Embed Size (px)
Citation preview

Prethrombolytic Versus Thrombolytic Era Risk Stratification of Patients With
Acute Myocardial InfarCtion John F. Murphy, MD, Michael G. Kahn, MD, PhD, and Ronald J. Krone, MD
T hrombolytic therapy significantly decreases the mor- tality of patients with acute myocardial infarction.’
However, high-risk patients still have a high mortality even though their predicted mortality is substantially decreased by thrombolytic therapy.* The early identifi- cation of high-risk patients would be important to indi- vidualize therapy through either alternate or additional therapy.3,4 To use established predictors of mortality in the prethrombolytic era, we sought to validate them in patients with acute myocardial infarction who received thrombolytic therapy. We then stratified patients based on clinical predictors that could be assessed on first pre- sentation to identify patients at high risk of short-term mortality.
. . . This study is a secondary analysis of the Thrombol-
ysis in Myocardial Infarction Phase II (TIM1 II) clinical trial data, performed independently from the TIM1 Re- search Group.5 Briefly, the purpose of the trial was to evaluate early arteriography and early cardioselective p blockade in patients with acute myocardial infarction who had received recombinant tissue-type plasminogen acti- vator (t-PA). Inclusion criteria included age ~76 years, chest discomfort suggestive of myocardial ischemia last- ing 230 minutes, ST-segment elevation 20.1 mV in 2 leads, and initiation of t-PA within 4 hours of the onset of chest pain. Exclusion criteria included a history of cerebrovascular disease, blood pressure >180/110 mm Hg, a bleeding disorder, recent surgery, prolonged car- diopulmonary resuscitation, trauma, previous coronary angioplasty, coronary artery bypass surgery, prosthetic valve surgery, left bundle branch block, and dilated car- diomyopathy. The 195 patients who underwent immedi- ate catheterization were not included in the analysis. Of the remaining 3,339 patients, we excluded patients who received 150 mg of t-PA, a dose no longer used, leaving 2,819 patients who received 100 mg of t-PA.
We selected 23 clinical variables that have been shown to be related to short-term mortality in the prethrombolytic era. 6-I’ Variables within these references were selected by their presence in the TIMI II data. Most of the mortality occurs early, the optimal time to inter- vene, but we also included variables associated with late
From the Cardiovascular Division and the Division of General Med ical Sciences, Department of Medicine, Washin ton School of Medicine, St. Louis, Missouri, and the Car c?
University lovascular Divi-
sion, Department of Medicine, Jewish Hospital, St Louls, Missouri. Dr. Murphy IS a training fellow of the National Heart, Lung, and Blood Institute, and IS supported by Grant 5-T32-Hl0708 l-l 9, Bethesda, Ma
a land. Dr. Kahn is supported in part by Grants UOl-
lMO5845 an R29-LM05387 from the National tlbrary of Medi- tine. Dr. Murphy’s address is: Cardiovascular Divlslon, Washington University School of Medicine, Box 8086, 660 South Euclid Avenue, St. Louis, Missouri 63 1 10. Manuscript received May 10, 1995; revised manuscript received and accepted July 1 8, 1995.
mortality in our assessment of short-term mortality.12-I4 In clinical practice, the values of all of these variables could be obtained in the emergency room. The primary outcome was overall mortality at 6 weeks. Univariate analysis was done with logistic regression using the SAS system (SAS Institute, Cary, North Carolina). Statistical significance was determined by p ~0.05.
