Embed Size (px)
Citation preview
Presentor : Norlida Binti SuhaimiModerator : Dr Khairuddin Bin Ismail
Dr Nik Azman Bin Nik Adib
Dr Benedict SimInfectious disease physicianHosp Sg Buloh
Dr. Wan Noraini ; Surveillance Section, Disease Control Division
Dr. Shahanizan bt Mohd Zin; Medical Development Division
Dr Anilawati ; ID Physician, Kota Bahru
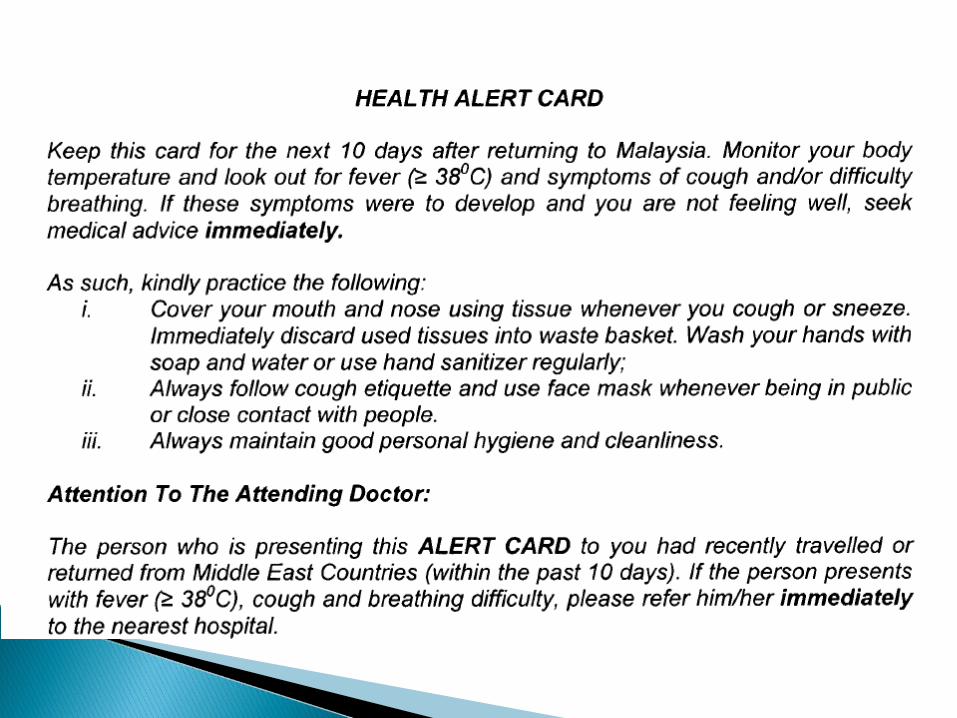
What will MERS-CoV look like? Who has MERS-CoV? Who do test? How do test? When to admit? Where to admit? What infection control needed? How to treat ?


Coronaviruses :- large family of viruses that can cause a range of illnesses in humans
- from the common cold to severe acute respiratory syndrome (SARS).
- cause disease in a wide variety of animal species.
In late 2012, a novel coronavirus that had not previously been seen in humans was identified for the first time in a resident of the Middle East - known as the Middle East Respiratory Syndrome Coronavirus (MERS-CoV)
Thus far, all patients infected with MERS-CoV have had a direct or indirect link to the Middle East
however, local non-sustained human-to-human transmission has occurred in other countries, in people who had recently travelled to the Middle East.
The MERS-CoV virus is thought to be an animal virus that has sporadically resulted in human infections, with subsequent limited transmission between humans.
MERS – CoV : genetic similarity to viruses previously described in bats.
However, even if an animal reservoir is identified, it is critical to identify the types of exposures that result in infection and the mode of transmission.
It is unlikely that transmission occurs directly from animals to humans
route of transmission may be complex requiring intermediary hosts, or through contaminated food or drink.
Human-to-human transmission has occurred in health care settings, among close family contacts, and in the work place.
