Embed Size (px)
Citation preview

Pregnancy-relatedPelvic Girdle Pain
Guidance for Health Professionals


Contents 1. Introduction .................................................................................................................22. What is pregnancy-related pelvic girdle pain (PGP)? ...................................................23. Epidemiology ...............................................................................................................34. Aetiology ......................................................................................................................35. Risk factors ..................................................................................................................36. Diagnosis of PGP ..........................................................................................................47. Management ................................................................................................................5 i) Referral and care pathway. ........................................................................................5 ii) Management consideration ......................................................................................6 iii) General advice. ........................................................................................................7 iv) Previous history of PGP ............................................................................................8 8. Physiotherapy ...............................................................................................................8 i) Assessment ................................................................................................................8 ii) Treatment and management ....................................................................................89. Emotional effects of PGP ..............................................................................................910. Planning birth .............................................................................................................10 i) Informed choice .......................................................................................................10 ii) Active birth .............................................................................................................10 iii) Pain-free range of movement ................................................................................11 iv) Obstetric considerations ........................................................................................12 11. Postnatal care on the ward .........................................................................................13 i) Postnatal care on the ward ......................................................................................13 ii) Breast feeding.........................................................................................................13 iii) Care and support ...................................................................................................13 iv) Emotional well-being .............................................................................................1412. Postnatal care after discharge ....................................................................................14 i) Physiotherapy referral ..............................................................................................14 ii) Breastfeeding..........................................................................................................14 iii) Dyspareunia ...........................................................................................................14 iv) Return of symptoms ...............................................................................................15 v) Further investigations and medical imaging ...........................................................15 vi) Planning future pregnancies ..................................................................................1513. Websites and contact details .....................................................................................16References ...........................................................................................................................16Appendix 1 Commonly used terms ................................................................................19 Misused terms .............................................................................................19Appendix 2 Other useful reading ...................................................................................19Appendix 3 Expert panel ................................................................................................19
1

1. Introduction This booklet was commissioned by ACPWH (Association of Chartered Physiotherapists in Women’s Health) - now known as POGP (Pelvic Obstetric and Gynaecological Physiotherapy) and has been written and peer reviewed by a multidisciplinary group including obstetricians, physiotherapists, midwives and patient representatives.
Where possible, statements are based on the evidence available; otherwise they are informed by expert opinion, patient experience and best practice. Pregnancy-related pelvic girdle pain (PGP) is a term used to describe pain in the lumbo-sacral, sacro-iliac and symphysis pubis joints.
• Itisimportanttoacknowledgethatpregnancy-relatedPGPisacommon,recognisedcondition. It is common, but not normal, to have PGP in pregnancy.
• PGP is better managed with prompt identification and together with assessment and appropriate treatment, recovery can be anticipated.
• It can be treated safely at any stage during pregnancy (or after birth) as soon as symptoms arise.
• Inmanywomenitcanbetreatedeffectivelyandmayresolvewithinoneortwotreatments by a physiotherapist.
• Itisknownthat,ifleftuntreated,thisconditionmaylastmorethantwoyears1.
The aims of this leaflet are to:• increaseawarenessamongallrelevanthealthcareprofessionalsofpregnancy-related
PGP • providerecommendationsforaseamlesscarepathwayforwomenaffectedbyPGP• describeaetiology,riskfactors,signsandsymptomswithmanagementoptions
throughout pregnancy, birth, the postnatal period and beyond
2. What is pregnancy-related Pelvic Girdle Pain (PGP)?• ThetermSymphysisPubisDysfunction(SPD)hasbeenusedpreviouslytodescribethe
pregnancy-associatedpain,instabilityanddysfunctionofthesymphysispubisjoint(SPJ)and/orsacro-iliacjoint(SIJ).
• InlinewiththeEuropeanGuidelines(www.backpaineurope.org)thetermPelvicGirdlePain (PGP) is now the accepted umbrella term2.
• PGPwillbeusedthroughoutthisleaflettorelatespecificallytopregnancy-relatedpaininthelumbosacralregion,SIJsandSPJ.
• PGPmayhaveabiomechanicaloriginandberelatedtonon-optimalstabilityofthepelvic joints3.
• DiastasisSymphysisPubis(DSP)isaseparatebutrelatedcondition.Itcanonlybeconfirmedbydiagnosticimagingwhenitisshownthatthereisanabnormal,pathological, horizontal or vertical displacement of the symphysis pubis 4;5.
DSPcanoccurantenatally,duringdelivery,orpostnatally.• Forothercommonlyused/misusedtermsseeAppendix1.
2

