Embed Size (px)
Citation preview

Case presentationCase presentation

consult from surgery- 51y female consult from surgery- 51y female
51y female with Traumatic Brain injury @ 12yo51y female with Traumatic Brain injury @ 12yo Obese (BMI > 40)Obese (BMI > 40) HTN- well-controlled on lisinopril 40mg/dHTN- well-controlled on lisinopril 40mg/d OSAOSA Chronic cough + intermittent hemoptysis Chronic cough + intermittent hemoptysis
Extensive pulmonary w/u normal to date Extensive pulmonary w/u normal to date (PFT+bronch)(PFT+bronch)
Hx of left fem/pop DVT ~9mo agoHx of left fem/pop DVT ~9mo ago Recent Pap normalRecent Pap normal

What issues are pertinent to her surgery?What issues are pertinent to her surgery?
What tests need to be done now?What tests need to be done now?
Should she be cleared for the surgery?Should she be cleared for the surgery?

The Pre-operative evaluationThe Pre-operative evaluation
August Hein, M.D.August Hein, M.D.
LtCol USAF, MC, SFSLtCol USAF, MC, SFS

StratificationStratification Patient factorPatient factor
Different classification systemsDifferent classification systems Goldman 1977Goldman 1977 Detsky 1986Detsky 1986 Lee’s revised 1999Lee’s revised 1999
Recognize similar key pointsRecognize similar key points
Surgical factors/riskSurgical factors/risk LowLow IntermediateIntermediate HighHigh

Surgery classificationSurgery classification
InvasivenessInvasiveness
Emergent / RoutineEmergent / Routine

Surgical StratificationSurgical Stratification
Cardiac riskCardiac risk High (> 5% risk of cardiac event*):High (> 5% risk of cardiac event*):
Emergent major operations, esp. in elderlyEmergent major operations, esp. in elderly Aortic/ major vascular surgeryAortic/ major vascular surgery Peripheral vascular surgeryPeripheral vascular surgery Anticipated large fluid shifts and/or blood lossAnticipated large fluid shifts and/or blood loss
*Cardiac event = fatal and non-fatal MI*Cardiac event = fatal and non-fatal MI

Intermediate risk (< 5% risk of event)Intermediate risk (< 5% risk of event) Carotid endarterectomyCarotid endarterectomy Head and neck surgeryHead and neck surgery Intraperitoneal and intrathoracic surgeryIntraperitoneal and intrathoracic surgery Orthopedic or Prostate surgeryOrthopedic or Prostate surgery

Low risk (< 1% risk of cardiac event)Low risk (< 1% risk of cardiac event) Endoscopic proceduresEndoscopic procedures Superficial proceduresSuperficial procedures Cataract surgeryCataract surgery Breast surgeryBreast surgery

Pulmonary riskPulmonary risk
Definite factorsDefinite factors Upper abdominal surgeryUpper abdominal surgery Thoracic surgeryThoracic surgery AAA repairAAA repair Surgery > 3hrsSurgery > 3hrs
Probable factorsProbable factors General anesthesiaGeneral anesthesia Emergency surgeryEmergency surgery

Patient FactorsPatient Factors
Exercise CapacityExercise Capacity Medication useMedication use ObesityObesity AgeAge LabsLabs EKGEKG CXRCXR PFTPFT

Source: http://uptodateonline.com/utd/content/image.do?imageKey=prim_pix/preop_pa.gif

Source: AAFP
15 April 2004


Exercise CapacityExercise Capacity Good capacity = 4 METs Good capacity = 4 METs
Two level blocks without symptomsTwo level blocks without symptoms One flight of stairs with two bags of groceriesOne flight of stairs with two bags of groceries
Poor exercise capacity: < four level blocks or two flights of stairsPoor exercise capacity: < four level blocks or two flights of stairs
Expected Complications:Expected Complications:Total: 20% vs 10%Total: 20% vs 10%Cardiac: 10% vs 5%Cardiac: 10% vs 5%Pulmonary: 9% vs 6% (not statistically signif.)Pulmonary: 9% vs 6% (not statistically signif.)

