Embed Size (px)
Citation preview

Prepared and Presented by:
Ms. Sohad Noorsaeed, RN. MSN

Learning Outcomes Upon the completion of “ Skin integrity” lecture, the learners
will be able to:
1. Describe factors affecting skin integrity.
2. Identify clients at risk for pressure ulcers.
3. Describe the four stages of pressure ulcer development.
4. Identify assessment data pertinent to skin integrity, and
pressure sites.
5. Discuss measures to prevent pressure ulcer formation.
6. Describe nursing strategies to treat pressure ulcers.
7. Applying nursing process to patient with skin problems.

Introduction The skin is the largest organ in the body and serves a
variety of important functions in maintaining health and
protecting the individual from injury. It provides
mechanical and immunological protection,
thermoregulation, neurosensorial function, vitamin D
synthesis, and homeostasis of fluids, electrolytes, and
proteins.

SKIN INTEGRITY Intact skin refers to the presence of normal skin and skin
layers uninterrupted by wounds.
factors affecting skin integrity:
• Genetics (skin color, allergies, sense to light).
• Age.
• Health status ( clients with impaired peripheral arterial circulation may have skin on the legs that appears shiny, has lost its hair, and damages easily
Internal
• Activity, diet… External
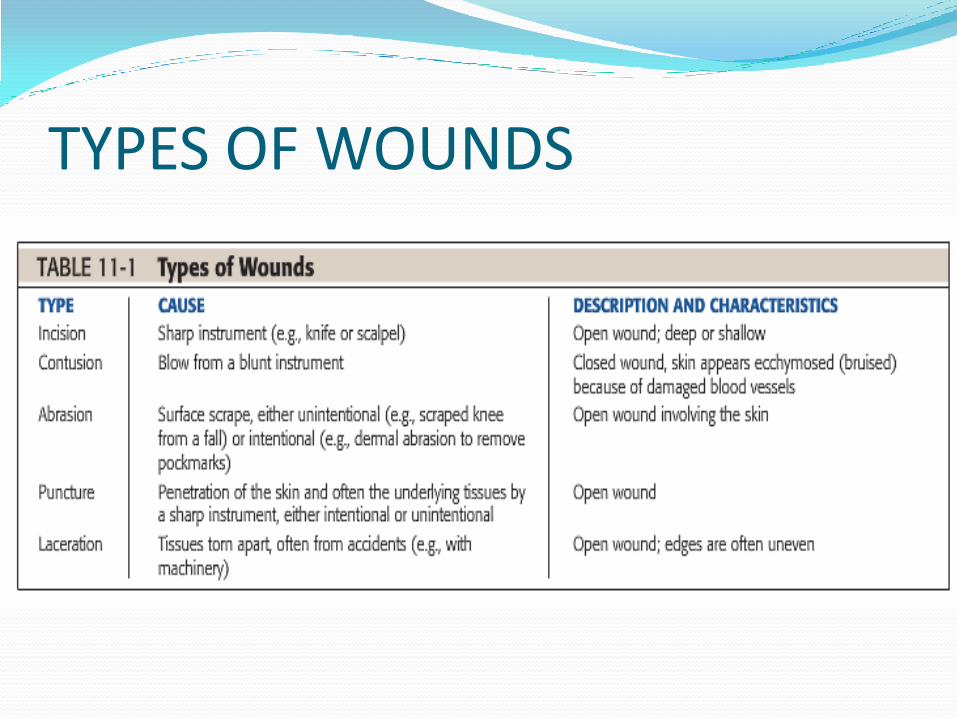
TYPES OF WOUNDS

Incision

Contusion

Abrasion

Puncture

Laceration

PRESSURE ULCERS Pressure ulcers (also called bed sores, pressure sores,
or decubitus ulcers).
a pressure ulcer is defined as “a localized injury to the
skin and/or underlying tissues usually over bony
prominences, as a result of pressure, or pressure in
combination with shear (cut).

Etiology of pressure ulcers Pressure ulcers are due to localized ischemia, a deficiency in the
blood supply to the tissue. The tissue is compressed between two
surfaces, usually the surface of the bed and the bony skeleton, with
greater than 32 mmHg pressure. When blood cannot reach the
tissue, the cells are deprived of oxygen and nutrients and the tissue
consequently dies.
After the skin has been compressed, it appears pale, as if the blood
has been squeezed out of it. When pressure is relieved, the skin takes
on a bright red flush, called reactive hyperemia due to vasodilation.
If the redness disappears in that time, no tissue damage can be
anticipated. If, however, the redness does not disappear, then tissue
damage has occurred.
Risk factors of pressure ulcers Immobility and inactivity. Inadequate nutrition. Fecal and urinary incontinence. Decreased mental status. Diminished sensation. Excessive body heat. Advanced age. Presence of certain chronic conditions. Friction (a force acting parallel to the skin surface by
sheets rubbing against skin) shearing force (a combination of friction and pressure) are
other factors frequently acting in conjunction with pressure to produce pressure ulcers.