Sustained transmission in the community beyond these clusters has not been observed and would represent a major change in the epidemiology of MERS-CoV.
Male to female ratio 2.6 : 1.0 Median age 56 years (range: 2–94 years) All aged >24 years, except 2 children(2 & 14 yrs)
Deaths:
Case fatality rate = 31/55 = 56%
4~14d after onset, 2~10d after hospitalization
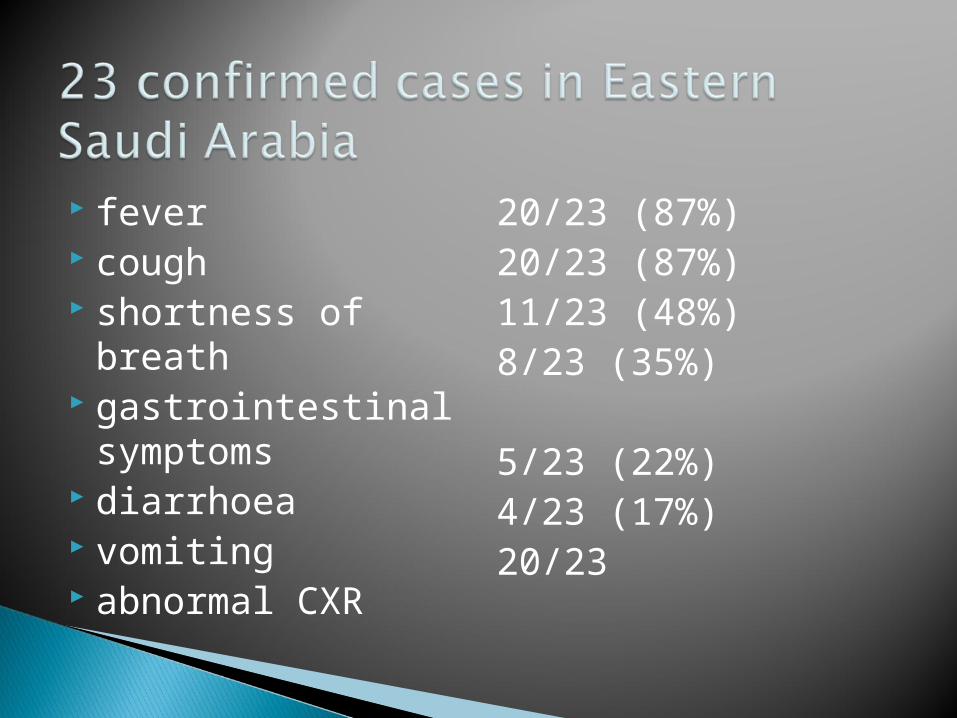
fever cough shortness of breath gastrointestinal
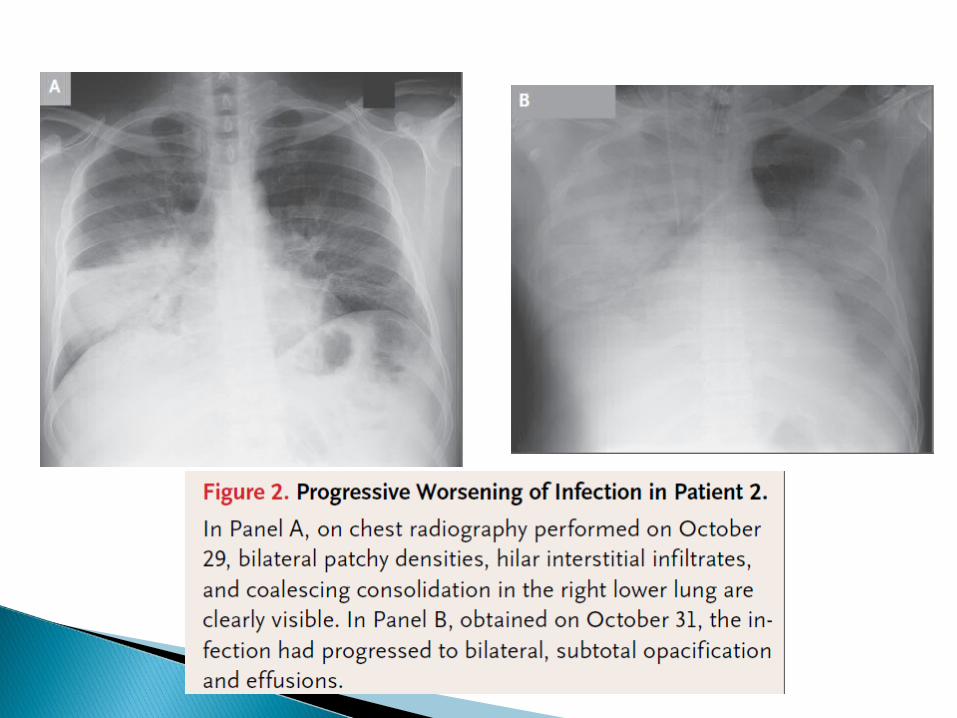
symptoms diarrhoea vomiting abnormal CXR
20/23 (87%) 20/23 (87%) 11/23 (48%)8/23 (35%)