All statistically significant univariate independent predictors of 6-week mortality were entered into a mul- tiple logistic regression analysis, with the dependent variable overall mortality at 6 weeks. Independent pre- dictors were identified using stepwise selection with p ~0.05. A clinical classification algorithm was devised using these independent predictors. Patients with car- diogenic shock were excluded from the classification algorithm because immediate catheterization with coro-
TABLE I Univoriate and Multivariate Predictors of Six-Week Mortality
Variable Odds Missing
p Value Ratio Observations
Univariate Predictors
Shock 0.0001 13.514 0 Hypotension 0.0001 3.774 0 Diabetes mellitus 0.0001 2.451 9 Prior myocardial infarction 0.0001 2.331 0 Number of leads with ST 0.0001 1.235 1
elevation Age 0.0001 1.080 0 Diastolic blood pressure 0.0001 0.978 46 Sex 0.0002 2.084 0 Pulmonary edema 0.0004 6.329 0 Anterior myocardial 0.0004 1.953 0
infarction Heart rate 0.0002 1.019 1 Atrial fibrillation 0.0023 3.289 0 Peripheral vascular disease 0.0027 2.852 14 Tobacco use 0.0033 0.523 5 Systolic blood pressure 0.0035 0.988 1 Type Ii otrioventricular block 0.0061 2.898 0 History of congestive heart 0.0128 2.933 9
failure History of hypertension 0.0769 12 Weight 0.1 122 26 History of angina 0.1219 0 Third-degree atrioventricular 0.1666 0
block Time 0.1997 Third heart sound 0.2529 2;
Multivariate Predictors
Number of leads with ST 0.0001 1.245 total: 80 elevation
Age 0.0001 1.080 Heart rate 0.0003 1.023 Diabetes mellitus 0.0011 2.105 Shock 0.0024 4.425 Prior myocardial infarction 0.0119 1.818 biastolic blood pressure 0.0376 0.986
BRIEF REPORTS 827

nary intervention has been established as most effica- tients can be identified by 2 criteria. The first is the com- cious for these patients. bination of age 260 years and >3 leads with ST eleva-
Table I lists results of the univariate analyses. Sev- enteen of the 23 variables were associated with 6-week
tion. The second is the presence of diabetes in a patient who is either 260 years of age or has >3 leads of ST ele-
mortality. For continuous variables, the odds ratio per- vation. These criteria address risk stratification of indi- tains to a single increment. For example, each addition- vidual patients with several clinical variables simulta- al year of age is associated with an odds of death at 6 weeks of 1.08. Larger increments can lead to substantial
neously considered. The c statistic for the training set,
odds ratios: the odds ratio for mortality in a patient >65 the 2,819 patients who received 100 mg of t-PA, was
years of age compared with age 165 years is 3.3. 0.68. When these criteria were used on a prospectively
Results of multivariate analysis are also listed in identified test set-the 519 patients in TIM1 II who received 150 mg of t-PA-the c statistic was 0.59, indi-
Table I. Almost all variables had highly significant p val- ues. The c statistic for the whole regression model
eating relatively low discriminatory ability of these cri- teria when used alone without other relevant informa-
applied to the training set from which it was derived is tion. 0.78. For a dichotomous outcome, the c statistic is equiv- . . . alent to both the area under the receiver-operating char- acteristic curve and the Wilcoxon statistic. For 2 patients,
In the prethrombolytic era, predictors of decreased
1 of whom has an outcome of interest, the c statistic is survival from the history included age, prior myocardial
the probability that the prediction rule will correctly infarction, diabetes, impaired myocardial function, and limited cardiac reserve.6,7 Predictors obtained from
identify which patient has the outcome of interest. The value of 0.78 indicates that given 2 TIM1 patients, 1 who
physical examination included evidence of hemody-
survives and 1 who dies, the regression model has a 78% namic compromise such as tachycardia, hypotension,
chance of correctly predicting which patient will die. and rales.* Predictors from the electrocardiogram includ- ed the number of leads with ST elevation, anterior loca-
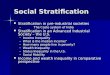
An example of the proposed stratification can be seen in Figure 1. In this algorithm, patients are first divided
tion, ST depression, and the sum of the amplitudes of ST elevation.9J0 A regression model with 6 clinical vari-
according to the most significant variables emerging from the multivariate analysis, age and number of leads
ables demonstrated a reasonable ability to discriminate
with ST elevation. When high risk is arbitrarily defined patients at high risk for mortality based on area under the receiver-operating characteristic curve.ii However,
as double the baseline treated-mortality, high-risk pa- predictors of mortality in the thrombolytic era may be
MI 2619 pts received 1 OOmg t-PA
I
exclude
<
missing data 11 pts age > 75 1 pt shock or hypotension 182 patients
AMI 2625 98/2625 (3.7%)
/ \
age < 60 age 60-75 29/1512 (1.9%) 69/l 113 (6.2%)
/ \ / \
d 3 leads ST elevation > 3 leads ST elevation < 3 leads ST elevation > 3 leads ST elevation E/808 (1 .O%) 211704 (3.0%) 29/623 (4.7%) 40/490 (6.2%)
A A A /--A
no F& AMI prior AMI no prior AMI prior AMI t-o prior AMI prior AMI no prior AMI prior AMI 31709 (0.4%) 5199 (5.1%) 18/636 (2.8%) 366 (4.4%) 2X519 (4.4%) 6004 (5.8%) 31/41X (7.6%) 9/84 (10.7%)
no diabetes diabetes no diabetes diabetes no diabetes diabetes no diabetes diabetes
6/718 (0.8%) 2/90 (2.2%) 151628 (2.4%) W6 (7.9%) 2IY541 (3.7%) Q/82 (11 .O%) 32/395 (8.1%) 8/95 (8.4%)
HR<lOO HR > 100 HR < 100 HR>lOU HR<lOO HR>lCO HR 5 100 HR>lGU
71783 (0.9%) l/25 (4.0%) 17/648 (2.6%) 456 (7.1%) 291603 (4.6%) w20 (0.0%) 35/453 (7.7%) 5137 (13.5%)
FIGURE 1. Al taliiy in the Tf
orithm for clinical risk stratification of patients who received thrombolytic therapy. or romboiysis in Myocardial Infarction Phase II trial. HR = heart rate; Ml = myocardial m rction.