Stages of Pressure Ulcers

Stage I

Stage II

Stage III
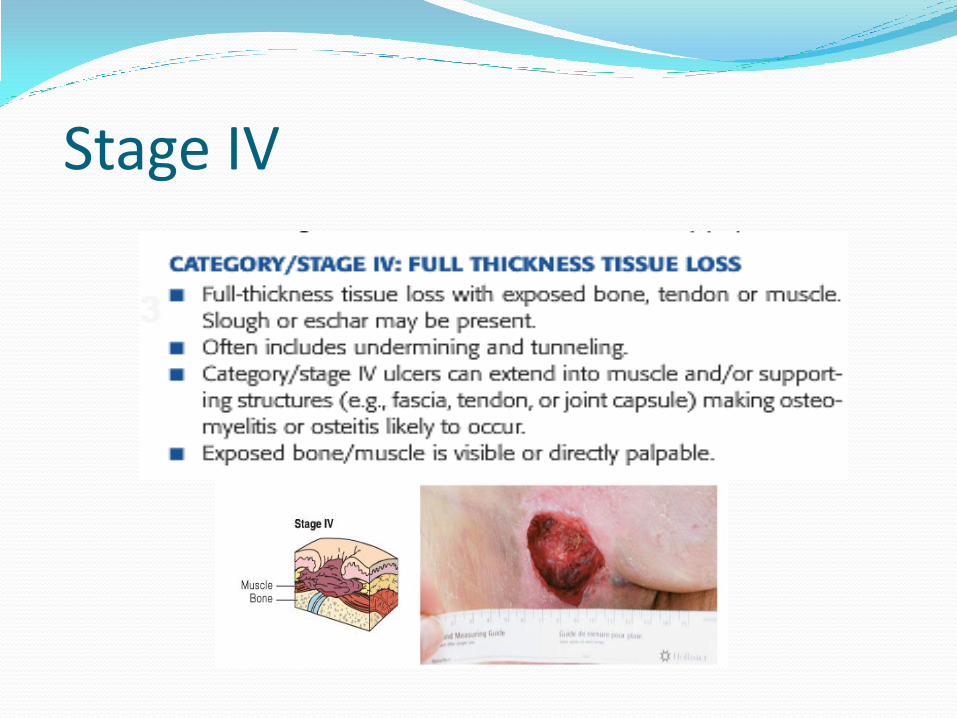
Stage IV
Risk Assessment Tool Risk assessment tools (also called risk assessment
scales, calcu-lators, or scores) are key components in any prevention guidelines and constitute an initial step in pressure ulcer prevention models that aim to identify those patients at risk. Risk assessment tools are structured models including categories of factors that are associatedto varying degrees of reliability, with pressure ulcer development. There are several published risk assessment tools such as the Norton scale, Waterloo scale, and Braden scale.
Braden Scale In the Braden scale six risk factors (or risk indicators)
are considered: sensory perception, moisture, activity,
mobility, nutritional status, and shear/friction.
Each category is rated 1 to 4 except shear/friction,
which is rated 1 to 3. The minimum risk score is 6 and
the maximum is 23. Patients are deemed to be at risk
when their cutoff score is ≤18.

