Embed Size (px)
Citation preview

Proc. Natl. Acad. Sci. USAVol. 82, pp. 5915-5919, September 1985Immunology
Prazosin, an a1-adrenergic receptor antagonist, suppressesexperimental autoimmune encephalomyelitis in the Lewis rat
(delayed-type hypersensitivity/edema/blood-brain barrier/autoimmunity)
CELIA F. BROSNAN*, ELLEN A. GOLDMUNTZtt, WENDY CAMMERtt, STEPHEN M. FACTOf*,BARRY R. BLOOM§¶ AND WILLIAM T. NORTONttDepartments of *Pathology, tNeurology, tNeuroscience, §Ceil Biology, and Microbiology and Immunology, Albert Einstein College of Medicine, 1300 MorrisPark Avenue, Bronx, NY 10461
Communicated by Dominick P. Purpura, May 13, 1985
ABSTRACT Prazosin, an antagonist of a1-adrenergic re-ceptors, has been found to suppress the clinical and histologicalexpression of experimental autoimmune encephalomyelitis(EAE) in the Lewis rat. Suppression was more significant infemales than in males and was a dose-dependent phenomenon.Analysis of the effect of other adrenergic receptor antagonistssupports the conclusion that the suppressive effect of prazosinis a consequence of blockade of the a,-receptor since treatmentwith either the a2-antagonist yohimbine or the P-antagonistpropranolol exacerbated the disease, whereas treatment withthe long-acting mixed al/a2-antagonist phenoxybenzaminehad some suppressive activity. Treatment with prazosin wasalso able to suppress clinical and histological signs of EAE inanimals sensitized by adoptive transfer with activated spleen orlymph node cells. Whether prazosin acts through alteringvascular permeability or the immune response, or both,remains to be determined.
Experimental autoimmune encephalomyelitis (EAE) is aninflammatory demyelinating disease of the central nervoussystem (CNS) that has been studied extensively as a modelof multiple sclerosis. The development of EAE has beenshown to be dependent on the sensitization ofT lymphocytesagainst the single protein antigen myelin basic protein (MBP).In the Lewis rat EAE can be passively transferred bylymphoid cells or spleen cells from donors sensitized againstMBP (1-3) and it has been shown that transfer is dependenton the W3/25-positive (helper) subset ofT cells (4). By usingmorphologic criteria and cell surface markers, analysis of thecell types in the perivascular infiltrates in the CNS during theacute stage of actively induced EAE has shown that W3/25-positive T cells and Ia-positive macrophages predominate (5).The lesions that develop in the CNS of recipients of passivelytransferred EAE resemble those that develop during activelyinduced EAE. Studies have shown that although some of thelymphocytes in the lesion are derived from the donor, themononuclear cells as well as additional lymphocytes arederived from the recipient. Furthermore, the development ofEAE after passive transfer is dependent on host bone marrowcells (2).The recruitment of mononuclear cells by T cells and their
entry into the CNS during the acute stage of EAE is typicalof the inflammatory response that develops as a consequenceof a delayed-type hypersensitivity (DTH) reaction. In 1975Gershon et al. (6) suggested that vasoactive amines may playa role in DTH reactions by facilitating the perivascular transitof the augmenting inflammatory cells that do not normallyleave the blood. Recently, several authors have shown thatdepletion or inhibition of vasoactive amines can modulate the
course ofEAE (7, 8) or experimental allergic neuritis (9). Aspart of a study on drugs that affect vascular tone, we havefound that prazosin gave significant protection against theclinical expression of EAE in the Lewis rat (10). Prazosin(Minipress), a quinazoline derivative, is a specific a1-adre-nergic receptor antagonist that has widespread clinical use asan antihypertensive agent. As a result of this observation wehave explored further the involvement of adrenergic recep-tors in EAE. The results support the conclusion that antag-onists of adrenergic receptors can modulate the expression ofEAE in the Lewis rat.
