Embed Size (px)
Citation preview

INTRODUCTIONNARCOLEPSY IS CHARACTERIZED BY UNCONTROL-LABLE SLEEPINESS (ALSO CALLED EXCESSIVE DAY-TIME SLEEPINESS) AND INTERMITTENT MANIFESTA-TIONS OF REM SLEEP AT TIMES WHEN A PERSONWOULD NORMALLY BE AWAKE. Beside sleepiness, theREM manifestations may include cataplexy, sleep paralysis, andhypnagogic hallucinations. Narcolepsy is not a common disease.The largest population study estimates the prevalence of nar-colepsy at 26 per 100,000 people in Finland, which is similar tothe prevalence of myasthenia gravis, Marfan’s syndrome, sys-temic lupus erythematosis, and Crohn’s disease. The actualprevalence may be higher in the United States,1 where approxi-mately 5% of patients seen at AASM accredited sleep disordercenters have narcolepsy.2
Narcolepsy has clinical importance which exceeds its preva-lence. A lifelong, often disabling, condition such as narcolepsydemands that many health care providers besides sleep special-ists must be familiar with optimum treatments. Sleep attacksassociated with narcolepsy can lead to serious accidents or lossof employment, so treatment to reduce excessive sleepiness hasclinical and societal value. Nevertheless, many health careproviders are overly cautious in approaching treatment of nar-colepsy, because stimulant medications, which are the mainstayof narcolepsy treatment, are regulated by government agencies toprevent abuse.
Because of the importance of narcolepsy treatment, theAmerican Academy of Sleep Medicine (AASM) sponsored areview paper on the use of stimulants for treatment of narcolep-sy in 1994.3 Based on that review, the Standards of Practice
Committee (SPC) of the AASM published practice parameters onnarcolepsy therapy with stimulants4
Since publication of the initial review and practice parametersseveral developments have occurred. Researchers have identifieda potential biochemical basis of narcolepsy in dogs andhumans.5,6 The genetic defect in canine narcolepsy associatedwith cataplexy results in a nonfunctional receptor (OX2R) forhypocretin (orexin), a neurotransmitter previously associatedwith feeding behavior and energy metabolism. In humans,hypocretin is reduced or undetectable in many but not all patientswith narcolepsy associated with cataplexy. Also, the UnitedStates Food and Drug Administration (FDA) approved modafinilfor treatment of narcolepsy. There is optimism that theseresearch and clinical developments will result in better treatmentand quality of life for patients with narcolepsy.
In 1999, the Agency for Healthcare Research and Quality inpartnership with the American Medical Association (AMA) andthe American Association of Healthplans, established theNational Guideline Clearinghouse™ (NGC), a comprehensivedatabase of evidence-based clinical practice guidelines and relat-ed documents. The clearinghouse provides a central repositoryof practice parameters from all medical specialties. To be listed,practice parameters must have been developed, reviewed, orrevised every five years and must be based on a systematicreview of scientific evidence published in peer-reviewed jour-nals.7
In view of the new treatments, basic research advances, andthe NGC protocol, the AASM decided to update the practiceparameters for treatment of narcolepsy. This update concernsadvances in therapy for narcolepsy since the publication of theexpert review;3 grades the evidence available; and modifies andreplaces the1994 practice parameters.
METHODSThe SPC examined the published practice parameters and the
review upon which they were based.3,4 The references cited in
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 451
Practice Parameters for the Treatment of Narcolepsy: An Update for 2000
PRACTICE PARAMETERS
Standards of Practice Committee—Michael Littner MD,1 Stephen F. Johnson MD,2 W. Vaughn McCall MD, MS,3 W. McDowell Anderson MD,4 David Davila MD,5Kristyna Hartse PhD,6 Clete A. Kushida MD, PhD,7 Merrill S. Wise MD,8 Max Hirshkowitz PhD,9 B. Tucker Woodson MD, FACS10
1VA Greater Los Angeles Healthcare System and UCLA School of Medicine, Sepulveda, CA; 2Saint Patrick Hospital Sleep Center, Missoula, MT;3Department of Psychiatry and Behavioral Medicine, Wake Forest University School of Medicine, Winston-Salem, NC; 4College of Medicine,University of South Florida, Tampa, FL; 5Baptist Medical Center, Little Rock, AR; 6Sleep Consultants, Inc., Fort Worth, TX; 7Stanford UniversityCenter of Excellence for Sleep Disorders, Stanford, CA; 8Departments of Pediatrics and Neurology, Baylor College of Medicine, Houston, TX; 9BaylorCollege of Medicine and Houston VAMC Sleep Disorders and Research, Houston, TX; 10Department of Otolaryngology and Communication Sciences,Medical College of Wisconsin, Milwaukee, WI
Abstract: Successful treatment of narcolepsy requires an accurate diag-nosis to exclude patients with other sleep disorders, which have differenttreatments, and to avoid unnecessary complications of drug treatment.Treatment objectives should be tailored to individual circumstances.Modafinil, amphetamine, methamphetamine, dextroamphetamine,methylphenidate, selegiline, pemoline, tricyclic antidepressants, and flu-oxetine are effective treatments for narcolepsy, but the quality of published
clinical evidence supporting them varies. Scheduled naps can be benefi-cial to combat sleepiness, but naps seldom suffice as primary therapy.Regular follow up of patients with narcolepsy is necessary to educatepatients and their families, monitor for complications of therapy and emer-gent of other sleep disorders, and help the patient adapt to the disease.