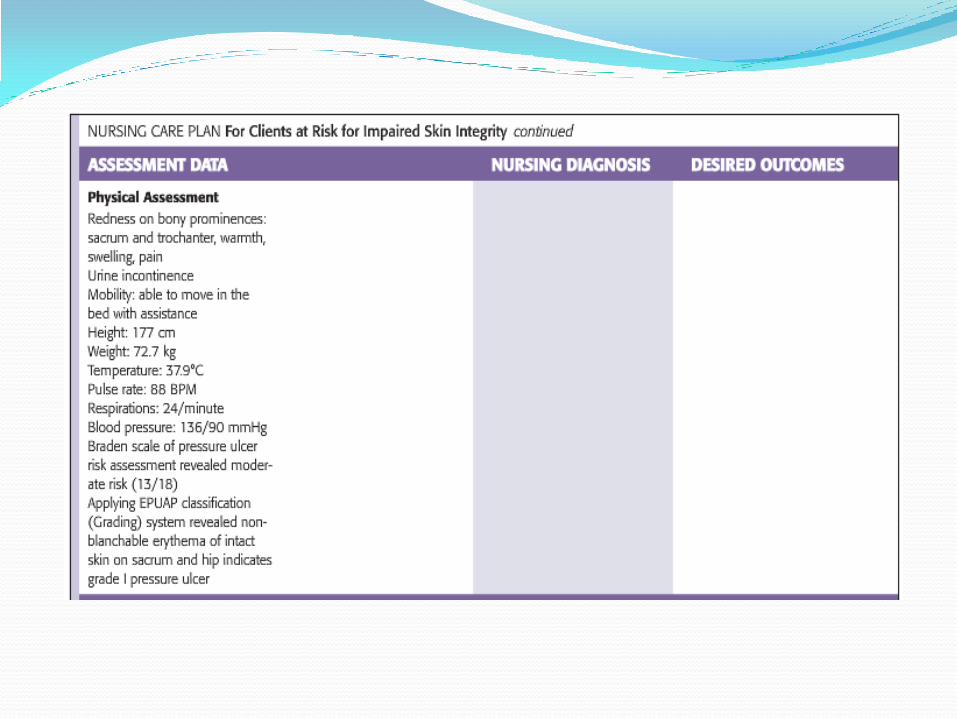
NURSING MANAGEMENT Assessing: When a pressure ulcer is present, the nurse notes the
following: Location of the ulcer, related to a bony prominence. Size of ulcer in centimeters. Presence of undermining or sinus tracts, assessed as a clock face, with 12 o’clock as the client’s head. Stage of the ulcer. Color of the wound bed and location of necrosis (dead tissue) or eschar. Condition of the wound margins. Integrity of the surrounding skin. Clinical signs of infection, such as redness, warmth, swelling, pain,
odor, and exudate (note color of exudate).

Diagnosing The NANDA nursing diagnoses (2007) that relate to clients who
have skin wounds or who are at risk for skin breakdown are
Risk for Impaired Skin Integrity: At risk for skin being
adversely altered
Impaired Skin Integrity: Altered epidermis and/or dermis
Impaired Tissue Integrity: Damage to mucous
membrane,
corneal, integumentary, or subcutaneous tissues.

Additional nursing diagnoses may be appropriate for clients with existing impaired skin or tissue integrity. Examples of these diagnoses include:
Risk for Infection if the skin impairment is severe, the client is immunosuppressed, or the wound is caused by trauma
Pain related to nerve involvement within the tissue impairment or as a consequence of procedures used to treat the wound.

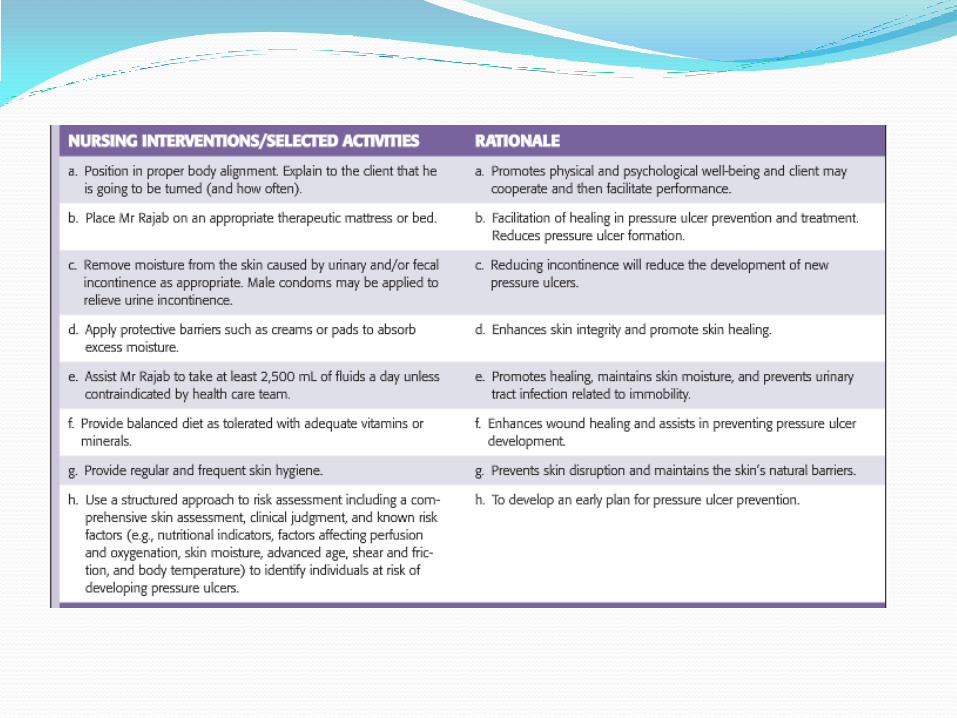
Nursing Intervention
Preventing and Treating Pressure Ulcers
To reduce the likihood of pressure ulcer development in
all clients, the nurse employs a variety of preventative
measures to maintain skin integrity.
1- MAINTAINING SKIN HYGIENE.
2- AVOIDING SKIN TRAUMA.