Embed Size (px)
Citation preview

Prevascularization of cardiac patch on the omentumimproves its therapeutic outcomeTal Dvira, Alon Kedemb, Emil Ruvinova, Oren Levyc, Inbar Freemana, Natalie Landad, Radka Holbovad,Micha S. Feinbergd, Shani Drore, Yoram Etzione, Jonathan Leord, and Smadar Cohena,1
aDepartment of Biotechnology Engineering and cDepartment of Life Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel 84105; bDepartment ofObstetrics and Gynecology and dNeufeld Cardiac Research Institute, Sheba Medical Center, Tel-Aviv University, Tel-Hashomer, Israel 52621; and eCardiacArrhythmia Research Laboratory, Soroka University Medical Center, Beer-Sheva, Israel 84105
Edited by Robert Langer, Massachusetts Institute of Technology, Cambridge, MA, and approved July 14, 2009 (received for review December 3, 2008)
The recent progress made in the bioengineering of cardiac patchesoffers a new therapeutic modality for regenerating the myocar-dium after myocardial infarction (MI). We present here a strategyfor the engineering of a cardiac patch with mature vasculature byheterotopic transplantation onto the omentum. The patch wasconstructed by seeding neonatal cardiac cells with a mixture ofprosurvival and angiogenic factors into an alginate scaffold capa-ble of factor binding and sustained release. After 48 h in culture,the patch was vascularized for 7 days on the omentum, thenexplanted and transplanted onto infarcted rat hearts, 7 days afterMI induction. When evaluated 28 days later, the vascularizedcardiac patch showed structural and electrical integration into hostmyocardium. Moreover, the vascularized patch induced thickerscars, prevented further dilatation of the chamber and ventriculardysfunction. Thus, our study provides evidence that grafting pre-vascularized cardiac patch into infarct can improve cardiac functionafter MI.
cardiac tissue engineering � myocardial infarction � SDF-1 �vascularization � affinity-binding alginate scaffolds
The adult heart has limited regeneration capacity, with con-sequent loss of myocardium and scar formation after exten-
sive myocardial infarction (MI) often leading to heart failure (1,2). Cell therapy approaches used in recent years, involving thetransplantation of suspensions of autologous stem cells or pro-genitors into the damaged myocardium that have been tested inpreclinical and early clinical studies, have only met with marginalsuccess (3, 4). In parallel, cardiac patches produced by tissueengineering methods are being developed for cardiac repair(5–7). Such patches can replace scar tissue or after grafting to thescar, improve cardiac function by supporting and thickening thedamaged zone. Another advantage of this approach is thatbioengineering of heart muscle can be achieved ex vivo, underprecise and controllable conditions.
To realize the therapeutical potential of the bioengineeredcardiac patch approach for cardiac repair, vascularization of thepatch is a prerequisite for maintaining its viability after trans-plantation onto the infarcted zone. Ex vivo methods for theprevascularization of skeletal or cardiac muscle patches thatinvolve the coculturing of capillary-forming cells with functionalcells have been developed (8, 9). Although the formation ofcapillaries in ex vivo engineered cardiac patch generated ac-cording to such protocols was recently documented (9), theefficacy of such approaches for cardiac repair has not yet beentested. Furthermore, previous work with other patches revealedthat in vitro engineered microvessels tended to leak aftertransplantation, when the comprising endothelial cells had mi-grated toward the center of the lumen (10).
In the present study, we sought to employ the body as abioreactor for the engineering of a cardiac patch containing astable and functional network of blood vessels, before trans-plantation onto infarcted hearts. Accordingly, we have devel-oped a technique wherein a cardiac patch was first engineered in
vitro and then matured and vascularized upon transplantationonto the omentum, a blood vessel-enriched membrane. Thepatch consisted of neonatal rat heart cells, seeded in macro-porous alginate scaffolds designed to allow cardiac cell organi-zation and blood vessel penetration after transplantation (11,12). To enhance vascularization and patch viability on theomentum, a mixture of prosurvival and angiogenic factors wasincorporated into the patch by exploiting their affinity binding tothe alginate matrix (13). Seven days after transplantation ontothe omentum, the cardiac patch was explanted and transplantedonto 7-day infarcted rat hearts. Cardiac patch engraftment,electrical coupling and cardiac function were evaluated 28 dayslater by histological, electrophysiological, and echocardiographicexamination. The in vivo experiments and analyses were per-formed by independent technicians and investigators blinded tothe experimental groups and the study protocol.