Medication useMedication use
Back door route to forgotten medical hxBack door route to forgotten medical hx HTNHTN HypothyroidHypothyroid Asthma/COPDAsthma/COPD
May forget OTCs (aspirin, NSAIDS)May forget OTCs (aspirin, NSAIDS) So ask!So ask!

ObesityObesity
DESPITEDESPITE Reduced lung volumeReduced lung volume V/Q mismatchV/Q mismatch Relative hypoxemiaRelative hypoxemia
NOT a risk factor, but considered in NOT a risk factor, but considered in pulmonary and upper abdominal surgerypulmonary and upper abdominal surgery
Studies that show increased RR tend to not Studies that show increased RR tend to not use multivariate analysisuse multivariate analysis

AgeAge
Mortality riskMortality risk < 60 = 1.3%< 60 = 1.3% 80-89 = 11.3%80-89 = 11.3%
Multiple factors present, not a good sole Multiple factors present, not a good sole criterion for withholding surgerycriterion for withholding surgery

LabsLabs
CBCCBC Asymptomatic anemia <1% prevalenceAsymptomatic anemia <1% prevalence Surgically significant anemia is even lowerSurgically significant anemia is even lower
Mortality for surgery with expected blood lossMortality for surgery with expected blood loss Hct >12 Hct >12 1.3% 1.3% Hct < 6 Hct < 6 33%33%
Remainder of CBC not useful (wbc,plt) in Remainder of CBC not useful (wbc,plt) in asymptomatic individualsasymptomatic individuals

Labs (cont’d)Labs (cont’d) LytesLytes
History/medication use more usefulHistory/medication use more useful
BUN/CrBUN/Cr Reasonable over 50 – recent emphasis on CRIReasonable over 50 – recent emphasis on CRI Major surgeryMajor surgery Hypotension expectedHypotension expected Nephrotoxic meds anticipatedNephrotoxic meds anticipated

Labs (cont’d)Labs (cont’d)
FBS/FBG/FSG – or just serum glucoseFBS/FBG/FSG – or just serum glucoseNot recommended for surgical screeningNot recommended for surgical screening
**Recent control hx imperative for diabetics****Recent control hx imperative for diabetics**
LFT – only if history/exam suggest diseaseLFT – only if history/exam suggest disease
PT/PTT – low correlation of abnl to postop comp.PT/PTT – low correlation of abnl to postop comp.““perfectly unhelpful” predictor perfectly unhelpful” predictor
+ likelihood ratio 0.0+ likelihood ratio 0.0 - likelihood ratio 1.01- likelihood ratio 1.01

Labs (cont’d)Labs (cont’d)
UAUA ? id renal disease or UTI?? id renal disease or UTI?
Serum Cr would id renal dz betterSerum Cr would id renal dz better UTIs may contribute to 4-5 post-op UTIs may contribute to 4-5 post-op
infections/yearinfections/year If UA for all non-prosthetic knee operationsIf UA for all non-prosthetic knee operations $1.5 million per infection prevented!$1.5 million per infection prevented! Post-op infection adds ~$3000 to surgical costsPost-op infection adds ~$3000 to surgical costs

EKGEKG
Low likelihood of changing managementLow likelihood of changing management Recent MI important to detectRecent MI important to detect Cardiac event risk increased by:Cardiac event risk increased by:
Non-sinus rhythmNon-sinus rhythm PACsPACs >5 PVCs>5 PVCs
No risk increase with BBBNo risk increase with BBB

EKGEKG
RecommendationsRecommendations Men > 45 Women > 55Men > 45 Women > 55 Known cardiac dzKnown cardiac dz H&P suggesting possibility of cardiac dzH&P suggesting possibility of cardiac dz Electrolyte imbalance risk (ie diuretic use)Electrolyte imbalance risk (ie diuretic use) DM/HTN DM/HTN Candidates for major surgeriesCandidates for major surgeries

