Embed Size (px)
Citation preview
Optimizing Early Prenatal Care for
Your Patients: What’s new on the Ontario Perinatal
Record?
Dr. Miranda Sheppard Dr. Nisha Arora
Ms. Wendy McCradyWednesday May 9, 2018
Learning Objectives
1. To review investigations in the first trimester including: dating ultrasound, prenatal screening, early diabetes screening
2. To review which immunizations are indicated in pregnancy, including pertussis and influenza, and how to assess rubella immunity.
3. To understand how and when to prescribe aspirin to your pregnant patient.
Presenter Disclosure
Faculty: Miranda Sheppard, Nisha Arora, Wendy McCrady
Relationships with commercial interests: none
Grants/Research Support: none
Speakers Bureau/Honoraria: none
Consulting Fees: none
Other: none
Disclosure of Commercial Support
This program has not received financial support or in-kind support.
Potential for conflict(s) of interest: none
Mitigating Potential Bias
Not applicable.

AgendaPrenatal Investigations
Immunizations
Aspirin
Discussion

Prenatal Investigations

When is your patient due?
Earliest T1 scan with CRL 10-84mm is best parameter
LMP underestimates US-based EDD by 2-3 days
US dating reduces IOL by 70% compared to “certain LMP” (in both T1/T2)
T1 scan should be offered to all, can be combined with scan for NT
Composite age on T2 scan (<23wk) more accurate than LMP
SOGC Clinical Practice Guideline. Determination of Gestational Age by Ultrasound, JOGC, February 2014

Prenatal Screening
Screening should be offered, regardless of maternal age
Discuss risks, benefits, alternatives
1) No screening
2) Standard prenatal screening → now eFTS (or MSS if presenting 14-20+6wk)
3) US-guided invasive testing, when appropriate
4) NIPT (maternal plasma cell-free DNA screening) - may not be covered by OHIP
Joint SOGC-CCMG Guideline: Update on Prenatal Screening for Fetal Aneuploidy, Fetal Anomalies, and Adverse Pregnancy Outcomes, JOGC, Sept 2017
Still offer T1 Ultrasound
Offered regardless of screening test chosen
Viability, GA, multiples & choronicity, early anatomy, NT
eFTS should not be done if NIPT being done
Not indicated solely to detect higher risk of adverse pregnancy outcomes
Joint SOGC-CCMG Guideline: Update on Prenatal Screening for Fetal Aneuploidy, Fetal Anomalies, and Adverse Pregnancy Outcomes, JOGC, Sept 2017

What is eFTS??
Screens for T21, can flag high T18 risk
Placental growth factor & T1 alpha fetoprotein added to PAPP-A and beta hCG; combined with NT & patient history
Still done 11+0 to 13+6wk
DOES NOT screen for NTD/spina bifida
Good quality T2 US more accurate, consider AFP if BMI >35
IPS can no longer be ordered at LHSC (Jan 2018)
SOGC Clinical Practice Guideline. Prenatal Screening, Diagnosis, and Pregnancy Management of
Fetal Neural Tube Defects, JOGC, Oct 2014
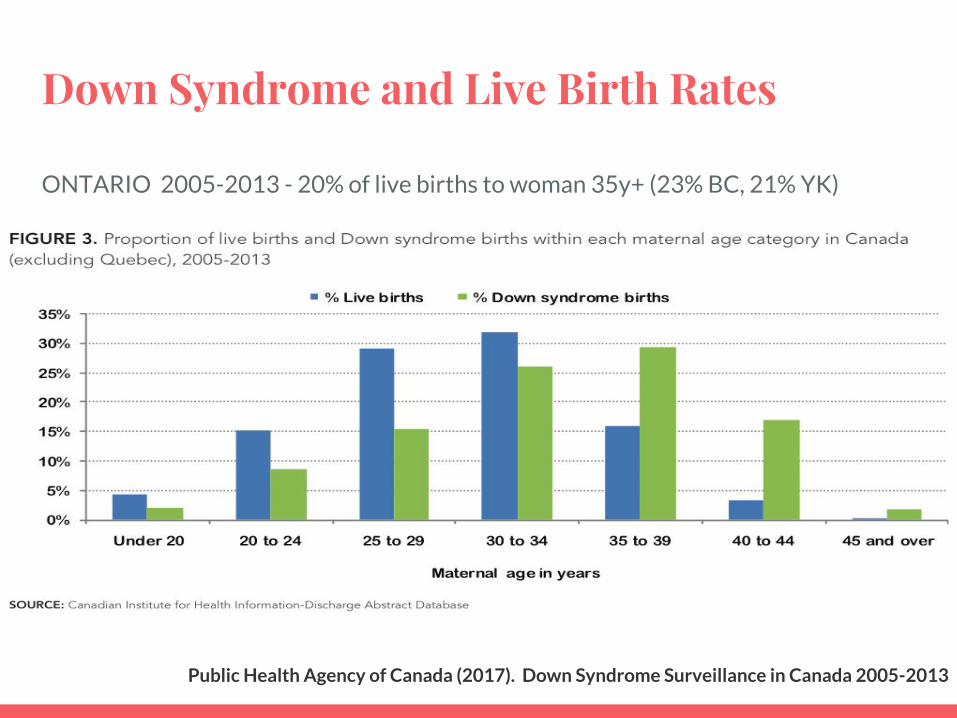
Down Syndrome and Live Birth Rates
ONTARIO 2005-2013 - 20% of live births to woman 35y+ (23% BC, 21% YK)
Public Health Agency of Canada (2017). Down Syndrome Surveillance in Canada 2005-2013