ResultsCardiac Patch Bioengineering. Neonatal rat cardiac cells (2.5 � 106
cells per scaffold) were seeded with factor-reduced Matrigel anda mixture of prosurvival and angiogenic factors into macro-porous alginate scaffolds (LVG, 5-mm diameter � 2-mm thick,100-�m average pore size) (Fig. 1 A–C). The mixture consistedof insulin-like growth factor-1 (IGF-1), stromal-cell derivedfactor 1 (SDF-1), and VEGF. To achieve controlled presentationand sustained release of the mixture factors, the alginate scaf-folds included alginate-sulfate (10% by dry weight), addition ofwhich enables high affinity binding of these factors to the matrix(13). We verified the activity of the mixture factors incorporatedinto the cardiac patch by demonstrating, via western blot anal-ysis, that the ERK1/2 and Akt signaling pathways, known topromote cardioprotection (14), are extensively activated in thesecultures (See Fig. S1 A). Using a chemotaxis chamber, we alsoverified that the release of SDF-1 from the cardiac patch was ableto attract human CD34-positive cells to a greater extent, ascompared with the attraction elicited by a cardiac patch lackingthe supplemented factors (See Fig. S1B).
The cardiac patch was cultured for 48 h to allow initial tissueorganization. Cell distribution throughout the alginate scaffoldwas confirmed by fluorescein diacetate (FDA)-staining of thepatch (See Fig. S1C) whereas the XTT viability assay revealedthat the patch retained 100% viable cells. The cardiac cells wereorganized in clusters within the pores, with some clusters
Author contributions: T.D., J.L., and S.C. designed research; T.D., A.K., E.R., O.L., N.L., R.H.,and S.D. performed research; I.F. and Y.E. contributed new reagents/analytic tools; T.D.,E.R., M.S.F., Y.E., J.L., and S.C. analyzed data; and T.D. and S.C. wrote the paper.
Conflict of interest statement: Y.E. and Mor Research Applications Ltd. have applied for apatent on the miniature bipolar hook electrode (International Patent Application No.PCT/IL2008/000161).
This article is a PNAS Direct Submission.
1To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/cgi/content/full/0812242106/DCSupplemental.
14990–14995 � PNAS � September 1, 2009 � vol. 106 � no. 35 www.pnas.org�cgi�doi�10.1073�pnas.0812242106
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021

presenting the highly differentiated sarcomeric organization ofcardiomyocytes (Fig. 1D). In cardiac patches raised without thesupplemented factor mixture, no cardiac muscle structures wereseen and cell viability was reduced to 70% of the initial seededcell number, as shown under static (i.e., with no mixing) culti-vation conditions (15).
Vascularization of the Cardiac Patch on the Omentum. To inducepatch vascularization before grafting onto infarcted heart tissue,we first implanted the mixture-supplemented cardiac patch ontorat omentum for 7 days (n � 8) as we envisioned that the bloodvessel-enriched omentum would provide a suitable site forinducing mature vasculature within the patch. To confirm thecontribution of factor supplementation to patch vascularizationand subsequent cardiac muscle regeneration, patches to whichno factors were supplemented were transplanted into controlanimals (n � 8).
Host blood vessels could be clearly seen entering the mixture-supplemented cardiac patch 7 days after transplantation onto theomentum (Fig. 2A). Hematoxylin and eosin (H&E)-stainedtissue cross-sections revealed extensive tissue ingrowth into themixture-supplemented cardiac patch (Fig. 2B and Fig. S2 A fora full cross section of the omental patch) whereas the patcheslacking the mixture supplement remained mostly acellular, withmost cells present at the patch edges (See Fig. S2B). The tissuewithin the mixture-supplemented patch was populated withblood vessels, could be immunostained with antibodies tosmooth muscle actin (SMA), indicating vessel coverage bypericytes and smooth muscle cells (SMC) (Fig. 2C). The bloodvessels were scattered throughout the patch and anastomized tothe host vasculature, as judged by their red blood cell content(Fig. 2D). Quantitatively, the vessel density and overall areaoccupied were 2.5–3 times greater in the mixture-supplemented
patches than in the control patches, that is, those patches with nomixture supplementation (Fig. 2 E and F).
We then assessed cardiac muscle formation in the omentum-generated patches by immunostaining with antibodies againstcardiac muscle markers, such as troponin T (Tn-T) and actinin.In the mixture-supplemented cardiac patches, bundles of cardiacmuscle structures could be identified throughout the entirepatch, as revealed by their distinctive Tn-T-staining (Fig. 2G).The cardiac muscle structures revealed typical cardiac cellstriation, indicating cardiac muscle formation with those patchesfused onto the omentum (Fig. 2H, green reflects anti-actinin
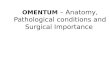
A B
C D
Fig. 1. Construction of a cardiac patch in an alginate-sulfate/alginate scaf-fold capable of binding and releasing mixture factors. (A and B) The scaffoldfeatures before cell seeding; macroscopic view (A) and internal porosity byscanning electron microscopy (B). (C and D) Cardiac patch, seeded with 2.5 �106 cardiac cells and supplemented with factor mixture, after 48 h of cultiva-tion. (C) Light microscope view of the cardiac patch, showing uniform distri-bution of cells in the matrix pores. (D) Cardiac cell organization within thescaffold, as judged by anti-actinin immunostaining (green) and nuclear stain-ing (red). Some of the cells reveal the typical striation of cardiac tissue. [Scalebar: 200 �m (C); 10 �m (D).]
