass P, Mendelsohn AL. Effectiveness of a primary care intervention to support reading aloud: a multicenter evaluation. Ambul Pediatr. 2005;5(4):209–215
7. Lucassen PL, Assendelft WJ, Gubbels JW, van Eijk JT, van Geldrop WJ, Neven AK. Effectiveness of treatments for infantile colic: systematic review. BMJ. 1998;316(7144):1563–1569
8. Pinilla T, Birch LL. help me make it through the night: behavioral entrainment of breast-fed infants’
sleep patterns. Pediatrics. 1993;91(2):436–444
9. Sege RD, Perry C, Stigol L, et al. Short-term effectiveness of anticipatory guidance to reduce early childhood risks for subsequent violence. Arch Pediatr Adolesc Med. 1997;151(4):392–397
10. Sia C, Tonniges TF, osterhus E, Taba S. history of the medical home concept. Pediatrics. 2004;113(suppl 5):1473–1478
11. Coker TR, Windon A, Moreno C, Schuster MA, Chung PJ. Well-child care clinical practice redesign for young children: a systematic review of strategies and tools. Pediatrics. 2013;131(suppl 1):S5–S25
12. Shah R, Kennedy S, Clark MD, Bauer SC, Schwartz A. Primary care-based interventions to promote positive parenting behaviors: a meta-analysis. Pediatrics. 2016;137(5):e20153393
13. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–1012
14. oxford Centre for Evidence-Based Medicine. oCEBM levels of evidence. 2011. Available at: www. cebm. net/ index. aspx? o= 5653. Accessed october 15, 2017
15. Johnston BD, huebner CE, Anderson ML, Tyll LT, Thompson RS. healthy Steps in an integrated delivery system: child and parent outcomes at 30 months. Arch Pediatr Adolesc Med. 2006;160(8):793–800
16. Ertem Io, Atay G, Bingoler BE, Dogan DG, Bayhan A, Sarica D. Promoting child development at sick-child visits: a controlled trial. Pediatrics. 2006;118(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 118/ 1/ e124
17. Mendelsohn AL, Dreyer BP, Flynn V, et al. Use of videotaped interactions during pediatric well-child care
to promote child development: a randomized, controlled trial. J Dev Behav Pediatr. 2005;26(1):34–41
18. Mendelsohn AL, Valdez PT, Flynn V, et al. Use of videotaped interactions during pediatric well-child care: impact at 33 months on parenting and on child development. J Dev Behav Pediatr. 2007;28(3):206–212
19. Mendelsohn AL, huberman hS, Berkule SB, Brockmeyer CA, Morrow LM, Dreyer BP. Primary care strategies for promoting parent-child interactions and school readiness in at-risk families: the Bellevue Project for Early Language, Literacy, and Education Success. Arch Pediatr Adolesc Med. 2011;165(1):33–41
20. Berkule SB, Cates CB, Dreyer BP, et al. Reducing maternal depressive symptoms through promotion of parenting in pediatric primary care. Clin Pediatr (Phila). 2014;53(5):460–469
21. Canfield CF, Weisleder A, Cates CB, et al. Primary care parenting intervention and its effects on the use of physical punishment among low-income parents of toddlers. J Dev Behav Pediatr. 2015;36(8):586–593
22. Cates CB, Weisleder A, Dreyer BP, et al. Leveraging healthcare to promote responsive parenting: impacts of the Video Interaction Project on parenting stress. J Child Fam Stud. 2016;25(3):827–835
23. Weisleder A, Cates CB, Dreyer BP, et al. Promotion of positive parenting and prevention of socioemotional disparities. Pediatrics. 2016;137(2):e20153239
24. Caughy MoB, huang K-Y, Miller T, Genevro JL. The effects of the healthy Steps for Young Children Program: results from observations of parenting and child development. Early Child Res Q. 2004;19(4):611–630
25. Minkovitz CS, hughart N, Strobino D, et al. A practice-based intervention to enhance quality of care in the first 3 years of life: the healthy Steps
PEDIATRICS Volume 140, number 6, December 2017 17
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
POTenTIAL COnFLICT OF InTeResT: The authors have indicated they have no potential conflicts of interest to disclose.
