Embed Size (px)
Citation preview

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 1/29
Premedication
Goals of premedication: – Calm and sedate the patient
– Reduce stress of handling
– Smooth anesthetic induction,
maintenance and recovery – Reduce induction and
maintenance drugs required
– Provide pre-emptive analgesia
and muscle relaxation – Decrease airway secretions
and salivation
– Obtund autonomic reflexes
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 2/29
• Hypnosis:
– A depth of sedation fromwhich the patient is not
easily aroused – Loss of ability to
maintain a patent airway
– Lack of response to
surgical stimuli – Propofol, ketamine,
thiobarbiturates,etomidate
– Indistinguishable fromgeneral anesthesia withvolatile anesthetics
• Sedative
– Drug that relieves anxiety
– “Conscious” sedation
– Drowsiness
– Benzodiazepines andalpha-2 agonists
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 3/29
• Tranquilizer:
• A drug with apredominant action inrelieving anxiety without producingundue sedation.
• These drugs are also
called anxiolytics orantianxiety drugs.
• An example of this typeof drug would be
diazepam and otherbenzodiazepines
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 4/29
Anti-cholinergics
• Competitivelyantagonize Ach atcholinergic
postganglionic muscarinic receptors (parasympatholytic)
• Receptors found in:
– Heart – Salivary glands
– Smooth muscles ofthe GIT and UT
• Postganglionic nicotinicreceptors located at the NMJ
and autonomic ganglia• Anticholinergics are
selectively anti-muscarinicand only anti-nicotinic at toxic
doses
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 5/29

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 6/29
• Atropine is an alkaloid ofbelladonna
• Semi-synthetic
belladonna alkaloids(e.g., glycopyrrolate) arequaternary ammoniumderivatives which aremore potent
• Glycopyrrolate does notcross the BBB, so has noocular or CNS effects
• Atropine crosses the BBBand cause sedation,excitement, andmydriasis
• Potent antisialogouges
• Reduce salivary and bronchial
secretions
• Mydriasis (atropine)
• Central AnticholinergicSyndrome (rare)

