Embed Size (px)
Citation preview
Preventing venous thromboembolism
during pregnancy and postpartum
Prof. Anne Angelillo-Scherrer
Department and Central Laboratory of Hematology
Inselspital, Bern University Hospital
Bern, Switzerland
SAOA 2019 - SPRING MEETINGNEUCHATEL
Saturday – March 16th, 2019
Overview
• Introduction
•Risk assessment and patient’s perspective
•Choice of the anticoagulant
•Bleeding risk under anticoagulation duringpregnancy
•Thrombophilia
•Antiphospholipid syndrome
•Take home message

Venous thromboembolism (VTE) and pregnancy
• VTE may manifest as:− Pulmonary embolism (PE)
− Deep vein thrombosis (DVT)
• VTE complicates 0.5-2.2 per 1000 deliveries
• During pregnancy, the risk of VTE increases 5- to 10-fold (comparedto non-pregnant women)
• The risk is higher in postpartum− greatest during the first 3-6 weeks
− Daily-risk is increased 15- to 35-fold (compared to non-pregnant women)
• VTE, an important cause of maternal morbidity and mortality
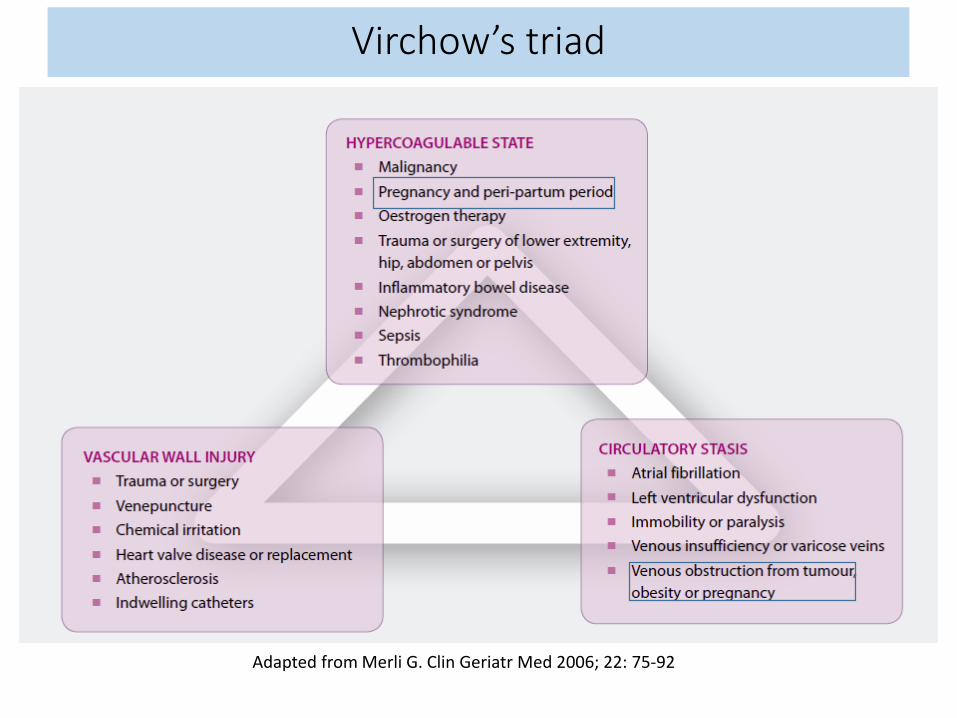
Adapted from Merli G. Clin Geriatr Med 2006; 22: 75-92
Virchow’s triad
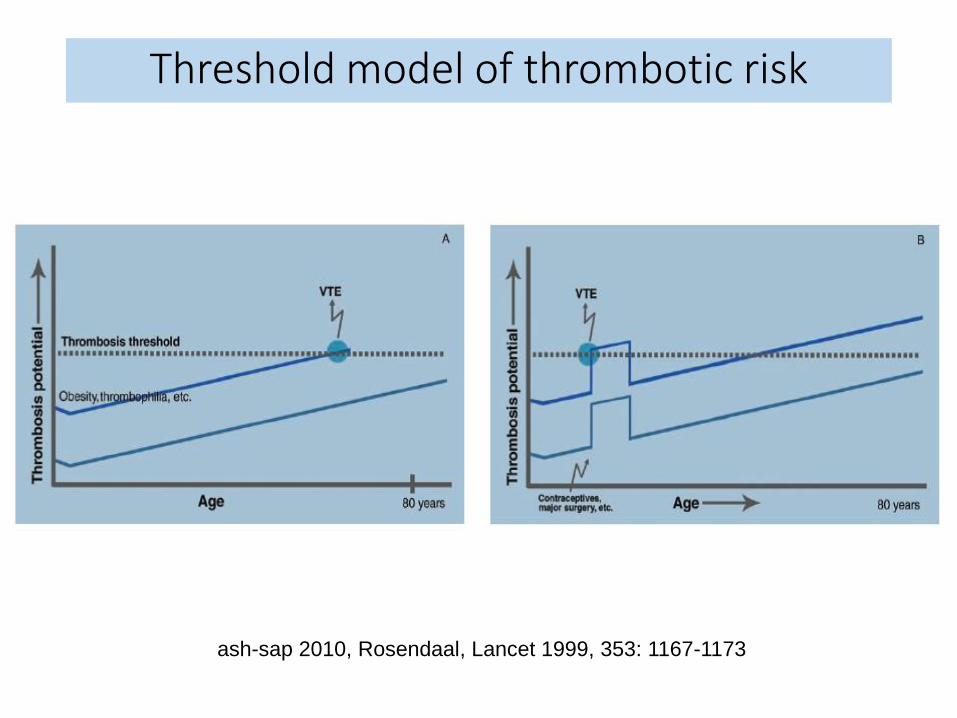
ash-sap 2010, Rosendaal, Lancet 1999, 353: 1167-1173
Threshold model of thrombotic risk
• 10th week of pregnancy
• Past history of DVT 10 days after hip and pelvis surgery(post-traumatic) 3 years ago
• No risk factor
• No thrombophilia testing
• No current anticoagulation
What is your proposition for the current pregnancy?
Case # 1: 35 year-old woman
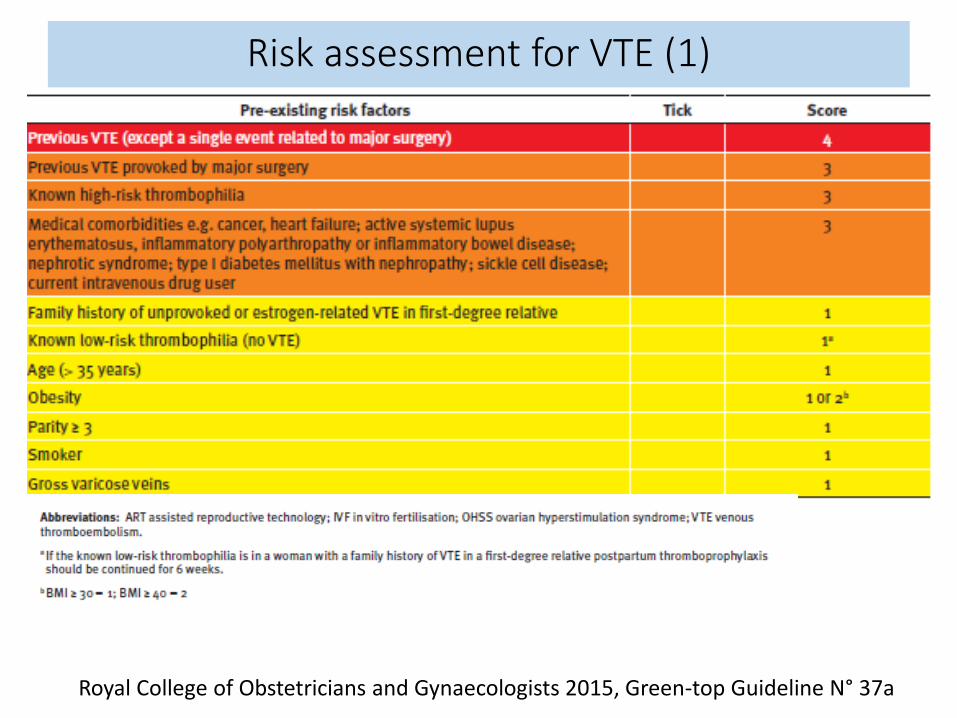
Risk assessment for VTE (1)
Royal College of Obstetricians and Gynaecologists 2015, Green-top Guideline N° 37a