eFTS: How does it compare?
Screening Test Detection Rate False Positive Rate
Current FTS 78-85% 8-9%
Enhanced FTS (eFTS)
85-90% 3-6%
eFTS (no NT ) ~80% ~5%
IPS 85-90% 2-4%
MSS (quad screen)
75-85% 5-10%
Trillium Health Partners. Enhanced FTS Information FAQs. Accessed Mar 22, 2018
9%
eFTS is positive, now what??
Counsel patient - remind eFTS is screening test, additional screening/diagnostic tests available
1. cfDNA → MD/NP can order, refer to genetics if + screen
2. If pt would not be reassured by neg cfDNA (2nd screening test) → offer referral to genetics
● CVS (11-13wk) SA risk 1%
● Amnio (15-17wk) SA risk 0.01-0.5%
● Results: QI-PCR 2-3d, microarray 2wk, single gene test 2-6wk
Carroll, J. et al. (Aug, 2007). Reference Guide for Health Care Providers Prenatal Screening Tests for the
Detection of: Down Syndrome, Trisomy 18 and Open Neural Tube Defects..

eFTS is positive, now what??
NT >3.5mm in T1 → REQUIRES GENETIC COUNSELLING
Will be offered additional testing
Risk T21, T18, T13, XO
Risk microdeletions, other chromosome anomalies
(genetics will offer microarray, karyotype)
Risk single gene conditions
Risk structural fetal anomalies, esp cardiac

cfDNA testing/NIPT STILL A SCREENING TEST● ~10wk GA mean amount of circulating fetal cfDNA 10% in maternal serum
● Can be performed after 9wk GA
● Turn-around-time 10 business days
● Harmony (Gamma Dynacare), Panorama (Life Labs)
○ Considered equivalent
○ Can be used with twins but data limited
○ NOT to be used with “vanishing twin” or twin demise
● Primary Care Provider can order ○ >= 40 years at EDD
○ Abnormal serum screen i.e. eFTS/MSS
○ NT >= 3.5mm or greater → consider direct referral to genetics
○ Previous pregnancy/child with aneuploidy

What does a positive NIPT result mean?T21
● 99% detection rate, <1% false positive
● PPV 90.9%
T18
● 96.4% detection rate, <1% false positive
● PPV 93.1%
T13
● 99% detection rate, <1% false positive
● PPV 38.1%
Monosomy X
● 92.9% detection rate, <1% false positive
● PPV 50.0%
28,739 samples
82.9% PPV for all aneuploidies
Dar, P. et al. (2014). Clinical experience and follow-up with large scale single-nucleotide polymorphism-based noninvasive prenatal aneuploidy testing. Am J Obstet Gynecol 211(5): 527.

