Embed Size (px)
Citation preview

Walid Habre, MD, PhDUnit for Anesthesiological Investigations
& Pediatric Anesthesia Unit Geneva University Children’s Hospital
www.walidhabre.org
Respiratory physiology of the premature newborn

I have no COI to disclose

Learning objectives
1. Physiological characteristics of the premature newborn
2. Challenges raised by the premature birth and the lungs condition
3. How to adjust controlled ventilation to improve gas exchange and decrease the deleterious effects on haemodynamic, cardiac output and cerebral perfusion

Lung development
Schittny JC Cell Tissue Res (2017) 367:427–444

Biochemical and biomechanical regulators of lung growth
Warburton D. et al. Curr Top Dev Biol. 2010; 90: 73-158
Periodic peristaltic contractions
Promotes lenghteningepithelial cells
FGF10+ precursor pool
Airway smoothmuscle
Epithelial signaling
Fibronectin (FN)
Vasculature

Premature Newborn = Saccular stage 24 weeks GA to term
Characteristics:• Formation of thick immature inter-airspace septa• Further condensation of the mesenchyme• The primary septa contain a double-layered capillary network• The terminal ends of the bronchial tree represent wide spaces: saccules• Alveolar epithelial cells are differentiated into mature squamous
type I Pneumocytes and secretory rounded type II pneumocytes
Schittny JC Cell Tissue Res (2017) 367:427–444
Maturation of surfactant synthesis and secretion = key factor in determining whether the newborn lung can sustain gas exchange without collapsing.

Lamellar bodies containing surfactantAlveolar lining fluid
SURFACTANT
Pneumocytes II
Pneumocytes I
ALVEOLI
Water molecules
High surface tension
Strong attractive forces
Alveolar Collapse
Reduces surface tension
Surfactant interperses the water molecules
Lung stabilityLucia J et al. Paed Respir Rev 2010; 11: 135 – 142
Surfactant are capable of function by 24-28 weeks

Fetal lung liquidPulmonary epithelial cells
Secretion of lung liquid (vol ≅ FRC)
Flushes debris from the airways
Prevent collapse of lung tissues
(Lung Pressure > amniotic Pressure)
Stimulates lung developmentwith the fetal breathing movements
Diaphragm responsible for fetal breathing

Pathophysiological impact of the saccular stageReaching the canalicular stage is crucial: first future air–blood barriers are formed
and at least a minimal production of surfactant
Survival depends on the surface of gas exchange and amount of available surfactant
Switch of epithelial cells to absorb fetal lung liquid Fetal adrenaline & oxygen at birth
Priming sodium channels, aquaporin and transmembrane protein
Steroid & thyroid hormones
Fate of the fetal lung liquid
AIR-LIQUID INTERFACE

Alveolarization stage: 36 weeks GA to 3 years
Smooth muscle cell precursors move in
Fibrous network of elastic fiber and collagen fibrils
Upfolding of one of the 2 capillary layers
Formation of secondary septa: subdivide preexisting airspaces
New alveoli
Microvascular maturation
The double-layered capillary network fuses to a single-layered one

Premature neonate has more elastin than collagen fibers
Suki B et al. Compr Physiol 2011; 1:1317-1351
Viscoelasticityof the lung
CollagenElastinCoupling of the elastic and dissipative properties
Low strain Increased strain

Properties of muscle fiber typesType I Type IIa Type IIb
Contractile propertiesVelocity of shorteningTetanic forceFatigue resistance
++
++++
+++
+++
+++++++
Biochemical propertiesMitochondrial densityATP consumption rateOxidative enzymesGlycolytic enzymesGlycogen content
++++
+++++
+++++
+++++++
+++++
+++++++
Type I : slow-twitch, high-oxidative: posture and respirationType II: fast-twitch, low-oxidative: expulsive efforts and active movements