CXRCXR
Abnormalities not well associated with Abnormalities not well associated with post-operative riskpost-operative risk 0.1% affected management0.1% affected management Routine use not recommendedRoutine use not recommended
2 exceptions (by consensus)2 exceptions (by consensus) >60y>60y Suspected cardiac or pulmonary diseaseSuspected cardiac or pulmonary disease

Pulmonay Function TestPulmonay Function Test
No improvement over clinical evalNo improvement over clinical eval Where the money is:Where the money is:
Decreased breath soundsDecreased breath sounds Prolonged expiratory phaseProlonged expiratory phase Rales, rhonchi, wheezesRales, rhonchi, wheezes
PFTs for unexplained dyspnea after good PFTs for unexplained dyspnea after good clinical evalclinical eval

Minor risk predictorsMinor risk predictors
Advanced age Advanced age Abnormal electrocardiogram Abnormal electrocardiogram
Left ventricular hypertrophy Left ventricular hypertrophy Left bundle branch block Left bundle branch block ST-T-wave abnormalities ST-T-wave abnormalities
Rhythm other than sinus rhythm (e.g., atrial fibrillation) Rhythm other than sinus rhythm (e.g., atrial fibrillation) Low functional capacity: < 4 METs (e.g., inability to Low functional capacity: < 4 METs (e.g., inability to
climb one flight of stairs holding a bag of groceries) climb one flight of stairs holding a bag of groceries) History of stroke History of stroke Uncontrolled systemic hypertension Uncontrolled systemic hypertension

Intermediate risk predictorsIntermediate risk predictors
Mild angina pectorisMild angina pectoris Previous MI based on the history or the Previous MI based on the history or the
presence of pathologic Q waves presence of pathologic Q waves Compensated or previous CHFCompensated or previous CHF Diabetes mellitus, particularly insulin-Diabetes mellitus, particularly insulin-
dependent diabetes dependent diabetes Renal insufficiency Renal insufficiency

Major risk predictorsMajor risk predictors
Unstable coronary syndromesUnstable coronary syndromes Acute (<7d) or recent (7-30d) MI w/ evidence of important Acute (<7d) or recent (7-30d) MI w/ evidence of important
ischemic risk by clinical symptoms or noninvasive study ischemic risk by clinical symptoms or noninvasive study Unstable or severe angina Unstable or severe angina
Decompensated CHF Decompensated CHF Significant arrhythmiasSignificant arrhythmias
High-grade atrioventricular block High-grade atrioventricular block Symptomatic ventricular arrhythmia in the presence of Symptomatic ventricular arrhythmia in the presence of
underlying heart disease underlying heart disease Supraventricular arrhythmias with uncontrolled ventricular rate Supraventricular arrhythmias with uncontrolled ventricular rate
Severe valvular diseaseSevere valvular disease

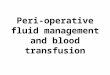
YesHigh
YesHigh
YesHigh
YesHighNoLowGood
Stress Testing
Surgical Risk:
Functional Status:
Consider delay for medical management, risk-factor modification. Consider angiography
Major RiskPredictors
Yes/NoLowGood
YesLowPoor <4 MEts
Intermediate Risk Predictors
NoLowPoorMinor Risk Predictors

Indications for Ambulatory ECG Indications for Ambulatory ECG for ischemia monitoringfor ischemia monitoring
Class I: NoneClass I: None Class IIaClass IIa Patients with suspected variant anginaPatients with suspected variant angina Class Class IIbIIb Evaluation of patients with chest pain who cannot exerciseEvaluation of patients with chest pain who cannot exercise **Preoperative evaluation for **Preoperative evaluation for vascular surgeryvascular surgery of patients of patients
who cannot exercise*who cannot exercise*** Patients with known CAD and atypical chest pain syndromePatients with known CAD and atypical chest pain syndrome Class IIIClass III Initial evaluation of chest pain patients who are able to exerciseInitial evaluation of chest pain patients who are able to exercise Routine screening of asymptomatic subjectsRoutine screening of asymptomatic subjects
source: source: http://www.americanheart.org/presenter.jhtml?identifier=1925http://www.americanheart.org/presenter.jhtml?identifier=1925