Failed NIPT Results
● Increased BMI, early GA → lower fetal fraction
● Can order repeat sample x1
● If failed x2 → suggest another form of screening or diagnostic testing
○ Aneuploidy can have lower fetal fraction

Prenatal Screening - Twin Pregnancy
● eFTS - PAPP-A and beta hCG; combined with NT & patient history
○ Previously risk quoted based on NT alone
○ 85% detection rate, 5% false positive rate
● eFTS will report ONE risk for a twin pregnancy
○ Monochorionic → the chance that both affected
○ Dichorionic → the chance that one or both affected
● If twin demise or “vanishing twin”
○ NYGH advises against eFTS, suggest NT and MSS instead
○ Can call lab to discuss individual cases
North York General Hospital. (Feb, 2017). Enhanced-FTS for TWINS - FAQs Handout.

Abnormal US findings
● NT >3.5mm in T1 → REQUIRES GENETIC COUNSELLING, offered additional testing, detailed T2 US with good heart views
● If negative eFTS - “soft markers” associated with fetal trisomy 21 (echogenic intracardiac focus) or trisomy 18 (choroid plexus cysts) ARE NOT clinically relevant (poor PV) and DO NOT warrant further testing
● Fetal structural abnormality → requires genetic counselling/FDC referral
Joint SOGC-CCMG Guideline: Update on Prenatal Screening for Fetal Aneuploidy, Fetal Anomalies, and
Adverse Pregnancy Outcomes, JOGC, Sept 2017

Prenatal Screening Resources
● Genetics Education Canada - Knowledge Organization (GEC-KO)
○ “Guide to Understanding Prenata Screeningl Tests” (21page PDF)
○ http://www.geneticseducation.ca/uploads/Prenatal_screening_Public_Brochure_ONTARIO_Jan2018_v2.pdf
● North York General Hospital Prenatal Services
○ Prenatal Screening Requisition
■ http://www.nygh.on.ca/data/2/rec_docs/2978_MSS_Requisition.pdf
○ eFTS for singleton and twin pregnancies info sheets
■ http://www.nygh.on.ca/data/2/rec_docs/2720_FAQ_eFTS_Singleton_Feb_2017.pdf
■ http://www.nygh.on.ca/data/2/rec_docs/2721_FAQ_eFTS_Twins_Feb_2017.pdf
Does your patient have diabetes?
If there is a high risk of gestational diabetes mellitus based on multiple risk
factors, screening or testing should be offered during the first half of the pregnancy and repeated at 24
to 28 weeks’ gestation if initially normal.
Almost 25% of the time, GDM can be diagnosed before 24weeks.

When to screen early for diabetes
● maternal age > 35 years● obesity (pre-preg BMI > 30)● ethnicity (Aboriginal, African, Asian, Hispanic, South Asian)● family history of diabetes● polycystic ovary syndrome● acanthosis nigricans● corticosteroid use● previous pregnancy complicated with GDM● previous macrosomic infant
SOGC 2016

Immunizations

Ontario Antenatal Record 2005
Ontario Perinatal Record 2017

Benefits of Immunizations in Pregnancy
● Protect pregnant woman: altered immune response - increased risk for infection and severe outcomes if infected. Pregnant women respond adequately to vaccines even though pregnancy is an immunologically altered state.
● Protect fetus: passive immunity - maternal antibodies transferred to fetus transplacentally, majority during T3
● Protect neonate and young infant: passive immunity through colostrum/breast-feeding; prevents mother from acquiring infection that may be passed on to newborn baby

General Considerations
● Are vaccines safe for pregnant women and their fetus if given during pregnancy?
● Do vaccines provide effective protection to pregnant women if given during pregnancy?
● Does vaccinating mothers increase the protection of infants?
● Does maternal antibody transferred across the placenta interfere with neonatal immune response to immunization?

