Embed Size (px)
Citation preview
Primary Care Asthma
Program
Spirometry Manual
Version 2018

Primary Care Asthma Program SPIROMETRY MANUAL TABLE OF CONTENTS
PCAP SPIROMETRY MANUAL: TABLE OF CONTENTS Version: January 2018
1.0 Introduction/Background
Primary Care Asthma Program (PCAP) Background-Spirometry - 1 page
2.0 PCAP Policy & Procedures
PCAP Spirometry Policy and Procedures (April 2012) - 10 pages
PCAP Medical Directive for Ordering Spirometry at a Primary Care Site (Jan 2018) - 2 pages
PCAP Medical Directive for Administration of Salbutamol for Spirometry Testing at a Primary Care Site (Jan
2018) – 2 pages
PCAP Medical Directive for Performing Spirometry Pre & Post Bronchodilator at a Primary Care Site (Jan 2018)
– 4 pages
Sample of a Spirometry Requisition Order Form (From Coates AL et al. Spirometry in Primary Care. Can Respir J
2013; 20(1); 13-20) - 1 page
Sample of a Spirometry Report Form (From Coates AL et al. Spirometry in Primary Care. Can Respir J 2013;
20(1); 13-20) – 1 page
3.0 Spirometry Practicum
The Lung Association Spirometry Interpretation Guide (Jan 2018) - 1 page
PCAP Spirometry Operator Checklist Tool (December 2013) – 2 pages
Get Valid Spirometry Results Every Time (From U.S. Department of Health and Human Services : Centers for Disease Control and Prevention National Institute for Occupational Safety and Health (NIOSH)) – 1 page
4.0 Standards
ATS/ERS Task Force Standardisation of Lung Function Testing: Standardisation of Spirometry (2005) – 20 pages
CTS 2013 Spirometry in Primary Care – 10 pages
ATS/ERS Recommendations for a Standardized Pulmonary Function Report – 9 pages
PCAP Resource Links for Standards in Spirometry – 1 page

Section 1 Introduction/Background
1
Primary Care Asthma Program SPIROMETRY MANUAL
PCAP Spirometry Manual Version: December 2011 Page 1 of 1
Introduction/Background
The Primary Care Asthma Program (PCAP) is an evidence-based asthma program
intended to provide primary care providers with decision aids to support best practice
regarding asthma assessment, diagnosis and management. Its development,
implementation and evaluation as a pilot project were funded through the Ontario
Ministry of Health and Long-Term Care, as one of the initiatives of the Asthma Plan of
Action. The pilot for this program was evaluated in 8 primary care sites from 2002-2006.
Currently, the Primary Care Asthma Program is delivered within a multi disciplinary
team of primary care providers with the support of a Certified Asthma/Respiratory
Educator. The Certified Asthma/Respiratory Educator assists with program
implementation, mentoring, education of patients and staff and ensuring the ongoing
sustainability of the program. The program is modeled on fostering patient and family
self-management.
Key to the success of this primary care program is the expertise of the educator who
provides current evidence-based knowledge and assist with on-site objective
measurements via spirometry. Spirometry, in accordance with American Thoracic
Society/European Respiratory Society (ATS/ERS) 2005 Standards, will be used as the
primary objective measure for the confirmation of the diagnosis of asthma and as the
objective measure for the monitoring of asthma clients for all clients capable of
performing this test.
This Spirometry Manual was developed by the PCAP Spirometry Working group for
health care providers in the primary care setting. The purpose of the manual is to
promote quality spirometry in primary care with a strong focus on technical skills set.

Section 2 PCAP Policy & Procedures
2

Primary Care Asthma Program SPIROMETRY MANUAL
Page 1
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
2.1 Primary Care Asthma Program (PCAP) Spirometry Policy and Procedures
Purpose: To assist “PCAP” primary care providers with policies and procedures for performing spirometry testing in accordance with current American Thoracic Society/European Respiratory Society (ATS/ERS) Standardization of Lung Function Testing (1) as well as the Canadian Thoracic Society (CTS) guidelines for Spirometry in Primary Care (2).
Policy: Spirometry is a non-invasive, diagnostic test that measures ventilatory capacity as a function of time, reflecting the flow resistive properties of the airways. Spirometry, pre- and post-bronchodilator, in accordance with ATS/ERS standards, will be used as the primary objective measure for clients who are able to perform the test for the confirmation of the diagnosis of asthma and as an objective measure of lung function for the monitoring of asthma clients. Refer to PCAP Generic Program Standards (GPS) # 5. (3)
Procedure: Instrumentation, calibration, hygiene, infection control, performance of the test to meet criteria for acceptability and repeatability, reporting results for interpretation, and spirometry training recommendations are essential elements of performing spirometry that can have a significant impact on the quality of the test and the interpretation of the results.
2.1.1 Instrumentation
Spirometer equipment recommendations apply to all spirometers and are minimal requirements.
Instrumentation recommendations should be followed to provide accurate spirometric data and
information that is comparable from laboratory to laboratory and from one time period to another. The
accuracy of a spirometry system depends on the characteristics of the entire system, from the volume
or flow transducer and the use of an in-line filter, to the recorder, display or processor. Changes in any
aspect of the equipment or errors at any step in the process can affect the accuracy of the results. All
spirometry should be reported at BTPS (Body Temperature and Pressure Saturated) by any method
(measuring temperature and barometric pressure). When a subject performs an FVC maneuver into a
spirometer, the air leaving the lungs is approximately 33ºC-35ºC and saturated with water vapour. If the
expired gas is assumed to be at BTPS, an error of ~1% will occur. Most volume-type spirometers
assume instant cooling of the gas but this is not always the case. If the flow sensor is located further
from the mouth, such as adding an in-line filter, more cooling will occur allowing for more errors. For
example, if the BTPS correction factor is wrong, an accurately measured FVC will be incorrectly
reported (1).
Flow-Sensing Spirometers – currently the most widely used instruments
Utilizes a sensor that measures flow as the primary signal and calculates volume by
electronic (analog) or numerical (digital) integration of the flow signal producing a FLOW-

Primary Care Asthma Program SPIROMETRY MANUAL
Page 2
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
VOLUME curve
Most commonly used flow sensors detect and measure flow from: the pressure drop across a
resistance (pneumotach); cooling of a heated wire; or by electronically counting the rotation
of a turbine blade
General Considerations (2):
All spirometers must meet the latest ATS/ERS standards (Please refer to section 3.0 of this
manual: ATS/ERS Standardization of Spirometry)
Exhalation-only spirometers are not recommended (e.g. Spirometers where the patient
inhales to maximal lung volume, then while holding their breath, places mouth on mouthpiece
and does a forced exhalation into the spirometer). This is because it requires more
coordination from the patient and can cause inaccurate measurement due to leakage that
occurs between the time when the patient reaches maximal lung volume and when the
patient places their mouth on the mouthpiece. It is recommended that the spirometer chosen
allows the patient to take tidal breaths with their mouth on the mouthpiece prior to the FVC
maneuver. This allows for the person conducting the test to evaluate a proper seal around
the mouthpiece and the nose clip is functioning properly. Any leakage that occurs at maximal
lung volume will be captured and will be used to determine whether the test meets ATS/ERS
standards.
Display (2):
The Display must show both the flow-volume loop and the volume-time curve with sufficient
resolution so that the person conducting the testing can determine whether test results have
met the ATS/ERS standards (see page 6 of this Policy and Procedure)
It should be possible for the person conducting the spirometry testing be able to observe both
the display and the patient effort allowing for instant coaching and for the person conducting
the spirometry testing to terminate the test early if the test is unacceptable
The spirometer should be able to analyze each maneuver to determine whether each effort
meets ATS/ERS standards (acceptability and repeatability) and provide “warning messages”
to indicate if the maneuver was not acceptable (e.g. “end of test criteria not met – blow out
longer”) Note: Most of the ATS/ERS standards are based on the adult population and many
children can meet requirements with submaximal efforts and poor quality tests. This should
be recognized by the person conducting the spirometry testing and an effort will be repeated
even if the computerized system has accepted the test. Information about special
considerations in children are available at the end of this document.
2.1.2 Calibration
Attention to equipment quality control and calibration is an important part of good laboratory practice, necessary for valid reliable results. At a minimum, the requirements are as follows: (Refer to Appendix 1: PCAP Spirometry Operator Checklist)
Primary Care Asthma Program SPIROMETRY MANUAL
Page 3
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
A Spirometer should have a Calibrating syringe. ATS/ERS standards specify that a 3L
syringe be used for checking and calibrating a spirometer daily.
A simple leak test (to test if there is a leak in the calibration syringe) using a stopper in the
calibration syringe should be done monthly by pushing or pulling the syringe (2)
Spirometers using pre-calibrated inserts must still be checked daily for accuracy using a 3L
calibration syringe. (2)
Daily calibration log should be maintained for all equipment requiring calibration; Room temperature, Barometric Pressure and Relative Humidity should be measured, not
estimated. If a barometer is unavailable, pressure reported from a nearby weather station can be accessed from the Environment Canada website: http://weather.gc.ca/canada_e.html and must be corrected for altitude: http://www.engineeringtoolbox.com/air-altitude-pressure-d_462.html (3)
Calibration should be conducted with mouthpiece/filter in-line with the calibration syringe;
Monthly normal biological tests (e.g. perform spirometry on a staff member (with no
underlying lung condition) on all spirometers in the clinic on a monthly basis for comparison (must be within 150mL of each other)
Documentation of repairs or other alterations which return the equipment to acceptable
operation; & preventative maintenance, corrective actions;
Dates of computer software and hardware updates or changes; and
If equipment is changed or relocated (e.g. industrial surveys), calibration checks and quality-control procedures must be repeated before further testing begins.
Follow manufacturer’s manual for complete calibration procedures. While manufacturers are responsible for demonstrating the accuracy and reliability of the systems that they sell, it is the user who is responsible for ensuring that the equipment’s measurements remain accurate (1).
2.1.3 Hygiene and Infection Control
Each site is responsible to follow their site specific infection control policy. Each site will establish specific responsibilities and guidelines related to Spirometry for their site safety and the prevention of infectious disease transmission (Refer: Provincial Infectious Diseases Advisory Committee, Infection Prevention and Control for Clinical Office Practice, 2013(8)). The goal of infection control is to prevent the transmission of infection to patients and staff during spirometry testing. The number of documented cases of infection transmission is very small, but the potential is real. Assume all patients have the potential of acquiring and transmitting infectious disease so implementation of the nationally recognized program of Universal/Routine Standard Precautions should be followed:
Effective hand washing before and after direct patient contact or contact with body
substances.
For infection control purposes, disposable filters are strongly recommended unless the
circuitry is changed after each patient or a non-rebreathing technique is used. Some
spirometers may incorporate a disposable breathing tube, making a filter unnecessary (2)
Gloves for contact with blood, secretions, mucous membranes, non-intact skin and moist
body substances.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 4
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
Additional barriers - gowns, masks, protective eyewear and plastic aprons when body
substances are likely to soil clothing, skin or mucous membranes (10).
2.1.4 Performing the Spirometry Test Who Can Conduct Spirometry?
By a trained and qualified personnel in a setting with a regular quality assurance program
(e.g. Trained health care professionals who are Registered Respiratory Therapist (RRT) or
Registered Cardio-pulmonary Technologist, RCPT(P) or other regulated health care
professionals who received formal training which included studies in anatomy and physiology
of the cardiorespiratory system and who successfully completed a recognized spirometry
training course, and other trained health care technologists who successfully completed a
recognized spirometry training course (please refer to section 2.1.8 of this document for
training programs) (2).
Reference Values: Performing the test not only includes attention to the instrumentation, calibration and infection control but also to how the test is performed and attention to the quality of the measurements produced. All measurements are expressed as litres (L) or litres/second (L/s) and as % predicted, with the predicted values being derived from standardized data sets. Predicted values should reflect the patient population of your clinic. The current CTS guidelines recommend the use of Lower Limit of Normal (LLN). The Lower Limit of Normal (LLN) is defined as the 5th percentile (i.e. the value that marks the lower 5th percentile of the normal population). The 5th percentile is considered the threshold below which a value is considered to be abnormal. The Global Lung Function Initiative (GLI) recommends the all-age spirometry values developed by Quanjer et al. be used as reference values (age 3.5 - 90yrs). Most major spirometer have committed to implementing the Quanjer et al. reference values (www.lungfunction.org/93-manufacturers.html). Another choice of reference equations is the National Health and Nutrition Examination Survey (NHANES III) for Caucasian, African-American and Hispanics between 8-80 years of age. These equations should not be used outside this age range. This set is contained in almost all current spirometry systems. There are no reference equations for the Canadian Aboriginal population and therefore, spirometry tests involving this population should be interpreted with caution using the Caucasian reference values (2). More recently, the Canadian Health Measurement Survey (CHMS) provides reference values for the Canadian Caucasian population from 6 to 79 years of age and guidelines to approximate correction for other ethnic groups (12). Clinics may want to align with labs in their geographical region using the same reference sets understanding that if different reference sets are used only the patient’s absolute values can be compared between tests. Predicted values take into account height, age, gender, ethnic origin. Weight is normally recorded for monitoring but is not in the equation for predicted spirometry values. The height should not be estimated but measured using a measuring tape (attached to the wall) with the patient standing without shoes with his/her back flat against the wall with a right angle device making contact with the top of the head and the measuring tape. When height cannot be measured using this method (e.g. chest wall deformities) arm span (middle finger tip to middle finger tip) can be used as an approximate (2).

Primary Care Asthma Program SPIROMETRY MANUAL
Page 5
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
The spirometer selected must have specific sets of normal reference values, both adult and
pediatric, pre-programmed into its software. If it does not, insist that they be installed prior to
purchase (2)
Reference values must be appropriate for the age and ethnicity of the population and be able
to provide the Lower Limit of Normal (LLN) (2). It is recommended that you inquire about a
software update to obtain the LLN with your spirometer equipment if not already available.
The interpretation of spirometry tests should be based on the LLN (2)
Table 1: Terminology and Definitions
Measurement Abbreviation Definition
Forced Vital Capacity (L) FVC Maximum volume of air that can be expired as
forcefully, quickly and completely as possible following a complete inspiration
Forced Expiratory Volume in FEV1 Volume of air expired in the first second of the FVC - Used to assess airflow
1 second (L/sec)
Ratio of FEV1 to FVC % FEV1/FVC Used for the assessment of airflow obstruction
Peak Expiratory Flow (L/sec) PEF The maximum flow rate at the onset of the FVC maneuver – judges max effort
Forced Expiratory Flow 25- FEF 25-75 The average flow rate during the middle half of 75% (L/Sec) the FVC maneuver – reflects airflow
*FEF50/FIF50 = The ratio of flow at 50% of expiration and flow at 50% inspiration (Maximum flow at 50% that
can be inspired as forcefully, quickly and completely as possible following a complete exhalation). Recognizing
that the inspiratory loop is not always done in primary care, this loop might be useful in evaluating any upper
airway obstruction (UAO). FEF50/FIF50 = 1 in fixed UAO, FEF50/FIF50 > 1 in variable extrathoracic UAO and
FEF50/FIF50 < 0.3 in variable intrathoracic UAO (13).

Primary Care Asthma Program SPIROMETRY MANUAL
Page 6
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
There are two types of graphs that are commonly displayed for Spirometry: the Flow Volume loop and the Volume Time curve. Your spirometer may be formatted to print out both curves.
Figure 1: Flow Volume loop - This is a record of how fast the air flows in/out (Flow) versus the amount (Volume) of air exhaled or inhaled within a certain time (8).
Flow (Y) versus Volume (X)
Figure 2: Volume time curve - This is a record of the expired volume in relation to time (8).
Volume (Y) versus Time (X)
FIF 50

Primary Care Asthma Program SPIROMETRY MANUAL
Page 7
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
Test Procedures for the Spirometry / Flow Volume loop maneuver
The Provider should demonstrate the appropriate technique and follow the procedure described in Table 2 from the ATS/ERS: Standardization of Spirometry 2005. Table 2: Test Procedures for the Forced Vital Capacity maneuver (Flow-Volume loop) Preparation
Ensure the spirometer has daily calibration performed Contraindications should be listed on the spirometry order requisition form or checklist form (2) Additional Patient Preparation/ Documentation (review contraindication as in Appendix 1-
Operator’s Checklist) Ask the patient about:
Smoking Recent illness Inhaler/ medication use
Activities that should preferably be avoided prior to lung function testing Smoking within at least 1 h of testing Consuming alcohol within 4 h of testing Performing vigorous exercise within 30 min of testing Wearing clothing that substantially restricts full chest and abdominal expansion Eating a large meal within 2 h of testing Inhaler Medication (Refer to Medication Section: Post Bronchodilator Testing to withhold prior to
spirometry testing) Measure weight and height without shoes
Wash hands
Instruct and demonstrate the test to the subject Test Performance Perform maneuver (closed circuit method- most commonly used)
Have subject assume the correct seated posture (a chair without wheels, feet flat on the ground) Attach nose clip*, place mouthpiece in mouth and close lips around the mouthpiece, perform 2-4 tidal
breaths Inhale completely and rapidly with a pause of 1 s at TLC Exhale forcefully and rapidly until no more air can be expelled while maintaining upright posture
(minimum 6 sec for adults and 3 sec for children ≤ 10 years of age) Please refer to the Appendix: “Special Considerations in Young Children”
Assess the performance and acceptability of each flow volume loop, provide any instructions to ensure
test is performed properly and repeat the test until you have obtained quality curves ( as per ATS/ERS
Standards- 3 minimum and 8 maximum curves
*Recommendation is to use Nose Clips or manual occlusion of the nares, to avoid leaks, especially for
nose breathers. People must mouth breathe during the procedure
Primary Care Asthma Program SPIROMETRY MANUAL
Page 8
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
Post Bronchodilator Spirometry/Flow-volume loop
(Please refer to ATS/ERS: Standardization for Spirometry 2005, Reversibility Testing)
Spirometry testing and the administration of bronchodilators, requires a signed requisition from the Physician or a verbal or standing order as per site specific Medical Directives and provincial regulations that should indicate whether post bronchodilator testing is requested, and which bronchodilator is to be administered for the testing and how much bronchodilator should be given for testing
Medication to withhold prior to spirometry testing
The decision to avoid bronchodilators before testing is dependent on the reason for the test. If post bronchodilator testing is to be performed to diagnose an underlying lung condition, the patient may/should withhold the following medication prior to spirometry testing: Note: It is important to tell the patient that if they need to use their rescue inhaler for symptoms, they can do so and not withhold it for the test. Inhaled bronchodilators (7) Medication Withholding time prior to Spirometry
Testing Short-Acting Beta2 Agonist (SABA) 4 - 8 Hours Short-Acting Muscarinic Antagonist (SAMA) 6 Hours Long-Acting Beta2 Agonist (LABA) 24 hours Long-Acting Muscarinic Antagonist (LAMA) 24 Hours
Other medications to withhold: Theophylline: 48 hours (7), LTRA 24 hours (2)
Antihistamines and steroids (oral and inhaled) do not need to be withheld Note: if the test is to determine the response to a medication, then the referring physician may choose not to withhold the medication prior to testing. The spirometry requisition order form should indicate whether to withhold a medication before testing and specify which medication to withhold To standardize the evaluation of spirometry post-bronchodilator: Short Acting Beta Adrenergic (SABA) medications are the most commonly used bronchodilator,
other drugs can be used (e.g. Short-Acting Muscarinic Antagonist (SAMA) such as Ipratropium Bromide)
After the pre-bronchodilator test, administer SABA – 4 separate doses* of 100mcg each, Total of 400 mcg salbutamol, or 4 separate doses* of 40mcg each, Total of 160mcg of Ipratropium Bromide
*Inhale separate doses from a valved holding chamber device 30 seconds apart (7) ATS does not currently specify any recommendations for the pediatric population. Perform post-bronchodilator testing 15 minutes post for SABA and 30 minutes post for SAMA

Primary Care Asthma Program SPIROMETRY MANUAL
Page 9
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
2.1.5 Acceptability and Repeatability Test Criteria
Acceptability
A minimum of three (3) acceptable maneuvers must be obtained. Evidence for an acceptable test includes: Adequate understanding and performance of test procedure Unhesitating start without a variable effort Maximum effort with smooth continuous exhalation. Absence of cough, glottis closure, early termination or leakage For complete recommendations please review - ATS/ERS Standardization of Lung Function Testing: Standardization of Spirometry 2005 Repeatability
The FVC of the two largest accepted curves is within 150ml of each other. The FEV1 of the two largest accepted curves is within 150ml of each other.
Figure 3: Flow chart on application of Acceptability & Repeatability criteria.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 10
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
2.1.6 Reporting Results (3)
When considering a spirometer, consider whether it is compatible with your Electronic
Medical Record (EMR)
Flow and volume measures are reported at body temperature and pressure saturated with water vapor (BTPS)
The largest FVC and FEV1 from acceptable maneuvers is reported, even though the values may not come from the same maneuver
Largest PEF is reported All other flows i.e. FEF25-75% are reported from the “best curve” (defined as the maneuver
with the largest sum of FVC and FEV1) Final reports should include the technologist’s comments regarding the patient performance,
recent use of bronchodilators, quality of testing and whether or not the results were acceptable and reproducible (e.g. Patient had good effort, results reproducible, unable to perform reproducible curves, unable to attain residual volume, etc.)
Note: Please refer to Appendix A in this spirometry manual for what a sample report (2) should look like.
Who Can Interpret Spirometry?
Primary Care physicians and Nurse Practitioners who interpret spirometry should have completed a spirometry interpretation course or specific training in spirometry interpretation (2). Please refer to Page 11 of this policy and procedure for recommended courses.
2.1.7 Technical Support (2):
A spirometer must be sufficiently robust to be unaffected by drops or bumps. If a spirometer
is dropped, a calibration check is recommended before continuing testing
Ensure the vendor who provided you with the spirometer provide sufficient training initially in
the use of a spirometer. They should also be able to provide technical support for addressing
problems with the operation of the spirometer. If your spirometer needs to be checked,
request a loaner device. There should be regular notification of any software upgrades and
the spirometer should be thoroughly checked on a regular basis for any upgrades.
2.1.8 Training Recommendations for Performing Spirometry
Purpose: This policy will provide guidelines on the minimum criteria and core components of training based on the ATS/ERS/CPSO guidelines for personnel with regards to performing spirometry.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 11
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
Policy: The following minimum criteria are recommended by ATS/ERS to establish competency in spirometry testing:
Knowledge of theory and practical aspect of applied techniques, measurements, calibrations, hygiene, quality control, basic background in lung physiology and pathology;
Introduction to the standards of spirometry, review of spirometry role in the diagnosis, management of asthma and assess contraindications;
Test performance: Proper technique for performing spirometry including how to coach for
best results (practical workshop or hands on training);
Discuss predicted values and actual/absolute values;
Review reporting process.
Spirometry training can be attained through an accredited Institution. Recommended institutions: Certification in conducting spirometry:
“SpiroTrec” (Lung Association of Saskatchewan National program: http://www.resptrec.org/)
Additional Supports: The Lung Association Provider Education Program (PEP). Spirometry Interpretation
workshop and e-modules http://olapep.ca/
Job shadowing with a local/regional expert can enhance practical training objectives. This can be available but limited according to resources. Please contact PCAP Provincial Coordinator for more information (http://www.lungontario.ca/PCAP)
*Please Note: Permission and proper acknowledgement is required in any modification of the PCAP tools as per the PCAP process

Primary Care Asthma Program SPIROMETRY MANUAL
Page 12
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
APPENDIX 1: PCAP SPIROMETRY OPERATOR CHECKLIST (Page 1)
Barometric Pressure, Relative Humidity and Temperature updated daily
Daily calibration performed according to manufacturer’s and ATS/ERS Standards
Relative Contraindications (Refer to the list on the reverse side of this page)
Minimum of three acceptable FVC performed, with two repeatable maneuvers, maximum eight performed (ATS/ERS 2005)
Assess Patient Performance: (Acceptability)
o Maximum peak effort o No hesitation or cough within first second of exhalation o Extrapolated volume < 150 ml or 5% of FVC o No glottis closure, cough or early termination of effort o No leak observed or obstruction of mouthpiece o Six seconds of exhalation collected (3 sec for <10 yrs)
Assess Measurements: (Repeatability)
o Are the 2 largest FVCs within 150 ml of each
other?
o If FVC < 1.0 L then criteria is within 100ml of
each other
o Are the 2 largest FEV1s within 150 ml of each
other?
o If FVC < 1.0 L then criteria is within 100ml of
each other
Technical comments recorded on spirometry report
Primary Care Asthma Program SPIROMETRY MANUAL
Page 13
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
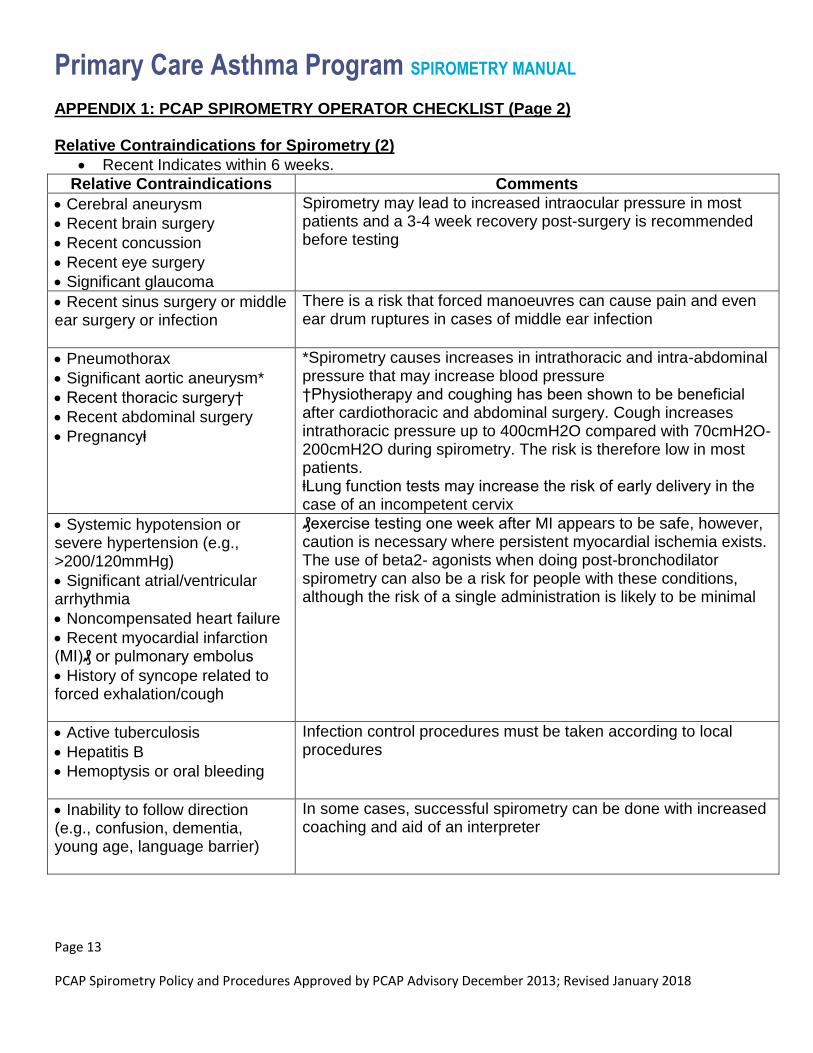
APPENDIX 1: PCAP SPIROMETRY OPERATOR CHECKLIST (Page 2)
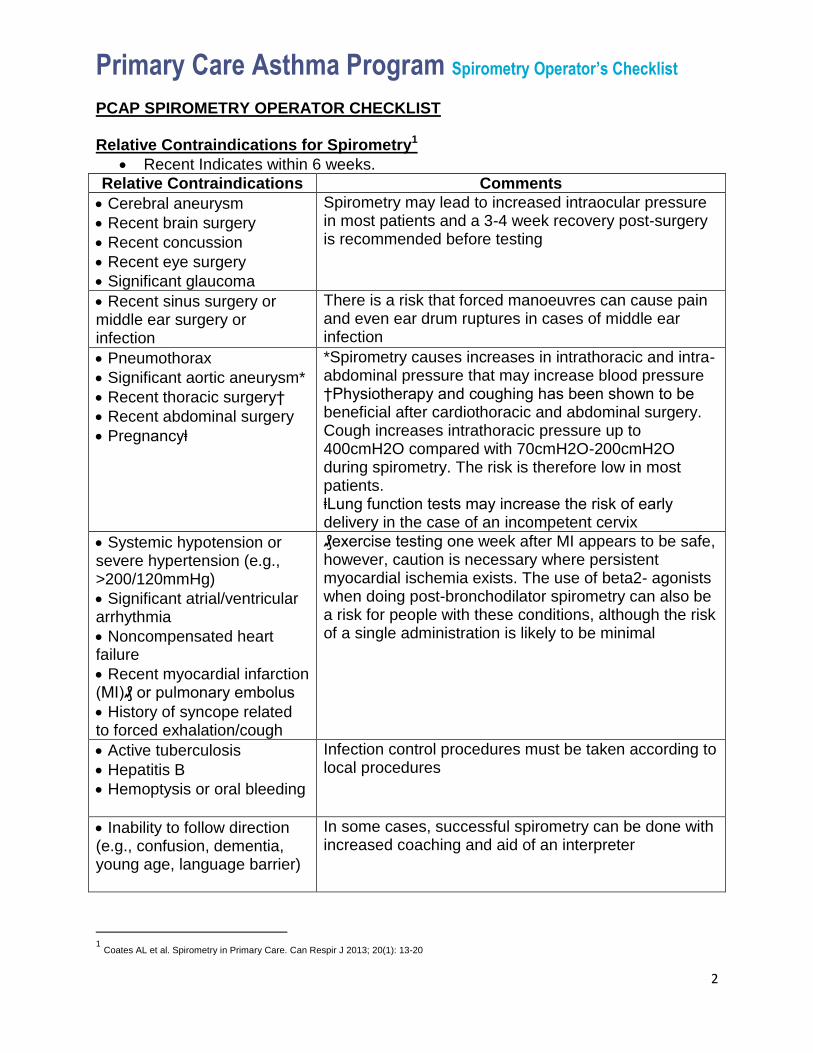
Relative Contraindications for Spirometry (2)
Recent Indicates within 6 weeks.
Relative Contraindications Comments
Cerebral aneurysm
Recent brain surgery
Recent concussion
Recent eye surgery
Significant glaucoma
Spirometry may lead to increased intraocular pressure in most patients and a 3-4 week recovery post-surgery is recommended before testing
Recent sinus surgery or middle ear surgery or infection
There is a risk that forced manoeuvres can cause pain and even ear drum ruptures in cases of middle ear infection
Pneumothorax
Significant aortic aneurysm*
Recent thoracic surgery†
Recent abdominal surgery
Pregnancyⱡ
*Spirometry causes increases in intrathoracic and intra-abdominal pressure that may increase blood pressure †Physiotherapy and coughing has been shown to be beneficial after cardiothoracic and abdominal surgery. Cough increases intrathoracic pressure up to 400cmH2O compared with 70cmH2O-200cmH2O during spirometry. The risk is therefore low in most patients. ⱡLung function tests may increase the risk of early delivery in the case of an incompetent cervix
Systemic hypotension or severe hypertension (e.g., >200/120mmHg)
Significant atrial/ventricular arrhythmia
Noncompensated heart failure
Recent myocardial infarction (MI)₰ or pulmonary embolus
History of syncope related to forced exhalation/cough
₰exercise testing one week after MI appears to be safe, however, caution is necessary where persistent myocardial ischemia exists. The use of beta2- agonists when doing post-bronchodilator spirometry can also be a risk for people with these conditions, although the risk of a single administration is likely to be minimal
Active tuberculosis
Hepatitis B
Hemoptysis or oral bleeding
Infection control procedures must be taken according to local procedures
Inability to follow direction (e.g., confusion, dementia, young age, language barrier)
In some cases, successful spirometry can be done with increased coaching and aid of an interpreter

Primary Care Asthma Program SPIROMETRY MANUAL
Page 14
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
APPENDIX 2: Special Considerations in Young Children (2)
Children have higher elastic recoil of the lungs than adults and therefore, have faster emptying
of the lungs (some children are able to exhale completely in 1 sec).
Minimum expiratory time is 3 sec for children ≤ 10 years of age rather than 6 sec for adults.
However, the requirement of a plateau < 25mL in the final 1 sec of exhalation remains
(ATS/ERS standards 2005)
If the child can exhale their lung volume in < 2 sec, the technologist must override the automatic
rejection of the test.
ATS/ERS repeatability is 150mL between tests for FEV1 and FVC or 100mL for FVC or FEV1 <
1L
The back-extrapolated volume used for the beginning of the test must be ≤ 150mL or 5% of
FVC, whichever is greater.
When a child performs spirometry testing, they must rapidly inspire to maximal lung volume and
prevent breathholding prior to forced exhalation (ATS/ERS 2005)
Ensure an appropriately sized mouthpiece for a better seal
Ensure the use of nose clips
Primary Care Asthma Program SPIROMETRY MANUAL
Page 15
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
APPENDIX 3: Quality Assurance Considerations (2)
Documentation of Quality Assurance components includes:
Daily Calibration of the spirometer with a 3L calibration syringe and a monthly assessment of
repeatability of the measures using biological controls and an evaluation of a log of calibration
results
Documentation of repairs/modifications/software upgrades to the spirometry equipment
Qualification of all personnel conducting spirometry testing, including education and training.
Documented infection control procedures
Please note:
Permission & Proper acknowledgement is required in any modification of the PCAP Tools as per PCAP process.

