Embed Size (px)
Citation preview

Aneta Manda-Handzlik


Detoxification:ammonia
Synthesis of proteins, including albumins and clotting factors
Heme methabolism
Stores iron and copper
Production of bile:digestion and absorptionof fats


It is more useful to run severaltests to create a biochemicalprofile of changes, as sensitivityof single tests may be very low
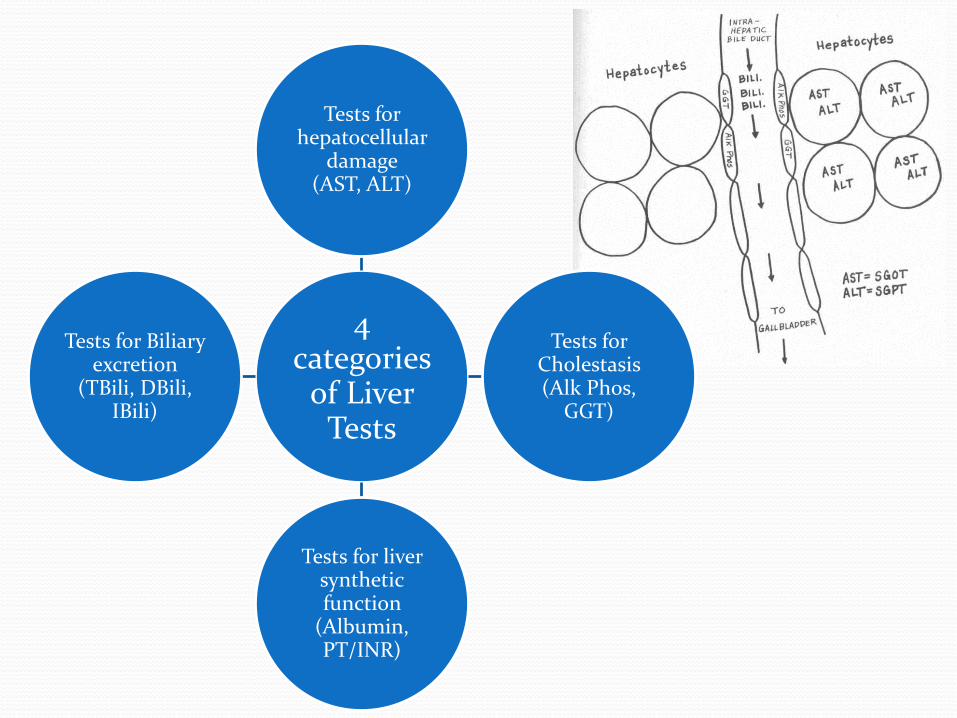
4 categories
of LiverTests
Tests for hepatocellular
damage(AST, ALT)
Tests for Cholestasis(Alk Phos,
GGT)
Tests for liversyntheticfunction
(Albumin, PT/INR)
Tests for Biliaryexcretion
(TBili, DBili, IBili)

Aminotransferases Physiological role:
Transfer of amino- groups from one carbon skeleton to another
ALT = GPT
AST = GOT

intracellular enzymes
not tissue-specific
ALT AST

Reference ranges
AST in adults: ALT in adults:
8-45 U/l 10-40 U/l
Elevated in:
Cholestasis, cirrhosis, biliary obstruction, hepatitis, hepatic ischemia, hepatic necrosis, liver cancer, statin theraphy!
AST
ALT

There are two ways of looking at ALT and AST as markers helpfulto assess the etiology of liver abnormalities:
De Ritis ratio =𝐴𝑆𝑇
𝐴𝐿𝑇
normally approximately 1 : 1
alcohol - induced hepatitis, cirrhosis, metastaticcancer of the liver, disorders affecting otherorgans: myocardial infarction, muscle injury
viral hepatitis, hemochromatosis, autoimmunehepatitis

The degree of increase in AT levels
>25 (>50) fold increase
ischemic and toxic liver injury
10-fold increase
acute hepatitis
3-4-fold increase
chronic hepatitis, cirrhosis
2-3 fold increase
obstructiveproblem

Biliru
bin
Breakdown of heme to bilirubin occurs in macrophages of the
rethiculoendothelial system (tissuemacrophages, spleen, and liver)