5/23 (22%) 4/23 (17%) 20/23
Most - pneumonia. Some - GI symptoms, diarrhoea
1 immuno-compromised patient - fever and diarrhoea; pneumonia only on CXR.
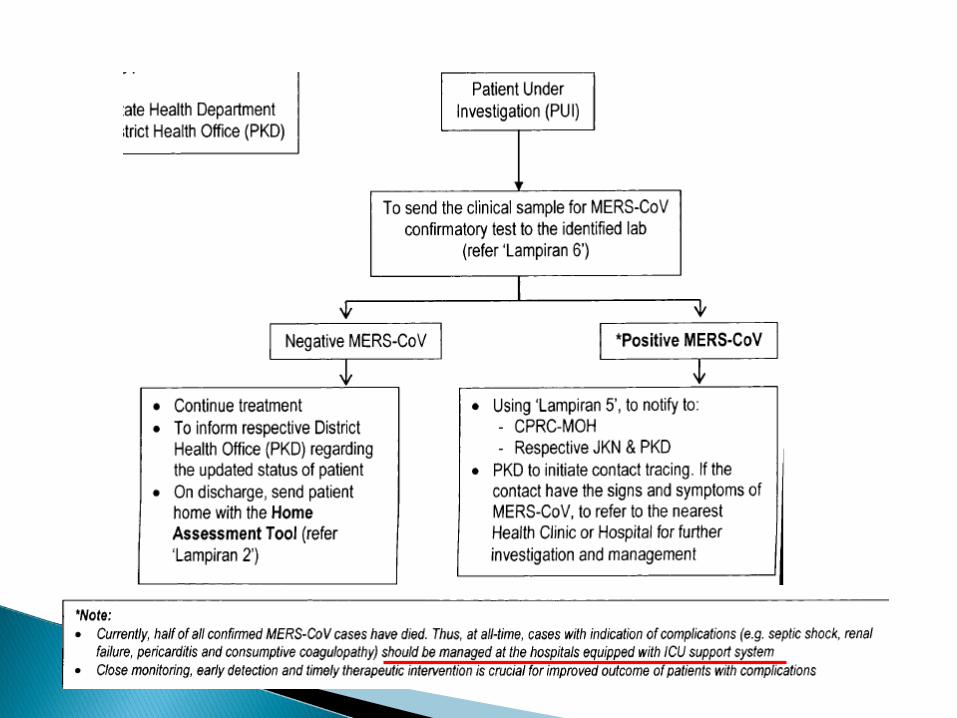
Half have died. Complications
◦ respiratory failure ◦ ARDS with multi-organ failure◦ renal failure requiring dialysis◦ consumptive coagulopathy ◦ pericarditis.
Co-infections - influenza, herpes simplex, and pneumococcus
The date of onset was defined:
among febrile patients as the first day of feverthat persisted for more than 48 hours
afebrile patients as the first day of new cough or shortness of breath.