Accepted for publication March 2001Address correspondence to: Standards of Practice Committee, AmericanAcademy of Sleep Medicine, 6301 Bandel Road, Suite 101, Rochester, MN55901; Tel: 507-287-6006; Fax: 507-287-6008; E-mail: [email protected]

Table 1 of the 1994 review paper were included in this reassess-ment, unless they were conference abstracts or letters to the edi-tor.3 Medline was searched from 1993 through and includingarticles published up to August 2000 with subject headings nar-colepsy or cataplexy. In addition, human clinical trials,Americans with Disabilities Act, quality of life, driving, andcompliance each were used as limiting terms. Finally, pemolineand methylphenidate were used as subject headings to discoverinformation about toxic side effects. For information about ter-atogenicity, a textbook8 about prescription medication use inpregnancy was employed and the medication graded according tothe FDA system as described in the Physicians’ Desk Reference,2000 edition. Case reports, abstracts, editorials, letters, andreviews were excluded except for reports of adverse effects oftreatments. All clinical trials of therapy were considered for theevidence tables. Case series and database articles about diagno-sis of narcolepsy were incorporated in the evidence tables only ifthey included greater than 20 subjects. Examination of the refer-ence lists from the articles found in the Medline search provideda few relevant studies from literature published prior to 1993.Evidence from the 1994 review and the updated Medline searchwas rated for the studies according to the classification outlinedin Table 1.
For an economic indicator about drug costs, the wholesaleprice, as listed in the Drug Topics Red Book Update was used.10
This is the current benchmark for drug price information.The Board of Directors of the American Academy of Sleep
Medicine reviewed the SPC for material conflicts of interest rel-evant to the recommendations and approved the final version ofthe parameters prior to publication.
On the basis of this review, the SPC of the American Academyof Sleep Medicine rated the recommendations of this paper asstandards, guidelines, and options (Table 2), based on evidence
from studies published in peer-reviewed journals that were eval-uated as noted in the evidence tables (Tables 3 and 4). However,when scientific data are absent, insufficient, or inconclusive, therecommendations were based on consensus opinion. Each rec-ommendation is based on the level and grade of the evidenceavailable, or on consensus when evidence is lacking.
These practice parameters define principles of practice thatshould meet the needs of most patients in most situations. Theseguidelines should not, however, be considered inclusive of allproper methods of care or exclusive of other methods of care rea-sonably directed toward obtaining the same results. The ultimatejudgment regarding the propriety of any specific care must bemade by health care providers in light of the individual circum-stances presented by the patient and the available diagnostic andtreatment options as resources.
The American Academy of Sleep Medicine expects theseguidelines to have a positive impact on professional behavior,patient outcomes, and, possibly, health care costs. These practiceparameters reflect the state of knowledge at the time of develop-ment and will be reviewed, updated, and revised, as new infor-mation becomes available.