Relative proportion of Type I muscle fibers in ventilatory muscles
Diaphragm IntercostalMuscles
Premature infants < 37 GA 10% 20%
Full-term newborns 25% 46%
Children > 2 years 55% 65%
Keens TG et al. J Appl Physiol Respir Environ Exerc Physiol 1978; 44: 909
Premature neonates and infants are more susceptible to fatigue

Darnall EA et al. Clinics in Perinatology 2006 33, 883-914
Diaphragmatic work of breathing decreases& Dynamic lung compliance increases with maturation

Other key features of premature neonates:
! Percentage of REM sleep is around 60% in premature newborn !During REM sleep: blunted ventilatory response to CO2
!Biphasic response to hypoxia ! Periodic breathing: alternating periods of
hyperpnea and apnea: common breathing pattern ! Prevalence of apnea and periodic breathing:- 10% from 33-38 weeks PCA - Up to 60% in infants born less than 1500 g

Apnoea: main problem AND multifactorial Immature brainstem
neuronal circuitryAnatomy of upper airways
and chest wall
Immature lung volume Immature upper airway control, Blunted ventilatory responses to hypoxia and CO2
Feeding problems
Anemia

Outline
!Clinical challenges raised by premature physiology

Difficulties to maintain pharyngeal patencyduring normal respiration
Darnall EA et al. Clinics in Perinatology 2006 33, 883-914

!FRC
Characteristics of infants complianceDecrease in FRC

Functional residual capacity in full term control (FTC; n=64); preterm control (PTC; n=59); preterm respiratory distress syndrome (RDS; n=54);
and preterm chronic lung disease (CLD; n=42).
G Hülskamp et al. Thorax 2009;64:240-245Reduction in FRC is independently associated with prematurity, intrauterine growthrestriction and severity of neonatal lung disease.
Consequences of low FRC
Increased airway resistance Airway closure
Impaired gas exchange
Increased work of breathing

Hardman, J. G. et al. Br. J. Anaesth. 2006 97:564-570
Time to hemoglobin desaturation is depending on FRC
Hypoxia will occur much quicker in neonates and infants
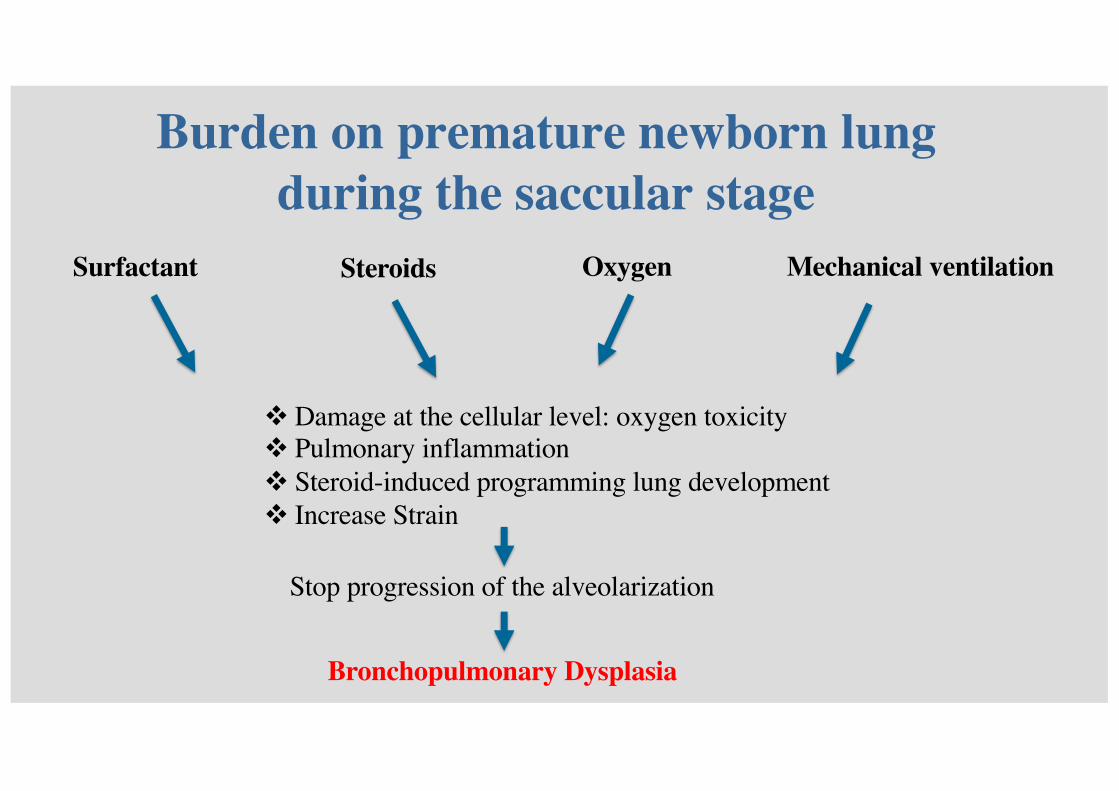
Burden on premature newborn lungduring the saccular stage
Mechanical ventilation
! Damage at the cellular level: oxygen toxicity! Pulmonary inflammation! Steroid-induced programming lung development! Increase Strain
Stop progression of the alveolarization
Bronchopulmonary Dysplasia
Surfactant Steroids Oxygen