3. Epidemiology • Lumbo-pelvicpainiscommonduringpregnancywithaprevalencedescribedvariously
as ranging from 50% to 70%6-12. • 14-22%ofallpregnantwomenhaveseriousPGPwith5-8%ofthesehavingproblems
with severe pain and disability13;14. • SeriousPGPispresentin7%ofwomenpostpartum10.
4. Aetiology • ThecausesofPGParemulti-factorialandoftenthereisnoobviousexplanation.• PGPismorelikelytobeacombinationoffactorsthatinclude:
• thepelvicgirdlejointsmovingasymmetrically3
• abnormalpelvicgirdlebiomechanicsfromalteredactivityinthespinal15, abdominal, pelvic girdle, hip16and/orpelvicfloormuscles17
• Asmallnumberofwomenmayhavenon-bio-mechanicalbuthormonally-inducedpainin the pelvic girdle. Occasionally the position of the baby may produce symptoms allied to PGP.
5. Risk factors • PGPmaydevelopinwomenwithnoidentifiableriskfactors.• Theevidenceforriskfactorsisinconclusiveandsomeevidenceiscontradictory2.• Themainriskfactorappearstobeahistoryofpreviouslow-back/pelvicgirdle/jointpain
and/or previous trauma to the pelvis8;18;19.• Earlierresearchfoundthatpoormusclefunctioninthebackandpelvisatthebeginning
of pregnancy is related to severe pain and disability throughout pregnancy51.
Other risk factors may include:• pelvicgirdlepaininapreviouspregnancy18
• multiparity8;20
• heavyworkload8;9
• poorworkplaceergonomicsandawkwardworkingconditions18
• highbodymassindexandweightpre-pregnancyandatendofpregnancy12;21
• generaljointhypermobility12;21
DSP - Evidence for risk factors is contradictory and often the exact cause is unknown but mayinclude:• precipitousdelivery22
• previousinjurytothepelvis22
• PGPinapreviouspregnancy22
• difficultbirth22
• forcefulandexcessiveabductionofthethighsduringdelivery1;23-27
• othertraumasuchasfallsinpregnancy23;26;27
Factors not associated with PGP include:• contraceptivepilluse,timeintervalsincelastpregnancy,height,smokingandage8;18-20
• breastfeeding
3

• Thediagnosiscanbereachedfromsignsandsymptomsexperiencedanddescribedbya woman during the pregnancy or in the postnatal period.
• Allwomenshouldbeaskedwhethertheyhaveanyproblemswiththeirbackorpelvis• Signsandsymptomsshouldnotbeignoredordismissedasachesandpainsof
pregnancy. Health professionals should always listen to the woman, have her problems investigatedand/orreferonasappropriate(seeSection7).
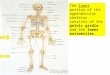
6. Diagnosis of PGP
Pain: distribution varies between individuals and includes:• lowerback• SPJ• SIJ(s)• groin• anteriorandposteriorthigh• posteriorlowerleg• hip/trochantericregion• pelvicfloor/perineum
4
LumbarspineSacroiliacjoint
SacrumCoccyx
Hip jointPubis ramus
SymphysispubisPerineum
Common signs and symptoms include:• difficultywalking(waddlinggait)• painonweightbearingononelege.g.climbingstairs,dressing• painand/ordifficultyinstraddlemovementse.g.gettinginandoutofbath;turningin
bed • clickingorgrindinginpelvicarea–maybeaudibleorpalpable• limitedandpainfulhipabduction(thoughsomewomenhavenormaloronlypartly
limited abduction)• difficultylyinginsomepositionse.g.supine,side-lying• painduringnormalactivitiesofdailylife• painanddifficultyduringsexualintercourse• difficultywalking(waddlinggait),withadiminishedendurancecapacityforstanding,
walking and sitting40
Anterior view Posterior view
Anterior view Posterior view

The posterior pelvic pain provocation test49andPatrick’s/Fabere’sTest(flexion,abductionand external rotation) have the best sensitivity if pain is evident in the sacroiliac joints
Differential diagnosis:Thediagnosiscanbereachedhavingexcluded:• urinarytractorotherinfection• lumbarspineproblems(requiresphysiotherapyreferral)• BraxtonHicksorlabourcontractions
7. Managementi) Referral and care pathway
5
Pain onset
Woman reports pain to GP, Midwife or Health Visitor or direct to Physiotherapist
Record PGP in notes
Midwife
Care planningfor pregnancy,
labour and postnatal
Referral as appropriate to:Physiotherapy referral
• Assessment•Treatment• Advice• Birthplanning
Treatment until symptoms
resolve
Onward referral in unresolving cases
Occupational therapy
SocialWorker Obstetrician Pain clinic
• Assessment•Treatment• Advice• Birthplanning
Treatment may include:• Manualtherapy• Exercise• Acupuncture• Provisionof
belt/crutches
• Adviceaboutbenefits
• Helpwithcarepackages for children/mother where necessary
• Housing
• Birthplanningoptions (Vaginal vs caesarean section)
• Timingofdelivery
• Alternativepaincontrol options
Orthopaedic opinion only when all other rehabilitation has been tried and it is unsuccessful
Storkx-rays,ultrasoundimaging(toexcludeDSP)and MRI scans or steroid injections
Surgeryisalastresortand has an unpredictable outcome

ii) Management considerations for health professionals at first point of contact
Give a clear and reasoned explanation of the condition to the woman and her family, partner, and/or carers
An acknowledgement of the physical and emotional aspects of the condition should be offered, together withfurtherinformationabout:• resourcese.g.aidsandappliances,otherservices
available• peersupportgroupse.g.PelvicPartnership
(seeSection13)• leafletsasrequired(Appendix2)
Paincontrol–considergivingor referring appropriately for advice, prescription and monitoring
• simpleanalgesia(paracetamol)• lowpotencyopiates(codeine,dihydrocodeine)• combinationsofabove(codydramol,etc)• considerusingprogressivelyandusingmost
potent/sedatingrestrictively–atworsttimes,perhaps overnight
• usuallyconsideredappropriatetoavoidnon-steroidalanti-inflammatorydrugsduringpregnancy
• acupuncture48
•TENS–refertophysiotherapist
6