Primary Care Asthma Program SPIROMETRY MANUAL
Page 16
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
References
1. American Thoracic Society /European Respiratory Society Task Force: Standardization of Lung
Function Testing: Standardization of Spirometry. Eur Respir J 2005;26: 319-338 http://www.thoracic.org/statements/
2. Coates AL et al. Spirometry in Primary Care. Can Respir J 2013; 20(1): 13-20.
3. Primary Care Asthma Program, Generic Program Standards, PCAP Group, June 2013
4. American Thoracic Society /European Respiratory Society Task Force: Standardization of Lung
Function Testing: General considerations for lung function testing. Eur Respir J 2005;26: 153-161 http://www.thoracic.org/statements/
5. American Thoracic Society/ European Respiratory Society Task Force: Standardization of Lung
Function Testing: Interpretative strategies for lung function tests. Eur Respir J 2005; 26: 948-968 http://www.thoracic.org/statements/
6. American Association for Respiratory Care- AARC Clinical Practice Guideline, Spirometry, 1996
Update, Respir Care 1996; 41(7):629–636 http://www.rcjournal.com/cpgs/spirupdatecpg.html
7. College of Physicians and Surgeons of Ontario (CPSO) Independent Health Facilities (IHF)-
Clinical Practice Parameters and Facility Standards for Diagnostic Spirometry & Flow Volume Loop Studies – 4th edition http://www.cpso.on.ca/CPSO/media/documents/CPGs/IHF/Pulmonary-Function-Studies.pdf
8. The Provincial Infection Diseases Advisory Committee, Infection Prevention and Control for
Clinical Office Practice, June 2013; Revised April 2015 (116 pages) http://www.publichealthontario.ca/en/eRepository/IPAC_Clinical_Office_Practice_2013.pdf
9. Ruppel, G. Manual of Pulmonary Function Testing. Seventh Edition. St. Louis, MO, the C.V.
Mosby Company, 1997.
10. NIOSH, Spirometry Training Guide 2003 http://www.cdc.gov/niosh/docs/2004-154c/
11. Coates, A.L. Wong, S.L., Tremblay, C., Hankinson, J.L. Reference Equations for Spirometry in
the Canadian Population. Ann Am Thorac Soc 2016 Vol 13, No 6 pp 833-841
12. Hankinson, J.L. Odencrantz, J.R. Spirometric Reference Values from a Sample of the General U.S. population, American Journal of Respiratory and Critical Care Medicine 1999 Vol 159 p179-

Primary Care Asthma Program SPIROMETRY MANUAL
Page 17
PCAP Spirometry Policy and Procedures Approved by PCAP Advisory December 2013; Revised January 2018
187 http://www.ndd.ch/UserData/Download_00141_00.pdf
13. Karkhanis VS, Joshi JM. Spirometry in Chronic Obstructive Lung Disease (COPD). Supplement to JAPI 2012; 60: 22-26

Page 1 of 2 PCAP Medical Directive on Ordering Spirometry (Sample)
2009 June; rev Jan 2018
[NAME OF PRIMARY CARE SITE]
Medical Directive: Ordering Spirometry
Approval Date: __________________
Review Date: ____________________
Approved by: ____________ Family Physician (Lead)
____________ Executive Director
Background Information
The Primary Care Asthma Program (PCAP) is an evidence-based asthma
program intended to provide primary care providers with decision aids to
support best practice regarding asthma assessment, diagnosis and
management. Its development, implementation and evaluation as a pilot
project were funded through the Ontario Ministry of Health and Long-Term
Care, as one of the initiatives of the Asthma Plan of Action. The pilot for
this program was evaluated in 8 primary care sites from 2002-2006.
CONDITIONS OF DELEGATING SPIROMETRY BY MEDICAL
DIRECTIVE
The practitioner follows the ________ [ORGANIZATION ] procedure for
performing spirometry, which follows the American Thoracic Society/
European Respiratory Society (ATS/ERS) standards for spirometry.
All staff ordering spirometry is aware of the __________
[ORGANIZATION ] policies and procedures for performing spirometry.
The practitioner is aware of the risks of ordering/performing spirometry
including all contraindications within the primary care site setting.
All new staff (RRTs, RNs, RN (EC)s, and MDs) are made aware of the
policies and procedures concerning spirometry testing.
I authorize the ___ [ORGANIZATION NAME ] RRTs, RNs, RN (EC)s and
to order spirometry testing according to the _______________________

Page 2 of 2 PCAP Medical Directive on Ordering Spirometry (Sample)
2009 June; rev Jan 2018
[ORGANIZATION ] policy and procedure when all conditions of this
directive are met.
Approved by (Medical Director of Organization):
Signature followed by Printed Name
Date
Page 1 of 2 PCAP Medical Directive on Spirometry Salbutamol Administration (Sample)
2009 June; rev Jan 2018
[NAME OF PRIMARY CARE SITE] Medical Directive: Administration of Salbutamol for Spirometry Testing
Approval Date: __________________
Review Date: ____________________
Approved by: ____________ Family Physician
____________ Executive Director
Background Information
The Primary Care Asthma Program (PCAP) is an evidence-based
asthma program intended to provide primary care providers with decision
aids to support best practice regarding asthma assessment, diagnosis and
management. Its development, implementation and evaluation as a pilot
project were funded through the Ontario Ministry of Health and Long-Term
Care, as one of the initiatives of the Asthma Plan of Action. The pilot for
this program was evaluated in 8 primary care sites from 2002-2006.
CONDITIONS OF DELEGATING THE ADMINISTRATION OF
SALBUTAMOL WHEN PERFORMING SPIROMETRY
The practitioner follows the ____________________ [ORGANIZATION ]
procedure for administering salbutamol (which is a beta 2 adrenergic
medication).
This drug is only to be administered by the above-mentioned health care
professionals when being used during a post bronchodilator spirometry test.
The practitioner is aware of the risks of administering salbutamol via
Metered Dose Inhaler (MDI) and holding chamber (spacer with a valve) for
spirometry testing within the community setting.
All new staff (RRTs, RNs, RN (EC)s and MDs) are made aware of policy
and procedures concerning the administration of salbutamol MDI for the
purpose of performing spirometry.

Page 2 of 2 PCAP Medical Directive on Spirometry Salbutamol Administration (Sample)
2009 June; rev Jan 2018
The physician(s) indicated below approves the act of delegating the
administering of salbutamol to be used in post bronchodilator spirometry
testing.
I authorize _______________[ORGANIZATION NAME ] RRTs, RNs, RN
(EC)s to administer salbutamol via MDI and valved holding chamber, for
post bronchodilator spirometry testing. This is to be done according to the
______________ policy and procedure when all conditions of this directive
are met.
APPROVED BY (Medical Director of Organization):
Signature followed by Printed Name
Date

Page 1 of 4 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
2013 June; rev Jan 2018
[NAME OF PRIMARY CARE SITE]
Medical Directive: Spirometry Pre & Post Bronchodilator
Approval Date: __________________
Review Date: ____________________
Approved by: ____________ Family Physician
____________ Executive Director
Background Information
The Primary Care Asthma Program (PCAP) is an evidence-based
asthma program intended to provide primary care providers with decision
aids to support best practice regarding asthma assessment, diagnosis and
management. Its development, implementation and evaluation as a pilot
project were funded through the Ontario Ministry of Health and Long-Term
Care, as one of the initiatives of the Asthma Plan of Action. The pilot for
this program was evaluated in 8 primary care sites from 2002-2006.
Setting where medical directive to be Implemented:
In house spirometry testing at ________ [ORGANIZATION NAME]
Note: not to be used for referral for external spirometry testing (since an
external lab cannot bill for a spirometry test ordered by an RN (EC) or a
Registered Respiratory Therapist [RRT])
Professional Staff covered by the Directive: Authorized staff that have
been observed and trained to perform spirometry according to American
Thoracic Society/European Respiratory Society (ATS/ERS) guidelines
under ____________ [ORGANIZATION NAME] quality assurance and
quality control policies for spirometry testing and that the undersigned
presently holds the designation and college certification in good standing as
within their respective regulated health colleges.
CONDITIONS OF DELEGATING SPIROMETRY BY MEDICAL
DIRECTIVE
The practitioner is aware of and follows the _________ [ORGANIZATION
NAME] procedure for performing spirometry, and administering salbutamol
that follows the ATS/ERS standards for pre/post bronchodilator testing.
Page 2 of 4 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
2013 June; rev Jan 2018
The practitioner is aware of the following risks of ordering/performing
spirometry including pre and post bronchodilator within the primary care
setting in the 2013 CTS guidelines for spirometry in primary care (1):
Relative Contraindications for spirometry:
Cerebral Aneurysm
Recent brain surgery (Most experts suggest a 3-6 week recovery
period following surgery before spirometry testing)
Recent concussion
Recent eye surgery
Significant glaucoma
Recent sinus surgery or middle ear surgery or infection
Pneumothorax
Significant aortic aneurysm (Increases in intrathoracic or intra-
abdominal pressures may increase blood pressure)
Recent thoracic surgery (Postoperative physiotherapy including
coughing is actually believed to be beneficial after cardiothoracic and
abdominal surgery. Cough generally increases intrathoracic pressures
up to 400cmH2O, compared with 70cmH2O-200cmH2O during
spirometry. The risk is likely low in most patients)
Recent abdominal surgery
Pregnancy (Lung function tests may increase the risk of early delivery
in case of cervical incompetence)
Systemic hypotension or severe hypertension (eg, >200/120mmHg)
Significant atrial/ventricular arrhythmia
Non-compensated heart failure
Recent myocardial infection or pulmonary embolus (Exercise testing
one week after myocardial infarction appears to be safe. A shorter
period could be appropriate following reperfusion therapy (eg,
angioplasty), whereas caution is necessary in case of persistent
myocardial ischemia
Active tuberculosis
Hepatitis B
Hemoptysis or oral bleeding
Inability to follow directions (eg, confusion, dementia, young age,
language barrier)
Clinical Criteria:
1. The client must be recognized as an existing client of the
[ORGANIZATION NAME] with either a diagnosis of asthma indicated in

Page 3 of 4 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
2013 June; rev Jan 2018
their chart or an order by a physician for a pre/post spirometry testing
to establish the diagnosis.
2. A physician or RN (EC) must be on site during the conducting of a
spirometry test in the effect of a medical emergency arising from the
test.
3. Informed verbal consent for the test is obtained from the client or the
legal guardian.
4. A list of medication to be put on hold prior to testing is provided to
patient.
5. Note contraindication for testing.
Process:
1. Review chart to confirm spirometry order
2. Assess the client’s ability to perform spirometry considering age and
comorbidities.
3. Obtain and document informed verbal consent.
4. Review contraindications
5. Write an order for pre-post spirometry testing
6. Complete the test correctly as per the instructions in the spirometry
and salbutamol administration procedure.
7. Make copies of the results with written comments included. Results
should be interpreted by the physician and then signed off by a
physician and/or RN (EC) before being added to the clients chart in
the asthma documentation section.
Signatures:
The physician(s) indicated below approves the act of delegating the ordering
and performing of pre/post spirometry testing to be used with asthma clients
at our center.
I authorize __________ [ORGANIZATION NAME] - RN(EC)s, RNs and
RRTs (see attached list) to order and administer spirometry testing according
to the ___________ [ORGANIZATION NAME] policy and procedure
when all conditions of this directive are met.
Physician authorizing delegation for ___________[ORGANIZATION NAME] :
_______________________________ Date: ____________________
Executive Director:
_______________________________ Date: ____________________

Page 4 of 4 PCAP Medical Directive on Spirometry Pre & Post Bronchodilator (Sample)
2013 June; rev Jan 2018
List of Authorized Staff for the Medical Directive
Ordering and performing pre/post bronchodilator Spirometry Testing
Name Date Certified Review Date_______
References:
1. Coates AL et al. Spirometry in Primary Care. Can Respir J 2013;
20(1): 13-20.

Pre-Bronchodilator Post-Bronchodilator
Spirometry Best LLN %Ref Best %Ref Change %Chg
FVC (L) 4.65 3.86 91% 5.01 94% 360 mL 8%
FEV1 (L) 3.26 2.91 84% 4.04 100% 780 mL 24%
FEV1/FVC 0.70 0.64 0.81
PEF (L/s) 10.2 14.3
FET (s) 15.3 14.8
Test quality B A
Reference values: Quanjer 2012 [Caucasian]
Family Physicians Clinic
123 Main St
Anytown, Prov, Z1Z 1Z1
987-321-6540
Age: 62 yr Male Name: Xxxxxxxx, Xxxx
Ht: 186 cm Race: Caucasian ID#: 333222111
Wt: 84 kg BMI: 24.3 kg/m2 Date of birth: 1949-Dec-31
Nonsmoker - pack-yrs: 0 Date of test: 14:20, 2012-Jan-02
Reason for test: Chronic cough
Interpretation: Pre-bronchodilator spirometry is in the normal range. There is a significant response to
bronchodilators.
Physician: Dr. Blow Hard
FVC
FEV1
FEV1/FVC
LLN reference
o
o
o
FVC
FEV1
FEV1/FVC
LLN reference
Pre-Bronchodilator
Post-Bronchodilator
o
o o
Pre
Post
Pre
Post
Technologist comments:
3 acceptable blows with 2
repeatable for both Pre- and
Post- tests.
No bronchodilators taken in
previous 24 hrs.
std dev
std dev
APPENDIX B: Sample spirometry report form

Reason for Test
Diagnosis ____________________________ Follow up_____________________________
Other _____________________________________________________________________________
Previous Test at this clinic? Yes No Clinical Diagnosis: ________________________________________________________
Smoking History: Current Smoker Former Smoker Never Smoker No. of Pack Years: _______
Spirometry Requested
Pre-bronchodilator Post-bronchodilator (400 mcg salbutamol)
Relative Contraindications:
Recent Surgery within 4 weeks (specify) Aneurysm - Cerebral, thoracic, abdominal
Pregnant (near term) Hemoptysis
Hypertension (uncontrolled) Pneumothorax
Unstable Cardiac Status M.I. within last month
Cross Infection Concerns Other Respiratory Medications: _________________________________________________________________
Appointment Date: Time:
Instructions to provide to the patient: Depending on the reason for doing the test, the patient should be instructed whether or not medications are to be withheld prior to testing, and, if so, precisely which medications should be withheld and for how long. It is important to instruct any patient withholding medications that, if needed for symptom relief, a rescue inhaler should be used and the time of use noted so that it can be reported to the technologist conducting the test.
Withhold medications? Yes No
List medications to withhold:_________________________________________________________________
Short-acting beta agonist 4 hours prior to test Anticholinergic 4 hours prior to test
Long-acting beta agonist 12 hours prior to test Long-acting anticholinergic 24 hours prior to test
The patient should be instructed to avoid the following prior to testing:
Smoking within at least 1 hour of testing
Consuming alcohol within 4 hours of testing
Performing vigorous exercise within 30 min of testing
Wearing clothing that substantially restricts full chest and abdominal expansion
Eating a large meal within 2 h of testing
Requisition for Spirometry
Family Physicians Clinic 123 Main St Anytown, Prov, Z1Z 1Z1
Tel (987) 321-6540 Fax (987) 321-1234
Patient Name: ____________________________ Patient ID# ____________________________ Referring Dr: ____________________________ Dr Signature: ____________________________ Date: ______________ Tel:________________
APPENDIX A: Sample Spirometry Requisition Form
Section 3 Spirometry Practicum
3

Spirometry Interpretation Guide(Consider patient history in all interpretation decision making)
FVC Normal ≥ LLN 4
Consistent with COPD
Consider methacholine
challenge
No
Adapted and revised with permission from Primary Care Respiratory Alliance of Canada (PCRAC)www.olapep.ca
Pre ß2-agonistFEV1 / FVC Ratio
Reduced: < LLN (or <0.70)5
ß2-agonist
FEV1 / FVC Reduced< LLN (or <0.70)5
FEV1 / FVC Normal≥ LLN (or ≥0.70)5
Improved FEV1
12% and 200mL1
Improved FEV1
12% and 200mL1
Consistent with Asthma or COPD or Asthma COPD
Overlap (ACO)
LLN=Lower Limit of Normal
Consistent with Asthma
1. 200mL criteria only necessary for adults (≥ 12 years)
2. Reversibility criteria not met. May occur with chronic asthma - consider methacholine challenge or referral
3. Normal Spirometry: in the context of persistent symptoms consider further clinical testing i.e. methacholine challenge
4. LLN may not be available on outdated systems – use 80% predicted
5. If the LLN is not available use 0.70 in an adult if COPD is suspected and 0.80 in a child
Note: Recommended reference equations: GLI, CHMS, and NHANES III
(not consistent with COPD)
Normal: ≥ LLN (or ≥0.70)5
ß2-agonist
Improved FEV1
12% and 200mL1
NoYes
Improved FEV1
12% and 200mL1
Normal Spirometry2,3
NoYes
Consider FULL PFT (+/- referral
to specialist)
Suspect Asthma
(Consistent with restriction)
Yes
Suspect Asthma
YesYes No No
(Consistent with obstruction)
© 2017 The Lung Association

Primary Care Asthma Program Spirometry Operator’s Checklist
1
PCAP SPIROMETRY OPERATOR CHECKLIST
Barometric Pressure, Relative Humidity and Temperature updated daily
Daily calibration performed according to manufacturer’s and ATS/ERS Standards
Relative Contraindications (Refer to the list on the reverse side of this page)
Minimum of three acceptable FVC performed, with two repeatable maneuvers, maximum eight performed (ATS/ERS 2005)
Assess Patient Performance: (Acceptability)
o Maximum peak effort o No hesitation or cough within first second of exhalation o Extrapolated volume < 150 ml or 5% of FVC o No glottis closure, cough or early termination of effort o No leak observed or obstruction of mouthpiece o Six seconds of exhalation collected (3 sec for <10 yrs)
Assess Measurements: (Repeatability)
o Are the 2 largest FVCs within 150 ml
of each other?
o If FVC < 1.0 L then criteria is within
100ml of each other
o Are the 2 largest FEV1s within 150
ml of each other?
o If FVC < 1.0 L then criteria is within
100ml of each other
Technical comments recorded on spirometry report
Primary Care Asthma Program Spirometry Operator’s Checklist
2
PCAP SPIROMETRY OPERATOR CHECKLIST
Relative Contraindications for Spirometry1
Recent Indicates within 6 weeks.
Relative Contraindications Comments
Cerebral aneurysm
Recent brain surgery
Recent concussion
Recent eye surgery
Significant glaucoma
Spirometry may lead to increased intraocular pressure in most patients and a 3-4 week recovery post-surgery is recommended before testing
Recent sinus surgery or middle ear surgery or infection
There is a risk that forced manoeuvres can cause pain and even ear drum ruptures in cases of middle ear infection
Pneumothorax
Significant aortic aneurysm*
Recent thoracic surgery†
Recent abdominal surgery
Pregnancyⱡ
*Spirometry causes increases in intrathoracic and intra-abdominal pressure that may increase blood pressure †Physiotherapy and coughing has been shown to be beneficial after cardiothoracic and abdominal surgery. Cough increases intrathoracic pressure up to 400cmH2O compared with 70cmH2O-200cmH2O during spirometry. The risk is therefore low in most patients. ⱡLung function tests may increase the risk of early delivery in the case of an incompetent cervix
Systemic hypotension or severe hypertension (e.g., >200/120mmHg)
Significant atrial/ventricular arrhythmia
Noncompensated heart failure
Recent myocardial infarction (MI)₰ or pulmonary embolus
History of syncope related to forced exhalation/cough
₰exercise testing one week after MI appears to be safe, however, caution is necessary where persistent myocardial ischemia exists. The use of beta2- agonists when doing post-bronchodilator spirometry can also be a risk for people with these conditions, although the risk of a single administration is likely to be minimal
Active tuberculosis
Hepatitis B
Hemoptysis or oral bleeding
Infection control procedures must be taken according to local procedures
Inability to follow direction (e.g., confusion, dementia, young age, language barrier)
In some cases, successful spirometry can be done with increased coaching and aid of an interpreter
1 Coates AL et al. Spirometry in Primary Care. Can Respir J 2013; 20(1): 13-20

L(B
VO
LU
ME
()
TP
S)
FL
(L)
(BT
P)
OW
/SS
U(B
P)
VO
LM
E(L
)T
S
U(B
P)
VO
LM
E(L
)T
S
FL
(L/S
)(B
TP
OW
S)
FLO
W(L
/S)
(BT
PS
)
UB
P)
VO
LM
E(L
)(
TS
FLO
W(L
/S)
(BT
PS
)
UM
EL
BP
)V
OL
()
(T
S
FLO
W(L
/S)
PS
)(B
T
OL
)S
)FL
W(
/S(B
TP
VO
LU
ME
(L)
(BT
PS
)
(LT
)V
OLU
ME
)(B
PS
FO
W(L
S)
TP
)L
/(B
S
RE VICE S N
A M
H
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Sharp peak
Smooth curve Smooth descent to baseline
Flat (plateau)before 15 seconds long
Steep climb Vertical rise
VLU
ME
()
(BT
PS
)O
L
FL
(/
(S
)O
WL
S)
BT
P
)V
OLU
ME
(L)
(BT
PS
(FLO
W(L
/S)
BT
PS
)
VO
LU
ME
(L)
(BT
PS
)
(FLO
W(L
/S)
BT
PS
)
VL
ME
((
T)
OU
L)
BP
S
L(
T)
FO
W(L
/S)
BP
S
A Valid Test has: 3 or More Good Curves and Repeatable FVC and FEV1*
Get Valid Spirometry Results EVERY Time
Green = Good CurveGreen = Good Curve Red = ErrorRed = Error
UB
P)
VO
LM
E(L
)(
TS
FLO
W(L
/S)
(BT
P)
S
)V
OLU
ME
(L(B
TP
S)
L(
(P
SF
OW
L/S
)B
T)
HOW TO CORRECT TEST ERRORS Poor Initial Blast
Coach: Blast air out HARDER
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Rounded or
flat peakSlow climb
Hesitation; Slow Start; Large Extrapolated Volume Delete Curve; Coach: Blast FASTER
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Peak shifted
to right
Slow take off
Cough in First Second Delete Curve; Correction: Try a drink of water
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Curve dips
Curve dips
Incomplete Inhalation Coach: Take a DEEPER breath
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Gap
Gap
Curves have same shape
but are different sizes
Difficult
to see
on this
curve
Does not flatten
for 1 second
No Plateau Before 15 Seconds Coach: Keep blowing until told to stop
6
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 TIME (sec)
12
10
8
6
4
2
0 0 1 2 3 4 5 6
VOLUME (L) (BTPS)
Inconsistent Effort Coach: One continuous blast and keep blowing
12
10
8
6
4
2
0 0 1 2 3 4 5 6
VOLUME (L) (BTPS)
Curve flattens out
Curve tilts
6
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 TIME (sec)
Partially Blocked Mouthpiece Coach: Position mouthpiece between teeth and
on top of tongue; secure dentures
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Smaller peak
and curve
wobblesCurve wobbles
Glottis Closure or Breath Holding Coach: Initial BIG BLAST then RELAX and keep blowing
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Drops straight
down
Abruptly flattens
Leak Correction: Check equipment and connections
6
5
4
3
2
1
0
12
10
8
6
4
2
0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6
TIME (sec) VOLUME (L) (BTPS)
Curve
moves
backwards
Curve drops down
Negative Zero Flow Error Correction: No airflow through sensor when spirometer zeroing
Hold sensor upright during test
TIME (sec) VOLUME (L) (BTPS)
Curve ends early
OR Curve drops down
8
7
6
5
4
3
2
1
1 2 3 4 5 6 7 8 9
14
12
10
8
6
4
2
0 1 2 3 4 5 6 7 8
Difficult
to see
on this
curve
Positive Zero Flow Error Correction: No airflow through sensor when spirometer zeroing
Hold sensor upright during test
TIME (sec) VOLUME (L) (BTPS)
Flat line
extends
to right
Continues to climb
NEVER flattens
–
Extra Breaths Correction: DELETE CURVE; Use nose clips and lips tightly sealed
TIME (sec) VOLUME (L) (BTPS)
12
10
8
6
4
2
0 0 1 2 3 4 5 6
Extra
breaths
6
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
1 or more extra breaths look like miniature additional curves
Extra breaths
Delivering on the Nation’s promise: Safety and health at work for all people through research and prevention. To receive documents or more information about occupational safety and health topics, please contact NIOSH:1-800-CDC-INFO (1-800-232-4636) TTY: 1-888-232-6348 email: [email protected] or visit the NIOSH Web site at www.cdc.gov/niosh
For a monthly update on news at NIOSH, subscribe to NIOSH eNews by visiting www.cdc.gov/niosh/eNews. For more information about NIOSH-Approved Spirometry Training go to http://www.cdc.gov/niosh/topics/spirometry/training.html
U.S. Department of Health and Human ServicesCenters for Disease Control and Prevention National Institute for Occupational Safety and Health DHHS (NIOSH) Publication No. 2011-135
S USAU
RAPED
&H
TL
AE
HF
OT
NE
MT
Section 4 Standards
4
SERIES ‘‘ATS/ERS TASK FORCE: STANDARDISATION OF LUNGFUNCTION TESTING’’Edited by V. Brusasco, R. Crapo and G. ViegiNumber 2 in this Series
Standardisation of spirometryM.R. Miller, J. Hankinson, V. Brusasco, F. Burgos, R. Casaburi, A. Coates,R. Crapo, P. Enright, C.P.M. van der Grinten, P. Gustafsson, R. Jensen,D.C. Johnson, N. MacIntyre, R. McKay, D. Navajas, O.F. Pedersen, R. Pellegrino,G. Viegi and J. Wanger
CONTENTS
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 320
FEV1 and FVC manoeuvre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Display . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 321
Validation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control for volume-measuring devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322
Quality control for flow-measuring devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 323
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Start of test criteria. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
End of test criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Additional criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 324
Summary of acceptable blow criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Manoeuvre repeatability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 325
Maximum number of manoeuvres . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Other derived indices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
FEVt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Standardisation of FEV1 for expired volume, FEV1/FVC and FEV1/VC . . . . . . . . . . . . . . . . . . . . 326
FEF25–75% . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
PEF . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Maximal expiratory flow–volume loops . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Within- and between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Flow–volume loop examples. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Reversibility testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327
Comment on dose and delivery method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 328
Determination of reversibility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 328
VC and IC manoeuvre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329
AFFILIATIONS
For affiliations, please see
Acknowledgements section
CORRESPONDENCE
V. Brusasco
Internal Medicine
University of Genoa
V.le Benedetto XV, 6
I-16132 Genova
Italy
Fax: 39 103537690
E-mail: [email protected]
Received:
March 23 2005
Accepted after revision:
April 05 2005
European Respiratory Journal
Print ISSN 0903-1936
Online ISSN 1399-3003
Previous articles in this series: No. 1: Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J 2005; 26:
153–161.
EUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 319
Eur Respir J 2005; 26: 319–338
DOI: 10.1183/09031936.05.00034805
Copyright�ERS Journals Ltd 2005
c
VC and IVC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
IC. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
VC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .329
IC. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Use of a nose clip . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .330
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .330
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Peak expiratory flow . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .331
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .331
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Maximum voluntary ventilation . . . . . . . . . . . . . . . . . . .331
Definition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Test procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Within-manoeuvre evaluation . . . . . . . . . . . . . . . . . . . . .331
Between-manoeuvre evaluation . . . . . . . . . . . . . . . . . . .331
Test result selection . . . . . . . . . . . . . . . . . . . . . . . . . . .331
Technical considerations . . . . . . . . . . . . . . . . . . . . . . . .331
Minimal recommendations for spirometry systems . . . . . .331
BTPS correction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .332
Comments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .332
Test signals for spirometer testing . . . . . . . . . . . . . . . . .333
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Accuracy test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Repeatability test . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Test signals for PEF meter testing . . . . . . . . . . . . . . . . .333
Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Accuracy test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .333
Repeatability test . . . . . . . . . . . . . . . . . . . . . . . . . . . .334
Test signals for MVV testing. . . . . . . . . . . . . . . . . . . . . .334
Abbreviations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .334
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .335
KEYWORDS: Peak expiratory flow, spirometry, spirometry standardisation, spirometry technique, spirometry traning,
ventilation
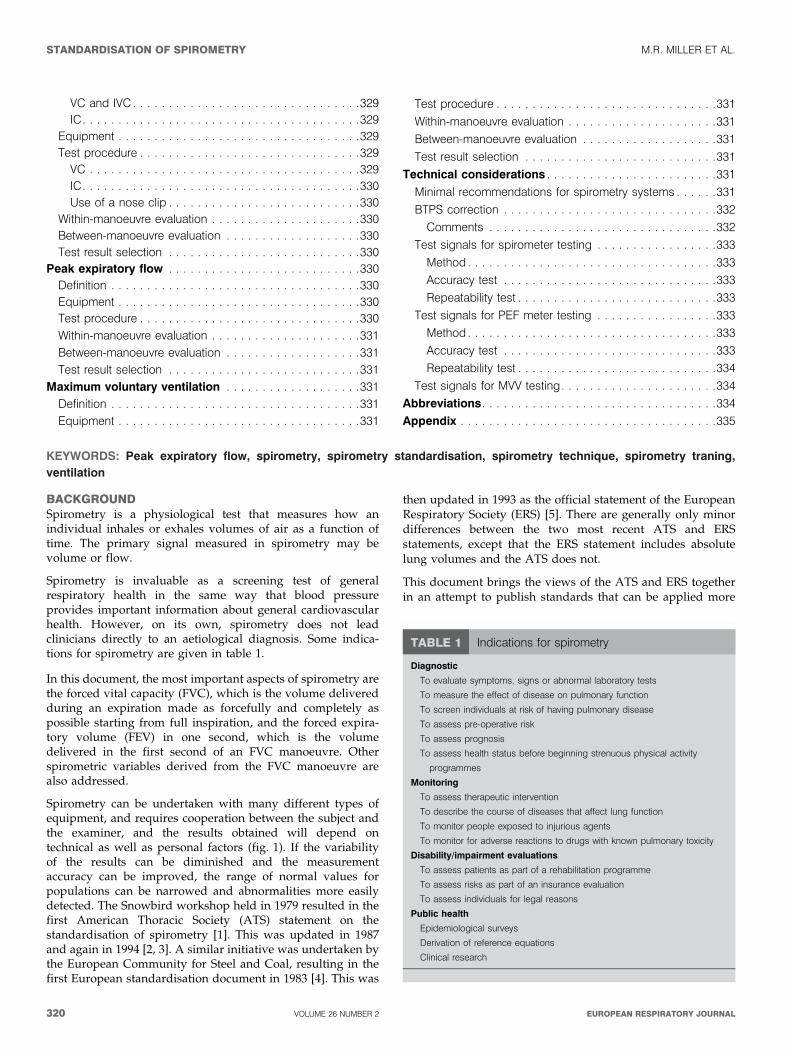
BACKGROUNDSpirometry is a physiological test that measures how anindividual inhales or exhales volumes of air as a function oftime. The primary signal measured in spirometry may bevolume or flow.
Spirometry is invaluable as a screening test of generalrespiratory health in the same way that blood pressureprovides important information about general cardiovascularhealth. However, on its own, spirometry does not leadclinicians directly to an aetiological diagnosis. Some indica-tions for spirometry are given in table 1.
In this document, the most important aspects of spirometry arethe forced vital capacity (FVC), which is the volume deliveredduring an expiration made as forcefully and completely aspossible starting from full inspiration, and the forced expira-tory volume (FEV) in one second, which is the volumedelivered in the first second of an FVC manoeuvre. Otherspirometric variables derived from the FVC manoeuvre arealso addressed.
Spirometry can be undertaken with many different types ofequipment, and requires cooperation between the subject andthe examiner, and the results obtained will depend ontechnical as well as personal factors (fig. 1). If the variabilityof the results can be diminished and the measurementaccuracy can be improved, the range of normal values forpopulations can be narrowed and abnormalities more easilydetected. The Snowbird workshop held in 1979 resulted in thefirst American Thoracic Society (ATS) statement on thestandardisation of spirometry [1]. This was updated in 1987and again in 1994 [2, 3]. A similar initiative was undertaken bythe European Community for Steel and Coal, resulting in thefirst European standardisation document in 1983 [4]. This was
then updated in 1993 as the official statement of the EuropeanRespiratory Society (ERS) [5]. There are generally only minordifferences between the two most recent ATS and ERSstatements, except that the ERS statement includes absolutelung volumes and the ATS does not.
This document brings the views of the ATS and ERS togetherin an attempt to publish standards that can be applied more
TABLE 1 Indications for spirometry
Diagnostic
To evaluate symptoms, signs or abnormal laboratory tests
To measure the effect of disease on pulmonary function
To screen individuals at risk of having pulmonary disease
To assess pre-operative risk
To assess prognosis
To assess health status before beginning strenuous physical activity
programmes
Monitoring
To assess therapeutic intervention
To describe the course of diseases that affect lung function
To monitor people exposed to injurious agents
To monitor for adverse reactions to drugs with known pulmonary toxicity
Disability/impairment evaluations
To assess patients as part of a rehabilitation programme
To assess risks as part of an insurance evaluation
To assess individuals for legal reasons
Public health
Epidemiological surveys
Derivation of reference equations
Clinical research
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
320 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL
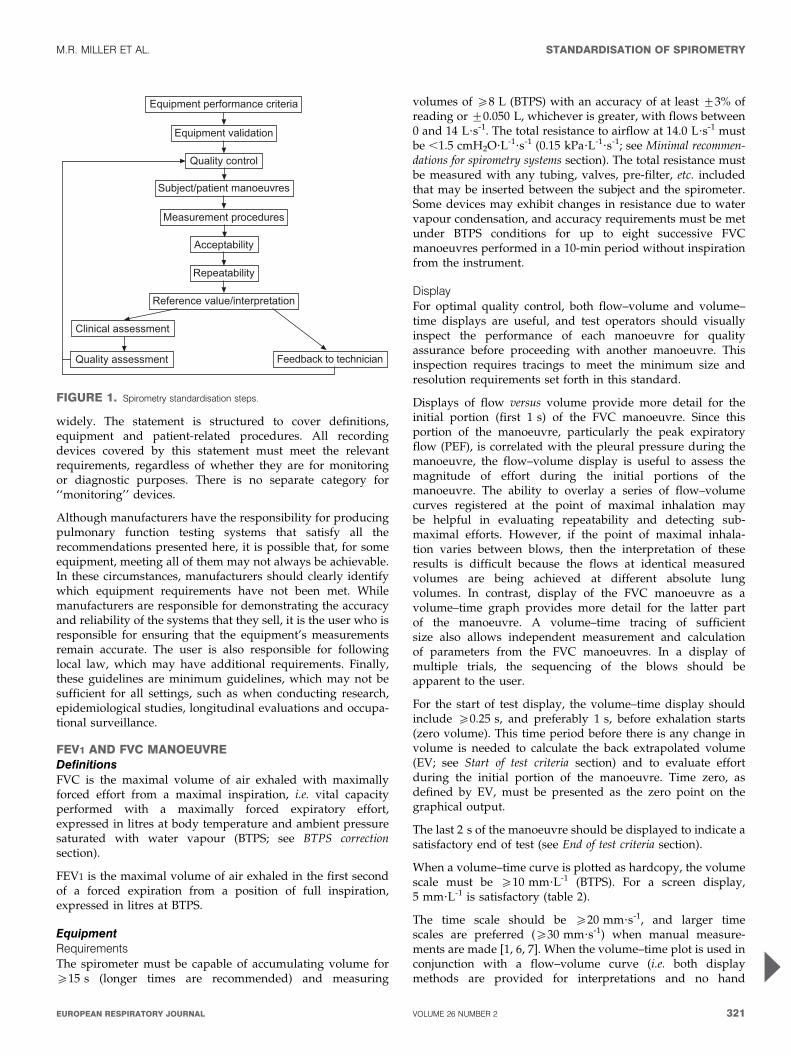
widely. The statement is structured to cover definitions,equipment and patient-related procedures. All recordingdevices covered by this statement must meet the relevantrequirements, regardless of whether they are for monitoringor diagnostic purposes. There is no separate category for‘‘monitoring’’ devices.
Although manufacturers have the responsibility for producingpulmonary function testing systems that satisfy all therecommendations presented here, it is possible that, for someequipment, meeting all of them may not always be achievable.In these circumstances, manufacturers should clearly identifywhich equipment requirements have not been met. Whilemanufacturers are responsible for demonstrating the accuracyand reliability of the systems that they sell, it is the user who isresponsible for ensuring that the equipment’s measurementsremain accurate. The user is also responsible for followinglocal law, which may have additional requirements. Finally,these guidelines are minimum guidelines, which may not besufficient for all settings, such as when conducting research,epidemiological studies, longitudinal evaluations and occupa-tional surveillance.
FEV1 AND FVC MANOEUVREDefinitionsFVC is the maximal volume of air exhaled with maximallyforced effort from a maximal inspiration, i.e. vital capacityperformed with a maximally forced expiratory effort,expressed in litres at body temperature and ambient pressuresaturated with water vapour (BTPS; see BTPS correctionsection).
FEV1 is the maximal volume of air exhaled in the first secondof a forced expiration from a position of full inspiration,expressed in litres at BTPS.
EquipmentRequirementsThe spirometer must be capable of accumulating volume foro15 s (longer times are recommended) and measuring
volumes of o8 L (BTPS) with an accuracy of at least ¡3% ofreading or ¡0.050 L, whichever is greater, with flows between0 and 14 L?s-1. The total resistance to airflow at 14.0 L?s-1 mustbe ,1.5 cmH2O?L-1?s-1 (0.15 kPa?L-1?s-1; see Minimal recommen-dations for spirometry systems section). The total resistance mustbe measured with any tubing, valves, pre-filter, etc. includedthat may be inserted between the subject and the spirometer.Some devices may exhibit changes in resistance due to watervapour condensation, and accuracy requirements must be metunder BTPS conditions for up to eight successive FVCmanoeuvres performed in a 10-min period without inspirationfrom the instrument.
DisplayFor optimal quality control, both flow–volume and volume–time displays are useful, and test operators should visuallyinspect the performance of each manoeuvre for qualityassurance before proceeding with another manoeuvre. Thisinspection requires tracings to meet the minimum size andresolution requirements set forth in this standard.
Displays of flow versus volume provide more detail for theinitial portion (first 1 s) of the FVC manoeuvre. Since thisportion of the manoeuvre, particularly the peak expiratoryflow (PEF), is correlated with the pleural pressure during themanoeuvre, the flow–volume display is useful to assess themagnitude of effort during the initial portions of themanoeuvre. The ability to overlay a series of flow–volumecurves registered at the point of maximal inhalation maybe helpful in evaluating repeatability and detecting sub-maximal efforts. However, if the point of maximal inhala-tion varies between blows, then the interpretation of theseresults is difficult because the flows at identical measuredvolumes are being achieved at different absolute lungvolumes. In contrast, display of the FVC manoeuvre as avolume–time graph provides more detail for the latter partof the manoeuvre. A volume–time tracing of sufficientsize also allows independent measurement and calculationof parameters from the FVC manoeuvres. In a display ofmultiple trials, the sequencing of the blows should beapparent to the user.
For the start of test display, the volume–time display shouldinclude o0.25 s, and preferably 1 s, before exhalation starts(zero volume). This time period before there is any change involume is needed to calculate the back extrapolated volume(EV; see Start of test criteria section) and to evaluate effortduring the initial portion of the manoeuvre. Time zero, asdefined by EV, must be presented as the zero point on thegraphical output.
The last 2 s of the manoeuvre should be displayed to indicate asatisfactory end of test (see End of test criteria section).
When a volume–time curve is plotted as hardcopy, the volumescale must be o10 mm?L-1 (BTPS). For a screen display,5 mm?L-1 is satisfactory (table 2).
The time scale should be o20 mm?s-1, and larger timescales are preferred (o30 mm?s-1) when manual measure-ments are made [1, 6, 7]. When the volume–time plot is used inconjunction with a flow–volume curve (i.e. both displaymethods are provided for interpretations and no hand
������������ �������������
��������������� �
������� �� �
��������������� ������
������������ �������
�����������
�����������
������������������������ �
�����������������
��������������� �������� �� ������
FIGURE 1. Spirometry standardisation steps.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 321