MATERIALS AND METHODSChemicals. Chemically pure prazosin hydrochloride was a
gift of Pfizer. Propranolol hydrochloride (Inderal) was pur-chased from Ayerst Laboratories (New York, NY); phenoxy-benzamine hydrochloride (Dibenzyline) was purchased fromSmith Kline & French; yohimbine and isoproterenol werepurchased from Sigma. All drugs were suspended in saline,using sonication where necessary, and were injected by thei.p. route.
Animals. Lewis rats weighing -200-250 g were obtainedfrom Charles River Breeding Laboratories.
Sensitization. Myelin was prepared from guinea pig spinalcord by the method of Norton and Poduslo (11), lyophilized,and stored at -200C. Immediately prior to use the myelin wasresuspended in sterile distilled water and saline in a ratio of1:1 at 5 mg/ml and was emulsified in an equal volume ofcomplete Freund's adjuvant (CFA) containing 10 mg ofMycobacterium tuberculosis H37Ra (Difco) per ml. Animalswere sensitized by inoculation with 0.05 ml in each hindfootpad on day 0. CFA control animals were inoculated withCFA emulsified 1:1 with saline.
Clinical Assessment of Disease. Beginning on day 7, animalswere weighed and assessed for clinical signs of disease on adaily basis. A clinical index (CI) was used to grade animalson a scale of 1-5: grade 1, abnormal gait and flaccid tailaccompanied by weight loss (>10 g); grade 2, a mild butdefinite weakness of one or both hind legs or severe ataxia;grade 3, minimal hind leg movement; grade 4, no hind legmovement accompanied by forelimb involvement; and grade5, moribund state with impaired respiration and little or nospontaneous movement.
Histological Assessment of Disease. For assessment ofdemyelination, animals under sodium pentobarbital anesthe-sia were perfused through the heart with an initial flush of4%paraformaldehyde followed by 5% glutaraldehyde inSorensen's phosphate buffer for 10 min. Tissue samples werepostfixed in 2% Dalton's chrome osmium solution, dehydrat-
Abbreviations: CI, clinical index; CFA, complete Freund's adjuvant;dpi, days postinoculation; DTH, delayed-type hypersensitivity;EAE, experimental autoimmune encephalomyelitis; MBP, myelinbasic protein; CNS, central nervous system.
5915
The publication costs of this article were defrayed in part by page chargepayment. This article must therefore be hereby marked "advertisement"in accordance with 18 U.S.C. §1734 solely to indicate this fact.
Dow
nloa
ded
by g
uest
on
Apr
il 5,
202
0

Proc. Natl. Acad. Sci. USA 82 (1985)
ed in graded concentrations of ethanol, immersed inpropylene oxide, and embedded in Epon. Sections 1 Am thickwere cut and stained with toluidine blue. For assessment ofperivascular infiltration, the brain and spinal cord were fixedin 10o formalin in phosphate buffer and embedded inparaffin, and the sections were stained with hematoxylin/eo-sin.
Passive Transfer of Activated Lymphocytes. Inguinal lymphnodes and spleens were removed 10 days postinoculation(dpi), freed of fat and connective tissue, and pressed throughstainless steel mesh grids. Lymph node cells were washedthree times in Hanks' balanced salt solution. Spleen cellswere treated with 0.83% ammonium chloride for 5 min to lyseerythrocytes and were washed with Hanks' balanced saltsolution. Cells were resuspended at a count of 2 x 106 per mlin RPMI 1640 medium containing 10% heat-inactivated fetalbovine serum (GIBCO), 1% glutamine, and 2-mercaptoeth-anol (Eastman Kodak) at a final concentration of 20 AM.Cells were cultured in 24-well plates (1 ml, Linbro) or 75-cm2T flasks (25 ml, Falcon) at 370C in 5% CO2 in air for 72 hr inthe presence of 2 pug ofguinea pig MBP per ml for spleen cellsand 10 ,ug of guinea pig MBP per ml for lymph node cells.MBP was prepared according to the method publishedpreviously (12). Cells, at a count of 4 x 107 in RPMI mediumcontaining 5% fetal bovine serum, were transferred by i.v.inoculation into syngeneic recipients. Animals were weigheddaily and assessed for clinical expression of disease.