As of June 12…- 15 patients (65%) died
- 6 patients (26%) had recovered
- 2 patients (9%) remained hospitalized.
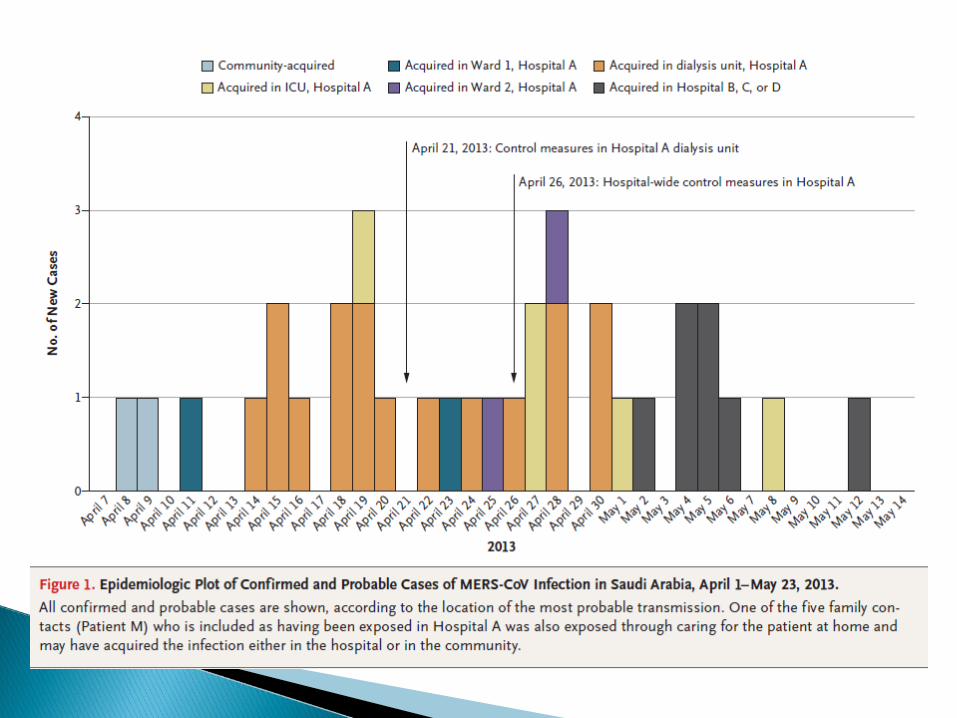
A total of 21 of the 23 cases were acquired by person-to-person transmission in hemodialysis units, intensive care units, or in-patient units in three different health care facilities.
Among 217 household contacts and more than 200 health care worker contacts whom identified
- MERS-CoV infection developed in 5 family members (3 with laboratory- confirmed cases)
- and in 2 health care workers (both with laboratory-confirmed cases).
Where exposure is known or strongly suspected - generally < 1/52
In at least one case, 9 to 12 days.
In a minority of cases, may exceed one week but is less than 2 weeks
Limited person-to-person transmission
Settings: Hospital, Household
Most family members and HCWs closely exposed did not develop disease
No evidence at present of sustained person-to-person transmission
Coinfection with influenza & parainfluenza - ? Roles in transmissibility and/or the severity of the illness.
Transmissibility pattern ? SARS
Reported case of milder nCoV illness – spectrum of clinical disease maybe wider
Undetermined
Presumably universal
Presumable vulnerability in elder people with
pre-existing medical condition
Lower risk for children and women?
Undetermined
Droplet and direct contact probably
Large droplet transmission is suspected as the most likely route.B Guery et al. Clinical features and viral diagnosis of two cases of infection with Middle East Respiratory Syndrome coronavirus: a report of nosocomial transmission. Lancet (2013).
Confirmed Case: lab confirm Probable Case:SARI* with clinical, radiological, or HPE evidence of pulm parenchymal ds [e.g. pneumonia or ARDS]; ANDno possibility of lab confirmation ANDclose contact** with lab-confirmed case.