Safety of Inactivated Vaccines in Pregnancy
● Inactivated vaccines, and toxoids are considered safe in pregnancy● No data showing teratogenicity, embryotoxicity, or specific adverse pregnancy
outcomes● Reactions following vaccination usually limited to injection site● No increase in anaphylactic reactions or events that might induce preterm
labour has been observed● There is no safety reason to avoid the use of thimerosal-containing vaccines
(EngerixB, Fluviral, Fluzone, Vaxigrip) for pregnant women.
NACI

Risks/Contraindications
● Live and live-attenuated vaccines contraindicated: ○ MMR, VZ, HZ, Yellow Fever, oral Typhoid, (Small Pox-special access), (Flumist, Rotavirus)
○ Due to a theoretical risk to the fetus. (SOGC II-3)
● Non-pregnant women immunized with live/live-attenuated vaccine should be counselled to delay pregnancy for at least 4 wks. (SOGC III)
● Women who have inadvertently received immunization with live or live-attenuated vaccines during pregnancy should not be counselled to terminate the pregnancy because of a teratogenic risk. (SOGC 2018)
○ No evidence of CRS in any of the offspring of the 226 women inadvertently vaccinated with
MMR during pregnancy (NACI)
○ CRS in 1%-2% of 321 women inadvertently vaccinated while pregnant (CDC/SOGC 2018)

Assess Risk/Benefit
● Harm of contracting wild disease >> harm from immunization
● In some situations, potential benefits of vaccination with MMR vaccine may outweigh risks such as during measles or rubella outbreaks, in which case vaccination may be considered based on recommendations from public health officials
● Yellow fever vaccine may be considered in a pregnant woman travelling to an endemic area
● Pregnancy is considered a medical reason for exemption for YF vaccination to enter some countries
NACI, SOGC 2018
Maternal vaccination effect on newborn
● Recommended infant immunization schedules take into consideration the potential effect that maternally transferred antibodies may have on infant vaccinations
● Maternal antibodies typically have a half-life of 3 to 4 weeks in the newborn, and progressively decrease during the first 6 to 12 months of life.
● Example: Live vaccines scheduled for children >12 mo old and not counted if given prior
NACI

Influenza Vaccine - Safety
● Good evidence demonstrating safety of inactivated influenza vaccine in pregnancy
● Live attenuated flu vaccine (Flumist) should not be given to pregnant women
● Most flu vaccines contain thimerosal – safe in pregnacy (not in Agriflu)
● Active surveillance following influenza vaccination during pregnancy has not shown evidence of associated harm to the mother or fetus
Pregnancy = High Priority for Flu Shot
● Increased risk of influenza-associated morbidity
● Adverse neonatal outcomes associated with maternal influenza
● Vaccination of pregnant women protects their newborns from influenza and influenza-related hospitalization
● Infants born during influenza season to vaccinated women are less likely to be premature, small for gestational age, and low birth wt
NACI
Influenza
Women who did not receive influenza vaccination during pregnancy should receive influenza vaccine post-partum before discharge from hospital if it is influenza season (NACI)