Statistical significance was calculated by using a two-tailedStudent's t test.
RESULTSSensitization of Lewis rats with guinea pig spinal cord myelinemulsified in CFA results in an acute episode ofparalysis thatcommences 10 dpi with an abrupt onset of weight loss. Theclinical course progresses rapidly ovet the next few days,with peak clinical incidence of disease occurring at 13 dpi.Resolution of the disease then also progresses fairly rapidly,with full clinical recovery occurring by 21 dpi. The diseasecourse is essentially the same in male and female rats, withthe exception that at the peak of clinical disease male rats aremore severely affected than female rats.
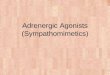
Effect ofPrazosin on Cliuickl Expression ofEAE. To test forthe effect of prazosin on the disease course animals wereinjected with 2 mg i.p. twice a day commencing 7 dpi andcontinuing through 16 dpi. The results obtained for femaleand male rats are shown in Fig. 1 a and b, respectively.
4- 4la b
3' 3I
2 2I
For female rats, the clinical signs ofEAE were reduced inthe prazosin-treated group. These animals did not developany signs before 11 dpi and reached a peak CI of 1.1 ± 0.1(mean ± SEM) at 14 dpi as compared to a peak CI of 3.0 ±0.2 at 13 dpi in the saline-treated group. The animals in bothgroups recovered without further clinical incidence. Thedifferences in clinical disease between the saline-treatedanimals and the prazosin-treated animals were significantfrom 11 dpi through 15 dpi (P < 0.001) and on 16 dpi (P <0.01).
In male rats inoculated with 2 mg of prazosin twice dailyfrom 7 dpi through 16 dpi, clinical signs first appeared at 10dpi and peaked at 15 dpi with a CI of 2.2 ± 0.3 (mean ± SEM)as compared to a peak index of 3.9 ± 0.2 in saline-treatedanimals at 13 dpi. Although clinical expression ofdisease wasmarkedly reduced in the prazosin-treated male rats, the datawere not as significant for as many days as those obtainedwith female rats. The difference at this dose was significantat a P < 0.001 for days 12 through 14.To test for the effect of the initiation of treatment at a later
time, 20 female rats were inoculated with 2 mg of prazosinstarting at 9 dpi instead of 7 dpi, as in Fig. 1 a and b, andcontinuing through 16 dpi. In these animals the clinical signsof EAE (Fig. ic) were clearly ameliorated with a peak CI of1.7 ± 0.5 (mean ± SEM) at 14 dpi as compared with a peakCI of 3.3 + 0.2 at 13 dpi in the saline-injected control animals(n = 20). The data were significant at a P <0.001 for days 12and 13.Dose Dependence. To examine the relationship between
dosage and disease suppression, prazosin was given twicedaily in doses ranging from 0.5 mg to 2.5 mg to groups of fivefemale rats, commencing at 7 dpi and continuing through 16dpi. The effects on the clinical expression of EAE are shownin Fig. 2. A dose of 0.5 mg offered no protection; 1.0 mg,slight protection; 2.0 mg, significant protection; and 2.5 mg,almost complete protection. Similarly, in males a dose of 3mg twice a day offered almost complete protection (data notshown). Thus, the effect of prazosin on the clinical expres-sion of EAE is dose dependent.Treatment of EAE with Drugs That Modulate Adrenergic
Receptor Function. Prazosin is an antagonist of the a,-adrenergic receptor. At 1 mM to 0.1 mM, concentrations thatare unlikely to be obtained in vivo and that are toxic tolymphocytes in vitro, it inhibits 3',5'-cyclic AMP phospho-diesterase (13) and thus could also act as an immunosuppres-sant (14). To elucidate the role of adrenergic receptor
10 12 14 16 18 20Days Postinoculation
FIG. 1. CI of prazosin-treated Lewis rats compared with saline-treated rats. Data are expressed as the mean + SEM. (a) Female rats injectedtwice daily i.p. with 2 mg ofprazosin (o, n = 70) or saline (e, n = 78) beginning at 7 dpi and continuing through 16 dpi. The values were significantlydifferent for days 11 through 15 (P < 0.001) and for day 16 (P < 0.01). (b) Male rats injected with prazosin (r, n = 20) or saline (e, n = 20)as in a. The values were significantly different for day 11 (P < 0.05) and for days 12 through 14 (P < 0.001). (c) Female rats injected with 2mg of prazosin (E, n = 20) or saline (e, n = 20) beginning at 9 dpi and continuing through 16 dpi. The values were significantly different forday 11 (P < 0.01), for days 12 and 13 (P < 0.01), and for day 14 (P < 0.01).