A B
C D
E F
G H
Fig. 2. Vascularization of the 7 day omentum-transplanted, mixture-supplemented cardiac patch. (A) The cardiac patch (arrow) is stitched to theomentum. No contamination or inflammation were observed in any of thepatches (n � 16). (B) H&E-stained cross-section from the omentum-generatedcardiac patch supplemented with the prosurvival and angiogenic factorsshows extensive tissue in-growth into the scaffold. Lower right is the patchedge. (C) Mature blood vessels populate the cardiac patch supplemented withmixture, as judged by anti-SMA immunostaining (brown). (D) The vessels arefunctional and anastomized with host vessels, as reflected in their red bloodcell content. (E and F) Blood vessel density (E) and the area (F) (in %) occupiedby the vessels in the omentum-implanted patches. The results represent meanvalues � SEM. (n � 8 per group). Statistical evaluations were performed byunpaired Student’s t tests, P � 0.05. (G) Anti-Tn-T immunostaining of thinsection in the omentum-generated cardiac patch supplemented with mixturefactors (brown). (H) Typical cardiac cell striation is revealed in an omentum-generated, mixture-supplemented cardiac patch, as revealed by anti-actininimmunostaining (green) and confocal microscopy. [Scale bar: 200 �m (B); 100�m (C); 20 �m (D and G); 10 �m (H).]
Dvir et al. PNAS � September 1, 2009 � vol. 106 � no. 35 � 14991
MED
ICA
LSC
IEN
CES
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021

antibody immunostaining). By contrast, in those cardiac patcheswhere no mixture supplementation had been made, no distinc-tive cardiac muscle structures were observed 7 days after at-tachment to the omentum (See Fig. S2 C and D).
Effect of Prevascularization on Patches Grafting onto Infarcted Heart.The prevascularized cardiac patches were implanted onto theinfarcted heart of male SD rats (n � 11) 7 days after MI, inducedby ligation of the left descending coronary artery (See Fig. S3).Stitched rat hearts after MI induction served as negative controls(n � 7) whereas the implantation of in vitro-grown mixture-supplemented cardiac patches (n � 6) served to test for theeffects of prevascularization on patch grafting onto infarctedmyocardium and subsequent cardiac repair. Only rats displayingfractional shortening (FS) � 40% as assessed by echocardiog-raphy were included in study.
Four weeks after implantation, the omentum-generatedpatches were fully integrated into the host myocardium andshowed thicker scars than those observed on the myocardium ofcontrol rats (Fig. 3 A–C). The prevascularized patch was popu-lated with striated and elongated cardiac cells, some of whichwere oriented perpendicular to the direction of the host myo-cardium (Fig. 3 C and D). The cardiac muscle structures couldbe positively stained with antibodies to Tn-T (Fig. 3E) andconnexin 43 (Cx-43) (Fig. 3F), indicating the formation ofmechanical contacts between the transplanted cells. By contrast,in most of the animals into which the in vitro grown cardiacpatches were transplanted, processing for histological examina-tion led to the patches being detached from the host myocar-
dium, indicative of these patches not integrating with the myo-cardial scar (Fig. 3B).
Morphometric analysis showed that the relative scar thickness(average scar thickness/average wall thickness) was significantlygreater in the omentum-generated patch-treated hearts, with avalue close to 1, reflecting normal wall thickness (Fig. 3G).Moreover, the infarct expansion index [(LV cavity area/wholeLV area)/relative scar thickness] was much smaller in theomentum-generated patch-treated hearts than in hearts of thecontrol groups (Fig. 3H). Together, these data indicate thattransplantation of the omentum-generated cardiac patch isattenuating LV dilatation after MI.
When evaluating blood vessel density in scars treated withomentum-generated patches (Fig. 3I), the density measured(65�9/mm2) is close to that found in the patches before theirimplantation onto the infarct (48�4/mm2, Fig. 2E), possiblyindicating that the scar neovessels mainly originated from theintegrated patch. In infarcts treated with the in vitro-growncardiac patch, vessel density was similar to that observed in thestitched scars, consistent with the lack of patch integration intothe scar in these cases.