Pertussis (Tdap)
● Increase in number of pertussis cases in Canada
● Greatest morbidity/mortality occurs in children < 6 mo old
● All adults: Substitute 1 time adult dose of Tdap for Td booster (most women of childbearing age), then boost with Td q10yr
● Generally takes 2-3 weeks post immunization to achieve immunity
NACI
Pertussis (Tdap)
SOGC (April 2018):All pregnant women should be offered the diphtheria and tetanus toxoids and acellular pertussis vaccine during the second or third trimester, preferably between 21 and 32 weeks gestation, during every pregnancy, irrespective of their immunization history (II-2A)
Passive antibody transfer minimal until 13-16 weeks gestation, maximized @ 27-32 weeks. Can start at 21 weeks to capture those who deliver prematurely, as it takes 3 weeks to reach immunity levels.
Protection of the newborn >85%
Rubella Vaccine
● Live attenuated – do not generally give if known pregnancy
● Immunity desirable prior to pregnancy – delay pregnancy until 4 weeks after immunization
● Highest risk of CRS in 1st trimester, progressive decrease in risk thereafter, very uncommon after 20 weeks gestation
● OB standard of care to check immunity early in pregnancy and given post partum if not immune
● Check immunity 6 weeks pp if given with RhIg
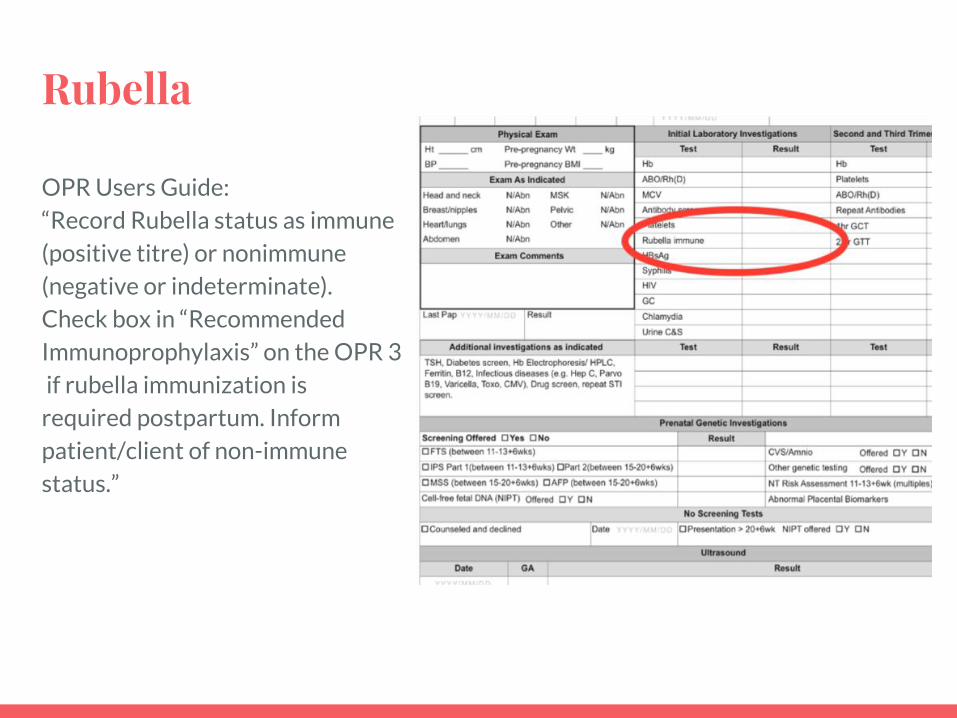
Rubella
OPR Users Guide:“Record Rubella status as immune(positive titre) or nonimmune (negative or indeterminate). Check box in “Recommended Immunoprophylaxis” on the OPR 3 if rubella immunization is required postpartum. Inform patient/client of non-immune status.”

Rubella - NACI and SOGC guidelines (2018)
MMR not needed - don’t screen for Rubella titre
1 dose MMR in immediate post-partum
● Documented 1 dose of MMR >12 mo, even if titre done and negative
● Rubella immune in previous pregnancy
● Rubella not immune/indeterminate AND no documentation of previous immunization (2 doses)


Aspirin

Aspirin can prevent preterm preeclampsia
● 2-8% pregnancies are affected by preeclampsia
● 2nd leading cause of maternal mortality world wide
● Over 1/3 of severe obstetric morbidity is related to preeclampsia
● Account for 15% of preterm birth
● Dramatically increased risk to neonate (IUGR, SGA, oligo, abruption, death)