5916 Immunology: Brosnan et al.
Dow
nloa
ded
by g
uest
on
Apr
il 5,
202
0

Proc. Nati. Acad. Sci. USA 82 (1985) 5917
x
'oa.
8 9 0 11 12 13 14 15 16 17 18 19 20 21Days Postinoculation
FIG. 2. CI of female rats injected twice daily i.p. with differentdoses of prazosin beginning at 7 dpi and continuing through 16 dpi.O, Saline; *, 0.5 mg twice daily; e, 1.0 mg twice daily; A, 2.0 mg twicedaily; and *, 2.5 mg twice daily.
blockade in prazosin-mediated suppression of EAE, severalother drugs known to act on adrenergic receptors were testedin rats sensitized with guinea pig spinal cord. As shown inTable 1, phenoxybenzamine, a relatively nonspecific antag-onist with 100-fold more potent activity against the a,- thana2-receptor subgroup (16), was able to suppress EAE to thesame extent as prazosin but had to be discontinued becauseof toxic effects (distended abdomen and aggressive behav-ior). Yohimbine, a selective a2-receptor antagonist, exacer-bated EAE when injected in small doses. To determinewhether modulation of 8-receptor activity could affect theclinical course of EAE, rats were treated with propranolol, a
p-receptor antagonist, and with isoproterenol, a a-receptoragonist. Isoproterenol did not alter the severity or duration ofdisease to a significant degree. Propranolol, at a dose of 1 mgtwice a day exacerbated and extended the duration of clinicaldisease in both male and female animals. The animalsdeveloped severe EAE and the drug was discontinued after14 dpi. With the cessation of propranolol treatment theanimals recovered rapidly. These data indicate that the abilityof prazosin to suppress EAE is most likely due to blockadeof the a,-receptor.Inflammatory Response in the Spinal Cord of Prazosin-
Treated Rats. Inflammatory cell infiltration into the spinalcord of prazosin-treated and saline-treated animals was
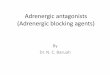
evaluated histologically. At 10 dpi, neither group showedevidence of inflammation but by 13 dpi widespread diffuseinflammation was evident in saline-treated female rats (Fig.3 a and b). Although the inflammatory response began tosubside by 15 dpi, perivascular cuffs were present at 20 dpi,well after the animals had completely recovered from clinicalsigns of EAE. In prazosin-treated animals, the initial infil-tration of inflammatory cells into the spinal cord was re-
duced. At 13 dpi some perivascular and submeningeal in-flammation was observed (Fig. 3 c and d), but it was markedlyless than in the saline-treated controls. By 15 dpi, however,
inflammation in the prazosin-treated animals was extensive,and by 20 dpi inflammation was indistinguishable from thesaline-treated animals.
