Embed Size (px)
Citation preview
Presenter: Linda Sharpen, MLT, ART, B. Admin
Co-Authors: Corey Boimer, BSc, Kenneth Lee, BSc, Raneen Shehadeh-Mashor, MD, Allan R. Slomovic, MA, MD
The authors have no financial interest in the subject matter of this poster.
Introduction Corneal transplantation is one of the most commonly performed transplant operations in
North America1,2.
Indications for penetrating keratoplasty (PKP) have changed over the past three decades 3. The most recent data from a Canadian tertiary referral centre suggests that the leading indication for PKP is regraft, followed by pseudophakic corneal edema, Fuch’s corneal dystrophy, and keratoconus2.
Since 2006, partial thickness transplant techniques have gained increasing favour in Ontario. There is little published information examining the frequency of these lamellar keratoplasties and their impact on the availability of donor corneal tissue and the common indications for transplantation.
The purpose of this study was to determine the changes in the leading indications and preferred surgical techniques for corneal transplantation in Ontario over a nine year period. To our knowledge, this is the largest study of its kind in North America to date.
Methods Records of all corneal tissues sent for transplantation in Ontario by the Eye Bank of
Canada (Ontario Division) from July 1st, 2000 to June 30th, 2009 were reviewed. The records consist of recipient information forms completed by surgeons at the time of corneal transplant surgery.
The records were analyzed with respect to the clinical indication for corneal transplantation, surgical technique used, and the year in which surgery took place.
The clinical indications for transplantation were grouped based on the standardized diagnostic tree proposed by Lindquist et al. (1994)4. The category of regraft was given priority over all other accompanying conditions.
Of the 8186 available recipient information forms, 7725 (94.4%) were sufficiently complete to meet the inclusion criteria for this study.

ResultsTable 1 – Indications for Corneal Transplantation, by Category
Indication Category No. of surgeries (%)
Aphakic Corneal Edema 142 (1.8%)
Chemical Injuries 21 (0.3%)
Congenital Opacities / Disorders 65 (0.8%)
Corneal Degenerations 9 (0.1%)
Corneal Scarring 96 (1.2%)
Ectasias / Thinning 1065 (13.8%)
Interstitial Keratitis 110 (1.4%)
Mechanical Trauma (Non-Surgical) 257 (3.3%)
Microbial / Post-Microbial 252 (3.3%)
Non-Infectious Ulcerative Keratitis / Perforation 110 (1.4%)
Other 15 (0.2%)
Primary Corneal Endotheliopathies 1281 (16.6%)
Pseudophakic Corneal Edema 2190 (28.3%)
Regraft 1659 (21.5%)
Stromal Corneal Dystrophies 90 (1.2%)
Surgical 20 (0.3%)
Viral / Post-Viral 343 (4.4%)
Total 7725 (100%)
Table 1 summarizes the major indication categories for all corneal transplantation operations performed in Ontario between 2000-2009.
The top four indications over this period were:
1. Pseudophakic Corneal Edema (28.3%)
2. Regraft (21.5%)
3. Primary Corneal Endotheliopathies (16.6%)
4. Ectasias/Thinning (13.8%)
However, this does not capture the year-to-year fluctuation in the order of the top indications for corneal transplantation.
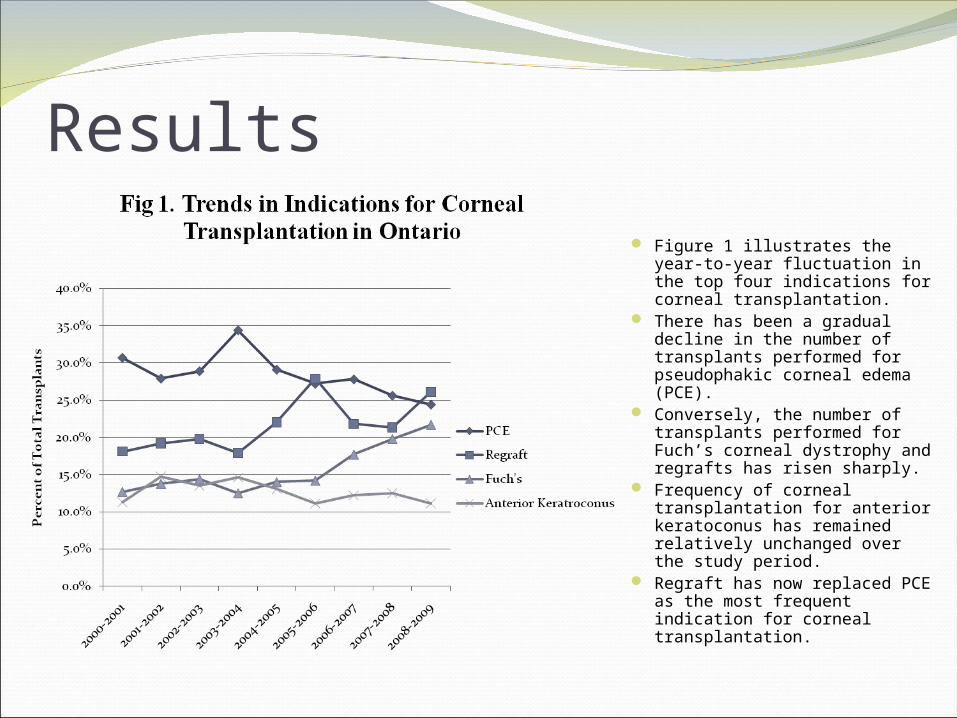
Results Figure 1 illustrates the year-to-
year fluctuation in the top four indications for corneal transplantation.