measurements are performed), the time scale requirementis reduced to 10 mm?s-1 from the usually required minimumof 20 mm?s-1 (table 2). The rationale for this exception isthat the flow–volume curve can provide the means forquality assessment during the initial portion of the FVCmanoeuvre. The volume–time curve can be used to evaluatethe latter part of the FVC manoeuvre, making the time scaleless critical.
ValidationIt is strongly recommended that spirometry systems should beevaluated using a computer-driven mechanical syringe or itsequivalent, in order to test the range of exhalations that arelikely to be encountered in the test population. Testing theperformance of equipment is not part of the usual laboratoryprocedures (see Test signals for spirometer testing section).
Quality controlAttention to equipment quality control and calibration isan important part of good laboratory practice. At a minimum,the requirements are as follows: 1) a log of calibration resultsis maintained; 2) the documentation of repairs or otheralterations which return the equipment to acceptable opera-tion; 3) the dates of computer software and hardwareupdates or changes; and 4) if equipment is changed orrelocated (e.g. industrial surveys), calibration checks andquality-control procedures must be repeated before furthertesting begins.
Key aspects of equipment quality control are summarised intable 3.
Calibration is the procedure for establishing the relationshipbetween sensor-determined values of flow or volume and theactual flow or volume.
A calibration check is different from calibration and is theprocedure used to validate that the device is within calibrationlimits, e.g. ¡3% of true. If a device fails its calibration check,then a new calibration procedure or equipment maintenance isrequired. Calibration checks must be undertaken daily, ormore frequently, if specified by the manufacturer.
The syringe used to check the volume calibration of spiro-meters must have an accuracy of ¡15 mL or ¡0.5% of the fullscale (15 mL for a 3-L syringe), and the manufacturer must
provide recommendations concerning appropriate intervalsbetween syringe calibration checks. Users should be awarethat a syringe with an adjustable or variable stop may be outof calibration if the stop is reset or accidentally moved.Calibration syringes should be periodically (e.g. monthly) leaktested at more than one volume up to their maximum; this canbe done by attempting to empty them with the outlet corked. Adropped or damaged syringe should be considered out ofcalibration until it is checked.
With regard to time, assessing mechanical recorder time scaleaccuracy with a stopwatch must be performed at leastquarterly. An accuracy of within 2% must be achieved.
Quality control for volume-measuring devicesThe volume accuracy of the spirometer must be checked at leastdaily, with a single discharge of a 3-L calibrated syringe. Dailycalibration checking is highly recommended so that the onset ofa problem can be determined within 1 day, and also to helpdefine day-to-day laboratory variability. More frequent checksmay be required in special circumstances, such as: 1) duringindustrial surveys or other studies in which a large number ofsubject manoeuvres are carried out, the equipment’s calibrationshould be checked more frequently than daily [8]; and 2) whenthe ambient temperature is changing (e.g. field studies), volumeaccuracy must be checked more frequently than daily and theBTPS correction factor appropriately updated.
The accuracy of the syringe volume must be considered indetermining whether the measured volume is within accep-table limits. For example, if the syringe has an accuracy of0.5%, a reading of ¡3.5% is appropriate.
The calibration syringe should be stored and used in such away as to maintain the same temperature and humidity of thetesting site. This is best accomplished by keeping the syringe inclose proximity to the spirometer, but out of direct sunlightand away from heat sources.
Volume-type spirometer systems must be evaluated for leaksevery day [9, 10]. The importance of undertaking this daily testcannot be overstressed. Leaks can be detected by applying aconstant positive pressure of o3.0 cmH2O (0.3 kPa) with thespirometer outlet occluded (preferably at or including themouthpiece). Any observed volume loss .30 mL after 1 minindicates a leak [9, 10] and needs to be corrected.
TABLE 2 Recommended minimum scale factors for time,volume and flow on graphical output
Instrument display Hardcopy graphical outputParameter
Resolution
required
Scale
factor
Resolution
required
Scale
factor
Volume# 0.050 L 5 mm?L-1 0.025 L 10 mm?L-1
Flow# 0.200 L?s-1 2.5 mm?L-1?s-1 0.100 L?s-1 5 mm?L-1?s-1
Time 0.2 s 10 mm?s-1 0.2 s 20 mm?s-1
#: the correct aspect ratio for a flow versus volume display is two units of flow
per one unit of volume.
TABLE 3 Summary of equipment quality control
Test Minimum interval Action
Volume Daily Calibration check with a 3-L syringe
Leak Daily 3 cmH2O (0.3 kPa) constant pressure
for 1 min
Volume linearity Quarterly 1-L increments with a calibrating syringe
measured over entire volume range
Flow linearity Weekly Test at least three different flow ranges
Time Quarterly Mechanical recorder check with stopwatch
Software New versions Log installation date and perform test using
‘‘known’’ subject
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
322 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

At least quarterly, volume spirometers must have theircalibration checked over their entire volume range using acalibrated syringe [11] or an equivalent volume standard. Themeasured volume should be within ¡3.5% of the reading or65 mL, whichever is greater. This limit includes the 0.5%accuracy limit for a 3-L syringe. The linearity check procedureprovided by the manufacturer can be used if it is equivalent toone of the following procedures: 1) consecutive injections of1-L volume increments while comparing observed volumewith the corresponding cumulative measured volume, e.g. 0–1,1–2, 2–3,…6–7 and 7–8 L, for an 8-L spirometer; and 2)injection of a 3-L volume starting at a minimal spirometervolume, then repeating this with a 1-L increment in the startposition, e.g. 0–3, 1–4, 2–5, 3–6, 4–7 and 5–8 L, for an 8-Lspirometer.
The linearity check is considered acceptable if the spirometermeets the volume accuracy requirements for all volumestested.
Quality control for flow-measuring devicesWith regards to volume accuracy, calibration checks must beundertaken at least daily, using a 3-L syringe discharged atleast three times to give a range of flows varying between 0.5and 12 L?s-1 (with 3-L injection times of ,6 s and ,0.5 s). Thevolume at each flow should meet the accuracy requirement of¡3.5%. For devices using disposable flow sensors, a newsensor from the supply used for patient tests should be testedeach day.
For linearity, a volume calibration check should be per-formed weekly with a 3-L syringe to deliver three relativelyconstant flows at a low flow, then three at a mid-range flowand finally three at a high flow. The volumes achieved at eachof these flows should each meet the accuracy requirement of¡3.5%.
Test procedureThere are three distinct phases to the FVC manoeuvre, asfollows: 1) maximal inspiration; 2) a ‘‘blast’’ of exhalation; and3) continued complete exhalation to the end of test (EOT).
The technician should demonstrate the appropriate techniqueand follow the procedure described in table 4. The subjectshould inhale rapidly and completely from functional residualcapacity (FRC), the breathing tube should be inserted into thesubject’s mouth (if this has not already been done), makingsure the lips are sealed around the mouthpiece and that thetongue does not occlude it, and then the FVC manoeuvreshould be begun with minimal hesitation. Reductions in PEFand FEV1 have been shown when inspiration is slow and/orthere is a 4–6 s pause at total lung capacity (TLC) beforebeginning exhalation [12]. It is, therefore, important that thepreceding inspiration is fast and any pause at full inspirationbe minimal (i.e. only for 1–2 s). The test assumes a fullinhalation before beginning the forced exhalation, and it isimperative that the subject takes a complete inhalation beforebeginning the manoeuvre. The subject should be prompted to‘‘blast,’’ not just ‘‘blow,’’ the air from their lungs, and then he/she should be encouraged to fully exhale. Throughout themanoeuvre, enthusiastic coaching of the subject using appro-priate body language and phrases, such as ‘‘keep going’’, is
required. It is particularly helpful to observe the subject withoccasional glances to check for distress, and to observe thetracing or computer display during the test to help ensuremaximal effort. If the patient feels ‘‘dizzy’’, the manoeuvreshould be stopped, since syncope could follow due toprolonged interruption of venous return to the thorax. This ismore likely to occur in older subjects and those with airflowlimitation. Performing a vital capacity (VC) manoeuvre (see VCand IC manoeuvre section), instead of obtaining FVC, may helpto avoid syncope in some subjects. Reducing the effort part-way through the manoeuvre [13] may give a higher expiratoryvolume in some subjects, but then is no longer a maximallyforced expiration. Well-fitting false teeth should not beroutinely removed, since they preserve oropharyngeal geome-try and spirometry results are generally better with them inplace [14].
With appropriate coaching, children as young as 5 yrs ofage are often able to perform acceptable spirometry [15].The technicians who are involved in the pulmonary functiontesting of children should be specifically trained to dealwith such a situation. A bright, pleasant atmosphere,
TABLE 4 Procedures for recording forced vital capacity
Check the spirometer calibration
Explain the test
Prepare the subject
Ask about smoking, recent illness, medication use, etc.
Measure weight and height without shoes
Wash hands
Instruct and demonstrate the test to the subject, to include
Correct posture with head slightly elevated
Inhale rapidly and completely
Position of the mouthpiece (open circuit)
Exhale with maximal force
Perform manoeuvre (closed circuit method)
Have subject assume the correct posture
Attach nose clip, place mouthpiece in mouth and close lips around the
mouthpiece
Inhale completely and rapidly with a pause of ,1 s at TLC
Exhale maximally until no more air can be expelled while maintaining an upright
posture
Repeat instructions as necessary, coaching vigorously
Repeat for a minimum of three manoeuvres; no more than eight are usually
required
Check test repeatability and perform more manoeuvres as necessary
Perform manoeuvre (open circuit method)
Have subject assume the correct posture
Attach nose clip
Inhale completely and rapidly with a pause of ,1 s at TLC
Place mouthpiece in mouth and close lips around the mouthpiece
Exhale maximally until no more air can be expelled while maintaining an upright
posture
Repeat instructions as necessary, coaching vigorously
Repeat for a minimum of three manoeuvres; no more than eight are usually
required
Check test repeatability and perform more manoeuvres as necessary
TLC: total lung capacity.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 323

including age-appropriate toys, reading material and art, isimportant in making children feel at ease. Encouragement,detailed but simple instructions, lack of intimidation andvisual feedback in the teaching are important in helpingchildren to perform the manoeuvre. Even if unsuccessful atthe first session, children will learn to be less intimidatedand may perform far better in a subsequent session. Testingchildren in ‘‘adult’’ laboratories, where no effort is made tocater for the specific needs of the younger subjects, is to bediscouraged.
The use of a nose clip or manual occlusion of the nares isrecommended, and, for safety reasons, testing should bepreferably done in the sitting position, using a chair witharms and without wheels. If testing is undertaken with thepatient standing or in another position, this must bedocumented on the report.
Within-manoeuvre evaluationStart of test criteriaThe start of test, for the purpose of timing, is determined by theback extrapolation method (fig. 2) [1, 3, 9, 16]. The new ‘‘timezero’’ from back extrapolation defines the start for all timedmeasurements. For manual measurements, the back extrapola-tion method traces back from the steepest slope on thevolume–time curve [17]. For computerised back extrapolation,it is recommended that the largest slope averaged over an 80-ms period is used [18]. Figure 2 provides an example andexplanation of back extrapolation and the derivation of EV. Toachieve an accurate time zero and assure the FEV1 comes froma maximal effort curve, the EV must be ,5% of the FVC or0.150 L, whichever is greater. If a manoeuvre has an obviouslyhesitant start, the technician may terminate the trial early toavoid an unnecessary prolonged effort.
Rapid computerised feedback to the technician when the startcriteria are not met is strongly encouraged. In addition to theexpiratory manoeuvre, the volume-time curve display (graph)
should ideally include the whole preceding inspiratorymanoeuvre, but must include o0.25 s and preferably o1 sprior to the start of exhalation (time zero). The equipmentshould display the EV value. Inspection of the flow–volumecurve may be added as a measure of the satisfactory start oftest. PEF should be achieved with a sharp rise and occur closeto the point of maximal inflation, i.e. the start of exhalation (seeEquipment section).
End of test criteriaIt is important for subjects to be verbally encouraged tocontinue to exhale the air at the end of the manoeuvre to obtainoptimal effort, e.g. by saying ‘‘keep going’’. EOT criteria areused to identify a reasonable FVC effort, and there are tworecommended EOT criteria, as follows. 1) The subject cannot orshould not continue further exhalation. Although subjectsshould be encouraged to achieve their maximal effort, theyshould be allowed to terminate the manoeuvre on their own atany time, especially if they are experiencing discomfort. Thetechnician should also be alert to any indication that the patientis experiencing discomfort, and should terminate the test if apatient is becoming uncomfortable or is approaching syncope.2) The volume–time curve shows no change in volume(,0.025 L) for o1 s, and the subject has tried to exhale foro3 s in children aged ,10 yrs and for o6 s in subjects aged.10 yrs.
The equipment should signal to the technician if the plateaucriteria were not met. A satisfactory EOT may still have beenachieved, but an equipment alert will help the technician topinpoint where the subject may need more encouragement.It is of note that a closure of the glottis may prematurelyterminate a manoeuvre at ,6 s, even when the apparentduration of the blow exceeds 6 s.
For patients with airways obstruction or older subjects,exhalation times of .6 s are frequently needed. However,exhalation times of .15 s will rarely change clinical decisions.Multiple prolonged exhalations are seldom justified and maycause light headedness, syncope, undue fatigue and unneces-sary discomfort.
Achieving EOT criteria is one measure of manoeuvre accept-ability. Manoeuvres that do not meet EOT criteria should notbe used to satisfy the requirement of three acceptablemanoeuvres. However, early termination, by itself, is not areason to eliminate all the results from such a manoeuvre fromfurther consideration. Information such as the FEV1 may beuseful (depending on the length of exhalation) and can bereported from these early terminated manoeuvres.
Some young children may have difficulty meeting the ATSEOT criteria [3], although they may meet other repeatabilitycriteria [19]. Curve-fitting techniques [20] may prove useful indeveloping new EOT criteria specific for young children.
Additional criteriaA cough during the first second of the manoeuvre can affectthe measured FEV1 value. Coughing in the first second or anyother cough that, in the technician’s judgment, interferes withthe measurement of accurate results [3] will render a testunacceptable.
!"#
�$!"!
%"!
!"&
!"'
!"(
$ ���
�)
!"*!!"(*!"!!+�,���-��
.����
FIGURE 2. Expanded version of the early part of a subject’s volume–time
spirogram, illustrating back extrapolation through the steepest part of the curve,
where flow is peak expiratory flow (PEF), to determine the new ‘‘time zero’’. Forced
vital capacity (FVC)54.291 L; back extrapolated volume (EV)50.123 L (2.9% FVC).
-----: back extrapolation line through PEF.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
324 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

A Valsalva manoeuvre (glottis closure) or hesitation during themanoeuvre that causes a cessation of airflow in a manner thatprecludes an accurate estimate of either FEV1 or FVC [3] willrender a test unacceptable.
There must be no leak at the mouth [3]. Patients withneuromuscular disease may require manual or other assistancefrom the technician to guarantee an adequate seal.
Obstruction of the mouthpiece, e.g. by the tongue being placedin front of the mouthpiece or by teeth in front of themouthpiece, or by distortion from biting, may affect theperformance of either the device or the subject.
Summary of acceptable blow criteriaThe acceptability criteria are a satisfactory start of test and asatisfactory EOT, i.e. a plateau in the volume–time curve. Inaddition, the technician should observe that the subjectunderstood the instructions and performed the manoeuvrewith a maximum inspiration, a good start, a smoothcontinuous exhalation and maximal effort. The followingconditions must also be met: 1) without an unsatisfactory startof expiration, characterised by excessive hesitation or falsestart extrapolated volume or EV .5% of FVC or 0.150 L,whichever is greater (fig. 2); 2) without coughing during thefirst second of the manoeuvre, thereby affecting the measuredFEV1 value, or any other cough that, in the technician’sjudgment, interferes with the measurement of accurate results[3]; 3) without early termination of expiration (see End of testcriteria section); 4) without a Valsalva manoeuvre (glottisclosure) or hesitation during the manoeuvre that causes acessation of airflow, which precludes accurate measurement ofFEV1 or FVC [3]; 5) without a leak [3]; 6) without an obstructedmouthpiece (e.g. obstruction due to the tongue being placed infront of the mouthpiece, or teeth in front of the mouthpiece, ormouthpiece deformation due to biting); and 7) withoutevidence of an extra breath being taken during the manoeuvre.
It should be noted that a usable curve must only meetconditions 1 and 2 above, while an acceptable curve must meetall of the above seven conditions.
It is desirable to use a computer-based system that providesfeedback to the technician when the above conditions are notmet. The reporting format should include qualifiers indicatingthe acceptability of each manoeuvre. However, failure to meetthese goals should not necessarily prevent reporting of results,since, for some subjects, this is their best performance. Recordsof such manoeuvres should be retained since they may containuseful information.
Between-manoeuvre evaluationUsing the previously described criteria, an adequate testrequires a minimum of three acceptable FVC manoeuvres.Acceptable repeatability is achieved when the differencebetween the largest and the next largest FVC is f0.150 Land the difference between the largest and next largest FEV1 isf0.150 L [21]. For those with an FVC of f1.0 L, both thesevalues are 0.100 L. If these criteria are not met in threemanoeuvres, additional trials should be attempted, up to, butusually no more than, eight manoeuvres. Large variabilityamong tests is often due to incomplete inhalations. Somepatients may require a brief rest period between manoeuvres.
Volume–time or flow–volume curves from at least the bestthree FVC manoeuvres must be retained. Table 5 gives asummary of the within- and between-manoeuvre evaluation.
Manoeuvre repeatabilityFor FVC measurements, acceptability must be determined byascertaining that the recommendations outlined previously onperforming the FVC test are met. The guidelines of the ATS [3]contain examples of unacceptable volume–time and corre-sponding flow–volume curves. Figure 3 shows a flow chartoutlining how the criteria for blow acceptability are appliedbefore those for repeatability.
The repeatability criteria are used to determine when morethan three acceptable FVC manoeuvres are needed; thesecriteria are not to be used to exclude results from reports or toexclude subjects from a study. Labelling results as beingderived from data that do not conform to the repeatabilitycriteria described previously is recommended. In addition, therepeatability criteria are minimum requirements. Many sub-jects are able to achieve FVC and FEV1 repeatability to within0.150 L. Manoeuvres with an unacceptable start of test or acough (unusable curve) must be discarded before applying therepeatability criteria and cannot be used in determining thebest values. Manoeuvres with early termination or a Valsalvamanoeuvre may be used for selecting the largest FVC andFEV1.
TABLE 5 Summary of within- and between-manoeuvreacceptability criteria
Within-manoeuvre criteria
Individual spirograms are ‘‘acceptable’’ if
They are free from artefacts [3]
Cough during the first second of exhalation
Glottis closure that influences the measurement
Early termination or cut-off
Effort that is not maximal throughout
Leak
Obstructed mouthpiece
They have good starts
Extrapolated volume ,5% of FVC or 0.15 L, whichever is greater
They show satisfactory exhalation
Duration of o6 s (3 s for children) or a plateau in the volume–time curve or
If the subject cannot or should not continue to exhale
Between-manoeuvre criteria
After three acceptable spirograms have been obtained, apply the following
tests
The two largest values of FVC must be within 0.150 L of each other
The two largest values of FEV1 must be within 0.150 L of each other
If both of these criteria are met, the test session may be concluded
If both of these criteria are not met, continue testing until
Both of the criteria are met with analysis of additional acceptable spirograms
or
A total of eight tests have been performed (optional) or
The patient/subject cannot or should not continue
Save, as a minimum, the three satisfactory manoeuvres
FVC: forced vital capacity; FEV1: forced expiratory volume in one second.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 325
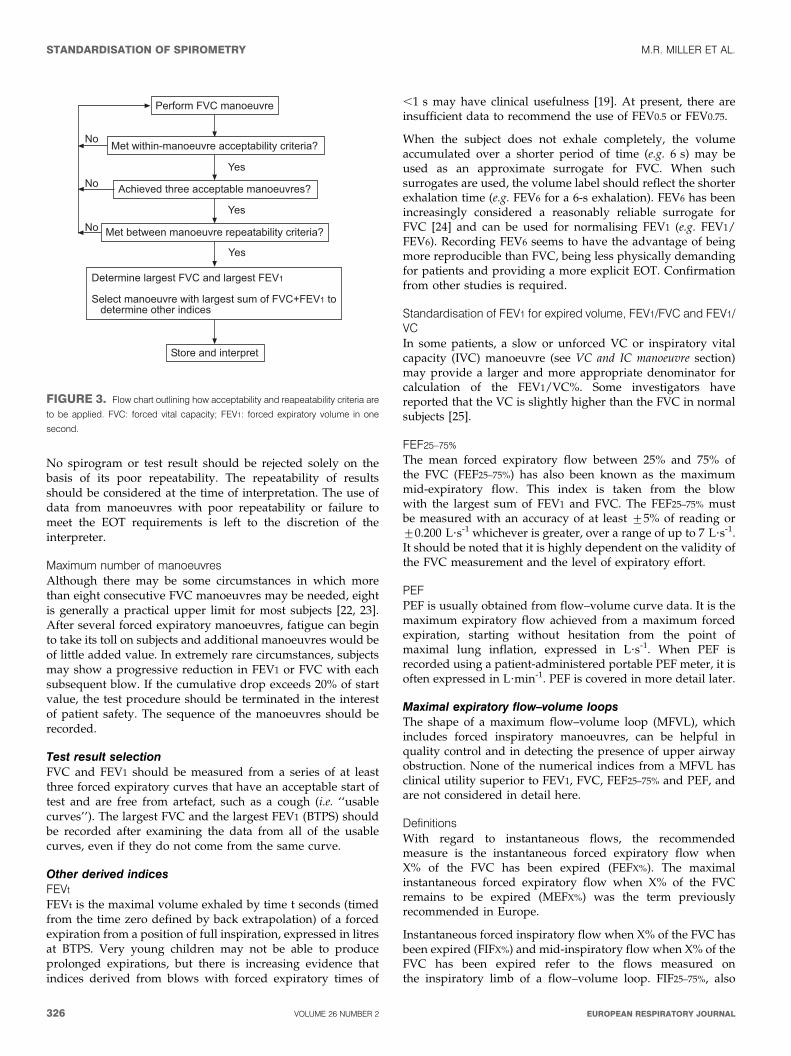
No spirogram or test result should be rejected solely on thebasis of its poor repeatability. The repeatability of resultsshould be considered at the time of interpretation. The use ofdata from manoeuvres with poor repeatability or failure tomeet the EOT requirements is left to the discretion of theinterpreter.
Maximum number of manoeuvresAlthough there may be some circumstances in which morethan eight consecutive FVC manoeuvres may be needed, eightis generally a practical upper limit for most subjects [22, 23].After several forced expiratory manoeuvres, fatigue can beginto take its toll on subjects and additional manoeuvres would beof little added value. In extremely rare circumstances, subjectsmay show a progressive reduction in FEV1 or FVC with eachsubsequent blow. If the cumulative drop exceeds 20% of startvalue, the test procedure should be terminated in the interestof patient safety. The sequence of the manoeuvres should berecorded.
Test result selectionFVC and FEV1 should be measured from a series of at leastthree forced expiratory curves that have an acceptable start oftest and are free from artefact, such as a cough (i.e. ‘‘usablecurves’’). The largest FVC and the largest FEV1 (BTPS) shouldbe recorded after examining the data from all of the usablecurves, even if they do not come from the same curve.
Other derived indicesFEVt
FEVt is the maximal volume exhaled by time t seconds (timedfrom the time zero defined by back extrapolation) of a forcedexpiration from a position of full inspiration, expressed in litresat BTPS. Very young children may not be able to produceprolonged expirations, but there is increasing evidence thatindices derived from blows with forced expiratory times of
,1 s may have clinical usefulness [19]. At present, there areinsufficient data to recommend the use of FEV0.5 or FEV0.75.
When the subject does not exhale completely, the volumeaccumulated over a shorter period of time (e.g. 6 s) may beused as an approximate surrogate for FVC. When suchsurrogates are used, the volume label should reflect the shorterexhalation time (e.g. FEV6 for a 6-s exhalation). FEV6 has beenincreasingly considered a reasonably reliable surrogate forFVC [24] and can be used for normalising FEV1 (e.g. FEV1/FEV6). Recording FEV6 seems to have the advantage of beingmore reproducible than FVC, being less physically demandingfor patients and providing a more explicit EOT. Confirmationfrom other studies is required.
Standardisation of FEV1 for expired volume, FEV1/FVC and FEV1/VCIn some patients, a slow or unforced VC or inspiratory vitalcapacity (IVC) manoeuvre (see VC and IC manoeuvre section)may provide a larger and more appropriate denominator forcalculation of the FEV1/VC%. Some investigators havereported that the VC is slightly higher than the FVC in normalsubjects [25].
FEF25–75%
The mean forced expiratory flow between 25% and 75% ofthe FVC (FEF25–75%) has also been known as the maximummid-expiratory flow. This index is taken from the blowwith the largest sum of FEV1 and FVC. The FEF25–75% mustbe measured with an accuracy of at least ¡5% of reading or¡0.200 L?s-1 whichever is greater, over a range of up to 7 L?s-1.It should be noted that it is highly dependent on the validity ofthe FVC measurement and the level of expiratory effort.
PEFPEF is usually obtained from flow–volume curve data. It is themaximum expiratory flow achieved from a maximum forcedexpiration, starting without hesitation from the point ofmaximal lung inflation, expressed in L?s-1. When PEF isrecorded using a patient-administered portable PEF meter, it isoften expressed in L?min-1. PEF is covered in more detail later.
Maximal expiratory flow–volume loopsThe shape of a maximum flow–volume loop (MFVL), whichincludes forced inspiratory manoeuvres, can be helpful inquality control and in detecting the presence of upper airwayobstruction. None of the numerical indices from a MFVL hasclinical utility superior to FEV1, FVC, FEF25–75% and PEF, andare not considered in detail here.
DefinitionsWith regard to instantaneous flows, the recommendedmeasure is the instantaneous forced expiratory flow whenX% of the FVC has been expired (FEFX%). The maximalinstantaneous forced expiratory flow when X% of the FVCremains to be expired (MEFX%) was the term previouslyrecommended in Europe.
Instantaneous forced inspiratory flow when X% of the FVC hasbeen expired (FIFX%) and mid-inspiratory flow when X% of theFVC has been expired refer to the flows measured onthe inspiratory limb of a flow–volume loop. FIF25–75%, also
/��� ���$���� �����
��,� ��0��� �����������������������1
�� ����� ��������������� ������1
����,������ �����������������������1
2����������3���$�������3����$%
�������� �����,� ���3����� ��$�4��$% �������� ���������
� ������������
5��
5��
5��
+
+
+
FIGURE 3. Flow chart outlining how acceptability and reapeatability criteria are
to be applied. FVC: forced vital capacity; FEV1: forced expiratory volume in one
second.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
326 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

