Embed Size (px)
Citation preview

PRENATAL DIAGNOSISPrenat Diagn 2002; 22: 1153–1162.Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pd.503
Preimplantation genetic diagnosis using FISH for carriers ofRobertsonian translocations: the Portuguese experience
Claudia Alves1*, Mario Sousa1,2,3, Joaquina Silva1,2 and Alberto Barros1,2
1Department of Genetics, Faculty of Medicine, University of Porto, Porto, Portugal2Centre for Reproductive Genetics3Lab Cell Biology, Institute of Biomedical Sciences Abel Salazar, University of Porto, Porto, Portugal
Preimplantation genetic diagnosis (PGD) is an alternative to prenatal diagnosis for couples at risk of transmittinggenetic disorders to their offspring. We present a fluorescence in situ hybridization (FISH) analysis ofembryos obtained after seven PGD cycles in six couples with Robertsonian translocations and male factorinfertility: 4 der(13;14), 1 der(14;21) and 1 der(15;21). Of 74 metaphase II (MII) injected oocytes, 61 (82.4%)fertilized normally and cleaved. Of these, 37/61 (60.7%) embryos were of high morphological quality with≥6 blastomeres. After biopsy of 44 embryos at day 3 of development, seven degenerated, seven arrestedin development and 30/44 (68.2%) evolved, of which 25/30 (83.3%) reached the morula/blastocyst stage.Analysis of biopsied blastomeres showed 23/44 (52.3%) of normal/balanced embryos, of which 15 (11 atthe morula/blastocyst stage) were transferred in six cycles. One term pregnancy was achieved, which endedby cesarean section at 37 weeks of gestation, giving birth to two healthy newborn. Analysis of 49 embryos(excluding 12 inconclusive cases) showed a predominance of alternate segregation (38/49, 77.6%) over adjacentsegregation (7/49, 14.3%), with one (2%) being a polyploid mosaic and three (6.1%) chaotic. Copyright 2002 John Wiley & Sons, Ltd.KEY WORDS: embryo biopsy; fluorescence in situ hybridization FISH; intracytoplasmic sperm injection (ICSI);preimplantation genetic diagnosis PGD; Robertsonian translocations
INTRODUCTION
Robertsonian translocations were first described byW. Robertson in 1916 and are among the most commonstructural rearrangements in humans, occurring with afrequency of 0.1% in the general population (Gard-ner and Sutherland, 1996; Gersen and Keagle, 1999).They represent the pericentric fusion between any oftwo acrocentric chromosomes (13, 14, 15, 21 and 22),with two non-homologous chromosomes being involvedin 95% of the cases. Robertsonian der(13;14) accountsfor almost 75% of these translocations and about 10%are associated with der(14;21).
Sperm analysis by FISH can be used to describe theproportion of abnormal gametes in male patients, thusproviding a basis for predicting the meiotic segregationpattern and the impact over sperm output and embryo-induced aneuploidy rates. In Robertsonian translocationmale carriers, FISH studies confirmed that the translo-cation is not a direct cause for male infertility, as only aslight increase in unbalanced sperm has been observed(Guichaoua et al., 1990; Rousseaux et al., 1995; Escud-ero et al., 2000; Honda et al., 2000; Frydman et al.,2001; Morel et al., 2001). On the contrary, high ratesof aneuploid sperm were shown in oligoasthenoter-atozoospermic (OAT) patients in relation to controls(Obasaju et al., 1999; Pang et al., 1999; Alves et al.,2002). Therefore, whilst studies have shown a tenfoldexcess of Robertsonian heterozygosity in men presentingwith oligozoospermia, there is a high frequency of male
*Correspondence to: Claudia Alves, Department of Genetics,Faculty of Medicine, University of Porto, Alameda Prof. HernaniMonteiro, 4200-319 Porto, Portugal. E-mail: [email protected]
infertility in the general population, most male Robertso-nian heterozygotes are fertile, and the same translocationcan occur in fertile and infertile members of the samefamily. Notwithstanding, sperm studies in Robertsoniantranslocation carriers might help to predict the risk ofembryo imbalance for each specific individual.
In accordance with these results, Robertsonian translo-cations do not predispose to malsegregation and/or lackof normal embryo development (Scriven et al., 2001). Infact, the significant chromosome aneuploidy and chaoticchromosome segregation observed in early humanembryos were demonstrated to occur spontaneously(Delhanty, 1997; Delhanty et al., 1997; Ruangvutilertet al., 2000), being additionally associated with embryofragmentation, embryo arrest and the presence of mult-inucleated blastomeres (Bongso et al., 1991; Lavergeet al., 1997), maternal age (Munne et al., 1995; Munneand Cohen, 1998; Marquez et al., 2000) and male infer-tility such as OAT (Obasaju et al., 1999).
PGD was developed as a treatment for couples at riskof transmitting genetic disorders to their progeny, bytransferring unaffected embryos into the uterus (Handy-side et al., 1990; Lissens and Sermon, 1997). Concern-ing Robertsonian translocations, PGD is a promising toolfor couples who do not wish to rely on the low riskassociated with the natural outcome, or have associatedinfertility or repeated spontaneous miscarriages (Ogilvieet al., 2001). For Robertsonian translocations, geneticdiagnosis is performed by FISH analysis of 1 to 2 blas-tomeres biopsied from embryos at the 6 to 8 cell stage(Conn et al., 1998; Munne et al., 1998a; Iwarsson et al.,2000; Fridstrom et al., 2001; Scriven et al., 2001) or bypolar body analysis in the case of female carriers (Munneet al., 1998b,c, 2000; Durban et al., 2001).
Copyright 2002 John Wiley & Sons, Ltd. Received: 31 July 2002Accepted: 23 September 2002

1154 C. ALVES ET AL.
In the present report, we present the Portugueseexperience of seven PGD cycles for Robertsoniantranslocations in which all male partners had spermio-genic defects.
MATERIALS AND METHODS
Patients and ethics
Six patients with Robertsonian translocations weretreated by ICSI and PGD and included the follow-ing karyotypes: cases A-C, 45,XY,der(13;14)(q10;q10);case D, 45,XX,der(13;14)(q10;q10); case E, 45,XY,der(15;21)(q10;q10); and case F, 45,XY,der(14;21)(q10;q10). All therapeutic procedures were in accor-dance with the National Ethical Committee guidelinesand informed consent was obtained from all patientsafter careful explanation of the treatment technique.
Couple A had three years of infertility, and themale partner was found to have oligoteratozoosper-mia (3.9 × 106/ml; 6% normal morphology, 28.8% pro-gressive motility). Couple B had three failed homolo-gous intra-uterine inseminations during seven years ofinfertility and the male partner had teratozoospermia(20 × 106/ml; 5% normal morphology, 47.3% progres-sive motility). Couple C had four years of infertility andthe male partner presented oligoasthenoteratozoospermia(12 × 106/ml; 2% normal morphology, 18.5% progres-sive motility). Couple D had five years of infertilityand the husband had teratozoospermia (20 × 106/ml, 5%normal morphology, 54.8% progressive motility). Forder(13;14), the total efficiency of the Lotus SpecificIdentifier (LSI) 13q14 and TelVysion 14q probe com-bination in the FISH work-up assay (200 lymphocytesfor each member of a couple) was 92.6%.