There has been a gradual decline in the number of transplants performed for pseudophakic corneal edema (PCE).
Conversely, the number of transplants performed for Fuch’s corneal dystrophy and regrafts has risen sharply.
Frequency of corneal transplantation for anterior keratoconus has remained relatively unchanged over the study period.
Regraft has now replaced PCE as the most frequent indication for corneal transplantation.
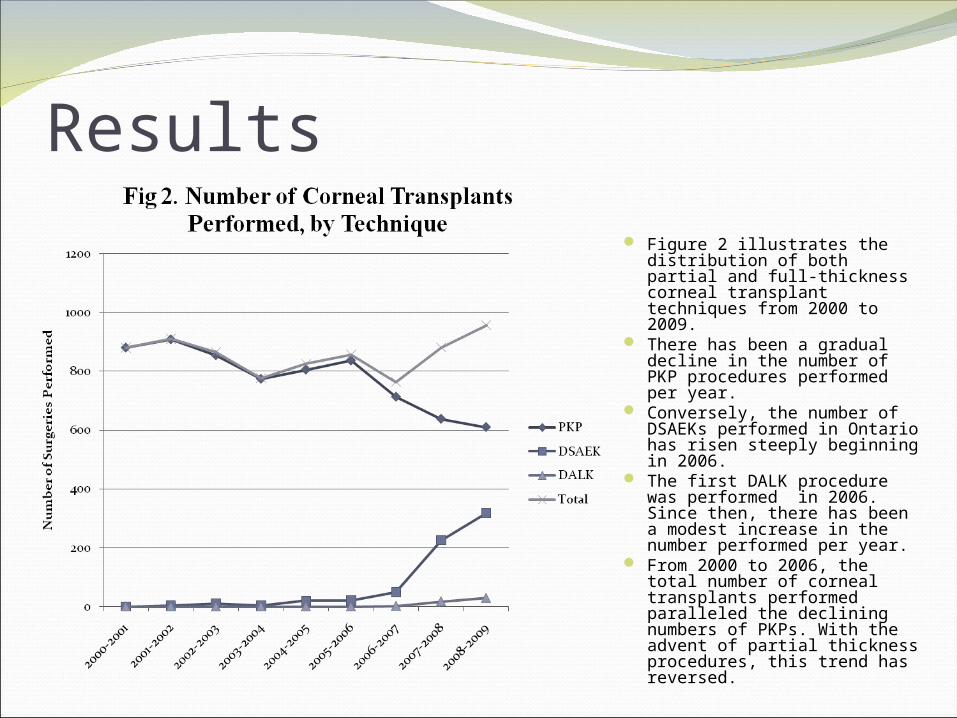
Results Figure 2 illustrates the
distribution of both partial and full-thickness corneal transplant techniques from 2000 to 2009.
There has been a gradual decline in the number of PKP procedures performed per year.
Conversely, the number of DSAEKs performed in Ontario has risen steeply beginning in 2006.
The first DALK procedure was performed in 2006. Since then, there has been a modest increase in the number performed per year.
From 2000 to 2006, the total number of corneal transplants performed paralleled the declining numbers of PKPs. With the advent of partial thickness procedures, this trend has reversed.
