Embed Size (px)
Citation preview

8/24/2015
1
Feeding Your Wound: Fuel to Heal
2014 NPUAP/EPUA
P/PPPIAGuidelines
Mary Ellen Posthauer,RDN,LD,CD,FAND
Objectives
1• Recognize the importance of screening and assessment to
identify malnutrition risk
22• Examine the building block of nutrition(macronutrients and micronutrients)
that dominate healing2. that dominate healing
3• Apply the 2014 NPUAP/EPUAP/Pan Pacific Pressure Injury Alliance nutrition
guidelines into practice
4. • Discuss practical nutrition and hydration strategies for healing wounds
Defining Pressure Ulcers
A pressure ulcer is a localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure, or pressure in combination with shear. ( def. NPUAP-EPUAP, 2009)
Normal Stage 1 Stage 2 Stage 3 Stage 4
Pathogenesis of Pressure Ulcers
Cell (and tissue) death Decrease in
capillary flow
Pressure, shear, friction
Oedema
Fluid escapes into extravascularspace
Adapted from: “ABC of Wound Healing”, Blackwell Publishing, 2006
Increased capillary permeability
Ischaemia, capillary thrombosis, and occlusion of lymphatic vessels
Pressure Ulcer Points:Source for diagram: Saha S, Smith MEB, Totten A, et al Gov. document
Effective pressure ulcer treatment: multidisciplinary & holistic
Support SurfacesMattresses
Wound CareD i
Nursing & CareT i i
NutritionD li f
Pressure Ulcer Care
Mattresses, cushions,
protection, etc.
Dressings,cleaning, drainage,
etc.
Turning regimes, hygiene, etc.
Delivery of nutrients to
stimulate healing

8/24/2015
2
NPUAP/EPUAP/PPPIA Pressure Ulcer Prevention and
Treatment Guidelines
Goal of Guideline
• The goal of this international collaboration was to develop evidence-based recommendations for the prevention and treatment of pressure ulcers that could be used by health
f i l h h h ldprofessionals throughout the world.• Produced by the Guideline Development
Group(GDG). • Each section had a small work group (SWG)
representatives from each organization.
Guideline Recommendations• SWG-reviewed the entire body of evidence
including new literature and existing evidence tables.
• Formulated conclusions and developed recommendations.
• Reviewed 2009 guidelines and revised based on d
gnew evidence rating.
• Determined strength of body of evidence.• Recommendations and evidence summaries
reviewed by GDG and 986 invited international stakeholders.
• Final draft approved by GDG.• Final stage was determining strength of each
recommendation statement.
General Guideline• The recommendations in this guideline are a general
guide to appropriate clinical practice, to be implemented by qualified health professionals subject to their clinical judgment of each individual case and in consideration of the patient consumer’s personal
f d il blpreferences and available resources.• The guideline should be implemented in a culturally
aware and respectful manner in accordance with the principles of protection, participation and partnership.
10
Criteria
InclusionsStudy designs: Clinical controlled trials with a
minimum of 10 subjectsSystematic reviews with
ExclusionsAnimal studies (unless
other not available)
Studies of chronicounds unless subSystematic reviews with
Cochrane methodologymeta-analyses
Qualitative studies as appropriate to the topic
wounds - unless sub-group of >10 subjects with Pressure Ulcers
was analyzed separately
Level of Evidence Ratingto Support Recommendations
• A – Direct scientific evidence from properly designed and implemented controlled trials on PrU in humans ( or humans at risk of PrUs), providing statistical results that consistently support the recommendation ( level 1 studies/clear cut evidence
• B Direct scientific evidence from properly designed• B –Direct scientific evidence from properly designed and implemented clinical series on PrU in humans ( or humans at risk of PrUs)providing statistical results that consistently support the recommendation
• C – Indirect evidence (e.g., healthy humans, animal models and/or other types of chronic wounds and/or expert opinion)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline

8/24/2015
3
Strength of Recommendations (SOR)Assists Health Professionals Prioritize Interventions
Strong positive recommendation: definitely do it
Weak positive recommendation: probably do it
No specific recommendationNo specific recommendation
Weak negative recommendation: probably don’t do it
Strong negative recommendation: definitely don’t do it
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Malnutrition
• Increases morbidity and mortality.
• Decreases function and quality of life.
• Increases frequencyIncreases frequency and length of hospital stay.
• Increases health care costs.
White, 2012 J Acad Nutr Diet. 2012 112(5): 730-738.
Diagnosing Adult Malnutrition
The following factors may make malnutrition diagnoses more difficult:
• Infection, stress • Hydration status• Multiple drug use • Chronic disease• Acute illness • Changes in organ
function
Inflammation and Malnutrition• Inflammation (d/t
infection, injury, surgery, etc.): an important underlying factor that increases risk for malnutrition.
• May contribute to suboptimal response to nutrition intervention and increased risk of mortality.
White J, J Acad Nutr Diet2012:112:730-738
Definitions: Adult Malnutrition
• “Malnutrition is most simply defined as any nutritional imbalance.” (Dorland 2011)
• Undernutrition: lack of calories, protein or other nutrients needed for tissue maintenance and repair.
• Undernutrition and malnutrition used interchangeably.
White J, J Acad Nutr Diet 2012:112:730-738
Diagnosing Malnutrition: 2009 Academy Workgroup (with ASPEN reps.)
Identification of >2 of the following characteristics:1. Insufficient energy intake2. Weight loss3. Loss of muscle mass4. Loss of subcutaneous fat5. Localized or generalized fluid accumulation that may
sometimes mask weight loss6. Diminished functional status as measured by hand
grip strength (strong research; cost effective)White J, J Acad Nutr Diet 2012:112:730-738

8/24/2015
4
Definitions: Adult Malnutrition
• Adult undernutrition: continuum of inadequate intake
Malnutrition ContinuumNon-severe Severe
qand/or increased requirements, impaired absorption, altered transport, and altered nutrient utilization.
• Weight loss can occur at multiple points along this continuum.
• May also have inflammatory, hypermetabolic, and/or hypercatabolic conditions.
White J, J Acad Nutr Diet 2012:112:730-738
Malnutrition and Pressure Ulcers
Fry Fry • Pre-existing malnutrition/weight loss increased the
odds of developing a PU 3.8 times. (2010)
• Australia, odds ration of having a pressure ulcer are hi h ith l t iti i t d LTC (2010)Banks higher with malnutrition in acute and LTC. (2010)
IizakaIizaka• Home care study in Japan: ≥ 65, rate of malnutrition
58.7% with pressure ulcers compared to 32.6% without them. (2010)
Nutrition Screening,
Assessment, and Care PlanningCare Planning
Nutrition Screening
Nutrition Screening
1. Screen nutritional status for each individual at risk of or with a pressure ulcer:– at admission to a health care setting; – with each significant change of clinical condition;
and/or – when progress toward pressure ulcer closure is
not observed. (Strength of Evidence = C, Strength of Recommendation -SOR = probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Nutrition Screening
2. Use a valid and reliable nutrition screening tool to determine nutritional risk. (Strength of Evidence = C, SOR= Probably do it)
3. Refer individuals screened to be at risk of malnutrition and individuals with an existing pressure ulcer to a registered dietitian or an interprofessional nutrition team for a comprehensive nutrition assessment. (Strength of Evidence = C; SOR=probably do it.)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Nutrition Screening Tool
Quick and Easy
Acceptable
Validated

8/24/2015
5
Validated Screening Tools
MST Malnutrition
Valid and reliable for use in acute care and ambulatory care to identify
MNA Mini-
Nutritional AssessmentValidated in individuals with PUs V lid d
MUS
T Malnutrition Universal Screening ToolTo identify risk of undernutrition
Malnutrition Universal Screening ToolTo identify risk of undernutrition
SNAQ Short
Nutrition Assessment QuestionnaireAcute care, residential care and
i
25
identify malnutrition(Ferguson, M et al. Nutrition1999 15:458-464.)
Validated and easy to use in older adults(Paudla 2012)
www.mna-elderly.com/
undernutrition (BAPEN, 2008)Validated for use in older adults admitted to acute carehttp://www.bapen.org.uk/must_tool.html
undernutrition (BAPEN, 2008)Validated for use in older adults admitted to acute carehttp://www.bapen.org.uk/must_tool.html
community adults >65.http://www.fightmalnutrition.eu/fight-malnutrition/screening-tools/snaq-tools-in-english/
Malnutrition Screening Tool (MST)Step 1:• Have you recently lost weight
without trying?• If yes, how much have you lost?• Have you been eating poorly
because of a decreased appetite?Step 2: Score to determine riskSt 3 I t ith t iti lStep 3: Intervene with nutritional support for those at risk of malnutrition
http://static.abbottnutrition.com/cms-prod/abbottnutrition.com/img/Malnutrition%20Screening%20Tool_FINAL.pdf
Mini Nutritional Assessment®
MNA®
Validated and easy to use in geriatric patients
Acute care, hospital based ambulatory care, LTC
http://www.mna-elderly.com
27
Malnutrition Universal Screening Tool
MUSTTo identify risk of undernutrition(BAPEN, 2008)
BMIWeight loss past 3-4 monthsAcute disease (no intake >5 days)
http://www.bapen.org.uk/must_tool.html
28
Short Nutritional Assessment Questionnaire Braden Nutrition Sub-Score
Information must be accurate at the time completed!
• How often does a person admitted to acute or LTC eat every meal?LTC eat every meal?
• Is the form completedprior to eating any meals?
• NPO & clear liquid diet?• Can you verify amount
of protein consumed?

8/24/2015
6
Comprehensive Nutrition AssessmentAcademy’s Nutrition Care Process
Nutrition:1. Assessment 2 Di i2. Diagnosis 3. Intervention4. Monitoring and
Evaluation
Purchase the NCPT online at [email protected]
Nutrition Assessment
Diagnosis/ Adequacy of Height weight
Medical Hx, Physical Exam
Diet History, Food Intake
Body Composition
Diagnosis/recent changes
in condition (depression)MedicationsRisk or S/S of malnutrition, dehydration
Adequacy of food/fluid
intake compared to
needsChewing,
swallowing, self feeding, GI
issues
Height, weight, wt. history,
UWL (>5% in 30 days or
>10% in 180 days), BMI <19
Insidious weight loss
Nutrition Assessment
d di i Wi h id
Current Interventions Interviews
Nutrition Focused Physical
ExaminationFood or dining
related interventionsOral nutrition supplements
Nutrition support
With resident, family and/or
staff Acceptance to interventions
Compare goals to outcomes
Overall appearance/ indicators of PEMOral examination Skin examination
Unintended Weight Loss
• May be best indicator of undernutrition
• Reflects poor intake and/or inability of body to metabolize nutrients
• LTC- 50%-75% leave 25% uneaten
Simmons,SF et al. Accurracy of Minimun Data Set in identifying resident at risk for undernutrion: oral intake and food complaints. 2002. Jr. of Am Ger S3(May/June:140-149.
Focus of Nutritional Assessment• Evaluation of:
– Energy intake– Unintended weight change
(insidious weight loss, obese individuals also at risk)
– Effect of psychological stress or neuropsychological problems
• Include a determination of the individual’s caloric, protein and fluid requirements.
Every Pound Counts Counts
Loss of Weight Complications Associated Mortality
10% ↓immunity, ↑ infections
10%
20% ↓ healing, weakness,infection
30%
30% too weak to sit, pressure ulcers, pneumonia,
no healing
50%
40% DEATH,usually from pneumonia
100%
R. Demling

8/24/2015
7
Dietary Intake
• Depression affects appetite of 30% of adult outpatients.
• Loss of appetite related to high risk of malnutrition.
• Increases risk of poor wound healing.
• Decreased ability to eat independently.
↓Risk for undernutrition and delayed healing.
Horn 2004; Gilmore 1995
What about Labs?
No lab test can specifically determine an individual’s nutritional status.
• Serum protein levels may beSerum protein levels may be affected by metabolic stress, inflammation, renal function, hydration and other factors.
What about Labs for Diagnosis of Malnutrition?
Not recommending any specific inflammatory markers for diagnosis at this time.
Inflammatory biomarkers, C-reactive protein and other positive acute phase reactants were excluded – no conclusive relationship to nutritional status White J, J Acad Nutr Diet 2012:112:730-730
Inflammation and StressRelease of Cytokines
Muscle
Decreased nitrogen retention
Decreased albumin synthesis
Extravasation of albumin from intravascular
Anorexia
usc eWasting
intravascular spaces
Decreased circulating levels of albumin and
cholesterolSource: Council for Nutrition Clinical Strategies in LTC
CytokinesInterleukin – 1Interleukin – 2Interleukin – 6Tumor necrosis
factor aCiliary
neurotrophic factor
Nutrition Assessment
1. Assess weight status for each individual to
determine weight hi t d
2. Assess the individual’s
3. Assess the adequacy of total
nutrient intakehistory and significant weight
loss from usual body weight (>5% change in 30 days or >10% in 180 days).
SOE = C; SOR= Probably do it
individual s ability to eat
independently. SOE = C; SOR= Definitely do it
nutrient intake (food, fluid, oral
supplements, enteral/parenteral
feedings). SOE = C; SOR= Definitely do it©2014
NPUAP-EPUAPPPIA
Pressure Ulcer
Prevention and
Treatment Guidelines
Care Planning1. Develop an individualized nutrition care plan for
individuals with or at risk of a pressure ulcer. (SOE = C, SOR= Probably do it)
1. Follow relevant and evidence-based guidelines on gnutrition and hydration for individuals who exhibit nutritional risk and who are at risk of pressure ulcers or have an existing pressure ulcer. ( SOE=C, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline

8/24/2015
8
Interprofessional Team
Resident: focus of
Resident: focus of
PhysicianPhysician
RDN,DTRRDN,DTRDining Service Director
Dining Service Director
Allen 2013- quasi-experimental study on effects of comprehensive interprofessional nutrition protocol
focus of care
focus of care
SLP/OTSLP/OT
Nursing staff Nursing staff
CNA/feeding assistants
CNA/feeding assistants
General Recommendations: Nutrition Interventions for Pressure Ulcers
General Recommendations
Use your clinical judgment based on a thorough medical
Individualized care plan should focus on:• improving and/or
maintaining overallgand nutritional assessment to make appropriate individualized recommendations
maintaining overall nutritional status
• acceptance of nutrition interventions
• clinical outcomes
What Does the Evidence Suggest?
Responsive increase in
metabolic rate Energy is
Need to provide
adequate calories to
Energy Intake
which increases
caloric needs (triggered by
PrU, infection, severe illness, trauma, etc.)
Energy is essential for
pressure ulcer healing
promote anabolism,
nitrogen and collagen synthesis Creda 2011,
Yamamoto 2009
The Non-healing Chronic WoundFailure to Heal by 12 Weeks
The Non-healing Wound The Healing Wound
Neutrophils O2
↑ Catabolism ↓ Anabolism
Energy Protein Synthesis
Wound contraction
↑ Anabolism ↓ CatabolismEnergy Protein Synthesis
Macronutrients
Energy Protein Synthesis
Macronutrients
EnergyStore
ProteinStore
Energy
Store
Protein
Store
Energy Intake1. Provide individualized energy intake based on
underlying medical condition and level of activity. (SOE = B, Probably do it)
2. Provide 30 to 35 kcalories/kg body weight for adults at risk of a pressure ulcer who are assessed as beingat risk of a pressure ulcer who are assessed as being at risk of malnutrition. (SOE = C, SOR= Probably do it)
3. Provide 30 to 35 kcalories/kg body weight for adults with a pressure ulcer who are assessed as being at risk of malnutrition. (SOE = C, SOR= Definitely do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline

8/24/2015
9
Energy Intake
4. Adjust energy intake based on weight change or level of obesity. Adults who are underweight or who have had significant unintended weight loss may need additional energy intake. (SOE = C, SOR= Definitely do it)
5. Revise and modify/liberalize dietary restrictions when limitations result in decreased food and fluid intake. These adjustments should be made in consultation with a medical professional and managed by a registered dietitian whenever possible. (SOE = C, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Energy Intake
6. Offer fortified foods and/or high calorie, high protein oral nutritional supplements between meals if nutritional requirements cannot be achieved by dietary intake. (SOE = B, SOR= Definitely do it)Definitely do it)
7. Consider nutritional support (enteral or parenteral nutrition) when oral intake is inadequate. This must be consistent with the individual’s goals. (Strength of Evidence = C, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Nutrition Support
NPO >3-5 days
Hydration with IVs does notHydration with IVs does not supply nutrients
Places individual at risk of undernutrition and pressure ulcer development
Enteral FeedingsDetermine if patient actuallyreceives TF as prescribed:• Is TF given as ordered
(product, mLs/hr)? • Are flushes given as ordered g
(flushes, flushes with meds)?• Is the strength correct?• Is the individual tolerating
the feeding?• Round the clock or
intermittent (turned off)?
Protein What Does the Evidence Suggest for PrUs?All stages require adequate protein
Increased protein levels have been linked to improved healing rates
Protein intake must be sufficient to prevent PEM, promote healing and a positive nitrogen balance

8/24/2015
10
Ensure Adequate Protein Intake
15%-38% of older men eat less than the RDI for protein.
27% 41% f ld27%-41% of older women eat less than the RDI for protein.
Morley J et. al. Nutritional recommendations for the management of sarcopenia J Am Med Dir 2010;11:391-396.)
55
What Does the Evidence Suggest for Optimal Protein Intake for Older Adults
• Positive association between protein ingestion and muscle mass
• Protein spread equally• Protein spread equally between breakfast lunch and dinner )
• If needed, additional protein supplementation should given between meals
Factors Influencing Protein Intake in Older Adults
• Inadequate intake = appetite loss or GI disturbances.
• Reduced ability to utilize available protein=insulin resistance, protein anabolic resistance immobilityresistance, immobility.
• Increased need for protein= inflammatory disease, increased oxidative modification of protein, catabolic conditions associated with acute and chronic diseases.
All Lead to Loss of FunctionalityEvidence-Based recommendations for optimal dietary protein intake in older people: a Position Paper from the PROT-AGE Study Group, JAMDA 2013.
Protein Distribution
Protein Intake
1. Provide adequate protein for positive nitrogen balance for adults assessed to be at risk of a pressure ulcer. (SOE = C, SOR= Probably do it)
2. Offer 1.25 to 1.5 grams protein/kg body weight daily for an adult at risk of a pressure ulcer who is assessed to be at risk of malnutrition when compatible with goals of care, and reassess as condition changes. (Strength of Evidence = C), SOR =Probably do it
3. Provide adequate protein for positive nitrogen balance for an adult with a pressure ulcer. (Strength of Evidence = B, Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Protein Intake
4. Offer 1.25 to 1.5 grams protein/kg body weight daily for adults with an existing pressure ulcer who is assessed to be at risk of malnutrition when compatible with goals of care, and reassess as condition changes. (SOE = C, SOR= Probably do it)g ( , y )
5. Offer high calorie, high protein nutritional supplements in addition to the usual diet to adults with nutritional risk and pressure ulcer risk, if nutritional requirements cannot be achieved by dietary intake. (SOE = A, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline

8/24/2015
11
Medical Food Supplements
Foods that are specially formulated & processed for the resident who is seriously ill or who requires the product as a major treatment modality
Criteria:Criteria: ◦ for oral or tube feeding◦ labeled for the dietary management of a specific
medical disorder, disease, or condition for which there are distinctive nutritional requirements◦ intended to be used under medical supervision
Protein Intake
6. Assess renal function to ensure that high levels of protein are appropriate for the individual. (SOE = C, SOR= Definitely do it)
– Clinical judgment is required to determine the appropriate level of protein for each individual, based on the number of pressure ulcers present, overall nutritional status, co-morbidities, and tolerance to nutritional interventions.
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Protein Intake
7. Supplement with high protein, arginine and micronutrients for individuals with a pressure ulcer Category/Stage III or IV or multiple pressure ulcers when nutritional requirements cannot be met with traditional high calorie and protein supplements. g p pp(SO E = B, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Evidence on Amino Acids
Arginine May become conditionally indispensible during
May have some immune stimulating
effects indispensible during acute stress. Stimulates collagen synthesis.
Several recent studies demonstrate
promising results such as the CUBE &
Oligo study
64
A multi-country, randomized, placebo-controlled trial to demonstrate the efficacy of a specific ‘arg+ONS-spec.’) on pressure ulcer healing in non-malnourished patients with stage III-IV ulcers
Ready-to-drink, high-protein, arginine
CUBE Trial
enriched nutritional supplement Containing per 200-ml serving:
20 g protein3 g L-arginine250 kcalVitamins and micronutrients including:250 mg vitamin C38 mg vitamin E (α-TE)9 mg zinc1.5 mg carotenoids
Patient inclusion
Patients• Between 18 yrs and 90 yrs• Stage III or IV pressure ulcers
(EPUAP & NPUAP grading)• BMI ≥18.5 (18-70 yrs) or BMI ≥21 (>70 yrs)• Nursing home or hospital based
Total group (ITT)
Age* 74.9 ± 14.6 y
BMI* 24.4 ± 4.8 kg/m2
Ulcer stage III/IV 31/12 (72/28%)
Pressure ulcer 10 5 ± 11 5 2Nursing home or hospital based
size* (ellipse)10.5 ± 11.5 cm2
PUSH tool score* 11.5 ± 3.1
Set-up43 patients in intention-to-treat analysis (ITT)-Intervention (‘arg+ONS-spec.’) group: 22 patients-Control (placebo) group: 21 patients-Product use: 3x200 ml/day; max. 8 weeks-Standard diets and pressure ulcer care were maintained
No sign. differences between groups at baseline* means ± SD

8/24/2015
12
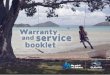
Faster Reduction in Ulcer Size
8
10
12
14
16
CubitanControl
ize
(cm
2 )
0 7 14 21 28 35 42 49 560
2
4
6
8
Days
Ulc
er s
i
Specific oral nutritional support improved ulcer healing -indicated by area reduction- compared to the control group over the period of 8 weeks.
Earlier Reduction in Ulcer Size from Baseline
0 10 20 30 40
Cubitan
Control
With specific oral nutritional support a significant reduction in ulcer size was reached 2 weeks earlier compared to the control group.
• First time-point with a significant reduction compared to baseline
• Arg+ONS-spec.= day 21, P=0.011
• Control group = day 35, P= 0.019
• Means ± SEM; data adjusted for center 68
0 10 20 30 40Days
Conclusion
• Supplementation with additional protein, arginine, and micronutrients accelerated pressure ulcer healing in non-malnourished patients.
• The number of wound dressings, as well as the time needed for changing the dressings, was lower with specific nutritional
t th i d f 8 ksupport over the period of 8 weeks.
• Specific nutritional support can be cost-saving by reducing overall health care costs.
• With specific nutritional support more nursing time is available for other relevant patient care related activities.
• These results warrant further health economics investigations into the benefits of specific ONS.
Oligo Element Trial Study Group
• Multicenter, RCT to evaluate supplementation with arginine, zinc & antioxidants in high-calorie, high-protein formula to improve PrUhealing
• 200 malnourished patients with stage II,III,andIV PrUs
• 8 week trial – LTC and home care in Italy• Majority of PrUs on sacrum
Malnourished criteria
• UWL – 5%(30 days) and 10% 3months• BMI< 20 age <65 and < 21 > 65• Food intake (<60% of estimated total daily
energy requirements in the week before the gy qstudy)
• Both groups received a 400 mL high-calorie, high-protein formula (100 Ml ,4x /day)
• Standard wound care for all
Nutritional Supplement in 100mL
Intervention• Protein 10 grams• Arginine-L 1.5• Zinc 4.5 mg
Standard: Control• Protein 10 grams• Arginine-0• Zinc 2.3 mg.g
• Copper 675 mg• Vitamin C 125 mcg• Vitamin E 19.0 mg
29.8% protein from calories
g• Copper 338 mg• Vitamin C 19mcg• Vitamin E 2.3 mg
29.5 % protein from calories

8/24/2015
13
Conclusion
• 69.9% in intervention formula group had 40% or greater reduction in PU size compared to 54.1% in control at 8 weeks
• The efficacy of these nutrients in wound healing is likely synergistic because there is no evidence y y gsupporting an independent effect when given alone
• This nutritional intervention may be beneficial when added to optimized local wound care for the treatment of pressure ulcers in malnourished patients.
Amino Acids
Meet total calorie/ protein
needs first…
…before trying specialized
interventions
Fluids: What Does the Evidence Suggest?
Dehydration is a risk factor for pressure ulcer development
Hydration needs must be met to assure proper
prevention and healing
Hydration
1. Provide and encourage adequate daily fluid intake for hydration for an individual assessed to be at risk of or with a pressure ulcer. This must be consistent with the individual’s comorbid conditions and goals. (SOE = C, SOR= Definitely do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Hydration
2. Monitor individuals for S/S dehydration: changes in weight, skin turgor, urine output, elevated serum sodium and/or calculated serum osmolality. (SOE = C, SOR= Probably do i )it)
3. Provide additional fluid for individuals with dehydration, elevated temp, vomiting, profuse sweating, diarrhea or heavily draining wounds. (SOE = C, SOR= Definitely do it)
77
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Fluids
Needs increase
di
Needs may
daccording to
insensible water loss
decrease for CHF,
renal failure

8/24/2015
14
Methods of Calculating Fluid Needs
In generally healthy individuals that
1 mL/calorie consumed
30 mL/kg BW/day
are adequately hydrated, food accounts for >20% of total fluid intake. (DRI 2004)
Total fluid needs include water content of food.
What Does the Evidence Suggest?
Micronutrients
Micronutrients
Most nutrient needs can be met through a healthy diet
However, individuals with pressure ulcers may not be consuming an adequate diet to meet established nutritional reference standards
Vitamins and Minerals1. Provide/encourage individuals
assessed to be at risk of pressure ulcers to consume a balanced diet that includes good sources of vitamins and minerals. (SOE = C, SOR = Definitely do it)
2. Provide/encourage an individual assessed to be at risk of a pressure ulcer to take vitamin ad mineral supplements when dietary intake is poor or deficiencies are confirmed or suspected. (SOE = C, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Vitamins and Minerals3. Provide/encourage an
individual with a pressure ulcers to consume a balanced diet that includes good sources of vitamins and minerals. (SOE = B, SOR = Definitely do it)
4. Provide/encourage an individual with a pressure ulcer to take vitamin and mineral supplements when dietary intake is poor or deficiencies are confirmed or suspected. (SOE = B, SOR= Probably do it)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Vitamin C
There is no evidence to support vitamin C above the RDI unless a deficiency is diagnosed or suspected.