Couple E had two years of infertility and the malepartner was found to have oligoteratozoospermia (4.5 ×106/ml, 6% morphology, 29.2% progressive motility).The assay efficiency of the probes was 94.7% andenabled differentiation of the two products of alternatesegregation (between normal and balanced embryos),since for the CEP15p11.2 probe the der(15;21) exhibitedone signal that was half the size of the signal found onnormal chromosome 15.
Couple F had 10.5 years of infertility, the male partnerpresented severe oligoteratozoospermia (0.86 × 106/ml,0% normal morphology, 25.5% progressive motility)and the female partner had acquired uterine/cervicallesions. The efficiency of the LSI 21q22.13-22.2 andTel 14q probe combination was 93.5%.
Ovarian stimulation
Female patients were treated with a long GnRH ana-logue suppression protocol combining buserelin acetate(Suprefact: Hoechst, Frankfurt, Germany) with pFSH(Metrodin HP: Serono, Geneve, Switzerland) or rFSH(Gonal F: Serono; or Puregon: Organon, Oss, TheNetherlands). Ovulation was induced with hCG (Pregnyl:Organon; or Profasi: Serono). Oocytes were recovered
from large ovarian follicles by ultrasonically guided fol-licular aspiration, 35 h after hCG, using flush medium(Medicult, Copenhagen, Denmark) (Sousa et al., 2002).
Microinjection and embryo follow-up
Oocytes were cultured in in vitro fertilization (IVF)medium (Medicult) for 2 to 4 h after collection, incu-bated for 30 s in 80 U of hyaluronidase/SPM solution (InVitro Hyadase, Medicult), follicle cells removed in SPMwith denudation pipettes (0.134–0.145 mm; Swemed,Frolunda, Sweden), and cultured in IVF medium for 1 hat 37 ◦C with 5% CO2 in air. Spermiograms followed thecombined WHO and Kruger strict morphological crite-ria (WHO, 1999). After liquefaction (30 min at 37 ◦C),the seminal fluid was removed by centrifugation inSPM (2 × 10 min, 1500 rpm), the pellet washed throughSuprasperm (Medicult) gradient (80–55%) centrifuga-tion (20 min, 1500 rpm), washed as above, and layeredwith 100 µl SPM for swim-up (1 h at 37 ◦C with 5%CO2 in air). Microinjection of metaphase II oocytes wasas described (Sousa et al., 2002). Injected oocytes werecultured in BlastAssist System medium 1 (Medicult)at 37 ◦C with 5% CO2 in air, with normal fertiliza-tion being assessed 14 to 18 hours after injection. Aftertwo days of culture, embryos were transferred to Blas-tAssist System medium 2 (Medicult). Embryo qualitywas evaluated daily as described (Staessen et al., 1995).All patients had luteal supplementation with three timesdaily intravaginal administration of 200 mg natural-micronized progesterone (Utrogestan; Jaba, Berlin, Ger-many) after oocyte collection. Pregnancy was confirmedby a rise in serum β-hCG on two consecutive days, twoweeks after embryo transfer. A clinical pregnancy wasconfirmed by ultrasonography at seven weeks of gesta-tion. All couples agreed in advance to have a prenataldiagnosis, which would be performed by amniocentesisat 12 to 14 weeks of pregnancy.
Embryo biopsy
Cleaving embryos were biopsied three days afterICSI as described (Carvalho et al., 2001), using aninverted Nikon microscope equipped with Hoffmanoptics, thermo-controlled stage, and Narishige microma-nipulators (Nikon, Tokyo, Japan). Briefly, each embryowas incubated for 5 min in Ca2+-Mg2+-free medium(EB-10; Vitrolife, Goteborg, Sweden), the zona pellu-cida was opened by acidified Tyrode solution (Medicult)using a hatching micropipette (0.008–0.014 mm; Swe-Med), and 1 to 2 blastomeres were gently aspirated witha blastomere biopsy micropipette (0.040–0.050 mm;SweMed) while the embryo was kept in place by a hold-ing pipette (0.009–0.017 mm; SweMed).
Cytogenetic studies and FISH work-upassays for PGD
The karyotype analysis with G bands using trypsin andgiemsa (GTG) bands was performed on both members of
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

PGD FOR ROBERTSONIAN TRANSLOCATIONS 1155
the couple, according to conventional cytogenetic pro-cedures. For the FISH work-up studies, 200 interphaselymphocyte nuclei and 10 metaphase spreads of eachpartner were scored to examine the efficiency of probebinding and characterization of the derivative chromo-some. The interpretation of the FISH signals was per-formed according to published scoring criteria (Munneet al., 1998d).
Blastomere spreading
Single blastomeres were spread as described (Harperet al., 1994). Briefly, they were washed in IVF mediumand transferred to 2 µl of lysis solution (0.05% Tween20/0.01N HCl in embryo tested water) on poly-L-lysinecoated slides (Sigma). After nuclei isolation, the slideswere left to air-dry, washed for 5 min each in 0.1 Mphosphate suffered saline (PBS), pH 7.2, and in water,and dehydrated in an ethanol series (70, 2 × 96, 2 ×100%, 15 s each). The slides were then incubated for20 min at 37 ◦C in 100 µg pepsin/ml PBS (Pepsin A,1 : 10 000; Sigma), rinsed in water and PBS (15 s each),fixed at 4 ◦C for 10 min in 1% paraformaldehyde/PBS(37% formalin, Sigma), rinsed in PBS and water, anddehydrated as above.
Probe combination for PGD and FISHprocedure
For cases A to D, the following probe mixture wasused: LSI 13q14 (Spectrum Green; Vysis Inc., Down-ers Grove, IL, USA) and TelVysion 14q (SpectrumOrange; Vysis). For case E, the probes used were CEP15(D15Z1/15p11.2, Spectrum Green; Vysis) and LSI21q22.13-22.2 (Spectrum Orange; Vysis). For case F, theprobes were 14q subtelomeric probe (Green; Appligene,Oncor Lifescreen) and LSI 21q22.13-22.2 (SpectrumOrange; Vysis). The probes were prepared according tothe manufacturer’s instructions. Ten microlitres of eachmixture was applied on the slides under a coverslip,codenatured at 75 ◦C for 3 min and left to hybridize forapproximately 16 h at 37 ◦C, in a moist chamber. Post-hybridization washes (Harper et al., 1994) consisted of60% formamide (Fluka Chemika, Switzerland)/2× stan-dard saline citrate (SSC)/0.05% Tween 20, at 42 ◦C for5 min, 2 × SSC for 5 min at 42 ◦C and 4 × SSC/0.05%Tween 20 for 5 min at room temperature. The slideswere then rinsed in water and PBS, dehydrated, airdried and mounted in 10 µl Vectashield (Vector) antifademedium containing 1.5 mg/ml 4,6-diamino-2-phenyl-indole (DAPI) to stain the nuclei (Vector Laboratories,Burlingame, USA). Images were recorded using a Nikon(Eclipse, E-400) epifluorescence microscope fitted with acool charged device (CCD) camera and appropriate soft-ware (Cytovision Ultra, Applied Imaging International,Sunderland, UK).