Risk assessment for VTE (2)
Royal College of Obstetricians and Gynaecologists 2015, Green-top Guideline N° 37a
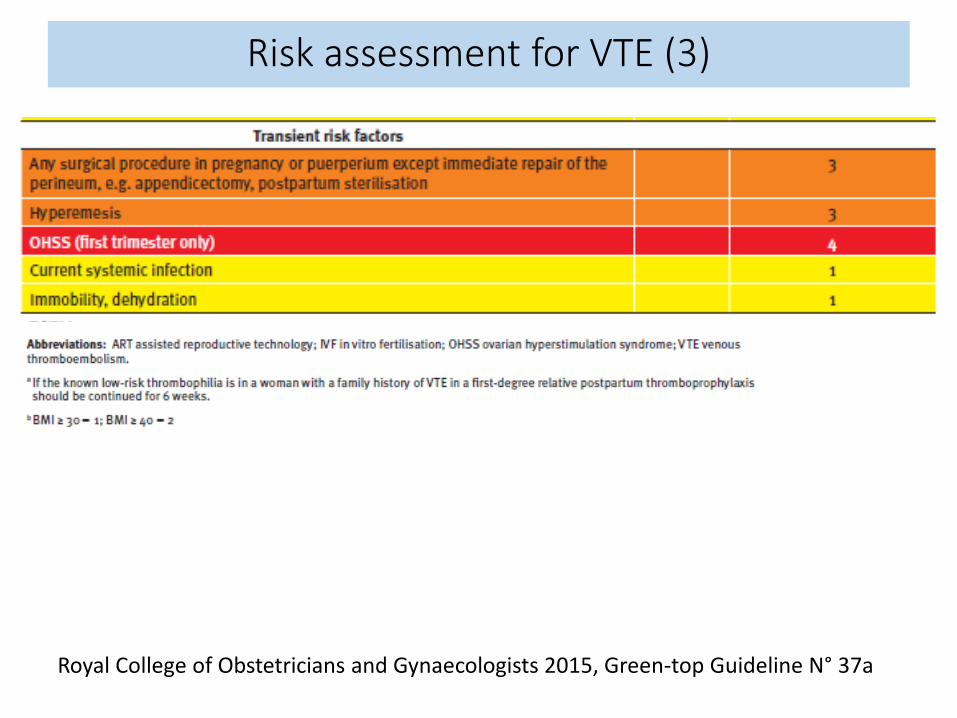
Risk assessment for VTE (3)
Royal College of Obstetricians and Gynaecologists 2015, Green-top Guideline N° 37a
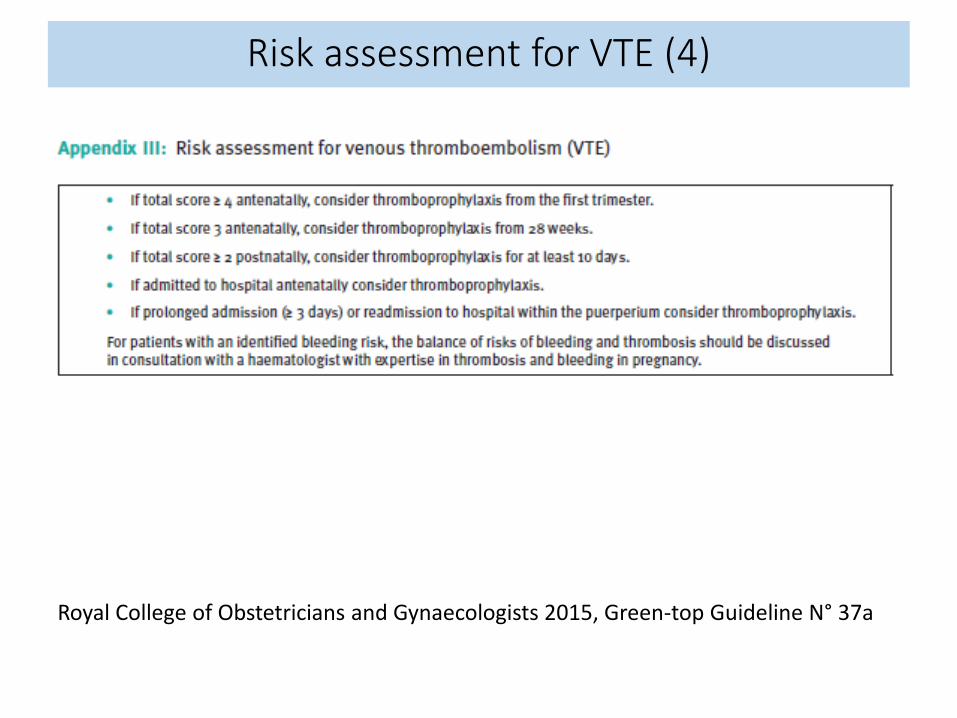
Risk assessment for VTE (4)
Royal College of Obstetricians and Gynaecologists 2015, Green-top Guideline N° 37a