COMPAnIOn PAPeR: A companion to this article is available online at www. pediatrics. org/ cgi/ doi/ 10. 1542/ peds. 2017- 3136.
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

for Young Children Program. JAMA. 2003;290(23):3081–3091
26. Minkovitz CS, Strobino D, Mistry KB, et al. healthy Steps for Young Children: sustained results at 5.5 years. Pediatrics. 2007;120(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 120/ 3/ e658
27. Zuckerman B, Parker S, Kaplan-Sanoff M, Augustyn M, Barth MC. healthy Steps: a case study of innovation in pediatric practice. Pediatrics. 2004;114(3):820–826
28. Niederman LG, Schwartz A, Connell KJ, Silverman K. healthy Steps for Young Children program in pediatric residency training: impact on primary care outcomes. Pediatrics. 2007;120(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 120/ 3/ e596
29. Johnston BD, huebner CE, Tyll LT, Barlow WE, Thompson RS. Expanding developmental and behavioral services for newborns in primary care; effects on parental well-being, practice, and satisfaction. Am J Prev Med. 2004;26(4):356–366
30. Jin X, Sun Y, Jiang F, Ma J, Morgan C, Shen X. “Care for development” intervention in rural China: a prospective follow-up study. J Dev Behav Pediatr. 2007;28(3):213–218
31. Farber ML. Parent mentoring and child anticipatory guidance with Latino and African American families. Health Soc Work. 2009;34(3):179–189
32. Brahm P, Cortázar A, Fillol MP, Mingo MV, Vielma C, Aránguiz MC. Maternal sensitivity and mental health: does an early childhood intervention programme have an impact? Fam Pract. 2016;33(3):226–232
33. Chang SM, Grantham-McGregor SM, Powell CA, et al. Integrating a parenting intervention with routine primary health care: a cluster randomized trial. Pediatrics. 2015;136(2):272–280
34. Shah R, DeFrino D, Kim Y, Atkins M. Sit Down and Play: a preventative primary care-based program to enhance parenting practices. J Child Fam Stud. 2017;26(2):540–547
35. Reedtz C, handegård Bh, Mørch WT. Promoting positive parenting practices in primary pare: outcomes and mechanisms of change in
a randomized controlled risk reduction trial. Scand J Psychol. 2011;52(2):131–137
36. Perrin EC, Sheldrick RC, McMenamy JM, henson BS, Carter AS. Improving parenting skills for families of young children in pediatric settings: a randomized clinical trial. JAMA Pediatr. 2014;168(1):16–24
37. McConnell D, Breitkreuz R, Savage A. Independent evaluation of the Triple P Positive Parenting Program in family support service settings. Child Fam Soc Work. 2012;17(1):43–54
38. Turner KM, Sanders MR. help when it’s needed first: a controlled evaluation of brief, preventive behavioral family intervention in a primary care setting. Behav Ther. 2006;37(2):131–142
39. McCormick E, Kerns SE, McPhillips h, Wright J, Christakis DA, Rivara FP. Training pediatric residents to provide parent education: a randomized controlled trial. Acad Pediatr. 2014;14(4):353–360
40. Leung C, Sanders MR, Leung S, Mak R, Lau J. An outcome evaluation of the implementation of the Triple P-Positive Parenting Program in hong Kong. Fam Process. 2003;42(4):531–544
41. Leung C, Sanders M, Ip F, Lau J. Implementation of Triple P Positive Parenting Program in hong Kong: predictors of programme completion and clinical outcomes. J Child Serv. 2006;1(2):4–17
42. Zubrick SR, Ward KA, Silburn SR, et al. Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prev Sci. 2005;6(4):287–304
43. Sanders MR, Markie-Dadds C, Tully LA, Bor W. The triple P-Positive Parenting Program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. J Consult Clin Psychol. 2000;68(4):624–640
44. Sanders MR, Bor W, Morawska A. Maintenance of treatment gains: a comparison of enhanced, standard, and self-directed Triple P-Positive Parenting Program. J Abnorm Child Psychol. 2007;35(6):983–998
45. Cann W, Rogers h, Matthews J. Family Intervention Services program evaluation: a brief report on initial outcomes for families. AeJAMH. 2003;2(3):208–215