8/24/2015
15
ZincZinc requirements can be met by 2 servings/ day of animal protein.• Meat • Liver• Milk• Milk• Eggs
A multivitamin/mineral supplement daily (15 mg zinc) may be adequate. (DRI 2004)
Zinc
No research has demonstrated an effect of zinc supplementation on improved pressure ulcer healing.
When clinical signs of zinc deficiency are present, zinc should be supplemented at <40 mg elemental zinc/day (UTL).
– Doses >40 mg/day can adversely affect copper status and possibly result in anemia.
– High serum zinc levels may inhibit healing. (Thomas 1997, Reed 1985, Dimant 1999, Goode 1992)
©2014 Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline
Obesity and Pressure Ulcers
.
87
Obese Individuals
• There are no evidence based guidelines available related to the nutritional needs of the obese person with pressure ulcers
• Adequate calories, protein, fluids and nutrients are needed for healing g– General consensus is that diets should be
liberalized to promote healing– Once the PrU is completely healed, diet
restrictions may be gradually implemented as needed
• Monitor skin integrity and coordinate with RDN (ongoing)
2013 NPUAP Unavoidable Pressure Injury State of the Science Census Conference
Unavoidable Pressure Ulcer
• In 2010 NPUAP defined an unavoidable PU as one that may occur even though providers have evaluated the individual’s clinical condition and PU risk factors have been evaluated and defined and interventions have been implemented that are consistent with individual needs, goals, and recognized standards of practice.
• Occurs even though providers have monitored and evaluated the impact of preventive interventions and revised these approaches as appropriate.

8/24/2015
16
2013 NPUAP Unavoidable Pressure Injury State of the Science Census Conference
• Individuals with malnutrition in combination with multiple comorbidities are at increased risk for the development of unavoidable pressure
• Cachexia is cytokine-associated wasting of protein reserves & energy stores due to the effect of diseases such as cancer, cardiac cachexia, ESRD, unavoidable pressure
ulcers. 91%
• Individuals with cachexiaare at increased risk for thedevelopment ofunavoidable pressureulcers. 100%
, ,COPD, cystic fibrosis, &rheumatoid arthritis.
• Cytokines directly cause feeding suppression & a lower intake of nutrients & is almost always accompanied by anorexia.
Older AgeAge-related skin changes: • flattening of the dermal
epidermal junction• slower cell turnover,
decreased elasticityhi i f b• thinning of subcutaneous
layers, • decrease in overall muscle
mass,• decreased intradermal
vascular perfusion and oxygenation.
Palliative Care Palliative/Hospice 2013 Diagnosis
• 37% terminal cancer
• 15% dementia• 13% heart disease• 10% lung disease• LOS 73 days• 20% > 90 days
Just One More Bite…
Personal feelings about death•Food is Life/Food is Love•Food is Life/Food is Love •Tendency to beg people to take just one more bite… •“We can’t let Mom starve!”
EthicsEthics:• Professional standards of
conduct • Philosophy dealing with
morals or how we protect the values of societythe values of society
Medical Training: • Treat aggressively• Save life at all costs• Food/fluid sustain life and
promote healing

8/24/2015
17
It is the position of the Academy of Nutrition and Dietetics…
“--that individuals have the right to request or refuse nutrition and hydration as medical treatment.
• RDs should work collaboratively as part of an interprofessional health care team to make recommendations on providing, withdrawing, or withholding nutrition and hydration in individual cases and serve as active members of institutional ethics committees.” Maillet JO’S, Schwart DB,Posthauer ME. Position of
Academy of Nutrition & Dietetics. Ethical and legal issues in feeding and hydration. J Acad Nutr Diet.
2013;113(6): 828-833..
Academy’s Position
• Affirms the patient’s right to self-determination as the overriding principle….
• Generally takes precedence over the beliefs or wishes of health care providers.
• Recognizes that each person approaches end of life with diverse cultural, religious, philosophical and personal values.
-Maillet JO’S, Schwartz DB,Posthauer ME. Position of Academy of Nutrition & Dietetics. Ethical and legal issues in feeding and hydration. J Acad Nutr
Diet. 2013;113(6): 828-833.
Health Literacy
• Degree to which individuals, process, and understand basic health information and services to make appropriate health care decisions.
• Involves range of social, culture, and individual factors, such as age, education, and raceReuben DB, Tinetti ME. Goal-oriented patient care —
an alternative health outcomes paradigm. N Engl J Med.2012;366(8):777-779.
Health Care Literacy
Health care provider• Due to the severity of the
PrUs and the dementia, enteral feeding is not recommended
Non-Health care person• The dementia is progressing and aggressive tube feeding will not reverse or cure the disease.
h li id f d b i l d i• It is time to stop nutrition support because if is not benefiting the individual
• Feeding your family member may result in aspiration pneumonia
•The liquid food being placed in the tube is not helping and may cause suffering. • Feeding your family member
when he is not sitting up or awake causes food to enter the lungs resulting in infection
When all other nutrition interventions have been tried and failed…
• The goals of palliative wound care are comfort for the individual and limiting the impact of the wound on quality of life, without the overt intentwithout the overt intent of healing
• Implement palliative care in accordance with the individual's wishes, and with consideration to overall health status
Older Age
• 70% of PU occur ≥ 70• Critically ill at higher
risk for PUs• End-stage dementia is
a terminal illness• PU risk increases as
feeding problems increase /ESD

8/24/2015
18
Palliative Care
1. Strive to maintain adequate nutrition & hydration compatible with the individual’s condition & wishes( SOE=C SOR=SOE=C, SOR= Definitely to it)
2. Offer nutritional supplements when ulcer healing is the goal. (SOE=C; SOR= Definitely do it)
Nutrition/Hydration Strategies
• Offer six small meals per day
• Liberalize (modify) diet restrictions
• Avoid highly seasoned foods unless requested
• Educate family/individual on food safety issues
Nutrition/Hydration Strategies
• Offer nutritional supplements or fortified foods when appropriate and if tolerated
• Commercial supplements, milkshakes, instant breakfastbreakfast
• Ice cream/ Cream soups, puddings,yogurt, hot cereal or mashedpotatoes with whole milk
Tube Feeding to Relieve Hunger and Thirst
• “Where true hunger and thirst exist, quality of life may be enhanced
• Most actively dying patients do NOT experience hunger or hithirst
• Dry mouth is a problem, but is NOT improved by tube feeding (or IV hydration).”
Hallenbeck J, Weissman D. Fast Fact and Concept #10: Tube Feed or Not Tube Feed?
MNT Goals: Ethical Issues
Promote quality of life.Treatment goals:• Client-centered • Respect individual’s
unique values and
Baird Schwartz D, Posthauer ME, O’Sullivan Maillet J. Practice Paper of the Academy of Nutrition and Dietetics: Ethical and Legal Issuesin Feeding and Hydration.http:www.eatright.orgHealthProfessionals/content.aspx?id6889. Accessed July2, 2013.
personal decisions• Shared decision making in
compliance with law
Individual’s desire is primaryguide for treatment
Steps to Successful Nutrition Care
1• Screen and Assess Nutrition Status• Individualize interventions and develop POC
• Provide diet based on estimated needs consider fortified
22• Provide diet based on estimated needs, consider fortified
foods• Offer supplements between meals if intake is inadequate
3
• Consider ONS fortified with arginine, vitamin or minerals if needs not met with high calorie/protein supplement
• Consider EN/PN based on resident's wishes, when needs cannot be met orally

8/24/2015
19
We cannot simply give a patient with PU or at risk of developing PU a new and healthy skin! 2015 White Paper
The Role of Nutrition for Pressure Ulcer Management: National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific Pressure Injury Alliance White Paper• Mary Ellen Posthauer, RDN, LD, CD, FAND
President, MEP Healthcare Dietary Services, Inc. llEvansville, IN
• Merrilyn Banks, PhD, Director Nutrition and Dietetics, Royal Brisbane & Women’s Hospital Herston, Queensland, Australia
• Becky Dorner, RDN, LD, FAND, President, Becky Dorner & Associates, Inc., and Nutrition Consulting Services, Inc., Naples, FL
• Jos M.G.A. Schols, MD, PhD, Professor of Old Age Medicine, Department of Family Medicine and Department of Health Services Research Maastricht University, Maastricht, The Netherlands
Advances in Skin and Wound Care –The Journal for Prevention and Healing
New 2014 NPUAP-EPUAP and Pan Pacific Injury Alliance Guidelines
• Quick Reference Guide: summary of the recommendations and excerpts of the supporting evidence for pressure ulcer prevention and treatment. Intended as a quick reference.
• Clinical Practice Guideline:comprehensive version of the guideline, a detailed analysis and discussion of available research, critical evaluations and description of the methodology used to develop guideline.
• www.npuap.org to order copies
References • Banks, M., J. Bauer, N. Graves, et al. (2010). "Malnutrition and pressure ulcer
risk in adults in Australian health care facilities." Nutrition in Clinical Practice 26(9):896-901. Evi
• Evidence -Based Recommendations for optimal dietary protein intake in older people: A Position Paper from the PORT-AGE study group JAMDA 2013; 14(8):542-559.
• 2014 National Pressure Ulcer Advisory Panel, European Pressure Ulcer d i l d ifi j lli i dAdvisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and
Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler(Ed.). Cambridge Media: Osborne Park, Western Australia.
• Position of the American Dietetic Association: Individualized Nutrition Approaches for Older Adults in Health Care Communities. J Am Diet Assoc. 2010;110: 1549-1553.
• Morley J et. al. Nutritional recommendations for the management of sarcopenia J Am Med Dir 2010;11:391-396.
• Fry, D.E., M. Pine, B.L. Jones, et al. (2010). "Patient characteristics and the occurrence of never events." Archives of Surgery 145(2):148-51.
• White J, et.al. Consensus Statement of the Academy of Nutrition and Dietetics/American Society of Parenteral and Enteral Nutrition: characteristics recommended for the iIdentification and documentation of Adult Malnutrition(Undernutrion) J Acad Nutr Diet 2012:112:730-738
• Edsberg, Langemo,Baharestani, Posthauer,Goldberg. Unavoidable pressure injury state of the science consensus conference. JWOCN. 2014;July: 313-334.
• . Cereda E, Klersy C, Serioli M, Crespi A, D’Andrea F; for the OligoElementl d l l h d hSore Trial Study Group. A Nutritional Formula Enriched with Arginine, Zinc,
and Antioxidants for the Healing of Pressure Ulcers: a Randomized, Controlled Trial. Ann Intern Med 2015;162(3):167-17
• van Anholt, R., L. Sobotka, E. Meijer, et al. (2010). "Specific nutritional support accelerates pressure ulcer healing and reduces wound care intensity in non-malnourished patients." Nutrition 26(9):867-72. .
• . Maillet,OSJ, SchwartzDB,Posthauer ME. Position of the Academy of Nutrition and Dietetics: ethical and legal issue of feeding and hydration. J Acad Nutr Diet. 2013;113:828-833
Questions