Advice: It can help to:
iii) General advice:Considerthewoman’sindividualneeds:ifanactivitydoesnotincreasepain,orifpainhasresolved after treatment, activity may not automatically be restricted.
remain active within the limits of pain
avoid activities which she knows make the pain worse
accept offers of help and involve partner, family and friends in daily chores
ask for other help if needed
rest is important restmorefrequently,orsitdownforactivitiesthatnormally involve standing e.g. ironing
avoid standing on one leg dress sitting down
consider alternative sleeping position
lie on her side with pillows between legs for comfort. Turn “under” when turning in bed, or turn overwithkneestogetherandsqueezebuttocks
explore alternative ways to climb stairs
go upstairs one leg at a time with the most pain-free legfirstandtheotherlegjoiningitonthestep
plan the day bring everything needed downstairs in the morning and set up changing stations both up and downstairshavedrinksonhande.g.thermosflasksa rucksack may be helpful to carry things around the house, especially if crutches have to be used
avoid activities that involve asymmetrical positions of the pelvis
avoid sitting cross-leggedavoid reaching, pushing or pulling to one side avoid bending and twisting to lift or carrying anything on one hip e.g. toddlers
consider alternative positions for sexual intercourse
try lying on the side or kneeling on all fours
organise hospital appointments for the same day if possible
combine appointments for antenatal care and physiotherapy
This is not an exhaustive list. Further ideas for managing day-to-day activities are available fromthePelvicPartnershipwebsite(seeSection13).
7

iv) Previous history of PGPIfawomanhasexperiencedPGPpreviously:• sheshouldbeencouragedtocontactthephysiotherapydepartment• apatientself-help/physiotherapyleafletshouldbegiven(Appendix2)• thehealthprofessionalshouldmakeanurgentphysiotherapyreferral• ifanNHSphysiotherapistisnotavailablequickly,thewomanmaywishtoaccess
anappropriatelyexperiencedprivatephysiotherapist(seeSection13)orotherprofessional, (including osteopath, chiropractor, or acupuncturist) with appropriate expertise
8. PhysiotherapyWomen can be treated safely at any stage in pregnancy with standard physiotherapy interventions.Women should be referred to a physiotherapist who has appropriate training and expertise in PGP management and treatment. This may be a women’s health or musculoskeletal physiotherapist.• Physiotherapistsofferaholisticapproachinthemanagementofantenatalandpostnatal
PGP28 and can advise about labour and birth.• Physiotherapyaimstooptimisephysicalandemotionalhealthofthemotherby
improving spinal and pelvic girdle biomechanics and stability, improving strength of trunk and pelvic girdle muscles, improving range of hip mobility, controlling pain and improving function29.
• Forbestpractice,thephysiotherapistwillperformadetailedphysicalexaminationofthe woman to determine the origin of the symptoms (which differ between women) and plan appropriate treatment29.
i) Assessment should include (for best practice): • spinal,pelvicgirdleandhipjointexamination• examinationofmusclesresponsiblefortrunk,pelvicgirdleandhipstabilityandstrength• assessmentofthenervessupplyingthemuscles• assessmentoffunctionalabilities
ii) Treatment and management may include (for best practice):• adviceandeducation:includingbackcare,ergonomics,lifting,lookingafterbabyand
toddlers and positions for sexual intercourse• exercisestoretrainmotorcontrolandstrengthofabdominal,spinal,pelvicgirdle,hip
andpelvicfloormuscles30-32
• appropriatemanualtherapyasrequired13;14 e.g. mobilisations, manipulation, muscle energytechniques,stretches.Manualtherapyshouldbeaimedatcorrectinganyspinal, pelvic and hip joint dysfunction including increasing hip joint mobility (especially abduction)
• paincontrolasanadjuncttotheabovemodalities,inparticularacupuncture30;33-36 or TENS(guidanceforuseofTENSinpregnancyisavailableonthePOGPwebsite-seeSection13)
• exercisesinwater36;50
• provisionofequipmentasanadjuncttotreatmente.g.crutches,pelvicgirdlesupportbelts37-40, wheelchairs
8

Remember that:• itiscommon,butnotnormal,tohavePGPinpregnancyandeverywoman
presents differently • PGPisatreatable/manageablecondition• womenshouldbeadvisedtoseekhelpearly
With a multidisciplinary, collaborative approach both short- and long-term physical and psychological morbidity may be reduced.
9. Emotional effects of PGPHealth professionals should ask all women about their psychological well-being.• WomenwithPGPmayexperiencearangeofemotionaleffects.Fearshavebeen
noted41;42about:• theconditionitself• increasedpainanddisability• causingfurtherdamage• prognosis• implicationsforlabouranddelivery• positionsforbirth• futurechildbearing
• Womenmayfeel:• guiltifunabletofulfiltheirmotheringrole• angerandfrustrationattheirdependencyonothersandinabilitytocarefor
themselves or their family41
• cheatedandisolatedbecausetheycannotenjoytheirpregnancyormaintaintheirfitness
• Relationshipswithpartnerandchildrenmaybecompromisedasthefamilyadjuststonew circumstances.
• DepressionmaybeassociatedwithPGPintheantenatalandpostnatalperiodandrequirespromptrecognitionandmanagement.
i) Effect of chronic pain• Significantpain(morethan7/10onavisualanaloguescale)intheearlystagesofa
condition is a major predictor of chronicity43 so effective pain relief and management in early stages is vital.
• Tissuedamagemayresultinamaladaptiveresponseinthecentralnervoussystemwhichinturnmaybeinfluencedbythepatient’semotionsandbeliefs43.
• Lowordepressedmoodsarelargelytheresultofthepainratherthanthecause,buttheseinfluencegeneralhealthandperceptionofpain.
ii) Management of chronic pain42
Considereffectivemeansofpainrelief(seeSections7ii)and8ii))inconjunctionwith:• pacing(workingwithinlimitsofpainandendurance)• gradedfitnessprogramme• relaxationtechniques• communicationandcopingskills
9