RESULTSThe Medline search for narcolepsy and clinical trials yielded
29 articles, of which 14 were relevant to this paper. The Medlinesearch of narcolepsy and human returned 450 articles. In the nar-colepsy and human search, several clinical trials were foundwhich did not show up in the more limited search. The Medlinesearch for narcolepsy and compliance yielded one relevant arti-cle. The search for narcolepsy and driving yielded 26 references,of which six proved relevant. Narcolepsy and quality of lifeyielded 15 references of which three proved to contain original
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 452
Table 1—AASM classification of evidence
Recommendation Evidence StudyGrades Levels Design A I Randomized well-designed trials with low-alpha & low-beta
errors* B II Randomized trials with high-beta errors* C III Nonrandomized controlled or concurrent cohort studies C IV Nonrandomized historical cohort studies C V Case series Adapted from Sackett9*Alpha error refers to the probability (generally set at 95% or greater) that a significant result (e.g., p<0.05) is the correct conclusion of the study or stud-ies. Beta error refers to the probability (generally set at 80% or 90% or greater) that a nonsignificant result (e.g., p>0.05) is the correct conclusion of thestudy or studies. The estimation of beta error is generally the result of a power analysis. The power analysis includes a sample size analysis which pro-jects the size of the study population necessary to ensure that significant differences will be observed if actually present.
Table 2—AASM recommendations
Term Definition Standard This is a generally accepted patient care strategy which reflects a high degree of clinical certainty. The term
standard generally implies the use of Level I Evidence, which directly addresses the clinical issue, or overwhelming Level II Evidence.
Guideline This is a patient care strategy which reflects a moderate degree of clinical certainty. The term guidelineimplies the use of Level II Evidence or a consensus of Level III Evidence.
Option This is a patient care strategy which reflects uncertain clinical use. The term option implies either inconclusive or conflicting evidence, or conflicting expert opinion.
Adapted from Eddy11

data. Other articles about quality of life in narcolepsy were foundin the reference sections of these articles. Although the searchunder Americans with Disabilities Act yielded 469 references,none were directly related to narcolepsy. The search under cata-plexy yielded 169 articles, of which 36 were human clinical stud-ies, but many turned out to be case reports or small case series.Tables 3 and 4 list most of the citations on which the updatedpractice parameters are based.
RecommendationsRecommendations that are similar to, or an expansion of, pre-
vious ones and new recommendations are noted as such in thetext.
1. An accurate diagnosis of narcolepsy should be estab-lished which shall include a thorough evaluation ofother possible contributing causes, apart from nar-colepsy, to the excessive daytime sleepiness{Standard}.For patients suspected of having narcolepsy, an all-nightpolysomnogram is done primarily to ascertain the pres-ence of concurrent sleep disorders and is followedimmediately by a multiple sleep latency test50,51 (MSLT)to help confirm the diagnosis. The MSLT also helpsdetermine the severity of daytime sleepiness. The read-er is referred for diagnostic criteria33-35,50 (Table 4).Other methods to evaluate sleepiness include objectivetests such as the maintenance of wakefulness test51
(MWT), and subjective approaches such as the EpworthSleepiness Scale.52 This part of the recommendation isbased on committee consensus and is similar to a rec-ommendation made previously.4
Chronic daytime sleepiness is a nonspecific symptomand conditions that produce such sleepiness may coexistwith narcolepsy. For example, the obstructive sleepapnea syndrome (OSAS) and periodic limb movementdisorder (PLMD) may be present as determined by theresults of the all-night polysomnogram. Insufficientsleep, idiopathic hypersomnia, inadequate sleephygiene, and circadian rhythm disorders, among othersshould be considered as possible contributors to sleepi-ness independent of narcolepsy.50 Management of otherdisorders possibly contributing to sleepiness in a patientwith narcolepsy may require approaches apart fromstimulants to treat sleepiness either directly or as thera-py of the underlying condition. This part of the recom-mendation is new and is based on committee consensus.