JaundiceReference values, total bilirubin: < 1 mg/dl, unconjugatedbilirubin 70-85%
Jaundice: total bilirubin >2-3 mg/dl
Liver function: bilirubin
conjugation and secretion
Hepatocellular
The flow of
bileObstructive
hemolytic anemia:
sickle cell anemia, pyruvate kinase or glucose 6-phosphate dehydrogenase deficiency, malaria
viral hepatitis
gallstones
stricture
tumors: gallbladder, bile duct, cancer of the head of pancreas
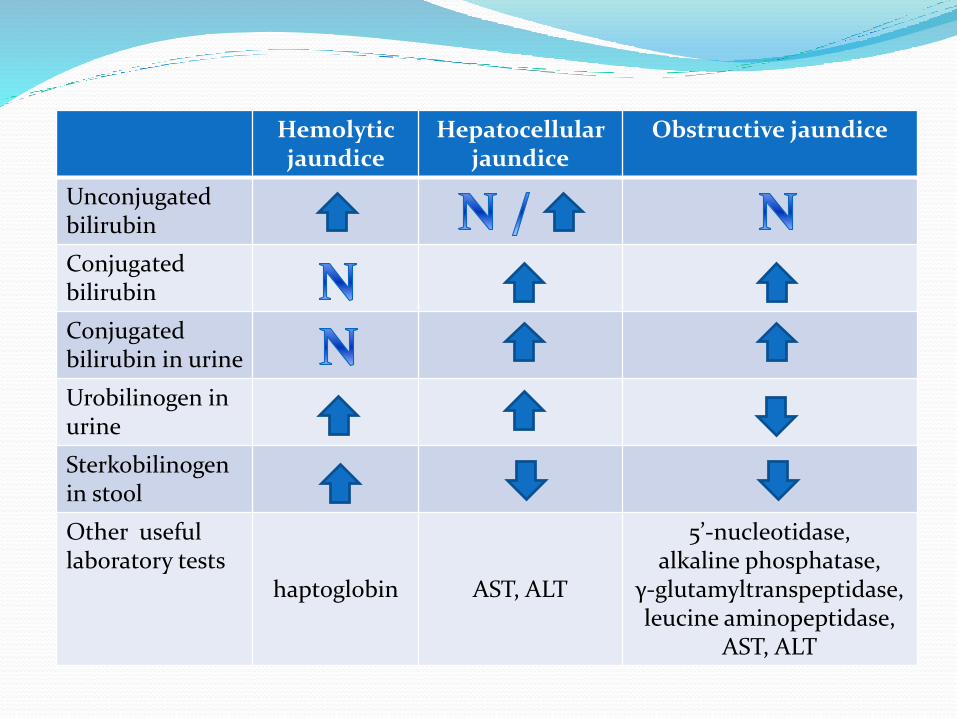
Hemolyticjaundice
Hepatocellularjaundice
Obstructive jaundice
Unconjugatedbilirubin
Conjugatedbilirubin
Conjugatedbilirubin in urine
Urobilinogen in urine
Sterkobilinogenin stool
Other usefullaboratory tests
haptoglobin AST, ALT
5’-nucleotidase, alkaline phosphatase,
γ-glutamyltranspeptidase, leucine aminopeptidase,
AST, ALT
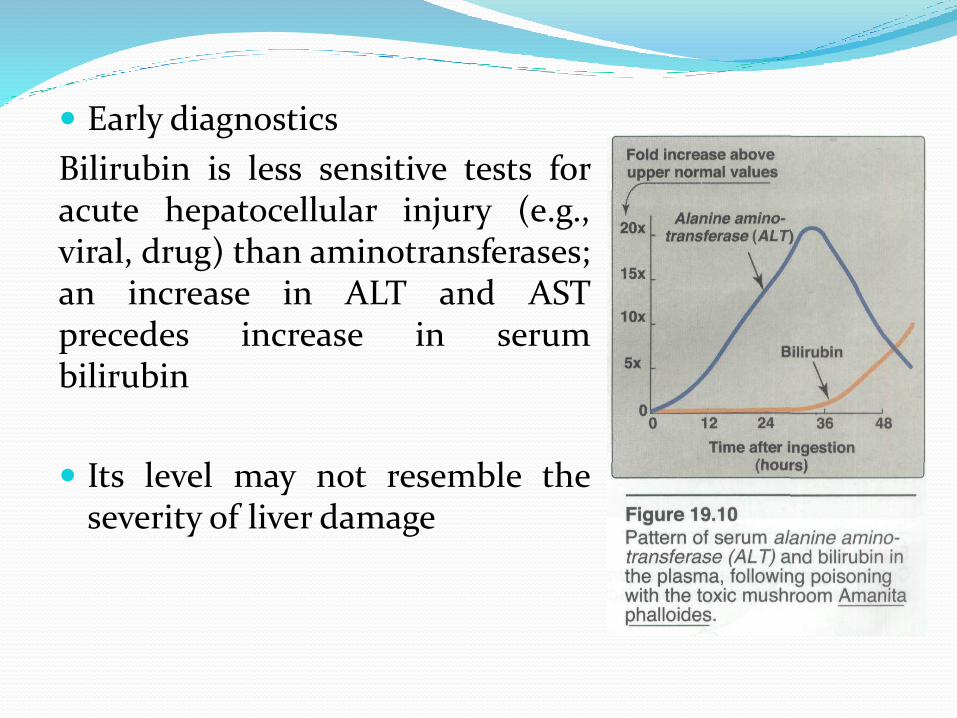
Early diagnostics
Bilirubin is less sensitive tests foracute hepatocellular injury (e.g.,viral, drug) than aminotransferases;an increase in ALT and ASTprecedes increase in serumbilirubin
Its level may not resemble theseverity of liver damage