Embryo classification
Following pre-established criteria (Munne et al., 1998d),the biopsied cell(s) were classified as normal/balanced
when two clear signals for each chromosome in theprobe combination could be observed. The embryo wasconsidered transferable if all biopsied blastomeres werenormal/balanced. Whenever at least one of the biopsiedblastomeres showed an abnormal or inconclusive signalpattern, embryos were not considered suitable for trans-fer. Biopsied embryos that were not selected for transferwere prepared for FISH analysis at the day of embryotransfer (day 4 or 5). Non-biopsied embryos were pre-pared for FISH analysis after embryo biopsy (day 3 or4). Whole embryos were spread using the HCl/Tweenmethod as mentioned above (Harper et al., 1994).
For FISH analysis of whole embryos (Scriven et al.,2001), they were classified as: (1) normal/balanced, ifthe cells had two signals for each chromosome tested,taking into account the FISH error rates (e.g. with aFISH assay efficiency of 92%, an embryo would beclassified as normal/balanced if 1 out of 12 nucleihad an abnormal signal pattern), (2) unbalanced, ifnuclei had an altered and uniform signal pattern, (3)if there were ≥2 different cell lines, based on ≥2nuclei for each cell line, the embryos were classifiedas: (i) normal/balanced mosaics, when the major cellline had two signals for each chromosome studied;(ii) unbalanced mosaics, when the major cell line hadan abnormal complement; in case of morulae/blastocystswith a high number of nuclei, unbalanced mosaics wereclassed when the proportion of the abnormal nuclei wassignificantly different from that of the control slide inthe same FISH experiment (Ruangvutilert et al., 2000);or (iii) polyploid mosaics, when the major cell line waspolyploid, (4) chaotic, when the signal pattern variedrandomly from nuclei to nuclei, and (5) inconclusive,when there were any doubts in the interpretation ofthe FISH results (overlapping signals, signals closetogether), remnants of cytoplasm covering the nucleithat became difficult or unable to observe, and/or whenthe embryo was degenerated and few/none nuclei werepresent after spreading.
RESULTS
Six couples underwent seven PGD cycles for Robertso-nian translocations (cases A–F). The mean female agewas 29.8 (range 26–31) and the mean male age was 32.3(range 28–38) years old. In total, 87 cumulus-oocytecomplexes were retrieved of which 7 were immature, 6were atretic and 74 were at the MII stage (mean 10.6;range 5–19). After ICSI, three oocytes degenerated, twowere activated (0PN/2PB), eight were abnormally fer-tilized (7x1PN/2PB; 1x3PN/2PB) and 61/74 (82.4%)were normally fertilized (2PN/2PB). All 2PN zygotescleaved, giving a mean number of 8.7 (range 5–12)embryos per cycle. At day 3 of development, 50/61(82%) embryos were of grade A/B (0–25% fragments),with 37/61 (60.7%) being of grade A/B and having ≥6cells (Tables 1 and 2).
At day 3 of development, 44/61 (72.1%) embryoswere biopsied and analysed with probes specific for eachtranslocation case. Of these, 37/44 (84.1%) embryos
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

1156 C. ALVES ET AL.
Table 1—Embryo evolution and FISH analysis on PGD cycles for der(13;14) Robertsonian translocations
Embryo gradeFISH analysis
Case/cycle before/after biopsy 1st blastomere 2nd blastomere Embryo follow-up
A1 7B-Bl Normal/balanced Embryo transfer45,XY 9B-Bl Normal/balanced Embryo transferder(13;14) 7B-Bl Normal/balanced Embryo transfer
8B-Mo-14n Normal/balanced Normal/balanced6B-Ar-9n Normal/balanced Normal/balanced7B-Ar-9n Unbalanced (−13) Normal/balanced mosaic
(44.4% diploid nuclei)4D, 2(−14), 2 tetraP, 1(−13)
10B-Dg Unbalanced tetraP (+13) Inconclusiveb
8B-Mo Unbalanced (−13) Inconclusiveb
5B-Ar Haploid Inconclusiveb
5B-Ar Normal/balanced Inconclusiveb
7C-Dg Tetraploid Inconclusiveb
4D-4n Polyploid mosaic (50% nuclei):2 heptaP, 1D, 1H
B1d 8B-Mo Normal/balanced Normal/balanced Embryo transfer45,XY 8B-Bl Normal/balanced Normal/balanced Embryo transferder(13;14) 7B-Bl Normal/balanced Normal/balanced Embryo transfer
8B-Bl Normal/balanced Normal/balanced Embryo transfer7B-Bl Normal/balanced Normal/balanced Inconclusiveb
8B-Dg-55n Normal/balanced Normal/balanced Normal/balanced mosaic(78.2% diploid nuclei) 43D,3P, 3 tetraP, 1 nonaP, 2(−14),1(+13)
12B-Dg-31n Unbalanced (−14) 2 Unbalanced (+13)a Normal/balanced mosaic(80.6% diploid nuclei) 25D,4(+13), 2(−14)
6A-Mo-45n Unbalanced (−14) Normal/balanced mosaic(75.6% diploid nuclei) 34D,5(+13), 2(−14), 3 tetraP, 1H
7B-Bl-74n Unbalanced (+13) Unbalanced (+13) mosaic(81.1% nuclei) 60(+13), 5P, 4tetraP, 4D, 1(4 × 13)
5B-Mo-15n Unbalanced (−14) Unbalanced (−14)
C1 9B-11B Normal/balanced Embryo transfer45,XY 7B-10B Normal/balanced Embryo transferder(13;14) 7B-9B 2 Normal/balanceda Embryo transfer
7B-Dg Normal/balanced Inconclusivec
8B-Ar Haploid Inconclusivec
8B-8B-14n Haploid Normal/balanced Normal/balanced mosaic(71.4% diploid nuclei) 10D,2H, 1 tetraP, 1(−14)
7B-8B-6n Unbalanced (−14) Unbalanced (−14) mosaic(50% nuclei) 3(−14), 1(−13),1(4 × 13), 1H
5B-7n Unbalanced (+14) mosaic(57.1% nuclei): 4(+14), 2D,1H
4C-5n Normal/balanced mosaic (60%diploid nuclei): 3D, 2H
C2 8B-Bl Normal/balanced 2 Normal/balanceda Embryo transfer45,XY der(13;14) 8B-Bl-22n Unbalanced (−14) No nucleus found Normal/balanced mosaic (50%
diploid nuclei)11D, 8(−14), 2(+13), 1H
8B-Bl-25n Normal/balanced Haploid Normal/balanced mosaic (60%diploid nuclei) 15D, 4H,1(4 × 13), 2P, 2 triP, 1 tetraP
6B-Mo-30n No nucleus found Normal/balanced mosaic(73.3% diploid nuclei) 22D,5(−14), 1(−13), 2 tetraP
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.