Why do you need to know about Aspirin?
It needs to be started BEFORE 16 weeks gestational age.
That means you!
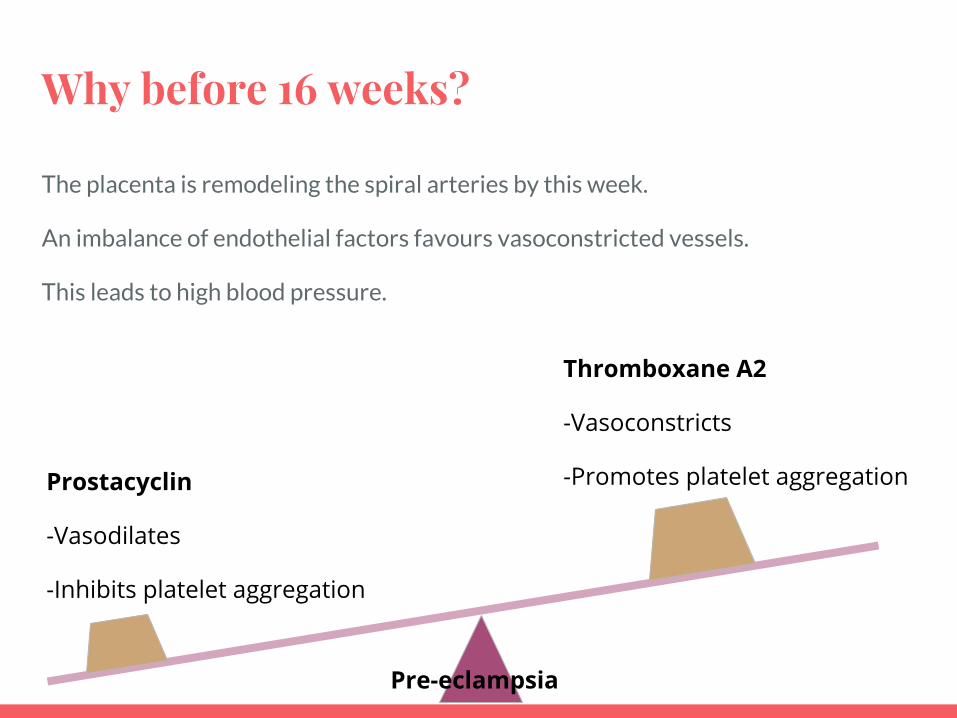
Why before 16 weeks?
The placenta is remodeling the spiral arteries by this week.
An imbalance of endothelial factors favours vasoconstricted vessels.
This leads to high blood pressure.
Prostacyclin
-Vasodilates
-Inhibits platelet aggregation
Thromboxane A2
-Vasoconstricts
-Promotes platelet aggregation
Pre-eclampsia
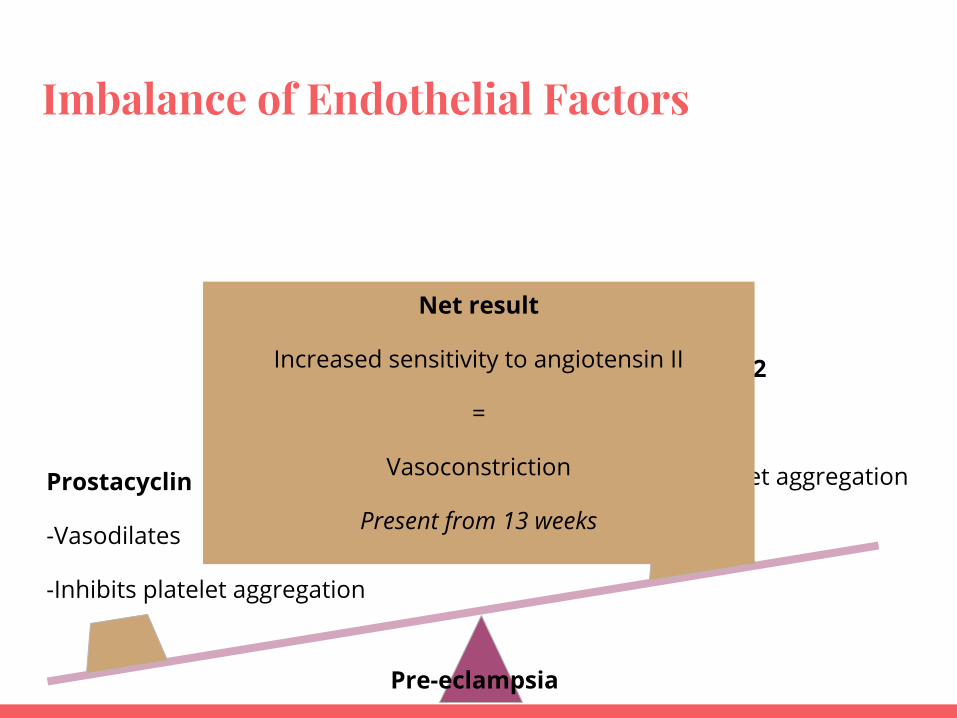
Imbalance of Endothelial Factors
Prostacyclin
-Vasodilates
-Inhibits platelet aggregation
Thromboxane A2
-Vasoconstricts
-Promotes platelet aggregation
Net result
Increased sensitivity to angiotensin II
=
Vasoconstriction
Present from 13 weeks
Pre-eclampsia