Omentum-Generated Patches Are Electrically Coupled with the HostMyocardium. Electrical coupling of the omentum-generated car-diac patch to the host myocardium was assessed 4 weeks afterengraftment using Langendorff-perfused isolated heart prepa-rations (n � 3). Similar preparations from empty scaffold-treated (n � 2, to rule out biomaterial effect) and stitched (n �2) infarcted hearts served as controls. To assess the level ofelectrical connectivity between the engrafted patch and the
A B C
D E F
G H I
Fig. 3. Assessment of the scar zone, 28 days after patch grafting onto an infarcted heart. (A–C) Representative figures of Masson’s trichrome-stainedcross-sections in a stitched only scar (A), a scar implanted with an in vitro-grown patch (B), or a scar grafted with an omentum-generated cardiac patch (C).Collagen in the scar is stained blue and viable cardiac tissue is shown in red. (D) H&E staining of cross-sections in the interface (dashed black line) of the hostmyocardium (M) and grafted omentum-generated patch (P). (E) Typical cardiac cell striation could be observed by anti-Tn-T immunostaining (brown). (F) Cx-43expression (brown) between adjacent cardiomyocytes in omentum-generated cardiac patch suggests mechanical coupling. (G and H) Morphometric analysis ofscar area and calculation of relative scar thickness (G) and expansion index (H), [(LV cavity area/whole LV area)/relative scar thickness]. (I) Blood vessel densityin the scar area was determined by counting anti-SMA-immunostained vessels. Results represent mean values � SEM. (n � 4–6). Statistical evaluations wereperformed by unpaired Student’s t tests, P � 0.05. [Scale bar: 500 �m (A–C); 200 �m (D); 20 �m (E and F).]
14992 � www.pnas.org�cgi�doi�10.1073�pnas.0812242106 Dvir et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021

myocardial tissue, two miniature bipolar hook electrodes wereblindly inserted on the epicardium at the base of the rightventricle (RV, healthy myocardium electrode) and on the scarzone, as close as possible to the stitch (scar electrode). Asexpected, spontaneous electrical activity was greater in healthymyocardium, as compared with scar tissue, in all seven prepa-rations. Recordings from scars treated with omentum-generatedcardiac patches showed greater amplitude signals than didrecordings made from the scars of control subjects (3.32 � 0.32mV vs. 1.55 � 0.34 mV, respectively) (Fig. 4 A, B, and E).Consistent with this observation, pacing through the scar elec-trode (2 ms square pulses, 400 beats per minute) resulted in amuch lower scar capture threshold (defined as the minimalstimulus intensity needed to reach synchronous activation of thehealthy tissue by pacing through the scar electrode) in heartstreated with the omentum-generated patches than was the casewith stitched scars (1.16 � 0.16 mA vs. 5.5 � 0.5 mA, respec-tively), indicating improved electrical connectivity between thescar zone and the healthy myocardium in those preparationstreated with omentum-generated patches (Fig. 4 C, D, and F).
Grafting of Omentum-Generated Cardiac Patches Improves CardiacFunction. Two-dimensional (2D) echocardiographic examina-tions were performed 6 days after MI induction, to obtainbaseline readings. Thirty of the 37 studied rats showed fractionalshortening (FS) �40%; these were subsequently subjected toechocardiography study, 28 days after patch grafting or scar
stitching. Herein, an additional group of implanted a-cellularconstructs supplemented with the factor mixture and grown onthe omentum for 7 days (n � 6) was transplanted on the infarctedhearts, to assess the omentum contribution to cardiac function.
Evaluation of the baseline showed the formation of scar tissue6 days after MI induction. Twenty-eight days after intervention,the fractional area change (FAC) and fractional shortening (FS)echocardiography data indicated further deterioration in thestitched infarcts and in hearts implanted with in grown patches(Fig. 5 A and B, Fig. S4 A and B, and Table S1). By contrast, FACand FS values did not differ from baseline values in animalstreated with the omentum-generated patches with the cellularpatches being more invariant (cardiac patches: P � 0.22 and 0.6;a-cellular patches: P � 0.09 and 0.17, in terms of percent changein FAC and FS, respectively) (Fig. 5 C and D and Fig. S4 C andD). Additionally, the percent changes in FAC, LV end diastolicdimension (LVEDD) and LV end systolic dimension (LVESD)were all significantly smaller in animals treated with the omen-tum-generated cardiac patches compared with the animals withthe stitched hearts (Fig. 5 E–G and Table S2).
DiscussionThis study demonstrates that the omentum can serve as anefficient bioreactor for producing cardiac patches with func-tional blood vessel network, which, after successful grafting toinfarcts, attenuate LV remodeling and dysfunction in rats that
Fig. 4. Electrical coupling of omentum-generated cardiac patch to hostmyocardium. Langendorff-perfused isolated hearts were blindly implantedwith two bipolar epicardial electrodes located at the base of the healthy rightventricle myocardium (RV) and the scar zone as close as possible to the stitch(scar). (A and B) Nonpaced (spontaneous) electrical signals recorded from thehealthy myocardium (RV) and scar zone (Scar) of hearts with an omentum-generated patch (A) or hearts with stitch only (B). (C and D) Pacing through thescar electrode using 2 ms square pulses (400 beats per min) in hearts treatedwith an omentum-generated patch (C) or stitched scar (D), at a stimulusintensity of 1.5 mA. This stimulus intensity could capture all hearts treatedwith omentum-generated patch, but none of the control hearts. (E) Compar-ison of signal amplitude in the scar zone after grafting an omentum-generated patch (black) or in stitched hearts (white). (F) Comparison ofcapture threshold intensity in hearts grafted with an omentum-generatedpatch (black) or only stitched (white).