Other guidelines
•Pregnant women with prior VTE who are not receiving long-term anticoagulation should receive6 weeks of postpartum prophylaxis
•Antepartum prophylaxis should be considered in pregnancy women with prior unprovoked VTE orpregnancy- or oestrogen-related VTE not receivinglong-term anticoagulation
Obstet Gynecol 2011, 118:718-729; J Obstet Gynaecol 2014, 36:527-53; Chest2012, 141:e419S-e3494S
• 11th week of pregnancy
• Past history of DVT 1 month after starting with oral contraception11 years ago
• No current anticoagulation
• No family history of VTE
What is your proposition for the current pregnancy?
Case # 2: 30 year-old woman
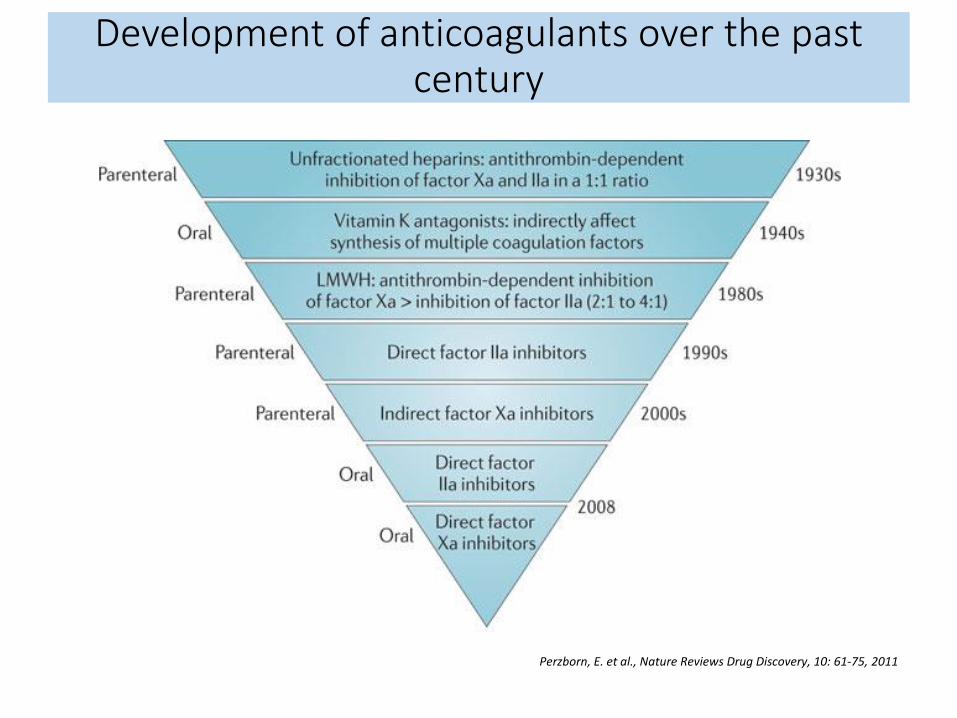
Perzborn, E. et al., Nature Reviews Drug Discovery, 10: 61-75, 2011
Development of anticoagulants over the pastcentury

Perzborn, E. et al., Nature Reviews Drug Discovery, 10: 61-75, 2011
Target of anticoagulants
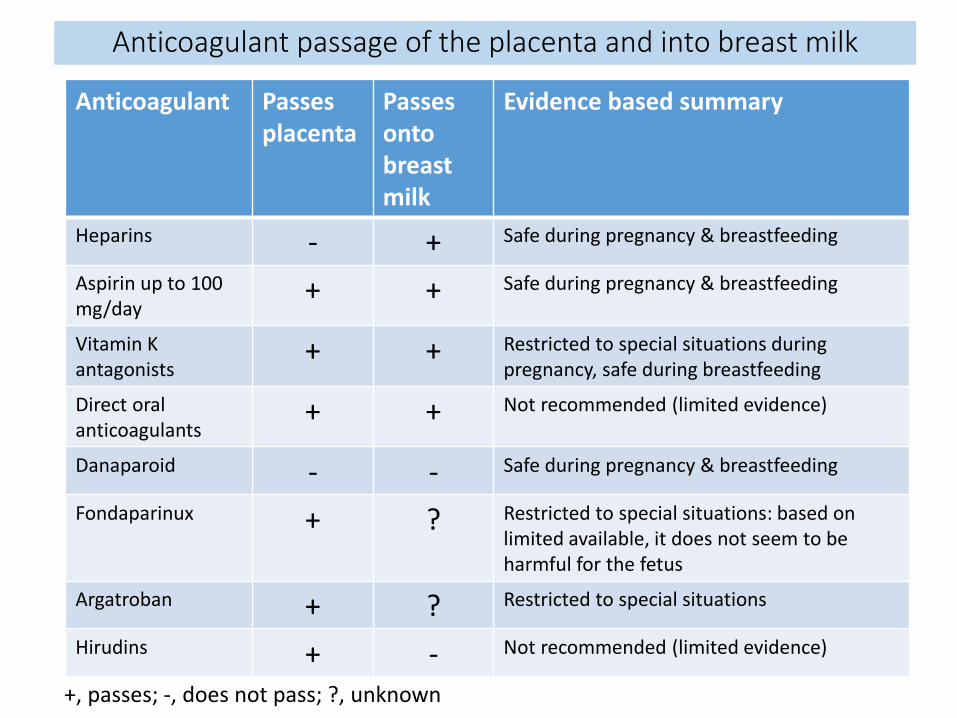
Anticoagulant Passes placenta
Passesontobreastmilk
Evidence based summary
Heparins - + Safe during pregnancy & breastfeeding
Aspirin up to 100 mg/day
+ + Safe during pregnancy & breastfeeding
Vitamin K antagonists
+ + Restricted to special situations duringpregnancy, safe during breastfeeding
Direct oral anticoagulants
+ + Not recommended (limited evidence)
Danaparoid - - Safe during pregnancy & breastfeeding
Fondaparinux + ? Restricted to special situations: based on limited available, it does not seem to beharmful for the fetus
Argatroban + ? Restricted to special situations
Hirudins + - Not recommended (limited evidence)
+, passes; -, does not pass; ?, unknown
Anticoagulant passage of the placenta and into breast milk

• 7th week of pregnancy
• Past history of bilateral, central PE 2 years ago
• Risk factor: oral contraception
• Current anticoagulation: Lixiana® (Edoxaban) 60 mg/day
What is your recommendation for the anticoagulation duringpregnancy?
What would you have been proposed during the pre-conception counseling?
Case # 3: 22 year-old woman

• Pre-conception counseling on the risk for both woman and fetus is key
• If using DOACs switch to VKA pre-pregnancy
• Perform pregnancy test immediately after missed menstrual period, re-assess frequently if negative
• If pregnancy test positive: switch to LMWH immediately and prescribe oral vitamin K
Preconception management of women alreadyusing anticoagulants when planning pregnancy
• Heparins
• Aspirin up to 100 mg/day
• Danaparoid
• Fondaparinux
Which anticoagulants/antithrombotics are safe in pregnancy ?
• Vitamin K antagonists (VKA)
• Direct oral anticoagulants (DOACs)
Which anticoagulants are not safe in pregnancy?

•7th week of pregnancy
•Past history of bilateral, central PE 2 years ago
•Risk factor: oral contraception
•Current anticoagulation: Lixiana® (Edoxaban) 60 mg/day
•Past history of heparin-induced thrombocytopenia
What is your recommendation for theanticoagulation during pregnancy?
Case # 3: 22 year-old woman
•At suspicion, switch to non-heparin anticoagulantdrug: first choice = danaparoid
•Consider or rule out the diagnosis, and manage appropriately
•Possible other non-heparin anticoagulant drugs, depending on the clinical situation−Fondaparinux−Argatroban
Heparin-induced thrombocytopenia & pregnancy