referred to as maximal mid-inspiratory flow, is analogous toFEF25–75% (see Other derived indices section).
EquipmentInstantaneous flows must be measured with an accuracy of¡5% of reading or ¡0.200 L?s-1, whichever is greater, over arange of -14–14 L?s-1. The level of minimum detectable flowshould be 0.025 L?s-1. When a maximum flow–volume loop isplotted or displayed, exhaled flow must be plotted upwards,and exhaled volume towards the right. A 2:1 ratio must bemaintained between the flow and volume scales, e.g. 2 L?s-1 offlow and 1 L of exhaled volume must be the same distance ontheir respective axes. The flow and volume scales, used inreviewing test performance, must be equivalent to that shownin table 2.
Test procedureThe subject has to make a full expiratory and inspiratory loopas a single manoeuvre. In many laboratories, this is theprimary manoeuvre for spirometry. The subject is asked totake a rapid full inspiration to TLC from room air through themouth, then insert the mouthpiece and, without hesitation,perform an expiration with maximum force until no more gascan be expelled, followed by a quick maximum inspiration. Atthis point, the manoeuvre is finished.
An alternative procedure is for the subject to insert themouthpiece while undertaking tidal breathing at FRC, andthen, in one continuous sequence, do the following: make aslow expiration to residual volume (RV); followed directly by aslow inspiration to TLC; follow this by a rapid full expirationwith maximal effort to RV; and followed by a rapid fullinspiration with maximal effort back to TLC.
This procedure is slightly more complicated and may not besuitable for all equipment, but it obtains a measurement of VCas well as FVC.
Within- and between-manoeuvre evaluationThese evaluations are the same as for FVC (see Within-manoeuvre evaluation and Between-manoeuvre evaluation sec-tions). Occasionally, a subject is unable to perform asatisfactory inspiratory limb immediately following a maximalforced expiratory manoeuvre. This is particularly common inthe elderly and the infirm. In these circumstances, it may benecessary for the subject to record an inspiratory manoeuvreseparately from the expiratory manoeuvre. Equipment shouldbe able to perform these separately and then present three ormore loops together on a graphical display or output.
Flow–volume loop examplesThe following figures (figures 4–10) give typical examples ofcommonly encountered flow–volume loop configurations. Theadvantages of visual pattern recognition from the MFVL canreadily be appreciated. The shapes of the manoeuvres must berepeatable (fig. 10) for any interpretation to be made. This isespecially true for the plateau effect on expiratory andinspiratory limbs of the manoeuvre found in upper airwayobstruction, as this can be mimicked by poor effort, which isusually variable from blow to blow. A further explanation isgiven in the ATS/ERS statement on lung function interpreta-tion [26].
Reversibility testingA determination of airflow-limitation reversibility with drugadministration is commonly undertaken as part of lungfunction testing. The choice of drug, dose and mode ofdelivery is a clinical decision depending on what the clinicianwishes to learn from the test.
If the aim of the test is to determine whether the patient’s lungfunction can be improved with therapy in addition to theirregular treatment, then the subject can continue with his/herregular medication prior to the test.
If the clinician wants to determine whether there is anyevidence of reversible airflow limitation, then the subjectshould undergo baseline function testing when not taking anydrugs prior to the test. Short-acting inhaled drugs (e.g. the b-agonist albuterol/salbutamol or the anticholinergic agentipratropium bromide) should not be used within 4 h of testing.Long-acting b-agonist bronchodilators (e.g. salmeterol orformoterol) and oral therapy with aminophylline or slow-release b-agonists should be stopped for 12 h prior to the test.Smoking should be avoided for o1 h prior to testing andthroughout the duration of the test procedure.
MethodThe following steps are undertaken. 1) The subject has threeacceptable tests of FEV1, FVC and PEF recorded as describedpreviously. 2) The drug is administered in the dose and by themethod indicated for the test. For example, after a gentle andincomplete expiration, a dose of 100 mg of albuterol/salbuta-mol is inhaled in one breath to TLC from a valved spacerdevice. The breath is then held for 5–10 s before the subjectexhales. Four separate doses (total dose 400 mg) are delivered at,30-s intervals. This dose ensures that the response is high onthe albuterol dose–response curve. A lower dose can be used ifthere is concern about any effect on the patient’s heart rate ortremor. Other drugs can also be used. For the anticholinergicagent ipratropium bromide, the total dose is 160 mg (4640 mg).
Three additional acceptable tests are recorded o10 min andup to 15 min later for short-acting b2-agonists, and 30 min laterfor short-acting anticholinergic agents.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 4. Flow–volume loop of a normal subject.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 327

Comment on dose and delivery methodStandardising the bronchodilator dose administered isnecessary in order to standardise the definition of asignificant bronchodilator response. The rate of pulmonarydeposition of a drug with tidal breathing from an unventednebuliser will depend on drug concentration, rate ofnebuliser output, particle-size distribution, and the ratioof the time spent in inspiration over the total respiratorytime (ti/ttot) [27]. The fraction of the aerosol carried inparticles with a diameter of f5 mm that is expected todeposit in adult lungs if inhaled through a mouthpiece [28]is defined as the respirable fraction (RF). For example,2.5 mg of salbutamol (albuterol) in 2.5 mL of solution,placed in a Hudson Updraft II (Hudson RCI, Temecula,CA, USA) driven by a PulmoAide compressor (De Vilbiss,Somerset, PA, USA), would produce ,0.1 mg?min-1 in theRF. For a respiratory rate of 15 breaths?min-1 and a ti/ttot
of 0.45, this would give ,3 mg deposited in the lungs perbreath, or 45 mg?min-1. For adults using a metered dose
inhaler (MDI) with a valve-holding chamber (spacer),between 10 and 20% [29, 30] of a 100-mg ‘‘puff’’ (or ,15mg per activation) would be expected to be deposited inthe lung of an adult. Without a spacer, the deposition willbe less, and heavily technique dependent [31]. Pulmonarydeposition from dry-powder inhalers is device specific, andbreath-enhanced nebulisers deposit much more thanunvented ones [32, 33]. CFC-free MDIs produce a smallerparticle-size distribution and improved (up to 50% of dose)lung deposition compared with those with CFC propellant[34]. For children, pulmonary deposition is less than that inadults [35], possibly relating to the size of the upperairway. Each laboratory should be familiar with thepulmonary-deposition characteristics of the devices theyuse.
Determination of reversibilityThis aspect is covered in detail in the interpretative strategydocument of the ATS and ERS [26].
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 5. Flow–volume loop of a normal sub-
ject with end expiratory curvilinearity, which can be
seen with ageing.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 6. Moderate airflow limitation in a
subject with asthma.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 7. Severe airflow limitation in a subject
with chronic obstructive pulmonary disease.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 8. Variable intra-thoracic upper airway
obstruction.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 9. Variable extra-thoracic upper airway
obstruction.
%(
%!
#
&
'
(
!
0(
0'
0&
0#
�� ,)6�0%
! % ( 7 ' * &$ ����)
FIGURE 10. Fixed upper airway obstruction
shown by three manoeuvres.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
328 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL
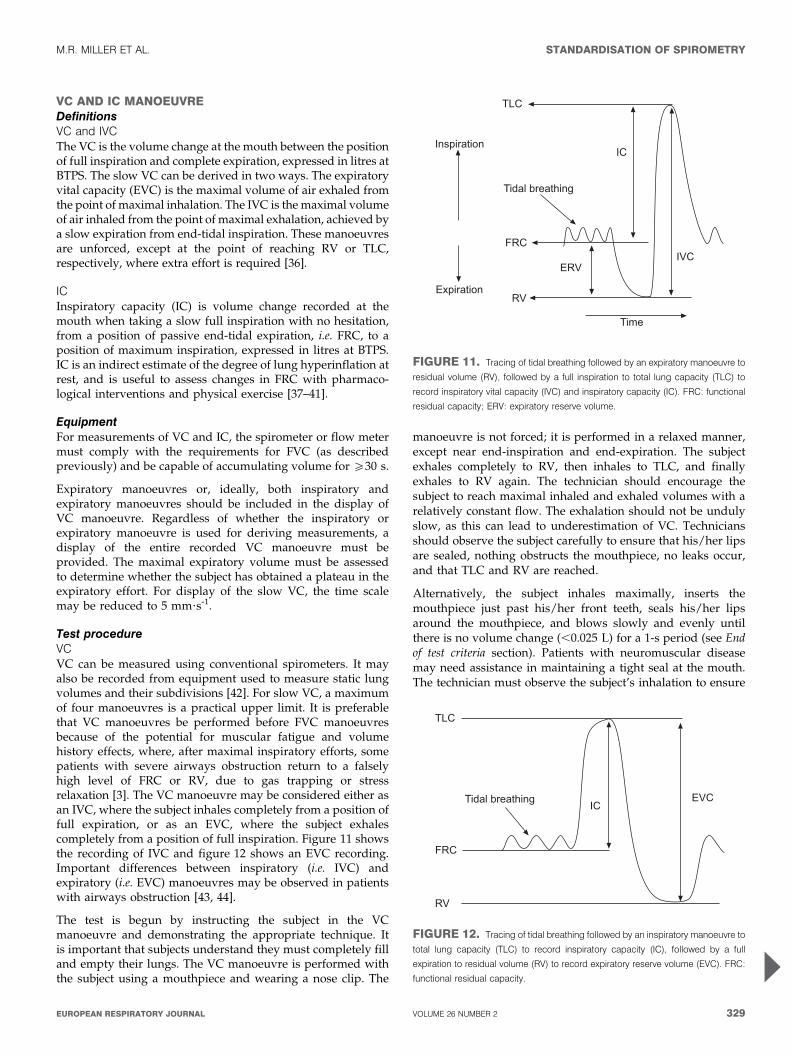
VC AND IC MANOEUVREDefinitionsVC and IVCThe VC is the volume change at the mouth between the positionof full inspiration and complete expiration, expressed in litres atBTPS. The slow VC can be derived in two ways. The expiratoryvital capacity (EVC) is the maximal volume of air exhaled fromthe point of maximal inhalation. The IVC is the maximal volumeof air inhaled from the point of maximal exhalation, achieved bya slow expiration from end-tidal inspiration. These manoeuvresare unforced, except at the point of reaching RV or TLC,respectively, where extra effort is required [36].
ICInspiratory capacity (IC) is volume change recorded at themouth when taking a slow full inspiration with no hesitation,from a position of passive end-tidal expiration, i.e. FRC, to aposition of maximum inspiration, expressed in litres at BTPS.IC is an indirect estimate of the degree of lung hyperinflation atrest, and is useful to assess changes in FRC with pharmaco-logical interventions and physical exercise [37–41].
EquipmentFor measurements of VC and IC, the spirometer or flow metermust comply with the requirements for FVC (as describedpreviously) and be capable of accumulating volume for o30 s.
Expiratory manoeuvres or, ideally, both inspiratory andexpiratory manoeuvres should be included in the display ofVC manoeuvre. Regardless of whether the inspiratory orexpiratory manoeuvre is used for deriving measurements, adisplay of the entire recorded VC manoeuvre must beprovided. The maximal expiratory volume must be assessedto determine whether the subject has obtained a plateau in theexpiratory effort. For display of the slow VC, the time scalemay be reduced to 5 mm?s-1.
Test procedureVCVC can be measured using conventional spirometers. It mayalso be recorded from equipment used to measure static lungvolumes and their subdivisions [42]. For slow VC, a maximumof four manoeuvres is a practical upper limit. It is preferablethat VC manoeuvres be performed before FVC manoeuvresbecause of the potential for muscular fatigue and volumehistory effects, where, after maximal inspiratory efforts, somepatients with severe airways obstruction return to a falselyhigh level of FRC or RV, due to gas trapping or stressrelaxation [3]. The VC manoeuvre may be considered either asan IVC, where the subject inhales completely from a position offull expiration, or as an EVC, where the subject exhalescompletely from a position of full inspiration. Figure 11 showsthe recording of IVC and figure 12 shows an EVC recording.Important differences between inspiratory (i.e. IVC) andexpiratory (i.e. EVC) manoeuvres may be observed in patientswith airways obstruction [43, 44].
The test is begun by instructing the subject in the VCmanoeuvre and demonstrating the appropriate technique. Itis important that subjects understand they must completely filland empty their lungs. The VC manoeuvre is performed withthe subject using a mouthpiece and wearing a nose clip. The
manoeuvre is not forced; it is performed in a relaxed manner,except near end-inspiration and end-expiration. The subjectexhales completely to RV, then inhales to TLC, and finallyexhales to RV again. The technician should encourage thesubject to reach maximal inhaled and exhaled volumes with arelatively constant flow. The exhalation should not be undulyslow, as this can lead to underestimation of VC. Techniciansshould observe the subject carefully to ensure that his/her lipsare sealed, nothing obstructs the mouthpiece, no leaks occur,and that TLC and RV are reached.
Alternatively, the subject inhales maximally, inserts themouthpiece just past his/her front teeth, seals his/her lipsaround the mouthpiece, and blows slowly and evenly untilthere is no volume change (,0.025 L) for a 1-s period (see Endof test criteria section). Patients with neuromuscular diseasemay need assistance in maintaining a tight seal at the mouth.The technician must observe the subject’s inhalation to ensure
.)�
8�
��$8$�
���
�$
.�������� ��3
8������� �
�9����� �
.���
FIGURE 11. Tracing of tidal breathing followed by an expiratory manoeuvre to
residual volume (RV), followed by a full inspiration to total lung capacity (TLC) to
record inspiratory vital capacity (IVC) and inspiratory capacity (IC). FRC: functional
residual capacity; ERV: expiratory reserve volume.
.�������� ��3
.)�
���
�$
8��$�
FIGURE 12. Tracing of tidal breathing followed by an inspiratory manoeuvre to
total lung capacity (TLC) to record inspiratory capacity (IC), followed by a full
expiration to residual volume (RV) to record expiratory reserve volume (EVC). FRC:
functional residual capacity.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 329
that it is complete, and that air is not exhaled while themouthpiece is being inserted. The technician should assurethat the expiratory manoeuvre is not forced. In healthysubjects, adequate maximal inspiratory and expiratory levelsare achieved within 5–6 s.
ICSubjects should be tested in the seated position wearing a noseclip with no air leaks between the mouth and the mouthpiece.Subjects should be relaxed (shoulders down and relaxed) andasked to breathe regularly for several breaths until the end-expiratory lung volume is stable (this usually requires at leastthree tidal manoeuvres). They are then urged to take a deepbreath to TLC with no hesitation. Figure 12 shows a tracingfrom the recording of IC.
Use of a nose clipThe use of a nose clip is encouraged in VC measurements,since some people breathe through the nose when performinga slow VC manoeuvre. A nose clip must be used whenperforming inspiratory manoeuvres such as the IVC or IC.
Within-manoeuvre evaluationThese are the same as for FVC EOT criteria as describedpreviously. There must be no leak at the mouth, no hesitationduring the manoeuvre, and no obstruction of the mouthpiece(see Additional criteria section). The IC may be underestimatedif the inspiratory manoeuvre is too slow due to poor effort orhesitation, or if there is premature closure of the glottis.
Between-manoeuvre evaluationAs with spirometry, a minimum of three acceptable VCmanoeuvres must be obtained. If the difference in VC betweenthe largest and next largest manoeuvre is .0.150 L, additionaltrials should be undertaken. Meeting repeatability criteria mayrequire that up to, but usually no more than, four manoeuvresare performed, with a rest period of o1 min between themanoeuvres. Large variability in this test is often due toincomplete inhalations. Volume–time curves from the best twoVC manoeuvres must be retained. For the IC, at least threeacceptable manoeuvres should be performed. The meancoefficient of variation for IC in chronic airflow obstructionhas been found to be 5 ¡3% [39].
Test result selectionFor VC, the largest value from at least three acceptablemanoeuvres should be reported. For IC, the average of at leastthree manoeuvres should be reported.
PEAK EXPIRATORY FLOWStudies on the measurement of PEF are ongoing. Recentevidence has suggested that the previously applied standardsmay allow incorrect measurements to be made [45], and it ispossible that more stringent requirements may be required. Afurther statement will be made when the position on theclinical significance of this is clear. However, since PEFmeasurements are part of asthma-management programmes,the previous recommendations [3, 46] are reiterated here.
Other instantaneous flow measurements (e.g. FEF50%, FEF75%)are not proven to be superior to conventional spirometric
indices in a clinical setting, and, therefore, are not consideredfurther.
DefinitionPEF is the highest flow achieved from a maximum forcedexpiratory manoeuvre started without hesitation from a posi-tion of maximal lung inflation [46]. When it is obtained fromflow–volume curve data, it is expressed at BTPS in L?s-1. Thedefining characteristics of the flow–time curve, in relation toPEF, are the time taken for flow to rise from 10% of PEF to 90%of PEF, i.e. the rise time (RT), and the duration that flow is .90%of PEF, called the dwell time (DT). When PEF is obtained withportable monitoring instruments, it is expressed in L?min-1.
EquipmentIdeally, PEF should be recorded by an instrument thatprimarily records flow. Measuring PEF requires an instrumentthat has a flat frequency response (¡5%) up to 15 Hz [46].Although there is evidence of significant frequency content inPEF up to 20 Hz [47], it is recommended, at this stage, thatmanufacturers achieve a goal of recording fidelity up to 15 Hz.The PEF must be measured with an accuracy of ¡10%or ¡0.3 L?s-1 (20 L?min-1), whichever is the greater. Meaninstrument resistance measured across the range of theinstrument should be ,2.5 cmH2O?L-1?s-1 (0.25 kPa?L-1?s-1;table 6). PEF is sensitive to the resistance of the meter; forexample, a resistance of 0.25 kPa?L-1?s-1 decreases PEF by ,8%compared with PEF measured with a low-resistance pneumo-tachograph [48].
Intra-instrument repeatability must be ,5% or 0.150 L?s-1
(10 L?min-1), whichever is the greater. Inter-device reproduci-bility must be ,10% or 0.300 L?s-1 (20 L?min-1), whichever isthe greater. Calculating PEF by differentiating volume–timedata may introduce noise; hence, a parabolic-fitting algorithmmay be used [2] as a smoothing procedure.
Equipment validation is covered in the Test signals for PEFmeter testing section.
Test procedurePEF is dependent on effort and lung volume, with subjectcooperation being essential. PEF must be achieved as rapidlyas possible and at as high a lung volume as possible, in orderto obtain the maximum value [49]. The subject must beencouraged to blow as vigorously as possible. The neck shouldbe in a neutral position, not flexed or extended, and the subjectmust not cough. A nose clip is not necessary.
After the point of full lung inflation, the subject must deliverthe blow without any delay. Hesitating for as little as 2 s orflexing the neck allows the tracheal visco-elastic properties torelax and PEF to drop by as much as 10% [50]. Tonguing,spitting or coughing at the start of the blow may falsely raisethe recorded PEF in some devices.
In the laboratory, the subject must perform a minimum of threePEF manoeuvres. When PEF is a self-administered recording,it is important that the subject has been adequately taught howto perform the test, when to perform it and what action to takedepending on the resulting value obtained. Regular checks ofthe patient’s PEF technique and meter are an important part ofthe follow-up.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
330 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

Within-manoeuvre evaluationThe subject must be observed to ensure a good seal at themouth, no hesitation occurred, and there was no abnormalstart to the manoeuvre.
Between-manoeuvre evaluationThe PEF values and their order must be recorded so thatmanoeuvre-induced bronchospasm can be detected. If thelargest two out of three acceptable blows are not reproduciblewithin 0.67 L?s-1 (40 L?min-1), up to two additional blows canbe performed. Ninety-five per cent of untrained healthysubjects and patients can reproduce PEF to within 0.67 L?s-1
(40 L?min-1), and 90% to within 0.5 L?s-1 (30 L?min-1) [48]. Ifsatisfactory repeatability has not been in achieved in fiveattempts, more are not likely to be helpful [51].
Test result selectionThe largest value from at least three acceptable blows isrecorded.
MAXIMUM VOLUNTARY VENTILATIONThis test has been largely superseded by FEV1, which wasdefined as the index from a single maximum forced expiratorymanoeuvre that best correlated with maximum voluntaryventilation (MVV). If FEV1 is available, then MVV has littleadditional contribution to make in a clinical setting. However,it may be useful in those conditions where ventilatory capacitymay be impaired by mechanisms that are different from thoseaffecting FEV1 [26].
DefinitionThe MVV is the maximum volume of air a subject can breatheover a specified period of time (12 s for normal subjects). It isexpressed in L?min-1 at BTPS.
EquipmentA spirometer used for measuring MVV must have anamplitude–frequency response that is flat (¡10%) from zeroto o4 Hz, at flows of up to 12 L?s-1, over the volume range.The time for exhaled volume integration or recording must beno less than 12 s and no more than 15 s [52]. The indicated timemust be accurate to within ¡3%. The MVV must be measuredwith an accuracy of ¡10% of reading or ¡15 L?min-1,whichever is greater.
The evaluation of equipment is covered in the Test signals forMVV testing section.
Test procedureThe technician should provide proper instructions anddemonstrate the manoeuvre prior to the start of testing.The subject should be tested in the sitting position wearinga nose clip. After the subject makes an airtight seal aroundthe mouthpiece, at least three resting tidal breaths should beobtained, followed by breathing as rapidly and deeply aspossible. The tongue and teeth must be positioned so as tonot obstruct airflow. The technician should enthusiasticallycoach the subject throughout the manoeuvre, and may needto suggest faster or slower breathing to achieve an ideal rateof 90–110 breaths?min-1 [53, 54], although subjects withdisease may not always achieve this rate. The technicianwill need to carefully observe the subject with occasional
glances at the tracing to help the subject to obtain anacceptable manoeuvre. An acceptable manoeuvre should beperformed with maximal effort without evidence of leakage,hesitation or measurement artefact. The subject is instructedto breathe as deeply and rapidly as possible and the tidalvolume (VT) during the manoeuvre should be greater thanthe subject’s resting VT.
The test interval (e.g. 12 s) should be reported. A rest betweenmanoeuvres will improve subsequent efforts.
The MVV should be calculated from the sum of all individualexhalations, multiplied by the appropriate BTPS correctionfactor during the best 12 s of the manoeuvre. From a technicalstandpoint, changes in respiratory rate or VT during themanoeuvre will influence test results.
Within-manoeuvre evaluationIn normal subjects, the goal for an acceptable MVV should be aVT that is ,50% of the VC, with a breathing frequency that is,90 breaths?min-1 [54]. It is unlikely that an acceptablemanoeuvre will be obtained when the breathing frequency is,65 breaths?min-1 [54]. However, since there are little data onMVV acceptability criteria, no specific breathing frequency orvolume is required. The emphasis should be on maximal effortwith a goal of 90 breaths?min-1 and a volume representing,50% of the VC. VT during the manoeuvre is probably not asimportant as breathing frequency, since patients tend tobreathe on the portion of the expiratory curve where air isbest moved at a given frequency.
Between-manoeuvre evaluationThe subject should perform a minimum of two acceptablemanoeuvres. There are no clinical studies addressing repeat-ability; however, additional trials should be considered whenthe variability between acceptable manoeuvres exceeds 20%.
Test result selectionThe highest acceptable MVV (L?min-1 BTPS) and MVV rate(breaths?min-1) should be reported. An MVV/(406FEV1),0.80 indicates that the MVV is low relative to the FEV1,and suggests disease or poor effort. Volume versus timetracings from at least two acceptable manoeuvres should beretained and available for inspection.
TECHNICAL CONSIDERATIONSMinimal recommendations for spirometry systemsAccurate results require accurate equipment. Spirometer equip-ment recommendations apply to all spirometers and are minimalrequirements. In some circumstances, it may be appropriateto exceed these requirements (i.e. in some research/surveillance applications). Instrumentation recommendationsshould be followed to provide accurate spirometric data andinformation that is comparable from laboratory to laboratory andfrom one time period to another [1]. The accuracy of a spirometrysystem depends on characteristics of the entire system, from thevolume or flow transducer and the use of an in-line filter, tothe recorder, display or processor. Changes in any aspect ofthe equipment or errors at any step in the process can affect theaccuracy of the results. For example, if the BTPS correction factoris wrong, an accurately measured FVC will be incorrectlyreported.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 331

Spirometers and PEF meters are not required to measure all ofthe indices in table 6, but must meet the recommendations forthose that are measured. Accuracy and repeatability recom-mendations apply over the entire volume range of theinstrument.
BTPS correctionAll spirometry values should be reported at BTPS by anymethod (measuring temperature and barometric pressure)proven effective by the manufacturer. For volume-type spirom-eters, the temperature inside the spirometer should be mea-sured for each breathing manoeuvre. Regardless of the BTPScorrection technique used, the ambient temperature mustalways be recorded with an accuracy of ¡1 C. In situationswhere the ambient air temperature is changing rapidly (.3 C in,30 min), continuous temperature corrections may be neces-sary. Spirometer users should be aware of potential problemswith testing performed at lower ambient temperatures: 17 C isthe lower limit [55–63] for ambient temperature, unless amanufacturer states that their spirometer will operate accuratelyat lower ambient temperatures. If barometric pressure is notused in calculating the BTPS correction factor, the range ofbarometric pressures over which the BTPS correction factor isvalid must be published by the manufacturer.
CommentsThe rationale for this recommendation is based, in part, on theproblems with finite cooling times of gases in volume-typespirometers [55–57] and the problems of estimating BTPS
correction factors for flow devices [58–60]. When a subjectperforms an FVC manoeuvre, the air leaving the lungs is ,33–35 C [61, 62] and saturated with water vapour. If the expiredgas is assumed to be at BTPS, an error of ,1% will result. Mostvolume-type spirometers assume instantaneous cooling of theair as it enters the spirometer. This is not always the case, andFEVt can be incorrectly reported because of it. For capillaryand screen pneumotachometers, the signal depends on gasviscosity, which increases with increasing temperature.Therefore, for pneumotachometers, a different correction factoris needed for recording patients as compared with recordingfrom the calibrating syringe. Also, correction factors will bedifferent for inspiratory and expiratory manoeuvres. It isusually assumed that expired gas does not cool as it passesthrough the flow sensor. This may not be the case, particularlywith unheated flow sensors [58, 59]. The error will increase ifthe flow sensor is located further from the mouth and morecooling occurs, as is the case when a filter is placed in front ofthe flow sensor. Water condensation within or on the surfacesof a flow sensor may alter its calibration.
Depending on environmental temperature, the BTPS correctionfactor may be as large as 10%. The method used to calculate orestimate the BTPS factor can potentially introduce significanterrors; examples and a fuller explanation can be foundelsewhere [3, 4].
Changes in spirometer temperature can be a source ofvariability. Spirometer temperature should be measured andnot assumed to be constant, even over the course of one testing
TABLE 6 Range and accuracy recommendations specified for forced expiratory manoeuvres
Test Range/accuracy (BTPS) Flow range
L?s-1
Time s Resistance and
back pressure
Test signal
VC 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 30 3-L Calibration syringe
FVC 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 15 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
24 ATS waveforms,
3-L Cal Syringe
FEV1 0.5–8 L, ¡3% of reading or
¡0.050 L, whichever is greater
0–14 1 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
24 ATS waveforms
Time zero The time point from which
all FEVt measurements are taken
Back extrapolation
PEF Accuracy: ¡10% of reading or
¡0.30 L?s-1 (20 L?min-1), whichever is
greater; repeatability: ¡5% of reading
or ¡0.15 L?s-1 (10 L?min-1), whichever
is greater
0–14 Mean resistance at 200, 400,
600 L?min-1 (3.3, 6.7, 10 L?s-1)
must be ,2.5 cmH2O?L-1?s-1
(0.25 kPa?L-1?s-1)
26 ATS flow waveforms
Instantaneous
flows (except PEF)
Accuracy: ¡5% of reading or
¡0.200 L?s-1, whichever is greater
0–14 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
Data from manufacturers
FEF25–75% 7.0 L?s-1, ¡5% of reading or
¡0.200 L?s-1, whichever is greater
¡14 15 Same as FEV1 24 ATS waveforms
MVV 250 L?min-1 at VT of 2 L within
¡10% of reading or ¡15 L?min-1,
whichever is greater
¡14 (¡3%) 12–15 ,1.5 cmH2O?L-1?s-1
(0.15 kPa?L-1?s-1)
Sine wave pump
BTPS: body temperature and ambient pressure saturated with water vapour; VC: vital capacity; FVC: forced vital capacity; ATS: American Thoracic Society; FEV1: forced
expiratory volume in one second; FEVt: forced expiratory volume in t seconds; PEF: peak expiratory flow; FEF25–75%: mean forced expiratory flow between 25% and 75%
of FVC; MVV: maximum voluntary ventilation; VT: tidal volume.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
332 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