Fig. 5. Changes in left ventricle function after patch grafting. The FAC {[(LVend-diastolic area � LV end-systolic area)/LV end-diastolic area] �100} ofinfarcted hearts treated with stitches only (A) (n � 7), hearts treated with invitro-grown patches (B) (n � 6), treated with a-cellular omentum-grownscaffolds (C) (Om., n � 6), or treated with omentum-generated cardiac patches(D) (Om.�, n � 11), was determined by echocardiography. ‘‘Pre’’ indicatesreadings 6 days after MI induction by LAD ligation and 1 day before interven-tion. ‘‘Post’’ indicates readings taken 28 days after intervention. Comparisonof FAC (E) change, LVEDD (F), and LVESD (G). Changes were calculated asfollows: [(values obtained after 4 weeks – baseline values)/baseline values] �100%. Statistical evaluations were performed by paired Student’s t tests, P �0.05 (A–D) or un-paired t test and one-way ANOVA, P � 0.05 (E–G).
Dvir et al. PNAS � September 1, 2009 � vol. 106 � no. 35 � 14993
MED
ICA
LSC
IEN
CES
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021

experienced MI. The functional vascular network that developedin omentum-generated cardiac patches enabled the maintenanceof transplanted and resident viable cardiac muscle structures.After grafting onto scar tissue, the cardiac patches were struc-turally and electrically coupled with the host myocardium,leading to beneficial effects on systolic and diastolic left ven-tricular function.
A prerequisite for successful myocardial regeneration is thatthe implanted cardiac patch retains viability and integrates intothe infarct. Prevascularization of the patch and rapid anastemo-sis of the patch vasculature with host myocardial vessels wouldensure the rapid engraftment and integration of the patch intothe infarcted myocardium. Implantation on omentum for induc-ing vasculogenesis in tissue explants was previously explored(16–18). Here, we have used the omentum for prevascularizationand cardiac tissue engineering given that this tissue is enrichedwith blood vessels.
The incorporation of prosurvival and angiogenic factors intothe cardiac patch protected the scaffold-seeded cells and inducedcardiac muscle formation during in vitro cultivation and afterpatch implantation, increased survival of the nascent cardiactissue and induced cardiac tissue maturation on the omentum.Furthermore, the mixture factors enhanced patch vasculariza-tion on the omentum, inducing the formation of a stable networkof functional blood vessels to nourish the transplanted cardiactissue within the patch. The mixture consisted of Matrigel, shownto prevent anoikis (19) and enhance capillary formation (20),SDF-1, a chemoattractant for bone marrow-derived stem cells(BMSC) and endothelial progenitor cells (EPC) (21, 22), andshown to act as a cardioprotective agent (23), IGF-1, a cardio-protective and angiogenic agent (24), and VEGF, an angiogenicfactor (12, 25, 26). The maintenance of mixture factor activity inthe patch during in vitro cultivation and later, in vivo, isattributed to their affinity binding to alginate-sulfate within thematrix and via their sustained release (13, 27).
An important observation of this study is that the omentum-generated prevascularized patch was structurally and electricallyintegrated into the host myocardium, 28 days after transplanta-tion onto the infarct. By this point, the scaffold disappeared fromthe infarct, thereby allowing the bioengineered cardiac tissue toform mechanical and electrical contacts with the host myocar-dium. The successful grafting of the omentum-generated patchresulted in the formation of thicker scars with an average relativescar thickness close to 1, the same value as measured for thenormal LV wall and 2-fold higher than in the control groups.Importantly, the electrical recordings provided compelling evi-dence for the improved electrical coupling between the omentum-generated patch and healthy myocardium, as evidenced by thehigher amplitude of electrical signals in the scar zone and by themarkedly lower capture threshold for pacing, indicating betterexcitability and/or electrical connectivity between the scar andhealthy myocardium.
The integration of the omentum-generated cardiac patch tothe host myocardium is attributed to the fact that bioengineeringon the omentum resulted in a consistent tissue with a stablenetwork of blood vessels able to anastomize with the hostmyocardium. Consistent with this claim is the finding that bloodvessel density in the transplanted omentum-generated patchresembled that of the scar zone after grafting. Further, infiltra-tion of host cells like fibroblasts possibly contributed to integra-tion by enhancing patch adhesion to the scar. By contrast, the invitro grown patch, although initially supplemented with the samemixture factors, could not integrate into the infarct because ofthe acellular nature of patches so raised.