10. Planning birthThis section has been based on expert opinion and evidence where available. All relevant health professionals should be competent to discuss the following information.
The majority of women will be able to have a normal spontaneous vaginal delivery and should be involved in discussion to achieve this.
Women may use a birth plan to record their wishes.
i) Informed choice may include discussion on: • painrelief• waterbirth• modeofdelivery• labourandbirthingpositions
ii) Active Birth55;56: women should be encouraged to be upright and mobile during labour. Alternative positions for the birth should be discussed e.g. • allfours• supportedkneeling• sidelyingwithpillows/kneestochest• labourandbirthinwater• discussiononcaesareansection,insomeexceptionalcases
CAUTION Advise not to put feet on attendants’ hips or shouldersFeetonmidwives’hipsshouldbecompletelyavoidedbecauseof–a)Risktomother(seeSection5)b) Risk to midwife
10

iii) Pain-free range of movement (hip abduction)• Anyantenatalrestrictionofthepain-freerangeofhipabduction(gapbetweenthe
knees) should have increased with physiotherapy. However if restriction persists thepain-freerangeofabduction(withthewomanlyingflatorinasupportedlyingposition with her knees bent and feet together), should be assessed and recorded both antenatally and early in labour. It is important that care is taken to avoid as far as possible any intrapartum damage to the pelvic girdle joints.
• Careshouldbetakennottoexceedthepain-freerangeofabduction,particularlyifepidural or spinal anaesthesia is used, as this might mask pain and cause damage to the pelvic joints.
• Hipabductionbeyondprelabourpain-freerangeandunsupportedsquattingshouldbeavoidedifpossible.Forcedhipabductionmayberequiredforsafedeliveryofbabyandshould only be used as part of the McRoberts procedure for shoulder dystocia.
• Vaginalexaminationsmaybeperformedinarangeofpositionssuchassidelyingoronall fours.
• Forinstrumentaldeliveryorsuturingwhenusingthelithotomyposition,careshouldbetaken to lift both legs together keeping within the pain-free range.
Measuring the pain-free range of abductionMeasure the distance between the inside of both the knees. Where possible the woman should not deliver with her knees wider apart than was comfortable before labour. Forced abduction and abduction beyond pain-free range should be avoided.
11

iv) Obstetric considerations
Expert opinion suggests:
a) Normal vaginal delivery• Thebestoptionformostwomen,ifitcanbeachieved.
Ideally:- Spontaneousonsetoflabour- ‘Comfortable’ birthing position e.g. high supported kneeling or left lateral position- Noforcedabductionofthighs
b) Induction, if indicated for reasons other than PGP• Parouswomen,previousnormalvaginaldeliveryattermwhopresentat38+weeks.
- Likelytoresultinnormalvaginaldelivery,butmayhavelonger‘latent’phase,especially if cervix is unfavourable.
• Primiparouswomen–especiallyiflessthan41weeksandcervixunfavourable.- SignificantriskofneedforemergencyCaesareanSection(CS)orassistedvaginal
delivery.
c) Elective Caesarean Section (CS)• MaybetheonlyrealoptioninwomenwhoareveryseverelyaffectedbyPGP–
where a comfortable birthing position cannot be achieved or maintained.• Maybeanoptionforotherlessseverecases,butnoevidencethatelectiveCS
(vsnormalvaginaldelivery)confersanybenefitonrecovery,prognosisorriskofrecurrence.
• Mayimpactonfertilityandabilitytoreproduce.• Limitsscopeforinductioninfuturepregnancies.• Futureattemptsatvaginalbirthaftercaesarean(VBAC)carrysomerisk.
d) Assisted vaginal delivery• Ventousepreferred.• Maybepossibleintheleftlateralposition.• Avoidexcessiveabductionofthighs.• Unlesslikelytobeeasy–emergencyCSmaybeabetteroption.• EmergencyCS(especiallyatfulldilatation)associatedwithitsownrisks.
e) Epidural analgesia• ‘Mobilemix’preferable.• Essentialtoobserve/maintainpain-freeabduction/gap.
12