.yrtianr indicate 6-week mor-
828 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 OCTOBER 15, 1995

different not only because of the thrombolytic agent itself, but also because only a fraction of patients actu- ally receive thrombolytic therapy, a selection bias. For example, in a prethrombolytic era assessment as detailed by the Multicenter Postinfarction Research Program, the population upon which the stratification was based was older, included more patients with decreased left ven- tricular function and rales, and more patients with New York Heart Association class III or IV heart failure than the population in the TIM1 II study.i5
Our results indicate that prethrombolytic era predic- tors of early mortality remain important predictors in the thrombolytic era, despite the selection bias and the effect of the thrombolytic agent. Age, prior myocardial infarc- tion, diabetes, heart rate, infarct size determined by the number of leads with ST elevation, and cardiogenic shock all remain independent predictors. Note that these variables identify patients who will both benefit from thrombolytic therapy and yet still have a relatively high- er mortality than the average patient treated with throm- bolytic therapy. l6
These findings contirm results of previous studies of patients who received thrombolytic therapy and allow identification of high-risk patients based on clinical vari- ables available on presentation.17 Simoons and Arnold’* determined the risk by the total number of risk factors present. In the TIM1 II data set, 2 criteria based on 3 clinical variables allow identification of high-risk patients. Both the presence of ST-segment elevation in >3 leads in a patient 260 years of age, or the presence of diabetes in a patient with either >3 leads with ST ele- vation or age 260 years, will identify patients who have a 6-week mortality twice that of the average patient who receives t-PA. The clinician can better manage myocar- dial infarction with an awareness of which patients are high risk. Mortality is related to early reperfusion, and close monitoring for early reperfusion is therefore imper- ative in high-risk patients.19
The relatively low values of the c statistics of the multivariate regression model and the predictive algo- rithm are a limitation. Although some high-risk patients are identified, additional variables need to be considered to identify patients who do not have these risk factors, yet do not survive. The prediction algorithm allows a rough classification; more information must be consid- ered to arrive at the positive predictive value for mor- tality, a key piece of information necessary for the man- agement of individual patients. The use of angiographic and other studies would certainly improve prediction of early mortality, but the focus of this analysis was on the use of immediately available clinical information for ear- ly management and on validating the prethrombolytic era studies in the present era. Some of the most impor- tant considerations from the point of view of therapy are the amount of myocardium at risk and the intensity of the ischemia.2 Additional risk stratification is helpful to place the overall prognosis in context.
In conclusion, predictors of short-term mortality for patients with acute myocardial infarction have not changed with the advent of the thrombolytic era. Two criteria based on age, diabetes, and number of leads with ST elevation suggest which patients are at highest risk and may warrant further consideration for either additional or alternate therapy.