Amanita phalloides, also known as the death cap
Widely distributed across Europe

Concentrations above 5 mg/dl are rarely observed in hemolysis with no complications
Bilirubin levels are lower in hepatocellular jaundicethan in obstructive conditions
Bilirubin levels are higher when obturation is causedby cancer than in obturation related to gallstones
In viral hepatitis higher concentrations of bilirubin indicate more severe liver damage and longer course

Blood tests Hemolysis of the blood sample will alter test
results.
Exposure to sunlight or artificial light for >=1hour will decrease the bilirubin content of thesample.
Testing with contrast media within 24 hourswill alter test results.
Drugs may increase (i.a. anabolic steroids, oralcontraceptives, ascorbic acid, diuretics) ordecrease (barbiturates, salicylates, penicillin) total bilirubin

Urine tests
False positive:
phenothiazines, salicylates
False negative:
ascorbic acid.
Exposure of the specimen to light may affect test results.

Alkaline phosphatase(markers of cholestasis)
Family of enzymes - hydrolysis of a large variety of phosphate esters at an alkaline pH

The methods for separation of isoforms/isoensymes include:
o Electrophoretic mobility
o Heat stability test
„bone burns, liver lasts”
Exists in multiple forms (isoforms, isoenzymes)

Reference ranges:
35–120 IU/L
Pregnant women
appears at 16th–20th week of normal pregnancy, increases progressively to two times normal up to onset
of labor
Infant and children
1.0–2.0 times adult levels

Elevated in:
o Liver dysfunction: obstruction of bile flow – cholestasiscirrhosis, hepatitis
o Opioids
o Bone diseases: Paget’s disease, cancer metastatic to the bone
o Eclampsia
o Cancers: Regan isoensyme, e.g. cancer of the lung, breast, colon, pancreas, ovary and cervical cancers
Decreased in:hypothyroidism, excessive vitamin D intake, malnutrition

Limitations of the test:
Day-to-day variation is 5–10%.
Recent food ingestion can increase as much as 30 U/L.
ALP is 10-15% higher in African Americans
25% higher with increased BMI, 10% higher withsmoking, 20% lower with the use of oral contraceptives.
Blood levels elevated:e.g. penicillin derivatives, antihistamines and cardiovascular drugs.

Gamma-glutamyltranspeptidase(markers of cholestasis)
Where?
Most sensitive enzymaticindicator of cholestasis
Often measured alongwith AlkalinePhosphatase
Normal range:≥16 years: 7–50 U/l

Alcoholic abuse and alcoholic hepatitis
24 hours of abstinence prior to test
Elevated in:
Cholecystitis, cholangitis, cholelithiasis biliaryobstruction
Liver metastases, hepatitis, cirrhosis
Acute pancreatitis, pancreatic cancer, renal cancer, myocardial infarction, some cases of carcinoma of the prostate

Normal in pregnancy and children older than 3 monthsof age; may aid in differential diagnosis of hepatobiliarydisease occurring during pregnancy and childhood
The test has several limitations:
o day-to-day variations are 10-15%
o 25–50% increase with higher BMI
o 25% lower during early pregnancy.