PGD FOR ROBERTSONIAN TRANSLOCATIONS 1157
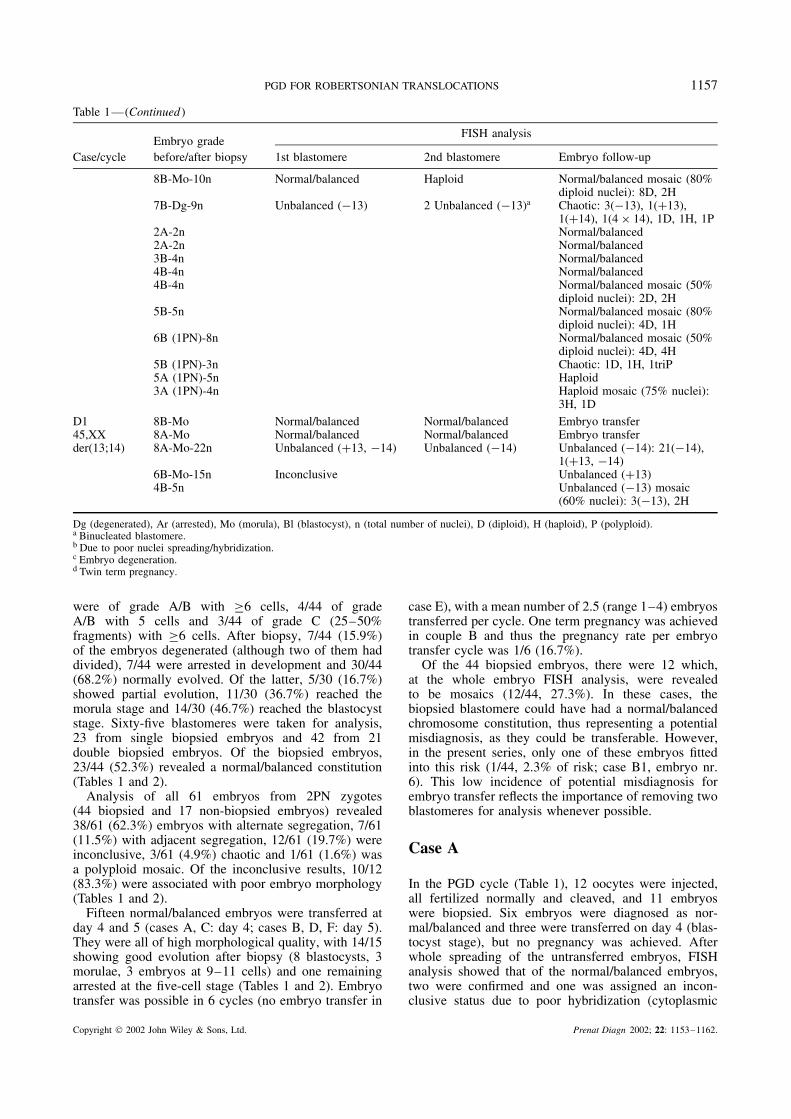
Table 1—(Continued )
Embryo gradeFISH analysis
Case/cycle before/after biopsy 1st blastomere 2nd blastomere Embryo follow-up
8B-Mo-10n Normal/balanced Haploid Normal/balanced mosaic (80%diploid nuclei): 8D, 2H
7B-Dg-9n Unbalanced (−13) 2 Unbalanced (−13)a Chaotic: 3(−13), 1(+13),1(+14), 1(4 × 14), 1D, 1H, 1P
2A-2n Normal/balanced2A-2n Normal/balanced3B-4n Normal/balanced4B-4n Normal/balanced4B-4n Normal/balanced mosaic (50%
diploid nuclei): 2D, 2H5B-5n Normal/balanced mosaic (80%
diploid nuclei): 4D, 1H6B (1PN)-8n Normal/balanced mosaic (50%
diploid nuclei): 4D, 4H5B (1PN)-3n Chaotic: 1D, 1H, 1triP5A (1PN)-5n Haploid3A (1PN)-4n Haploid mosaic (75% nuclei):
3H, 1D
D1 8B-Mo Normal/balanced Normal/balanced Embryo transfer45,XX 8A-Mo Normal/balanced Normal/balanced Embryo transferder(13;14) 8A-Mo-22n Unbalanced (+13, −14) Unbalanced (−14) Unbalanced (−14): 21(−14),
1(+13, −14)6B-Mo-15n Inconclusive Unbalanced (+13)4B-5n Unbalanced (−13) mosaic
(60% nuclei): 3(−13), 2H
Dg (degenerated), Ar (arrested), Mo (morula), Bl (blastocyst), n (total number of nuclei), D (diploid), H (haploid), P (polyploid).a Binucleated blastomere.b Due to poor nuclei spreading/hybridization.c Embryo degeneration.d Twin term pregnancy.
were of grade A/B with ≥6 cells, 4/44 of gradeA/B with 5 cells and 3/44 of grade C (25–50%fragments) with ≥6 cells. After biopsy, 7/44 (15.9%)of the embryos degenerated (although two of them haddivided), 7/44 were arrested in development and 30/44(68.2%) normally evolved. Of the latter, 5/30 (16.7%)showed partial evolution, 11/30 (36.7%) reached themorula stage and 14/30 (46.7%) reached the blastocyststage. Sixty-five blastomeres were taken for analysis,23 from single biopsied embryos and 42 from 21double biopsied embryos. Of the biopsied embryos,23/44 (52.3%) revealed a normal/balanced constitution(Tables 1 and 2).
Analysis of all 61 embryos from 2PN zygotes(44 biopsied and 17 non-biopsied embryos) revealed38/61 (62.3%) embryos with alternate segregation, 7/61(11.5%) with adjacent segregation, 12/61 (19.7%) wereinconclusive, 3/61 (4.9%) chaotic and 1/61 (1.6%) wasa polyploid mosaic. Of the inconclusive results, 10/12(83.3%) were associated with poor embryo morphology(Tables 1 and 2).
Fifteen normal/balanced embryos were transferred atday 4 and 5 (cases A, C: day 4; cases B, D, F: day 5).They were all of high morphological quality, with 14/15showing good evolution after biopsy (8 blastocysts, 3morulae, 3 embryos at 9–11 cells) and one remainingarrested at the five-cell stage (Tables 1 and 2). Embryotransfer was possible in 6 cycles (no embryo transfer in
case E), with a mean number of 2.5 (range 1–4) embryostransferred per cycle. One term pregnancy was achievedin couple B and thus the pregnancy rate per embryotransfer cycle was 1/6 (16.7%).