11. Postnatal care on the wardi) Mobility
Mobilisation or bed rest? • Bedrestmayberequireduntilpainiscontrolled.Care should be taken not to cause further pain during mobilisation as analgesia may mask severe symptoms. Thromboprophylaxis should be considered.
• Whenpossible,conferwiththephysiotherapistabout length of bed rest, mobilisation and provision of crutches and belts.
Physiotherapy referral • Forearlyevaluationandtreatmentandtoassessmobility needs.
Pain relief • Regularanalgesia-NSAIDsandlowpotencyopiates (codeine) should be given.
If PGP occurs immediately postnatally
• Womenneedtobemanagedasabove.• IfthePGPhasoccurredduringlabourordelivery
refertophysiotherapy.Storkx-raysshouldbeconsideredinduecoursetoexcludeDSP.
Discharge • Womenshouldbedischargedhomewithappropriate package of care and follow-up arranged.
ii) Breast feeding• Earlyattachmentofthebabytothebreastwillpromotesuccessfulandlong-term
breastfeeding.• BreastfeedingwillnotslowtherateofrecoveryfromPGP.Itisanimportantrole
thatonlythemothercanfulfilandthesuccessislikelytoimproveself-esteemandpsychological well-being.
• Followingbirththemothershouldbeofferedhelptofindapositionofphysicalcomforte.g. side-lying, supported sitting. This also applies to mothers who are bottle feeding or expressing milk.
• MostNSAIDsandopiatesareconsideredsafetotakewhilebreastfeeding.Itistheprescriber’s responsibility to ensure safety of any medication.
iii) Care and support that may be offered:• helpwithpersonalcare• helpcaringforthenewbaby:
- lifting baby out of the cot for feeding- changing nappies- bathing the baby
13

• wherefacilitiespermit,apartnercanbeencouragedtostaytohelpwiththecareofmother and baby
• wherepossible,en-suitefacilitiesshouldbeprovidedorabedallocatedclosetothetoilet• foodanddrinkshouldbebroughttothemother• earlyreferralforphysiotherapyreview• referraltooccupationaltherapistorsocialservicesandmanualhandlingadviserforany
aidsandequipmentasappropriate
Useful equipment: • bolt-oncot• electricbed• walk-inshowerfacility• shower/bathseat• raisedtoiletseat
For mobilising:• wheelchair• crutches• frames
For turning in bed • slidingsheet• monkeypole• ropeladder• bedlever
Other• z-bedsforpartner/family
or specially allocated family rooms for women with PGP or other disabilities
iv) Emotional well-being• EffectivemanagementofPGPandappropriateemotionalsupportmayreducelong
term physical and psychological morbidity.• Ifsymptomsofanteorpostnataldepressionaresuspected,referforappropriate
treatment.
12. Postnatal care after discharge – best practiceAt any postnatal contact women should be asked whether they have pelvic girdle or lower back pain. A woman with existing PGP or who has developed a new episode of pain needs referral for physiotherapy.
i) Physiotherapy referral• Ifsymptomspersist,physiotherapyshouldberesumedassoonasthewomanfeelsable
to attend.• Reassessmentofthespineandpelvisshouldbeundertakenandanappropriate
treatment programme agreed.
ii) Breastfeeding. • Mothersshouldbeencouragedtocontinuetobreastfeedforaslongastheywish.
iii) Dyspareunia (painful intercourse) • Differentpositionsforsexualintercourseoralternativewaystobesexuallyintimateto
avoid discomfort should be suggested. • Otherpossiblereasonsfordyspareuniashouldbeconsidered(e.g.poorscarhealingetc).
iv) Return of symptoms • Whenmenstruationreturnssomewomenreportarecurrenceofsymptomsthatmay
resolve after a couple of months, but for some they persist with every cycle. Intensity
14

varies considerably but women should be reassured that this does not signal a return of severe disability.
• Ifsymptomsrecur,thepelvicgirdleshouldbere-assessedbyaphysiotherapistandappropriatetreatmentgivenandadequatepainreliefoffered.
• Thewomanshouldbeencouragedtoavoidknownpainprecipitators,suchaspushingasupermarket trolley.
v) Further investigation and medical imaging• Ifsymptomsarenotresolvingdespitemusculoskeletalphysiotherapyinterventions,
relevant orthopaedic opinion may be sought. • Therearenorecommendedtime-scalesforthis,butimagingshouldbecarriedout
when there is concern about length of recovery. • Furtherinvestigationsmayinclude:
• storkx-raystoassesstheamountofverticalandhorizontalshiftatthesymphysispubis when weight-bearing on one leg
• MRIimagingtoassessinflammationaroundtheSPandSIjoints.• ultrasoundscanning(canalsobedoneduringpregnancy)toassesssizeofSPJgap
• IthasbeensuggestedthatProlotherapycouldbeusedforLBPandSIJdysfunctionfollowing successful but not permanent relief from manual therapy46;47. However no full clinicaltrialshaveassesseditsefficacyinPGP.ItisavailableinsomepartsofthecountryontheNHSand,morewidely,privately.
There is no relationship between amount of pain and increased range of motion in the pelvic joints1;2 or between the size of the gap between the two pubic bones on imaging and amount of pain4.
vi) Planning future pregnancies • PGPrecursfrequentlyinsubsequentpregnancies,thoughitwillnotnecessarilybeas
severe if well managed. • Thereisnoparticularadvantageinleavingalonggapbetweenbabiesthoughsome
abdominal muscles may not have recovered by 12 months postpartum44.• ThewomanmayconsiderreducingthesymptomsofPGP,becomingfullyfit,losing
excess weight and waiting until other toddlers can walk before considering another pregnancy.
• WomenwithmoreseverePGPeitherconsideringafurtherpregnancyorwhoarealreadyin early pregnancy, may wish to seek a referral for physiotherapy for review and advice.
In conclusion: • PGPiscommon,butnotnormal,inpregnancyandeverywomanpresents
differently.• Itisatreatable,manageablecondition.• Womenshouldbeadvisedtoseekhelpearly.• Withamultiprofessional,collaborativeapproachbothshortandlong-term
physical and psychological morbidity may be reduced.
15