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 7/29
Parasympatholytic
• Competitively antagonizes Achat cholinergic postganglionicmuscarinic receptors
• Decreases vagal tone andprevents vagally inducedbradycardia
• Increases and maintains HRand improves CO
• Sinus bradycardia, sinusarrest, sinus block, 1o,2o, and 3o AV blockade
• CPR = atropine
• Bronchodilation
Cardiac Output = HR x SV
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 8/29
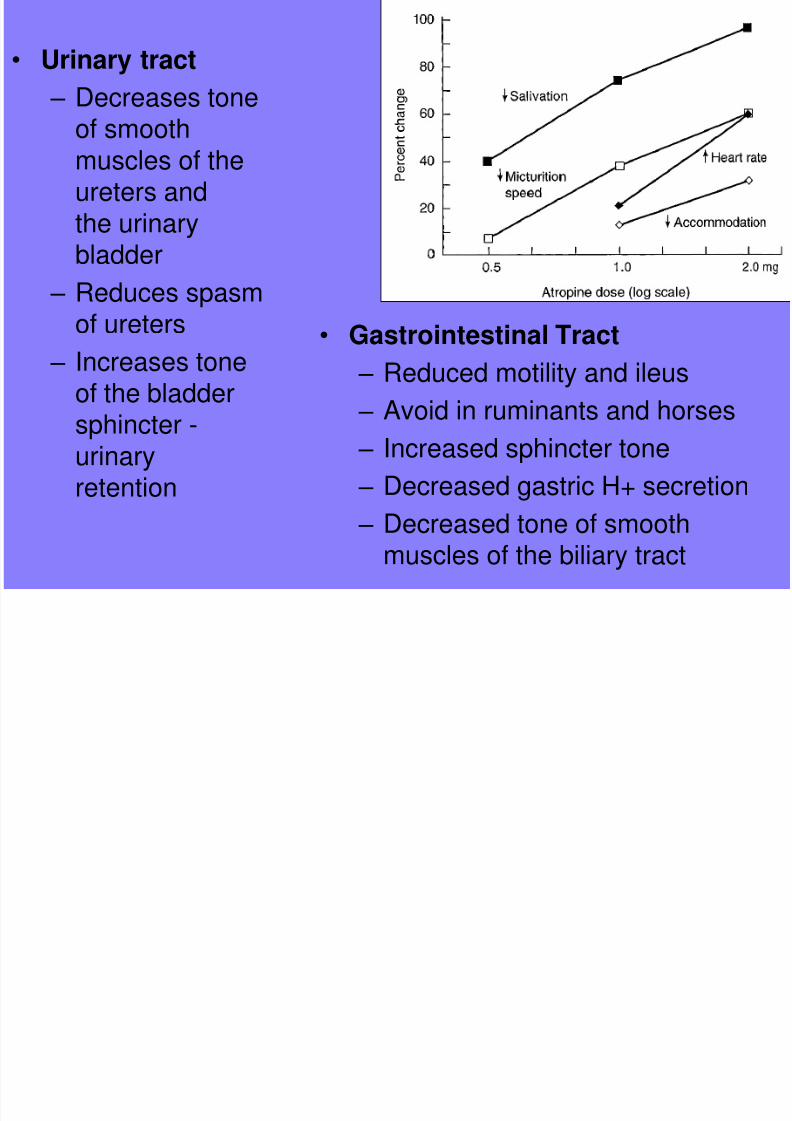
• Gastrointestinal Tract
– Reduced motility and ileus
– Avoid in ruminants and horses – Increased sphincter tone
– Decreased gastric H+ secretion
– Decreased tone of smooth
muscles of the biliary tract
• Urinary tract
– Decreases tone
of smoothmuscles of theureters andthe urinarybladder
– Reduces spasmof ureters
– Increases toneof the bladder
sphincter -urinaryretention
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 9/29
Clinical Use
• Included as pre-medication:
• Maintain heart rate and CO
• Offset vagal reflexes
• Decrease GIT, salivary and respiratory secretions
• To treat sinus bradycardia, sinus arrest, sinus block, andfirst, second, and third degree atrioventricular blockade
• Contraindications:
– Pre-existing tachycardia
– GI motility problems (horses, rabbits, ruminants)
Asystole = Atropine!