• Inform all women about measures to be taken regarding theiranticoagulant therapy and discuss delivery options (spontaneaousdelivery, induction, elective caesarean section, CS)
• Discontinue LMWH when contractions start or membranes rupture
• Last dose of low prophylactic dose LMWH at least 12h prior toplanned delivery/CS
• Last dose of higher doses LMWH at least 24h prior to planneddelivery
• Blood analysis: CBC, creatinin, PT, aPTT, TT, fibrinogen, anti-Xa activity
• Unfractionated heparin IV, therapeutic dosage in cases with high riskfor VTE recurrence, to be interrupted 4h before delivery; startprogressive anticoagulation 6-8h after delivery with preferentiallyLMWH
Peripartal management
• Low
• Increases with the intensity of the anticoagulation
• Highest at the time of delivery
• Be carefull in case of thrombocytopenia
Bleeding risk under anticoagulation during pregnancy
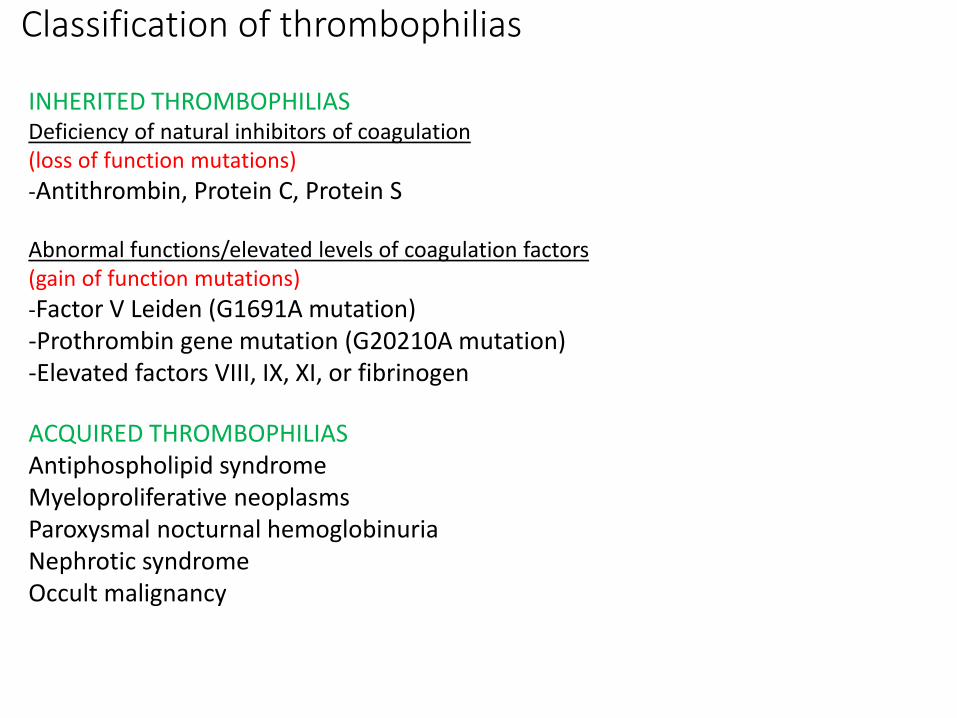
Classification of thrombophilias
INHERITED THROMBOPHILIASDeficiency of natural inhibitors of coagulation(loss of function mutations)
-Antithrombin, Protein C, Protein S
Abnormal functions/elevated levels of coagulation factors(gain of function mutations)
-Factor V Leiden (G1691A mutation)-Prothrombin gene mutation (G20210A mutation)-Elevated factors VIII, IX, XI, or fibrinogen
ACQUIRED THROMBOPHILIASAntiphospholipid syndromeMyeloproliferative neoplasmsParoxysmal nocturnal hemoglobinuriaNephrotic syndromeOccult malignancy