Pathophysiology
Placenta
-----------
Decidua
-----------
Myometrium
High pressureLow flow

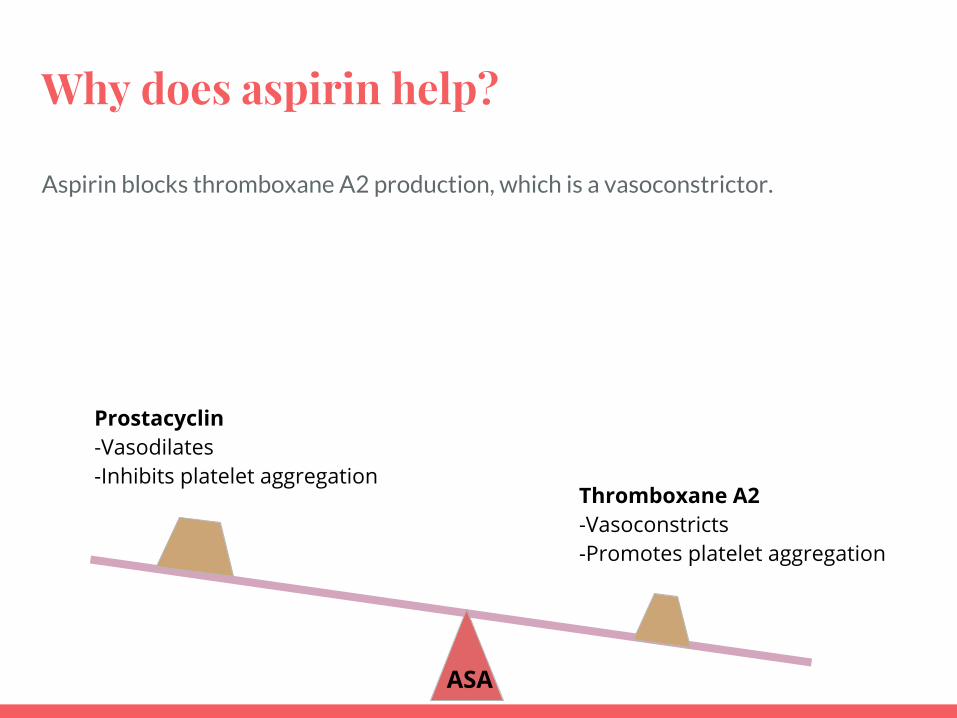
Why does aspirin help?
Aspirin blocks thromboxane A2 production, which is a vasoconstrictor.
Arachidonic acid
PGH2 Thromboxane A2
COX2ASA
Why does aspirin help?
Aspirin blocks thromboxane A2 production, which is a vasoconstrictor.
Prostacyclin-Vasodilates-Inhibits platelet aggregation
Thromboxane A2-Vasoconstricts-Promotes platelet aggregation
ASA