8/24/2015
1
Practice Competencies:pYour Pathway to Quality
Indiana DHCC
1083 Ashfield WayG b P l i
Gretchen E. RobinsonMS RDN LD LDN FAND FADA
Greensburg, Pennsylvania 15601
Email: [email protected]: 419-230-5124
Disclosure
Certification as a Registered Dietitian Nutritionist (RDN) or Registered Dietitian (RD), and a Nutrition and Dietetics Technician, Registered (NDTR) or Dietetic Technician, Registered (DTR), is a voluntary process. Certification by CDR indicates that a person has met the specific requirements of the certification process, but is not a warranty or guarantee of competency, accuracy, or any particular treatment result. CDR does not assume any duty to any individual or entity receiving professional services from CDR credentialed nutrition and dietetics practitioners. CDR shall not be liable for any loss, damage, injury, claim or otherwise, whether an action in contract or tort, and shall further not be liable for any lost profits, or direct, indirect, special, punitive, or consequential damages of any kind (including without limitation attorneys’ fees and expenses) arising from the provision of services by any CDR credentialed nutrition and dietetics practitioner.
Session Objectives
• Describe practice competencies with regard to the upcoming revision of the Professional Development Portfolio (PDP) recertification process.
• Explain the relationship of practice competencies and performance indicators to CDR’s current PDP Goals and Learning Need Codes (LNCs).
• Identify changes to the PDP process as they will affect the practitioner’s Portfolio.
• Describe the timeline for this conversion process. • Illustrate how the newly developed Goal Wizard tool will
enhance the PDP process
Enhanced Professional Development Portfolio
Shift from Goals and Learning Need Codes to
Competencies and Performance Indicators
Insert competency document front cover
The Big PictureLegislation /
External Regulatory Bodies
Regulations Scope of Practice
6
Continuing Practice Competencies
Standards of Practice/
Guidelines
Job Descriptions/
ReviewRecertification
Toolkit of Resources

8/24/2015
2
Timeline
Mandatory 75 CPEUs for Recertification
System Evaluation
Code of Ethics Specialist Certification
Professional Development Portfolio (PDP) Implementation
Practice Competencies Development
Practice Competencies Implementation
Standards of Practice
Self-Assessment Series for Dietetics Professionals
Recertification Redesign
PDP Evaluation
Practice Competencies Validation Study
1969 2015
Essential Practice Competencies
•A competency is a set of defined behaviors that provide a structured guide enabling the identification, evaluation, and development of the behaviors in an individual.
•The Essential Practice Competencies for CDR Credentialed
8
Nutrition and Dietetics Practitioners defines the knowledge, skill, judgment and attitude requirements throughout a credentialed practitioner's career, across practice settings, and within focus areas.
Functional Analysis of Competency FrameworkLevel 1: SPHERESDefine an area in which someone acts, exists or has
influence or significanceBroad, high-level wording that describes a group of
competencies and focus areasDescribe the major functions for effective performance
Level 2: COMPETENCIESDescribe the identifiable components of expected
performance (knowledge skill judgment and attitude)performance (knowledge, skill, judgment and attitude)
Level 3: PERFORMANCE INDICATORSDescribe an inter-related set of factors that define the
level of expected performance
Level 4: PRACTICE ILLUSTRATION EXAMPLESExamples to illustrate the application of competencies in day-to-day performance
Core Essential Practice Competencies Functional Essential Practice Competencies
1) Ethics and Professionalism 10) Clinical Care2) Communications 11) Business, Industry and Product Development and Marketing3) Leadership and Advocacy 12) Community and Population Health
) l h k d k ) d
Competency Framework for RDNs or RDs and NDTRs or DTRs
4) Critical Thinking and Decision Making 13) Foodservice Management5) Informatics 14) Organization Management 6) Research, Evidence-Informed Practice
and Quality Improvement 7) Safety and Risk Management8) Food, Nutrition and Dietetics and Physical Activity 9) Education and Counseling
Practice Competencies
Competency Performance Indicators
Practice Illustration Examples
10.2 Implementsthe Nutrition Care Process to ensure individual health goals are established,
10.2.1 Identifies and selects valid and reliable tools to conduct a comprehensive nutrition
•Uses comparative standards to estimate energy, fat, protein, carbohydrate, fiber, fluid, vitamin, and mineral needs and determine recommended body weight, Body Mass Index, and desired growth patterns.
•Takes into consideration blood laboratory values and test results.
monitored and achieved while adhering to the Standards of Practice in Nutrition Care for RDNs
assessment •Determines if adaptive equipment is required (e.g., grip on food utensils) and makes referrals.
•Independently screens patients for needed internal and external services and resources (e.g., nursing, occupational therapy, speech-language pathology, social work, physician, community resources).
10.2.2 Works collaboratively with interdisciplinary team to identify and implement valid and reliable nutrition assessment tools to support access to care.
Competencies and the Revised PDP
•The PDP has been revised to better incorporate the competencies. The PDP is now a 3-step recertification processrecertification process.
•Using the Goal Wizard, practitioners will create a Practice Competency Profile by selecting competencies and performance indicators to develop their learning plans.

8/24/2015
3
Revised PDP Process: Knowledge-Based to Competency-based
PDP PROCESS(KNOWLEDGE-BASED) NEW! PDP PROCESS(COMPETENCY-BASED)
ep 1
: Lea
rnin
g Pl
an U
sing
Goal
Wiza
rd
Professional Self-Reflection
Learning Needs Assessment
Learning Plan
Step 1: Professional Self-Reflection
Step 2: Learning Needs Assessment
Step 3: Learning Plan
Ste
Step 4: Activity Log
Step 5: Professional Development Evaluation
Step 2 :Activity Log
Step 3: Professional Development Evaluation
Revised PDP
1: Le
arni
ng P
lan
g Go
al W
izard
Professional Self-Reflection
Learning Needs Assessment
Step
1Us
in Learning Plan
Step 2: Activity Log
Step 3: Professional Development Evaluation
Goal Wizard: Reflect, Assess, and Plan
Select t i
Select performance indicator(s):
Identifycurrent employment status
Answer a series of questions
Confirm competency profile
competencies (will replace goals)
( )(will replace learning need codes)
Series of Questions to Reflect and Assess
Practicing (Recertifying)
Current role and responsibilities
Change in practice
Role and responsibilities
Mandatory learning
External requirements/ Practice setting
CDR - Ethics Prior role and responsibility
Non-Practicing(Recertifying)
p y
Future direction Roles and responsibilities
Mandatory learning
External requirements
CDR - Ethics
Newly Credentialed
Future direction Role and responsibilities
Mandatory learning CDR - Ethics
Goal WizardStep 1 Learning Plan: Reflect and Assess to Create Your Learning Plan

8/24/2015
4
Step 1 Learning Plan (con't): Defining Your Practice Status
Step 1 Learning Plan (con’t): Defining Your Practice
Step 1 Learning Plan (con't): Reflecting on day-to-day activities
Step 1 Learning Plan (con't): Skills, Knowledge, and Judgment
Step 1 Learning Plan (con't): Interests and Future Work
Step 1 Learning Plan (con't): Outlook for Next Five Years

8/24/2015
5
Step 1 Learning Plan (con't): Anticipated Future Role Step 1 Learning Plan (con't): Mandatory Learning
Step 1 Learning Plan (con't): Required Ethics Learning Goal
Step 1 Learning Plan (con't): Display Practice Competency Profile
Your Personalized Practice Competency Profile: Add Competencies Not Selected by Goal Wizard (if desired)
Step 1 Learning Plan (con’t): Review Competencies on Your Practice Competency Profile Before Creating Your Learning Plan

8/24/2015
6
How many competencies and performance indicators must I select?
• You must select at least one competency and one performance indicator for this competency.
• You must identify at least one competency from Ethics and Professionalism (1.0 – 1.6) and one ( )performance indicator for this competency.
Step 1 Learning Plan (con't): Final Version of Practice Competency Profile Before Creating Your Learning Plan
Create Your Learning Plan Using Your Personalized Practice Competency Profile
Creating Your Step 1 Learning Plan Using Practice CompetencyProfile (con't): Assessing Learning Needs and Adding Learning Plan Goals
Creating Step 1 Learning Plan Using Practice Competency Profile (con't): Selecting Performance Indicators
Creating Step 1 Learning Plan Using Practice Competency Profile (con't): Performance Indicators and Examples of CPE Activities Mapped to Performance Indicators

8/24/2015
7
Creating Step 1 Learning Plan Using Practice Competency Profile (con't): Review and Finish Your Plan
Step 1 Learning Plan: Final Review Before Submitting Your Completed Learning Plan
Competencies Are Posted on CDR Website The Dream Wizard
The Dream Wizard, a demo version of the Goal Wizard, is available to all practitioners. This exciting opportunity to try out the Goal Wizard prior to their recertification cycle can be experienced by visiting:experienced by visiting:
http://www.cdrnet.org/competencies .
Just click on Dream Wizard!
Will there be materials available as resources for Educators, Accredited Providers, and Practitioners?
• Yes, an Educator Toolkit will be available on the CDR website
• Yes, an Accredited Provider Toolkit will be available on the Accredited Provider Portal
• Yes, Practitioner resources will be available on the CDR b it tCDR website at http://www.cdrnet.org/competencies
When is the goal wizard going to be available?
• New registrants beginning their very first cycles will use the Goal Wizard starting June 2, 2015
• Current registrants beginning new cycles will use the Goal Wizard starting June 1, 2016
• Continue using the current PDP process until your cycle begins
f• The 5-year cycle dates for practitioners beginning the Essential Practice Competencies program are:
First Group: June 2, 2015-May 31, 2021Second Group: June 1, 2016-May 31, 2021Third Group: June 1, 2017-May 31, 2022Fourth Group: June 1, 2018-May 31, 2023Fifth Group: June 1, 2019-May 31, 2024Sixth Group: June 1, 2020-May 31, 2025

8/24/2015
8
Thank you for attending!

8/24/2015
1
Sanitation
L I S A H A R R I S O N , I S D H F P P T R A I N I N G S P E C I A L I S TB R E N DA B U R O K E R , R .N . DE P U T Y DI R E C T O R –
D I V I S I O N O F L O N G T E R M C A R E
Are you Competent in the Kitchen?
Food Safety by the Numbers
According to the Centers for Disease Control (CDC) 1 in 6 Americans (48 million)get sick 128,000 hospitalized3,000 dies from food born illness each year
Breakdown in the Numbers
The graph shows the single food commodity as the cause of 1,565 illnesses from 2003-32008Look at how much of your diet include these items!!
Objectives
What is the role of the health departmentTrained staffHow to identify the risks Proper food preparation
Health Department
The Indiana State Department of Health (ISDH) is authorized by law to ensure that foods are safe, wholesome and sanitary; regulated products are honestly and accurately represented; and, these products are in compliance with the state laws andproducts are in compliance with the state laws and regulations. (Preface 410 IAC 7-24)

8/24/2015
2
Health Department
92 countiesFountain/Warren share East Chicago and Gary have separate city HD from Lake CountyCounty93 local health departmentIndiana State Department of Health
Non-Profit
Senate Enrolled Act (SEA 190) Certain organizations, such as religious, nonpublic educational, civic, fraternal, veterans or charitable that are exempt under IRS 501(c)(3) exemptions are exempt from the definition of “Food Establishment”
Unless they operate more than 15 days in a calendar yearThe county may ask for documentation through a “letter of determination” from the IRS
Preparing for Work
Each kitchen must have proper equipment to assess the control of foodborne illness risk factorsMinimum supplies include:
Thermocouple or suitable thermometerThermocouple or suitable thermometerAlcohol swabsChemical test kits Heat-sensitive tape or maximum registering thermometerFlashlightHead covering
Definitions
Time/Temp. Controlled for Safety (TCS) – Also known as potentially hazardous foods, a food that is natural or synthetic and requires temperature control because it is in a form capable of supporting progressive growth of infectious or toxigenic microorganisms.Critical Control Point a point where failure of a standardCritical Control Point – a point where failure of a standard operation procedure could cause harm Danger Zone – a range of temperatures in which foodbornebacteria can reproduceFATTOM – a mnemonic device that is used to describe 6 favorable conditions required for the growth of foodbornepathogens
Equipment
Calibrate your equipmentEven digital thermometers need to be checked for accuracy
Taking Temperatures
Infrared thermometers should not be used for taking food temperaturestemperatures
A thermocouple or digital thermometer should be used for taking internal temperatures of food

8/24/2015
3
Identifying the Risks
The Centers for Disease Control and Prevention (CDC) identified the most frequently reported contributing factors to foodborne illness
b d t i th t di tl l t t5 broad categories that directly relate to food safety concerns within retail establishmentsThe categories are termed “Foodborne Illness Risk Factors”
Foodborne Illness Risk Factors
1. Food from Unsafe Sources
2. Inadequate Cooking
3. Improper Holding Temperatures
4. Contaminated Equipment
5. Poor Personal Hygiene
Determining the Risk
Remember you are trying to identify foodborne illness risk factors within the establishment and determine if any are out of control
Food from unsafe sourcesInadequate cookingImproper holding temperaturesContaminated equipmentPoor personal hygiene
Certified Food Handler
Certification of Food Handler Requirements Title 410 7-22
This is a separate rule for the purpose of food handler certification onlyOne certified food handler (CFH) per establishment butOne certified food handler (CFH) per establishment but doesn’t have to be there during all hours of operation The certificate must be from an accredited sourceSome establishments are exempthttps://secure.in.gov/isdh/21059.htm
Identifying the Correct CFH Certificate
*The approved certificate must contain the Conference of Food Protection (CFP) Logo and the ANSI Logo
*As a non-profit you are not required to have this certification
Employee Illness Policy
An employee illness policy should be part of your food safety protocolThis is the mechanism for employees to report symptoms or diagnosis of foodborne illness to the PIC All h PIC h lik lih d f f dbAllows the PIC to prevent the likelihood of foodborne disease transmissionNo requirement for it to be in writing so you will have to ask the PIC

8/24/2015
4
Employee Illness Policy
Policy should include big 5 pathogensH- Hepatitis AE- E. coli (shiga-toxin)N- Norovirus
Policy should include symptoms
DiarrheaVomitingJaundice
S- SalmonellaS- Shigella
Sore throat with feverLesions
Special Circumstances
Some food establishments do a little more than others
Variances (https://secure.in.gov/isdh/21066.htm)Lists all requests/approvals for variances
Time as a public health controlpUsing local produceBottling their own productValue added foodsConsumer advisory Guidance documents can be found on the state website
What Do You Prepare
Operational steps for food preparationCookingCoolingReheating
Ask enough questions pertaining to the food served in the establishment to get a general picture of the operationDo a walk-through before work begins
The Walk-Through
Start with the FOODWhat are you going to prepare?What are the proper food temperature for the foods we are ppreparing?Is anything being reheated today?Are we going to cool leftovers?What are the high risk food items?
Take Temperatures
Cooking temperatures should be verifiedChicken……….165 degrees F. for 15 secondsGround beef…155 degrees F. for 15 secondsPork 145 degrees F for 15 secondsPork…………… 145 degrees F. for 15 secondsFish……………..145 degrees F. for 15 secondsPre-cooked …..135 degrees F. for 15 seconds
These temperatures are know as Critical Limits
Danger Zone
Hot HoldingAll hot must be hot held at 135 degrees F. or above
Cold HoldingAll cold food must be cold held at 40 degrees F. or below
Refrigerator TemperaturesAny temperature that will maintain food below 41 degrees F.