The American College of Obstetricians and Gynecologists, Practice Bulletin Number197, 2018, 132:e18-e34
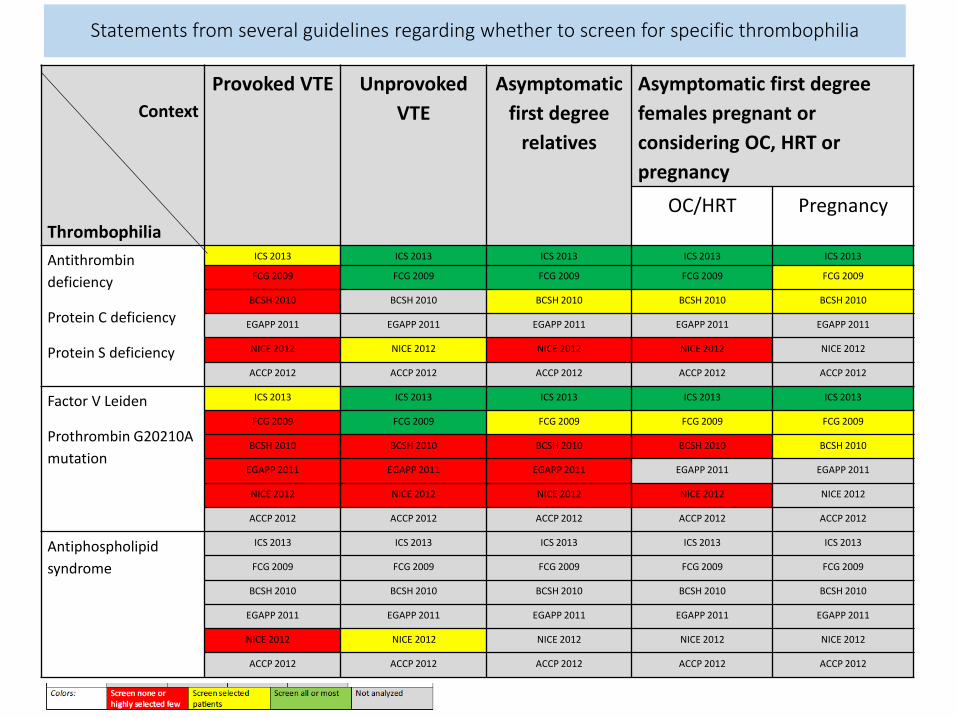
Context
Thrombophilia
Provoked VTE Unprovoked
VTE
Asymptomatic
first degree
relatives
Asymptomatic first degree
females pregnant or
considering OC, HRT or
pregnancy
OC/HRT Pregnancy
Antithrombin
deficiency
Protein C deficiency
Protein S deficiency
ICS 2013 ICS 2013 ICS 2013 ICS 2013 ICS 2013
FCG 2009 FCG 2009 FCG 2009 FCG 2009 FCG 2009
BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010
EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011
NICE 2012 NICE 2012 NICE 2012 NICE 2012 NICE 2012
ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012
Factor V Leiden
Prothrombin G20210A
mutation
ICS 2013 ICS 2013 ICS 2013 ICS 2013 ICS 2013
FCG 2009 FCG 2009 FCG 2009 FCG 2009 FCG 2009
BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010
EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011
NICE 2012 NICE 2012 NICE 2012 NICE 2012 NICE 2012
ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012
Antiphospholipid
syndrome
ICS 2013 ICS 2013 ICS 2013 ICS 2013 ICS 2013
FCG 2009 FCG 2009 FCG 2009 FCG 2009 FCG 2009
BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010 BCSH 2010
EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011 EGAPP 2011
NICE 2012 NICE 2012 NICE 2012 NICE 2012 NICE 2012
ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012 ACCP 2012
Statements from several guidelines regarding whether to screen for specific thrombophilia
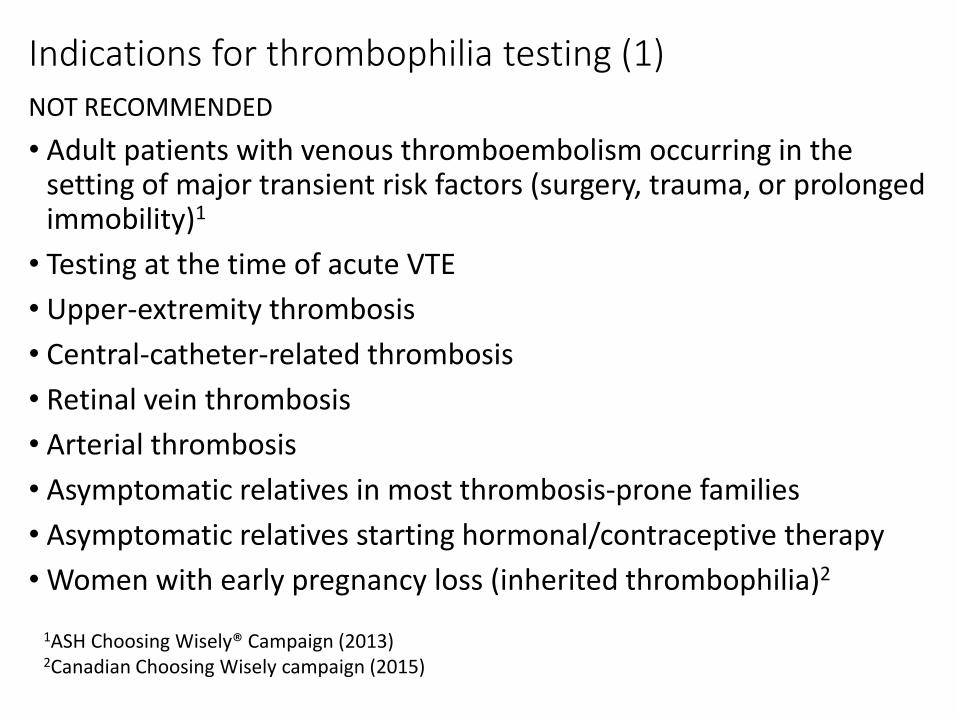
Indications for thrombophilia testing (1)
NOT RECOMMENDED
• Adult patients with venous thromboembolism occurring in the setting of major transient risk factors (surgery, trauma, or prolonged immobility)1
• Testing at the time of acute VTE
• Upper-extremity thrombosis
• Central-catheter-related thrombosis
• Retinal vein thrombosis
• Arterial thrombosis
• Asymptomatic relatives in most thrombosis-prone families
• Asymptomatic relatives starting hormonal/contraceptive therapy
• Women with early pregnancy loss (inherited thrombophilia)2
1ASH Choosing Wisely® Campaign (2013)2Canadian Choosing Wisely campaign (2015)
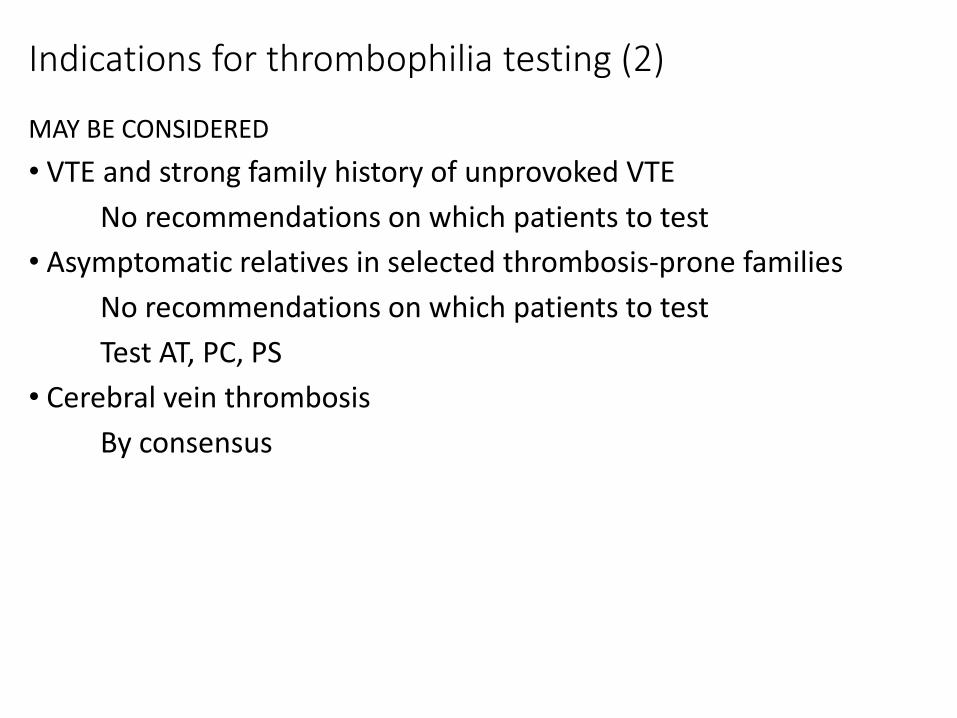
Indications for thrombophilia testing (2)
MAY BE CONSIDERED
• VTE and strong family history of unprovoked VTE
No recommendations on which patients to test
• Asymptomatic relatives in selected thrombosis-prone families
No recommendations on which patients to test
Test AT, PC, PS
• Cerebral vein thrombosis
By consensus

Indications for thrombophilia testing (3)
RECOMMENDED
• Patients who develop skin necrosis while on AVKTest PC and PS only, after AVK is discontinued
• Intra-abdominal vein thrombosisScreening for MPN (JAK2 mutation, calreticulin) recommended, other testing may beconsidered
• Patients with clinical clues of antiphospholipid syndromeTest for antiphospholipid antibodies (lupus anticoagulant, anticardiolipin antibodies, anti-beta-2 glycoprotein I antibodies)