*Include hx of fever or measured fever**Close contact – anyone who - Provided care for the pt, including HCW or family member; - Stayed at the same place (e.g., lived with, visited) while pt ill
1) Confirmed case A person with laboratory confirmation of
MERS-CoV infection. ◦ molecular diagnostics including either +ve PCR on
at least two specific genomic targets or a single +ve target with sequencing on a second.
2) Probable case
1. Febrile ARI with clinical, radiological, or HPE evidence (C/R/HPE) of pulm parenchymal ds (PPD) e.g. pneumonia or ARDS AND
Testing for MERS-CoV - unavailable / negative on a single inadequate specimen ANDDirect epid-link with a confirmed MERS-CoV case
1. Febrile ARI with C/R/HPE of PPD ANDInconclusive MERS-CoV (+ve screening test w/out confirmation)ANDA resident of or traveler to Middle East 14/7 before
onset of illness.
Febrile ARI of any severity
ANDInconclusive MERS-CoV (+ve screening test w/out confirmation)
ANDDirect epid-link with a confirmed MERS-CoV case.
Inadequate sp • NP swab without lower resp sp, • sp with improper handling, • judged to be poor quality by lab, • taken too late.
◦ A direct epid link may include:• Close physical contact• Working together in close proximity or sharing the
same classroom environment• Traveling together in any kind of conveyance • Living in the same household• 14/7 period before or after the onset of illness in the
case under consideration.
Inconclusive tests :
• A positive screening test without further confirmation eg positive on a single PCR target• A serological assay positive.
1. Should undergo additional virologic and serologic testing.
2. Strongly advised that lower resp sp such as sputum, ET aspirate, or BAL be used.
3. If no S&S of LRTI and lower track sp not available or clinically indicated, both NP and OP swab sp should be collected.
4. If NP swab is negative in a pt strongly suspected to have MERS-CoV infection, retest using a lower resp sp or a repeat NP sp with additional OP sp and paired acute and convalescent sera.
SARI, (include history of fever and cough) and indications of PPD (e.g., pneumonia or ARDS), based on clinical or radiological evidence of consolidation, (possibility of atypical presentations in immunocompromised) AND
Travel to the Middle East 10/7 before AND Not explained by other aetiology
ARI of any severity, ◦ 10 days before onset of illness, ◦ close physical contact* with a confirmed or
probable case of MERS-CoV infection
HCW ◦ working where pt with SARI cared for, (esp ICU)◦ without regard to history of travel (WRTHOT)◦ Not explained by other aetiology
1. Detect early, sustained human-to-human transmission.2. Determine the geographic risk area for infection with the virus.
Clinical and epidemiological Ix to:1. Determine clinical characteristics - incubation
period, spectrum of disease, and natural history.
2. Determine epidemiological characteristics - exposures that result in infection, risk factors, secondary attack rates, and MOT

SARI + PPD + either◦ In a cluster (within 14/7)◦ HCW exposed to pt with severe LRTI◦ Traveled to middle east - 14/7◦ unexpected clinical course unexplained by
current aetiology
ARI of any severity ◦ close contact with confirmed/probable MERS-
CoV within 14/7 Middle East, any ventilated pt
cluster (>1 persons in a specific setting -classroom, workplace, household, extended family, hospital, other residential institution, military barracks or recreational camp) that occurs within 14-days, WRTHOT unless another aetiology identified (UAAI).
HCW working with severe ARI patients
(particularly ICU) WRTHOT UAAI
travel to the Middle East within 14 days before onset of illness, UAAI.
unusual or unexpected clinical course, especially sudden deterioration despite appropriate treatment, WRTHOT , even if another aetiology has been identified, if it does not fully explain the presentation or clinical course of the patient.
Stronger recommendations for lower respiratory specimens, rather than NP swabs, to be used to diagnose MERS-CoV infection.
A longer period of observation for contacts of cases.