Results
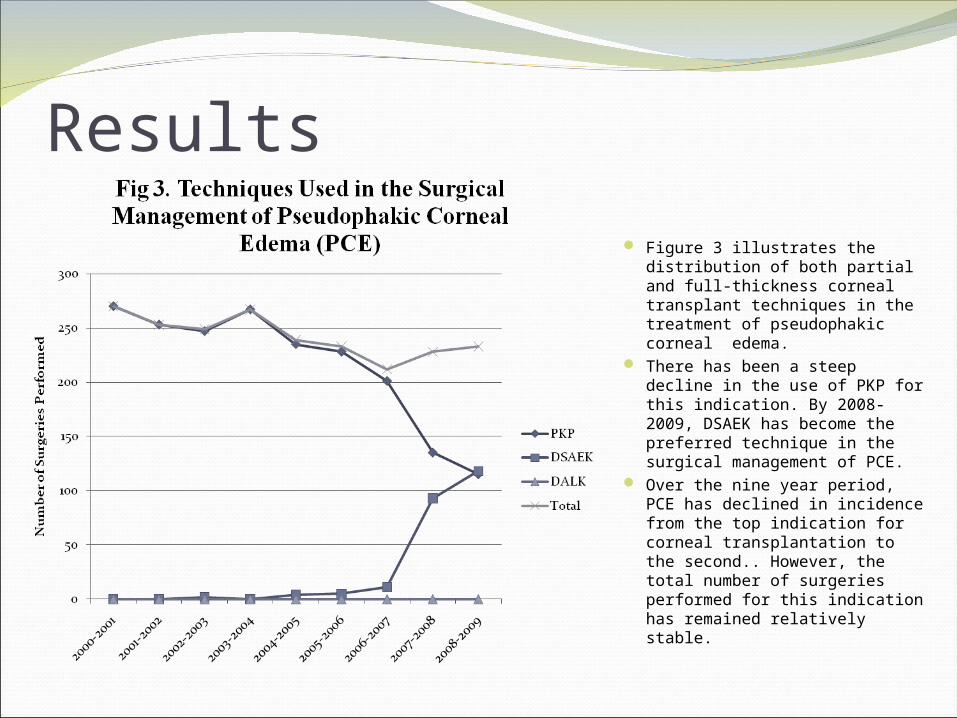
Figure 3 illustrates the distribution of both partial and full-thickness corneal transplant techniques in the treatment of pseudophakic corneal edema.
There has been a steep decline in the use of PKP for this indication. By 2008-2009, DSAEK has become the preferred technique in the surgical management of PCE.
Over the nine year period, PCE has declined in incidence from the top indication for corneal transplantation to the second.. However, the total number of surgeries performed for this indication has remained relatively stable.
Results
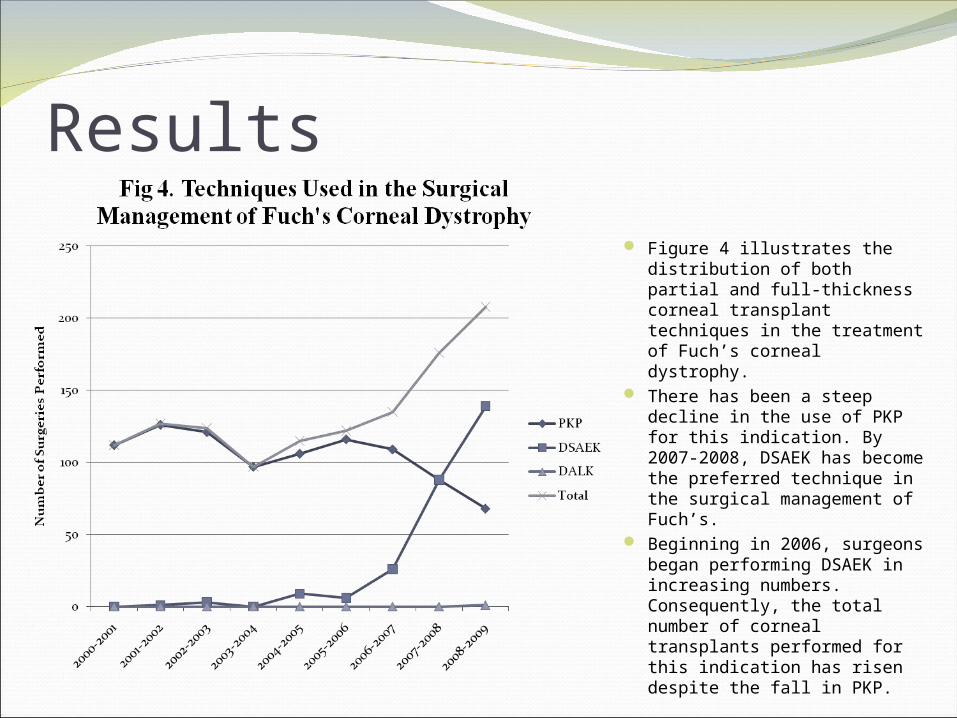
Figure 4 illustrates the distribution of both partial and full-thickness corneal transplant techniques in the treatment of Fuch’s corneal dystrophy.
There has been a steep decline in the use of PKP for this indication. By 2007-2008, DSAEK has become the preferred technique in the surgical management of Fuch’s.
Beginning in 2006, surgeons began performing DSAEK in increasing numbers. Consequently, the total number of corneal transplants performed for this indication has risen despite the fall in PKP.