1. GISSI Investigators. Effectiveness of intravenous tbmmbolytic treatment in acute myocardial infarction. Lancer 1986;1:397-401. 2. Mauri R, Gaspwini M, Barbonaglia L, Santoro E, Franzosi MG, Tognoni G, Rovelli F. Prognostic significance of the extent of myocardial injury in acute myo- cardial infarction treated by streptokinase (the GISSI trial). Am J Car&l 1989;63: 1291-1295. 3. Ellis SG, Ribeiro da Silva E, Heyndrickx G, Talley JD, Cemigliaro C, Steg G, Spaulding C, Nobuyoshi M, Erbel R, Vassanelli C, Top01 ET, for the RESCUE Investigators. Randomized comparison of rescue angioplasty with conservative management of patients with early failure of tbmmbolysis for acute anterior myo- cardial infarction. Circulation 1994;90:228&2284. 4. Stone GW, Grines CL, Browne KF, Marco J, Rotbbaum D, O’Keefe J, Hattzler GO, Overlie P, Donohue B, Chelliah N, Timmis GC, Vliestra R, Strzelecki M, Puchrowicz-Ochocki S, O’Neill WW. Predictors of in-hospital and 6-month out- come after acute myowdial infarction in the reperfusion era: the Primary Angio- plasty in Myocardial Infarction (PAMI) Trial. JAm Co0 Cardiol 1995;25:370-377. 5. TIM1 Study Group. Comparison of invasive and conservative strategies after treatment with intravenous tissue plasminogen activator in acute myocardial infarc- tion. Results of the Thrombolysis in Myocardial Infarction (TIMI) Phase II trial. N En@ J Med 1989;320:618627. 6. Stone PH, Muller JE, Hartwell T, York BJ, Rutherford JD, Parker CB, Turi ZG, Strauss W, Willerson IT, Robertson T, Braunwald E, Jaffee AS, and the MILIS Study Group. The effect of diabetes mellitus on prognosis and serial left ventricu- lar function after acute myocardial infarction: contribution of both coronary disease and diastolic left ventricular dysfunction on adverse prognosis. J Am Coil Cardiol 1989;14:49-57. 7. Nicod P, Gilpin E, Dittrich H, Polikar R, Hjalmarson A, Blacky R, Henning H. Ross J Jr. Shalt- and long-term clinical outcome after Q wave and non-Q wave myocardial infarction in a large patient population. Circulation 1989;79:528-536. 8. Henning H, Gilpin EA, Cove11 JW, Swan EA, O’Rourke RA, Ross J Jr. Prog- nosis after acute myocardial infarction: a multivariate analysis of mortality and sur- vival. Circulation 1979;59: 1124-I 136. 9. Hackworthy RA, Vogel MB, Harris PI. Influence of infarct artery patency on the relation between initial ST segment elevation and final infarct size. Br Heart J 1986;56:222-225. IO. Krone RJ. The role of risk stratification in the early management of a myo- cardial infarction. Ann Intern Med 1992;116:223-237, 11. Selker HP, Griffith JL, D’Agostino RB. A time-insensitive predictive instm- ment for acute myocardial infarction mortality: a multicenter study. Med Care 1991; 29:119&1211. 12. Bigger JT Jr, Heller CA, Wager TL, Weld FM. Risk stratification after acute myocardial infarction. Am J Cardiol 1978;42:202-210. 13. Schechtman KB, Capone RJ, Kleiger RE, Gibson RS, Schwartz DJ, Roberts R, Bode” WE, and the Diltiazem Reinfarction Study Group. Differential risk pat- terns associated with 3 month as compared with 3 to 12 month mortality and rein- farction after non-Q wave mywardial infarction. J Am Coil Cardiol 1990.15: 94&947. 14. Pierard LA, Chapelle JP, Albert A, Dubois C, Kulberh~s HE. Characteristics associated with early (53 months) Venus late (>3 months to 53 years) mortality after acute myocardial infarction. Am J Cardiol 1989;64:315-318. 15. Multicenter Postinfarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med 1983;309:331-336. 16. Fibrinolytic Therapy Trialists’ Collaborative Group. Indications for fibrinolyt- ic therapy in suspected acute myocardial infarction: collaborative overview of ear- ly mortality and major morbidity results from all randomised trials of more than loo0 patients. Lancet 1994;343:31 l-322. 17. Mueller HS, Cohen LS, Braunwald E, Forman S, Feit F, Ross A, Schweiger M, Cabin H, Davison R, Miller D, Solomon R, Knattemd GL, for the TIMI Inves- tigators. Predictors of early morbidity and mortality after tbrombolytic therapy of acute myocardial infarction. Circulation 1992;85:1254-1264. 18. Simoons ML, Arnold AER. Tailored thrombolytic therapy: a perspective. Cir- culation 1993;88:255&2564. 19. Rawles J. Halving of mortality at 1 year by domiciliary thmmbolysis in the Grampian Region Early Anistreplase Trial (GREAT). JAm Coil Cardiol 1994;23: l-5.
BRIEF REPORTS 829