Passive Transfer of EAE. Ten days after Lewis rats were
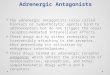
sensitized with guinea pig myelin, the lymph node cells andspleen cells were removed and incubated in vitro for 3 daysin the presence of guinea pig MBP according to the methodofPanitch and McFarlin (3). On day 0 the activated cells wereinjected into the tail veins of naive female Lewis rats and onday 1 treatment with prazosin at 2 mg or saline twice a daywas initiated. In rats receiving lymph node cells (six animalsper group, Fig. 4a), clinical signs consisting of flaccid tailswere first observed in the saline-treated group at 4 dpi. TheCI peaked at 6 dpi (CI = 2.5 + 0.7) and had returned to 0 by8 dpi. In the prazosin-treated group, clinical signs consistingof marginally flaccid tails with no weight loss were observedin only two animals (CI = 0.3) on day 6. These animals were
followed through 13 dpi and no clinical relapses were detect-ed in either group. In the rats that had received spleen cells(three animals per group) and had been treated with saline,clinical signs became apparent at 5 dpi and escalated through7 dpi. All animals had a CI of 3.0. In the prazosin-treatedgroup clinical signs were only observed in one of the threeanimals, with a CI of 1+ on day 5, 2+ on day 6, and 1+ onday 7. The other two animals were clinically uninvolved. Onday 7 the animals in both groups were sacrificed for histologyby whole-body perfusion. Epon and paraffin blocks wereprepared from the cord of each animal at the lumbar,thoracic, and cervical levels. Histological sections showedperivascular inflammation in both groups but to a lesserextent in the prazosin-treated group than in the saline-treatedgroup. Lesions were more extensive in the lumbar regionthan in other regions of the cord.
DISCUSSIONPrazosin is the most specific a1-adrenergic receptor antago-nist available (17). Its antihypertensive activity is the resultof vasodilation, believed to be caused by blockade of vas-cular a1-adrenergic receptors, with little effect on pre-synaptic a2-neuronal receptors. It is 10 times more potent, ona molar basis, than phentolamine, a mixed a1/a2-antagonist,in inhibiting the vasoconstrictive action of norepinephrine.When prazosin is administered in hypotensive doses,tachycardia and increased renin release are relatively infre-quent, probably because of the absence of blocking activityagainst the presynaptic a-receptor and the combined actionof the drug in reducing vascular tone in both resistance(arterioles) and capacitance (veins) beds (13, 18-20). there islittle evidence to support a CNS site of action for prazosinand, consistent with a specific a1-adrenergic receptor effect,it does not have any demonstrable ganglionic, vagal, X3-blocking, or sympathetic neuronal-blocking properties (19,20).A role for the a,-receptor in EAE is supported by our
finding that the long-acting mixed a1/a2-receptor antagonist
Table 1. CI of female Lewis rats at 13 dpi that had been injected i.p. twice daily beginning at 7dpi with antagonists and agonist of the adrenergic receptor
Dose twiceDrug daily, mg CI SEM P value n Receptor action
Prazosin 2 0.6 0.1 0.001 67 a,-AntagonistPhenoxybenzamine 2 0.4 0.2 0.001 15 al/a2-AntagonistYohimbine 0.1 4.0 0 0.01 11 a2-AntagonistPropranolol 1 3.6 0.2 NS 11 f-Antagonist
0.1 2.7 0.5 NS 5 8-AntagonistIsoproterenol 0.1 2.8 0.2 0.5 10 (-AgonistDoses used were based on data obtained from the handbook ofdrug dosage in laboratory animals (15).
NS, not significant.
Immunology: Brosnan et al.