What to test ?
Risk factors Screening testsConfirmation
tests
CBC, PT and aPTT are performed together with the thrombophilia screning. PTT-LA, PTT lupus sensitive; dRVVT, diluted Russel viper venom time.
Antithrombin deficiency Antithrombin activity Antithrombin antigen Unfractionated heparin, LMWH, liver
insufficiency, DIC, nephrotic syndrome
Protein C deficiency Protein C activity Chromogenic and
antigenic protein C
VKA, vitamin K deficiency, liver insufficiency,
DIC
Protein S deficiency Free protein S Total and coagulant
protein S
VKA, vitamin K deficiency, liver insufficiency,
DIC
pregnancy, estrogen
Factor V Leiden Factor V Leiden (PCR)
Prothrombin mutation Prothrombin mutationG20210A (PCR)
Lupus anticoagulant 2 tests: for ex.: PTT-LA
and dRVVT. Lupus
anticoagulant is present
when one of the test is
positive.
Resistance to activated
protein C (APCR)
Anticoagulants: heparin inlfuences PTT-LA and
VKA prolong dRVVT ; before12 weeks
after an acute thromboembolic event
Anticardiolopin
antibodies
ELISA (isotypes IgG &
IgM)
Prothrombin mutation
(PCR)
Before12 weeks
after an acute thromboembolic event
Anti-2-glycoprotein 1
antibodies
ELISA (isotypes IgG &
IgM)
Before12 weeks
after an acute thromboembolic event
Hyperhomocysteinemia Fasten homocystein level
To avoid in the
following conditions
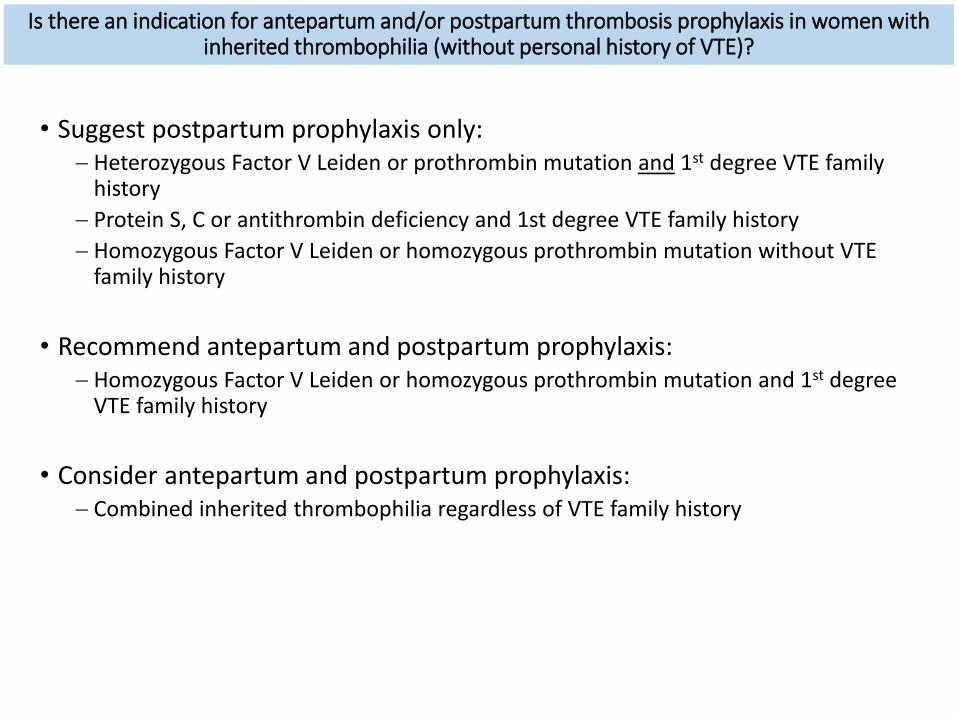
• Suggest postpartum prophylaxis only:− Heterozygous Factor V Leiden or prothrombin mutation and 1st degree VTE family
history
− Protein S, C or antithrombin deficiency and 1st degree VTE family history
− Homozygous Factor V Leiden or homozygous prothrombin mutation without VTE family history
• Recommend antepartum and postpartum prophylaxis:− Homozygous Factor V Leiden or homozygous prothrombin mutation and 1st degree
VTE family history
• Consider antepartum and postpartum prophylaxis:− Combined inherited thrombophilia regardless of VTE family history
Is there an indication for antepartum and/or postpartum thrombosis prophylaxis in women withinherited thrombophilia (without personal history of VTE)?
• Consider and discuss in women at high VTE risk, i.e. those withsimilar risk factors as considered for antepartum prophylaxis
• Recommend to use prophylaxis dose LMWH for 3 months in severeovarian hyperstimulation syndrome
Is there an indication for antepartum and/or postpartum thrombosis prophylaxis in womenundergoing assisted reproductive technology?

Garcia, D. & Erkan, D. , NEJM, 2018, 378:2010-21
Overview of the initial pathogenesis

Ruiz-Irastorza, G. et al., Lancet, 2010, 376:1498-1509
Pathogenesis of thrombosis in APS
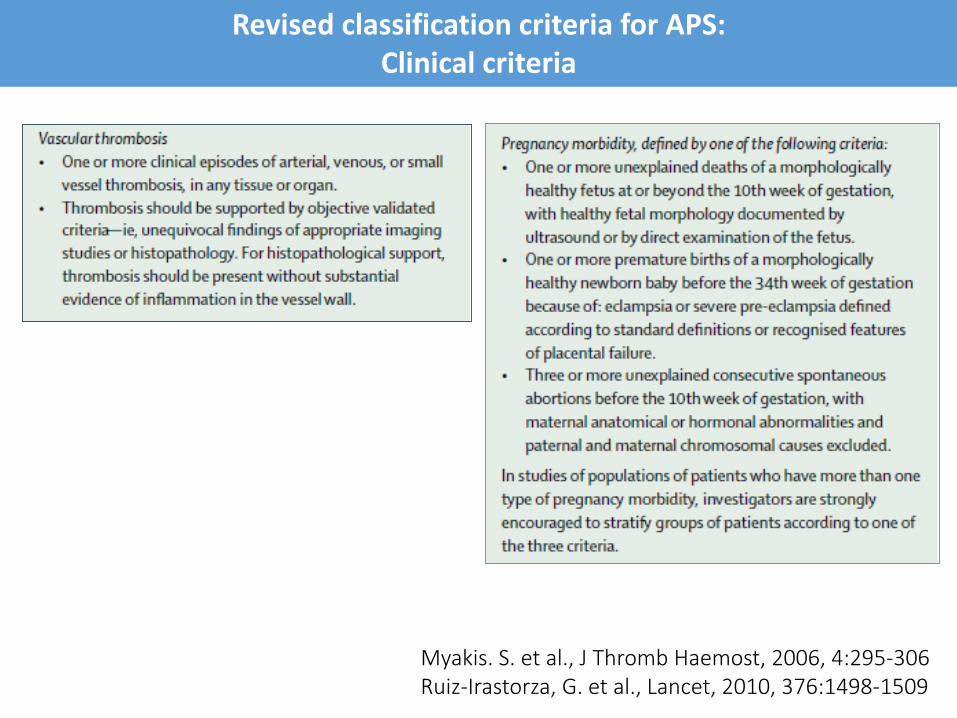
Myakis. S. et al., J Thromb Haemost, 2006, 4:295-306Ruiz-Irastorza, G. et al., Lancet, 2010, 376:1498-1509
Revised classification criteria for APS:Clinical criteria

Revised classification criteria for APS:Laboratory criteria
• I > 1 criteria
• IIa LA alone
• IIb ACL alone
• IIc anti-2GP1alone
Classification
Minimum 12 weeks betweenclinical symptoms and laboratory tests
Do not perform laboratory test >5 years after clinicalmanifestations
Myakis. S. et al., J Thromb Haemost, 2006, 4:295-306Ruiz-Irastorza, G. et al., Lancet, 2010, 376:1498-1509