Who should get aspirin?
Some debate of how inclusive the list should be.
Generally:1. Prior preeclampsia, especially if with adverse outcome2. Chronic hypertension3. Type 1 or 2 Diabetes4. Renal disease5. Autoimmune disease (SLE, Antiphospholipid)6. Pre-pregnancy BMI >307. ART8. Multifetal gestation
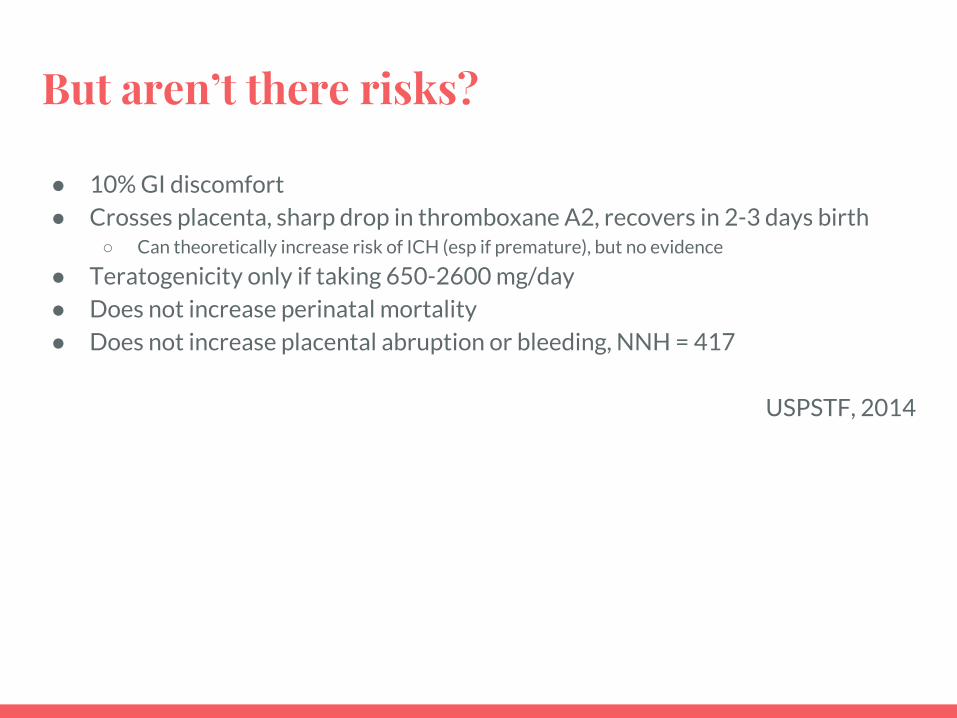
But aren’t there risks?
● 10% GI discomfort● Crosses placenta, sharp drop in thromboxane A2, recovers in 2-3 days birth
○ Can theoretically increase risk of ICH (esp if premature), but no evidence
● Teratogenicity only if taking 650-2600 mg/day● Does not increase perinatal mortality● Does not increase placental abruption or bleeding, NNH = 417
USPSTF, 2014

From the Ontario Perinatal Record

References

References
1. SOGC Clinical Practice Guideline No. 307. (2014). Diagnosis, Evaluation, and Management of the
Hypertensive Disorders of Pregnancy. JOGC, 36(5): 416–438.
2. SOGC Clinical Practice Guideline No. 334. (2016). Diabetes in Pregnancy. JOGC, 38(7): 667-679..
3. USPSTF. (2014). Low-dose aspirin use for the prevention of morbidity and mortality from
preeclampsia. Ann Intern Med. 161(11): 819-26.
4. Williams Obstetrics, 24e, Chapter 40: Hypertensive Disorders
5. SOGC Clinical Practice Guideline. Determination of Gestational Age by Ultrasound No. 303, (2014). JOGC, 36(2): 171-181.
6. Joint SOGC-CCMG Guideline: Update on Prenatal Screening for Fetal Aneuploidy, Fetal Anomalies, and Adverse Pregnancy Outcomes No. 348. (2017). JOGC, 39(9): 805-817.
7. SOGC Clinical Practice Guideline. Prenatal Screening, Diagnosis, and Pregnancy Management of Fetal Neural Tube Defects No. 314 (2014). JOGC, 36(10): 927-939.
8. Trillium Health Partners. Enhanced FTS Information FAQs. Retrieved from https://trilliumhealthpartners.ca/patientservices/genetics/Pages/Enhanced-FTS-FAQs.aspx.
9. Carroll, J., Allanson, J., Esplen, MJ. et al. (Aug, 2007). Reference Guide for Health Care Providers
Prenatal Screening Tests for the Detection of: Down Syndrome, Trisomy 18 and Open Neural Tube
Defects.. Retrieved from http://www.cheo.on.ca/documents/3/genetics-provider-guide-e.pdf.
10. Public Health Agency of Canada (2017). Down Syndrome Surveillance in Canada 2005-2013. Retrieved from https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/healthy-living/down-syndrome-surveillance-2005-2013/pub1-eng.pdf.
References
11. Dar, P., Curnow, KJ., Gross, SJ. . et al. (2014). Clinical experience and follow-up with large scale single-nucleotide polymorphism-based noninvasive prenatal aneuploidy testing. Am J Obstet Gynecol 211(5): 527. 12. North York General Hospital. (Feb, 2017). Enhanced-FTS for TWINS - FAQs Handout. Retrieved from http://www.nygh.on.ca/data/2/rec_docs/2721_FAQ_eFTS_Twins_Feb_2017.pdf.





