The most important outcome of the successful grafting of theomentum-generated cardiac patch to scar tissue was its ability toimprove after MI cardiac function (% change in FS) and toinhibit ventricular dilatation (% change in FAC) after MI. The
effect of treatment on these parameters was more pronouncedin animals implanted with omentum-generated cardiac cellularpatches than in those transplanted with omentum-generateda-cellular patches (although the difference between these groupsdid not reach significance). We attribute this to the addition viapatch grafting of contractile structures to the infarct site as seenin Fig. 3 C–F. Additionally, the cellular and acellular omentum-generated patches could contribute to enhanced angiogenesisand to preservation of remaining resident cardiac tissue at theinfarct zone after MI; the two patches affinity-bound and deliverangiogenic and cardioprotective factors as well as their gener-ation on the omentum most likely supplement them with addi-tional cells and factors from the omentum which add to theirbeneficial effects.
The successful cardiac patch grafting onto the scar increasedscar thickness and stabilized the chamber size. By thickening thescar, wall stress is reduced (according to Laplace’s law) and thedegree of outward motion of the infarct that occurs duringsystole (dyskinesis) is reduced. This effect is significant becauseone of the most important predictors of mortality in patientsafter MI is the degree of LV systolic dilatation (28). During theechocardiography studies, we observed variability in infarct sizesand functional consequences, in those rats with initially largeinfarcts (FS, 10–30%) showing substantial improvement aftertreatment with engineered cardiac tissues. Our results are inagreement with those of Zimmermann et al. (29), indicating thatthe cardiac patch approach is able to treat large infarcts andimprove cardiac function after MI.
Using the body as a bioreactor to engineer cardiac tissue withstable and functional blood vessel networks represents a signif-icant improvement in cardiac patch performance over ex vivomethods currently used for patch production. Others havesuccessfully exploited the omentum for the vascularization ofhepatic tissues and for bladder construction (30, 31). Recently,our group transplanted cardiac cell-seeded scaffolds into theperitoneal cavity in an attempt to induce tissue engineering ofthe patch (32). In those studies, however, no cardiac musclestructures were detected in the peritoneal-generated patch, withtissue in-growth consisting of myofibroblasts being embeddedinto collagen bundles and infiltrated with blood vessels. Theresults of the present study reveal that cardiac muscle structuresare regenerated on the omentum and can survive transplantationonto infarcted heart in the presence of an appropriate maturevasculature. Furthermore, our study reports structural and elec-trical integration of a cardiac patch resulting in improved afterMI heart function. This can be attributed to the improvedprevascularization of the cardiac patch by supplementation ofmixture factors.
We realize that explanting the cardiac patch from the omen-tum is associated with transient discontinuation of blood flow toengineered tissue. Yet, the time interval from explantation toimplantation on the infarct is short (�5 min) and the vesselinfrastructure is probably preserved during this time interval. Itis also likely that blood fluid remaining in the graft vesselsthroughout this procedure, nourishes the cells until anastomosiswith the host is achieved. The survival of the engineered cardiactissue after explantation and implantation on the infarct and thetherapeutic outcome of the patch support the continuous supplyof oxygen and nutrients to the cells.
Surgically, the procedure described herein can be applied inhuman because of its simplicity, safety and efficacy for cardiacrepair. However, because most MI patients are old and multiplesurgeries can pose a large risk on them, the clinical applicationof our strategy is currently not an option for these patients.Regenerative strategies by employing instructive biomaterials orcombination of biomaterials and growth factors should befurther explored as more simple approaches for cardiac regen-eration after MI (5).
14994 � www.pnas.org�cgi�doi�10.1073�pnas.0812242106 Dvir et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021

Materials and MethodsThe study, performed in accordance with the guidelines of the Animal Careand Use Committee of Sheba Medical Center, Tel Aviv University, was ap-proved by the institutional review board and was supervised by institutionalanimal protection officials.
Patch Construction and Analysis. The cardiac patch was prepared as described(15, 33). Briefly, cardiac cells were isolated from the LV of SD neonatal (1–2days old) rat hearts and seeded onto alginate-sulfate/alginate scaffolds (5 �2-mm, d � h, 0.7 � 108 cells per cm3). In cardiac patches supplemented withmixture, the cells were seeded with Matrigel (30% vol/vol) and SDF-1, IGF-1,and VEGF (100 ng each) in M199 medium. After cultivation under staticconditions in a humidified incubator for 48 h, the patches were analyzed forviability or implanted. All factors, excluding the cells were added to thea-cellular patches.
Transplantation of Patches onto Rat Omentum. Recipient SD male rats (150–200g) were anesthetized with a combination of ketamine (40 mg/kg) and xylazine(10 mg/kg). After a midline abdominal incision was made, the patches (after48 h cultivation) were placed on the omentum and were secured in place witha 6–0 prolene suture. Seven days after transplantation, the animals werekilled and the patches were gently cut and cleaned with scalpel. The patcheswere then either taken for evaluation or transplanted onto the infarctedheart of a rat MI model.