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 10/29
Tranquilizers and Sedatives
Phenothiozines
Benzodiazepines
Alpha-2 agonists and antagonists
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 11/29
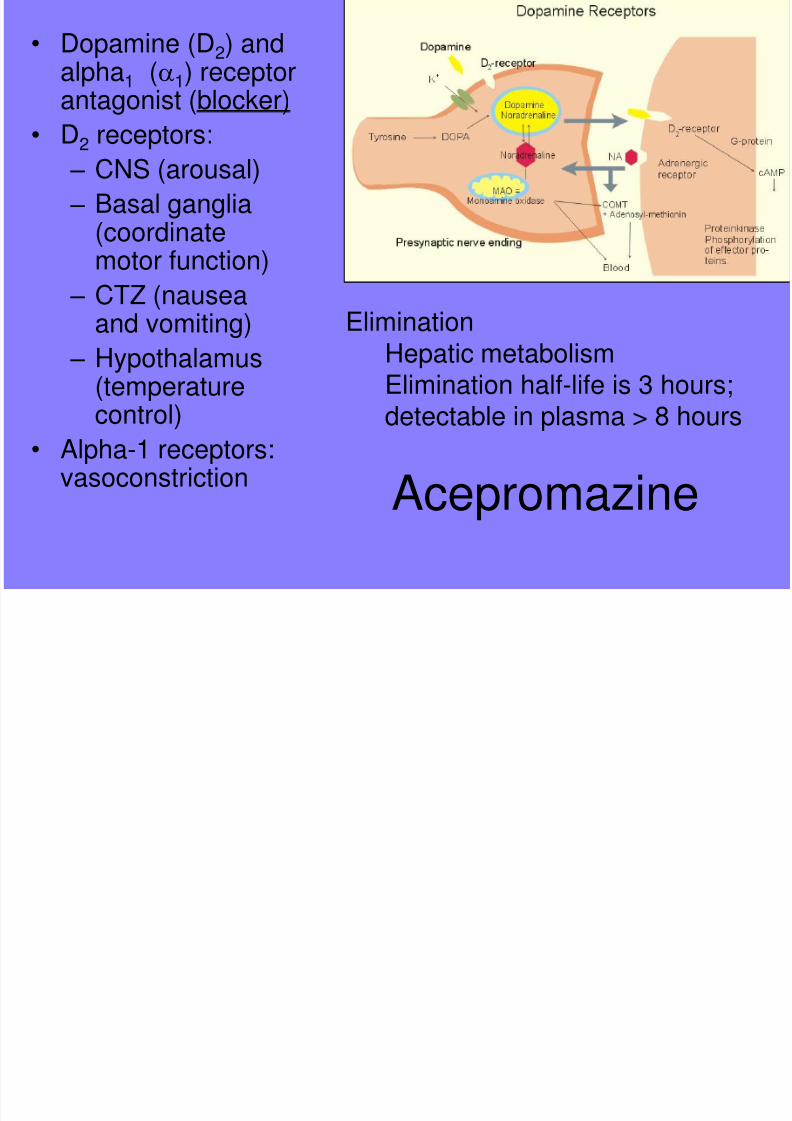
Acepromazine
• Dopamine (D2) andalpha1 (a1) receptorantagonist (blocker)
• D2 receptors: – CNS (arousal)
– Basal ganglia(coordinatemotor function)
– CTZ (nauseaand vomiting)
– Hypothalamus(temperature
control)• Alpha-1 receptors:
vasoconstriction
EliminationHepatic metabolismElimination half-life is 3 hours;
detectable in plasma > 8 hours
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 12/29
Cardiovascular Effects - Ace
• Respiratory effects
– Minimal effects
• Dose dependent decrease in blood pressure due to:
– Alpha1 R blockade - vasodilation
– Depression of CNS vasomotor centers – CV collapse in patients with high SNS tone or
hypovolemia
• Epinephrine reversal
• Anti-arrhythmic• Decreases sensitivity to catecholamines
• Cardiac output and heart rate minimally affected a lowdosage rates
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 13/29
CNS Effects of Acepromazine
• Sedation (prolonged period of sedation – at least 4 hours)
• Anxiolytic (likely not)
• Muscle relaxation and decreased motor activity
• Third eyelid prolapse
• Reduces required dosages of other drugs, includinginhalants (MAC reduction)
• Anti-emesis (CTZ)
• Inhibits hypothalamic thermoregulation
• Rigidity or tremors with overdosage (Extra-pyramidal orParkinsonian-like signs)
• Acepromazine has the reputation for lowering the seizurethreshold, but there is little evidence to support this.

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 14/29
Other EffectsAcepromazine• Anti-emetic (CTZ)
• Anti-histamine
• Hypothermia
• Penile prolapse and priapism in stallions
• Splenic sequestration of RBC’s
• Prolonged sedation (4 to 8 hours or longer)
• Premedication prior to anesthesia
• Contraindicated in head trauma, increased ICP
• Contraindicated in neonates, elderly, shocky patients
• Caution in Boxers; always combine with an anticholinergic
• Lower dosages in larger animals
• Caution with aggressive animals

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 15/29
Benzodiazepines
• Distribution &Elimination
– Highly protein
bound (96-98%)
– Unbound drugcrosses theblood brainbarrier and isactive
• Metabolism
– Hepatic with
renal excretionof metabolites
• Mechanism of Action
– Receptors in cerebral cortex,hypothalamus, cerebellum,
midbrain, hippocampus, medullaand spinal cord
– Increase GABA and glycine
– Sedation due to increased
GABA activity in the CNS – Anxiolysis & muscle relaxation
due to increased glycine activity
– Mild analgesic effects - possiblydue to increased GABA
– Retrograde amnesia