5’-nucleotidase(markers of cholestasis)
Membrane-bound enzyme found only in liver cells and cells of the bile duct
Normal values:
2-8 U/l
Testing in conjuction with ALP to differentiate between hepatobiliary diseases and bone diseases
Not as subject to drug induction as GGT and ALP
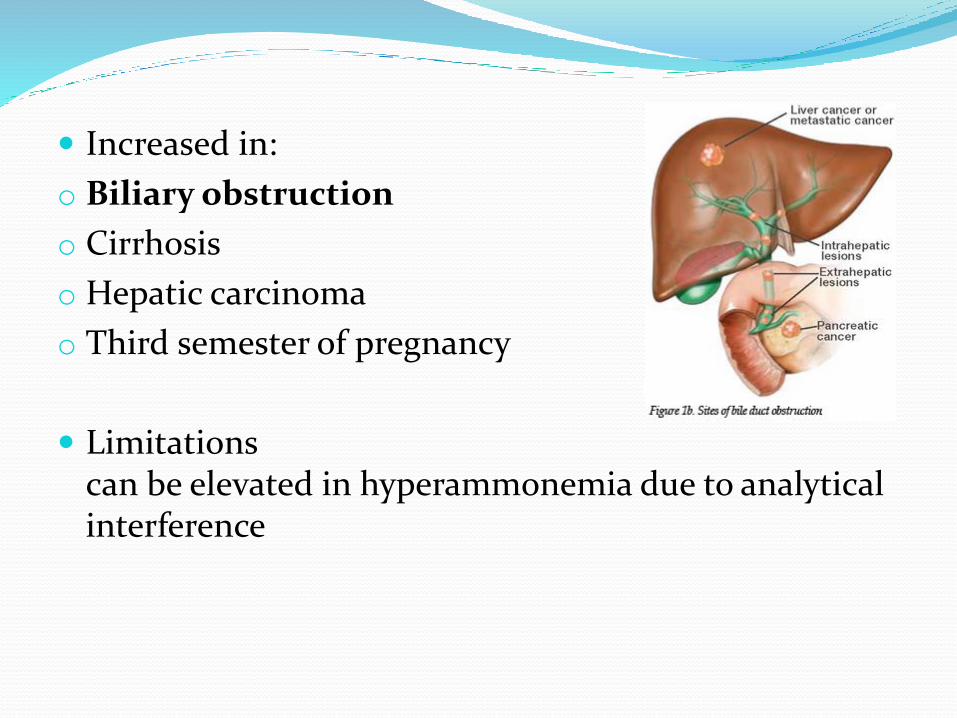
Increased in:
o Biliary obstruction
o Cirrhosis
o Hepatic carcinoma
o Third semester of pregnancy
Limitationscan be elevated in hyperammonemia due to analyticalinterference

Leucine aminopeptidase (LAP)(markers of cholestasis)
Exopeptidase that catalyzes the hydrolysis of amino acid residues from the amino terminus of polypeptide chains
Normal values:
Female: 75–185 U/mL
Male: 80–200 U/mL

Increased in:
o Obstruction of bile duct, cirrhosis, hepatic carcinomaless sensitive indicator of liver disease than other liver enzymes
o Pancreatic carcinoma
o Indicator of SLE activity
o Pregnancy
Measured also in urine
Ammonia
Derived mostly from protein degradation
Most of the ammonia in the blood comes from the intestine
Urea cycle (liver): conversion to urea
Normal values:
16–65 μmol/l

Indicator of the ability of the liver to detoxify ammonia
Increased in:
o inborn errors of metabolism (e.g. defects in urea cycle)
o severe liver disease - increased in most cases of hepatic coma but correlates poorly with degree of encephalopathy
o Smoking, strenous exercise
o GI hemorrhage
o Renal failure