46. Berkovits MD, o’Brien KA, Carter CG, Eyberg SM. Early identification and intervention for behavior problems in primary care: a comparison of two abbreviated versions of Parent-Child Interaction Therapy. Behav Ther. 2010;41(3):375–387
47. hiscock h, Bayer JK, Price A, Ukoumunne oC, Rogers S, Wake M. Universal parenting programme to prevent early childhood behavioural problems: cluster randomised trial. BMJ. 2008;336(7639):318–321
48. Bayer JK, hiscock h, Ukoumunne oC, Scalzo K, Wake M. Three-year-old outcomes of a brief universal parenting intervention to prevent behaviour problems: randomised controlled trial. Arch Dis Child. 2010;95(3):187–192
49. Patterson J, Barlow J, Mockford C, Klimes I, Pyper C, Stewart-Brown S. Improving mental health through parenting programmes: block randomised controlled trial. Arch Dis Child. 2002;87(6):472–477
50. Stewart-Brown S, Patterson J, Mockford C, Barlow J, Klimes I, Pyper C. Impact of a general practice based group parenting programme: quantitative and qualitative results from a controlled trial at 12 months. Arch Dis Child. 2004;89(6):519–525
51. Feinberg ME, Jones DE, hostetler ML, Roettger ME, Paul IM, Ehrenthal DB. Couple-focused prevention at the transition to parenthood, a randomized trial: effects on coparenting, parenting, family violence, and parent and child adjustment. Prev Sci. 2016;17(6):751–764
52. Breitenstein SM, Fogg L, ocampo EV, Acosta DI, Gross D. Parent use and efficacy of a self-administered, tablet-based parent training intervention: a randomized controlled trial. JMIR Mhealth Uhealth. 2016;4(2):e36
53. Schilling S, French B, Berkowitz SJ, Dougherty SL, Scribano PV, Wood JN. Child-Adult Relationship Enhancement in Primary Care (PriCARE): a randomized trial of a parent training
PEACoCK-ChAMBERS et al18
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

for child behavior problems. Acad Pediatr. 2017;17(1):53–60
54. Gurwitch Rh, Messer EP, Masse J, olafson E, Boat BW, Putnam FW. Child-Adult Relationship Enhancement (CARE): an evidence-informed program for children with a history of trauma and other behavioral challenges. Child Abuse Negl. 2016;53:138–145
55. Salisbury AL, high P, Twomey JE, et al. A randomized control trial of integrated care for families managing infant colic. Infant Ment Health J. 2012;33(2):110–122
56. hiscock h, Cook F, Bayer J, et al. Preventing early infant sleep and crying problems and postnatal depression: a randomized trial. Pediatrics. 2014;133(2). Available at: www. pediatrics. org/ cgi/ content/ full/ 133/ 2/ e346
57. McRury JM, Zolotor AJ. A randomized, controlled trial of a behavioral intervention to reduce crying among infants. J Am Board Fam Med. 2010;23(3):315–322
58. Sheidaei A, Abadi A, Zayeri F, Nahidi F, Gazerani N, Mansouri A. The effectiveness of massage therapy in the treatment of infantile colic symptoms: a randomized controlled trial. Med J Islam Repub Iran. 2016;30(1):356–363
59. high PC, LaGasse L, Becker S, Ahlgren I, Gardner A. Literacy promotion in primary care pediatrics: can we make a difference? Pediatrics. 2000;105(4 pt 2):927–934
60. Silverstein M, Iverson L, Lozano P. An English-language clinic-based literacy program is effective for a multilingual population. Pediatrics. 2002;109(5). Available at: www. pediatrics. org/ cgi/ content/ full/ 109/ 5/ e76
61. Jones VF, Franco SM, Metcalf SC, Popp R, Staggs S, Thomas AE. The value of book distribution in a clinic-based literacy intervention program. Clin Pediatr (Phila). 2000;39(9):535–541
62. Jones VF, Brown ET, Molfese V, et al. The development and initial assessment of Reach out and Read plus Mathematics for use in primary care paediatrics. Early Child Dev Care. 2015;185(5):694–708
63. Chamberlin RW, Szumowski EK, Zastowny TR. An evaluation of efforts to educate mothers about child development in pediatric office practices. Am J Public Health. 1979;69(9):875–886