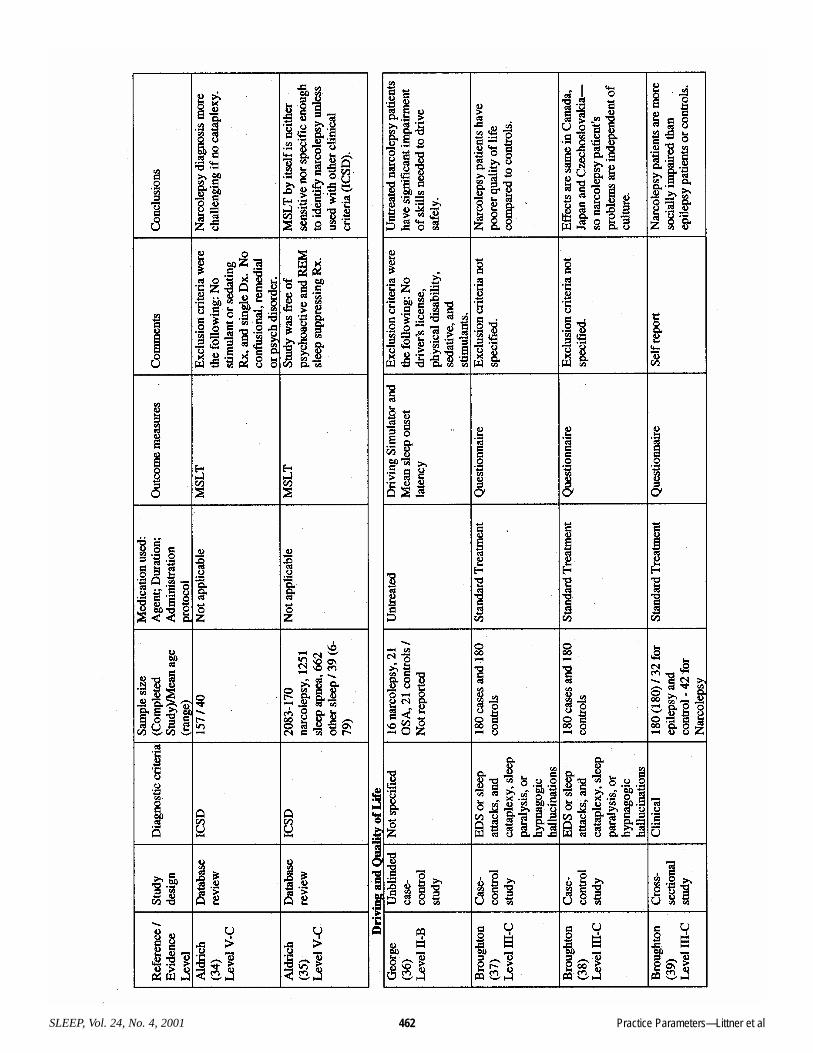
2. Individual treatment objectives should be estab-lished for each patient with narcolepsy to improvequality of life {Standard}.One level II, grade B, four level III, grade C, and onelevel V, grade C, studies, and committee consensus, pro-vide evidence that symptoms of narcolepsy mayadversely impact quality of life18,36-41 (Tables 3 and 4).In keeping with the previous practice parameters,4 amajor objective of treatment should be to alleviate day-time sleepiness with stimulants. The goal should be toproduce the fullest possible return of normal function
for patients at work, at school, at home, and socially. Anew recommendation is to control cataplexy, hypnagog-ic