session. For volume spirometers, errors up to 6% in FEV1 andFVC can occur if ambient temperature is used instead ofinternal spirometer temperature [64]. For volume spirometers,the temperature inside the spirometer should be measured foreach breathing manoeuvre.
Test signals for spirometer testingThe diversity of FVC manoeuvres encountered in clinicalpractice is currently best simulated by the 24 standard volume–time waveforms developed by the ATS [3] and HANKINSON andGARDNER [65]. These waveforms can be used to drive acomputer-controlled mechanical syringe, or its equivalent, fortesting actual hardware and software [66, 67], or, when put in adigital form, they can evaluate only the software. Computer-controlled mechanical syringes (i.e. pump systems) used forvalidation should be accurate within ¡50 mL, which is 0.5% oftheir full range up to 10 L for FVC and FEV1. Pump systemsmay have accuracy values better than this for many profiles,but reproduce less accurately those test profiles with short DTsand RTs to peak flow [68, 69]. The ATS spirometry statement[3] shows the measured values for each of the 24 standardwaveforms. On request, the ATS can provide these waveformsin an electronic format. Appropriate corrections for using gasat the ambient temperature and humidity instead of BTPS mayneed to be made for some mechanical syringe–spirometercombinations.
MethodA production spirometer is connected to the pump system fortesting, orientated as it would be to test human subjects.Connecting tubing must be kept to the minimum (,0.300 L)and must not be distensible. If an in-line filter is required fortesting human subjects, one must be included when theinstrument is tested. Each of the 24 ATS waveforms isdischarged into the spirometer five times under ambientconditions, and all of the readings are recorded.
BTPS conditions are simulated by discharging waveforms 1–4to the spirometer three times, using air heated to 37¡1 C andat .98% relative humidity. The time between each of the threetests should be ,2 min.
Accuracy testThe average of the five tests under ambient conditions iscompared with the standard value in the following way:
Deviation~average{standard ð1Þ
Percentage deviation~100|(average{standard)=standard ð2Þ
The accuracy validation limits for volumes, which include the
waveform-generator inaccuracy, are ¡3.5% of reading or
¡0.100 L, whichever is greater. An accuracy error occurs if
the deviation (for volumes ,2.857 L) or percentage deviation
(for volumes .2.857 L) exceed these limits. These limits
include the allowable inaccuracy of the pump system.
Acceptable spirometer performance is defined as fewer thanthree accuracy errors for either FVC or FEV1 across the 24waveforms (,5% error rate).
The average FVC and FEV1 values of the three tests simulatingBTPS conditions are compared with the standard values. The
validation limits for these tests under BTPS conditions are¡4.5% or 0.200 L, whichever is the greater, and these limitsinclude the allowable inaccuracy for the pump system.
Acceptable spirometer performance under BTPS conditions isdefined as the accuracy requirement being met for all of thefour profiles used.
Repeatability testThe FEV1 and FVC data from the accuracy test are used toderive the span of the five recordings:
Span~maximum�minimum ð3Þ
Percentage span~100|span=average ð4Þ
The repeatability validation limits for the volume measured atambient conditions are ¡3.5% or ¡0.100 L, whichever isthe greater, and, for BTPS conditions, ¡4.5% or ¡0.200 L,whichever is the greater. A repeatability error occurs if thespan (for volumes ,2.857 L at ambient or 4.444 L at BTPS) orpercentage span (for volumes above this) exceeds these limits.
Acceptable spirometer performance for repeatability underambient conditions is defined as fewer than three accuracyerrors for either FVC or FEV1 across the 24 profiles (,5% errorrate). For BTPS conditions, the acceptable spirometer perfor-mance for repeatability is defined as the accuracy requirementbeing met for all of the four profiles.
Test signals for PEF meter testingThe 26 flow–time ATS waveforms were chosen to represent arange of PEF profiles suitable for delivery by mechanicalsyringe or pump systems to test PEF meters [3]. The range ofprofiles and method of delivery may need to be revised, asresearch on PEF measurement continues [45]. The mechanicalsyringe or suitable pump system used to validate PEFmeasuring equipment must have an accuracy of ¡2% indelivering PEF. Pump systems may have difficulty meetingthis accuracy standard for profiles more demanding than theset of 26 [68, 69]. Recent evidence suggests that the frequencycontent in the first second of the blow that contributes to PEF ishigher [47] than previously determined [70, 71]. The 26waveforms may not cover the range of RT and DT found in,25% of the client population [72], and, hence, moredemanding test profiles may be required in future [45].
MethodTwo randomly chosen production models of the flow metersshould each have the 26 waveforms delivered to them fivetimes under ambient conditions and the readings recorded.Any waveforms with a PEF outside the meter’s statedoperational range would not be included in the testingsequence. Appropriate correction factors for testing underambient conditions should be applied as recommended by themanufacturer.
Accuracy testThe average reading for each of the two meters is comparedwith the standard, as for volumes.
The accuracy validation limits are ¡12% or ¡25 L?min-1,whichever is the larger, and these limits include the 2%inaccuracy limit for the waveform generator. An accuracy error
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 333

for a given meter and given waveform occurs if the deviationand percentage deviation exceed these limits.
Acceptable performance is defined as fewer than threeaccuracy errors out of the total of 52 tests (26 waveforms,two meters).
Repeatability testFlow waveforms 1, 4, 8 and 25 are discharged three times toeach of 10 production meters. The repeatability validationlimits are ¡6% or ¡15 L?min-1, whichever is the greater, andthese limits include 1% for waveform-generator variability. Arepeatability error occurs if the span and percentage spanexceed these limits.
Acceptable performance is defined as six or fewer errors in the120 tests (i.e. maximum error rate of 5%).
Test signals for MVV testingA spirometry system used to measure MVV should be testedunder ambient conditions with a pump producing a sinusoidalwaveform, with stroke volumes up to 2 L using the fourpatterns of delivery previously specified [3]. Testing at BTPS isnot required, and each pattern is tested twice. The accuracyvalidation limits of the spirometer used for measuring MVVwith flows up to 250 L?min-1 are ¡10.5% of reading or¡20 L?min-1, whichever is greater. The pressure at themouthpiece must not exceed ¡10 cmH2O (1 kPa) at any pointduring MVV testing. These requirements apply to volumespirometers throughout their volume range.
Acceptable performance is defined as no errors in the eighttests (four patterns, twice).
ABBREVIATIONSTable 7 contains a list of abbreviations and their meanings,which will be used in this series of Task Force reports.
TABLE 7 List of abbreviations and meanings
ATPD Ambient temperature, ambient pressure, and dry
ATPS Ambient temperature and pressure saturated with water vapour
BTPS Body temperature (i.e. 37 C), ambient pressure, saturated with
water vapour
C Centigrade
CFC Chlorofluorocarbons
cm Centimetres
COHb Carboxyhaemoglobin
DL,CO Diffusing capacity for the lungs measured using carbon
monoxide, also known as transfer factor
DL,CO/VA Diffusing capacity for carbon monoxide per unit of alveolar
volume, also known as KCO
DM Membrane-diffusing capacity
DT Dwell time of flow .90% of PEF
EFL Expiratory flow limitation
ERV Expiratory reserve volume
EV Back extrapolated volume
EVC Expiratory vital capacity
FA,X Fraction of gas X in the alveolar gas
FA,X,t Alveolar fraction of gas X at time t
FEF25-75% Mean forced expiratory flow between 25% and 75% of FVC
FEFX% Instantaneous forced expiratory flow when X% of the FVC has
been expired
FEV1 Forced expiratory volume in one second
FEVt Forced expiratory volume in t seconds
FE,X Fraction of expired gas X
FIFX% Instantaneous forced inspiratory flow at the point where X% of the
FVC has been inspired
FI,X Fraction of inspired gas X
FIVC Forced inspiratory vital capacity
FRC Functional residual capacity
FVC Forced vital capacity
H2O Water
Hb Haemoglobin
Hg Mercury
Hz Hertz; cycles per second
IC Inspiratory capacity
IVC Inspiratory vital capacity
KCO Transfer coefficient of the lung (i.e.DL,CO/VA)
kg Kilograms
kPa Kilopascals
L Litres
L?min-1 Litres per minute
L?s-1 Litres per second
lb Pounds weight
MEFX% Maximal instantaneous forced expiratory flow where X% of the
FVC remains to be expired
MFVL Maximum flow–volume loop
mg Milligrams
MIF Maximal inspiratory flow
mL Millilitres
mm Millimetres
MMEF Maximum mid-expiratory flow
ms Milliseconds
MVV Maximum voluntary ventilation
PA,O2 Alveolar oxygen partial pressure
PB Barometric pressure
PEF Peak expiratory flow
PH2O Water vapour partial pressure
PI,O2 Inspired oxygen partial pressure
h (theta) Specific uptake of CO by the blood
RT Rise time from 10% to 90% of PEF
RV Residual volume
s Seconds
STPD Standard temperature (273 K, 0 C), pressure (101.3 kPa,
760 mmHg) and dry
TB Tuberculosis
TGV (or VTG) Thoracic gas volume
tI Time taken for inspiration
TLC Total lung capacity
Tr Tracer gas
ttot Total time of respiratory cycle
VA Alveolar volume
VA,eff Effective alveolar volume
VC Vital capacity
Vc Pulmonary capillary blood volume
VD Dead space volume
VI Inspired volume
VS Volume of the expired sample gas
mg Micrograms
TABLE 7 (Continued)
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
334 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

APPENDIXProposal for a standard data format for spirometryThis proposal would not preclude the use of other dataformats, but would require that a spirometer should at least beable to output data in the required format. The advantage of astandard format is the ease of moving data into datarepositories, such as quality control, healthcare and researchdatabases. It should simplify and reduce the cost of datatransfer when users change instrument models and manufac-turers. Easier transfer of data into healthcare databases has thepotential for improving the utility of lung function by makingmore complete data readily available to clinicians andhealthcare researchers. In research and clinical settings, astandard data format should simplify and reduce the cost oftransferring data into quality control software and couldcontribute to improved overall test quality. Finally, it is timefor this change; pulmonary function is one of the last medicalarenas without a standard data format.
Proposed formatThe spirometry data file will consist of an American StandardCode for Information Interchange, comma-delineated file withvariable length records. Comma-delineated text files are easilygenerated and are standard import formats for severaldatabase programs. Although some redundancies will exist,each record shall represent one curve and will be terminatedwith a carriage return and line feed. The ATS will distributeexamples of this data format from their web site.
Table 8 shows a list of parameters that must be included inevery record. If a parameter is unavailable, the space mustremain blank (‘‘,,’’). The flow–time data points must beprovided with a sampling interval of 0.01 s (100 samples?s-1)in mL?s-1. If necessary, interpolation or other techniques must
TABLE 8 List of parameters#
ID (patient identification)
Patient name
Data type (SP followed by E5expiratory or I5Inspiratory, followed by S5single
or B5best curve)
Barometric pressure (mmHg)
Temperature ( C) used in BTPS calculation
Relative humidity (%)
FVC quality attribute (A, B, C, D or F)
FEV1 quality attribute (A, B, C, D or F)
Effort attribute (A, B, C, D or F)
Interpretation code (see ATS interpretation scheme)
Deleted manoeuvre (Y or N)
Acceptable manoeuvre (Y or N)
Technician quality control code (A, B, C, D or F)
Computer quality code (A, B, C, D or F)
Plateau achieved (Y or N)
Review (N or R for ‘‘needs review’’ or ‘‘was reviewed’’)
Date of review (DD/MM/YYYY)
Reviewer initials
BTPS factor (x.xxx)
Spirometer manufacturer
Spirometer model
Spirometer serial number
Spirometer type
Testing facility name
City
State/region
Zip/post code
Country
Phone number
Calibration date (DD/MM/YYYY)
Calibration time (HH:MM)
Calibration result (P or F for ‘‘passed’’ or ‘‘failed’’)
Date (DD/MM/YYYY)
Time (HH:MM)
Technician ID (technician identification code or initials)
Manoeuvre number
Age (integer years)
Height (cm)
Weight (kg)
Sex (M or F)
Race (2-character race code)
Date of birth (DD/MM/YYYY)
Reference values source (first author surname and date of publication, e.g.
‘‘Knudson 1983’’)
Reference values correction factor (x.xx, 1.00 for no correction)
Testing position (standing, sitting or supine)
Test type (pre-, post-, bronchodilator, methacholine concentration or dose)
FVC (mL)
Extrapolated volume (mL)
FEV1 (mL)
FEV6 (mL)
PEF (mL?s-1)
FEF25–75% (mL?s-1)
VC (mL)
Forced expiratory time (s)
Time to PEF (ms)
Predicted FVC (mL)
Predicted FEV1 (mL)
Predicted FEV6 (mL)
Predicted FEV1/FVC% (xxx.x%)
Predicted FEV1/FEV6% (xxx.x%)
Comments text
Original sampling interval (ms)
Blank 1 or FEF25%
Blank 2 or FEF50%
Blank 3 or FEF75%
Blank 4 or FEF90%
Blank 5
Blank 6
Blank 7
Blank 8
Blank 9
Blank 10
Number of data points
Flow data points (mL?s-1; variable number contained in number of data points)
Carriage return
Line feed
#: All text type variables should be enclosed with double quotes (‘‘) to prevent
confusion with control or data separator type characteristics.
TABLE 8 (Continued)
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 335

ACKNOWLEDGEMENTSM.R. Miller: University Hospital Birmingham NHS Trust,Birmingham, UK; J. Hankinson: Hankinson Consulting, Inc.,Valdosta, GA, USA; V. Brusasco: Universita degli Studi diGenova, Genova, Italy; F. Burgos: Hospital Clinic Villarroel,Barcelona, Spain; R. Casaburi: Harbor UCLA MedicalCenter, Torrance, CA, USA; A. Coates: Hospital for SickChildren, Toronto, ON, Canada; R. Crapo and R. Jensen:LDS Hospital, Salt Lake City, UT, USA; P. Enright: 4460E Ina Rd, Tucson, AZ, USA; C.P.M. van der Grinten:University Hospital of Maastrict, Maastricht, theNetherlands; P. Gustafsson: Queen Silvias Children’sHospital, Goteborg, Sweden; D.C. Johnson: MassachusettsGeneral Hospital and Harvard Medical School, Boston, MA,USA; N. MacIntyre: Duke University Medical Center,Durham, NC, USA; R. McKay: Occupational Medicine,Cincinnati, OH, USA: D. Navajas: Universitat de Barcelona- IDIBAPS, Barcelona, Spain; O.F. Pedersen: University ofAarhus, Aarhus, Denmark; R. Pellegrino: AziendaOspedaliera S. Croce e Carle, Cuneo, Italy; G. Viegi: CNRInstitute of Clinical Physiology, Pisa, Italy; J. Wagner:Pharmaceutical Research Associates, Inc., Lenexa, KS, USA.
REFERENCES1 Renzetti AD Jr. Standardization of spirometry. Am Rev
Respir Dis 1979; 119: 831–838.2 American Thoracic Society. Standardization of spirometry:
1987 update. Am Rev Respir Dis 1987; 136: 1285–1298.3 American Thoracic Society. Standardization of spirometry,
1994 update. Am J Respir Crit Care Med 1995; 152:1107–1136.
4 Quanjer PH, ed. Standardized lung function testing.Report Working Party Standardization of Lung FunctionTests. European Community for Coal and Steel. Bull EurPhysiopathol Respir 1983; 19: Suppl. 5, 1–95.
5 Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF,Peslin R, Yernault J-C. Lung volume and forced ventilatoryflows. Report Working Party Standardization of LungFunction Tests, European Community for Steel and Coal.Official Statement of the European Respiratory Society. EurRespir J 1993; 6: Suppl. 16, 5–40.
6 Morgan KC. The assessment of ventilatory capacity(committee recommendations). Chest 1975; 67: 95–97.
7 Gardner RM, Crapo RO, Billings RG, Shigeoka JW,Hankinson JL. Spirometry: what paper speed? Chest 1983;84: 161–165.
8 Gardner RM, Clausen JL, Crapo RO, et al. Qualityassurance in pulmonary function laboratories. Am RevRespir Dis 1986; 134: 626–627.
9 Morris AH, Kanner RE, Crapo RO, Gardner RM. Clinicalpulmonary function testing: a manual of uniform labora-tory procedures. 2nd Edn. Salt Lake City, UT,Intermountain Thoracic Society, 1984.
10 Townsend MC. The effects of leaks in spirometers onmeasurement of pulmonary function. J Occup Med 1984; 26:835–841.
11 Association for the Advancement of MedicalInstrumentation, Standard for spirometers (draft),October 1980. AAMI Suite 602, 1901 N. Ft. Myer Drive,Arlington, VA 22209–1699.
12 D’Angelo E, Prandi E, Milic-Emili J. Dependence ofmaximal flow-volume curves on time course of precedinginspiration. J Appl Physiol 1993; 75: 1155–1159.
13 Stoller JK, Basheda S, Laskowski D, Goormastic M,McCarthy K. Trial of standard versus modified expirationto achieve end-of-test spirometry criteria. Am Rev RespirDis 1993; 148: 275–280.
14 Bucca CB, Carossa S, Colagrande P, et al. Effect ofedentulism on spirometric tests. Am J Respir Crit CareMed 2001; 163: 1018–1020.
15 Eigen H, Bieler H, Grant D, et al. Spirometric pulmonaryfunction in healthy preschool children. Am J Respir CritCare Med 2001; 163: 619–623.
16 Smith AA, Gaensler EA. Timing of forced expiratoryvolume in one second. Am Rev Respir Dis 1975; 112:882–885.
17 Horvath EP Jr, ed. Manual of spirometry in occupationalmedicine. Division of Training and ManpowerDevelopment, National Institutes for Occupational Safetyand Health. Cincinnati, NIOSH, 1981.
18 Hankinson JL, Gardner RM. Standard waveforms forspirometer testing. Am Rev Respir Dis 1982; 126: 362–364.
19 Aurora P, Stocks J, Oliver C, et al. Quality control forspirometry in preschoolchildren with and without lungdisease. Am J Crit Care Med 2004; 169: 1152–1159.
20 Desmond KJ, Allen PD, Demizio DL, Kovesi T, Coates AL.Redefining end of test (EOT) criteria for pulmonaryfunction testing in children. Am J Respir Crit Care Med1997; 156: 542–545.
21 Hankinson JL, Bang KM. Acceptability and reproducibilitycriteria of the American Thoracic Society as observed in asample of the general population. Am Rev Respir Dis 1991;143: 516–521.
22 Ferris BG Jr, Speizer FE, Bishop Y, Prang G, Weener J.Spirometry for an epidemiologic study: deriving optimumsummary statistics for each subject. Bull Eur PhysiopatholRespir 1978; 14: 146–166.
23 Kanner RE, Schenker MB, Munoz A, Speizer FE.Spirometry in children: methodology for obtaining optimalresults for clinical and epidemiological studies. Am RevRespir Dis 1983; 127: 720–724.
24 Swanney MP, Jensen RL, Crichton DA, Beckert LE,Cardno LA, Crapo RO. FEV(6) is an acceptable surrogatefor FVC in the spirometric diagnosis of airway obstructionand restriction. Am J Respir Crit Care Med 2000; 162:917–919.
25 Paoletti P, Pistelli G, Fazzi P, et al. Reference values forvital capacity and flow-volume curves from a generalpopulation study. Bull Eur Physiopathol Respir 1986; 22:451–459.
be used to provide the 0.01-s sampling interval. The recordlength will vary, depending on the number of data pointspresent in the flow–time portions of the record. The curve datamust include o0.25 s of data points prior to the onset of theinspiratory or expiratory manoeuvre.
Volume–time curves may be calculated by adding the flow–time values (mL?s-1) and multiplying the sum by 0.01 s. Toobtain the highest precision, the sum of the flow values shouldbe calculated for each volume data point before multiplying by0.01 s.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
336 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

26 Pellegrino R, Viegi G, Enright P, et al. Interpretativestrategies for lung function tests. Eur Respir J 2005 (Inpress).
27 Coates AL, Allen PD, MacNeish CF, Ho SL, Lands LC.Effect of size and disease on expected deposition of drugsadministered using jet nebulization in children with cysticfibrosis. Chest 2001; 119: 1123–1130.
28 Coates AL, Ho SL. Drug administration by jet nebulization.Pediatr Pulmonol 1998; 26: 412–423.
29 Newman SP, Clark AR, Talaee N, Clark SW. Pressurizedaerosol deposition in the human lung with and without an‘‘open’’ spacer device. Thorax 1989; 44: 706–710.
30 Tal A, Golan H, Grauer N, Aviram M, Albin D,Quastel MR. Deposition pattern of radiolabeled salbutamolinhaled from a meter-dose inhaler by means of a spacerwith mask in young children with airway obstruction. JPediatr 1996; 128: 479–484.
31 Newhouse MT. Asthma therapy with aerosols: arenebulizers obsolete? A continuing controversy. J Pediatr1999; 135: 5–8.
32 Coates AL, MacNeish CF, Lands LC, Meisner D,Kelemen S, Vadas EB. A comparison of the availability oftobramycin for inhalation from vented versus unventednebulizers. Chest 1998; 113: 951–956.
33 Devadason SG, Everard ML, Linto JM, LeSouef PN.Comparison of drug delivery form conventional versus‘‘Venturi’’ nebulizers. Eur Respir J 1997; 10: 2479–2483.
34 Leach CL, Davidson PJ, Hasselquist BE, Boudreau RJ.Lung deposition of hydofluoroalkane-134a beclometha-sone is greater than that of chlorofluorocarbon fluticasoneand chlorofluorocarbon beclomethasone: a cross-overstudy in healthy volunteers. Chest 2002; 122: 510–516.
35 Wildhaber JH, Devadason SG, Hayden MJ, Elber E,Summers QA, LeSouef PN. Aerosol delivery to wheezyinfants: a comparison between a nebulizer and two smallvolume spacers. Pediatr Pulmonol 1997; 23: 212–216.
36 Guidelines for the measurement of respiratory function.Recommendations of the British Thoracic Society and theAssociation of Respiratory Technicians and Physiologists.Respir Med 1994; 88: 165–194.
37 Babb TG, Viggiano R, Hurley B, Staats B, Rodarte JR. Effectof mild-to-moderate airflow limitation on exercise capa-city. J Appl Physiol 1991; 70: 223–230.
38 O’Donnell DE, Lam M, Webb KA. Spirometric correlates ofimprovement in exercise performance after cholinergictherapy in chronic obstructive pulmonary disease. Am JRespir Crit Care Med 1999; 160: 542–549.
39 Pellegrino R, Rodarte JR, Brusasco V. Assessing thereversibility of airway obstruction. Chest 1998; 114:1607–1612.
40 Pellegrino R, Brusasco V. Lung hyperinflation and flowlimitation in chronic airway obstruction. Eur Respir J 1997;10: 543–549.
41 Younes M, Kivinen G. Respiratory mechanics and breath-ing pattern during and following maximal exercise. J ApplPhysiol 1984; 57: 1773–1782.
42 Wanger J, Clausen JL, Coates A, Pedersen OF.Standardisation of the measurement of lung volumes.Eur Respir J 2005; (In press).
43 Brusasco V, Pellegrino R, Rodarte JR. Vital capacitiesduring acute and chronic bronchoconstriction: dependence
on flow and volume histories. Eur Respir J 1997; 10:1316–1320.
44 Hansen LM, Pedersen OF, Lyager S, Naerra N.[Differences in vital capacity due to the methodsemployed]. Ugerkr Laeger 1983; 145: 2752–2756.
45 Miller MR, Atkins P, Pedersen OF. Inadequate peakexpiratory flow meter characteristics detected by acomputerised explosive decompression device. Thorax2003; 58: 411–416.
46 Quanjer PH, Lebowitz MD, Gregg I, Miller MR,Pedersen OF. Peak expiratory flow: conclusions andrecommendations of the European Respiratory Society.Eur Respir J 1997; 10: Suppl. 24, 2s–8s.
47 Miller MR, Lloyd J, Bright P. Recording flow in the firstsecond of a maximal forced expiratory manoeuvre: influ-ence of frequency content. Eur Respir J 2002; 19: 530–533.
48 Pedersen OF, Rasmussen TR, Omland Ø, Sigsgaard T,Quanjer PH, Miller MR. Peak expiratory flow and theresistance of the mini-Wright peak flow meter. Eur Respir J1996; 9: 828–833.
49 Pedersen OF, Pedersen TF, Miller MR. Gas compression inlungs decreases peak expiratory flow depending onresistance of peak flow meter. J Appl Physiol 1997; 83:1517–1521.
50 Kano S, Burton DL, Lanteri CJ, Sly PD. Determination ofpeak expiratory flow. Eur Respir J 1993; 6: 1347–1352.
51 Ferris BG Jr, Speizer FE, Bishop Y, et al. Spirometry for anepidemiologic study: deriving optimum summary statis-tics for each subject. Bull Eur Physiopathol Respir 1978; 14:145–166.
52 Federal Register, 38:4265, Feb. 12, 1973, Section ofpulmonary function specifications. Washington, DC,United States Government Printing Office.
53 Bernstein L. The effect of the rate of breathing onmaximum breathing capacity determined with a newspirometer. Thorax 1952; 7: 255–262.
54 Miller WF, Johnson RL Jr, Wu N. Relationships betweenmaximal breathing capacity and timed expiratory capa-cities. J Appl Physiol 1959; 14: 510–516.
55 Hankinson JL, Viola JO. Dynamic BTPS correction factorsfor spirometric data. J Appl Physiol 1983; 44: 1354–1360.
56 Hankinson JL, Castellan RM, Kinsley KB, Keimig DG.Effects of spirometer temperature on FEV1 shift changes.J Occup Med 1986; 28: 1222–1225.
57 Pincock AC, Miller MR. The effect of temperature onrecording spirograms. Am Rev Respir Dis 1983; 128: 894–898.
58 Hankinson JL, Viola JO, Petsonk EL, Ebeling TR. BTPScorrection for ceramic flow sensors. Chest 1994; 105:1481–1486.
59 Miller MR, Pincock AC. Linearity and temperature controlof the Fleisch pneumotachograph. J Appl Physiol 1986; 60:710–715.
60 Perks WH, Sopwith T, Brown D, Jones CH, Green M.Effects of temperature on Vitalograph spirometer readings.Thorax 1983; 38: 592–594.
61 Cole P. Recordings of respiratory air temperature. JLaryngol 1954; 68: 295–307.
62 Madan I, Bright P, Miller MR. Expired air temperature atthe mouth during a maximal forced expiratory manoeuvre.Eur Respir J 1993; 6: 1556–1562.
M.R. MILLER ET AL. STANDARDISATION OF SPIROMETRY
cEUROPEAN RESPIRATORY JOURNAL VOLUME 26 NUMBER 2 337

63 Liese W, Warwick WJ, Cumming G. Water vapourpressure in expired air. Respiration 1974; 31: 252–261.
64 Johnson LR, Enright PL, Voelker HT, Tashkin DP. Volumespirometers need automated internal temperature sensors.Am J Respir Crit Care Med 1994; 150: 1575–1580.
65 Hankinson JL, Gardner RM. Standard waveforms forspirometer testing. Am Rev Respir Dis 1982; 126: 362–364.
66 Nelson SB, Gardner RM, Crapo RO, Jensen RL.Performance evaluation of contemporary spirometers.Chest 1990; 97: 288–297.
67 Gardner RM, Hankinson JL, West BJ. Evaluating commer-cially available spirometers. Am Rev Respir Dis 1986; 134:626–627.
68 Hankinson JL, Reynolds JS, Das MK, Viola JO. Method toproduce American Thoracic Society flow–time waveformsusing a mechanical pump. Eur Respir J 1997; 10: 690–694.
69 Miller MR, Jones B, Xu Y, Pedersen OF, Quanjer PH. Peakexpiratory flow profiles delivered by pump systems:limitations due to wave action. Am J Respir Crit Care Med2000; 162: 1887–1896.
70 Peslin R, Jardin P, Bohadana A, Hannhart B. Contenuharmonique du signal de debit pendant l’expiration forceechez l’homme normal [Harmonic content of the flow signalduring forced expiration in normal man]. Bull EurPhysiopath Respir 1982; 18: 491–500.
71 McCall CB, Hyatt RE, Noble FW, Fry DL. Harmoniccontent of certain respiratory flow phenomena of normalindividuals. J Appl Physiol 1957; 10: 215–218.
72 Miller MR, Pedersen OF, Quanjer PH. The rise and dwelltime for peak expiratory flow in patients with and withoutairflow limitation. Am J Respir Crit Care Med 1998; 158:23–27.
STANDARDISATION OF SPIROMETRY M.R. MILLER ET AL.
338 VOLUME 26 NUMBER 2 EUROPEAN RESPIRATORY JOURNAL

COPYRIGHT PULSUS GROUP INC. – DO NOT COPY
Can Respir J Vol 20 No 1 January/February 2013 13
Spirometry in primary careAllan L Coates MD1, Brian L Graham PhD2, Robin G McFadden MD3, Colm McParland MD4,
Dilshad Moosa BSc RRT CRE MASc(c)5, Steeve Provencher MD MSc6, Jeremy Road MD7
1Division of Respiratory Medicine, The Hospital for Sick Children, Toronto, Ontario; 2Division of Respirology, Critical Care and Sleep Medicine, University of Saskatchewan, Saskatoon, Saskatchewan; 3Division of Respirology, Department of Medicine, University of Western Ontario, London, Ontario; 4Division of Respirology, Dalhousie University, Halifax, Nova Scotia; 5Provider Education Program, Ontario Lung Association, Toronto, Ontario; 6Centre de recherche de l’Institut Universitaire de cardiologie et de pneumologie de Québec, Service de Pneumologie, Québec, Quebec; 7Respiratory Division, University of British Columbia, Vancouver, British Columbia
Correspndence and reprints: Dr Allan L Coates, Canadian Thoracic Society, 300-1750 Courtwood Crescent, Ottawa, Ontario K2C 2B5. Telephone 613-569-6411, fax 613-569-8860, e-mail [email protected]
Position statement develoPment ProcessThe present position statement was developed by the CTS Pulmonary Function Standards Committee, comprised of experts with experience in the development of international spirometry guidelines, the use of spirometry in asthma and COPD, the training of individuals to con-duct quality spirometry, the training of physicians and nurse practi-tioners to interpret spirometry, the development of normal values for spirometry and the evaluation of spirometers. The position statement reflects the key issues found in spirometry training in primary care and interpretation of spirometry testing conducted in primary care.
consensus processThe present position statement is based on the joint standards for lung function testing by the American Thoracic Society (ATS) and the European Respiratory Society (ERS) published in 2005 (1,2). Where there may be either controversial issues or changes based on new data, these are indicated.
The recommendations were agreed on by consensus from the full committee through extensive discussions, review of the evidence, and review of existing guidelines and accreditation standards.
Who can conduct spirometrySpirometry is not controlled under medical services regulations and, there-fore, there are no legal restrictions on who can perform spirometry testing.
Provincial accreditation guidelines are variable across the country.British Columbia, Alberta and Ontario have guidelines that specify that a suitably trained and qualified “Medical Director” or “Quality Advisor” oversee spirometry testing.
Because spirometry requires the very active participation of the patient, the technologist must have the skills and ability to proceed well beyond the usual level of patient interaction in medical tests and should have basic life-support training. Spirometry testing can be con-ducted by the following:
1. Trained health care personnel who are registered respiratory therapists (RRT) or registered cardiopulmonary function technologists (RCPT[P]);
2. Other health care professionals whose formal training included studies in the anatomy and physiology of the cardiorespiratory system, and who subsequently successfully completed a recognized spirometry training course; and
3. Other trained health care technologists who subsequently successfully completed a recognized spirometry training course.For all of the above, an additional requirement is one month of
supervised training in the performance and quality control of spirom-etry testing (3).
Key message:Spirometry should be conducted by trained and qualified personnel in a setting with a regular quality assurance program.
Training courses for conducting quality spirometry testing are available; including the CTS-endorsed SpiroTrec®course which is offered by RESPTrec® (www.resptrec.org). SpiroTrec© teaches individuals how to conduct quality spirometry including know-ledge of spirometers, understanding of the ATS/ERS standards for spirometry, quality control, patient instruction and basic inter-pretation of the results. This course includes 16 h of preworkshop learning and assignments, an 8 h workshop and a subsequent qual-ity assurance review of five to 10 spirometry tests per month for three months.
A recent study (4) found that asthma educators who enrolled in a 4 h course in conducting spirometry were able to meet ATS/ERS spi-rometry testing standards (2) 77% of the time. Short-term follow-up and supplementary training is important to maintain the quality of spirometry testing (5).
Special article
©2013 Pulsus Group Inc. All rights reserved
al coates, Bl Graham, rG mcFadden, et al. spirometry in primary care. can respir J 2013;20(1):13-22.
Canadian Thoracic Society (CTS) clinical guidelines for asthma and chronic obstructive pulmonary disease (COPD) specify that spirome-try should be used to diagnose these diseases. Given the burden of asthma and COPD, most people with these diseases will be diagnosed in the primary care setting. The present CTS position statement was developed to provide guidance on key factors affecting the quality of spirometry testing in the primary care setting. The present statement may also be used to inform and guide the accreditation process for spirometry in each province.
Although many of the principles discussed are equally applicable to pulmonary function laboratories and interpretation of tests by respirol-ogists, they are held to a higher standard and are outside the scope of the present statement.
Key Words: Primary care; Pulmonary function; Quality control; Reference values; Spirometry
la spirométrie en première ligne
Dans les lignes directrices cliniques sur l’asthme et la maladie pulmo-naire obstructive chronique (MPOC) de la Société canadienne de thoracologie (SCT), il est précisé que la spirométrie devrait être utili-sée pour diagnostiquer trois maladies. Étant donné le fardeau de l’asthme et de la MPOC, la plupart des personnes atteintes de ces maladies seront diagnostiquées en première ligne. Le présent docu-ment de principes de la SCT vise à fournir des directives sur les princi-paux facteurs qui touchent la qualité de la spirométrie en première ligne. Il peut également être utilisé pour étayer et orienter le processus d’agrément de la spirométrie dans chaque province.
Même si bon nombre des principes abordés peuvent s’appliquer aux laboratoires d’évaluation de la fonction pulmonaire et à l’interprétation des tests par des pneumologues, ceux-ci doivent respecter des normes plus élevées qui dépassent la portée du présent document.