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 16/29
CNS Effects-Benzodiazepines
• Anticonvulsant• Very mild sedation or
even excitement whenused alone in dogs, cats,
horses• Mild to profound sedation
in sick animals
• Mild sedation in ruminants
• Muscle relaxation (spinallymediated)
• Analgesia (mild)
• Appetite stimulant
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 17/29
Benzodiazepines
• Respiratory
– Minimal effects
– Respiratory depression whencombined with opiates orother anesthetic agents
• Cardiovascular
– Minimal effects
– Slight increase in HR
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 18/29
• Diazepam (Valium)
– Water insoluble (dissolved in propylene glycol)
– Pain on injection
– Mixes poorly with other drugs (except ketamine)
• Diazepam usually given IV, but can be given orally
– Unreliable absorption when given IM or SQ
• Midazolam (Versed)
– Water soluble at low pH
– Given IM, IV or subcutaneously
– 2-3 x’s more potent than diazepam
– Shorter acting than diazepam – No pain on injection
– Can be mixed with other drugs
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 19/29
Benzodiazepines
• Zolazepam
– Found only combined withTiletamine as Telezol
– Only benzodiazepinelicensed for use inveterinary patients
• Flumazenil - reversal agent forall benzodiazepines

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 20/29
Clinical Usage:
• Rarely used alone in healthy patients as sedation ispoor and excitement may occur
• Often combined with ketamine to induce anesthesia
• Administered with opiates for sedation of higher riskpatients (neurolept anesthesia)
• Sedative affects are good in debilitated, sick patients,especially if combined with an opiate
• Generally used for sedation of pediatric, geriatric, andcompromised patients
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 21/29
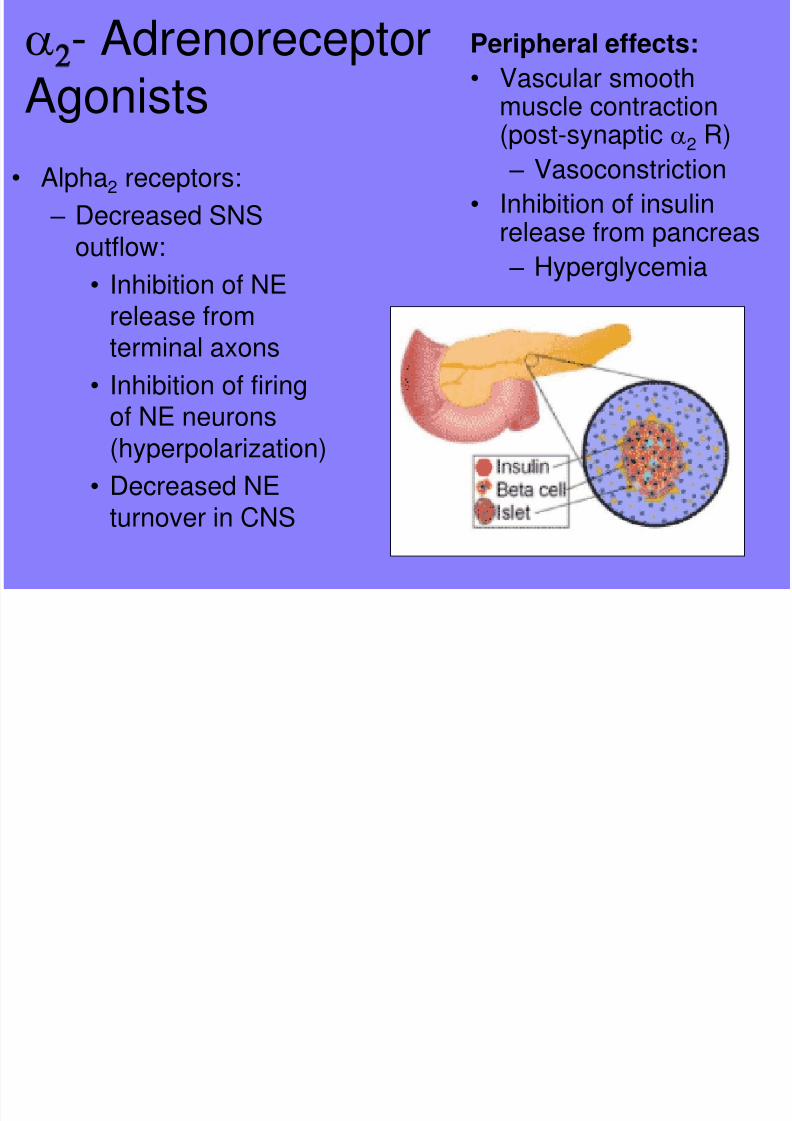
a2- Adrenoreceptor
Agonists
• Alpha2 receptors:
– Decreased SNSoutflow:
• Inhibition of NErelease fromterminal axons
• Inhibition of firing
of NE neurons(hyperpolarization)
• Decreased NEturnover in CNS
Peripheral effects:
• Vascular smoothmuscle contraction
(post-synaptic a2 R) – Vasoconstriction
• Inhibition of insulinrelease from pancreas
– Hyperglycemia