13. Websites and contact details• PelvicObstetric&GynaecologicalPhysiotherapy(POGP)-pogp.csp.org.uk• PelvicPartnership-pelvicpartnership.org.uk• CharteredSocietyofPhysiotherapy(CSP)-csp.org.uk;Tel02073666666• ManipulationAssociationofCharteredPhysiotherapists(MACP)-
macpweb.org • OrganisationofCharteredPhysiotherapistsinPrivatePractice(OCPPP)-
physiofirst.org.uk• AcupunctureAssociationofCharteredPhysiotherapists(AACP)-aacp.uk.com• BritishMedicalAcupunctureSociety-medical-acupuncture.co.uk
With help the woman should not become disabled during pregnancy, but if she does, the followingtwowebsitesofferpracticaladviceandsupport:
• DisabledParentsNetwork-disabledparentsnetwork.org.uk• Disability,PregnancyandParenthoodInternational-dppi.org.uk
References (1) AlbertH,GodskesenM,WestergaardJ.Prognosisinfoursyndromesofpregnancy-
relatedpelvicpain.ActaObstetGynecolScand2001;80(6):505-510.(2) VleemingA,AlbertH,OstgaardHC,StugeB,SturessonB.Europeanguidelineson
the diagnosis and treatment of pelvic girdle pain. European Commission, Research Directorate-General,DepartmentofPolicy,CoordinationandStrategy2004.
(3) DamenL,BuyrukHM,Guler-UysalF,LotgeringFK,SnijdersCJ,StamHJ.Pelvicpainduring pregnancy is associated with asymmetric laxity of the sacroiliac joints. Acta ObstetGynecolScand2001;80(11):1019-1024.
(4) BjorklundK,NordstromML,BergstromS.Sonographicassessmentofsymphysealjoint distention during pregnancy and post partum with special reference to pelvic pain.ActaObstetGynecolScand1999;78(2):125-130.
(5) BjorklundK,LindgrenPG,BergstromS,UlmstenU.Sonographicassessmentofsymphysealjointdistentionintrapartum.ActaObstetGynecolScand1997;76(3):227-232.
(6) MantleMJ,GreenwoodRM,CurreyHL.Backacheinpregnancy.RheumatolRehabil1977;16(2):95-101.
(7) FastA,ShapiroD,DucommunEJ,FriedmannLW,BouklasT,FlomanY.Low-backpaininpregnancy.Spine1987;12(4):368-371.
(8) BergG,HammarM,Moller-NielsenJ,LindenU,ThorbladJ.Lowbackpainduringpregnancy.ObstetGynecol1988;71(1):71-75.
(9) OstgaardHC,AnderssonGB,KarlssonK.Prevalenceofbackpaininpregnancy.Spine1991;16(5):549-552.
(10) WuWH,MeijerOG,UegakiK,MensJM,VanDieenJH,WuismanPIetal.Pregnancy-relatedpelvicgirdlepain(PPP),I:Terminology,clinicalpresentation,andprevalence.EurSpineJ2004.
16

(11) GutkeA,OstgaardHC,ObergB.Pelvicgirdlepainandlumbarpaininpregnancy:acohortstudyoftheconsequencesintermsofhealthandfunctioning.Spine2006;31(5):E149-E155.
(12) MogrenIM,PohjanenAI.Lowbackpainandpelvicpainduringpregnancy:prevalenceandriskfactors.Spine2005;30(8):983-991.
(13) DalyJM,FramePS,RapozaPA.Sacroiliacsubluxation:acommon,treatablecauseoflow-backpaininpregnancy.FamPractResJ1991;11(2):149-159.
(14) McIntyreIN,BroadhurstNA.Effectivetreatmentoflowbackpaininpregnancy.AustFamPhysician1996;25(9Suppl2):S65-S67.
(15) SihvonenT,HuttunenM,MakkonenM,AiraksinenO.Functionalchangesinbackmuscle activity correlate with pain intensity and prediction of low back pain during pregnancy.ArchPhysMedRehabil1998;79(10):1210-1212.
(16) Pool-GoudzwaardAL,VleemingA,StoeckartR,SnijdersCJ,MensJM.Insufficientlumbopelvicstability:aclinical,anatomicalandbiomechanicalapproachto‘a-specific’lowbackpain.ManTher1998;3(1):12-20.
(17) Pool-GoudzwaardAL,SliekertenHoveMC,VierhoutME,MulderPH,PoolJJ,SnijdersCJetal.Relationsbetweenpregnancy-relatedlowbackpain,pelvicflooractivityandpelvicfloordysfunction.IntUrogynecolJPelvicFloorDysfunct2005;16(6):468-474.
(18) LarsenEC,Wilken-JensenC,HansenA,JensenDV,JohansenS,MinckHetal.Symptom-givingpelvicgirdlerelaxationinpregnancy.I:Prevalenceandriskfactors.ActaObstetGynecolScand1999;78(2):105-110.
(19) Ostgaard HC, Andersson GB. Previous back pain and risk of developing back pain in afuturepregnancy.Spine1991;16(4):432-436.
(20) KristianssonP,SvardsuddK,vonSchoultzB.Backpainduringpregnancy:aprospectivestudy.Spine1996;21(6):702-709.
(21) Mogren IM. BMI, pain and hyper-mobility are determinants of long-term outcome for womenwithlowbackpainandpelvicpainduringpregnancy.EurSpineJ2006Jul;15(7):1093-1102.
(22) LindseyRW,LeggonRE,WrightDG,NolascoDR.Separationofthesymphysispubisinassociationwithchildbearing.Acasereport.JBoneJointSurgAm1988;70(2):289-292.
(23) GhermanRB,OuzounianJG,IncerpiMH,GoodwinTM.SymphysealseparationandtransientfemoralneuropathyassociatedwiththeMcRoberts’maneuver.AmJObstetGynecol1998;178(3):609-610.
(24) Ostgaard HC, Roos-Hansson E, Zetherstrom G. Regression of back and posterior pelvicpainafterpregnancy.Spine1996;21(23):2777-2780.
(25) HeathT,GhermanRB.Symphysealseparation,sacroiliacjointdislocationandtransient lateral femoral cutaneous neuropathy associated with McRoberts’ maneuver.Acasereport.JReprodMed1999;44(10):902-904.
(26) Cappiello GA, Oliver BC. Rupture of symphysis pubis caused by forceful and excessiveabductionofthethighswithlaborepiduralanesthesia.JFlaMedAssoc1995;82(4):261-263.
(27) KharraziFD,RodgersWB,KennedyJG,LhoweDW.Parturition-inducedpelvicdislocation:areportoffourcases.JOrthopTrauma1997;11(4):277-281.
17