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYCoates et al
Can Respir J Vol 20 No 1 January/February 201314
Who can interpret spirometryUnfortunately, some provincial legislation and regulations permit physicians and, in some jurisdictions, nurse practitioners, to interpret spirometry with no special qualifications. While they will have had training in the respiratory system, many primary care physicians have little specific training in the interpretation of spirometry data. There
are spirometry interpretation courses available both through work-shops and on-line training (eg, the Ontario Lung Association Provider Education Program [www.olapep.ca/spirometry]).
Key messages:Primary care physicians and nurse practitioners who interpret spi-rometry should have completed a spirometry interpretation course or specific training in spirometry interpretation.
Patient conditions and testinG environment
indications and contraindicationsSpirometry is performed to objectively assess individuals’ pulmonary function. It enables measuring the effect of a disease on lung function, monitoring its course or the result of therapeutic interventions, assess-ing preoperative risk and prognosticating many pulmonary conditions. Conversely, spirometry may be contraindicated (6). International guidelines regarding contraindications for lung function tests have been proposed; however, their evidence base is generally founded only on expert opinion (1). Moreover, recent developments in patient management, surgical practice and technology have decreased the invasive nature of procedures; therefore, some of the contraindications may no longer be justified. Additionally, patients with contraindica-tions that would prevent testing in the primary care setting can be tested in a pulmonary function laboratory where there is access to resuscitation personnel and equipment.
Potential risks associated with lung function testing primarily relate to the following: maximal pressures generated in the thorax and their impact on abdominal and thoracic organs; venous return and systemic blood pressure; expansion of the chest wall and lung; and active com-municable diseases that pose a risk to staff and other patients (eg, tuber-culosis). Spirometry and other forced expiratory manoeuvres will result in increased intrathoracic, intra-abdominal and intracranial pressures (7). Performing lung function tests can also be physically demanding for patients, thus increasing myocardial demand. This calls for prudence in patients with medical conditions that could be adversely affected by these physiological consequences (Table 1). Although there is no large-scale registry documenting the incidence of adverse events following pulmonary function testing, such risks are likely to be minimal in most patients. Importantly, the potential risks associated with testing should always be weighed against the benefit of obtaining information about lung function (6). When a spirometry test is unlikely to be of real clin-ical benefit to a compromised patient, it should be postponed until the patient has recovered from surgery, an infection or, for example, pneumothorax, hypo- or hypertension, or unstable arrhythmias. Conversely, a dogmatic approach of refusal to test patients with any contraindication must be tempered. For cases in which the benefit of obtaining objective measures of lung function may outweigh the risk of testing, referral to a specialist should be considered.
Although pre- and postbronchodilator spirometry testing is com-mon for an initial visit, subsequent testing may not require postbron-chodilator testing, depending on the reason for ordering spirometry. Some clinics may routinely conduct pre- and postbronchodilator testing to improve office efficiency and convenience for the patient (two tests in one session instead of two sessions) unless otherwise indicated.
Patient preparationContraindications should be listed on the spirometry requisition or checklist form. The requisition should clearly state the reason for requesting spirometry and include comments or questions by the refer-ring physician or nurse practitioner. Spirometry may give rise to stress incontinence; therefore, appropriate precautions should be taken (see a sample form in Appendix A).
Testing should occur in a bright and comfortable environment. The patient should be seated. A chair with arms (to prevent falling sideways should syncope occur), without wheels and that can be adjusted so that the feet are flat on the floor is recommended.
Table 1Relative contraindications for spirometryRelative contraindications Mechanisms CommentsCerebral aneurysmRecent brain surgeryRecent concussionRecent eye surgerySignificant glaucoma
Increases in intracranial/ intraocular pressure due to decreased venous return
Increases in intraocular pressure during weightlifting (5) suggest spirometry testing may lead to clinically significant changes in intraocular pressures in most patients.
Most experts suggest a three- to six-week recovery period following surgery before spirometry testing
Recent sinus surgery or middle ear surgery or infection
Increases in sinus and middle ear pressures
There is a risk that forced manoeuvres cause excessive pain or even ear drum rupture in cases of middle ear infection
PneumothoraxSignificant aortic
aneurysm*Recent thoracic surgery†
Recent abdominal surgery
Pregnancy‡
Increases in intrathoracic and intra-abdominal pressure
*Increases in intrathoracic or intra-abdominal pressures may increase blood pressure, but are not expected to increase aortic transmural pressure.
†Postoperative physiotherapy including coughing is actually believed to be beneficial after cardiothoracic and abdominal surgery. Cough generally increases intrathoracic pressures up to 400 cmH2O, compared with 70 cmH2O – 200 cmH2O during spirometry. The risk is likely low in most patients
‡Lung function tests may increase the risk of early delivery in case of cervical incompetence
Systemic hypotension or severe hypertension (eg, >200/120 mmHg)
Significant atrial/ventricular arrhythmia
Noncompensated heart failure
Recent myocardial infarction§ or pulmonary embolus
History of syncope related to forced exhalation/cough
Increases in myocardial demand or changes in blood pressure
§Exercise testing one week after myocardial infarction appears to be safe. A shorter period could be appropriate following reperfusion therapy (eg, angioplasty), whereas caution is necessary in case of persistent myocardial ischemia
Prudence is also called in many of these conditions with the use of ß2-sympathomimetics, although the risk of a single administration is likely to be minimal
Active tuberculosisHepatitis BHemoptysis or oral
bleeding
Infection control issues
General infection control measures should be adopted in accordance to local procedures
Inability to follow directions (eg, confusion, dementia, young age, language barrier)
In some cases, successful spirometry can be obtained with increased coaching and aid of an interpreter

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYSpirometry in primary care
Can Respir J Vol 20 No 1 January/February 2013 15
explanations: Spirometry requires cooperation between the subject and the examiner; the results obtained will depend on technical and personal factors. The test should be fully explained to the patient, and delaying the test should be strongly considered in case of transient confusion or absence of cooperation (1). Videos that demonstrate the test procedure to help educate the patient are available from The Lung Association (www.youtube.com/watch?v=--7ORNHWVrY).
Details of smoking history and any recent illness that could influ-ence the results should be recorded. Ideally, patients should avoid heavy exercise within 30 min, large meals within 2 h, alcohol con-sumption within 4 h and smoking within 1 h of testing (1).medications: The technologist should record the name, dosage and the last administration of any medication that may alter lung func-tion. The decision to avoid bronchodilators before testing is depend-ent on the reason for the test. If the study is performed to diagnose an underlying lung condition, then avoiding bronchodilators is use-ful. In this case, short-acting inhaled drugs should not be used within 4 h of testing, whereas long-acting bronchodilators should be stopped for longer periods (eg, 12 h for salmeterol and formoterol, 24 h for tiotropium, indacaterol and montelukast). Conversely, if the test is performed to determine a response to an existing therapeutic regi-men, then the referring physician may choose not to withhold bron-chodilator medications. The requisition form or checklist should state whether the patient should withhold medications before the test, and, if so, precisely which medications should be withheld and for how long.anthropometric measures: Before testing, it is essential that height be measured accurately because height, ethnicity, age and sex deter-mine the spirometry reference values. To properly measure height, the subject must be standing without shoes with his/her back flush against a hard surface, such as a wall, with a measuring tape attached to the wall with a right angle device making contact with top of the head and the tape. Ideally, this is accomplished with a proper stadiometer (8). The use of measuring devices attached to scales is inappropriate because it is exceedingly difficult to ensure that the back is held straight. In the presence of chest wall deformities or when height can-not be measured, arm span (middle finger tip to middle finger tip) can be used as an approximation of height (9).
Key messages:•Achecklistincludingallrelativecontraindicationsshouldbecom-
pleted before testing•Inthecaseofacontraindication,theriskandbenefitofthetest
should be weighed by the treating physician or the medical director of the laboratory, and testing should be referred to a laboratory where emergency facilities are available.
•Appropriate explanations and coaching aremandatory toobtainreliable pulmonary function tests. Precise anthropometric measure-ments are mandatory for determining reference values.
•Infectioncontrolprogramsshouldbefollowed.
sPirometer selection considerationsAlthough some older spirometer systems use volume measurement devices, whereby all of the air that the patient exhales is collected in an expandable chamber, almost all spirometers used in physician office settings (and many pulmonary function laboratories) measure air flow and calculate the volume from this signal. Only flow measurement devices are considered here. Other guidelines to assist in spirometer selection are available (10,11).
ats/ers standardsThe ATS/ERS Standardisation of Spirometry document (2) contains technical specifications for spirometers. All spirometers must meet the most current ATS/ERS standards, which at time of writing is the 2005 edition. Some spirometers are advertised as meeting ATS standards; how-ever, the fine print will say state ‘meets ATS 1994 Standards’.
exhalation-only versus full flow-volume loopsSome less expensive spirometers are designed for exhalation-only use. The patient inhales to maximal lung volume; then, while holding his/her breath, inserts the mouthpiece between the teeth, seals his/her lips around the mouthpiece and then forcibly exhales into the spirometer. This requires more coordination on the part of the patient and increases difficulty for the technologist conducting spirometry to assess test quality. Any leakage that occurs after the patient reaches maximal lung volume and before the mouthpiece is in place is lost and, there-fore, not included in the calculation of forced vital capacity (FVC) or the back-extrapolated volume. Furthermore, some exhalation-only models are not equipped with real-time displays that permit proper coaching to obtain a best effort. The use of such spirometers is not recommended.
Select a spirometer that enables the patient to take tidal breaths while the technologist can observe that the mouthpiece and nose clip are functioning properly. The technologist then has better control of the manoeuvre and can better coach patients to reach maximal lung volume. Additionally, if any leakage is observed at maximal lung vol-ume before the start of forced exhalation, it will be measured by the spirometer and used to determine whether it is within ATS/ERS stan-dards for the back-extrapolated lung volume. Furthermore, the time spent at total lung capacity can be assessed to determine whether there is a pause at end inspiration and, if >1 s, the manoeuvre can be repeated (12).
displayThe spirometer display, whether using a built-in screen or via a con-nection to a computer screen, must show both the flow-volume loop and the volume-time graph with sufficient resolution for the technolo-gist to distinguish whether end-of-test criteria are met, whether the shape of the flow volume curve is consistent with a maximal exhala-tion, and whether a cough or other artefact occurred in the first 1 s of exhalation. In most instances, the display will appear on a computer screen that is not supplied with the system. Most spirometers will have a USB cable to connect to a computer. Ensure that computer hardware and software are compatible with the spirometry system.
It must be possible to position the display so that the technologist can observe both the display and the patient simultaneously during the manoeuvres. This allows for instant coaching and also enables the technologist to terminate a poor effort early, rather than to push the patient to continue a tiring forced expiration.Warning messages and suggested corrections: The spirometer must analyze each manoeuvre to determine whether ATS/ERS require-ments were met and provide warning messages for any condition that is not met. Examples include “false start – don’t hesitate” and “end of test criteria not met – blow out longer”. The spirometer must also analyze the set of manoeuvres to determine whether ATS/ERS repeat-ability criteria are met. Some systems offer real-time messages to indi-cate when 6 s of exhalation has been achieved, which can aid the technologist in coaching to achieve a good quality test. Most of the ATS/ERS requirements are based on adults rather than children, and many children can meet these requirements with submaximal efforts and poor quality tests. A good technologist recognizes this and repeats the effort even if the computerized system has accepted the test.
calibrationA calibrating syringe is a required accessory for spirometers. ATS/ERS standards specify that a 3 L calibrating syringe be used for checking and calibrating the spirometer and additional specify accuracy requirements, including scheduled accuracy checks of the syringe. If filters are used for patient testing, calibration must be performed with a filter inline. Simple leak tests should be conducted monthly using a stopper in the syringe and checking for changes in syringe volume with pushing or pulling excursions. It may be necessary to purchase a special adaptor to connect the calibration syringe to your spirometer. Some calibrating syringes fit directly onto a disposable mouthpiece or filter.

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYCoates et al
Can Respir J Vol 20 No 1 January/February 201316
Some spirometers are equipped with precalibrated disposable breathing-tube inserts that cannot be calibrated by the user. Spirometers using such precalibrated inserts must still be checked daily for accuracy use a 3 L calibrating syringe.
Some spirometers require environmental information such as room temperature, barometric pressure and/or altitude. If so, these parameters should be measured, not estimated. If a barometer is not available, pres-sure reported from a nearby weather station (refer to the Environment Canada website) must be corrected for altitude (table available at www.engineeringtoolbox.com/air-altitude-pressure-d_462.html).normal reference values: To determine appropriate sets of reference values, refer to the following section in the present document. Select a spirometer that has these specific sets of normal reference values, both adult and pediatric, preprogrammed into its software. If these reference value sets are not included in the defaults provided by the spirometer, insist that they be installed before purchase.
reportsThe spirometry system must be capable of producing a report as described in the next section of the present document. When selecting a spirometer, consider whether it is compatible with the electronic medical record (EMR) system used in the facility. Some systems will permit customized EMR reports, other require reports to be printed to a portable document format (ie, PDF) file for attachment to an EMR.
disposablesIn the selection process, consider the cost and availability of mouth-pieces, which usually incorporate a filter. Some models have different mouthpieces for adult and pediatric use. Some models have a mouth-piece incorporated into a disposable breathing tube, making a filter unnecessary. Although filters are not required by ATS/ERS standards, many health regions specify their use for infection control. Nose clips are recommended whenever conducting spirometry.
robustnessThe spirometer must be sufficiently robust to be unaffected by inci-dental bumps or drops. If the spirometer has been dropped or jarred significantly, a calibration check is recommended before continuing the test.
technical supportThe vendor from whom the spirometer is purchased should provide initial training on the use of the spirometer. It should also provide tech-nical support for addressing problems with the operation of the spirom-eter. Request a ‘loaner’ device in the event that the spirometer needs to be returned to the company for servicing. There should be regular noti-fication of software upgrades or patches to fix problems. The spirometer should be thoroughly checked following any updates to the software.
Key messages:
•Agoodqualityspirometerisessentialforreliableresults.
•ATS/ERStechnicalspecificationsmustbemet.•Chooseaspirometerthatcandisplaylargescreenflow-volumeand
volume-time graphs in real time.•ThesoftwaremustbeabletocheckforATS/ERSacceptabilityand
repeatability criteria and provide appropriate warning messages.
PrinciPles For routine sPirometry rePortsA sample spirometry report form is provided in Appendix B, which is based on the following principles:1. Report on a minimal set of variables. Do not clutter the report
with several extraneous variables.2. Patient identification should include name, date of birth and
institutional identification number.3. Report observed values in the first column following the variable
name. Avoid reporting reference values that can be confused with observed values and do not add any additional information.
4. Height should be reported in cm. Weight should be reported in kg to one decimal place.
5. Report the lower limit of normal (LLN). Per cent of reference values are reported because they are used to determine the degree of obstruction.
6. Report ratios as a decimal fraction so they are not confused with per cent of a reference value.
7. Print flow-volume and volume-time graphs with a sufficient size and scale them to make optimal use of the available plot area while maintaining the proper aspect ratio. For volume-time graphs, show the last second before start of maximal exhalation. Including all manoeuvres in the session rather than only the best pre- and post-curve is optional.
8. Include the source of the reference values on the report. If the age of the patient is outside of the age range for which the reference values were developed, flag the LLN values.
9. Report ethnicity and flag LLN values if the ethnicity does not match the reference value data set. Do not adjust the observed values or LLN for ethnicity by an arbitrary percentage.
10. Report the reason for the test.11. Report technologist comments, which include an assessment of
the quality of the spirometry session
order of columns1. Variable name with measurement units
Prebronchodilator2. Observed value (using ATS/ERS selection criteria)3. Lower limit of normal4. Per cent of reference value
Postbronchodilator5. Observed value6. Percent of reference value7. Volume change from prebronchodilator8. Per cent change from prebronchodilator (the latter two are
reported because a change ≥200 mL and ≥12% is required for a response to bronchodilators to be significant (2), although lower absolute volume change is acceptable for children or subjects with small lung volumes)
Spirometry variables to reportVariable UnitsForced vital capacity (FVC) LForced expiratory volume in first 1 s (FEV1) LRatio of FEV1 to FVC (FEV1/FVC) –Peak expiratory flow (PEF) L/sForced expiratory time (FET) s
optional variables: The forced expiratory flow from 25% to 75% of exhalation (FEF25-75) is only recommended for children (13,14) and is used in settings primarily designed for children. Interpretation of FEF25-75 requires experience with its high degree of variability and its dependence on FVC.
Although not recommended for office spirometry, some advanced laboratories may report other indexes, particularly the ratio of inspira-tory to expiratory flows at 50% vital capacity when upper airway obstruction is suspected.
GraphsAt a minimum, the best pre- and postbronchodilator tests should be displayed. The best manoeuvre is the one with the highest sum of FVC and FEV1. The individual graphs should be distinguishable by colour or line type (solid versus dashed), or by displacement along the x-axis. There should be an option to plot all acceptable manoeuvres for each of

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYSpirometry in primary care
Can Respir J Vol 20 No 1 January/February 2013 17
pre- and postbronchodilator tests and manoeuvres not meeting ATS/ERS criteria that the technologist has marked as acceptable or useable.Flow-volume graph: The graph must be present and must show both the expiratory and inspiratory limbs of the manoeuvre. The aspect ratio is such that 2 L/s on the flow axis equals 1 L on the volume axis. The graph should be scaled so that the maximum values are appropriate to the patient and the size of the graph must be adequate to show the detail of the flow-volume curve (eg, a fixed size of 16 L/s by 8 L is not acceptable).volume-time graph: The graph must be present and must show the final 1 s of inhalation before the forced exhalation. The aspect ratio may be changed to accommodate lengthy expiratory times. The graph should be scaled so that the maximum values are appropriate to the patient and the size of the graph must be adequate to show the detail of the curve (eg, a fixed volume axis of 8 L is not acceptable).standard deviation graph (recommended): The Global Lung Function Initiative (GLI) (15) suggests a visual plot of variables on a standard deviation (SD) scale, showing the reference value and the LLN (1.64 SDs below the mean value), which gives the interpreter a better sense of how the measured values compare with the normal range (see Figure 1 and Appendix B for examples).
technologist’s commentsThe technologist’s comments provide information about the testing session that may affect the interpretation. Recent use of bronchodila-tors should be noted (drug, dose and time taken). The comments should include any deviation from the standardized ATS/ERS proced-ures. If the technologist believed that he/she was unable to obtain a maximal effort, it should be noted with an explanation of the problem. If the testing session was terminated prematurely, the reason for the termination should be provided. The number of acceptable and repro-ducible manoeuvres should be given.
On occasion, the technologist may override the computer software, which automatically classifies a manoeuvre as acceptable or unaccept-able. For example, in cases where the technologist ends the expiratory phase of a manoeuvre after the preset limit (usually 12 s to 15 s), the technologist may reclassify it as acceptable. In such cases, the tech-nologist should note that while the ATS/ERS end-of-test criterion was not met, the exhalation was terminated after 12 s and the test was deemed acceptable, which is often the case in COPD.
If the spirometry system does not follow current ATS/ERS guide-lines, this information should be included in the comments. This will impact the application of the acceptability criteria because items, such as the back extrapolated volume, may not be measured.
test quality grading (optional)While various authors have recommended spirometry grading, such as the scholastic grading system (A, B, C, D and F [16]), there is no ATS or ERS standard. Furthermore, there is no uniform agreement regarding whether the grading is performed for each manoeuvre as a whole, or for the FEV1 and FVC separately (17). Some manufacturers have implemented one or other of the proposed systems. In general, A indicates that ATS/ERS standards were exceeded; B that standards were met; C and D that the data are useable but fall short of ATS/ERS standards (eg, only two acceptable manoeuvres but they are repeat-able); and F that the test is not useable for interpretation. These can be used as a guide for technologist comments, but should not be used as a substitute for technologist comments. If the spirometry grade is included in the report, it is important for both the technologist and the interpreter to be familiar with the particular grading system that is being used by the spirometry software.note: Grading systems were developed to determine which manoeuvres should be used in studies designed using healthy subjects to obtain nor-mal reference values for spirometry. Patients with COPD can usually meet all criteria except for the end-of-test criteria. If a patient has met all other criteria but has exhaled for 12 s to 15 s and still failed to reach a plateau (<25 mL in the final 1 s of exhalation), then the technologist should indicate that the test is acceptable in spite of a grade less than B.
Key message:The report form must be designed to provide all required information without extraneous values in a format that is easily understood with graphic data to support the numerical data.
reFerence valuesThe expected lung volume is most affected by height – the taller the individual, the larger the lung volume. The variation of lung volume with age is more complex. Lung volume increases as the lungs grow from birth to 18 to 20 years of age in females, and 20 to 24 years of age in males. Thereafter, lung volume declines with age because the lungs lose elastic recoil with reduced expiratory flows (18). Adult males have higher lung volumes than adult females of the same age and height. African Americans have lung volumes approximately 10% lower than Caucasians. Asians have lung volumes 2% to 8% lower than Caucasians (15).
Reference values for FEV1, FVC and FEV1/FVC are generated from population studies of healthy, asymptomatic individuals. For most biological measurements, the standard assumption is that for data with a normal distribution, values within 2 SDs of the mean value represent 95% of the population and are considered to be normal. This implies that 5% of the population (2.5% above and 2.5% below 2 SDs) are ‘abnormal’. For spirometry variables, values that are higher than the reference value are not considered to be abnormal. The LLN is defined as the 5th percentile (ie, the value that marks the lower 5% of the normal population). In a normal distribution, LLN is 1.64 SDs below the mean value (Figure 2) (19). Clearly, when using the LLN, 5% of the healthy, asymptomatic population will be classified as below nor-mal. On the other hand, some people with lung disease will have val-ues greater than LLN and will be classified as normal. The SDs graph on the report form helps to determine the likelihood and degree of abnormality (Figure 1). However, spirometry results are but one find-ing and must be considered in the context of history, symptoms and physical findings to make the diagnosis.
While some studies have produced reference values for adults and others for children, it is recommended that a continuous set of refer-ence values that applies to all ages be used. Errors often arise when trying to extrapolate reference values developed for adults to the ado-lescent range, or when trying to extrapolate children’s values above 18 or below the age range of the reference equations. The GLI recom-mends the all-age spirometry values developed by Quanjer et al (15),
Pre-Bronchodilator Post-Bronchodilator Spirometry Best LLN %Ref Best %Ref Change %Chg FVC (L) 3.01 3.04 75% 3.42 86% 410 mL 13% FEV1 (L) 1.34 2.36 44% 1.77 57% 430 mL 32% FEV1/FVC 0.45 0.66 0.52 Reference values: Quanjer 2012 [Caucasian]
Figure 1) Standard deviation graph. This graph helps to visualize where the measured values lie in relation to the reference values and the lower limit of normal (LLN). Chg Change; FEV1 Forced expiratory volume in 1 s; FVC Forced expiratory volume; Ref Reference

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYCoates et al
Can Respir J Vol 20 No 1 January/February 201318
which are a composite of spirometry measures worldwide. These refer-ence values are divided into Caucasians, African Americans, Southeast Asians and Northeast Asians.
Some spirometry systems have implemented the reference values from Stanojevic et al (20 [2008]) for ages six to 70 years. The Quanjer et al (15) 2012 reference values are the same over this age range but expand the age range to 3.5 to 90 years. Most major spirometer manu-facturers have committed to implementing the Quanjer et al (15) ref-erence values in their newest or forthcoming models (www.lungfunction.org/93-manufacturers.html).
Another choice of reference equations is the National Health and Nutrition Examination Survey (NHANES) III series (Hankinson et al [21]), with values for Caucasian, African Americans and Hispanics between eight and 80 years of age. These equations should not be used outside their age range, particularly for children younger than eight years of age (22). This set is contained in almost all current spirometry systems.
In terms of a ‘Made in Canada’ solution, recently published refer-ence values for Caucasian Canadian adults 20 to 90 years of age (23) supplement those of Gutierrez et al (24) for adults 20 to 80 years of age. The subjects are sufficiently numerous to enable an accurate LLN and agree well with other large series such as NHANES III. Its greatest disadvantage is the problem of discontinuity between paediatric and adult equations because a separate pediatric set is required. The dis-continuity occurs when the pediatric and adult reference equations produce significantly different values in the transition period.
There are no reference equations for the Canadian Aboriginal population. Not only is there a scarcity of data, but the various First Nations, Inuit and Métis cannot be considered a physiologically hom-ogenous population. There are some suggestions that this group has larger lung volumes than Caucasians. Research is currently underway to address this issue.
Key messages:•Referencevaluesmustbeappropriatefortheageandethnicityof
the population, and ideally capable of providing the LLN•Theinterpretationofspirometrictestsshouldbebasedonthe
LLN•Recommendedreferencevalues,inorderofpreferencebasedon
number of subjects studied and age range, are:1. Quanjer et al (GLI [15]), 2012 (age 3.5 to 90 years) 2. Stanojevic et al (20), 2009* (age six to 70 years) 3. NHANES III (21), 1999 (age eight to 80 years)
4. Tan et al (23), 2012 (age 20 to 90 years) or Gutierrez et al (24), 2004 (age 20 to 80 years) adult Caucasians only
•SpirometrytestsinvolvingAboriginalCanadiansandothereth-nic groups should be interpreted with caution using Caucasian reference values
*The GLI recommends the use of Quanjer et al GLI 2012 (15) refer-ence values for all spirometry. The Caucasian values for the Stanojevic et al 2009 (20) reference set are the same as the Quanjer GLI 2012 set for ages six to 70 years. While some existing spirometer systems have the Stanojevic 2009 reference values implemented, which can be used as an interim measure, almost all manufacturers have agreed to implement the Quanjer GLI 2012 values on their spirometry systems. A reference value calculator for the Quanjer GLI 2012 reference values is available at <www.lungfunction.org/component/content/article/85-equations-and-tools/equations/151-excel-individual-calculator.html>
sPecial considerations For sPirometry in younG children
Spirometry testing began mainly in adults as a means to diagnose and monitor the progress of asthma and COPD, and was subsequently used in children even though measurement techniques and principles are not always directly comparable or applicable. Forced expiratory flow depends heavily on the static elastic recoil of the lungs. Various studies involving adults have demonstrated that the FEV1 correlates well with the degree of disability from lung disease. Children have higher elastic recoil than adults with faster emptying of the lung, which means that the FEV1 can be relatively insensitive to early lung disease. Some chil-dren are able to exhale completely in 1 s.
While the ATS/ERS standards (2) for the minimum expiratory time allow for 3 s in children ≤10 years of age rather than 6 s in adults, the requirement for a plateau (<25 mL in the final 1 s of exhalation) remains. In young children who empty their lungs in <2 s, it can be very difficult to resist inspiration before the 3 s limit. In such cases, the technologist must override the automatic rejection of the test.
The ATS/ERS standards (2) set tolerances for repeatability of FEV1 and FVC between tests of 150 mL or 100 mL for FVC or FEV1 ≤1 L. The back-extrapolated volume used for the beginning of test criterion must be ≤150 mL or 5% of FVC, whichever is greater. This results in larger percentage errors in children’s spirometry being deemed acceptable by the spirometry software. In a child-friendly environment, a technologist experienced in working with children can frequently exceed these minimal standards and produce higher-quality spirometry.
Another challenge in testing children is the inspiratory man-oeuvre. The ATS/ERS standards specify a rapid inspiration with no breath hold at end inspiration (2); however, knowing when the child has reached maximal inspiration can be challenging. Often, the tech-nologist continues to encourage the child to breathe in, which trans-lates to breath holding at total lung capacity. This problem is accentuated when using portable spirometers that are inserted in the mouth while at maximal lung volume (which are not recommended). The resulting FVC and FEV1 are lower after a slow inspiration and 4 s breath hold in the presence of any significant disease such as cystic fibrosis (12).
There was a brief spike in enthusiasm for the FEF25-75 in the adult literature; however, this rapidly waned when it was realized that the coefficient of variation of the test, particularly in those with COPD, was excessive because of the dependence of FEF25-75 on FVC. With COPD, where a plateau may not be reached, FVC may depend, in part, on the highly variable expiratory time. For children and young adults with greater elastic recoil, the variability of FVC is less and, hence, the FEF25-75 is more meaningful. Interpretation of this variable may still require an adjustment for the FVC (25).
environmentIt is helpful for the area where testing is taking place to have a bright and pleasant atmosphere (ie, pictures on the wall, children’s art and
reference value
Lower Limit of Normal
FEV1 values less than LLN are considered to be below normal
5%
Figure 2) Lower limit of normal (LLN). A plot of the forced expiratory volume in 1 s (FEV1) values from a theoretical population of normal men of age 60 years of age and height 180 cm. The mean FEV1 is 3.69 L (the refer-ence value) and the LLN is 2.78 L using Quanjer et al (15) 2012 Caucasian reference values