Pre-op eval “take home”Pre-op eval “take home” Screening questionnaireScreening questionnaire Exercise toleranceExercise tolerance Blood pressure and pulseBlood pressure and pulse Expand H & P if above abnl, pt >60y or major surgeryExpand H & P if above abnl, pt >60y or major surgery
HCG for young womenHCG for young women HCT for bloody surgeryHCT for bloody surgery Serum Cr for major surg/ possible hypotension/ Serum Cr for major surg/ possible hypotension/
nephrotoxic meds/ pt > 50nephrotoxic meds/ pt > 50
Beta-blocker for known Ischemic dz --> vascular surgeryBeta-blocker for known Ischemic dz --> vascular surgery Stress-testing if exercise capacity in questionStress-testing if exercise capacity in question

ECG Men > 45 ECG Men > 45 Women > 55Women > 55 Known cardiac dzKnown cardiac dz Eval suggesting possibility of cardiac dzEval suggesting possibility of cardiac dz Electrolyte imbalance risk (ie diuretic use)Electrolyte imbalance risk (ie diuretic use) DM/HTN DM/HTN Candidates for major surgeriesCandidates for major surgeries

2007 Dental update2007 Dental update Antimicrobial prophylaxis = FOUR cardiac conditions w/ highest risk of adverse Antimicrobial prophylaxis = FOUR cardiac conditions w/ highest risk of adverse
outcome from endocarditis:outcome from endocarditis: 1. Prosthetic cardiac valves1. Prosthetic cardiac valves 2. Cardiac transplantation with subsequent valvulopathy 2. Cardiac transplantation with subsequent valvulopathy 3. Previous history of infective endocarditis3. Previous history of infective endocarditis 4. Congenital Heart Disease (CHD), including only:4. Congenital Heart Disease (CHD), including only:
Unrepaired cyanotic CHD, including palliative shunts and conduitsUnrepaired cyanotic CHD, including palliative shunts and conduits Completely repaired congenital heart defects with prosthetic material or device, whether Completely repaired congenital heart defects with prosthetic material or device, whether
placed by surgery or by catheter intervention, during the placed by surgery or by catheter intervention, during the first six months afterfirst six months after the the procedureprocedure
Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)or prosthetic device (which inhibit endothelialization)
B. Dental Procedures for Which Endocarditis Prophylaxis is Recommended:B. Dental Procedures for Which Endocarditis Prophylaxis is Recommended: ““All dental procedures that involve All dental procedures that involve manipulation of gingival tissuemanipulation of gingival tissue or the periapical or the periapical region of teeth or region of teeth or perforation of the oral mucosaperforation of the oral mucosa.”*.”*
* No prophylaxis needed: routine anesthetic injections through non-infected * No prophylaxis needed: routine anesthetic injections through non-infected tissue, taking dental radiographs, placement of removable prosthodontic or tissue, taking dental radiographs, placement of removable prosthodontic or orthodontic appliances, adjustment of orthodontic appliances, placement of orthodontic appliances, adjustment of orthodontic appliances, placement of orthodontic brackets, shedding of deciduous teeth, and bleeding from trauma to the orthodontic brackets, shedding of deciduous teeth, and bleeding from trauma to the lip or oral mucosa.lip or oral mucosa.
C. What Antibiotic Regimens for a Dental Procedure? The same single dose C. What Antibiotic Regimens for a Dental Procedure? The same single dose antibiotic regimens from the 1997 Guidelines can be given 30 to 60 minutes before antibiotic regimens from the 1997 Guidelines can be given 30 to 60 minutes before the procedure.the procedure.