Dow
nloa
ded
by g
uest
on
Apr
il 5,
202
0

Proc. Natl. Acad. Sci. USA 82 (1985)
\ P* -I ' s.q:oA
A:,Wf,4+~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~1S,~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~O
Z-~~~~~~~ ;4Ad e ft. At
t'~~'-~'4' 9 ,,',
' 4 - is > *'-'4 ' e ,
.FX.4~t,..;'.'.m-,^',.' "dc t w .sv 'v' t X 'am- - ''; *4'
I* *~~- 4 4'. I,-1..4
I,
I
.4
:9
FIG. 3. Hematoxylin/eosin-stained sections from the lumbar region of the spinal cord of rats sensitized for EAE 13 days previously.Extensive perivascular infiltration is evident in the saline-treated animals (arrows) in a (x40) and b (x 150), whereas in the animals treated withprazosin no inflammation was evident either at low (c, x40) or high magnification (d, x 150).
phenoxybenzamine also suppressed disease. The exacerba-tion of EAE by yohimbine, an a2-antagonist, is also consist-ent with this postulate. The presynaptic a2-receptor exerts anegative-feedback control on transmitter release; thus antag-onism of this receptor could lead to unrestrained release ofnorepinephrine. The exacerbation of EAE by propranolol isinteresting and supports the speculation that epinephrine,acting through 3-receptor-mediated changes in adenyl cy-clase activity, may oppose the effect of other vasoactiveamines in promoting vascular permeability (8, 21-23).
It is clear that alteration in blood-brain-barrier permeabil-ity is an early and significant event in EAE. Several studieshave shown that clinical signs of disease correlate moreclosely with the extent of edema in the spinal cord than withhistological evidence of inflammation (24-26). The factorsinvolved in this alteration of blood-brain-barrier function arenot well understood, but in the mouse the histamine-sensi-tizing factor of Bordetella pertussis appears to play a majorrole (27, 28). Furthermore, in the Lewis rat EAE can bereactivated by resensitizing the animal with MBP plus CFAplus B. pertussis (8). In both the mouse model and thereactivated rat model (but not in the primary clinical episodein the rat) antagonists of histamine can suppress clinical signsof disease, thus implicating this vasoactive amine in thedisease process. In addition to a role in edema, a requirementfor vasoactive amines in the development of a DTH reactionhas been proposed (6). In DTH reactions the augmentinginflammatory response is known to play a major role in theinitiation of tissue damage (29). This augmenting inflamma-tory response consists primarily of cells of the monocyte/macrophage lineage that do not normally leave the blood.Gershon et al. (6) have suggested that vasoactive aminescause constriction ofthe endothelial cells, thus facilitating the
egress of the bone marrow-derived cells from the circulation.In the mouse serotonin appeared to be the major mediator,consistent with the observations of Majno and Palade thatendothelial cells were 100-fold more sensitive to serotoninthan to histamine (30). When this hypothesis was tested inexperimental allergic neuritis in the Lewis rat, the resultssupported a role for serotonin (but not histamine) in thisautoimmune disease but also suggested a role for catechol-amines (9). Thus, prazosin, by blocking a vasoconstrictiveevent, could suppress clinical signs of EAE by preventingeither the augmenting inflammatory event or vascular edema,or both.
In addition to effects on vascular tone, catecholaminescould modulate the immune response through interactionwith cell-surface receptors. As early as 1936 (31) it wasknown that epinephrine could inhibit the release of histaminethat occurred during the course of an anaphylactic reaction inguinea pig lung. Subsequent work showed a /-adrenergicreceptor to be involved; however, attempts to define theP-receptor subgroup have been inconclusive (32). /3-Receptoragonists (epinephrine and/or isoproterenol) have also beenfound to enhance the activity of cytotoxic T cells (33),suppress antibody production (34, 35), and affect lymphocyteproliferation following mitogen stimulation (36). Further-more, catecholamines enhance the synthesis of complementcomponents by monocytes. This effect is abrogated byprazosin and the mixed a1/a2-receptor antagonistphentolamine but not by the /-receptor antagonist propran-olol, results that define the monocyte receptor as belongingto the a1-subclass (37). Thus, antagonists of adrenergicreceptors could modify the immune response by severalmechanisms. However, with the exception of the monocytereceptor, very little information is available on the distribu-