Nieman GF et a. J Appl Physiol 2017; 22: 1516–1522
Alveolar instability
Repetitive alveoli recruitment and collapse with each breath
Heterogeneous ventilation
Excessive dynamic shear stress on alveolar walls of the unstable alveoli
Overdistension of adjacent alveoli during expiration
Dynamic strain during each breath

Mitochondrial fragmentation in fASM cells with increasing concentration of oxygen
Hartman W R et al. Am J Physiol Lung Cell Mol Physiol 2012;303:L711-L719
Apoptosis
> 50% FiO2
Mitochodrialfragmentation

Consequences of high O2 concentrations
↑BPD
↓cerebral blood flow
↑SVR↓FRC ↑atelectasis
↑oligodendrocyte apoptosis
↓ductus arteriosus patency
↑cerebral vascular ischemia
Target FiO2: 21 to 30%
Habre W et al. Br J Anaesth. 2014;113 Suppl 2:ii26-3
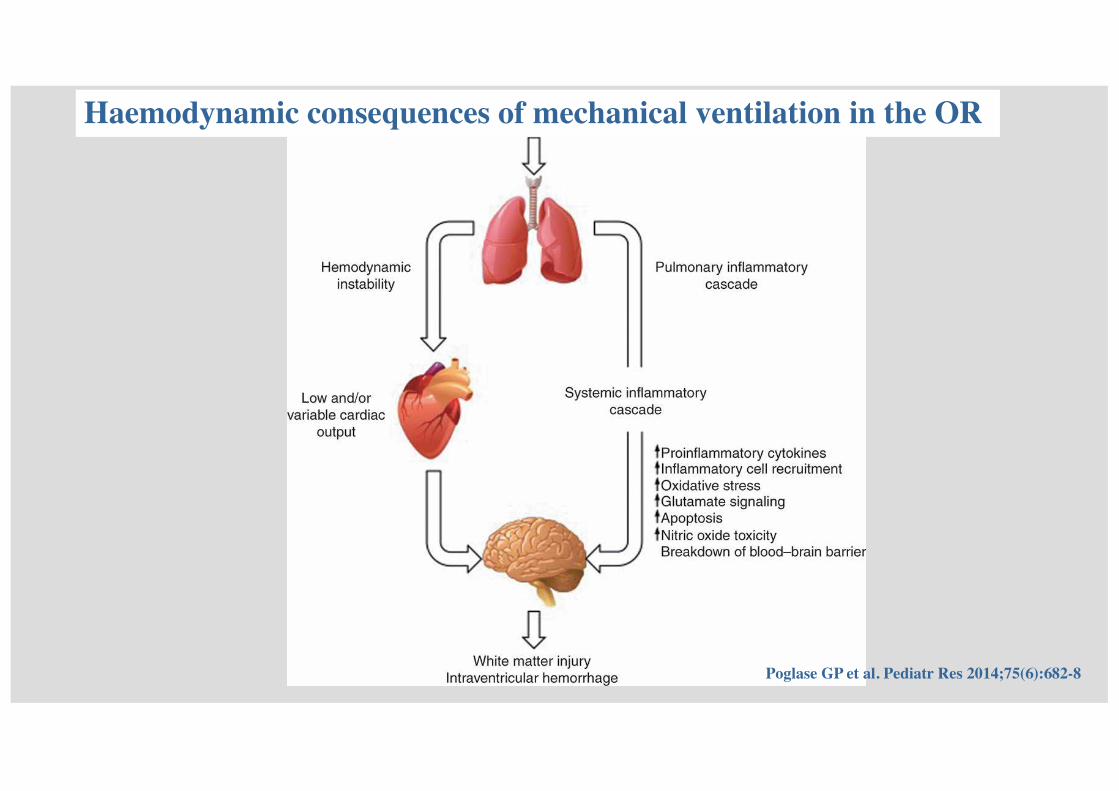
Haemodynamic consequences of mechanical ventilation in the OR
Poglase GP et al. Pediatr Res 2014;75(6):682-8
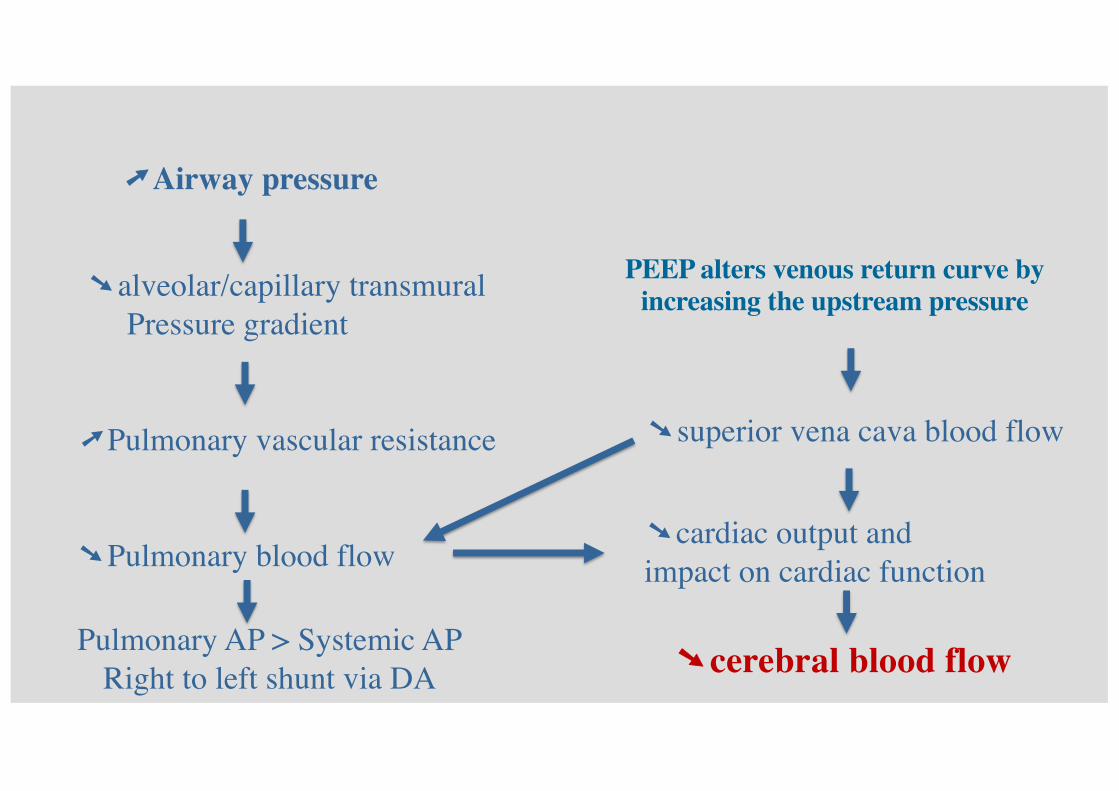
�Airway pressure
�alveolar/capillary transmuralPressure gradient
�Pulmonary vascular resistance
�Pulmonary blood flow
Pulmonary AP > Systemic APRight to left shunt via DA
�cardiac output and impact on cardiac function
PEEP alters venous return curve by increasing the upstream pressure
�superior vena cava blood flow
�cerebral blood flow