High-protein diet may cause increased levels.
The blood is put into a heparinizedtube and packed in ice for transport tothe laboratory. The specimen is stableonly for about 20 minutes.
Ammonia increases due to cellular metabolism:20% in 1 hour and 100% by 2 hours.
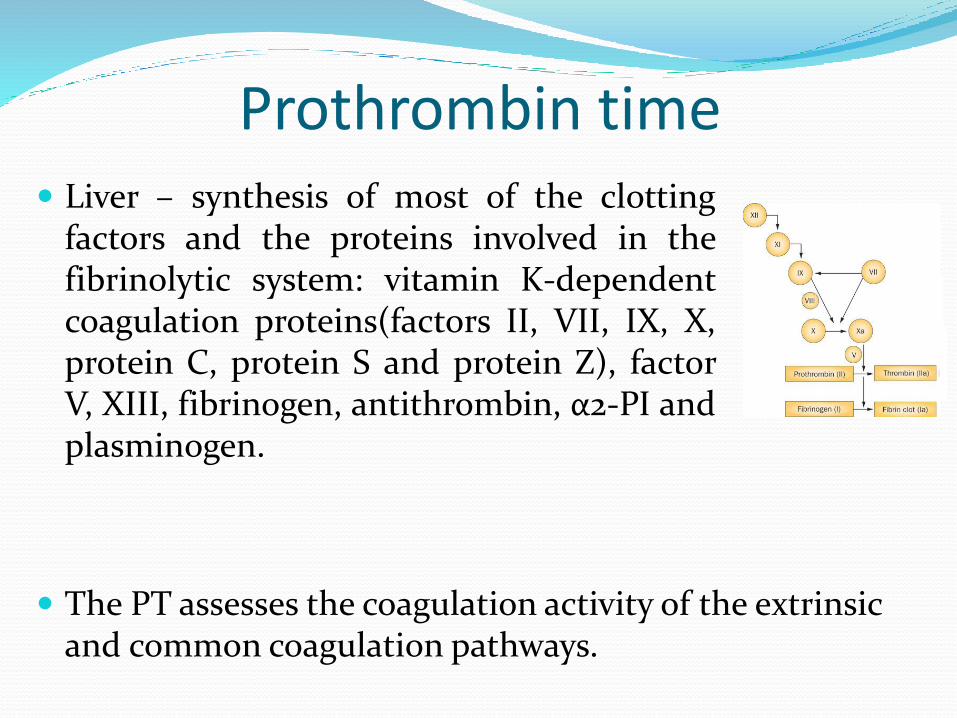
Prothrombin time
The PT assesses the coagulation activity of the extrinsic and common coagulation pathways.
Liver – synthesis of most of the clottingfactors and the proteins involved in thefibrinolytic system: vitamin K-dependentcoagulation proteins(factors II, VII, IX, X,protein C, protein S and protein Z), factorV, XIII, fibrinogen, antithrombin, α2-PI andplasminogen.

Marked prolongation of the PT in liver disease indicates advanced disease. PT is a good indicator of severity of acute liver disease.
In mild liver disease, the PT is prolonged, but the aPTTis usually normal. As the liver disease progresses, both PT and aPTT levels are prolonged
Chronic liver disease:Standard coagulation tests such as prothrombin time (PT) and activatedpartial thromboplastin time (aPTT) may not reflect the true coagulationstatus of patients with liver cirrhosis. These tests do not take into accountthe activation of the primary endogenous anticoagulant protein C, levels ofwhich are considerably reduced in cirrhosis.

Total serum protein and albumin
Synthesis of most plasma proteins; albumin is totallysynthesized by the liver
Indicator of severity of chronic liver disease - it takesseveral weeks of lack of production before the albuminlevel decreases.
The most common reason for lowered levels is cirrhosis

Hepatitis viridae
ALT and AST are very high
Bilirubin, alkaline phosphatase and GGT rise later in course, only mildly elevated

serological markers:
IgM – active disease
IgG – protective
HAV

HBV
disease?(live virus)
protective,immunity, no activedisease
high infectivity
not protective,how old is the infection?
low infectivity

Hepatitis B: HBsAg anti-HBsAg HBeAg anti-HBeAg anti-HBcAg
Acute + - + - IgM
Chronic(high infectivity)
+ - + - IgG
Chronic(lowinfectivity)
+ - - + IgG
Recovery - + - + IgG
Immunized - + - - -

HCV Serologic assays
HCV Ab test – initial test, does not differentiatebetween current and past infection
Genetic tests:
o HCV RNA qualitative
o HCV RNA quantitative – Viral Load
o viral genotyping

Case # 1 19 y/o female college student
c/o severe fatigue of new onset, jaundice, mild pruritus of few days duration
No EtOH
Meds: minocycline, multivit
No Hx. of contacts with viral hepatitis
PE: heent: mild scleral icterusabd: nl bs, no organomegaly, no tenderness orpalpable mass

Lab tests results:
albumin 4.2 g/dl 3.5-5 g/dl
total bilirubin 4.2 mg/dl <1 mg/dl
ALP 248 IU/l 35–120 IU/l
AST 180 U/l 8-45 U/l
ALT 252 U/l 10-40 U/l
Hgb 13.1 12-16 g/dl
Hct 36% 37-47%
Wbc 5.2 x 103/μl 4-10 x 103/μl
Platelets 210 x 103/μl 150-450 x 103/μl
Acute viral hepatitis serologies neg.
What is the most likely diagnosis?