5918 Immunology: Brosnan et al.
-;I-
Dow
nloa
ded
by g
uest
on
Apr
il 5,
202
0

Proc. Natl. Acad. Sci. USA 82 (1985) 5919
20
1.5
0 2 3 4 5 6 7 8 9a
3.0
2.5
2.0
1.5
1.0
0.5
0
AR/\,0 2 3 4 5
Days Postinoculation6 7
FIG. 4. CI of prazosin-treated and saline-treated female rats withEAE induced by adoptive transfer. Data are expressed as the mean± SEM. (a) Female rats sensitized by i.v. inoculation of activatedlymph node cell (4 x 10') and injected twice daily beginning at 1 dpiwith prazosin (r, n = 6) or saline (e, n = 6). (b) Female rats injectedwith activated spleen cells as in a and injected with prazosin (0, n =
3) or saline (a, n = 3) until 7 dpi, when they were perfused forhistological examination.
tion and role of a1-adrenergic receptors on cells of theimmune system. We recognize, however, that prazosin couldhave effects on the immune system that are as yet undiscov-ered.At the present time our data show that treatment with
prazosin significantly suppresses the clinical and histologicalexpression of EAE in the Lewis rat. The suppression ofclinical signs consists of both a reduction in severity and adelay in peak incidence of disease and appears to be completesince clinical relapse was not observed following cessation oftreatment or during a 30-day follow-up period. Suppression ofhistological signs is, however, incomplete since by 20 dpi theextent of inflammation is similar in prazosin- and saline-treated animals. Unpublished results show that prazosin alsosuppresses the CNS edema but has little effect on lymphocyteresponses to the sensitizing antigens MBP and PPD (thepurified protein derivative of the tubercle bacilli present inCFA) or to the T-cell mitogen concanavalin A. Additionalexperiments in vivo have shown that treatment with prazosincommencing on day 10 or 11 has some suppressive activity,whereas treatment on days 1 through 6 has no effect onclinical expression of disease, indicating that prazosin acts onthe effector but not the inductive phase of the disease. Thus,although we must consider that prazosin could act on both thevasculature and the immune system, the data are reasonablyconsistent with a postulate that its primary action is on thevasculature. The fact that prazosin also suppresses clinicalsigns of EAE in animals sensitized by adoptive transfer withactivated lymph node or spleen cells provides an additionalmodel system in which to pursue the question of the mech-anism of action of this drug in the absence of adjuvant andexogenous antigen.
We thank Camille Basile and Clemens Cayetano for technicalassistance. This research was supported by Public Health ServiceGrants NS 11920, NS 02476, NIHR GOO-83-00040, and T32 GM 7288and by Grants 1089 and 1006 from the National Multiple SclerosisSociety.
1. Paterson, P. Y. (1976) in Textbook ofImmunopathology, eds.Meischer, P. A. & Muller-Eberhard, H. J. (Grune & Stratton,New York), pp. 179-213.
2. Werdelin, 0. & McCluskey, R. T. (1971) J. Exp. Med. 133,1242-1263.
3. Panitch, H. S. & McFarlin, D. E. (1977) J. Immunol. 119,1134-1137.
4. Swanborg, R. H. (1983) J. Immunol. 130, 1503-1505.5. Hickey, W. F., Gonatas, N. K., Kimura, H. & Wilson, D. B.
(1983) J. Immunol. 131, 2805-2809.6. Gershon, R. K., Askenase, W. W. & Gershon, M. D. (1975) J.
Exp. Med. 142, 732-747.7. Linthicum, D. S. & Frelinger, J. A. (1982) J. Exp. Med. 155,
31-40.8. Waxman, F. J., Taguiam, J. M. & Whitacre, C. C. (1984) Cell.