Poglase GP et al. Pediatr Res 2014;75(6):682-8
Developmental immaturityImpairment in0CBF0autoregulation
Preterm neonatal brain Injury
Suboptimal ventilation
Systemic circulatory disturbances

Outline
!Adjust Ventilation Mode to decrease respiratory and hemodynamic effects

Hypocarbia
Hypoxaemia
Periventricular leukomalacia
Hypercarbia
Intraventricular hemorrhage
Neurodevelopmentalimpairment
Ventilating a premature neonate in the OR:chase the enemies
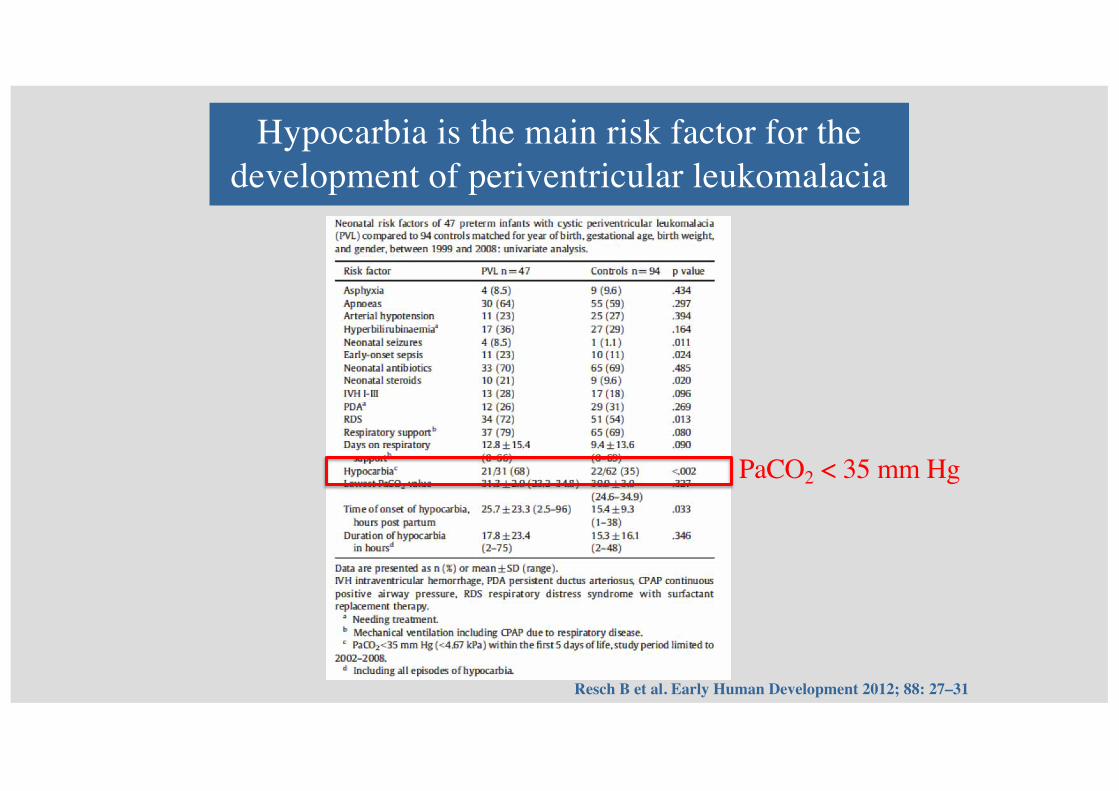
Hypocarbia is the main risk factor for the development of periventricular leukomalacia
Resch B et al. Early Human Development 2012; 88: 27–31
PaCO2 < 35 mm Hg