Associated with APS but not diagnostic criteria
• Heart valves pathology:
11,6% of patients with APS, independently from SLE
• Livedo:
increased prevalence if SLE, sexe F
• Thrombocytopenia (platelets < 100 G/l, confirmed 12 weekslater):
− prevalence 20-40% in ref. 1 (in ref. 2, prevalence 6% in triple positive patients and 100% in CAPS patients)
− for diagnosis and treatment cf. ITP
− ITP + APL: more thrombotic events, 5 years follow-up
− exclusion of other causes of thrombocytopenia
• Nephropathy
1Myakis, S. et al., J. Thromb Haemost, 2006, 4:295-306
2Pontara E. et al., JTH 2018, 16:529-532
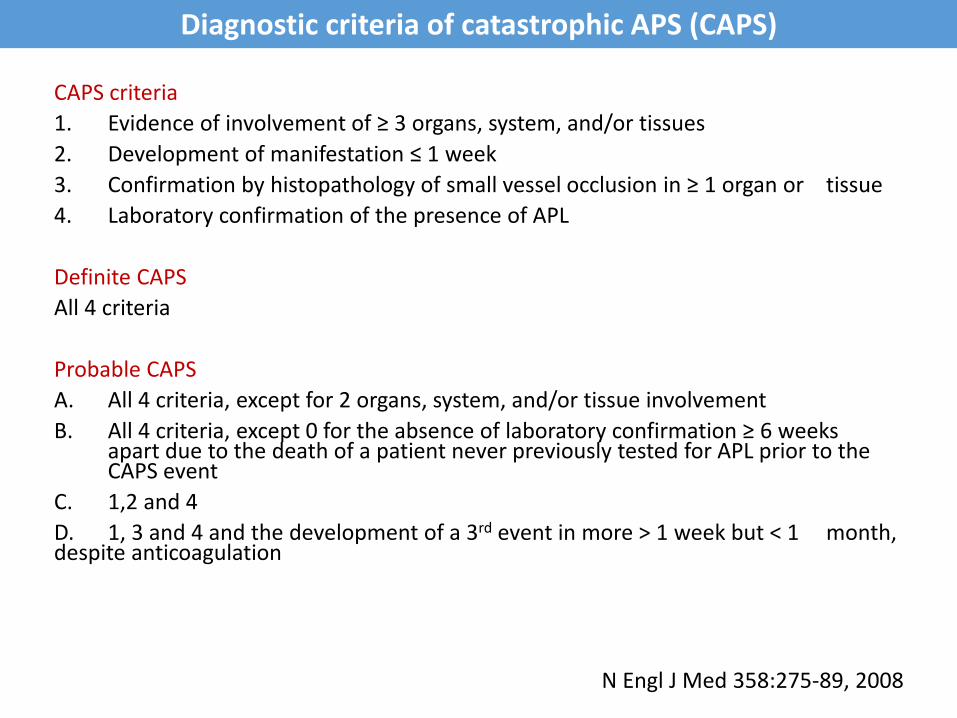
Diagnostic criteria of catastrophic APS (CAPS)
CAPS criteria
1. Evidence of involvement of ≥ 3 organs, system, and/or tissues
2. Development of manifestation ≤ 1 week
3. Confirmation by histopathology of small vessel occlusion in ≥ 1 organ or tissue
4. Laboratory confirmation of the presence of APL
Definite CAPS
All 4 criteria
Probable CAPS
A. All 4 criteria, except for 2 organs, system, and/or tissue involvement
B. All 4 criteria, except 0 for the absence of laboratory confirmation ≥ 6 weeksapart due to the death of a patient never previously tested for APL prior to the CAPS event
C. 1,2 and 4
D. 1, 3 and 4 and the development of a 3rd event in more > 1 week but < 1 month, despite anticoagulation
N Engl J Med 358:275-89, 2008


1. Lupus anticoagulant (LA) present in plasma detected according to the SSC on Lupus Anticoagulant/Phospholipid Antibodies recommendations2
2. β2GPI-dependent anticardiolipin antibodies (ACL) of IgG/IgM isotype in plasma or serum, present at higher levels (>99th percentile of normal controls), measured by solid phaseassays (ELISA or automated systems), according to the SSC on Lupus Anticoagulant/Phospholipid Antibodies recommendations3
3. β2GPI-antibodies (Aβ2GPI) of IgG/IgM isotype in plasma or serum, present at higherlevels (> 99th percentile), measured by solid phase assays (ELISA or automated systems), according to the SSC on Lupus Anticoagulant/Phospholipid Antibodies recommendations2
4. LA, ACL and Aβ2GPI should be positive on ≥ 2 occasions at least 12 weeks apart2-4
5. Laboratory results need to be reviewed and interpreted in a collaboration between a clinical pathologist and a clinician who is skilled at interpreting the data
6. Comprehensive APL antibody testing (LA, ACL and Aβ2GPI IgG and IgM) should be carriedout as triple APL-positive patients are at high risk of thrombosis or APL-related pregnancymorbidity
7. Other APL antibody tests are not recommended yet
Recommended laboratory testing for the APS1
1Devreese KMJ et al. JTH, 2018, 16:809-8132Pengo V et al. JTH, 2009, 7:1737-17403Devreese KMJ JTH, 2014, 12:792-7954Myakis S et al., JTH, 2006, 4:295-306
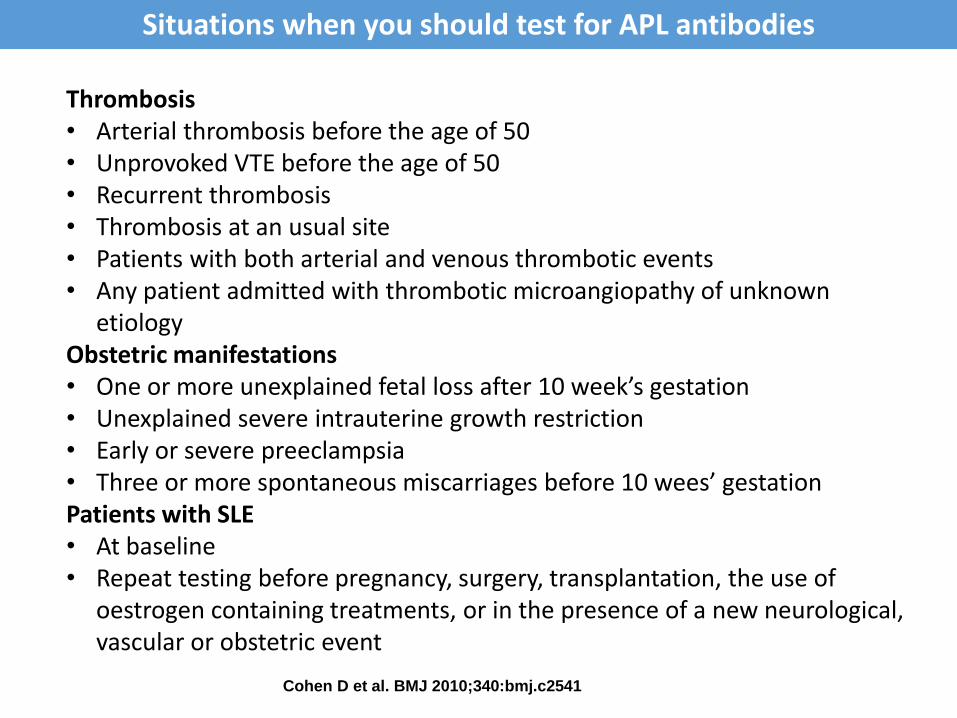
Cohen D et al. BMJ 2010;340:bmj.c2541
Situations when you should test for APL antibodies
Thrombosis• Arterial thrombosis before the age of 50• Unprovoked VTE before the age of 50• Recurrent thrombosis• Thrombosis at an usual site• Patients with both arterial and venous thrombotic events• Any patient admitted with thrombotic microangiopathy of unknown
etiologyObstetric manifestations• One or more unexplained fetal loss after 10 week’s gestation• Unexplained severe intrauterine growth restriction• Early or severe preeclampsia• Three or more spontaneous miscarriages before 10 wees’ gestationPatients with SLE• At baseline• Repeat testing before pregnancy, surgery, transplantation, the use of
oestrogen containing treatments, or in the presence of a new neurological, vascular or obstetric event
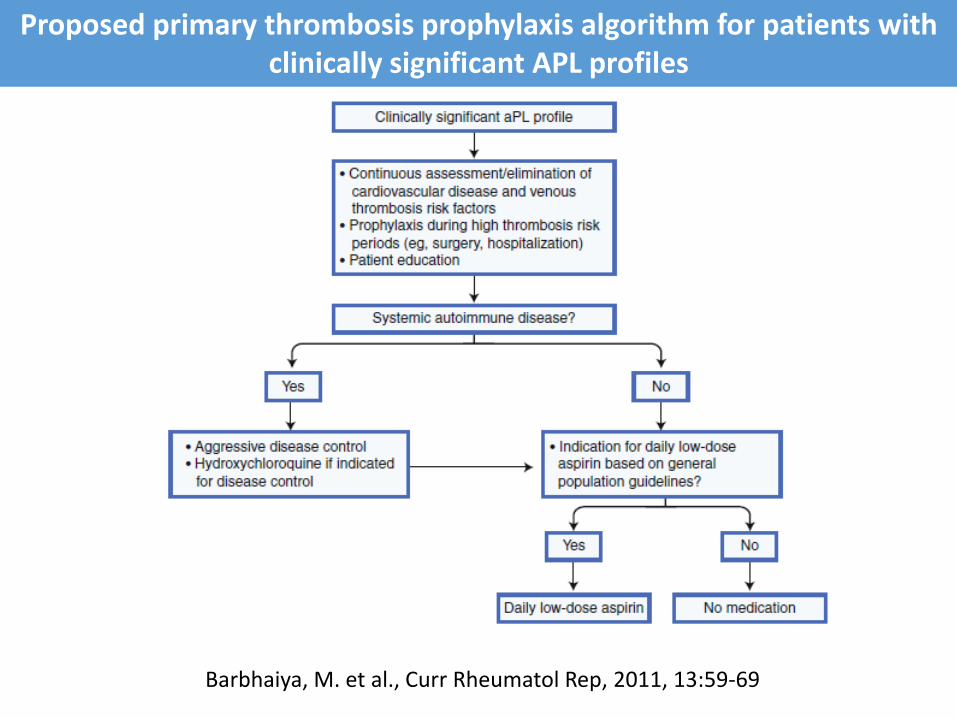
Proposed primary thrombosis prophylaxis algorithm for patients withclinically significant APL profiles
Barbhaiya, M. et al., Curr Rheumatol Rep, 2011, 13:59-69
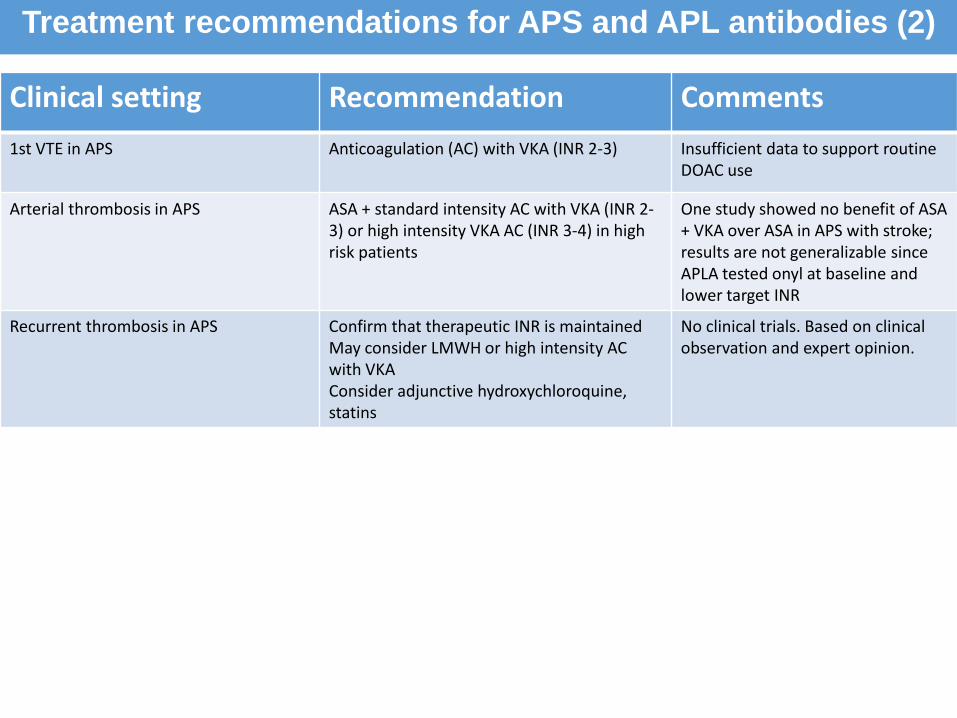
Clinical setting Recommendation Comments
1st VTE in APS Anticoagulation (AC) with VKA (INR 2-3) Insufficient data to support routineDOAC use
Arterial thrombosis in APS ASA + standard intensity AC with VKA (INR 2-3) or high intensity VKA AC (INR 3-4) in high risk patients
One study showed no benefit of ASA + VKA over ASA in APS with stroke;results are not generalizable sinceAPLA tested onyl at baseline and lower target INR
Recurrent thrombosis in APS Confirm that therapeutic INR is maintainedMay consider LMWH or high intensity AC with VKAConsider adjunctive hydroxychloroquine, statins
No clinical trials. Based on clinicalobservation and expert opinion.
Treatment recommendations for APS and APL antibodies (2)