Rat Model of Myocardial Infarction and Patch Grafting. MI was induced asdescribed in ref. 6. SD male rats (�250 g) were anesthetized with a combina-tion of ketamine (40 mg/kg) and xylazine (10 mg/kg), intubated, and mechan-ically ventilated. The chest was open by left thoracotomy, the pericardium wasremoved, and the proximal left coronary artery was permanently occulatedwith an intramural stitch. Seven days after MI, omentum-generated patches(acellular or containing cardiac cells) or in vitro-grown (7 days under staticconditions) patches were implanted onto the scar tissue by a single stitch.Twenty-eight days after implantation, the rats were either killed or taken forfurther evaluation.
Morphometric Analyses. For morphometric analyses, the slides were stainedwith Masson’s trichrome, microscopically examined and analyzed with Cell-Psoftware (Olympus). The average LV wall thickness was calculated from threemeasurements of septum thickness whereas average scar thickness was de-
termined from three measurements of scar thickness in each animal. Relativescar thickness was calculated as average scar thickness divided by average wallthickness. The expansion index was calculated as follows: expansion index �
[(LV cavity area/whole LV area)/relative scar thickness].
Electrophysiology. Hearts were excised as described in ref. 34. Briefly, rats wereheparinized (500 U/kg, IP) and hearts were rapidly excised with constantperfusion with Hepes Tyrode’s solution preheated to 37 °C (100-mm perfusionpressure). Miniature bipolar hook electrodes were attached to the epicardialsurface at the patch/scar and to the base portion of the right ventricle (34).Electrophysiological signals were recorded, filtered and interfaced with a PCusing an A/D converter (PCI-6024E, National Instruments) and a programdeveloped by YE, as described in ref. 34. Electrical stimulation (2 ms squarepulses) was applied through an optically isolated pacer (Pulsar 6bp-as, FHC).The operator of these experiments was blinded as to whether the examinedanimal was treated with the omentum-generated patch (n � 3), by stitch only(n � 2) or with an empty scaffold (n � 2).
Echocardiography. Transthoracic echocardiography was performed on all an-imals, 6 days after MI (baseline echocardiogram) and 28 days after interven-tion. Echocardiograms were performed with commercially available echocar-diography system (Vivid i, GE Healthcare) equipped with a 12-MHz phased-array transducer (Hewlett Packard). All measurements were averaged overthree consecutive cardiac cycles and were performed by an experiencedtechnician blinded to the treatment group.
Statistical Analysis. Statistical analysis data are presented as means � SEM.Univariate differences between the control and treated groups were assessedwith Student’s t test. Changes in echocardiographic data between baselinereadings and 28 days after treatment, as well as LV function, were assessed bypaired and unpaired t tests and by one-way ANOVA. All analyses wereperformed using GraphPad Prism version 5.00 for Windows (GraphPad Soft-ware). P � 0.05 was considered significant.
For additional information see SI Text.
ACKNOWLEDGMENTS. We thank Ms. Lena Shoval for technical assistance.This work was supported by Israel Science Foundation Grant 793/04. S.C. holdsthe Claire and Harold Oshry Professor Chair in Biotechnology.The work is partof the doctoral thesis of T.D. at Ben-Gurion University of the Negev.
1. Pasumarthi KB, Field LJ (2002) Cardiomyocyte cell cycle regulation. Circ Res 90:1044–1054.2. Rubart M, Field LJ (2006) Cardiac regeneration: Repopulating the heart. Ann Rev Physiol
68:29–49.3. Assmus B, et al. (2002) Transplantation of progenitor cells and regeneration enhancement
in acute myocardial infarction (TOPCARE-AMI). Circulation 106:3009–3017.4. SchachingerV,etal. (2004)Transplantationofprogenitor cellsandregenerationenhance-
ment inacutemyocardial infarction:Finalone-year resultsof theTOPCARE-AMITrial. JAmColl Cardiol 44:1690–1699.
5. Landa N, et al. (2008) Effect of injectable alginate implant on cardiac remodeling andfunction after recent and old infarcts in rat. Circulation 117(11):1388–1396.
6. Leor J, et al. (2000) Bioengineered cardiac grafts: A new approach to repair the infarctedmyocardium? Circulation 102:III56–61.
7. Kofidis T, et al. (2005) Novel injectable bioartificial tissue facilitates targeted, less invasive,large-scale tissue restoration on the beating heart after myocardial injury. Circulation112:I173–177.
8. Levenberg S, et al. (2005) Engineering vascularized skeletal muscle tissue. Nat biotechnol23:879–884.
9. Caspi O, et al. (2007) Tissue engineering of vascularized cardiac muscle from humanembryonic stem cells. Circ Res 100:263–272.
10. Nor J, et al. (2001) Engineering and characterization of functional human microvessels inimmunodeficient mice. Lab Invest 81:453–463.