Driving pressure = specific tidal volume
.
VT/Crs
‘Specific’ tidal volume Tidal volume standardized for the end-expiratory lung volume
EELV
VT/EELV STRAIN

Pressure regulated volume controlled = Volume target ventilation = Volume guarantee
secondstrigger
Time
Pmax
Flow
Flow trigger
25%
Psupp
Vt
Minimal pressure in the airways and thus preventing elevated peak pressures
Decelerated flow like for PCV but with volume guaranteed
Gradual adjustment of the pressure generated by the
ventilator to lung condition

Rapid changes in lung compliance and resistance:Alveolar instability, surfactant, surgery, position changes
Initial requirement of high flow to reopen closed pulmonary areas (atelectasis)
Reduce high ventilatory peak pressure in premature infants
In patients with CHD in whom PEEP levels must be reduced to avoid hemodynamic complications
Marraro G. Ped Crit Care Med 2003; 4: 8-20
PRVC : 1st choice in neonatal anaesthesia

Spontaneous Ventilation
Pressure Support Ventilation Mechanical Ventilation
Age VC PC PRVC< 28 days ETT, n=294 2.4% 2.4% 17.3% 72.1% 3.4%
LMA, n=14 50% 21.4% 14.3% 14.3% 0
< 1 year ETT, n=1589 3.6% 5.4% 21.7% 61.4% 7.4%
LMA, n=610 45.1% 17.4% 9.8% 24.4% 3.1%
1-6 years ETT, n=5630 9.2% 7.9% 32.0% 45.3% 5.5%LMA: 4797 48.4% 13.6% 8.3% 27.5% 2.1%
6-12 years ETT, n=3825 6.2% 5.3% 39.6% 41.8% 6.9%LMA, n=3646 44.5% 12.1% 11.9% 29.0% 2.4%
> 12 years ETT, n=2318 2.3% 5.2% 43.8% 40.6% 7.9%LMA, n=1820 40.0% 11.2% 14.3% 31.0% 3.5%
Engelhardt T. et al. Br J Anaesth 2018; 121(1):66-75.

Cheema IU et al. Early Hum Dev. 2007;83(3):183-9.
PaCO2 was significantly higher in the VG group (VG: 5.7 kPa, SIPPV: 4.9 kPa; p = 0.03)
Lower incidence of out of range PaCO2 (< 5 kPa (35 mmHg) or > 7 kPa (50 mmHg) in infants 26 to 33 weeks of GA with PRVC

Klingenberg C et al. Cochrane Database of Systematic Reviews 2017, 10. CD003666.
RR 0.49 (95% CI: 0.33-0.72) NNTB 3 (95%CI: 2-5)
Reduction in the rates of hypocarbia < 4.7 kPa (35 mmHg) with PRVC

Outcomes Anticipated absolute effects* (95% CI)
Relative effect(95% CI)
No of participants(studies)
Quality of the evidence(GRADE)
Comments
Risk with PLV Risk with VTV
Death before discharge from hospital
Study population RR 0.75(0.53 to 1.07)
771(11 RCTs)
⊕⊕⊝⊝Low
Unblinded studies. Imprecision of estimates. 95% CI < 0.75.
163 per 1000 122 per 1000(86 to 175)
Death or BPD (36 weeks)
Study population RR 0.73(0.59 to 0.89)
584(8 RCTs)
⊕⊕⊕⊝Moderate
Unblinded studies.458 per 1000 334 per 1000
(270 to 408)
Duration of positive pressure ventilation(days)
MD of positive pressure ventilation (days); PLV group 0
MD 1.35 lower(1.83 lower to 0.86 lower) in VTV group
# 736(12 RCTs)
⊕⊕⊕⊝Moderate
Unblinded studies.
Pneumothorax Study population RR 0.52 (0.31 to 0.87)
825(13 RCTs)
⊕⊕⊕⊝Moderate
Unblinded studies.88 per 1000 46 per 1000
(27 to 77)IVH grade 3#4 Study population RR 0.53
(0.37 to 0.77)712(10 RCTs)
⊕⊕⊕⊝Moderate
Unblinded studies.184 per 1000 97 per 1000
(68 to 141)
IVH grade 3#4 or PVL
Study population RR 0.47(0.27 to 0.80)
441(6 RCTs)
⊕⊕⊕⊝Moderate
Unblinded studies.164 per 1000 77 per 1000
(44 to 131)
BPD (supplemental oxygen at 36 weeks)
Study population RR 0.68 (0.53 to 0.87)
620(9 RCTs)
⊕⊕⊝⊝Low
Unblinded studies. Possible publication bias based on funnel plot.
346 per 1000 235 per 1000(183 to 301)
*The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
Evidence that PRVC is superior to PCV in neonates up to 44 weeks GA
Klingenberg C et al. Cochrane Database Syst Rev 2017 Oct 17;10:CD003666

