Embed Size (px)
Citation preview

Precision Medicine & Epilepsy
Yuwu Jiang
Dept. of Pediatrics & Pediatric Epilepsy CenterPeking University First Hospital

Disclosures
No Conflicts of Interest
2

Outline
Precision medicine: why epilepsy?
Precision medicine: practice in epilepsy diagnosis and treatment
3

OutlinePrecision medicine: why epilepsy?
Precision medicine: practice in epilepsy diagnosis and treatment
4

5
Epidemiology
1. Camfield P. Epileptic Disord 2015; 17: 117‐1232. Wilmshurst JM, et al. Epilepsia 2015;56:1185‐1197
• Incidence of epilepsy in children 41‐187/100,0001
consistently reported to be highest in the first year of life2
• Prevalence ranges from: 3.2‐5.5/1,000 in developed countries1
3.6‐44/1,000 in underdeveloped countries1 ( ~10 million in China, 7/1000)
• Totally, ~1/3 refractory


Genetic EpilepsyEtiology‐Genetic
Monogenic‐Single gene, Mendelian
Rare variants‐Copy number variations (CNVs)
Common/Complex epilepsies‐Multigenic‐multiple genes, non‐Mendelian
Etiology‐Structure/Metabolic
A component of the phenotype spectrum for other Mendelian syndromes with brain structure or metabolic abnormalities due to genetic disease
7

Precision Medicine & Epilepsy
8
After cancer, epilepsy offers one of the possibly best model to achieve precision medicine
The rapid progress in epilepsy gene discovery
The existence of good animal and in‐vitro models allowing the development of medications tailored to genetically defined subtypes of epilepsy
The ability to assess efficacy of experimental targeted treatments in cost‐effective, small, brief clinical trials
National/International large scale multi‐center trail gradually established
N Engl J Med 2015; 372:793‐795

Precision Medicine & Epilepsy
9N Engl J Med 2015; 372:793‐795
All types of non‐acquired epilepsy will be assessed, and basic, clinical, and translational science will be closely integrated to drive the development of precision therapies

OutlinePrecision medicine: why epilepsy?
Precision medicine: practice in epilepsy diagnosis and treatment
10

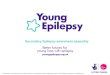
• Detection rate: 18% (84/467)• 84 patients were identified with causative mutations• 34 genes involved• 63 novel and 26 reported mutations• 39 severe mutations and 49 missense mutations• SCN1Amutation accounted for the largest proportion
(15/84), followed by SCN8A (10/84) and KCNQ2 (5/84)• 53% (18/34) of the mutated genes occurred only in one
case
Num
ber o
f patients
Epilepsy with ID‐ our data

Treatment Guided by Genetic Testing
Case 1
Male, 4 yrs
Afebrile convulsion occurred at 3 months after birth, staring to one side, develop to focal seizures with generalization. Seizure frequency increased gradually. Seizures occurred every time during fever or getting cold, which were always status epilepticus
12

Treatment Guided by Genetic Testing
Case 1
Treated by antiepileptic drugs since 1yr
Seizures not controlled well by valproate, topiramate and oxcarbazepine. During his best time, no fever no seizures
Nervous system examination (‐), cranial MRI (‐), biochemical examination (‐), blood (urine) metabolism screening (‐)
EEG: normal at onset; multifocal spikes, with slow background at late stage
13

Case 1
Dravet syndrome‐clinically
But, gene mutation screening of SCN1A(‐)
Diagnose? Further Treatment?
14
Treatment Guided by Genetic Testing

Case 1
Dravet syndrome‐clinically
Targeted epilepsy genes panel
ALDH7A1,c.1553G>C/p.Arg518Thr, hetero, paternal; c.1061A>G/p.Tyr354Cys, hetero, maternal
Diagnosis: pyridoxine‐dependent seizures
Treated by vitamin B6(50mg, tid)since 2yrs, gradually tapered AEDs, seizure free for over 2 yrs (no seizures even in fever)
15
Treatment Guided by Genetic Testing

Case 2
male,4 yrs
Seizures occurred at 2 yrs, all during sleep, occurred almost every night, multiple seizures each sleep, asymmetric tonic seizures, 10 sec (duration), poor sleep when seizures occurred frequently
Ineffective: oxcarbazepine, levetiracetam, valproate
16
Treatment Guided by Genetic Testing