NP swabs are not as sensitive as lower respiratory specimens – BAL, tracheal aspirate, sputum
If patients do not have LRTI or specimens not possible, both NP and OP should be collected
Respiratory impairment: any of the followingTachypnoea, respiratory rate > 24/minInability to complete sentence in one breathUse of accessory muscles of respiration, supraclavicular recessionOxygen saturation < 92% on pulse oximetryDecreased effort tolerance since onset of ILIRespiratory exhaustionChest painsEvidence of clinical dehydration or clinical shockSystolic BP < 90mmHg and/or diastolic BP < 60mmHgCapillary refill time > 2 seconds, reduced skin turgor
Altered Conscious level (esp. in extremes of age)New confusion, striking agitation or seizuresOther clinical concerns:Rapidly progressive (esp. high fever > 3 days) or serious atypical illnessSevere & persistent vomiting

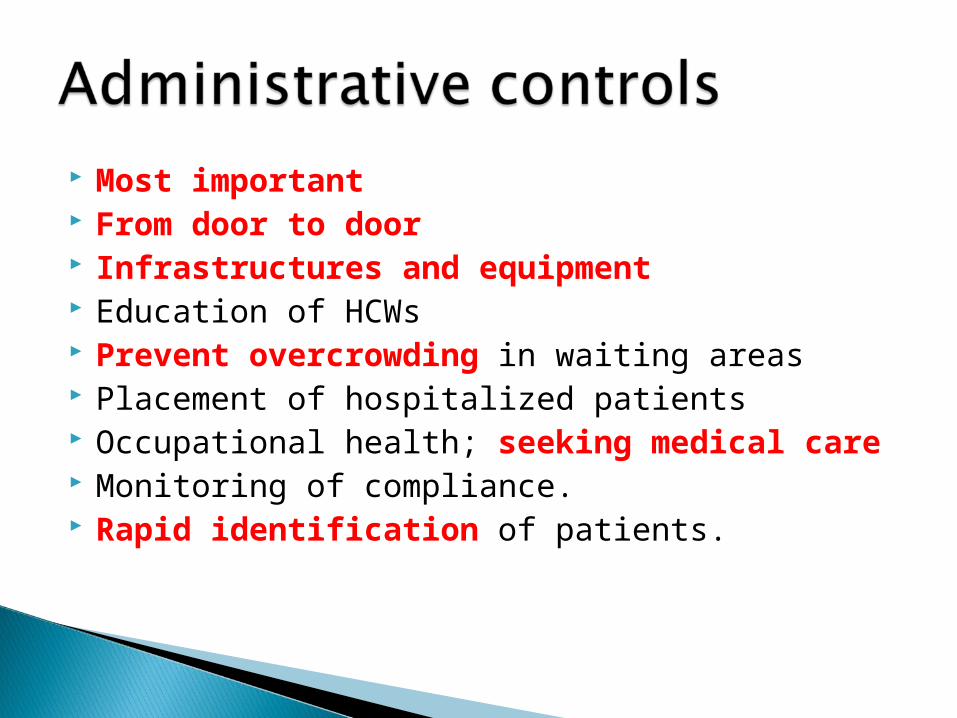
Most important From door to door Infrastructures and equipment Education of HCWs Prevent overcrowding in waiting areas Placement of hospitalized patients Occupational health; seeking medical care Monitoring of compliance. Rapid identification of patients.
Adequate ventilation Regular environmental cleaning Spatial separation of at least 1 m
Rational and consistent use of PPE and appropriate hand hygiene.
??