Immunol. 85, 82-93.9. Brosnan, C. F. & Tansey, F. A. (1984) J. Neuropathol. Exp.
Neurol. 43, 84-93.10. Goldmuntz, E. A., Brosnan, C. F., Chiu, F.-C., Cammer, W.
& Norton, W. T. (1984) Trans. Am. Soc. Neurochem. 15, 230a(abstr.).
11. Norton, W. T. & Poduslo, S. (1973) J. Neurochem. 21,749-757.
12. Brosnan, C. F., Bornstein, M. B. & Bloom, B. R. (1981) J.Immunol. 126, 614-620.
13. Hess, H. J. (1974) in Prazosin-Evaluation of a New Hyper-tensive Agent, ed. Cotton, D. W. K. (Excerpta Medica,Amsterdam), pp. 3-15.
14. Richert, J. R., Kies, M. W. & Alvord, E. C., Jr. (1983)Neurochem. Pathol. 1, 81-90.
15. Barnes, C. D. & Eltherington, L. G. (1973) Drug Dosage inLaboratory Animals (Univ. Cal. Press, Los Angeles).
16. Weiner, N. (1980) in The Pharmacologic Basis of Therapeu-tics, eds. Gilman, A. G., Goodman, L. S. & Gilman, A.(MacMillan, New York), p. 178.
17. Ruffolo, R. R., Jr. (1984) Fed. Proc. Fed. Am. Soc. Exp. Biol.43, 2910-2916.
18. Cavero, I. & Roach, A. G. (1980) Life Sci. 27, 1525-1540.19. Graham, R. M. & Pettinger, W. A. (1979) N. Engl. J. Med.
300, 232-236.20. McGrath, J. C. (1983) Trends Pharmacol. Sci. 3, 14-18.21. Green, K. L. (1972) Br. J. Pharmacol. 45, 322-332.22. Bergman, R. K., Munoz, J. J. & Portis, J. L. (1978) Infect.
Immun. 21, 627-635.23. O'Donnell, S. R. & Persson, C. G. A. (1978) Br. J.
Pharmacol. 62, 321-324.24. Oldstone, M. B. A. & Dixon, P. J. (1968) Am. J. Pathol. 52,
251-263.25. Leibowitz, S. & Kennedy L. (1972) Immunology 22, 859-869.26. Stohl, W., Kaplan, M. S. & Gonatas, N. K. (1979) J. Immu-
nol. 122, 920-925.27. Linthicum, D. S., Munoz, J. J. & Blaskett, A. (1982) Cell.
Immunol. 73, 299-310.28. Linthicum, D. S. (1982) Immunobiology 162, 211-220.29. Waksman, B. H. & Adams, R. D. (1962) Am. J. Pathol. 41,
135-146.30. Majno, G. & Palade, G. E. (1961) J. Biophys. Biochem. C vtol.
11, 571-626.31. Schild, H. 0. (1936) Q. J. Exp. Physiol. 26, 165-179.32. Butchers, P. R., Skidmore, I. F., Vardey, C. J. & Wheeldon,
A. (1980) Br. J. Pharmacol. 71, 663-667.33. Henney, C. S., Bourne, H. R. & Lichtenstein, L. M. (1972) J.
Immunol. 108, 1526-1534.34. Ishizuka, M., Braun, W. & Matsumato, T. (1971) J. Immunol.
107, 1027-1035.35. Melmon, K. L., Bourne, H. R., Weinstein, Y., Sheaver,
G. M., Bauminger, S. & Kram, J. (1974) J. Clin. Invest. 53,13-21.
36. Hirschhorn, R., Grossman, R. & Weissman, G. (1970) Proc.Soc. Expt. Biol. Med. 133, 1361-1365.
37. Lappin, D. & Whaley, K. (1982) Clin. Exp. Immunol. 47,606-612.
Immunology: Brosnan et al.
Dow
nloa
ded
by g
uest
on
Apr
il 5,
202
0