64. Chamberlin RW, Szumowski EK. A follow-up study of parent education in pediatric office practices: impact at age two and a half. Am J Public Health. 1980;70(11):1180–1188
65. Dworkin Ph, Allen D, Geertsma A, Solkoske L, Cullina J. Does developmental content influence the effectiveness of anticipatory guidance? Pediatrics. 1987;80(2):196–202
66. Casey Ph, Whitt JK. Effect of the pediatrician on the mother-infant relationship. Pediatrics. 1980;65(4):815–820
67. Bandura A. human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–1184
68. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211
69. Slade M, Thornicroft G, Glover G. The feasibility of routine outcome measures in mental health. Soc Psychiatry Psychiatr Epidemiol. 1999;34(5):243–249
70. Sartorius N. Patient-reported outcomes in psychiatry. Dialogues Clin Neurosci. 2014;16(2):123–124
71. Pincus hA, England MJ. Improving the quality of psychosocial interventions for mental and substance use disorders: a report from the IoM. JAMA. 2015;314(12):1227–1228
72. hart B, Risley TR. Meaningful Differences in the Everyday Experience of Young American Children. Baltimore, MD: P.h. Brookes; 1995
73. Johnson SB, Riis JL, Noble KG. State of the art review: poverty and the developing brain. Pediatrics. 2016;137(4):e20153075
74. Bashir AS, Scavuzzo A. Children with language disorders: natural history and academic success. J Learn Disabil. 1992;25(1):53–65; discussion 66–70
75. Silva PA, Williams S, McGee R. A longitudinal study of children with developmental language delay at age three: later intelligence, reading and behaviour problems. Dev Med Child Neurol. 1987;29(5):630–640
76. McCormick MC, Brooks-Gunn J, Buka SL, et al. Early intervention in low birth weight premature infants: results at 18 years of age for the Infant health and Development Program. Pediatrics. 2006;117(3):771–780
77. Eckenrode J, Campa M, Luckey DW, et al. Long-term effects of prenatal and infancy nurse home visitation on the life course of youths: 19-year follow-up of a randomized trial. Arch Pediatr Adolesc Med. 2010;164(1):9–15
78. Wissow L, Anthony B, Brown J, et al. A common factors approach to improving the mental health capacity of pediatric primary care. Adm Policy Ment Health. 2008;35(4):305–318
79. Moses EB, Barlow Dh. A new unified treatment approach for emotional disorders based on emotion science. Curr Dir Psychol Sci. 2006;15(3):146–150
PEDIATRICS Volume 140, number 6, December 2017 19
Peacock-Chambers et alPrimary Care Interventions for Early Childhood Development: A Systematic Review
2017
https://doi.org/10.1542/peds.2017-1661
6PediatricsROUGH GALLEY PROOF
December 2017
140
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-1661 originally published online November 14, 2017; 2017;140;Pediatrics
Elizabeth Peacock-Chambers, Kathryn Ivy and Megan Bair-MerrittReview
Primary Care Interventions for Early Childhood Development: A Systematic
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/140/6/e20171661including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/140/6/e20171661#BIBLThis article cites 76 articles, 23 of which you can access for free at:
Subspecialty Collections
milestones_subhttp://www.aappublications.org/cgi/collection/growth:development_Growth/Development Milestonesal_issues_subhttp://www.aappublications.org/cgi/collection/development:behaviorDevelopmental/Behavioral Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on May 12, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2017-1661 originally published online November 14, 2017; 2017;140;Pediatrics
Elizabeth Peacock-Chambers, Kathryn Ivy and Megan Bair-MerrittReview
Primary Care Interventions for Early Childhood Development: A Systematic
http://pediatrics.aappublications.org/content/140/6/e20171661located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2017 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 12, 2020www.aappublications.org/newsDownloaded from





