Case 2
Nervous system examination (‐), cranial MRI (‐),
biochemical examination (‐), blood (urine)
metabolism screening (‐)
EEG: paroxysmal slow waves at bilateral frontal
lobes ‐interictal
17
Treatment Guided by Genetic Testing

Case 2
Targeted epilepsy genes panel
KCNT1, c.1058G>A/p.Arg353Gln, de novo, not found in his parents
Diagnosis: Nocturnal frontal lobe epilepsy, KCNT1mutation‐induced
Treated by quinidine
KCNT1 gain of function in epilepsy reversed by quinidine
Ann Neurol. 2014 Apr;75(4):581‐90
18
Treatment Guided by Genetic Testing

0
5
10
15
20
25
30
35
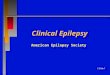
K+ channel gene mutations
Num
ber o
f patients
32
21
9
3 3 31 1 1 1
75 K+ channel gene mutations involved 72 patients
54 novel and 21 reported mutations
KCNQ2mutations accounted for the largest population(42.7%, 32/75), followed by KCNT1(28.0%, 21/75), and KCNMA1(12.0%, 9/75)‐2 cases reported
All the mutations are de novo

Precision medicine in epilepsy
20
AEDs choice‐based on gene, not on clinic
SCN8Amutations in Chinese children with early onset epilepsy and intellectual disability. ‐OXC
Epilepsia. 2015; 56(3):431‐8.
Early and effective treatment of KCNQ2 encephalopathy. ‐CBZ,PHT
Epilepsia. 2015; 56(5):685‐91.
STXBP1 related epileptic encephalopathy‐LEV
Brain Dev. 2016 Jan;38(1):128‐31.

Num
ber o
f patients
362 Na+ channel gene mutations involved 362 patients
277 novel and 85 reported mutations
SCN1Amutations accounted for the largest
population(81.8%, 296/362), followed by SCN2A(8.6%,
31/362), and SCN8A(8.0%, 29/362)
All the mutations are de novo

Precision medicine in epilepsy
22
Re‐purposed drug choice‐treatment trials based on mutation realted mechanism KCNT1 gain of function in 2 epilepsy phenotypes is reversed by
quinidine. Ann Neurol. 2014; 75(4):581‐90.
GRIN2Amutation and early‐onset epileptic encephalopathy: personalized therapy with memantine. Ann Clin Transl Neurol. 2014; 1(3):190‐198.
SCN1Amutated epilepsy‐Clemizole (histamine antagonist), a re‐purposed drug from available library of 300 compounds Neurobiol Dis. 2015;79: 135–49

Predict Severe AEDs‐induced cutaneous reactions‐Genetic Test?
HLA‐B*1502 allele: highly associated with carbamazepine‐induced Stevens‐Johnson syndrome (SJS) in Han Chinese (Taiwan, Hong Kong, Mainland), as well as phenytoin, and lamotrigine induced SJS; not associated with maculopapular exanthema (MPE) .Not found in Caucasian cases (but in Caucasian with Asian ancestry)‐indicate the role of ethnicityCommercial detecting kit is available
Epilepsia. 2007;48(5):1015-8; Pharmacogenomics J. 2006;6(4):265-8
23

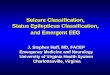
Predict Severe AEDs‐induced cutaneous reactions
N Engl J Med 2011;364:1126-33
24

N Engl J Med 2011;364:1126-33
25
Predict Severe AEDs‐induced cutaneous reactions

Precision medicine related main companies in China
Equipment Service
Comprehensive
SpecializedReagnents
Domestic
Foreign
Imported
Domestic
Bioinformatic

What’s next for PM in epilepsy?Large scale (national & international) cohort and registration study for all non‐acquired epilepsy
More fast, convenient and economic genetic test: next generation sequence
Enhancing bioinformatics capacity for data analysis to improve the accuracy of risk assessment and genetic counseling
Better functional study for pathogenic variation
Developing more specific / “tailored” AEDs therapy, even gene therapy through specific genetic markers or targets, or based on certain pathogenic pathway
27

What’s next for PM?
28
Clinical practice
Genetic and molecular
Investigation
Clinical trial &
Big data
Mutual & active interaction in health care whole process
‐e.g. our JI project for epilepsy