Standard precautions
+
Droplet precautions
Airborne for aerosol generating proceedures

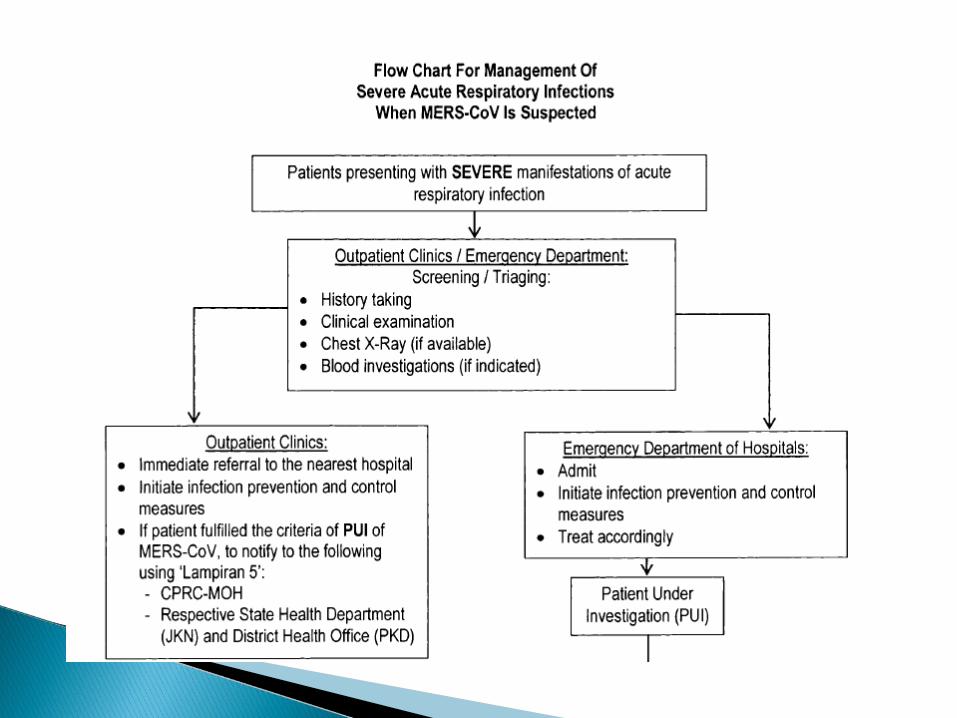
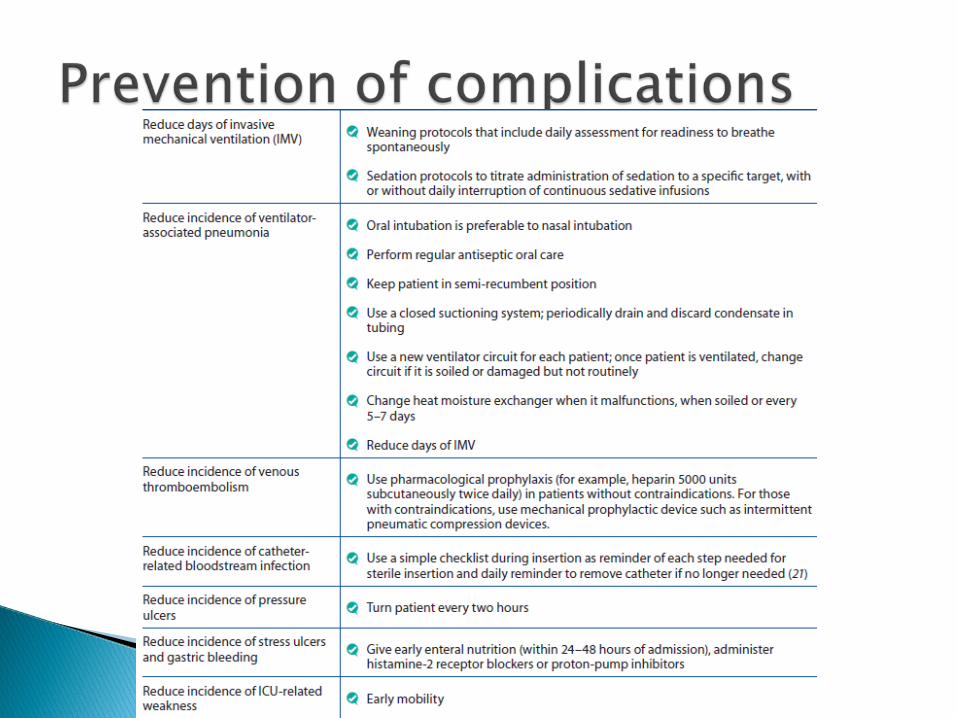
Recognize SARI Initiate infection control measures Give supplemental O2 therapy Collect respiratory and other sp for lab testing Empiric antimicrobials for suspected pathogens Conservative fluids when no shock No high-dose steroids or other adjunctive
therapies outside the context of clinical trials Watch for clinical deterioration, eg severe resp
distress/resp failure; tissue hypoperfusion/shock
Recognize severe cases, where high flow of O2 are inadequate
Mechanical ventilation - early in pt with tachypneoa or hypoxemia that persists despite high-flow O2
Consider NIV if local expertise is available, when immunosuppression is also present, or mild ARDS without impaired consciousness or CV failure
If equipment available and staff trained, proceed with ET intubation to deliver invasive mechanical ventilation