8/24/2015
5
Consider This Take Temperatures
Assess hot and cold holdingStart with food that is being used at the moment
Salad bars, steam tables and warming unitswarming units
Take temperatures of foods that have been reheated
Verify that the CL have been metUnderstand why
Temperatures
How to check food temperatures
Place thermometer in the thickest portion of foodpIf a large amount of food take temperatures in various placesWait for the thermometer to stop before removing it
Display of Food
If you have foods available for consumers to handle
Provide adequate utensilsProvide adequate utensilsMonitor consumersKeep food hot/cold
Are we worried about the condensate on the glass?
Cool Down
Cooling temperatures/times need to be closely evaluated
What is the method being used for coolingIce bathIce wandIce wandOpen in the coolerAdding ice as an ingredient
What You Might See
Cool Down 2 hrs 70/4 hrs 41Food cooled from ambient air ingredients 4 hrs
It fi dItems you may find cooling
Breakfast itemsSoups, gravy’sFoods to be used for other items laterLarge pieces of meat

8/24/2015
6
Time/Immediate Service/Undercooked
Time as a public health controlTime used in lieu of time-temperature combinationsApproved plan through the health departmentdepartment
Cooking for immediate serviceCook temperature is not required
UndercookedConsumer advisory required
Unless whole intact beef-steak or pasteurized eggs
Special Processes
Certain inspections involve specialized processes that carry a considerable risk if not conducted under strict controls
VariancesHazard Analysis Critical Control Point (HACCP)Reduced Oxygen packaging (ROP)Low acid and acidified foods
Personal Hygiene
Special attention should be given to the potential for hands as a vehicle of contamination
Observe employee behaviorHandwashingHandwashing facilitiesIll employeesBare hand contact with ready to eat foods
Personal Hygiene
Food From Approved Souces
Foods that are approved come from inspected facilities
h l lWholesale or manufacturing facilities inspected by the state or FDA
Food Storage
Coolers/freezers should maintain food items at the appropriate temperature
Don’t use ambient temperatures as a way to determine functionality of the unitThermometers
Storage of food in unitsAre raw foods being stored to prevent cross-contaminationFood off the floorProtected from other sources of contamination

8/24/2015
7
Food Storage
Date marking is the mechanism by which the control of time-temperature combinations can prevent the growth of Listeria monocytogenes in TCS, ready-to-
t f d i ld teat foods in cold storageThere should be an adequate date marking system in place to control ListeriaThe date on the package of food can indicate either the date prepared or the date to discard
Food Storage
Dry storageFood should be stored up off the floor and protected from sources of contaminationToxic chemicals should not be storedToxic chemicals should not be stored with food items or single service itemsDented or damaged food items
Food-Contact Surfaces & Equipment
Assess the cleaning, sanitation and storage of food-contact surfaces, equipment and utensils
Look at all equipment involved with the production of foodproduction of foodWhat are the procedures for cleaning and sanitizing
Clean in placeManual warewashingDish machine
Cleaning and Sanitizing
Sanitation of food contact surfaces
3 bay sink or dish machineStorage for clean/dirty utensilsutensilsAir drying
Bleach or Quaternary Ammonium
Appropriate test kitsWiping clothes and sanitizer bucket
Basic Sanitation and Facilities
The overall control of foodborne illness risk factors is an important part of the routine inspection; however, overall sanitation is not to be completely
l k doverlookedPest controlEquipment maintenanceWater/sewage/plumbingRestroom facilitiesGarbage disposalUtility sink
Plumbing/Backflow Prevention
Plumbing No direct connect lines to wastewater drains at food prep areas
Air Gap2 times the diameter and at least 1 inch
Air Break2 times the pipe diameter of the pipe discharging water

8/24/2015
8
Plumbing/Backflow Prevention
Hose BibbOnly used on a faucet which has an open ended hose attachedNever can be used under constant pressure
Dual Check ValveSome may have ventsCannot be installed below grade subject to
Atmospheric Vacuum BreakerPositioned at least 6 inches higher than the highest point you are trying to protectCan’t use with a spray hose for more than 12 hours in a 24 hour period
flooding
Things We Don’t Want to See
Questions
Lisa Harrison, Training SpecialistISDH Food Protection Program
You can call me at 317 412 2106You can call me at 317-412-2106or send me an email at [email protected]
Surveying Long Term Care
F371 Dietary SanitationThe facility must-Procure food from sources approved or considered satisfactory by Federal, State or local authorities;
andStore, prepare, distribute and serve food under sanitary conditions
The Initial Brief Tour of the Kitchen
Looking for:Potentially hazardous foods thawing at room temperatureFood Items in the refrigerator unlabeled or undatedPotentially hazardous foods like uncooked meat not stored separately from other foodsAppropriate hand washing facilities with soap and water convenient for staff to use
OBSERVING DURING FOOD PREP
Staff hand washing practicesCracked egg useFood that is not prepared, cooked, or stored under appropriate temperaturesStaff hygiene practices (touching hair, face, nose, then food)

8/24/2015
9
MONITORING STAFF
Who monitors staff for illness?Policy for illness or infected skin lesionsin dietary staff
HANDWASHING
Hands must be washed for twenty (20) seconds.
Surveyors will count or watch their watch to ensure 20 seconds is not really 5 seconds. Singing Happy Birthday is not the answer since everyone sings at a different rate.
Antimicrobial Hand Gel cannot be used in place of proper handwashing techniques in food service setting.
Hair Restraints/Jewelry/Nails
Hair and beard restraints as appropriate must be worn by everyone entering the food preparation and service area. This includes:Repair menDelivery personsNursing and Administrative Staff
SNACKS AND SUPPLEMENTS
Temperature Control and Freedom from Contamination is important for these food items, also.
What time were the snacks delivered to floor?When were they served to the resident?yWhat was the temperature when eaten or drank?
EQUIPMENT AND UTENSIL SANITATION
Dishwashing TemperaturesManual WashingStorage to Prevent Contamination
How do staff monitor temperatures and chemical concentration
DINNERWARE SANITATION & STORAGE
STORED TO PREVENT CONTAMINATIONCLEAN AND SOILED WORK AREAS SEPARATE

8/24/2015
10
REFUSE AND PEST CONTROL
DUMPSTER COVEREDNO EVIDENCE OF INSECTS OR RODENTS
QUESTIONS
Brenda Buroker, RNDeputy Director - Division of Long Term CareIndiana State Department of Health
(317) [email protected]
Thanks for having us today.

8/3/2015
1
Managing Dysphagia in the Elderly
TERESA MCCLAIN, M.A., CCC-SLP
AUGUST, 2015
Learner Objectives & Disclosure1. Learn warning signs & symptoms of dysphagia in older adults.
2. Learn modified food & liquid diets and their appropriate use in dysphagia management.
3. Learn strategies for managing dysphagia in adults with dementia.
Disclosure:
•Employed as an Assistant Professor in Speech Pathology & Audiology at Ball State University
•Received an honorarium for this presentation
What is Dysphagia?Dysphagia: Impaired swallowing. Difficulty moving food from the mouth to the stomach
Dysphagia can occur in any the phase of swallowing
50-60% of residents in long-term care facilities have dysphagia
33% of patients in acute rehab settings have dysphagia
http://www.nlm.nih.gov/medlineplus/ency/anatomyvideos/000126.htm
Medical & Psychosocial Consequences of Dysphagia
•Risk for aspiration pneumonia
•Dehydration
•Malnutrition
•Respiratory system strains
•Weight loss
•Social Isolation
•Caregiver burden
•Quality of life impact
Age Related Swallowing Changes
•Poor dentition or dentures results in increased food chewing time
•Reduced opening to the esophagus, which can lead to solid food or pills getting “stuck”
•Reduced smell and taste, resulting in decreased appetite or overuse of flavor enhancers
•Delayed onset of airway protection
•Slower swallow
https://vimeo.com/60944584
Signs & Symptoms of Dysphagia
•Coughing during or right after eating or drinking
•Wet or gurgly sounding voice during or after eating or drinking
•Extra effort or time needed to chew or swallow
•Food or liquid leaking from the mouth or getting stuck in the mouth
•Recurring pneumonia or chest congestion after eating
•Weight loss or dehydration from not being able to eat enough
•http://www.asha.org/public/speech/swallowing/Swallowing-Disorders-in-Adults/

8/3/2015
2
Texture Modified DietsPureed - blended food that can be consumed without chewing
Examples: applesauce, whipped potatoes
Mechanical Soft - Cooked food or soft textured food that is not “crisp”
Examples: cooked vegetables, scrambled eggs, meatloaf, pasta, most fruits
National Dysphagia DietNDD Level 1: Dysphagia-Pureed
•homogenous, very cohesive, pudding-like, requiring very little chewing ability
NDD Level 2: Dysphagia-Mechanical Altered
•cohesive, moist, semisolid foods, requiring some chewing
NDD Level 3: Dysphagia-Advanced
•soft foods that require more chewing ability
•National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: The American Dietetic Association; 2002.
Texture Modified Diets –Points to Consider
•Limited guidelines for determining correct diet level
•Patient acceptance of diet may be greater if aesthetics of food are enhanced (how does it look? Smell? Taste?)
•At least 1 study has found 91% of patients on a modified diet in 2 long-term care facilities were on overly restrictive diets (they could safely handle less modified diet levels)
•Patients should be monitored & reevaluated at regular intervals to determine if diet changes are needed
Texture Modified Diets –What to Avoid
•Raw vegetables, including lettuce
•Dry, crumbly foods (rice, corn, crackers)
•Cooked asparagus, broccoli, Brussels sprouts, cabbage, and other fibrous or rubbery vegetables
•Chewy candies, sticky food items, popcorn, and corn chips
•Mixed Consistency foods (vegetable soup, cereal with milk, Jell-O with fruit)
•Peanut butter, unless used as part of a recipe that is easy to swallow.
Liquid Consistencies
Thin - Liquids made up largely of water, having no additional density
Examples: water, coffee, tea, lemonade, ice cream
Nectar Thick - Liquid having a syrup like consistency; easily sipped through straw; Falls off a tipped spoon slowly
Examples: tomato juice, buttermilk, cream-based
Liquid Consistencies
Honey Thick - Liquid that is substantially thickened to resemble honey thickness; too thick to sip through a straw, but can drink through a cup
Less pourable, will drizzle from a cup or spoon
Pudding Thick - Liquids thickened to the density of a creamy shake; generally needs spoon for intake
Examples: creamy milkshake, blended yogurt