Of the 44 biopsied embryos, there were 12 which,at the whole embryo FISH analysis, were revealedto be mosaics (12/44, 27.3%). In these cases, thebiopsied blastomere could have had a normal/balancedchromosome constitution, thus representing a potentialmisdiagnosis, as they could be transferable. However,in the present series, only one of these embryos fittedinto this risk (1/44, 2.3% of risk; case B1, embryo nr.6). This low incidence of potential misdiagnosis forembryo transfer reflects the importance of removing twoblastomeres for analysis whenever possible.
Case A
In the PGD cycle (Table 1), 12 oocytes were injected,all fertilized normally and cleaved, and 11 embryoswere biopsied. Six embryos were diagnosed as nor-mal/balanced and three were transferred on day 4 (blas-tocyst stage), but no pregnancy was achieved. Afterwhole spreading of the untransferred embryos, FISHanalysis showed that of the normal/balanced embryos,two were confirmed and one was assigned an incon-clusive status due to poor hybridization (cytoplasmic
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

1158 C. ALVES ET AL.
Table 2—Embryo evolution and FISH analysis on PGD cycles for der(15;21) and der(14;21) Robertsonian translocations
Embryo gradeFISH analysis
Case/cycle before/after biopsy 1st blastomere 2nd blastomere Embryo follow-up
E1 8C-Bl-21n Balanced 2 Balanceda Balanced45,XY 6C-Ar Unbalanced (+21) No nucleus found Inconclusiveb
der(15;21) 5C Inconclusiveb
5C Inconclusiveb
4C Inconclusiveb
3D-2n Normal3D-4n Chaotic: 1 tetraP, 1H, 1(-21),
1(+21)3D-7n Chaotic: 1H, 1(4 × 21),
1(+21), 1P, 2(0 × 13, −21),1(0 × 13)
4B (1PN) Inconclusiveb
2C (3PN)-2n Triploid
F1 7B-Ar Normal/balanced Normal/balanced Embryo transfer45,XY 5B-Bl 2 Normal/balanceda Embryo transferder(14;21) 7B-Dg-5n Normal/balanced Normal/balanced Normal/balanced
7B-Bl-47n 2 Normal/balanceda Inconclusive Normal/balanced mosaic(59.6% diploid nuclei) 28D, 8tetraP, 1 triP, 6(−14), 3H,1(4 × 14)
4B-7n Normal/balanced mosaic(42.9% diploid nuclei) 3D, 2P,1 heptaP, 1(−21)
3D (0PN)-3n Polyploid mosaic (66.7%nuclei): 2P, 1D
Dg (degenerated), Ar (arrested), Mo (morula), Bl (blastocyst), n (total number of nuclei), D (diploid), H (haploid), P (polyploid).a Binucleated blastomere.b Due to nuclei fragmentation.
debris covering most of the nuclei). Of the five embryos,which at biopsy were considered not suitable for trans-fer, four were inconclusive and one with monosomy 13was found to be a normal/balanced mosaic. There wasonly one embryo that was not biopsied, and this wasshown to be a polyploid mosaic.
Case B
In the PGD cycle (Table 1) 10 oocytes were injected,all fertilized normally and cleaved, and 10 embryoswere biopsied. Six embryos were normal/balanced, ofwhich four were transferred on day 5 (1 morula and 3blastocysts). A dizygotic twin pregnancy was achieved,but the couple later refused prenatal diagnosis to confirmthe PGD result. Ultrasonography examination showedthat both fetuses were healthy and developing well.One male (2610 Kg, 45 cm) and one female (2350 Kg,45 cm) healthy baby was born by cesarean sectionat 37 weeks of gestation (4th August 2002). Analysisof the untransferred embryos showed that of the twonormal/balanced embryos, one was a balanced mosaicand the other was inconclusive; of the two unbalanced(−14) embryos, one confirmed to have monosomy 14and the other was a balanced mosaic; the embryo withtrisomy 13 was an unbalanced (+13) mosaic; and theembryo with discordant biopsied cells, (−14) and (+13),was a balanced mosaic.
Case C
In the first PGD cycle, 10 oocytes were injected, 9fertilized normally and cleaved, and 7 embryos werebiopsied (Table 1). Of these, four were normal/balancedwith three having been transferred on day 4 (at the9–11 cell stage), but no pregnancy was achieved. Theremainder biopsied embryos were spread for follow-up: one normal/balanced and one haploid gave noconclusive diagnosis; one with monosomy 14 was shownto be an unbalanced (−14) mosaic; and one had ahaploid blastomere and one had a normal/balancedblastomere, which was then shown to be a balancedmosaic. Of the two non-biopsied embryos, one was abalanced mosaic and the other was an unbalanced (+14)mosaic.
In the second PGD cycle (Table 1), 19 oocytes wereinjected, 12 normally fertilized and cleaved, and 6embryos were biopsied (Table 1). Of these, only onewas normal/balanced and was transferred on day 4(blastocyst), but no pregnancy was achieved. Of theremainder five biopsied embryos, one (−13) showedto be chaotic; all the other four were normal/balancedmosaics and included at biopsy 1 (−14), two mosaics(one normal/balanced and one haploid blastomere) andone with no diagnosis (no nucleus found). Six embryosarrested at the two- to five-cell stage were not biop-sied. Of these, four were normal/balanced and two werebalanced mosaics. Four embryos resulting from abnor-mally fertilized zygotes (1PN) were shown to be one
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

PGD FOR ROBERTSONIAN TRANSLOCATIONS 1159
balanced mosaic, one chaotic, one haploid mosaic andone haploid.
Case D
In the PGD cycle (Table 1), five oocytes were injected,all fertilized normally and cleaved, and four embryoswere biopsied. Of these, two were normal/balanced andwere transferred on the fifth day (morulae), but nopregnancy was established. Of the other two biopsiedembryos, one with monosomy 14/trisomy 13 was con-firmed to have monosomy 14 on follow-up, whereasthe other was inconclusive and showed to be unbal-anced (+13). The non-biopsied embryo was consideredan unbalanced (−13) mosaic.
Case E
In the PGD cycle (Table 2; Figure 1), 11 oocyteswere injected, 8 normally fertilized and cleaved, and2 embryos were biopsied. Of these, one was balanced(with the derivative chromosome) and one was withtranslocation trisomy 21. The balanced embryo evolvedto a blastocyst with poor morphological quality and
was not transferred. Whole embryo analysis then con-firmed the balanced embryo, whereas embryo (+21)gave inconclusive results because of nuclei fragmenta-tion. Of the six non-biopsied embryos, three were incon-clusive (due to nuclear fragmentation), two were chaoticand one was normal. There were two embryos that werederived from abnormal zygotes, one (1PN) being incon-clusive and the other (3PN,3PB) being triploid with thederivative chromosome.
Case F
In the PGD cycle (Table 2), seven oocytes were injected,five fertilized normally and cleaved, and four embryoswere biopsied. Of these, three were normal/balancedand two were transferred on day 5 of development(one arrested, one blastocyst), but no pregnancy wasachieved. The third normal/balanced embryo was con-firmed on follow-up analysis. The fourth biopsiedembryo (one normal/balanced and one inconclusive blas-tomere) was found to be a normal/balanced mosaic. Thenon-biopsied embryo was considered a normal/balancedmosaic, whereas one embryo from an abnormal (0PN)zygote was shown to be a polyploid mosaic.