Case #2Case #2
76y male with debilitating Rt hip OA76y male with debilitating Rt hip OA Scheduled for Rt Total HipScheduled for Rt Total Hip
s/p inferior MI 1yr ago – TPA, resolutions/p inferior MI 1yr ago – TPA, resolution No tobacco useNo tobacco use No CVD, no DM, EF wnl, Bun/Cr wnlNo CVD, no DM, EF wnl, Bun/Cr wnl Walked 1-2 mi/day until 2mo ago – painWalked 1-2 mi/day until 2mo ago – pain Simvastatin, HCTZ,Simvastatin, HCTZ, Rx’d Atenolol, stopped after bronchitis 2 wks agoRx’d Atenolol, stopped after bronchitis 2 wks ago BP 157/92; Exam wnl; ECG =inf Q wavesBP 157/92; Exam wnl; ECG =inf Q waves

Lee's Revised Cardiac Risk IndexLee's Revised Cardiac Risk Index
Clinical variableClinical variable PointsPointsHigh-risk surgery (i.e., intraperitoneal, High-risk surgery (i.e., intraperitoneal,
intrathoracic, or suprainguinal vascular intrathoracic, or suprainguinal vascular surgery)surgery) 1 1
Coronary artery diseaseCoronary artery disease 1* 1*Congestive heart failureCongestive heart failure 1 1 History of CVDHistory of CVD 1 1
Insulin for diabetes mellitusInsulin for diabetes mellitus 1 1Preoperative SCr > 2.0 mg/dLPreoperative SCr > 2.0 mg/dL 1 1
TotalTotal:__1__:__1__

Interpretation of Risk ScoreInterpretation of Risk Score Risk class Risk class Points Points Complication* risk Complication* risk
I. Very low I. Very low 0 0 0.4% II. 0.4% II. Low Low 1 1 0.9% 0.9% III. ModerateIII. Moderate 2 2 6.6% 6.6% IV. HighIV. High 3 3 +11.0% +11.0%
*- MI, PE, VF, *- MI, PE, VF, cardiac arrest, or complete cardiac arrest, or complete
heart block.heart block.

ReviewReview
*Exercise tolerance*Exercise tolerance *Blood pressure and pulse*Blood pressure and pulse *Expand H & P if above abnl, pt >60y or major surgery*Expand H & P if above abnl, pt >60y or major surgery
HCG for young womenHCG for young women *HCT for bloody surgery*HCT for bloody surgery *Serum Cr for major surg/ possible hypotension/ *Serum Cr for major surg/ possible hypotension/
nephrotoxic meds/ pt > 50nephrotoxic meds/ pt > 50
*Beta-blocker for known Ischemic dz --> vascular *Beta-blocker for known Ischemic dz --> vascular surgery or history of taking themsurgery or history of taking them
*Stress-testing*Stress-testing

SummarySummary
Pre-op eval is not “clearance”Pre-op eval is not “clearance” Determine risks, then minimizeDetermine risks, then minimize Let surgeon, anesthesia do the “clearing”Let surgeon, anesthesia do the “clearing”
Screening Labs/Tests rarely useful aloneScreening Labs/Tests rarely useful alone Should be driven by suspicions from eval/hxShould be driven by suspicions from eval/hx

LinksLinks
ArticlesArticles http://www.acc.org/clinical/guidelines/perio/update/periupdate_index.htmhttp://www.acc.org/clinical/guidelines/perio/update/periupdate_index.htm http://www.aafp.org/afp/20040415/poc.htmlhttp://www.aafp.org/afp/20040415/poc.html http://www.americanheart.org/presenter.jhtml?identifier=1960http://www.americanheart.org/presenter.jhtml?identifier=1960 Smetana, Gerald W. in: http://uptodateonline.com/utd/contenthttp://uptodateonline.com/utd/content http://www.aafp.org/afp/20070301/656.htmlhttp://www.aafp.org/afp/20070301/656.html http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.106.183095v1http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.106.183095v1
formsforms http://www.aafp.org/afp/20040415/pocform.htmlhttp://www.aafp.org/afp/20040415/pocform.html http://uptodateonline.com/utd/content/image.do?imageKey=prim_pix/preop_pa.gif