11. Dar A, Shachar M, Leor J, Cohen S (2002) Optimization of cardiac cell seeding anddistribution in 3D porous alginate scaffolds. Biotechnol Bioeng 80:305–312.
12. Kedem A, et al. (2005) Vascular endothelial growth factor-releasing scaffolds enhancevascularization and engraftment of hepatocytes transplanted on liver lobes. Tissue Eng11:715–722.
13. Freeman I, Kedem A, Cohen S (2008) The effect of sulfation of alginate hydrogels on thespecificbindingandcontrolledreleaseofheparin-bindingproteins.Biomaterials29:3260–3268.
14. Wakatsuki T, Schlessinger J, Elson EL (2004) The biochemical response of the heart tohypertension and exercise. Trends Biochem Sci 29:609–617.
15. Dvir T, Benishti N, Shachar M, Cohen S (2006) A novel perfusion bioreactor providing ahomogenous milieu for tissue regeneration. Tissue Eng 12:2843–2852.
16. UeyamaK,etal. (2004)Developmentofbiologiccoronaryarterybypassgrafting inarabbitmodel: Revival of a classic concept with modern biotechnology. J Thorac Cardiovasc Surg127:1608–1615.
17. Goldsmith H, Griffith A, Kupferman A, Catsimpoolas N (1984) Lipid angiogenic factor fromomentum. J Am Med Assoc 252:2034–2036.
18. Levy Y, et al. (1998) Effect of omental angiogenic lipid factor on revascularization ofautotransplanted spleen in dogs. Eur Surg Res 30:138–143.
19. Laflamme MA, et al. (2007) Cardiomyocytes derived from human embryonic stem cells inpro-survival factors enhance function of infarcted rat hearts. Nat Biotechnol 25:1015–1024.
20. Asahara T, et al. (1997) Isolation of putative progenitor endothelial cells for angiogenesis.Science 275:964–967.
21. Shao H, et al. (2008) Statin and stromal cell derived factor-1 additively promote angio-genesis by enhancement of progenitor cells incorporation into new vessels. Stem cells26:1376–1384.
22. Tan Y, et al. (2007) Stromal cell-derived factor-1 enhances pro-angiogenic effect ofgranulocyte-colony stimulating factor. Cardiovasc Res 73:823–832.
23. Zhang M, et al. (2007) SDF-1 expression by mesenchymal stem cells results in trophicsupport of cardiac myocytes after myocardial infarction. Faseb J 21:3197–3207.
24. Tokunou T, et al. (2008) Engineering insulin-like growth factor-1 for local delivery. FasebJ 22:1886–1893.
25. Leach JK, Kaigler D, Wang Z, Krebsbach PH, Mooney DJ (2006) Coating of VEGF-releasingscaffolds with bioactive glass for angiogenesis and bone regeneration. Biomaterials27:3249–3255.
26. Peters MC, Polverini PJ, Mooney DJ (2002) Engineering vascular networks in porouspolymer matrices. J Biomed Mater Res 60:668–678.
27. Freeman I, Cohen S (2009) The influence of the sequential delivery of angiogenic factorsfrom affinity-binding alginate scaffolds on vascularization Biomaterials 30:2122–2131.
28. Migrino R, et al. (1997) End-systolic volume index at 90 to 180 minutes into reperfusiontherapyforacutemyocardial infarctionisastrongpredictorofearlyandlatemortality.Theglobal utilization of streptokinase and t-PA for occluded coronary arteries (GUSTO)-Iangiographic investigators. Circulation 96:116–121.
29. ZimmermannWH,etal. (2006)Engineeredhearttissuegrafts improvesystolicanddiastolicfunction in infarcted rat hearts. Nat Med 12:452–458.
30. Lee H, et al. (2003) Effect of implantation site on hepatocytes heterotopically transplantedon biodegradable polymer scaffolds. Tissue Eng 9:1227–1232.
31. Hattori K, et al. (2006) Bladder reconstruction using a collagen patch prefabricated withinthe omentum. Int J Urol 13:529–537.
32. Amir G, et al. (2009) Evaluation of a peritoneal-generated cardiac patch in a rat model ofheterotopic heart transplantation. Cell Transplant 18:275–282.
33. Dvir T, Levy O, Shachar M, Granot Y, Cohen S (2007) Activation of the ERK1/2 cascade viapulsatile interstitial fluid flow promotes cardiac tissue assembly. Tissue Eng 13:2185–2193.
34. Etzion Y, et al. (2008) New insights into the atrial electrophysiology of rodents using anovel modality: The miniature-bipolar hook electrode. Am J Physiol Heart Circ Physiol.295:H1460–469.
Dvir et al. PNAS � September 1, 2009 � vol. 106 � no. 35 � 14995
MED
ICA
LSC
IEN
CES
Dow
nloa
ded
by g
uest
on
Mar
ch 1
7, 2
021