Answer & Clinical Questions
Drug induced cholestasis secondary to minocycline.
Symptoms resolved within 2 weeks of drug d/c, liver profile normalized in 8 weeks.
What is the most common cause of Drug Induced Liver Injury (DILI)?
Is this cause more often intentional or unintentional?

Acetaminophen (paracetamol) is the most commoncause of drug induced liver injury
The majority of cases are unintentional
Poor understanding that the drug is contained in many different medications

Case # 2 53 year old female Recent bowel and ovarian cancer 30g alcohol per day Polyarthritis Bilirubin 15 mg/dl <1 mg/dl ALT 743 U/l 10-40 U/l AST 417 U/l 8-45 U/l
ALP 68 IU/l 35–120 IU/l GGT 42 U/l 7-50 U/l Globulins 54 g/l 23-35 g/l Alb, INR, Platelets normal

Old liver tests:
Bilirubin normal
ALT 200‐700
AST 100‐400
ALP <200
GGT <200
US normal
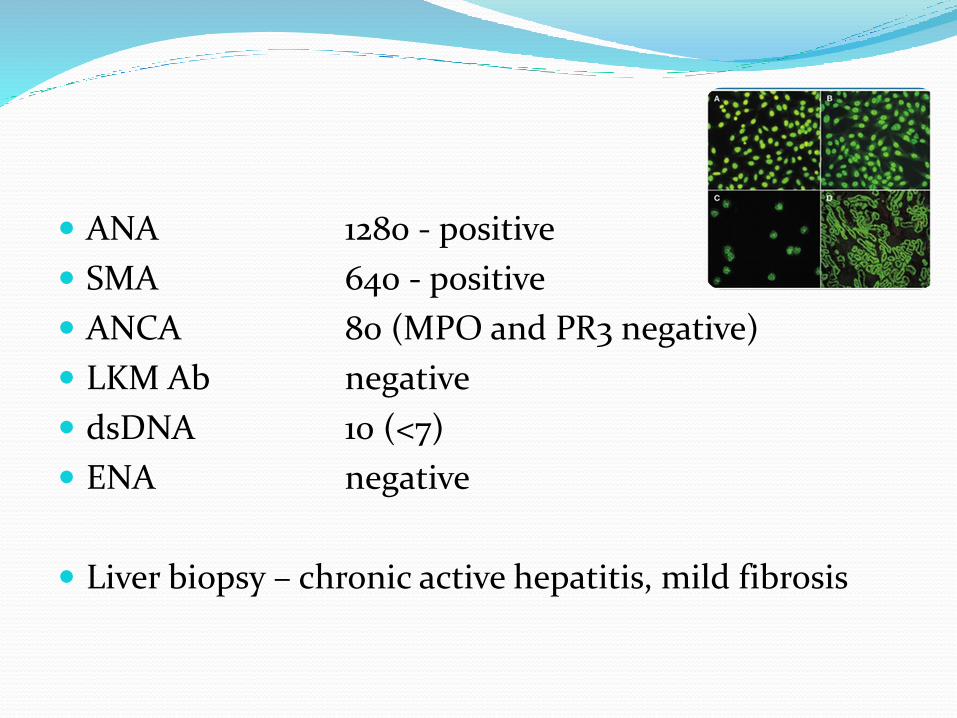
ANA 1280 - positive
SMA 640 - positive
ANCA 80 (MPO and PR3 negative)
LKM Ab negative
dsDNA 10 (<7)
ENA negative
Liver biopsy – chronic active hepatitis, mild fibrosis

Diagnosis
Type 1 autoimmune hepatitis
Settled with prednisone and azathioprine

Aneta Manda-Handzlik
Amylase A hydrolase that degrade complex carbohydrates into
fragments
In healthy persons, 40% of total serum amylase is pancreatic type and 60% is salivary type
Normal values:
Adult: 53–123 U/L
Elderly: Slightly higher norms
Acute pancreatitis Increase in serum begins in 3–6 hours, reaches
maximum in 20–30 hours, and may persist for 48–72hours
The magnitude of the elevation does not correlate withthe severity of the disease or prognosis
Amylase >3× ULN is very suggestive of acutepancreatitis
Of patients with acute alcoholic intoxication, 10–40%have elevated serum amylase (about half are salivarytype), but increased serum amylase is usually <3×URL.