8/3/2015
3
Thickeners Starch vs. Gum Based
STARCH
•Modified cornstarch
•Thickening hot drinks is more challenging
•Clear liquids will appear cloudy & beverages will have a slightly grainy texture
•Stir 1-3 minutes to reach proper consistency, depending on brand; Can continue to thicken over time
GUM
•Xanthan or cellulose gums
•Works well in both hot & cold beverages
•Clear beverages remain clear & smooth, with a slightly slippery texture
•Require vigorous mixing for 5 minutes to reach consistency, but then will remain at that consistency
Pre-thickened Liquids•Ready to drink
•Can be chilled
•Available in 8 oz. and 64 oz. containers
•Available in nectar & honey consistencies
•Variety of juices, milk & water products
•Will not thicken over time or with temperature change
•Some studies have found products may be thicker than nectar-thick liquid guidelines**Kyzima, J B; Strowd, L., Pillsbury, D., Rubin, B. (2008) Managing Dysphagia: Lack of Standardization on Food Viscosities May Compromise Patient Care. Clinical Nutrition INSIGHT: August 2008 -Volume 34 - Issue 8 - p 1–5.
Thickened Liquids –Points to Consider
•Will patients accept thickened liquids?
•Hydration – will they drink less fluids if they are thick?
•Frazier Water Protocol – will access to water between meals (along with stringent oral care) increase fluid intake?
•In general, the research indicates that the frequency of penetration/aspiration decreases as the liquid viscosity increases
•However, the risk of post-swallow residue in the throat increases for liquids with higher viscosities
Other Food Modifications
Volume - smaller bolus for better oral control & safe transit with less residue
Temperature - cold is believed to enhance awareness of a bolus
Taste/Smell - sour taste may result in faster onset of swallow
Carbonation - carbonated liquids may result in less airway penetration than noncarbonated thin liquids
Dysphagia in Patients with Dementia
Mild Dementia
• Changes in taste & smell
• Reduced oral intake
• Weight loss
Moderate to Severe Dementia
• Oral & pharyngeal phase swallowing deficits, including reduced ability to prepare food to swallow, delayed initiation of the swallow, reduced airway protection resulting in aspiration & residue in the throat after the swallow
•Estimated prevalence of 84-93% of patients with dementia
• Behavioral deficits include refusal to eat/drink, reduced oral intake & suspected dehydration
Maximizing Oral Intake –Dining Environment
•Dining Room Size –25 or less residents to reduce distraction
•Reduce Noise – TVs, noisy carts, staff conversations, alarms
•Ambient Music - use quiet music to reduce agitation
•Table Settings – avoid plastic fruit, provide only the necessary utensils
•High Contrast Dishes – maximize patient’s visual recognition of food by high contrast between dishes & food
http://www.eatwellset.com/

8/3/2015
4
Maximizing Safe Oral Intake –Food & Meal Modifications
•Provide smaller meals more frequently; offer liquids throughout the day
•Offer more finger foods
•Include foods that are spicy, sweet & sour to maximize sensory input
•Position patient upright at 90 degrees with head in a neutral or chin tuck position to maximize airway protection
•Use hand-over-hand assistance to encourage self feeding
•Encourage patient to alternate between bites of food & sips of liquid to reduce pharyngeal residue & post swallow aspiration
•Check the patient’s mouth for residue after the meal and provide frequent oral hygiene
•Encourage staff to feed patient small bites/sips and allow extra time for patient to swallow
•Collaborate with staff & family members to address negative behaviors – is patient refusal due to discomfort or pain?
Feeding Tubes in Patients with Dementia
Feeding tubes (specifically PEG) are often used in patients with advance dementia as a means of maintaining nutritional support and reducing dysphagia related comorbid conditions
However, published evidence says:◦ Feeding tubes do not reduce risk of aspiration pneumonia◦ Feeding tubes do not prolong survival◦ Feeding tubes have no impact on overall functional status
http://graymattertherapy.com/peg-tube-prolong-survival-people-dementia/http://geriatricscareonline.org/ProductAbstract/american-geriatrics-society-feeding-tubes-in-advanced-dementia-position-statement/CL017
Comments & QuestionsResources
DEMENTIA
Alzheimer’s Association
http://www.alz.org/
Alzheimers.net
http://www.alzheimers.net/
Dementia Queen
http://thedementiaqueen.com/
DYSPHAGIAAmerican Speech-Language Hearing Association (ASHA)
http://www.asha.org/public/speech/swallowing/Swallowing-Disorders-in-Adults/
Dysphagia Café
http://www.dysphagiacafe.com/
National Foundation of Swallowing Disorders (NFSD)
http://swallowingdisorderfoundation.com/
Swallow Study Blog
http://www.swallowstudy.com/

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
Points to Ponder
Recognize the role of the RDN in documenting malnutrition using characteristics associated with severe and nonseveremalnutrition in adults.
Discuss the relationship between inflammatory stress, inflammatory biomarkers, cachexia and lab test results.
Identify assessment techniques for nutrient deficiencies and functional status to incorporate into current clinicalassessment practices.
Discuss the use of nutrition focused physical assessment as a tool used in conjunction with lab test results and dietaryintake data.
I. Nutrition Care Process & NFPA
Ask Yourself…
1. What is my level of expertise in doing NFPA?
2. Do I think of myself as an ‘expert’ in identifying malnutrition?
3. Do I automatically look for malnutrition &/or V/M deficiencies?
4. How often do other medical team members identify malnutrition &/or V/M deficiencies as a problem?
5. How do I use my NFPA findings in collaborating with other medical team members?
2013 Practice Paper: Academy of Nutrition & Dietetics Critical Thinking Skills in Nutrition Assessment and Diagnosis
What is NFPA?
1. Does it replace a physical exam conducted by a physician or nurse?
2. Does it replace the things I’m doing now for nutrition assessment?
3. Does it mean more paperwork?
4. Is this really THAT important?
NFPA & Nutrition Assessment Domains
NFPA & IDNT
IDNT* Definition: Findings from an evaluation of bodysystems, muscle and subcutaneous fat wasting, oralhealth, suck, swallow/breathe ability, appetite andaffect.
*IDNT-International Dietetics & Nutrition Terminology
II. Steps in Clinical Reasoning
1. Identify abnormal findings or symptoms
2. Localize the findings anatomically
2.1. Skin, nails, numbness in feet
3. Interpret findings in terms of probable process
4. Make hypothesis about the nature of the patient’s problem
4.1. Looking for nutrition diagnosis
5. Test the hypothesis and establish a working diagnosis
5.1. Request more lab tests, swallowing evaluation or consultation with other team members
6. Develop a plan agreeable with the patient
6.1. Plan or intervention for each problem identified

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
III. Systems Approach to Assessment
Overall appearance Vital signs SkinHEENT-head, eyes, ears, nose & throat Cardio-pulmonary system Extremities, muscles & bonesDigestive system Nerves & cognitionA. Learn the Lingo…Signs vs Symptoms
1. Sign - an objective or measured finding as perceived by an examiner. Example: lab test data, color of urine2. Symptom - a subjective indication of a disease or a change in condition as perceived by the patient. Example: chest pain,
headache3. Some symptoms may be objectively confirmed.
B. Cardinal Techniques of Exam
1. Inspection- General observation that progresses to a more focused observation using the senses of sight, smell, and hearing;most frequently used technique
2. Palpation- Tactile examination to feel pulsations and vibrations; assessment of body structures, including texture, size,temperature, tenderness, and mobility
3. Percussion- Assessment of sounds to determine body organ borders, shape, and position; not always used in a NFPA4. Auscultation- Use of the naked ear or a stethoscope to listen to body sounds (e.g., heart and lung sounds, bowel sounds,
blood vessels)
C. First Impressions to Note During Interview
1. What is the apparent state of health?
2. What is the level of consciousness?
3. Does the patient show signs of physical distress?
4. Does the patient show signs of emotional distress?
5. How is the person dressed?
6. If the patient is wearing shoes, have the toes been cut out?
7. Do you see any obvious signs of nutrient deficiencies?
8. Do you notice any unexpected odors such as the fruity aroma of diabetes or alcohol?
9. Are there any involuntary movements or signs of paralysis?
D. Physical Characteristics to Note During Interview
Overall appearance Body habitus AffectBody positioning- muscle contractures Amputations Tanner stageCushingoid appearance Ability to communicate
H. Vital Signs
Blood pressure (mm Hg)/ Pulse Pressure Heart rate ( beats/min) Oxygen saturation (percentage)Respiratory rate (breathes/min) Temperature (degrees)
Blood Pressure/ HR Oxygen Saturation Temperature BP w dehydration < 90% poor wound healing RMR BP w falls SOB Cytokines trigger sickness syndrome
BP w Na sensitivity Fatigue w meals Elderly less likely to have fever
HR w SOB, vertigo, fallsSOB Fatigue w meals

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
IV. NFPA & Hydration
A. Hands, face, lips, tongue, eyes, arms & legsS/S Moderate Dehydration Severe DehydrationLevel of Consciousness Lethargic Unresponsive
Capillary Refill 4 Seconds > 4 Seconds, Cool Limbs
Mucous Membranes Dry Parched or CrackedHeart Rate Increased RapidBlood Pressure Normal, but Orthostasis Decreased
Skin turgor Slow Tenting
Eyes Sunken Very Sunken
Urine Output Oliguria Oliguria or Anuria
Urine Color ( may be medication or food related) Medium yellow Golden
Capillary refill time- palpate nails to assess circulation, gently squeeze nail between thumb & index finger. Appears white whensqueezed, the color should return to normal pink color within < 2-3 seconds. Time to return to original color is capillary refill time.Lab Test Hypernatremia-related Hyponatremia -related
Osmolality
Na, (S)
Albumin, (S)*
BUN
BUN: Creat ratio**
Urine specific gravity
B. Assessment of tongue1. Dry, furrowed tongue consistent with dehydration2. Healthy moist tongue consistent with normal hydration3. Slick tongue consistent with malnutrition4. Sore red tongue consistent with vitamin deficiencies
V. Case Study RubyRuby, 82 yr old F, resident of ABC Nursing Home, was sent to City Hospital for evaluation following a fall in the bathroom.Admitting Dx: fractured right hip. Admission Data: Ht 155 cm, Wt 46 kg.BP 110/63, HR 112, RR 22, Temp 101 F, SpO2 without supplemental oxygen 87%
Health History: Dx osteoporosis, kyphosis, sarcopenia, insidious wt loss of 3-4 kg in last 12 mos, type 2 DM, CHF, HTN, orthostatichypotension, & depression. Ambulatory w walker & 1 person assists w transfers prior to fall & fractured hip.Social History: widow,1 son, son has stage IV pancreatic cancer & is under Hospice Care.Mini Nutrition Assessment (MNA): 8Braden Score: 10
Notes from RDN at nursing home: Food intake is 25-50% of meal served and about 4-6 oz water or other beverage per meal, oftenskips evening meal, intake has diminished in recent weeks since her son moved to a Hospice Care facility.
Question: Based on the data provided, what factors have contributed to her recent fall?

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
Data D-1 Admission HospitalHt in/Wt # 155 cm /46 kg (61 in/101 lbs)BP /HR 110/63;112Na mEq/L 147Cl mEq/L 105Glu mg/dL/A1c 160/NABUN/cr mg/dL 35/1.1ALP/AST/ALT U NAH/H/MCV gm/dL, %, fL 13/37%/99Alb/PAB g/dL, mg/dL 4.0/NA
Review of Ruby’s medical data:
low BP & history of orthostatic hypotension may manifest as _________or _______which could have contributed to the fall
dehydration as evidenced by low___, labs, coupled with _____________intake may manifest as dizziness which could havecontributed to the fall
tachycardia as evidenced by HR may manifest as _______& _____________which could have contributed to the fall
diagnosis of sarcopenia is associated with loss of muscle _______& loss of muscle _______which could have contributed tothe fall
Question: Ruby has a MNA score = 8 & Braden score=10 How might the healthcare team interpret the scores as part of the initialhealth assessment?
MNA = 8 indicates that she is at ______________& BMI =19 is __________weight range.
MNA = 8 coupled with ____________________________________________________________________________________________________puts her at increased risk for development of pressure ulcers
Braden score of 10 suggest ________risk for development of pressure ulcers; it is _______________with MNA score anddiet history
Question: Based on data provided, identify nutrition risk indicators to assess in NFPA
Physical signs of:
Dehydration Malnutrition Anemia Skin breakdown Oral exam for chewing & swallowing abilities
V. Malnutrition