Results Figure 5 illustrates the
distribution of both partial and full-thickness corneal transplant techniques in the treatment of anterior keratoconus.
There has been a gradual decline in the number of PKP procedures performed for this indication.
The first DALK procedure was performed in 2006. Since then, there has been a modest increase in the number performed per year.
From 2000 to 2007, the total number of corneal transplants performed for anterior keratoconus paralleled the declining numbers of PKPs. This trend has reversed with the advent of DALK.
Results
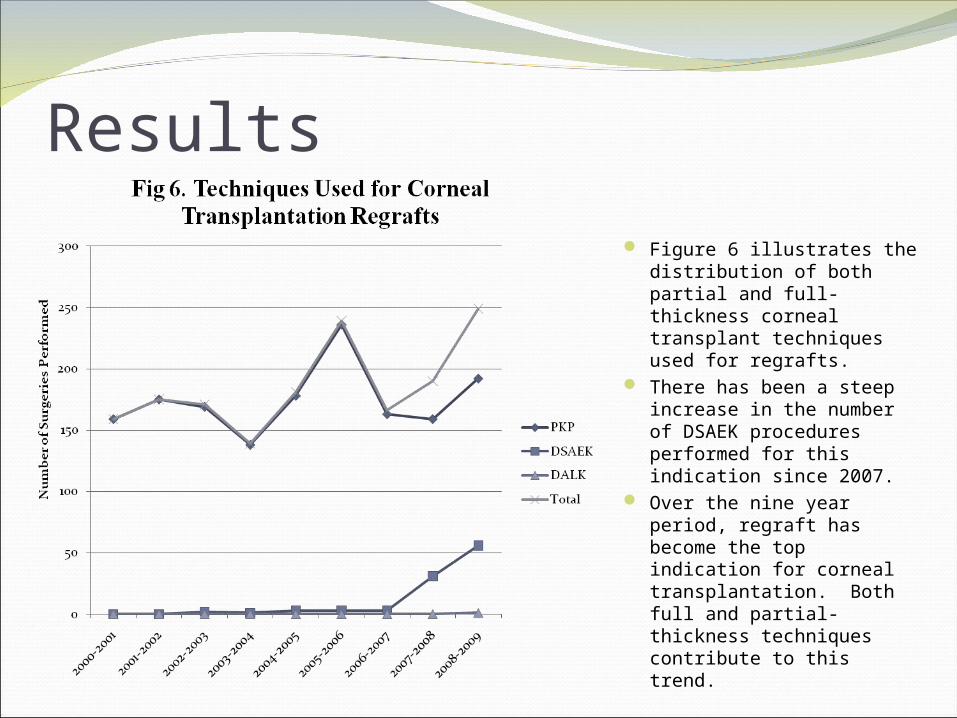
Figure 6 illustrates the distribution of both partial and full-thickness corneal transplant techniques used for regrafts.
There has been a steep increase in the number of DSAEK procedures performed for this indication since 2007.
Over the nine year period, regraft has become the top indication for corneal transplantation. Both full and partial-thickness techniques contribute to this trend.
Discussion The top indications for corneal transplantation have changed over the past decade.
Regraft is now the leading indication in Ontario, followed by PCE, Fuch’s, and anterior keratoconus. An aging population and the expected eventual failure of grafted tissues may contribute to the higher frequency of regrafts. Advances in cataract surgery have likely led to the decrease in transplants performed for PCE. Surgery for Fuch’s appears to be on an upwards trend, due at least in part to the increasing popularity of DSAEK.
The number of PKPs has been declining since 2000. The total number of transplants performed per year has paralleled PKPs until 2006, at which point it began to rise sharply due to the introduction of partial thickness transplant techniques. Greater confidence in the success of these procedures and the patient benefit of reduced recovery time have likely driven this change.
DSAEK has become the favoured technique used in the surgical management of Fuch’s and PCE. DALK is gaining momentum in the context of anterior keratoconus. The changes in preference for these newer techniques and their continued evolution should prompt a re-evaluation of the mismatch between the supply and demand for corneal tissues in Ontario.
References1. Council on Scientific Affairs. Report of the organ transplant
panel: corneal transplantation. JAMA 1988;259:719.22.
2. Dorrepaal SJ, Cao KY, Slomovic AR. Indications for penetrating keratoplasty in a tertiary referral centre in Canada, 1996-2004. Canadian Journal of Ophthalmology 2007;42:244.50.
3. Maeno A, Naor J, Lee HM, Hunter WS, Rootman DS. Three decades of corneal transplantation: indications and patient characteristics. Cornea 2000;19:7.11.
4. Lindquist TD, McNeill JI, Wilhelmus KR. Indications for keratoplasty [editorial]. Cornea 1994;13:105.7.





