Use lung-protective ventilation strategy (LPV) for ARDS In severe ARDS, consider adjunctive therapeutics
early, especially if failing to reach LPV targets Use conservative fluid mx for non shocked ARDS pt
Recognize sepsis-induced shock - hypotension (SBP < 90 mm Hg) that persists after initial fluid challenge or signs of tissue hypoperfusion (lactate concentration > 4 mmol/L) and initiate resuscitation by protocol
Early and rapid infusion of crystalloid for septic shock
Vasopressors when shock persists despite fluid resus
Consider iv hydrocortisone (up to 200 mg/day) or prednisolone (up to 75 mg/day) in persistent shock requiring escalating doses of vasopressors
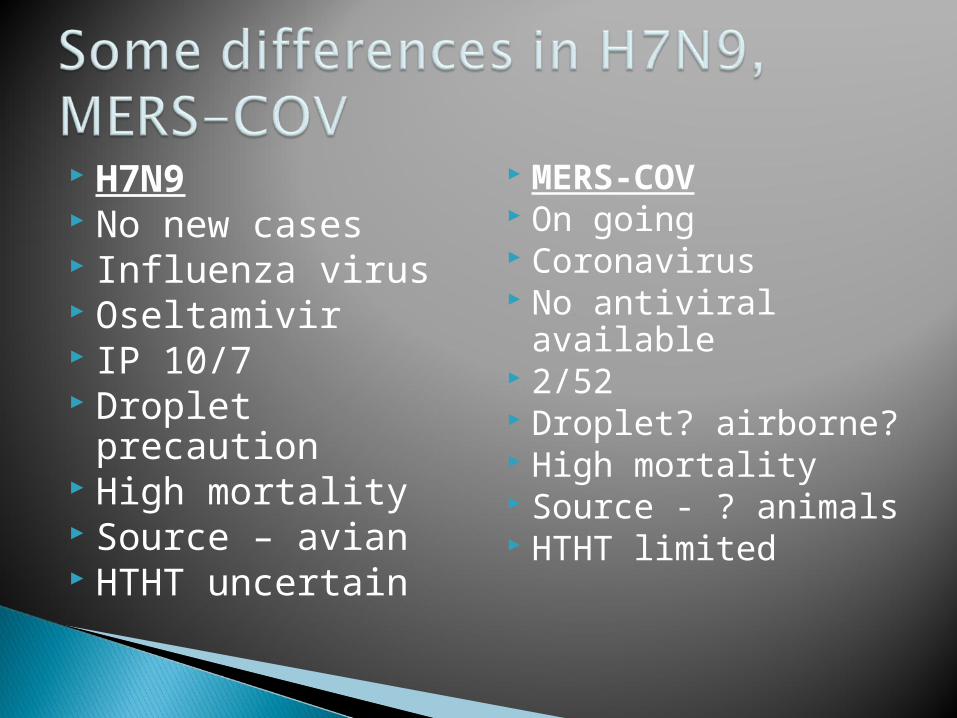
H7N9 No new cases Influenza virus Oseltamivir IP 10/7 Droplet precaution High mortality Source – avian HTHT uncertain
MERS-COV On going Coronavirus No antiviral
available 2/52 Droplet? airborne? High mortality Source - ? animals HTHT limited






