A B
F G H I
C D E
ba
Figure 1—FISH results obtained in embryos from case E, with der(15;21). Note that the signal on the normal chromosome 15 is twice the size ofthe der15 (green; arrows); the specific probe for chromosome 21 is labelled in red. Inserts a and b show the probe hybridization in a lymphocytemetaphase from the patient. A. Nucleus from a blastomere with a normal complement, B. Nucleus from a biopsied blastomere (embryo 8C-Bl),showing a balanced complement, C. Nucleus from a biopsied blastomere (embryo 6C-Ar), showing an unbalanced (+21) complement, withpresence of the derivative chromosome. D–I. Nuclei from a chaotic embryo. Arrow indicates the derivative chromosome
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

1160 C. ALVES ET AL.
DISCUSSION
In seven PGD cycles for six couples with Robertso-nian translocations, the fertilization rate was 82.4% andall 2PN zygotes cleaved, with 60.7% of the embryosbeing of grade A/B with ≥6 blastomeres. After biopsyof 44 embryos (84.1% of grade A/B with ≥6 cells),30/44 (68.2%) normally evolved and 25/30 (83.3%)reached the morula/blastocyst stage. Of the biopsiedembryos, 23/44 (52.3%) revealed a normal/balancedconstitution, of which 15 were transferred (73.3% atthe morula/blastocyst stage) in 6 cycles. One termtwin pregnancy was achieved. The pregnancy rate perembryo transfer cycle was thus 1/6 (16.7%), which isapparently different to the clinical pregnancy rate perembryo transfer of 11/38 (28.9%) obtained in 51 totalcycles for Robertsonian translocations (ESHRE PGDConsortium Steering Committee, May 2001, 2002). Thelow pregnancy rate presented here can be attributedto the low number of cycles performed. Alternatively,it could be related to the poor sperm morphologyrate that was the main reason for couple infertil-ity. In fact, a strong correlation has been shown toexist between spermiogram abnormalities and aneu-ploidy rates in sperm and embryos (Obasaju et al., 1999;Pang et al., 1999).
Of the 61 embryos from 2PN zygotes that wereanalysed (including 44 biopsied embryos and 17 non-biopsied embryos), 24 were normal/balanced, 14 werenormal/balanced mosaics, 3 were unbalanced, 4 wereunbalanced mosaics, 3 were chaotic, 1 was a polyploidmosaic and 12 were inconclusive. Excluding 12 incon-clusive cases, the 49 embryos showed a predominanceof alternate segregation (24/49, 49%) over adjacent seg-regation (3/49, 6.1%), and the percentage of mosaicismwas 36.7% (18/49), with 28.6% (14/49) normal/balancedmosaics and 8.2% (4/49) unbalanced mosaics. However,most authors suggest that in mosaic embryos the majorcell line defines the most probable mode of chromo-some segregation. Therefore, if one includes mosaics,alternate segregation occurred in 77.6% (38/49) andadjacent segregation in 14.3% (7/49) of the embryos.The present results are thus in accordance with previouspublished PGD series on Robertsonian translocations,which showed a predominance of the alternate segrega-tion pattern over adjacent segregation (Conn et al., 1998;Munne et al., 1998a; Escudero et al., 2000; Iwarssonet al., 2000; Scriven et al., 2001) (Table 3).
FISH analysis of sperm in Robertsonian transloca-tion carriers showed a variable (3–36%) risk for unbal-anced gamete formation, although in most studies themean risk was about 10% (Guichaoua et al., 1990;Rousseaux et al., 1995; Escudero et al., 2000; Honda
Table 3—Review of FISH analysis on embryo-PGD cycles for Robertsonian translocations
Segregation pattern (%)
Translocation Embryos (N) Alternate Adjacent Unknown Inconclusive References
der(13q;14q) 27 4 5 14 4 Conn et al., 199832 15 6 9 2 Escudero et al., 200031 21 4 6 — Iwarsson et al., 200020 14 3 1 2 Scriven et al., 200148 31 7 2 8 Present study
Total 158 85/142 (59.9) 25/142 (17.6) 32 16
der(14q;21q) 14 10 2 1 1 Scriven et al., 20015 4 — 1 — Present study
Total 19 14/18 (77.8) 2/18 (11) 2 1
der(13q;21q) 18 2/17 (11.8) 6/17 (35.3) 9 1 Conn et al., 1998der(14q;15q) 11 6 3 2 — Munne et al., 1998a
4 2 — 2 — Iwarsson et al., 2000Total 15 8/15 (53.3) 3/15 (20) 4 0
der(15q;21q) 8 2/4 (50) — 2 4 Present studyTotal 218 111/196 (56.6) 36/196 (18.4) 49 22
Table 4—Review of FISH analysis on polar body-PGD cycles for Robertsonian translocations
Segregation pattern (%)
Translocation Embryos (N) Alternate Adjacent Unknown Inconclusive References
der(13q;14q) 77 47 21 9 — Munne et al., 200020 5 7 — 8 Durban et al., 2001
Total 97 52/89 (58.4) 28/89 (31.5) 9 8
der(14q;21q) 101 50 35 16 — Munne et al., 200013 3 4 — 6 Durban et al., 2001
Total 114 53/108 (49.1) 39/108 (36.1) 16 6
Total 211 105/197 (53.3) 67/197 (34) 25 14
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

PGD FOR ROBERTSONIAN TRANSLOCATIONS 1161
et al., 2000; Frydman et al., 2001; Morel et al., 2001).These results thus suggest that the possible impact ofabnormal sperm on embryo chromosome imbalance isnot greatly increased (Gardner and Sutherland, 1996).On the contrary, FISH polar body analysis indicates asignificant higher risk (32–36%) of unbalanced oocytesin female Robertsonian translocation carriers (Munneet al., 1998b,c, 2000; Durban et al., 2001) (Table 4).However, for Robertsonian translocations, PGD analysisof the embryos demonstrated that even if the transloca-tion does influence the embryo chromosome constitu-tion, other factors seem responsible for the large rateof aneuploidies found in early human embryos (Connet al., 1998; Munne et al., 1998a; Iwarsson et al., 2000;Friedstrom et al., 2001; Scriven et al., 2001), such asthe absence of cell cycle check-points in the earlyembryo mitotic divisions (Delhanty et al., 1997), abnor-mal embryo morphology (Laverge et al., 1997), maternalage (Marquez et al., 2000) and male infertility (Obasajuet al., 1999).