Clinical setting Recommendation Comments
1st VTE in APS Anticoagulation (AC) with VKA (INR 2-3) Insufficient data to support routineDOAC use
Obstetric APS without prior thrombosis ASA + LMWHProphylactic dose LMWH continued until6 weeks post-partum
Obstetric APS with prior thrombosis ASA + therapeutic LMWH. After pregnancy may be transitioned back toVKA to continue AC indefinitively
Start LMWH (and stop VKA) at diagnosis of pregnancy
Catastrophic APS UFH + high dose steroids Observational data supports the use ofeculizumab, rituximab, plasmapheresisand defibrotide
Treatment recommendations for APS and APL antibodies (2)

• ITP diagnosed 3 years ago (platelet count 80 G/L)
• Spontaneous abortion 10th week of gestation 4 years ago
• Death in utero (16th week of pregnancy) 2 years ago
• Placenta: increase of fibrin (subchorial, peri-villeous)
• Currently: pregnancy 10th week of gestation
• Triple-positivity for APL antibodies, current platelet count 30 G/L
What is your diagnosis? What do you suggest?
Case 4: 31-year old woman
Take home message (1)
• Assess the VTE risk
• Importance of preconception management of women already usinganticoagulants when planning pregnancy
• Importance of providing in advance a detailed plan for the management of the anticoagulation around delivery
• Identify and manage carefully patients with antiphospholipid syndrome (importance of a multidisciplinary approach)
• Importance of well informating the patient and considering patient choices
Take home message (2)
• Thrombophilia testing does not predict anticoagulation failure and does not alter the initial treatment for VTE.
• No studies have shown that management strategies based on thrombophiliatesting affect patients risk of recurrence.
• The strongest predictor for recurrence is whether the initial VTE event was unprovoked.
Cohn et al., Cochrane Database of Systematic Reviews 2012; American College of Chest
Physicians Evidence-Based Clinical Practice Guidelines, Chest 2012; Baglin, T. et al., Br J
Haematol 2010
Take home message (3)
• Routine screening for inherited thrombophilia is not recommended in patients with unprovoked VTE
→ no major impact on the duration of anticoagulation.
• In selected patients, testing for thrombophilia may assist in their counseling about prognosis ; the implications of test results should be discussed withpatients before testing is done.
Cohn et al., Cochrane Database of Systematic Reviews 2012; American College of Chest
Physicians Evidence-Based Clinical Practice Guidelines, Chest 2012; Baglin, T. et al., Br J
Haematol 2010

Thank you for your attention



