Increased in:
Pancreatic disease:Pancreatitis, pancreatic trauma, cancer of the pancreas(P-AMY)
Intraabdominal diseases other than pancreatitisPerforated peptic ulcer, (P-AMY), biliary tract disease (P-AMY), gastritis (P-AMY), acute appendicitis
Genitourinary disease:Ovarian malignancy (S-AMY), ectopic, ruptured tubal pregnancy(S-AMY), renal insufficiency (mixed)
Others:Mumps (S-AMY), diabetic ketoacidosis (S-AMY), postoperative hyperamylasemia, acute alcoholic abuse (S-AMY) P -pancreatic, S – salivary isoensyme

1% of randomly selected patients with no specificsymptoms or disease states may have elevated amylaseresults
Macroamylase - Complex of amylase (usually S-AMY)with IgA, IgG, or other high molecular weight plasmaproteins that cannot be filtered through theglomerulus due to its large size and is thus retained inplasma
Identification: special gel filtration orultracentrifugation technique. Serum lipase is normal,urine amylase may be normal or low
Macroamylasemia – in vivo artifact

Amylase in urine
Useful after the acute peak in the serum hasdiminished
A minimum of a 2-hour urine collection, a 24-hour urine collection, or a variety of other timeperiods
To avoid the problem of timed urine specimen:ratio of amylase clearance to creatinine clearance
Begins elevation Peaks Duration
Serum amylase 3-6 hours 20-30 hours 2-3 days
Urinary amylase 6-10 hours varies 1-2 weeks
Limitations When healthcare workers talk over an uncovered urine
or blood sample, this can falsely elevate total amylaselevels.
Normal in patients with hypertriglyceridemia (technical interference with test)
Frequently normal in acute alcoholic pancreatitis

Lipase breaks down fat into glycerol and fatty acids
Acute pancreatitis:
increases in the blood 4-8 hours after the onset of thedisease, increases to a greater extent and remains elevatedup to 14 days longer than amylase
lipase ≥5× upper reference limit
Pancreatitis highly likely

Lipase : amylase ratio >3 (especially >5) alcoholicrather than nonalcoholic pancreatitis
Increased in:
o Acute pancreatitis
o Perforated or penetrating peptic ulcer
o Obstruction of the pancreatic duct, also drug-inducedobstruction after drugs, such as opiates
o Diabetic ketoacidosis
o Acute and chronic renal failure
Pancreatic elastase (elastase-1) Serine endopeptidase
extraordinarily stable during its passage through the GI tract its concentration in stool accuratelyreflects the amount of enzyme secreted
Highly specific and sensitive diagnostic test
Stool or serum, immunoenzymatic assay

Indications:Stool - diagnosis or exclusion of pancreatic exocrine
insufficiency:
o chronic pancreatitis
o Cystic Fibrosis
o diabetes mellitus
Serum- diagnosis or exclusion of:
o acute pancreatitis
o inflammatory episode of chronic pancreatitis

Diabetes
Goals of laboratory testing are:
o to screen for high blood glucose levels to detect and diagnose diabetes and prediabetes
o to determine the type of diabetes
o to monitor glucose levels over time
o to detect and monitor complications

The role of laboratory in diabetes
Screening, preclinical stage:
o Genetic markers: HLA-DR 3 and HLA DR-4
o Immunological markers: ICAM – islet cell cytoplasmic autoantibodiesGADA – glutamic acid decarboxylase autoantibodiesIA-2-A – insulinoma-associated-2-autoantibodiesIAA – insulin autoantibodies
o Glucose concentration
o Concentration of insulin

Clinical stage:
o Glucose concentration
o Oral glucose tolerance test
o Ketone bodies – urine, blood
o Others: insuline, C-peptide
Treatment follow-up, acute stages:
o Glucose concentration – urine, blood
o Ketone bodies, blood and urine
o Acid-base balance
o Lactate
o Electrolites – ions, osmolality

Treatment follow-up, chronic phase:
o Glucose concentration – blood, urine
o Glycated proteins
o Assessment of complications – lipids, creatinine,microalbuminuria, proteinuria
o Assessment of pancreas transplantation – insulin,C-peptide