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
A. New Guidelines to Define Malnutrition: Identification of > 2 of the following characteristics
1. Insufficient energy intake
2. Weight loss (unplanned & significant)
3. Loss of muscle mass
4. Loss of subcutaneous fat
5. Fluid accumulation that may mask weight loss
6. Diminished functional status i.e. hand grip strength
Academy/ASPEN: Characteristics of Adult Malnutrition, http://malnutrition.andjrnl.org/Content/articles/1-Consensus_Statement.pdf
ASPEN: Defining Pediatric Malnutrition, http://pen.sagepub.com/content/37/4/460.full
B. Albumin Nutritional Marker or Inflammatory Marker???
A. Kwashiorkor Sx: B. Marasmus Sx:1. Edema 1. Severe loss LBM2. rates of infection 2. Skeletal appearance3. Fatty liver 3. Apathetic4. Sparse subcutaneous fat 4. Listless5. Low albumin 5. Normal albumin6. Diet: Adequate Kcal, or no Pro 6. Diet: Kcal & Pro
Minnesota Starvation Study, 1944; Kalm L, Semba R. J. Nutr. 2005;135:1347-1352
Parameter Baseline 6 mo semi-starvation diet
BMI 21.7 16.4
Body composition: LBM 33.9% 29.2%
Fat 9.8% 3.1%
Serum Albumin 4.3 g/dL 3.9 g/dL
Inflammatory Biomarkers
Inflammatory Biomarker Suggest InflammationAlbumin
Pre-albumin
Ferritin levels may be related to inflammation & NOT reflect Fe stores
C-Reactive Protein > 1.0 mg/dL; > 10 mg/L
Fibrinogen > 400 mg ( malnutrition)
Plasminogen Activator Inhibitor 1 elevated
D-dimer > 600 ng/mL; > 600 mcg/L
Erythrocyte Sedimentation Rate elevated

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
Emerging Inflammatory Biomarkers
Interleukin-1 beta
Interleukin-6
Tumor necrosis factor-alpha
Interferon-gamma
C. NFPA for fat loss - use palpation and observation
1. Orbital loss in face2. Fat loss in torso , arms and legs
D. NFPA for Muscles of mastication- Ask individual to ‘clench teeth”, & move jaw side to side several times and palpate massetermuscle.
1. Temporal Loss2. Masseter Loss
E. NFPA for Muscle Loss in Hands- observation, palpation, handshake or grip
1. Interosseous Loss2. Thenar Loss
F. NFPA for Muscle Loss in Upper Body- observation, palpation, handshake or grip, flex arm muscles
1. Clavicle Loss2. Triceps Loss3. Biceps Loss4. Deltoid Loss (flat shoulders, clothing off shoulder, sleeves too long)5. Trapezius
G. NFPA for Muscle Loss in Lower Body- observation, palpation, flex muscles, sit to stand, Up and Go test
1. Quadriceps- note dimpling of muscle2. Gastrocnemius- feels stringy and weak3. Thigh gap seen in patients with disordered eating
VI. NFPA for Anemias & Nutrient Deficiencies
A. Physical Signs
1. Color of skin
2. Pale lips & conjunctive
3. Fatigued, malaise
4. Mouth sores & Bleeding gums
5. Abnormal nails
Physical s/s Fe deficiency ACD B12 deficiency Folate deficiencyEnergy level/ overall Tired, dizziness Tired, dizziness Tired, lightheaded Tired, lightheaded
Pallor, skin & nails Pale, Koilonychia Pale Pale, yellow tinged PaleConjunctive Pale Pale Pale PaleExtremities Cold/stiff Cold/stiff/
fibromyalgiaTingling, numb, senseof touch, stiff
Cold
Sleeping Leg cramps w/ insomnia Leg cramps w/insomnia
Leg cramps w/ insomnia Leg cramps w/insomnia

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
Physical s/s Fe deficiency ACD B12 deficiency Folate deficiency
Tongue/Mouth
Sores around or in mouth Sore, smooth, beefy red Smooth, soretongue
Heart rate RapidSOB w/ exercise
RapidSOB w/ exercise
RapidSOB w/ exercise
RapidSOB w/ exercise
GI Diarrhea alternating w/constipation
Diarrheaalternating w/constipation
Mental status Difficulty concentrating Difficultyconcentrating
Confused, dementia,hallucinations, paranoia
Difficultyconcentrating
Other Pica IrritableAnorexia
IrritableAnorexia
IrritableAnorexia
B. NFPA for Nail Abnormalities
Koilonychia (Spoon Nails) Onychorrhexis (Central Ridge Lines)
Malnutrition- IAAs methionine, cysteine Malnutrition
Fe deficiency Fe deficiency
Diabetes mellitus Folic acid deficiencyMedications
Transverse Linear Depressions(Beau’s Lines)
Clubbing
Malnutrition Cystic Fibrosis
Severe infections, Surgery, MI Cancer (lung, Hodgkin’s lymphoma)Zn Deficiency Crohn’s & Ulcerative Colitis
Uncontrolled Diabetes Cirrhosis of Liver
Hypotension, Hypocalcemia Graves’ Disease
White Nails Brown-gray NailsAnemia Vitamin B12 deficiencyEdema DM
Renal failure or DM CVDCirrhosis
C. NFPA for Vitamin Deficiencies: Scurvy1. Purpura (large areas of bleeding)2. Corkscrew hairs3. Petechiae (small pinpoint hemorrhages in the skin)4. Very poor wound healing5. Fragile bleeding gums

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
D. NFPA for Vitamin Deficiencies: Vitamin A
Etiology Deficiency SymptomsPrimary deficiency Changes in hair
inadequate intake Alopecia of eyebrows fat malabsorption (gastric bypass surgery) Dry, rough skin, follicular hyperkeratosis liver disorders Dry eyes, impaired night vision, keratomalacia, Bitots Spots
Secondary deficiency Cracked lips
decreased bioavailability of provitamin A carotenoids Severe headache (pseudotumor) interference with vitamin A absorption, storage or
transport Generalized weakness
Keratomalacia- hazy, softened corneaBitot Spots- shiny gray spots on conjunctiveSkin: Vitamin A Deficiency: Follicular Hyperkeratosis- resemble ‘gooseflesh’. Bumps don’t disappear when skin is rubbed. Lesionscommonly appear on lateral surface of arm and extensor surface of thigh.
VII. CASE STUDY
Al is 78 yr old M bachelor living in assisted living; retired firefighter. Hospital admission data: 70 in. 210 lbs.
Health Hx: HTN, Type 2 DM, GERD. Meds: Lasix 40 mg 2X d, metformin 500 mg 2Xd. OTC antacids for GERD. Smoker for 35 yrs, quit 5yrs ago. He fell at church & couldn’t get up. He hit his head on corner of table. 911 is called & he is sent to ED. He has laceration tohead requiring stitches, bruises & broken right femur. Plan of care: Femur fix scheduled, short-term rehabilitation and return to AL
Hospitalized 5 days, d/c to Rehab. Today is Day 7 at Rehab unit. Participates in PT most days. Complains of being too tired, lightheaded & feet hurt. Prefers to stay in bed most of day instead of getting up as recommended by PT.
Nursing reports poor food intake- about 50% at most meals. Complains that food was better at AL unit. Friends bring in burgers,fries, pizza, but he eats < 50%
Nutrition Rx: Consistent Carbohydrate , Heart Healthy Diet. Protein Shake 1 X d. Diet provides 2500 Kcal. Est energy needs 2400 kcal.
Meds: Lasix 80 mg 2X day, metformin 500 mg 3Xd, Ativan 1 mg PRN.
D-1 Hosp D-5 d/c to Rehab D-10 ( in rehab 5 d) D-12 (in rehab 7 d)
Ht in/Wt # 70 /210 70 /199 70/195 70/191
BP /HR 160/107;110 100/67; 105 112/88;83 99/65Na mEq/L 140 138 NA 149Cl mEq/L 100 91 NA 98Glu mg/dL 130 139 NA 142BUN/cr mg/dL 25/1.1 30 /1.3 NA 32/1.3ALP/AST/ALT U NA 30 /26/31 NA 30/25/30H/H/MCVGm/dL, %, fL
NA 11/32%/105 NA 10.5/31%/108
Alb/PABg/dL, mg/dL
NA 3.2/NA NA 2.9/8
B12/MMA/FA
pg/mL,ng/mL,ng/mLNA NA NA 310/82/13

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
I. Overall Appearance & body language II. Vital Signs, Cardio-pulmonary
overwt, alert M, complaining about food, anxious about future Temp hovering bet 99-100, BP is lower than baselinewith hx HTN
III. Hydration IV. Skin & Nails
Mucous membranes are dry and lips are cracked Dry, scaly. Surgical sites healing. Nails flat, most arechewed. Stage II Pr Ulcer 1.5 cm X 2.2 cm on sacrumper nursing
V. Oral Cavity VI. Digestive System
Tongue is dry but not furrowed. Color is deep red. Patient shows signs ofdiscomfort when tongue is touched with depressor. Angular stomatitis atcorners of mouth
VII. Extremities- bones and muscles VIII. HEENT & cognition
No evident kyphosis or scoliosis No evidence of muscle or fat wasting in face, canclench teeth, no chewing issues
IX. Characteristics of Malnutrition Context of Malnutrition /Severity
Loss of upper body muscle mass in clavicle, deltoid and triceps; quadsdimpled, gastrocnemius feels stringy
Handgrip WNL
Question: Review NFPA & labs for indicators of deficiencies.
In the interview, what are you going to look for?
Positioning Body habitus Cushingoid appearance? Ability to communicate Affect Body language
What ‘Red Flags” do you see?
Write PES Statements for problems.
1. Abnormal nutrition-related labs r/t suboptimal intake of _____AEB dietary ______________________________which areconsistent with ___________deficiency
2. Abnormal nutrition-related labs r/t suboptimal intake of ________AEB _______________________________which areconsistent with _____________
3. Impaired nutrient utilization of vitamin ______r/t ___________& OTC antacids AEB dietary ____________________
_____________________________________________________which are consistent with __________deficiency
4. Abnormal NF Physical Findings r/t _______________________________AEB _____________________________
________________________________________which are consistent with ______________________________

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
VIII. Using NFPA to Assess Functional Status
Advanced activities of daily living (AADLs)
Intermediate activities of daily living (IADLs)
Basic activities of daily living (ADLs)
AADL IADL ADL Participating in a community activity Driving or using public transportation Shopping beyond basic grocery needs Preparing multi-step recipes/multi-course meals Evaluating & coordinating home or car maintenance
& repair Evaluating & coordinating computer upgrades, anti-
virus maintenance & repair
Safely navigating home setting Picking up the mail/paper Doing light housekeeping Simple cooking Making phone calls, text messaging or
email Keeping track of bills, writing checks,
paying bills online
Bathing Dressing Using the toilet Basic mobility- bed to chair
& chair to toilet Eating without assistance
A. Stations of Decline in Older Adults
McCullough, D (2008) Your Mother, My Mother: Embracing Slow Medicine. NY: Harper Press
Stability Compromise Crisis Recovery Decline Prelude to dying Death
1. Stability Characteristicsa. Elder successfully manages all aspects of daily living.b. Uncomfortable shift from the vigor and resilience of middle age into new areas limitation.c. Functional capacities are beginning to wane due to neglect or aging.d. Recognition is often dulled by too much television and too few challenges for problem solvingAction Plana. Improve nutrient density of the dietb. Be alert to sales pitches for anti-aging products, i.e. high potency tropical juices, juice extracts, vegetable extracts,
specially formulated vitamins and minerals, herbal supplements, amino acid or enzyme therapyc. Be alert to products are advertised as ‘natural’ alternatives to prescription medicines.NFPAa. Fitness/strengthb. Nutrient deficiency or excessc. Proper use of supplements
2. Compromise Characteristicsa. Time of increased vulnerability and changing circumstances.b. Recognize new limitations, often in frightening circumstances.c. May discount the dangers, deny the ‘event’ occurred or try to cover up the ‘evidence’ to keep family and friends from
knowing the truth.Action Plana. Families and friends are vital to elders to ‘fill in the gaps.’b. Fine-tuning therapeutic and consistency modified diets.c. Evaluate for weakened jaw muscles, loss of teeth, dysfunction of smell and taste, and reduced salivation. Dysphagia
may be due to the side effect of medications.

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
NFPA
a. strength & stamina
b. Oral assessment for chewing abilities
c. Unplanned anthropometric changes
d. S/S nutrient deficiencies or potential toxicities.
e. Proper use of supplements & OTC meds
f. Cognitive decline ( B12)
g. risk for falls (vit D)
h. Skin breakdown
3. Crisis Characteristics
a. Acute illness or mismanaged chronic condition tips the delicate balance of well-being.
Action Plan
a. Elder is moved to an intensive health care facility
NFPA:
a. Acute illness: dehydration, dysphagia, meds mismanagementb. S/S nutrient deficiencies, malnutritionc. S/S chronic diseases requiring MNTd. Risk for pressure ulcers
4. Recovery Characteristics: physical & emotional
a. Medical crisis has subsided
b. Elders and their families may have unrealistic expectations for rapid recovery
c. Elder is weakened by inactivity. Nutrient stores are likely depleted
Action Plan
a. Successful recovery requires strength, stamina and determination to regain what has been lost. Rehabilitation is a rigorousand lengthy process (McCullough, 2008).
b. Meet nutrient needs
c. Customize food services to meet the unique needs of residents.
d. Collaborate with the swallowing therapist to ensure that foods and beverages are of the appropriate consistency.
e. The ultimate goal of rehabilitation is to return the elder to the pre-crisis functional capacity
NFPA:
a. strength & stamina
b. Unplanned anthropometric changes
c. S/S nutrient deficiencies, dehydration, dysphagia, malnutrition
d. MNT to fine tune chronic diseases management
e. S/S impaired cognitive function & emotional stability
5. Decline Characteristics
a. Frailty, disability, patterns of diminishment.
b. Unplanned weight loss, increased infections and skin breakdown.Action Plan
a. Liberalization of therapeutic diets, D/C prescription meds or changes in meds may improve appetite.