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYSpirometry in primary care
Can Respir J Vol 20 No 1 January/February 2013 19
drawings) (26). Having toys and books on hand is also useful if the child needs to wait a few minutes before testing and while waiting 10 min to 15 min for postbronchodilator testing.incentive displays: Some children are more willing and engaged in the spirometry test when an incentive is displayed on the computer screen such as a birthday cake with candles that extinguish during exhalation, a sailboat that moves across a pond or a balloon that expands and pops when exhalation is complete. However some tech-nologists find this more distracting to the children than helpful.mouthpiece: There is usually no need to use a mouthpiece in addition to the filter. Children are usually very adept at keeping their lips closed when reminded. An appropriately sized mouthpiece should be used if a better seal is needed.noseclips: Children do not generally encounter problems with the noseclips. When noseclips are applied, children automatically start breathing through their mouths. Noseclips with ‘spongey’ tips will stay on a child’s small nose and are not so tight on their delicate noses. Furthermore, these types of noseclips are available in different colours. Letting the child choose the colour he or she wants makes them feel a part of the testing. Of course, some children will not allow application of the noseclip. Sometimes they may allow a parent to hold their nose. As a last resort, the spirometry test can then be performed without the noseclips but one should try to introduce them as testing proceeds.chairs: Chairs should be adjustable to allow a small child to mount it. Ideally, they should also be able to sit straight with both feet on the floor.
Key message:Spirometry involving children requires technologists with specific skills working in a child-friendly environment to achieve optimal accuracy of the measurements and, hence, maximize the usefulness of spirometry in diagnosing and/or managing lung diseases in children.
Quality assurance and accreditationAny office, clinic or facility providing spirometry testing must be responsible for ensuring that the tests are performed to a high stan-dard. Physicians and nurse practitioners who interpret the tests must first ensure that the tests are of adequate quality because test results are used for the diagnosis and management of patients with respiratory disease. This section outlines the main points to evaluate the quality of spirometry testing.
Documentation of quality assurance procedures is mandatory in all offices, clinics and facilities conducting spirometry testing (2). The requirements include the following:1. Daily spirometer calibration checks, with additional calibrations
as necessary, and monthly assessment of repeatability of the measures using biological controls and analysis of a log of calibration results.
2. Documentation of repairs or other modifications of the equipment.3. Documentation of computer software and hardware updates or
changes.4. Qualification of all personnel conducting spirometry tests,
including education and training, to assure that they are familiar with the theory and practical aspects of applied techniques, measurements, calibrations, hygiene, quality control and a basic background knowledge in lung physiology and pathology (8).
5. Documented infection control procedures.
accreditation questions1. Has a suitably trained physician or nurse practitioner been
appointed as Medical Director/Quality Advisor to oversee spirometry testing?
2. Is there a quality assurance program in place and does it monitor staff competency, equipment performance, laboratory technique and procedure reporting, safety and utilization?
3. Has the individual conducting spirometry testing been adequately trained?
4. Has the individual interpreting the spirometry tests been adequately trained?
5. Does the spirometry requisition form or checklist comply with CTS recommendations?
6. Do spirometry reports comply with CTS recommendations?7. Are response times established for reporting spirometry test
results?8. Are the reference values used for the report appropriate for the
patient population?9. Are technologists’ comments available for the interpreter?10. Is there a policy manual, and does the manual include
organizational chart staff/office policies and procedures?11. Are there protocols for frequency of calibration for biological
control subjects?12. Are records of quality control procedures kept and routinely
reviewed?13. Are tolerance limits well defined for quality control checks?14. Is there a plan of action if tolerance limits are exceeded?15. Are there manuals available for equipment, policies and
procedures, and safety?16. Are these manuals site specific and updated annually?17. Do the procedures for spirometry testing define acceptable and
reproducible criteria for spirometry tests?18. Is there an equipment log that details any malfunctions with
spirometry equipment and corrective actions taken and does the log provide a history of the maintenance performed and by whom?
19. Are there default guidelines for cleaning, disinfecting and sterilizing equipment?
20. Are there specific procedures for individuals with known infections?
21. Is there a procedure for medical emergencies?
The above represents a general outline. For more detailed outline of a specific questionnaire, see the College of Physicians and Surgeons of Alberta Questionnaire (www.cpsa.ab.ca/services/Quality_of_Care_Main/Accreditation_Facilities/Pulmonary_Functions/Pulmonary_Standards.aspx) or Diagnostic Accreditation Program of British Columbia (http://www.dap.org/Default.aspx?p=57) for examples of questionnaires in current use for different levels of pulmonary function testing.
Distances travelled in Canada can be extensive, which may pre-clude onsite inspections for all facilities. In that case, the question-naire may be a remote way of quality control for the facilities. This could be accompanied by spirometry reports from the facilities to assess the final product.
Where provinces have an accreditation program that monitors the quality of diagnostic testing it is recommended that a questionnaire such as the one outlined above be part of that process.
disclosure oF comPetinG interests: Members of the CTS Pulmonary Functions Standards committee declared potential con-flicts of interest at the time of appointment and these were updated throughout the process, in accordance with accordance with the CTS Conflict of Interest Disclosure Policy. Individual member conflict of inter-est statements are posted at www.respiratoryguidelines.ca
editorial indePendence: The CTS Pulmonary Function Standards Committee is accountable to the CTS Respiratory Guidelines Committee and the CTS Board of Directors, and is functionally and editori-ally independent from any funding sources of the CTS. The CTS receives unrestricted grants to facilitate the knowledge translation activities of CTS clinical assemblies. No funders played a role in the collection, review, analy-sis or interpretation of the scientific literature or in any decisions regarding the recommendations or key messages presented in this document.
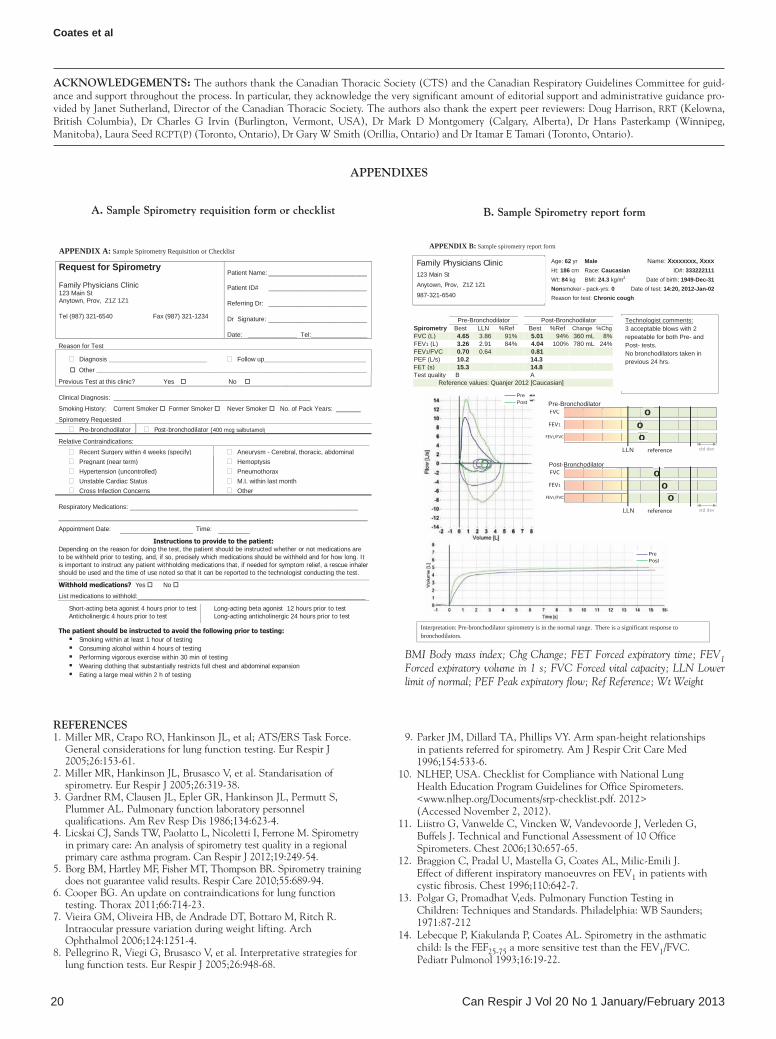
COPYRIGHT PULSUS GROUP INC. – DO NOT COPYCoates et al
Can Respir J Vol 20 No 1 January/February 201320
reFerences1. Miller MR, Crapo RO, Hankinson JL, et al; ATS/ERS Task Force.
General considerations for lung function testing. Eur Respir J 2005;26:153-61.
2. Miller MR, Hankinson JL, Brusasco V, et al. Standarisation of spirometry. Eur Respir J 2005;26:319-38.
3. Gardner RM, Clausen JL, Epler GR, Hankinson JL, Permutt S, Plummer AL. Pulmonary function laboratory personnel qualifications. Am Rev Resp Dis 1986;134:623-4.
4. Licskai CJ, Sands TW, Paolatto L, Nicoletti I, Ferrone M. Spirometry in primary care: An analysis of spirometry test quality in a regional primary care asthma program. Can Respir J 2012;19:249-54.
5. Borg BM, Hartley MF, Fisher MT, Thompson BR. Spirometry training does not guarantee valid results. Respir Care 2010;55:689-94.
6. Cooper BG. An update on contraindications for lung function testing. Thorax 2011;66:714-23.
7. Vieira GM, Oliveira HB, de Andrade DT, Bottaro M, Ritch R. Intraocular pressure variation during weight lifting. Arch Ophthalmol 2006;124:1251-4.
8. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948-68.
9. Parker JM, Dillard TA, Phillips VY. Arm span-height relationships in patients referred for spirometry. Am J Respir Crit Care Med 1996;154:533-6.
10. NLHEP, USA. Checklist for Compliance with National Lung Health Education Program Guidelines for Office Spirometers. <www.nlhep.org/Documents/srp-checklist.pdf. 2012> (Accessed November 2, 2012).
11. Liistro G, Vanwelde C, Vincken W, Vandevoorde J, Verleden G, Buffels J. Technical and Functional Assessment of 10 Office Spirometers. Chest 2006;130:657-65.
12. Braggion C, Pradal U, Mastella G, Coates AL, Milic-Emili J. Effect of different inspiratory manoeuvres on FEV1 in patients with cystic fibrosis. Chest 1996;110:642-7.
13. Polgar G, Promadhat V,eds. Pulmonary Function Testing in Children: Techniques and Standards. Philadelphia: WB Saunders; 1971:87-212
14. Lebecque P, Kiakulanda P, Coates AL. Spirometry in the asthmatic child: Is the FEF25-75 a more sensitive test than the FEV1/FVC. Pediatr Pulmonol 1993;16:19-22.
acKnoWledGements: The authors thank the Canadian Thoracic Society (CTS) and the Canadian Respiratory Guidelines Committee for guid-ance and support throughout the process. In particular, they acknowledge the very significant amount of editorial support and administrative guidance pro-vided by Janet Sutherland, Director of the Canadian Thoracic Society. The authors also thank the expert peer reviewers: Doug Harrison, RRT (Kelowna, British Columbia), Dr Charles G Irvin (Burlington, Vermont, USA), Dr Mark D Montgomery (Calgary, Alberta), Dr Hans Pasterkamp (Winnipeg, Manitoba), Laura Seed RCPT(P) (Toronto, Ontario), Dr Gary W Smith (Orillia, Ontario) and Dr Itamar E Tamari (Toronto, Ontario).
Pre-Bronchodilator Post-Bronchodilator Spirometry Best LLN %Ref Best %Ref Change %Chg FVC (L) 4.65 3.86 91% 5.01 94% 360 mL 8% FEV1 (L) 3.26 2.91 84% 4.04 100% 780 mL 24% FEV1/FVC 0.70 0.64 0.81 PEF (L/s) 10.2 14.3 FET (s) 15.3 14.8 Test quality B A Reference values: Quanjer 2012 [Caucasian]
Family Physicians Clinic 123 Main St
Anytown, Prov, Z1Z 1Z1
987-321-6540
Age: 62 yr Male Name: Xxxxxxxx, Xxxx Ht: 186 cm Race: Caucasian ID#: 333222111 Wt: 84 kg BMI: 24.3 kg/m2 Date of birth: 1949-Dec-31 Nonsmoker - pack-yrs: 0 Date of test: 14:20, 2012-Jan-02 Reason for test: Chronic cough
Interpretation: Pre-bronchodilator spirometry is in the normal range. There is a significant response to bronchodilators. Physician: Dr. Blow Hard
FVC FEV1 FEV1/FVC
LLN reference
o
o o
FVC FEV1 FEV1/FVC
LLN reference
Pre-Bronchodilator
Post-Bronchodilator o
o o
Pre Post
Pre Post
Technologist comments: 3 acceptable blows with 2 repeatable for both Pre- and Post- tests. No bronchodilators taken in previous 24 hrs.
std dev
std dev
APPENDIX B: Sample spirometry report form
Reason for Test
Diagnosis ____________________________ Follow up_____________________________ Other _____________________________________________________________________________
Previous Test at this clinic? Yes No Clinical Diagnosis: ________________________________________________________ Smoking History: Current Smoker Former Smoker Never Smoker No. of Pack Years: _______ Spirometry Requested
Pre-bronchodilator Post-bronchodilator (400 mcg salbutamol)
Relative Contraindications: Recent Surgery within 4 weeks (specify) Aneurysm - Cerebral, thoracic, abdominal Pregnant (near term) Hemoptysis Hypertension (uncontrolled) Pneumothorax Unstable Cardiac Status M.I. within last month Cross Infection Concerns Other
Respiratory Medications: _________________________________________________________________
Appointment Date: Time:
Instructions to provide to the patient: Depending on the reason for doing the test, the patient should be instructed whether or not medications are to be withheld prior to testing, and, if so, precisely which medications should be withheld and for how long. It is important to instruct any patient withholding medications that, if needed for symptom relief, a rescue inhaler should be used and the time of use noted so that it can be reported to the technologist conducting the test.
Withhold medications? Yes No
List medications to withhold:_________________________________________________________________
Short-acting beta agonist 4 hours prior to test Anticholinergic 4 hours prior to test
Long-acting beta agonist 12 hours prior to test Long-acting anticholinergic 24 hours prior to test
The patient should be instructed to avoid the following prior to testing: Smoking within at least 1 hour of testing Consuming alcohol within 4 hours of testing Performing vigorous exercise within 30 min of testing Wearing clothing that substantially restricts full chest and abdominal expansion Eating a large meal within 2 h of testing
Request for Spirometry Family Physicians Clinic 123 Main St Anytown, Prov, Z1Z 1Z1 Tel (987) 321-6540 Fax (987) 321-1234
Patient Name: ____________________________ Patient ID# ____________________________ Referring Dr: ____________________________ Dr Signature: ____________________________ Date: ______________ Tel:________________
APPENDIX A: Sample Spirometry Requisition or Checklist
aPPendiXes
a. sample spirometry requisition form or checklist B. sample spirometry report form
BMI Body mass index; Chg Change; FET Forced expiratory time; FEV1Forced expiratory volume in 1 s; FVC Forced vital capacity; LLN Lower limit of normal; PEF Peak expiratory flow; Ref Reference; Wt Weight

COPYRIGHT PULSUS GROUP INC. – DO NOT COPYSpirometry in primary care
Can Respir J Vol 20 No 1 January/February 2013 21
15. Quanjer PH, Stanojevic S, Cole TJ, et al; the ERS Global Lung Function Initiative. Multi-ethnic reference values for spirometry for the 3-95 year age range: The global lung function 2012 equations. Eur Respir J 2012;40:1324-43
16. Enright PL, Johanson LR, Connett JE, Voelker H, Buist AS. Spirometry in the lung health study. 1. Methods and quality control. Am Rev Respir Dis 1991;143:1215-23.
17. Centres for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHANES) 2009-2010 Data Documentation, Codebook, and Frequencies. <www.cdc.gov/nchs/nhanes/nhanes2009-2010/SPX_F.htm 2010> (Accessed November 2, 2012).
18. Mead J, Turner JM, Macklem PT, Little JB. Significance of the relationship between lung recoil and maximum expiratory flow. J Appl Physiol 1967;22:95-108.
19. Miller MR. Institute of Occupational & Environmental Medicine, University of Birmingham. <www.millermr.com/info.html> (Accessed October 29, 2012).
20. Stanojevic S, Wade A, Cole TJ, et al; Asthma UK Spirometry Collaborative Group. Spirometry centile charts for young Caucasian
children: The Asthma UK Collaborative Initiative. Am J Respir Crit Care Med 2009;180:547-52.
21. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med 1999;159:179-87.
22. Subbarao P, Lebecque P, Corey ML, Coates AL. Comparison of spirometric reference values. Ped Pulmonol 2004;37:515-22.
23. Tan WC, Bourbeau J, Hernandez P, et al. Canadian prediction equations of spirometric lung function for Caucasian adults 20 to 90 years of age: Results from the Canadian Obstructive Lung Disease (COLD) Study and the Lung Health Canadian Environment (LHCE) study. Can Respir J 2011;18:321-6.
24. Gutierrez C, Ghezzo RH, Abboud RT, et al. Reference values of pulmonary function tests for Canadian Caucasians. Can Respir J 2004;11:414-24.
25. Cockcroft DW, Berscheid BA. Volume adjustment of maximal midexpiratory flow. Importance of changes in total lung capacity. Chest 1980;78:595-600.
26. Seed L, Wilson D, Coates AL. Children should not be treated like little adults in the PFT lab. Respir Care 2012;57:61-71.

Can Respir J Vol 20 No 2 March/April 2013122 ©2013 Pulsus Group Inc. All rights reserved
Re: Coates AL, Graham BL, McFadden RG, et al. Spirometry in primary care. Can Respir J 2013;20(1):13-21.
In the ‘Reference values’ section on page 17, the following state-ments were made: “African Americans have lung volumes approxi-mately 10% lower than Caucasians. Asians have lung volumes 2% to 8% lower than Caucasians (15)”.
These statements should have read: “African Americans have lung volumes approximately 14% lower than Caucasians. South East Asians (southern China, Thailand, Korea) have lung volumes 10% to 14% lower than Caucasians (15).”
The authors apologize for the error.
corrigendum

AMERICAN THORACIC SOCIETYDOCUMENTS
Recommendations for a Standardized Pulmonary Function ReportAn Official American Thoracic Society Technical StatementBruce H. Culver, Brian L. Graham, Allan L. Coates, Jack Wanger, Cristine E. Berry, Patricia K. Clarke, Teal S. Hallstrand,John L. Hankinson, David A. Kaminsky, Neil R. MacIntyre, Meredith C. McCormack, Margaret Rosenfeld,Sanja Stanojevic, and Daniel J. Weiner; on behalf of the ATS Committee on Proficiency Standards for PulmonaryFunction Laboratories
THIS OFFICIAL TECHNICAL STATEMENT OF THE AMERICAN THORACIC SOCIETY WAS APPROVED OCTOBER 2017
Background: The American Thoracic Society committee onProficiency Standards for Pulmonary Function Laboratories hasrecognized the need for a standardized reporting format forpulmonary function tests. Although prior documents have offeredguidance on the reporting of test data, there is considerablevariability in how these results are presented to end users, leading topotential confusion and miscommunication.
Methods: A project task force, consisting of the committee as awhole, was approved to develop a new Technical Standard onreporting pulmonary function test results. Three working groupsaddressed the presentation format, the reference data supportinginterpretation of results, and a system for grading quality of testefforts. Each group reviewed relevant literature and wrote draftsthat were merged into the final document.
Results: This document presents a reporting format in test-specificunits for spirometry, lung volumes, and diffusing capacity thatcan be assembled into a report appropriate for a laboratory’spractice. Recommended reference sources are updated with datafor spirometry and diffusing capacity published since priordocuments. A grading system is presented to encourageuniformity in the important function of test quality assessment.
Conclusions: The committee believes that wide adoption of theseformats and their underlying principles by equipment manufacturersand pulmonary function laboratories can improve the interpretation,communication, and understanding of test results.
Keywords: pulmonary function testing; reporting spirometry;reference equations; pulmonary function quality grading
ContentsOverview
ConclusionsIntroductionMethodsReport Format for Spirometry andOther Lung Function Tests
General ConsiderationsSpirometryTests of Lung Volume
Diffusing Capacity (TransferFactor)
Comments and InterpretationSelecting and Reporting ReferenceValues
General ConsiderationsCurrent Spirometry ReferenceValues
Using Reference Data inInterpretation of Results
Reference SourceRecommendations
Grading the Quality of PulmonaryFunction Tests
SpirometryLung VolumesDiffusing Capacity (TransferFactor)
The Quality ReviewerConclusions
Supported by a project grant from the American Thoracic Society.
Correspondence and requests for reprints should be addressed to Bruce H. Culver, M.D., Division of Pulmonary, Critical Care and Sleep Medicine, Universityof Washington School of Medicine, Campus Box 356522, Seattle, WA 98195-6522. E-mail: [email protected]
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Am J Respir Crit Care Med Vol 196, Iss 11, pp 1463–1472, Dec 1, 2017
Copyright © 2017 by the American Thoracic Society
DOI: 10.1164/rccm.201710-1981ST
Internet address: www.atsjournals.org
American Thoracic Society Documents 1463

Overview
The American Thoracic Society Committeeon Proficiency Standards for PulmonaryFunction Laboratories (ATS PFT Committee)has been concerned about the wide variabilityin pulmonary function test (PFT) reportsamong laboratories and has discussed the needfor a more standardized format, to includeinformation to assist accurate interpretationand to enhance the communication of resultsto end users. ATS support was granted todevelop a technical standard to address thisneed and also to update reference sources andto propose a standardized quality gradingsystem.
Conclusionsd A uniform format for the presentation ofPFT results in reports to users and inthe medical record can reduce potentialmiscommunication ormisunderstanding.
∘ Only information with validatedclinical application should be included.
∘ The normal limit(s) of each testparameter should be displayed.
∘ Consistent with other laboratoryvalues, the measured value should beshown before reference values, ranges,or normal limits.
∘ Report and/or display of thedisplacement of the result from apredicted value in standard deviationunits (z-score) can help inunderstanding abnormality.
d For spirometry, many parameters can becalculated but most do not add clinicalutility and should not be routinelyreported.
∘ Only FVC, FEV1, and FEV1/FVC needbe routinely reported.
∘ Measurement of slow VC andcalculation of FEV1/VC are a usefuladjunct in patients with suspectedairflow obstruction.
∘ Reporting FEV1/FVC (or FEV1/VC) asa decimal fraction, and not reporting itas a percentage of the predicted valuefor this ratio, will help to minimizemiscommunication.
d Lung volumes
∘ The nitrogen washout plot formultibreath tests and the tracings forplethysmograph tests can be showngraphically to aid quality assessment.
d For diffusing capacity the report isconsistent with the 2017 EuropeanRespiratory Society (ERS)/ATS TechnicalStandard for this test.
∘ Barometric pressure should bemeasured and reported and themeasured value corrected to thestandard pressure of 760 mm Hg.
d Newer collated reference equations forspirometry and diffusing capacity havebeen developed since prior ATSdocuments and warrant wideimplementation.
∘ The Global Lung Function Initiative(GLI)-2012 multiethnic spirometryreference values are recommended foruse in North America and elsewhere forthe ethnic groups represented. Theirsmooth continuity throughout growthis advantageous for laboratories testingchildren or adolescents.
∘ The National Health and NutritionExamination Survey (NHANES) IIIreference values (recommended forNorth America in 2005 ATS/ERSdocuments) remain appropriate wheremaintaining continuity is important.
∘ Regardless of the reference source orlower limit of normal (LLN) chosen,interpreters should be aware ofuncertainty when interpreting valuesnear any dichotomous boundary.
∘ For lung volumes and diffusing capacity,no prior ATS recommendation has beenmade because of the wide divergence ofavailable reference values. A largecompilation of international data hasbeen completed for the diffusing capacityof the lung for carbon monoxide (DLCO)and is underway for lung volumes. Theresulting reference equations should bewidely adopted when published.
d Pulmonary function tests that fail tomeet optimal standards may still provideuseful information. A grading systemfor test quality can allow for this use,while providing an indication of theuncertainty imposed, and is most helpfulif widely standardized.
∘ For spirometry, FVC and FEV1 aregraded separately on an A–F scaleeither manually or by software. Thereis evidence that grades A–C areclinically useful, whereas grades D andE may have limited value, and grade Fshould not be used. The same scale,
with different criteria values, is usedfor children.
∘ For diffusing capacity a similar gradingscale is presented on the basis of 2017ERS/ATS standards.
Introduction
The range of reporting formats currentlyin use is wide; commercial PFT systemsoffer differing reports, and some clinicallaboratories customize their own. Differentlyarranged reports can lead to confusion orerrors and make comparisons of data fromdifferent laboratories unnecessarily difficult.PFT equipment manufacturers haveexpressed a desire for, and a willingness toimplement, a standardized form once it hasbeen established. Newer reference data forspirometry and diffusing capacity havebecome available since the publication ofprior guidelines, and a standardized systemfor grading the quality of lung function testswould be desirable.
Methods
For several years the ATS PFT Committee hasbeen discussing and sharing ideas forimprovement in the reporting of PFT results.A project task force, consisting of thecommittee as a whole, was approved todevelop this new technical standard. Thecommittee included adult and pediatricpulmonologists and physiologists andrespiratory therapists with extensive PFTexperience. Three working groups addressedthe presentation format, the reference datasupporting interpretation of results, and asystem for grading quality of test efforts. Eachgroup reviewed relevant literature and wrotedrafts that were merged into the finaldocument. As there is rather limited literatureto support the necessary choices, these weremade by consensus; all members approved thefinal document.
Report Format for Spirometryand Other Lung FunctionTests
General ConsiderationsThe following recommendations andrationale are based on developing a formatthat will be intuitive, will include onlyinformation with validated clinicalapplication, will be based on the use of
AMERICAN THORACIC SOCIETY DOCUMENTS
1464 American Journal of Respiratory and Critical Care Medicine Volume 196 Number 11 | December 1 2017

the LLN, and will be consistent withprior recommendations for PFTinterpretation and reporting (1–4). Somerecommendations are necessarily arbitrary(e.g., the order of rows or columns) butreflect a consensus of current and priorcommittee members and an informalsurvey of others (5). Although individualpreferences vary, there is wide agreementthat the benefit of uniformity outweighsthese.
The report format recommended ispresented in test-specific units that can beassembled into a report appropriate for alaboratory’s practice or even an individualtest session. It is designed so that for simpletesting it can be printed, along withinterpretive comments, on a single page asa report to a referring physician or forinclusion in the medical record. Of necessity,this contains limited information and is notintended as the only resource for theinterpreter, who should have the option ofdisplaying all individual maneuvers from agiven PFT session, increasingly done ondigital systems. Standardized electronicformats for the saving of all PFT data,including each individual maneuver, arebeing recommended (6). This will allowreviewers the flexibility to see additionaldetail or to reanalyze previous PFTs or applynew reference values as they becomeavailable. A standardized methodology toincorporate PFT data into electronic medicalrecords is needed, but is beyond the scopeof this report. See Appendix EA in theonline supplement for a suggested list of testresults to save to the electronic medicalrecord.
In designing the standardized report,the committee recognized that aspects ofdata presentation can affect decision-making (7). The use of boldface or coloredfonts to highlight measured values belowthe LLN can draw attention to these, butimposes a binary decision on a continuousvariable. The number of variables reportedcan also have an impact becauseincluding a large number of outcomesin the report increases the statisticallikelihood of one falling below anarbitrary LLN, with the risk of a falsepositive result (8).
All reports must begin withunambiguous patient identification,including patient name, medical recordnumber, sex, and date of birth; the latter canbe compared with previous records as acheck for possible identification errors, as
well as for calculating patient age (year toone decimal place for children andadolescents, e.g., age 6.3 yr) (9, 10). Otheressential information is height (to thenearest centimeter) and weight, ethnicity,and date of the test. Other usefulinformation includes smoking history,reason for the test, and referring physician’sname. Additional information may includeoxygen saturation and barometric pressure.
The display will vary with the testingdone, but the suggested order is spirometry,slow vital capacity, and/or lung volumemeasurement, and diffusing capacity of thelung for carbon monoxide (DLCO). Othertests could be added such as forcedoscillometry, maximal respiratory systempressure, levels of expired nitric oxide, orother tests, but the philosophy should besimilar, that is, reference source, normallimits, graphs that convey qualityinformation, and exclusion of informationwithout clinical value.
The recommended order of thecolumns in tabular data is the actual value,the LLN, the z-score (optional), and thepercent predicted value. The predictedvalue itself is unnecessary, as it does not aidin the interpretation of abnormality. Thez-score of a result is the number of standarddeviations it lies away from the mean or, forregression equations, the number ofstandardized residuals away from thepredicted value. Linear graphical displaysvisualize this in relationship to the normalrange and assist in assessing thesignificance of abnormal values (11, 12). (Ifnewly introduced to the reports, adding abrief explanation may be helpful.) Thereference source from which the LLN andpercent predicted value are derived must belisted, and whether or not these areadjusted or specific for race/ethnicity mustalso be stated in technician comments.
SpirometryAs shown in Figure 1, numerical values aregiven only for the FEV1, the FVC, and theFEV1/FVC ratio; the latter should bereported as a decimal fraction and the spacefor percent predicted value left blank tominimize miscommunications. Whenappropriate, an additional row can be addedfor FEV1/(slow) VC (1, 2). Forced expiratorytime (FET) is reported to aid qualityassessment. If bronchodilators are given, theLLN column need not be repeated; theabsolute and percent change should be givenonly for FEV1 and FVC. Other numerical
values such as the forced inspiratory flow at75% of FVC (FEF75%) and FEF25–75% havenot demonstrated added value foridentifying obstruction in adults or children,and therefore are not recommended forroutine use (13, 14). The flow–volumecurve and the volume–time curve aredisplayed, from which the peak flow andFET can be seen. These graphs must havesufficient resolution to evaluate the qualityof the data. For the volume–time curve,the volume scale should be at least 10 mm/L,the time scale at least 20 mm/s, and 1 secondprior to the start of expiration should bedisplayed (2). On the flow–volume plot, theflow display should be at least 5 mm/L/s,and the ratio of flow to volume should be2 L/s to 1 L. The scales of the graphsmay be adjusted to maximize the imagewithin the available space on the reportform, especially for tests on small children.The linear analog scales, where the valuesfor FEV1, FVC, and their ratio are plottedas z-scores relative to the predicted value(z = 0), give an intuitive sense of severity(12). Because there is always someuncertainty about the application of anyprediction to an individual and about theexact LLN, a large star rather than a discretepoint is used on the scale to suggest thatcaution is indicated when interpreting valuesclose to the LLN.
For slow vital capacity, the graph showsbaseline tidal breathing to assess whetherinspiration occurred from a stable end-expiratory volume (3). The largest vitalcapacity is reported along with theinspiratory capacity and, when appropriate,the FEV1/VC.
Tests of Lung VolumeValues derived by body plethysmography orgas dilution are displayed with the samecolumn order (Figure 2). We show a fullcomplement of volume parameters listed ina physiologically rational order; however,some laboratories may choose not to reportall. With a multibreath nitrogen (N2)washout the graph of the fall in N2
concentration gives an indication of anyleaks present (3). For helium dilutionfunctional residual capacity (no graphdisplayed), equilibration is considered to becomplete when the change in heliumconcentration is less than 0.02% for 30seconds. The histogram displays the actualvolume increments beside the predictedvolumes as an indication of severity, and z-scores are shown here in a vertical format.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 1465

Sample PulmonaryName:
Pre-Bronchodilator
Pre-Bronchodilator
Post-Bronchodilator
FVC
z-score –5 –4 –3 –2 –1 0 1 2 3
–5
6
4
8
6
4
2
0Flo
w (
L/s)
–2
–4
–6–1 0 1 2 3 4 5
2
Vol
ume
(L)
Vol
ume
[L]
Volume (L)0
–1 1 3
8
7
6
5
4
3
2
1
0
–1–14–12–10 –8 –6 –4 –2 0 2 4 6 8 10 12 14 16
5 7Time (s)
Time [s]
9 11 13 15
–4 –3 –2 –1 0 1 2 3
FEV1
FEV1/FVC
FVC
z-score
FEV1
FEV1/FVC
LLN
**
***
*predicted
LLN predicted
Post-Bronchodilator
Best Best z-score %Pred Change %Chng
99% 600 mL 20%
29%590 mL70%
–0.09
–2.21
–3.35
4.70
2.61
0.55
11.2
3.90
2.02
0.52
10.3
4.17
2.76
0.48
FVC (L)
FEV1 (L)
FEV1/FVC
FET (s)
Reference values: GLI 2012 Test quality: Pre: FEV1 - A, FVC - A; Post: FEV1 - A, FVC - B
LLN
3.70 –1.34 82%
54%–3.78
–3.54
2.91
0.68
z-score %Pred
Best
VC (L)
IC (L)
FEV1/VC
Reference values: VC - Gutierrez 2004; FEV1/VC – GLI 2012
TECHNICIAN COMMENTS: No medicationsin past 24 hr. 400 mcg albuterol given forreversibility testing.
Moderately severe, partially reversible airflow obstruction.
Dr. P. Pulmonologist 2017-Feb-24
LLN
4.0 6.0 –1.61
–3.86
83%
87%3.92.4
0.68
z-scoreULN %Pred
Referred by: Dr. G. Practitioner2017-Feb-20 14:30Short of breath99%69 in; 175 cm202 lb; 91.8 kg
30.0 kg/m2
Date of test:Reason:SpO2 at rest:Height:Weight:BMI:
Xxxxxxxxxx, Yyyyyyyyy111 222 333Male1965-Aug-0451Caucasian
SPIROMETRY
SLOW VITAL CAPACITY (Pre-Bronchodilator)
Ex-smoker
ID:Sex:Birth date:Age:Ethnicity:Smoking:
Function Laboratory
Anytown, [email protected]
prepost
Figure 1. Example of a single-page report for pre- and postbronchodilator spirometry testing. The linear graphic is divided in units of 1 SD, with theLLN shown at a z-score of 21.64. This simplified report is suitable for the medical record or referring physician, but the test interpreter should haveaccess to the data and curves of all acceptable spirometry efforts. FET = forced expiratory time; GLI = Global Lung Function Initiative; IC = inspiratorycapacity; LLN = lower limit of normal; SpO2
= oxygen saturation as measured by pulse oximetry; ULN = upper limit of normal; VC = vital capacity.
AMERICAN THORACIC SOCIETY DOCUMENTS
1466 American Journal of Respiratory and Critical Care Medicine Volume 196 Number 11 | December 1 2017