(28) JainS,EedarapalliP,JamjuteP,SawdyR.Symphysispubisdysfunction:apracticalapproachtomanagement.TheObstetricianandGynaecologist2006;8:153-158.
(29) ColdronY.“MindtheGap”-Symphysispubisdysfunctionrevisited.JournaloftheAssociationofCharteredPhysiotherapistsinWomen’sHealth2005;96(Spring) 3-15.
(30) EldenH,LadforsL,OlsenMF,OstgaardHC,HagbergH.Effectsofacupunctureandstabilising exercises as adjunct to standard treatment in pregnant women with pelvic girdlepain:randomisedsingleblindcontrolledtrial.BMJ2005;330(7494):761.
(31) StugeB,VeierodMB,LaerumE,VollestadN.Theefficacyofatreatmentprogramfocusingonspecificstabilizingexercisesforpelvicgirdlepainafterpregnancy:atwo-yearfollow-upofarandomizedclinicaltrial.Spine2004;29(10):E197-E203.
(32) StugeB,LaerumE,KirkesolaG,VollestadN.Theefficacyofatreatmentprogramfocusingonspecificstabilizingexercisesforpelvicgirdlepainafterpregnancy:arandomizedcontrolledtrial.Spine2004;29(4):351-359.
(33) TernovNK,GrennertL,AbergA,AlgotssonL,AkesonJ.Acupunctureforlowerbackandpelvicpaininlatepregnancy:aretrospectivereporton167consecutivecases.PainMed2001;2(3):204-207.
(34) GuerreirodaSilvaJB,NakamuraMU,CordeiroJA,KulayL,Jr.Acupunctureforlowbackpaininpregnancy-aprospective,quasi-randomised,controlledstudy.AcupunctMed2004;22(2):60-67.
(35) LundI,LundebergT,LonnbergL,SvenssonE.Decreaseofpregnantwomen’spelvicpainafteracupuncture:arandomizedcontrolledsingle-blindstudy.ActaObstetGynecolScand2006;85(1):12-19.
(36) YoungG,JewellD.Interventionsforpreventingandtreatingpelvicandbackpaininpregnancy.CochraneDatabaseSystRev2002;(1):CD001139.
(37) VleemingA,BuyrukHM,StoeckartR,KaramurselS,SnijdersCJ.Anintegratedtherapyforperipartumpelvicinstability:astudyofthebiomechanicaleffectsofpelvicbelts.AmJObstetGynecol1992;166(4):1243-1247.
(38) CholewickiJ,JuluruK,RadeboldA,PanjabiMM,McGillSM.Lumbarspinestabilitycan be augmented with an abdominal belt and/or increased intra-abdominal pressure.EurSpineJ1999;8(5):388-395.
(39) DamenL,SpoorCW,SnijdersCJ,StamHJ.Doesapelvicbeltinfluencesacroiliacjointlaxity?ClinBiomech(Bristol,Avon)2002;17(7):495-498.
(40) MensJM,DamenL,SnijdersCJ,StamHJ.Themechanicaleffectofapelvicbeltin patients with pregnancy-related pelvic pain. Clin Biomech (Bristol , Avon) 2006; 21(2):122-127.
(41) ShepherdJ.Symphysispubisdysfunction:ahiddencauseofmorbidity.BritJMidwif2005;13(5):301-307.
(42) PapadopoulosC,HardingV.Chronicpain,pregnancyandchildrearing.In:GiffordL,editor.TopicalIssuesinPain2.Falmouth:CNSPress,2000:187-195.
(43) GiffordL.Tissueandinputrelatedmechanisms.In:GilbertA,editor.TopicalIssuesinPain:2.Falmouth:NOIPress,1998:57-65.
(44) ColdronY,StokesMJ,NewhamDJ,CookK.Postpartumcharacteristicsofrectusabdominisonultrasoundimaging.ManTher2007:Inpress.
18