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
b. Protein fortified foods and beverages may serve as meal replacements while physical strength is regained.
c. Feeding assistance, consistency modified diets
NFPA:
a. strength & staminab. Unplanned anthropometric changesc. S/S nutrient deficiencies, dehydration, dysphagiad. S/S significant cognitive & emotional decline
6. Prelude to Death Characteristics
a. Death is not imminent, but the elders’ condition is deteriorating.b. Food and fluid intake usually declines and weight loss is common.c. Interventions that worked before are no longer accepted or effective.
Action Plan
a. Comfort foodsb. Palliative care
NFPA:
a. strength & staminab. Unplanned anthropometric changesc. S/S nutrient deficiencies, dehydration, dysphagiad. S/S significant cognitive & emotional decline
IX. Putting the Pieces Together: Write an Action Plan to incorporate NFPA into your practice.
1. Review Critical Thinking Skills in Nutrition Assessment and Diagnosis. Determine where you are on the continuum and where youNEED to be.
2. Write an Action Plan to incorporate NFPA & characteristics of malnutrition into your Practice.
3. Meet with your supervisor to discuss using NFPA & the characteristics of malnutrition.
4. Complete any inservice ed. requirements of your employer before doing hands on assessments ( i.e. standard & universalprecautions).
5. Ask for additional reference books & training at work to assess for fluid accumulation & changes in body composition.
6. Practice on family, friends and then patients.
7. Document your professional continuing education and clinical practicums including competency assessment.
8. Be alert to changes from The Academy & ASPEN. The ‘characteristics of malnutrition’ are a work in progress!
START NOW!

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
References1. Aasheim ET, Bjorkman S, Sovik TT, et al. Vitamin status after bariatric surgery: a randomized study of gastric bypass and duodenal switch.
Am J Clin Nutr. Jul 2009;90(1):15-22.2. Aasheim ET. Night blindness after duodenal switch. Surg Obes Relat Dis. 2008;4(5):685-63. Aasheim ET. Vitamin status after bariatric surgery: a randomized study of gastric bypass & duodenal switch. Am J Clin Nutr 2009:1;15 -
22.4. Aasheim ET. Wernicke encephalopathy after bariatric surgery.. Ann Surg. 2005;248(5):714–205. Aasheim, Erlend T. (2008) Peripheral Neuropathy and Severe Malnutrition following Duodenal Switch. Obesity Surgery 2008
Dec;18(12):1640-3. Epub 2008 May 8.6. ADA. Nutrition Care Manual. Characteristics of Malnutrition. Chicago, IL: ADA, 2011.7. ADA. International dietetics & nutrition terminology reference manual. Chicago, IL: ADA, 2011.8. ADA Practice Applications. Nutrition care process and model part I: the 2008 update. JADA. 2008:108:1113–1117.9. American Medical Directors Association (2001). Dehydration and fluid maintenance. Columbia, MD: ADMA.10. Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with
vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol2001;119:1417-36.
11. Aills L. Bariatric nutrition guidelines for the surgical weight loss patient. Surg Obes Relat Dis. 2008. Suppl;4(45).12. Angstadt JD, Bodziner RA. Peripheral polyneuropathy from thiamine deficiency following laparoscopic Roux-en-Y gastric bypass. Obes
Surg. Jun-Jul 2005;15(6):890-2.13. Arts, EO. Gastric Sleeve: Losing Weight as Fast as Micronutrients? OBES SURG, DOI 10.1007/s11695-010-0316-7, Nov 2010.14. Bauer, J, (2008) Mini Nutritional Assessment- its history, today’s practice & future perspectives. Nutr Clin Prac. 23:388-396.15. Bickley,L. Bates guide to physical examination, 10th ed. Philadelphia, PA: Lippincott, 2009.16. Blackburn,GL Bistrian,B Nutritional and metabolic assessment of the hospitalized patient. JPEN 1977,1:11-22.17. Bohannon, R (2010) Grip strength impairments among older adults receiving physical therapy in a home care setting. Perceptual and
Motor Skills: 111(3) 761-764.18. CMS: MDS 3.0 for Nursing Home. http://www.cms.gov/NursingHomeQualityInits/30_NHQIMDS30TechnicalInformation.asp#Top
OfPage.htm. Accessed November 17, 2011.19. Cooper, B (2002) Validity of SGA as a nutritional marker in end stage renal disease. AJKD 40(1) 126-132.20. Covinsky, KE (2002) Malnutrition and bad outcomes J Gen Intern Med 17(12) 956-7.21. Covinsky, KE, Martin, GE, (1999). The relationship between clinical assessment of nutritional status and adverse outcomes in older
hospitalized medical patients. JAGS 47(5) 532-8.22. Cuthbert,S. On the reliability and validity of manual muscle testing: a literature review. Chirorp Osteopat 2007 15:423. Doweiko JP. Role of albumin in human physiology and pathophysiology. JPEN 1991;15:207–211.24. Doweiko JP, Nompleggi DJ. The role of albumin in human physiology and pathophysiology, Part III: Albumin and disease states. JPEN J
Parenter Enteral Nutr 1991;15:476 –483.25. Faes, MC, Spigt, MG, Rikkert, MG (2007) Dehydration in geriatrics. Geriatrics & Aging 10(9):590-59626. Ferguson M et al. (1999) Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition 15,
(6): 458-464.27. Friedman,A. Reassessment of Albumin as a Nutritional Marker in Kidney Disease. J Am Soc Nephrol 21: 223–230, 201028. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. NEJM 1999;340(6):448 –454.29. Gardner,M. Practical implementation of an exercise-based falls prevention program. J Age & Ageing 2001: 30: 77-8330. Gloria L, Cravo M, Camilo ME, Resende M, Cardoso JN, Oliveira AG, Leitao CN, Mira FC. Nutritional deficiencies in chronic alcoholics:
Relation to dietary intake and alcohol consumption. Am J Gastroenterol 1997;92:485-9.31. Gollobin C. Bariatric beriberi. Am J Med 2004;117:804-5.32. Grandjean AC, Campbell SM. Hydration: Fluids for life. A monograph by the North American Branch of the International Life Science
Institute. Washington DC: ILSA North America; 2004.33. Guralnik , JM, Ferrucci , L. Lower-Extremity Function in Persons over the Age of 70 Years as a Predictor of Subsequent Disability. N Engl J
Med 1995; 332:556-562.34. Guralnik JM, A short physical performance battery assessing lower extremity function: association with self-reported disability and
prediction of mortality and nursing home admission. J Gerontol 1994;49:M85-M9435. Ha L, Hauge T, Individual, nutritional support prevents undernutrition, increases muscle strength and improves QoL among elderly at
nutritional risk hospitalized for acute stroke. Clin Nutr. 2010.29(5). 567-573.36. Hagan, JC. Acute and chronic diseases. In Mulner, RM, ed. Encyclopedia of Health Services Research. vol 1. Thousand Oaks, CA:Sage;
2009:25.37. Hoye RC, Bennett SH, Geelhoed GW, et al. Fluid volume & albumin kinetics occurring with major surgery. JAMA 1972;222(10):1255–1261.38. Humphreys J, de la MP, Hirsch S, Barrera G, Gattas V, Bunout D. Muscle strength as a predictor of loss of functional status in hospitalized
patients. Nutrition. 2002;18:616–62039. Institute of Medicine. Dietary Reference Intakes for water, potassium, Na, chloride & sulfate. Washington, DC: NAS, 2005.

Nutrition Focused Physical Assessment: Making Clinical Connections
Mary D. Litchford PhD, RDN, LDN
© CASE Software & Books, [email protected]
40. Jensen GL, Hsiao PY.(2010) Obesity in older adults: Relationship to functional limitation. Current Opinion Clinical Nutrition and MetabolicCare, 13: 46-51.
41. Jensen, G, Bistrian, B (2009) Malnutrition syndromes: a conundrum vs continuum JPEN 33(6) 710-716.42. Jensen, G, (2010) Adult starvation & disease-related malnutrition: a proposal for etiology-based diagnosis in the clinical practice setting
from the International Consensus Guideline Committee. JPEN 34(2) 156-159.43. Jequier E, Constant F. Water as an essential nutrient: The physiological basis of hydration. Eur J Clin Nutr. 2010;64:115-123.44. Johnson A. Low levels of plasma proteins: Malnutrition or inflammation? Clin Chem Lab Med 1999;37(2):91–96.45. Johnson , AM, Merlini,G. Clinical indications for plasma protein assays: transthyretin (prealbumin) in inflammation and malnutrition. Clin
Chem Lab Med 2007;45(3):419-42646. Kaburagi, T, Hirasawa (2011) Nutritional status is strongly correlated with grip strength and depression in community-living elderly
Japanese. Public Health Nutrition. DOI: 10.1017/S1368980011000346.47. Kaiser MJ, Bauer JM, Rämsch C, et al. (2010) Frequency of Malnutrition in Older Adults: A Multinational Perspective Using the Mini
Nutritional Assessment. J Am Geriatr Soc 58 (9) 1734-8.48. Kaiser R. Functionality & mortality in obese nursing home residents: example of risk factor paradox? JAMDA 2010;11(6):428-435.49. Kaiser, MJ, Bauer, C (2009)Validation of the Mini Nutritional Assessment short form (MNA®-SF): A Practical tool for identification of
nutritional status. J Nutrition, Health & Aging 13 (9).50. Kaur, N, Koley, S (2010) An Association of Nutritional Status and Hand Grip Strength in Female Laborers of North India. Anthropologist
12(4)237-243.51. Keys, A chronic undernutrition and starvation with notes on protein deficiency. JAMA. 1948: 138: 500-511.52. Klein, S, Kinney, J Nutrition support in clinical practice: review of published data and recommendations for future research directions.
NIH, ASPEN, ASCN. JPEN 1977: 21: 133-156.53. Litchford, MD (2012) Nutrition Focused Physical Assessment: Making Clinical Connections. Greensboro, NC: CASE Software & Books.54. Litchford, MD.(2011) Laboratory Assessment of Nutritional Status: Bridging Theory & Practice. Greensboro, NC: CASE Software & Books.55. Lovett RW, Martin EG. Certain aspects of infantile paralysis with a description of a method of muscle testing. JAMA. 1916, Mar 4, 729–33.56. Norman, K . Hand grip strength: Outcome predictor and marker of nutritional status. Clin Nutr 2011:30:135-142.57. Norman K, Three month intervention with protein & energy rich supplements improves muscle function & quality of life in malnourished
patients with non-neoplastic gastrointestinal disease. Clin Nutr. 2008;27:48–5658. Norman K, Schutz T, Kemps M, Josef LH, Lochs H, Pirlich M. The Subjective Global Assessment reliably identifies malnutrition-related
muscle dysfunction. Clin Nutr. 2005;24:143–15059. Norman, K, (2011) Hand grip strength: outcome predictor and marker of nutritional status. Clinical Nutrition 30(2) 135-142.60. Nursal, T, Noyan, T (2005) Simple two-part tool for screening of malnutrition. Nutrition 21(6) 659-665.61. Pieterse, S, Manandhar, M (2002) The association between62. nutritional status and handgrip strength in older Rwandan refugees EJCN 56(10) 933-939.63. Puskarich-May CL, Sullivan DH, Nelson CL, et al. The change in serum protein concentration in response to the stress of total joint surgery:
a comparison of older versus younger patients. J Am Geriatr Soc 1996;44:555–558.64. Rossiter-Fornoff, JE, Wolf, SL et al A cross-sectional validation study of the FICSIT common data base static balance measures. J Gerontol
Med Sci 1995, 50 A: M291-765. Rothschild MA, Oratz M, Schreiber SS. Serum albumin. Hepatology 1988;8:385– 401.66. Stankorb SM, Rigassio-Radler D, Khan H, Touger-Decker R. Nutrition-focused physical examination practices of registered dietitians. Top
Clin Nutr. 2010;25:335–344.67. Stieber,M Scope of practice & legal issues nutrition-focused physical examination. Support Line April, 2011, 2-6.68. Soeters, P, (2009) Advances in understanding & assessing malnutrition. Current Opinions Clin Nutr Metab Care 12: 487-494.69. Sullivan, DH, et al . Association between inflammation-associated cytokines, serum albumins, and mortality ion the elderly. JAMDA 2007
September 458-463.70. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA
2003;289:2560–71.71. Wang, A, Sea, M (2005)Evaluation of handgrip strength as a nutritional marker and prognostic indicator in peritoneal dialysis patients.
AJCN 81(1) 79-86.