Previous reports of PGD cycles from Robertso-nian translocation carriers also revealed extremely highrates of chromosome mosaicism/chaos, ranging from45 to 63% (Munne et al., 1998a; Conn et al., 1998;Iwarsson et al., 2000). In the present study, and afterexcluding 12/61 inconclusive cases, 49/61 (biopsiedand non-biopsied) embryos enabled a FISH diagnosisthat revealed chaotic cleavage divisions in 3/49 (6.1%)cases, balanced/unbalanced mosaicism in 18/49 (36.7%)embryos and polyploid mosaicism in 1/49 (2%) cases,which gives a total rate of 22/49 (44.9%) for chromo-some mosaicism/chaos, that is similar to the reportedvalues. Nevertheless, it is recognized that some patientsmight be more prone to produce abnormal embryos (Del-hanty et al., 1997; Munne and Cohen, 1998; Marquezet al., 2000), which could also be explained by differ-ences in the stimulation protocols and embryo cultureconditions (Munne et al., 1997).
In this study, we present a PGD series on 48 embryosfor der(13;14). Excluding 8 embryos with an incon-clusive diagnosis, a high proportion (7/40, 17.5%) ofembryos resulted from adjacent segregation, which isalso in accordance to previously published data on PGDcycles for der(13;14) translocations (Conn et al., 1998;Escudero et al., 2000; Iwarsson et al., 2000; Scrivenet al., 2001)(Table 3). Contrary to prenatal diagnosis(PND), calculated risks of <0.5% for male and of 10to 15% for female der(D;21) carriers of Robertsoniantranslocations (Gardner and Sutherland, 1996), mostFISH studies demonstrated a higher risk (7–16%) ofunbalanced sperm (Guichaoua et al., 1990; Rousseauxet al., 1995; Escudero et al., 2000; Honda et al., 2000;Frydman et al., 2001; Morel et al., 2001) and of unbal-anced oocytes (32–36%) (Munne et al., 2000; Durbanet al., 2001) (Table 4). In our study of der(13;14) cases,only 2/40 (5%) of the embryos were shown to have tri-somy 13 (both achieving the morula/blastocyst stage).However, one embryo was from a male carrier (threepatients, four cycles), which gives a risk of 1/35 (2.9%),whereas the other embryo was from a female carrier,thus only suggesting an individual relative higher riskof 1/5 (20%). Our values thus seem to corroborate the
low estimated risks at PND (Daniel et al., 1989; Gard-ner and Sutherland, 1996) and of miscarriage (Harriset al., 1979). Differences of PND to PGD results residein the different developmental stages studied, as most ofthe abnormal embryos have poor developmental capac-ity and probably do not proceed beyond implantation.In fact, most types of chromosome imbalance observedat PGD for Robertsonian translocations are never seenat amniocentesis, which comprise all the monosomiesand trisomies, with the exception of trisomy 13 (Patausyndrome) and trisomy 21 (Down syndrome).
We describe here a case of PGD in which the malepartner had a der(15;21) translocation. One PGD cycle toa female partner with a der(15;21) translocation has beenlisted in the ESHRE PGD Consortium, data collection IIIof May 2001 (2002). PGD probe sets ought to be testedon lymphocytes from both reproductive partners, assome of them cross-hybridize with other chromosomes.This applies to the D15Z1 probe, which cross-hybridizeswith one chromosome 14 in a significant proportion ofindividuals, rendering it unsuitable for interphase FISH.In our particular case, there was no cross-hybridizationand the size of the signals enabled us to differentiatebetween the normal and balanced forms of the segrega-tion. Using the general approach in FISH analysis withcommercial probes, this is first reported here for Robert-sonian translocations. For this couple, all the embryosobtained were of poor morphological quality, with threeinconclusive (due to extreme nuclei fragmentation), twochaotic, one normal, one balanced and one unbalanced(although with inconclusive results at whole embryospreading). As the derivative was found in two embryos,the rate of segregation (with exclusion of the three incon-clusive cases) was calculated to be about 2/5 (40%).Whether cell and nuclear fragmentation are related toeach other is still not clear, although such type of asso-ciation is supported by the present results as well asby other studies that suggest a relationship between thedegree of fragmentation and chromosome abnormalities,especially mosaicism (Bongso et al., 1991; Munne et al.,1995; Delhanty et al., 1997; Laverge et al., 1997; Munneand Cohen, 1998). Although an association between thistranslocation and the degree of fragmentation cannot beruled out, the high rate of good quality embryos pro-duced by patient F with a der(14;21) translocation doesnot favour this latter hypothesis.
In conclusion, we present the Portuguese experienceon embryo-PGD cycles for Robertsonian translocations,with the larger series of embryos analysed for der(13;14)and a novel PGD application to a male der(15;21)case. In accordance with previous published PGD series,the present results show a predominance of alternatesegregation over adjacent segregation in embryos, butconfirm the low risk of viable unbalanced segregationin Robertsonian translocations as observed at prenataldiagnosis.
ACKNOWLEDGEMENTS
We would like to thank the clinical participation ofDrs. Cristiano Oliveira and Jose Teixeira da Silva, and
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.

1162 C. ALVES ET AL.
of Profs. Nuno Montenegro and Jorge Beires, as alsothe IVF laboratorial assistance of Dr. Paulo Viana.This work was partially supported by FCT (43462/01,36363/99, 35231/99, 42812/01; UMIB).
REFERENCES
Alves C, Carvalho F, Cremades N, Sousa M, Barros A. 2002. Unique(Y;13) translocation in a male with oligozoospermia: cytogeneticand molecular studies. Eur J Hum Genet 10: 467–474.
Bongso A, Soon-Chye Ng, Lim J, Chui-Yee F, Ratnam S. 1991.Preimplantation genetics: chromosomes of fragmented humanembryos. Fertil Steril 56: 66–70.
Carvalho F, Sousa M, Fernandes S, Silva J, Saraiva MJ, Barros A.2001. Preimplantation genetic diagnosis for familial amyloidoticpolyneuropathy (FAP). Prenat Diagn 21: 1093–1099.
Conn CM, Harper JC, Winston RM, Delhanty JD. 1998. Infertilecouples with Robertsonian translocations: preimplantation geneticdiagnosis of embryos reveals chaotic cleavage divisions. Hum Genet102: 117–123.
Daniel A, Hook EB, Wulf G. 1989. Risk of unbalanced progeny atamniocentesis to carriers of chromosome rearrangements: data fromUnited States and Canadian laboratories. Am J Med Genet 31:14–53.
Delhanty JD. 1997. Chromosome analysis by FISH in humanpreimplantation genetics. Hum Reprod 12 Natl Suppl JBFS 2:153–155.
Delhanty JD, Harper JC, Ao A, Handyside AH, Winston RM. 1997.Multicolour FISH detects chromosomal mosaicism and chaoticdivision in normal preimplantation embryos from fertile patients.Hum Genet 99: 755–760.
Durban M, Benet J, Boada M, et al. 2001. PGD in female carriers ofbalanced Robertsonian translocations and reciprocal translocationsby first polar body analysis. Hum Reprod Update 7: 591–602.
Escudero T, Lee M, Carrel D, Blanco J, Munne S. 2000. Analysisof chromosome abnormalities in sperm and embryos from two45,XY,t(13;14)(q10;q10) carriers. Prenat Diagn 20: 599–602.