Start with PCV to establish desired tidal volume
respiration rateI/E: Time constant
Switch to PRVC
PEEP: 5 cm H2OMaximal pressure (30 cm H2O)
SlopeP support
Adapt the driving pressure

Best settings for Inspiratory time and RR in neonates?
Normal Ti in neonates: 0.35-0.5 sec
Determines somehow the RR
Start setting the ventilator with Ti of 0.5 sec
Be aware of haemodynamics with ➚TiAir trapping and PEEPi with ➘TeOptimal I/E ratio

Best Ventilation Strategy
Low Tidal Volume6-7 ml/kg
Normocapnia to Permissive mild Hypercapnia
Recruitment maneuver each time you loose PEEP
Restore FRC
Inflate(slowly(the(lungs(three(times(to(Paw of&30&cm&H2O&for(
at(least(5410(sec

High Frequency Oscillation Ventilation
In theory, ideally suited to the goals of lung-protective ventilation
Employs very small tidal volumes (usually less than anatomic dead space) around a constant mean airway pressure, delivered at a frequency typically between 9 -12 Hz.
High volume strategy: strategy to maintain lung volume
Better alveolar recruitment initial use of a higher mean airway pressure than on CV; initial weaning of high FiO2

Current Indications of HFOV
Respiratory Distress syndrome (RDS) refractory to conventional ventilationPersistent Pulmonary Hypertension of the Newborn (PPHN) Meconium Aspiration syndrome Air leak syndromesCongenital Diaphragmatic Hernia (CDH)Infants born at very low gestation and/or with very low birth weight to prevent CLD

There is no clear evidence that elective HFOV offers important advantages over CV when used as the initial ventilation strategy to treat preterm infants with acute pulmonary dysfunction. There may be a small reduction in the rate of CLD with HFOV use, but the evidence is weakened by the inconsistency of this effect across trials and the overall borderline significance.
High%frequency%oscillatory%ventilation%versus%conventional%ventilation%for%acute%pulmonary%dysfunction%in%preterm%infants
Cools F, and al. Cochrane Database Syst Rev. 2009 Jul 8;(3):CD000104.
There is evidence that the use of elective HFOV compared with CV results in a small reduction in the risk of CLD, but the evidence is weakened by the inconsistency of this effect across trials. Probably many factors, both related to the intervention itself as well as to the individual patient, interact in complex ways. In addition, the benefit could be counteracted by an increased risk of acute air leak. Adverse effects on short-term neurological outcomes have been observed in some studies but these effects are not significant overall. Most trials reporting long-term outcome have not identified any difference
Cools F. et al. Cochrane Database Syst Rev. 2015 Mar 19;(3):CD000104.