(45) AlbertH,GodskesenM,WestergaardJ.Evaluationofclinicaltestsusedinclassificationproceduresinpregnancy-relatedpelvicjointpain.EurSpineJ2000;9:161–6.
(46) Cusi,M.F.ParadigmforassessmentandtreatmentofSIJmechanicaldysfunctionJournalofBodywork&MovementTherapies(2010)14,152e161.
(47) Dagenais,SMayerJHaldeman,SBorg-Stein,JEvidence-informedmanagementofchroniclowbackpainwithprolotherapyTheSpineJournal8(2008)203–212.
(48) EldenH,OstgaardHC,Fagevik-OlsenM,LadforsLHagbergH(2008)Treatmentsofpelvicgirdlepaininpregnantwomen:adverseeffectsofstandardtreatment,acupuncture and stabilising exercises on the pregnancy, mother, delivery and the fetus/neonate. BMC Complement Altern Med. 26, 8, 34).
(49) Ostgaard HC, Zetherstrom G, Roos-Hansson E.The posterior pelvic pain provocation testinpregnantwomen.EurSpineJ1994;3:258–60. SlipmanCW,SterenfeldEB,ChouLH,HerzogR,VresilovicE.Thepredictivevalueof provocative sacroiliac joint stress maneuvers in the diagnosis of sacroiliac joint syndrome.ArchPhysMedRehabil.1998Mar;79(3):288-92.
(50) PennickVandYoungG(2007)Interventionsforpreventingandtreatingpelvicandbackpaininpregnancy.CochraneDatabaseofSystematicReviews2007,Issue2.Art.No.:CD001139.DOI:10.1002/14651858.CD001139.pub2. WallerB,LambeckJandDalyD(2009)Therapeuticaquaticexerciseinthetreatmentoflowbackpain:asystematicreview.ClinicalRehabilitation.23,(1),3-14.
(51) Sihvonen,T,HuttunenM,MakkonenM,AiraksinenO.FunctionalchangesinbackmuscleactivitycorrelatewithpainintensityandSihvonenT,predictionoflowbackpainduringpregnancy.ArchPhysMedRehabil1998;79:1210–12.
(52) WallerB,LambeckJandDalyD(2009)Therapeuticaquaticexerciseinthetreatmentoflowbackpain:asystematicreview.ClinicalRehabilitation.23,(1),3-14.
(53) vanBentenE,PoolJ,MensJ,Pool-GoudzwaardA.RecommendationsforPhysicalTherapistsonthetreatmentoflumbopelvicpainduringpregnancy:aSystematicreview.JournalofOrthopaedicandSportsPhysicalTherapy.Volume44Issue7.July2014.
(54) LawrenceA,LewisL,HofmeyrG,StylesC.Maternalpositionsandmobilityduringfirststagelabour.CochraneDatabaseofSystematicReviews2013,Issue10.
(55) GuptaJK,HofmeyrGJ,ShehmarM.Positioninthesecondstageoflabourforwomenwithoutepiduralanaesthesia.CochraneDatabaseofSystematicReviews2012, Issue 5.
19

20
Appendix 1 - Terminology1a. Commonly used terms • SPD(SymphysisPubisDysfunction–umbrellaterm)• Symphysiolysis/anteriorpelvicpain(UnspecifiedpainaroundtheSPJ)• Osteitispubis(InflammationoftheSPJwithbonychangesonX-Ray)• SIJpain(Paininthesacro-iliacjoints)• Pelvicgirdlerelaxation• Lowbackpain(Painoflumbarspineorigin)• Hippain(Painarisingfromthehipjoint)• Diastasissymphysispubis(DSP)(Separationofthesymphysispubisjoint).
1b. Misused terminology• “Gapping”,• “Relaxed/splitpelvis”,• “Splitortornmuscles”• “Separatedordisplacedjoints”• “Dislocatedpelvis”
These terms are unhelpful as they may increase the woman’s anxiety and are not accurate descriptions of the actual condition
Appendix 2 - Other useful reading• Pregnancy-relatedPelvicGirdlePain(ForMothers-to-beandNewMothers)-POGP• FitforPregnancy(Antenatalleaflet)-POGP• FitforBirth-POGP• FitforMotherhood(PostnatalLeaflet)-POGP• FitandSafe-POGP• TheMitchellMethodofSimpleRelaxation-POGP• NICEguidelinesonpostnatalcare• POGPguidanceonthesafeuseofTENSformusculoskeletalpainduringpregnancy
(SeethePOGPwebsite)
Appendix 3 - Expert PanelIn order to clarify current thinking around pregnancy-related PGP, POGP brought together a panel of experts who reviewed the literature and together with clinical experience developedthisleaflet.Theexpertpanelconsistedof:-
Dr.YvonneColdron(Physiotherapist)SarahFishburn(Patientrepresentative)Mr.MalcolmGriffiths(Obstetrician)Paula Igualada-Martinez (Physiotherapist)Ros Thomas (Physiotherapist)ShernazScrewala(Physiotherapist)JancisShepherd(Midwife)


©POGPH2015forreview2018Reproductionofthisleafletinpartorinwholeisprohibited