ESHRE PGD Consortium Steering Committee. 2002. ESHREpreimplantation genetic diagnosis consortium: data collection III(May 2001). Hum Reprod 17: 233–246.
Fridstrom M, Ahrlund-Richter L, Iwarsson E, et al. 2001. Clinicaloutcome of treatment cycles using preimplantation genetic diagnosisfor structural chromosome abnormalities. Prenat Diagn 21:781–787.
Frydman N, Romana S, Le Lorc’h M, Vekemans M, Frydman R,Tachdjian G. 2001. Assisting reproduction of infertile men carryinga Robertsonian translocation. Hum Reprod 16: 2274–2277.
Gardner RJM, Sutherland JR. 1996. Chromosome Abnormalities andGenetic Counselling (2nd edn), Oxford University Press: Oxford,UK.
Gersen SL, Keagle MB (eds). 1999. Structural chromosome rear-rangements. In The Principles of Clinical Cytogenetics. HumanaPress: Totowa, N.J.
Guichaoua MR, Quack B, Speed RM, Noel B, Chandley AC, LucianiJM. 1990. Infertility in human males with autosomal translocations:meiotic study of a 14;22 Robertsonian translocation. Hum Genet 86:162–166.
Handyside AH, Kontogianni EH, Hardy K, Winston RM. 1990.Pregnancies from biopsied human preimplantation embryos sexedby Y-specific DNA amplification. Nature 344: 768–770.
Harper JC, Coonen E, Ramaekers FCS, et al. 1994. Identification ofthe sex of human preimplantation embryos in two hours using animproved spreading method and fluorescence in situ hybridization(FISH) using directly labelled probes. Hum Reprod 9: 721–724.
Harris DJ, Hankins L, Begleiter ML. 1979. Reproductive risk oft(13q14q) carriers: case report and review. Am J Med Genet 3:175–181.
Honda H, Miharu N, Samura O, He H, Ohama K. 2000. Meioticsegregation analysis of a 14;21 Robertsonian translocation carrierby fluorescence in situ hybridization. Hum Genet 106: 188–193.
Iwarsson E, Malmgren H, Inzunza J, et al. 2000. Highly abnormalcleavage divisions in Preimplantation embryos from translocationcarriers. Prenat Diagn 20: 1038–1047.
Laverge H, De Sutter P, Verschraegen-Spae MR, De Paepe A,Dhont M. 1997. Triple colour fluorescent in-situ hybridization forchromosomes X, Y and 1 on spare human embryos. Hum Reprod12: 809–814.
Lissens W, Sermon K. 1997. Preimplantation genetic diagnosis:current status and new developments. Hum Reprod 12: 1756–1761.
Marquez C, Sandalinas M, Bahce M, Alikani M, Munne S. 2000.Chromosome abnormalities in 1255 cleavage-stage human embryos.Reprod Biomed Online 1: 17–27.
Morel F, Roux C, Bresson JL. 2001. FISH analysis of thechromosomal status of spermatozoa from three men with45,XY,der(13;14)(q10;q10) karyotype. Mol Hum Reprod 7:483–488.
Munne S, Cohen J. 1998. Chromosome abnormalities in humanembryos. Hum Reprod Update 4: 842–855.
Munne S, Alikani M, Tomkin G, Grifo J, Cohen J. 1995. Embryomorphology, developmental rates and maternal age are correlatedwith chromosome abnormalities. Fertil Steril 64: 382–391.
Munne S, Magli C, Adler A, et al. 1997. Treatment relatedchromosome abnormalities in human embryos. Hum Reprod 12:780–784.
Munne S, Fung J, Cassel MJ, Marquez C, Weier HU. 1998a.Preimplantation genetic analysis of translocations: case specificprobes for interphase cell analysis. Hum Genet 102: 663–674.
Munne S, Morrison L, Fung J, et al. 1998b. Spontaneous abortionsare reduced after preconception diagnosis of translocations. J AssistReprod Genet 15: 290–296.
Munne S, Scott R, Sable D, Cohen J. 1998c. First pregnancies afterpreconception diagnosis of translocations of maternal origin. FertilSteril 69: 675–681.
Munne S, Marquez C, Magli C, Morton P, Morrison L. 1998d.Scoring criteria for preimplantation genetic diagnosis of numericalabnormalities for chromosomes X,Y,12,16,18 and 21. Mol HumReprod 4: 863–870.
Munne S, Escudero T, Sandalinas M, Sable D, Cohen J. 2000.Gamete segregation in female carriers of Robertsonian transloca-tions. Cytogenet Cell Genet 90: 303–308.
Obasaju M, Kadam A, Sultan K, Fateh M, Munne S. 1999. Spermquality may adversely affect the chromosome constitution ofembryos that result from intracytoplasmic sperm injection. FertilSteril 72: 1113–1115.
Ogilvie CM, Braude P, Scriven PN. 2001. Successful pregnancyoutcomes after preimplantation genetic diagnosis (PGD) for carriersof chromosome translocations. Hum Fertil (Cam) 4: 168–171.
Pang MG, Hoegerman SF, Cuticchia AJ, et al. 1999. Detectionof aneuploidy for chromosomes 4,6,7,8,9,10,11,12,13,17,18,21,Xand Y by fluorescence in situ hybridisation in spermatozoafrom nine patients with oligoasthenoteratozoospermia undergoingintracytoplasmic sperm injection. Hum Reprod 14: 1266–1273.
Rousseaux S, Chevret E, Monteil M, et al. 1995. Sperm nucleianalysis of a Robertsonian t(14q21q) carrier, by FISH, using threeplasmid and two YAC probes. Hum Genet 96: 655–660.
Ruangvutilert P, Delhanty JDA, Serhal P, Simopoulou M, RodeckCH, Harper JC. 2000. FISH analysis on day 5 post-inseminationof human arrested and blastocyst stage embryos. Prenat Diagn 20:552–560.
Scriven PN, Flinter FA, Braude PR, Ogilvie CM. 2001. Robertsoniantranslocations-reproductive risks and indications for preimplantationgenetic diagnosis. Hum Reprod 16: 2267–2273.
Sousa M, Cremades N, Silva J, et al. 2002. Predictive value oftesticular histology in secretory azoospermic subgroups and clinicaloutcome after microinjection of fresh and frozen-thawed sperm andspermatids. Hum Reprod 17: 1800–1810.
Staessen C, Nagy ZP, Lui J, et al. 1995. One year’s experience withelective transfer of two good quality embryos in the human in-vitrofertilization and intracytoplasmatic sperm injection programmes.Hum Reprod 10: 3305–3312.
WHO. 1999. WHO Laboratory Manual for the Examination of HumanSemen and Sperm-Cervical Mucus Interaction (4th edn), CambridgeUniversity Press: Cambridge, UK.
Copyright 2002 John Wiley & Sons, Ltd. Prenat Diagn 2002; 22: 1153–1162.





