What is the optimal oxygen concentration to use during general anesthesia ?
Higher incidence of morbidityincluding ROP and BPD
85%-89% 90-95%
Higher risk of+deathnecrotizing enterocolitisPatent+ductus arteriosusPulm vasc resistanceApnoea
Set the FiO2 around 25%-35% to target SpO2 at 50th percentile: 90-95% (NEVER > 95%)

!pH"H+"DPG"T�"PCO2"HbS
"pH!H+!DPG!T�!PCO2"HbF
SpO2 values of >92% do not accurately correlate with PaO2
Cannot reliably prevent hyperoxic event
Fouzas S et al. Pediatrics 2011;128:740-752
Small variations of SpO2 might relate to disproportionally wider variations of PaO2
!The surfactant: key role for alveolar stability and major contributor to the viability of the premature
!At Full term, the number of alveoli is 15% of adult’s lung
!Alveolar instability promotes ventilation heterogeneity
!Unstable alveoli enhances shear stress and promotes dynamic strain
Key Points:

HypoxemiaHypocapnia
Cerebral'assault
Adapt'ventilation'to'rapid'changes'in'lung'complianceProtective'ventilation'strategy
NIRS'monitoring
Key Points:
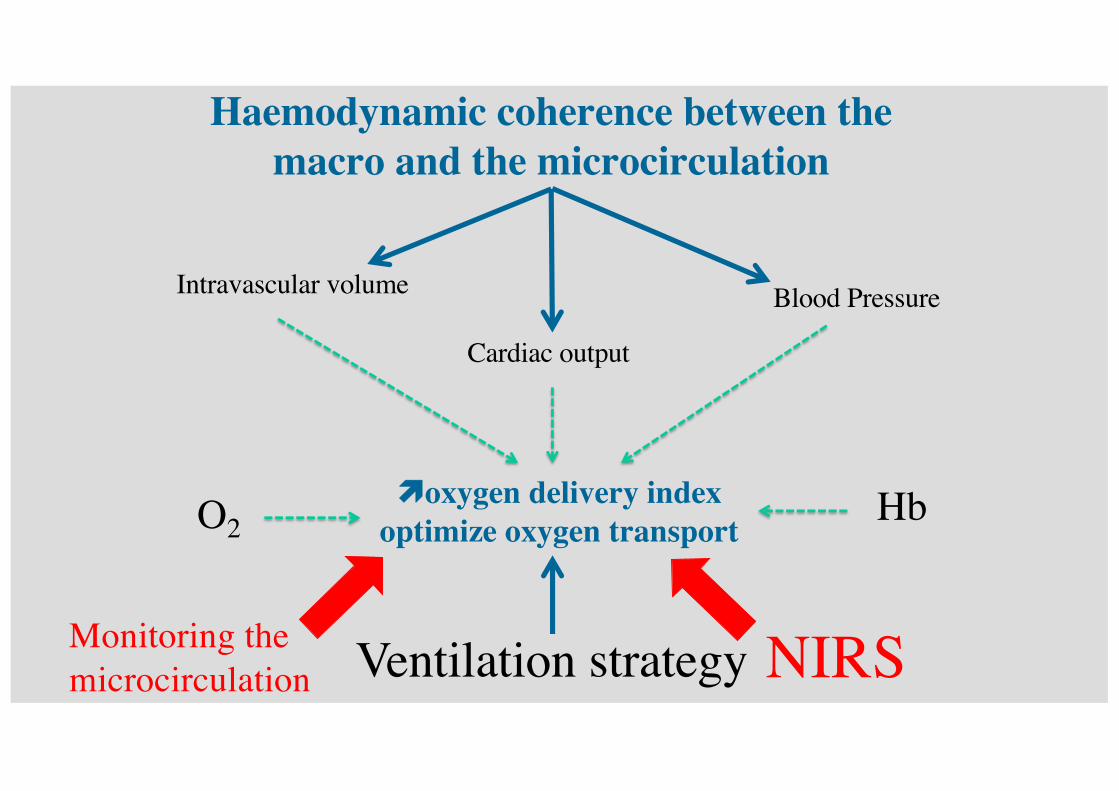
Haemodynamic coherence between the macro and the microcirculation
Blood Pressure
Cardiac output
Intravascular volume
!oxygen delivery indexoptimize oxygen transport O2 Hb
NIRSMonitoring the microcirculation Ventilation strategy






