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 22/29
a2- Adrenoceptor Agonists
• Decreased SNS outflow in the CNS results in:
– Sedation (Alpha-2 receptors in the locus ceruleus)
– Analgesia (spinal a2 receptors)
– Muscle relaxation (spinal a2 receptors)
– Cardiovascular depression (centrally mediated)
• Bradycardia
• Decreased contractility
• Vasodilation
• Decreased CO
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 23/29
Cardiovascular Effects• Administration results in initial vasoconstriction, followed by
reflex bradycardia, then centrally mediated SNS depression• Bradycardia, vasodilation, decrease in CO, tissue perfusion
• Dysrhythmias
• Xylazine causes premature ventricular contractions (PVC’s);
other a-2 agonists decrease PVC’s
• All cause sinus arrhythmias, bradycardia, sinoatrial block, 1stand 2nd degree A-V block
• Respiratory
– Mild respiratory depression
– More significant with opiates
– Hypoxemia in cattle and sheep
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 24/29
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 25/29
CNS Effects
• Analgesia
• Comparable to opioids in efficacy for visceral pain andact synergistically with opioids
• Duration of analgesia is much shorter (around 1 hour)
than duration of sedation
• Significant reduction of doses of other drugs used foranesthesia, including volatile anesthetics (MACreduction)
• Reversal agents available – alpha-2 antagonists
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 26/29
Unwanted Effects
• Vomition in dogs and cats (xylazine) • Decreased GI tract motility, resulting in ileus
• Inhibition of insulin release from pancreas resulting in hyperglycemia and osmotic diuresis
• Sweating and piloerection in horses • Increased myometrial contractions in cattle with xylazine,
which can lead to abortion in the third trimester
• Bradycardia -reversed with alpha-2 antagonists or
atropine or glycopyrrolate only if life-threatening• Indications: Young to middle-aged, healthy, exercise-
tolerant animals
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 27/29
Contraindications:
• Pre-existing CNS depression• Pre-existing cardiovascular disease
• Gastric or intestinal or urinary obstruction
• Diabetes mellitus
• Avoid xylazine in cattle in the last trimester of pregnancy
• In any animal that does not have normal cardiovascularand respiratory function
8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 28/29
a2- Adrenoceptor Antagonists
• Increase SNSoutflow and NErelease from CNS
• Reversibility is an
advantage
• Specificity for a2 receptors:atipamazole >
idozoxan >yohimbine >tolazoline
N l t l i

8/3/2019 Pre Medication 2010
http://slidepdf.com/reader/full/pre-medication-2010 29/29
Neuroleptanalgesia • Goal: production of a tranquil, calm patient with some
dissociation from environment and analgesI• Combination of a tranquilizer or sedative with an opioid
• A tranquil and analgesic state due to synergism of ananalgesic and a tranquilizer or sedative
• Better sedation results in:• -- Better restraint and decreased dosages of other agents
used (injectable and volatile anesthetics)
• Addition of the opiate allows decreased dosage of sedate
• Less CV depression with additional sedation• More rapid elimination of drugs when differing metabolic
pathways involved
• More rapid elimination and recovery because of lower dose






![MEDICATION THERAPY - jknj.jknj.moh.gov.myjknj.jknj.moh.gov.my/farmasi/garispanduan/[2010] Protocol Medication...Pharmaceutical care, which is comprehensive and patient focussed is](https://img.dokumen.tips/doc/110x75/5d04303b88c99322638c72de/medication-therapy-jknjjknjmohgov-2010-protocol-medicationpharmaceutical.jpg)






