Random plasma glucose/ casual plasmaglucose
measures blood glucose regardless of the timewhen a patient last ate
Fasting plasma glucose
measures blood glucose after a patient has not eaten for at least 8 hours
2–h plasma glucose(OGTT – Oral GlucoseTolerance Test)
venous plasma glucose 2–h after ingestion of 75g oral glucose load
3.9-5.5 mmol/l (70-99 mg/dl) = normal fastingglucose
< 140 mg/dl(7.8 mmol/l) = normal glucose tolerance
5.6-6.9 mmol/l (100-125 mg/dl) = impaired fastingglucose (IFG)
≥7.8 and <11.1mmol/l(140mg/dl and 200mg/dl)= impaired glucosetolerance (IGT)
≥ 11.1 mmol/l (200 mg/dl ) + symptoms, like polyuria, polydipsia, polyphagia) = diabetes
≥7.0mmol/l (126mg/dl) = diabetes*
≥11.1mmol/l (200mg/dl) = diabetes
Methods and criteria for diagnosing diabetes
prediabetes
*twice

How to diagnose diabetes? Your patient is a 48-year old man, whose mother
suffered from diabetes
During routine testing of the patient’s blood youdiscovered, that fasting plasma glucose is 6.2 mmol/l (111.6 mg/dl).
You decided to repeat the test and the result is as follows: 6.7 mmol/l (120.6 mg/dl)
Do you diagnose your patient with diabetes? What would be the nextlaboratory test you run?

Glucose concentration
Total error for this test is ≤ 7.9% and intrapersonalvariation ~ 7%
24-hour rhythm: peak in the mornig;
Plasma glucose concentration is 11% higher thanwhole blood glucose concentration

Falsely elevated glucose level Falsely lowered glucose level
Glucose concentration ex vivo falls approximately by5-7%/1 hour due to glycolysis, especially in blood withincreased amount of leukocytes and bacterialcontamination

Glucose in urine
Semi-quantitative methods – test strips
Low precision when glucose concentration is low
High rate of false-negative results
Falsely negative:
o vitamin C
o ketones
o salicylates

Hemoglobin A1c
Human hemoglobins: HbA, HbA2, HbF
Chromatographic analysis: fast hemoglobins, glycatedhemoglobins; HbA1a, 1b and 1c
As glucose combines with Hb continuously and nearly irreversibly during the life span of RBC, glycated Hbwill be proportional to mean plasma glucose level during previous 2-3 months
Lifespan – 120 days, continually being replaced
HbA1c level ≠ a simple average of the blood glucose level for 4 months
HbA1c = a weighted average of the glucose level over the last few months.
The blood glucose levels for the last month count themost, about one-half the total amount.

How often?ADA Polish Diabetological Association
The test is used for monitoring long-term blood glucose level control in patients with diabetes.

The relationship between A1C and eAG is described by the formula:
28.7 X A1C – 46.7 = eAG
Accordingly to American Diabetes Association (ADA) 2017 recommendations, A1c in (most) nonpregnantadults with diabetes should be below 7%.
mg/dl%

Pros:
o 8-hour fasting prior to test is not necessary
o Lower intrapersonal variation (2%) than the variation ofglucose (7%)
o Direct relationship between HgbA1c level anddevelopment of diabetic complications
Cons:
o Decreased in shortened RBC life span (e.g. blood loss,hemolytic anemias, sickle cell anemia and thalassemia)
o Decreased following transfusion
o Greater cost than FPG/OGTT
o Genetic variation in hemoglobin glycation

A1C≥6.5% (48 mmol/mol)The test should be performed in a laboratory usinga method that is NGSP certified and standardizedto the DCCT reference assay.
Hemoglobin A1c for the diagnosis of diabetes - ADA 2018
Fructosamine
Describes serum proteins that have been glycated
Reflects the mean glucose concentration in bloodover recent period (2–3 weeks)
The test is useful when glycated Hb cannot be used
should be compared with previous values in thesame patient rather than reference range

Inexpensive test
Usually used in pregnant women with diabetes
High rate of false positives
Low sensitivity
Sensitive to variations in the composition of the sample protein

Glycated albumin
Reflects the mean glucose concentration in blood over period of 17-21 days
Specificity and sensitivity: GA > fructosamine
Results: GA/albumin
No fasting required

Pregnancy: HbA1c exhibitsbiphasic changes, decreasingbetween the first and secondtrimester and increasing inthe third
GA or fructosamine offersadvantages over HbA1c ingestational diabetes mellitus.

Ketone bodiesGlucose unable to enter the cell
Metabolism of fatty acids for energy
Acetoacetic acid, acetone and betahydroxybutyric acidare formed and excreted in the urine
BHB present in the greatest concentration, but notdetectable by common tests with nitroprusside andnegative nitroprusside test result does not rule outketoacidosis





