When diffusion capacity is measured, acomparison of total lung capacity measuredby both techniques can be a useful qualitycontrol measure or an indication ofmaldistribution.
Diffusing Capacity (Transfer Factor)The display (Figure 3) gives the relevantvalues, the LLN, and the percent predicted
value along with the reference source, aquality assurance indication, and theconditions of the test, in this case post-bronchodilator. The barometric pressureshould be given, as well as stating whetherthe values were corrected to standardbarometric pressure (particularly importantfor laboratories at altitude) (6). Reportingthe carbon monoxide transfer coefficient
(KCO) is optional, but the term DL/VA (theratio of diffusing capacity to alveolarvolume) should be avoided as it iscommonly misunderstood. If measured, thehemoglobin should be shown as well as theadjusted predicted values for both DLCO
and KCO. The display shows the washout ofboth carbon monoxide and the tracer gasand the sample volume. The sample volume
Result
32%
83%81%88%78%61%89%1.90
0.782.683.274.055.95 8.5
6.0
4.6
2.9
–1.45–1.61
–1.03
–0.491.4
2.2
4.05.8
Reference values: Gutierrez 2004; Test quality: QA metRV/TLC (%)RV mb (L)ERV (L)FRC mb (L)ICmb (L)VC (L)TLC mb (L)
LLN ULN z-score %Pred 76543210
8 ULN
ULN
ULN
LLN
LLN
LLN
Vol
ume
(L)
Pred Result RVFRCTLC
0.50
1
10
N2
conc
entr
atio
n [%
] 80
20Volume [L]
40
MULTI-BREATH NITROGEN WASHOUT (Post-Bronchodilator)
45% 45%
109%87%
100%137%
76%160%
138%27%
3.89
8.684.793.425.261.29
5.92Reference values: Gutierrez 2004; Test quality: QA met
RV/TLCVtg (L)
RV pl (L)ERV (L)FRC pl (L)IC pl (L)VC (L)TLC pl (L)
Result LLN
3.1
0.90–1.15
2.00
3.07
9.36.54.15.02.13.2
5.5
1.71.3
2.72.7
4.56.6
ULN z-score %Pred76543210
89 ULN
ULN
ULN
LLN
LLN
LLN
Vol
ume
(L)
Pred Result RVFRCTLC
10
5
0
–5
–10
–15
15
20 mL
PressurePLETHYSMOGRAPHY (Post-Bronchodilator)
IC
IC
ERV
RV
ERV
RV
Figure 2. Examples of the recommended reporting format for lung volume testing in one subject by multibreath nitrogen (N2) washout and in another subjectby plethysmography. The N2 washout is plotted on a log scale, resulting in a nearly linear profile. On this plethysmography tracing the box pressure has beenconverted to volume to show the thoracic excursions at a scale of 20ml per division. The bar graphs on the right show the predicted and observed values of RV, FRC,and TLC, and the arrows show these results in relation to their normal range on vertical linear scales. The graphs depict RV in blue, ERV in orange, IC in gray, andnormal range in green. (See Figures E1 and E2 in the online supplement for examples of consolidated reports for full pulmonary function tests.) ERV=expiratoryreserve volume; IC= inspiratory capacity; LLN= lower limit of normal; mb=multibreath; pl = plethysmography; QA=quality assurance; RV= residual volume; TLC=total lung capacity; ULN=upper limit of normal; VC= vital capacity; Vtg= thoracic gas volume.
DLCO
VA
KCO
z-score –5 –4 –3 –2
* ** –1 0 1 2 3
LLN predicted10 12 14 16
Time (s)
COCH4
Reference values: GLI 2017; Test quality: one grade A test; PB: 721 mmHg
DLCO (mL / min / mmHg)
KCO (mL / min / mmHg / L)
DLCO (pred adj Hb 13.8 g/dL)DLCO (at standard PB)
TLCsb (L)VA (L)
VI/VC (%)
Result z-scoreLLN %Pred
5.75
3.25
23.4
52%
82%53%42%
–3.47
–1.55
–4.55
85%6.015.83
13.013.0
13.4
2.23
DIFFUSING CAPACITY (Post-Bronchodilator)
Figure 3. Example of the recommended reporting format for the single-breath diffusing capacity test. The 2017 Technical Standard for DLCO (6) requires thatthe CO and tracer gas concentrations be graphed versus exhaled volume, rather than versus time as shown here. When hemoglobin is measured, it should be shownon the report with a note indicating whether the predicted value has been adjusted for this. CH4=methane (tracer gas); DLCO=diffusing capacity of the lung forcarbon monoxide; GLI =Global Lung Function Initiative; KCO=carbon monoxide transfer coefficient; LLN= lower limit of normal; PB =barometric pressure; pred adjHb=hemoglobin adjusted for predicted value; sb= single breath; TLC= total lung capacity; VI/Vc= inspired volume/vital capacity.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 1467

is “virtual” and derived from rapid-actinganalyzers and can be adjusted for the size ofthe patient after the maneuver. However, thedisplay must show the sample volume thatwas used in the calculation (4). Again, thereis a linear graph where the result is plotted asz-scores away from the predicted value.
Comments and InterpretationThere is a place for technician comments onthe test session, any quality issues, and otherrelevant information that may aid ininterpretation. The accompanying figuresshow how the format units may becombined into one-page reports for bothspirometry (Figure 1) and more completetest sessions (Figures E1 and E2). The one-page form has space for only a briefinterpretive summary, and thereforelaboratories preferring a more detailedinterpretation and/or less crowdedcomponents may opt for a two-page report.Test tracings are shown for spirometry andother tests as well, but some laboratoriesmay choose not to include all of these forthe end user as long as the interpreter hasfull access to them. Although comparisonwith prior values is important tointerpretation, a format for this is notaddressed in this document.
Selecting and ReportingReference Values
General ConsiderationsInterpretation of PFTs requires comparisonwith reference values because lung functiondepends on body dimensions andphysiological changes throughout growthand aging. Reference equations use suchfactors as height, age, sex, and race/ethnicityto predict the average lung function as wellas the range of expected values, with the goalof distinguishing the effects of disease fromnormal variability among healthyindividuals.
PFT laboratories must selectappropriate reference values for the patientsbeing tested. These should be generatedfrom high-quality data collected from a largesample of healthy asymptomatic individualswho have never smoked or been affected byother respiratory illness or significantexposures. Not all published referencesources meet these criteria; therefore carefulconsideration of the advantages anddisadvantages of available reference valuesis necessary.
Lung function reports should identifythe source of reference values, because thesame measured values may be interpreteddifferently based on the reference sourceused. Furthermore, manufacturers need tobe transparent when reference values havebeen combined from various sources. Inthe event that a laboratory changes itsselected reference equations, this should benoted on the report, and percent predictedvalues for prior lung function data shouldbe recalculated, if possible. It is preferredthat there be no discontinuity betweenpediatric and adult equations in thereference values selected, and extrapolationof values beyond the age range of theequations should not be done during growthand will increase uncertainty in the elderly(9, 15). Any such extrapolation must benoted in technician comments.
Current Spirometry Reference ValuesIn 2005, the 1999 NHANES III spirometryreference equations (16) wererecommended for use in North America(1). This study provided values for whites,African Americans, and MexicanAmericans living in the United States. Theage span was 8–80 years in two sets ofequations with a break at age 18–20 years; aseparate recommendation was made forchildren under age 8. As there wasuncertainty whether these equations were agood fit for various European populations,no recommendation was made.
Subsequently, the GLI group wasformed with ERS sponsorship and with theparticipation of the ATS PFT Committee.The goal was to merge available data sets,including the NHANES III data, to developmore broadly applicable referenceequations. This effort resulted in newspirometry reference equations using datacollected from more than 74,000individuals, ages 3–95 years, from 26countries (12). The GLI establishedreference values for whites, AfricanAmericans, North East Asians, and SouthEast Asians. The equations for the whitepopulation were shown to be applicable notonly in the United States and Europe but inother parts of the world, including Hispanicregions, and for Hispanic Americans. Thesefindings confirm a reanalysis of theNHANES III data, which showed no needfor separate reference equations forHispanic and non-Hispanic whites (17).For individuals not represented by thesefour groups, or who are of mixed ethnic
origin, a composite equation is provided.(See Appendix EB for guidance on thechoice of equations.) The GLI data foundthe FEV1/FVC ratio to be generallyindependent of ethnic group, and thus itsLLN is a useful indication of airflowlimitation even when ethnicity is uncertain.
More recently, the Canadian HealthMeasures Survey has published population-based spirometry reference equations forwhites, using a format similar to NHANESIII (18). Average adjustment factors aregiven for several indigenous and immigrantgroups. Of note, they found that individualsof Chinese ancestry living in Canada hadvalues intermediate between white valuesand those predicted by GLI equations fromdata collected in China.
Since the GLI-2012 publication, thesewhite reference values have been comparedwith those of NHANES III. In large clinicalpopulations from Australia and Poland,the values predicted by GLI-2012 andNHANES III were similar and rates of airflowlimitation (FEV1/FVC, LLN) were similarin both men (GLI, 34.5 and NHANES III,33.3%) and women (GLI, 27.9 andNHANES III, 25.4%) (19). Similar findingshave been demonstrated in additionalclinical populations from Australia (20), theUnited States (21), and in children andadolescents (22). The Canadian predictedvalues compared somewhat more closelywith GLI-2012 than NHANES III values, butdifferences among the three were minor andnot likely to be clinically important (18).
In a simulation of NHANES III andGLI-2012 predicted values across a broadrange of age and height, the FEV1 predictiondifferences were within the recommendedrepeatability criterion of 6150 ml across awide range of heights and ages (21). Therewere larger differences at the extremes ofheight in older individuals, where moreuncertainty would be expected due torelatively few subjects of advanced age inthe GLI-2012 data and extrapolation of theNHANES III data beyond the age of itssubjects.
Using Reference Data inInterpretation of ResultsBoth the ATS and ERS recommend the useof the LLN, or the upper limit whereappropriate (e.g., lung volumes), to delineatebetween health and suspected disease. Theseare set at the fifth percentile (equivalent to az-score of 21.645) so that 95% of a healthypopulation falls within the normal range
AMERICAN THORACIC SOCIETY DOCUMENTS
1468 American Journal of Respiratory and Critical Care Medicine Volume 196 Number 11 | December 1 2017

and the lowest 5% would be false positives.However, clinical PFTs are typically donewhen disease is suspected, increasing thepretest probability of an abnormal result sothat the false positive rate is much lower inthis setting. The LLN does not necessarilyneed to be the fifth percentile but, withadequate outcome data, could be adjustedhigher when the pretest probability is highor lower for population screening (23, 24).More important than the applicability ofa particular LLN is recognition of theuncertainty that lies near any dichotomousboundary and where caution is required,especially when results are limited to asingle test occasion.
The respiratory community is familiarwith using the percent predicted value todescribe lung function results; however, thisvalue should not be used to defineabnormality. The true LLN is age- and/orheight-dependent and therefore will occurat varying percent values in differentindividuals. The fixed values commonlyused (e.g., 80% predicted for FVC, 0.70 forFEV1/FVC) are estimates based on middle-aged adults, and therefore erroneousclinical decisions based on these fixedcutoffs are more likely to occur in childrenand in older or shorter adults. Using fixedcutoffs also introduces a sex bias intoclinical assessments (25). Interpretation ofindividual results relative to the range ofvalues expected can be more appropriatelyincorporated into PFT reports using therecommended linear analog scale.
Reference Source RecommendationsFor spirometry, the GLI-2012 referencevalues are recommended for use in NorthAmerica for the ethnic groups represented,as well as in Europe, Australia–New Zealand(26), and other areas with representedpopulations. For laboratories wishing tomaintain continuity, the NHANES IIIequations also remain recommended forwhites (including Hispanics) and AfricanAmericans. Use of GLI-2012 isrecommended for clinical research studiesto facilitate comparisons with internationalstudies (27, 28). The GLI-2012 equationsare also preferred for laboratories testingchildren or adolescents because they permittracking during this time of rapid lunggrowth and development withoutdiscontinuities due to switching referencesources. The Canadian reference values alsoprovide a useful resource (18). Whateverreference source is used, interpretations
must be based on a parameter-specificlower limit determined from thedistribution of the reference data.
For DLCO, no prior ATS recommendationhas been made because of the widedivergence of available reference values.With ATS and ERS sponsorship a GLIgroup has assembled data from more than12,000 individuals in 14 countries to developnew (white-only) reference equations fromage 5 to 85 years. Publication of these isexpected in 2017 (29) and their rapidadoption is recommended.
For plethysmographic or dilutionallung volumes, no recommendation can bemade for reference values at this time. A newinternational project to address this needis underway. (Values from a Canadian study[30] are used as examples in theaccompanying figures.)
Grading the Quality ofPulmonary Function Tests
SpirometryWhereas considerable attention has beengiven to guidelines for the procedures toconduct spirometry (2), guidelines to assessthe quality of the testing are still needed.The purposes of quality review are toprovide feedback to the technicians and, inthe clinical setting, to indicate anylimitations to the interpretation of theresults. In clinical research, quality reviewhelps determine whether a subject can beincluded in a trial and whether data at anytime point can be used in the analysis.
Various quality-grading systems havebeen reported (31–38) and others have beenprovided by spirometer manufacturers, butusers would benefit from standardizedmethodology. The system recommendedfor adults and children is shown inTables 1 and 2. It is modified from a systemthat has been used in research andepidemiological studies (16, 18, 38). Foryounger children, 2–6 years of age, thecriteria are modified on the basis of the2007 ATS/ERS recommendations forspirometry testing in preschool children(39). These systems can be used manually,or as part of spirometry software, assigninga grade (A through F) separately for thequality of FVC and FEV1. In general, testswith a grade of A, B, or C are usable; testswith grade D are suspect; tests with gradeE might be used by the interpreter onlyto show values “within the normal range”
or “at least as high as,” withoutdemonstrated repeatability; and tests withgrade F should not be used.
The grading system consists ofacceptability and repeatability components.An ideal test session conforms to priorATS/ERS recommendations (2, 39) with atleast three acceptable maneuvers andrepeatable FVC and FEV1 values. Thesecriteria were intended to guide techniciansto achieve the best possible results, and thegoal should be to exceed them becausemany technicians can achieve better qualitytests. However, their strict application mayalso lead to the exclusion of useful results.A grading system allows the user toevaluate the likelihood that spirometryresults are representative of true values inthe face of test performance that is notideal. Failure to achieve optimal tests maybe due to underlying disease; thus bias maybe introduced into clinical researchstudies by eliminating subjects with moresevere disease. The reviewer must considerwhether or not the subject’s effort in amaneuver was maximal, and/or whetherlack of repeatability could be due to lungdisease, using all available informationincluding technician comments. When atest session with a poor-quality gradeis used as a baseline for pre/post-bronchodilator or longitudinalcomparisons, an apparent improvementin values may be the result of better effortor technique
While strict application of the gradingcriteria can be done by computer software,the reviewer’s role is to apply judgmentby reviewing the individual curves, whichmay change the scoring and allowinterpretation. For example, if a maneuverin the session is unacceptable only becauseof excessive back extrapolation volume, itcan still be used to confirm repeatability ofFVC. Determining whether the subject hasexhaled completely is difficult, and onereport has suggested that many subjects areunnecessarily excluded by the 2005ATS/ERS end-of-test criteria (38). The FETis used to determine whether the subjecthas tried to exhale long enough, and theend of the volume–time curve is assessed todetermine whether expiratory flow hasceased, defined as a volume change lessthan 0.025 L in 1 second. Often the FET isless than 6 seconds, because the softwarehas stopped data collection once this lowflow criterion is met, or an artifact duringexhalation may be falsely perceived as a
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 1469

plateau, thus stopping data collection andunderestimating FET and FVC. Subjectsshould be verbally encouraged to continue theexpiratory effort at the end of the maneuver toobtain optimal results (2). The technicianand/or reviewer must make a determination asto whether or not end-of-test criteria were metand whether the data are useful. Some subjects,especially children and adolescents, cannotexhale for the required 3 or 6 seconds. If thesesubjects have a 1-second plateau, and thereviewer judges that these maneuvers representa maximum FVC, the grade should be adjustedhigher. Subjects with airflow obstruction maynever reach a plateau even at the suggested 15-second limit and may have nonrepeatable FVCvalues only because of a difference in FET.Similarly, subjects with restrictive lung disease
may reach an early plateau and may not beable to maintain a 6-second effort. Theresults may still be considered acceptable insuch cases and an appropriate comment by thereviewer should be made.
FEV1 is graded separately because eventest efforts that are clearly unacceptable forFVC may contain a valid measurement ofFEV1 (or FEV0.75, the forced expiratoryvolume exhaled in the first 0.75 s of the FVCmaneuver, and a recommended measure inpreschool children) (2, 39). Anything thatoccurs later in the flow–time tracing (e.g., earlytermination, cough artifacts) does not affectthe FEV1 or FEV0.75 value, and thus these maybe used even with end-of-test errors.
Despite the attention paid to expiratoryparameters, the most common reason for
low FVC, FEV1, and PEF values is anincomplete inhalation. Achievement ofmaximal inhalation is best assessed bymeasures of repeatability and also by theconsistency of the shape of the flow–volume or volume–time curve (40).
FVC maneuvers that have lower PEFvalues compared with others in a sessionmay produce higher FEV1 values due to thenegative effort dependence of flow. Thetechnician should coach forceful initiationof the FVC maneuver (i.e., blast), to achievethe fastest/highest PEF (41). Rounded peakson the flow–volume curve may reflectsubmaximal blasts that can increasevariability in both FVC and FEV1.
Lung VolumesQuality review of lung volume measurementis more challenging as a variety ofmethods areavailable, including body plethysmography,nitrogen washout, helium dilution, andradiographic imaging. We are not aware ofany quality-grading systems that have beenvalidated for the measurement of absolutelung volumes. Until a validated system isavailable, we recommend adherence tothe 2005 ATS/ERS recommendations for themeasurement of lung volumes (3). If theacceptability and/or repeatability criteria arenot met but these data are reported, acomment should be included to caution usersof the test results.
Diffusing Capacity (Transfer Factor)The DLCO (or TLCO) test is complex,involving a number of technical factors,and variability can be high. In the absenceof quality-grading systems that have been
Table 2. Spirometry Test Acceptability Requirements for Adults and for Children
1. A good start of exhalation with extrapolated volume, 5% of FVC or 0.150 L, whichever isgreater (For age 2–6, extrapolated volume, 12.5% of FVC or 0.080L)
2. Free from artifacts
3. No cough during first second of exhalation (for FEV1)
4. No glottis closure or abrupt termination (for FVC)
5. No early termination or cutoff (for FVC). Timed expiratory volumes can be reported inmaneuvers with early termination, but FVC should be reported only with qualification. (Forage 2–6, if cessation of effort occurs at greater than 10% of peak flow, then the maneuvershould be classified as showing premature termination; although timed expiratoryvolumes can be reported in maneuvers with early termination, FVC should not)
6. Maximal effort provided throughout the maneuver
7. No obstructed mouthpiece
FVC and FEV1 are each considered separately for acceptability. FEV1 acceptability does not consideranything after the first second, whereas FVC does. The adult acceptability criteria extend to childrenage 7 or greater. Information on adults and children age 7 or greater is based on Reference 2.Information on children aged 2 to 6 is based on Reference 39.
Table 1. Quality Categories for FVC or FEV1 in Adults and Children
Grade Criteria for Adults and Older Children and for Children Aged 2–6 Years
A >3 acceptable tests with repeatability within 0.150 Lfor age 2–6, 0.100 L, or 10% of highest value, whichever is greater
B >2 acceptable tests with repeatability within 0.150 Lfor age 2–6, 0.100 L, or 10% of highest value, whichever is greater
C >2 acceptable tests with repeatability within 0.200 Lfor age 2–6, 0.150 L, or 10% of highest value, whichever is greater
D >2 acceptable tests with repeatability within 0.250 Lfor age 2–6, 0.200 L, or 10% of highest value, whichever is greater
E One acceptable test
F No acceptable tests
FVC or FEV1 are each graded separately. The quality categories for FVC and FEV1 are the same, but the definition of an acceptable curve differs in that FEV1acceptability does not consider anything after the first second, whereas FVC does (see Table 2). The adult quality criteria extend to children age 7 or greater.Information on adults and children age 7 or greater is based on Reference 2. Information on children aged 2 to 6 is based on Reference 39.
AMERICAN THORACIC SOCIETY DOCUMENTS
1470 American Journal of Respiratory and Critical Care Medicine Volume 196 Number 11 | December 1 2017

validated using the new recommendations(6), a grading scheme based on maneuveracceptability is proposed (Table 3). Theaverage DLCO value from at least two gradeA DLCO maneuvers that are repeatablewithin 2 ml/min/mm Hg, or 0.67mmol/min/kPa, should be reported. If onlyone grade A maneuver is acquired, theDLCO value from that maneuver is reported.If only maneuvers with grades B to D areavailable, DLCO values from these might stillhave clinical utility; therefore the average ofthe two best graded of these maneuversshould be reported, but this must be notedto caution the interpreter of the test results.Maneuvers with grade F are not usable.
The Quality ReviewerIn the clinical pulmonary functionlaboratory, technicians, supervisors/managers, or computer software canassign quality grades, whereas in theclinical research setting, an independentquality reviewer is commonly used. Thisreviewer should be an expert in pulmonaryfunction testing and have extensiveexperience, both in direct testing and inmonitoring testing performed by others.If more than one reviewer is used,comparisons across reviewers should bedone to ensure consistency, for example,with a blinded sample of good and bad testsessions.
Conclusions
The ATS PFT Committee believes that wideadoption of the formats presented above andtheir underlying principles by equipmentmanufacturers and pulmonary functionlaboratories can improve the interpretation,communication, and understanding of testresults. Limiting the number of parametersreported and showing the LLN next to themeasured value should improve interpretiveaccuracy, particularly for those less experienced.Consistency in the order of important dataand reserving the word percent to percentpredicted value should reduce errors. Showingthe measured values relative to the normaldistribution in a simple linear graphic (with orwithout reporting a z-score) can enhanceunderstanding of the result. Newer referencevalues for spirometry expand the applicableage range and ethnicities and eliminatetroublesome jumps between equations duringgrowth. New international (albeit only white)reference values for diffusing capacity will helpto resolve a long-standing problem. Qualityreview of PFTs needs to move beyond “did, ordid not, meet ATS standards,” but a gradingsystem is most helpful if the grades have acommon meaning; therefore adoption of auniform system is desirable. n
This official technical statement was prepared by an ad hoc subcommittee of the ATS Committee on Proficiency Standards forPulmonary Function Laboratories.
Members of the subcommittee are as follows:BRUCE H. CULVER, M.D. (Chair)ALLAN L. COATES, M.D. (Co-Chair)CRISTINE E. BERRY, M.D., M.H.S.PATRICIA K. CLARKE, R.R.T., R.P.F.T.BRIAN L. GRAHAM, PH.D.TEAL S. HALLSTRAND, M.D., M.P.H.JOHN L. HANKINSON, PH.D.DAVID A. KAMINSKY, M.D.NEIL R. MACINTYRE, M.D.MEREDITH C. MCCORMACK, M.H.S., M.D.
MARGARET ROSENFELD, M.D., M.P.H.SANJA STANOJEVIC, PH.D.JACK WANGER, M.SC., R.R.T., R.P.F.T.DANIEL J. WEINER, M.D.
Author Disclosures: D.A.K. served asa speaker for MGC Diagnostics. N.M.served as a consultant for Alana, BreatheTechnologies, InspiRx Pharmaceuticals, andVentec; and as a speaker for Medtronic.
M.M. received research support fromBoehringer Ingelheim Pharmaceuticals;and received royalties for authorship fromUpToDate. J.W. served as a speakerand consultant for MGC Diagnostics; as aconsultant for Vitalograph; and on anadvisory committee for Methapharm. B.H.C.,C.E.B., P.K.C., A.L.C., B.L.G., T.S.H., J.H.,M.R., S.S., and D.J.W. reported norelationships with relevant commercialinterests.
References
1. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R,Coates A, van der Grinten CP, Gustafsson P, Hankinson J, et al.Interpretative strategies for lung function tests. Eur Respir J 2005;26:948–968.
2. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A,Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al.; ATS/ERSTask Force. Standardisation of spirometry. Eur Respir J 2005;26:319–338.
3. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F,Casaburi R, Crapo R, Enright P, van der Grinten CP, et al.Standardisation of the measurement of lung volumes. Eur Respir J2005;26:511–522.
4. Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP,Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, et al.Standardisation of the single-breath determination ofcarbon monoxide uptake in the lung. Eur Respir J 2005;26:720–735.
5. Culver BH. How should the lower limit of the normal range be defined?Respir Care 2012;57:136–145, discussion 143–145.
6. Graham BL, Brusasco V, Burgos F, Cooper BG, Jensen R, Kendrick A,MacIntyre NR, Thompson BR, Wanger J. 2017 ERS/ATS standards forsingle-breath carbon monoxide uptake in the lung. Eur Respir J 2017;49:1600016.
7. Hildon Z, Allwood D, Black N. Impact of format and content of visualdisplay of data on comprehension, choice and preference: asystematic review. Int J Qual Health Care 2012;24:55–64.
Table 3. Quality Grading for DLCO Maneuvers
Grade VI/VC Breathhold Time Sample Collection
A >90%* 8–12 s <4 s
B >85% 8–12 s <4 s
C >80% 8–12 s <5 s
D >80% ,8 or .12 s <5 s
F Any test not meeting Grade A, B, C, or D.
Definition of abbreviations: DLCO = diffusing capacity of the lung for carbon monoxide; VC = largestvital capacity in the same test session; VI = inspired volume.*Or VI/VC> 85% and VA within 0.200 L or 5% of VA from another acceptable maneuver.
AMERICAN THORACIC SOCIETY DOCUMENTS
American Thoracic Society Documents 1471

8. Vedal S, Crapo RO. False positive rates of multiple pulmonary functiontests in healthy subjects. Bull Eur Physiopathol Respir 1983;19:263–266.
9. Quanjer PH, Hall GL, Stanojevic S, Cole TJ, Stocks J; Global LungsInitiative. Age- and height-based prediction bias in spirometryreference equations. Eur Respir J 2012;40:190–197.
10. Coates AL, Graham BL, McFadden RG, McParland C, Moosa D,Provencher S, Road J; Canadian Thoracic Society. Spirometry inprimary care. Can Respir J 2013;20:13–21.
11. Levy ML, Quanjer PH, Booker R, Cooper BG, Holmes S, Small IR.Diagnostic spirometry in primary care: proposed standards forgeneral practice compliant with American Thoracic Society andEuropean Respiratory Society recommendations. Prim Care Respir J2009;18:130–147.
12. Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, Enright PL,Hankinson JL, Ip MSM, Zheng J, et al.; ERS Global Lung FunctionInitiative. Multi-ethnic reference values for spirometry for the 3–95 yrage range: the global lung function 2012 equations. Eur Respir J 2012;40:1324–1343.
13. Quanjer PH, Weiner DJ, Pretto JJ, Brazzale DJ, Boros PW.Measurement of FEF25–75% and FEF75% does not contribute toclinical decision making. Eur Respir J 2014;43:1051–1058.
14. Lukic KZ, Coates AL. Does the FEF25–75 or the FEF75 have any value inassessing lung disease in children with cystic fibrosis or asthma?Pediatr Pulmonol 2015;50:863–868.
15. Subbarao P, Lebecque P, Corey M, Coates AL. Comparison ofspirometric reference values. Pediatr Pulmonol 2004;37:515–522.
16. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference valuesfrom a sample of the general U.S. population. Am J Respir Crit CareMed 1999;159:179–187.
17. Kiefer EM, Hankinson JL, Barr RG. Similar relation of age and height tolung function among whites, African Americans, and Hispanics. Am JEpidemiol 2011;173:376–387.
18. Coates AL, Wong SL, Tremblay C, Hankinson JL. Reference equationsfor spirometry in the Canadian population. Ann Am Thorac Soc 2016;13:833–841.
19. Quanjer PH, Brazzale DJ, Boros PW, Pretto JJ. Implications of adoptingthe Global Lungs Initiative 2012 all-age reference equations forspirometry. Eur Respir J 2013;42:1046–1054.
20. Brazzale DJ, Hall GL, Pretto JJ. Effects of adopting the new global lungfunction initiative 2012 reference equations on the interpretation ofspirometry. Respiration 2013;86:183–189.
21. Linares-Perdomo O, Hegewald M, Collingridge DS, Blagev D, Jensen RL,Hankinson J, Morris AH. Comparison of NHANES III and ERS/GLI 12for airway obstruction classification and severity. Eur Respir J 2016;48:133–141.
22. Quanjer PH, Weiner DJ. Interpretative consequences of adopting theGlobal Lungs 2012 reference equations for spirometry for childrenand adolescents. Pediatr Pulmonol 2014;49:118–125.
23. Miller MR. Spirometry in primary care. Prim Care Respir J 2009;18:239–240.
24. Culver B. Defining airflow limitation and chronic obstructive pulmonarydisease: the role of outcome studies. Eur Respir J 2015;46:8–10.
25. Miller MR, Quanjer PH, Swanney MP, Ruppel G, Enright PL. Interpretinglung function data using 80% predicted and fixed thresholdsmisclassifies more than 20% of patients. Chest 2011;139:52–59.
26. Brazzale D, Hall G, Swanney MP. Reference values for spirometry andtheir use in test interpretation: a position statement from theAustralian and New Zealand Society of Respiratory Science.Respirology 2016;21:1201–1209.
27. Swanney MP, Miller MR. Adopting universal lung function referenceequations. Eur Respir J 2013;42:901–903.
28. Miller MR. Choosing and using lung function prediction equations. EurRespir J 2016;48:1535–1537.
29. Stanojevic S, Graham BL, Cooper BG, Thompson BR, Carter KW,Francis RW, Hall GL; Global Lung Function Initiative TLCO WorkingGroup; Global Lung Function Initiative (GLI) TLCO. Official ERStechnical standards: Global Lung Function Initiative reference valuesfor the carbon monoxide transfer factor for Caucasians. Eur Respir J2017;50:1700010.
30. Gutierrez C, Ghezzo RH, Abboud RT, Cosio MG, Dill JR, Martin RR,McCarthy DS, Morse JLC, Zamel N. Reference values of pulmonaryfunction tests for Canadian Caucasians. Can Respir J 2004;11:414–424.
31. Enright PL, Johnson LR, Connett JE, Voelker H, Buist AS. Spirometry inthe lung health study. 1. Methods and quality control. Am Rev RespirDis 1991;143:1215–1223.
32. Banks DE, Wang ML, McCabe L, Billie M, Hankinson J. Improvementin lung function measurements using a flow spirometer thatemphasizes computer assessment of test quality. J Occup EnvironMed 1996;38:279–283.
33. Stoller JK, Buist AS, Burrows B, Crystal RG, Fallat RJ, McCarthy K,Schluchter MD, Soskel NT, Zhang R; a-1 Antitrypsin DeficiencyRegistry Study Group. Quality control of spirometry testing in theregistry for patients with severe a1-antitrypsin deficiency. Chest1997;111:899–909.
34. Pellegrino R, Decramer M, van Schayck CPO, Dekhuijzen PN, TroostersT, van Herwaarden C, Olivieri D, Del Donno M, De Backer W,Lankhorst I, et al. Quality control of spirometry: a lesson from theBRONCUS trial. Eur Respir J 2005;26:1104–1109.
35. Goss CH, McKone EF, Mathews D, Kerr D, Wanger JS, Millard SP;Cystic Fibrosis Therapeutics Development Network. Experienceusing centralized spirometry in the phase 2 randomized, placebo-controlled, double-blind trial of denufosol in patients with mild tomoderate cystic fibrosis. J Cyst Fibros 2008;7:147–153.
36. Perez-Padilla R, Vazquez-Garcıa JC, Marquez MN, Menezes AMB;PLATINO Group. Spirometry quality-control strategies in amultinational study of the prevalence of chronic obstructivepulmonary disease. Respir Care 2008;53:1019–1026.
37. Enright P, Vollmer WM, Lamprecht B, Jensen R, Jithoo A, Tan W,Studnicka M, Burney P, Gillespie S, Buist AS. Quality of spirometrytests performed by 9893 adults in 14 countries: the BOLD Study.Respir Med 2011;105:1507–1515.
38. Hankinson JL, Eschenbacher B, Townsend M, Stocks J, Quanjer PH.Use of forced vital capacity and forced expiratory volume in 1second quality criteria for determining a valid test. Eur Respir J 2015;45:1283–1292.
39. Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P,Bisgaard H, Davis GM, Ducharme FM, Eigen H, et al.; AmericanThoracic Society/European Respiratory Society Working Group onInfant and Young Children Pulmonary Function Testing. An officialAmerican Thoracic Society/European Respiratory Society statement:pulmonary function testing in preschool children. Am J Respir CritCare Med 2007;175:1304–1345.
40. Haynes JM, Kaminsky DA. The American Thoracic Society/EuropeanRespiratory Society acceptability criteria for spirometry: asking toomuch or not enough? Respir Care 2015;60:e113–e114.
41. Enright PL. How to make sure your spirometry tests are of good quality.Respir Care 2003;48:773–776.
AMERICAN THORACIC SOCIETY DOCUMENTS
1472 American Journal of Respiratory and Critical Care Medicine Volume 196 Number 11 | December 1 2017

Primary Care Asthma Program SPIROMETRY MANUAL Resource Links:
ATS:
ATS/ERS Task Force Standardisation of Lung Function Testing: Standardisation of spirometry (2005):
https://www.thoracic.org/statements/resources/pft/PFT2.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: General considerations for lung function
testing (2005): https://www.thoracic.org/statements/resources/pft/PFT1.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: Interpretative strategies for lung function
tests (2005): https://www.thoracic.org/statements/resources/pft/pft5.pdf
ATS/ERS Task Force Standardisation of Lung Function Testing: Standardisation of the measurement of
lung volumes (2005): https://www.thoracic.org/statements/resources/pft/pft3.pdf
ATS/ERS Recommendations for a Standardized Pulmonary Function Report (2017):
https://www.thoracic.org/statements/resources/pft/standardized-pulmonary-function-report.pdf
CPSO:
Independent Health Facilities Clinical Practice Parameters and Facility Standards: Diagnostic Spirometry
and Flow Volume Loop Studies – 4rd Edition, June 2014:
http://www.cpso.on.ca/CPSO/media/documents/CPGs/IHF/Pulmonary-Function-Studies.pdf
Independent Health Facilities Clinical Practice Parameters and Facility Standards: Pulmonary Function
Studies – 3rd Edition, April 2008:
http://www.cpso.on.ca/uploadedFiles/policies/guidelines/facilties/PulmonaryFunction08.pdf
CTS:
Spirometry in Primary Care:
http://www.respiratoryguidelines.ca/sites/all/files/CTS_Spirometry_Primary_Care_2013.pdf
Infection Control:
Infection Prevention and Control for Clinical Office Practice (Provincial Infectious Disease Advisory
Committee): http://www.cpso.on.ca/Policies-Publications/CPGs-Other-Guidelines/Other-
Guidelines/Infection-Prevention-and-Control-for-Clinical-Offi
Practicum:
The Lung Association Provider Education Program (PEP)
http://www.olapep.ca
Resptrec Spirotrec course (endorsed by the CTS, CLA and the FPAGC):
http://www.resptrec.org/spirotrec.php




















![Welcome [lapublichealth.org]lapublichealth.org/mch/asthmacoalition/docs/Meeting... · Spirometry Basics Future webinars will include: AE-C prep webinar, Exercise Induced bronchialspasms/asthma](https://img.dokumen.tips/doc/110x75/5f09152e7e708231d4252627/welcome-spirometry-basics-future-webinars-will-include-ae-c-prep-webinar-exercise.jpg)