hallucinations, and sleep paralysis, when present andtroublesome. The health care provider should considerthe benefit-to-risk ratio of medication for an individualpatient, the cost of medication, convenience of adminis-tration, and the cost of ongoing care including possiblelaboratory tests when selecting a medication for treat-ment of narcolepsy.
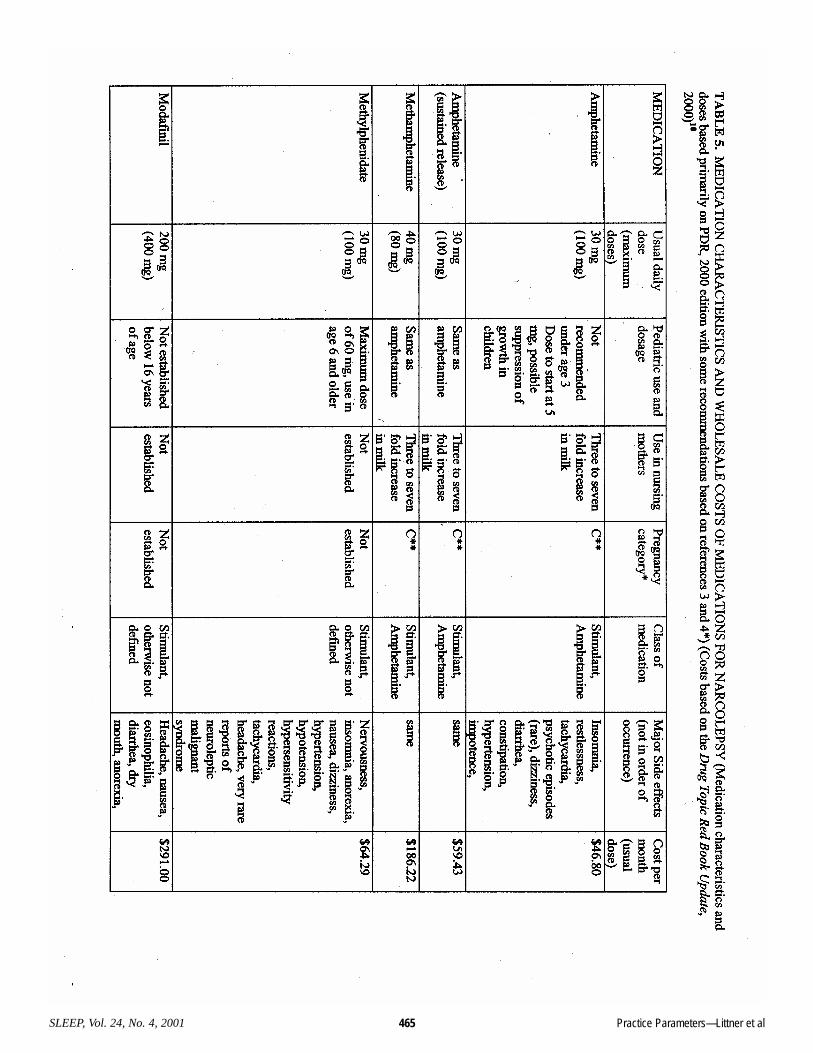
3. The following medications are effective treatmentsfor narcolepsy. Comparative safety and efficacy ofthe stimulant medications are not defined. The rat-ing of the recommendation is based on the grade ofevidence for each. See Table 5 for dosages.a. Modafinil is effective for treatment of day-
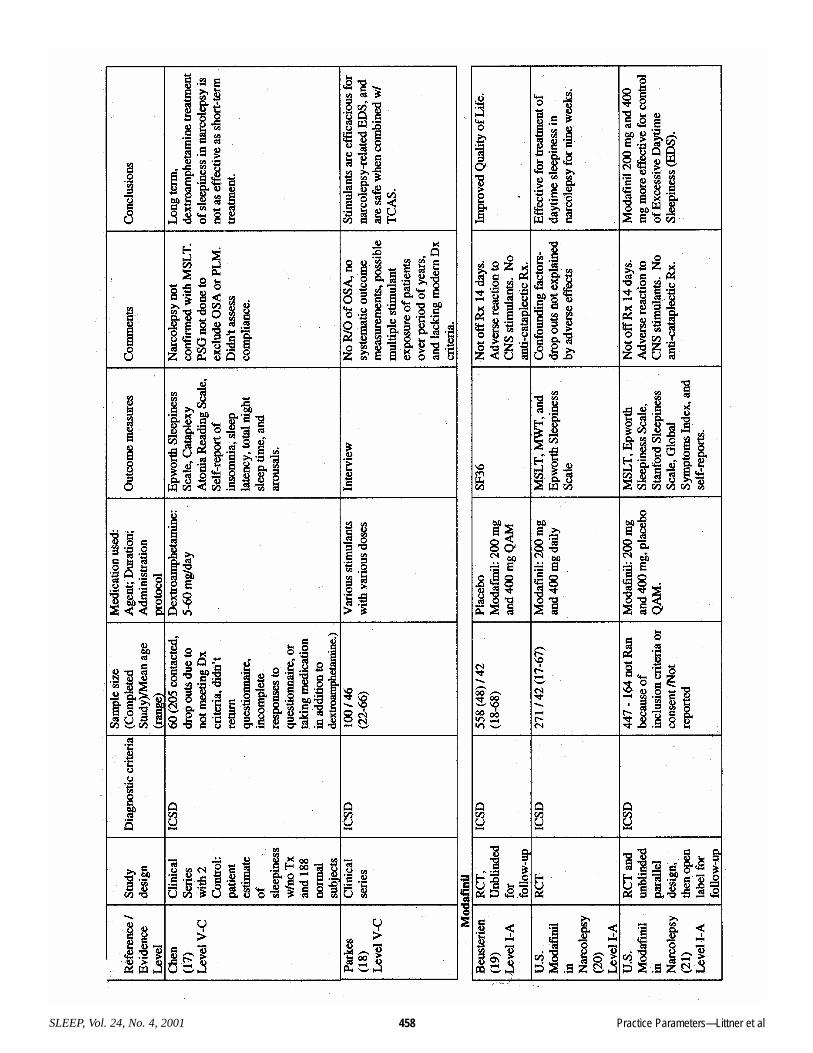
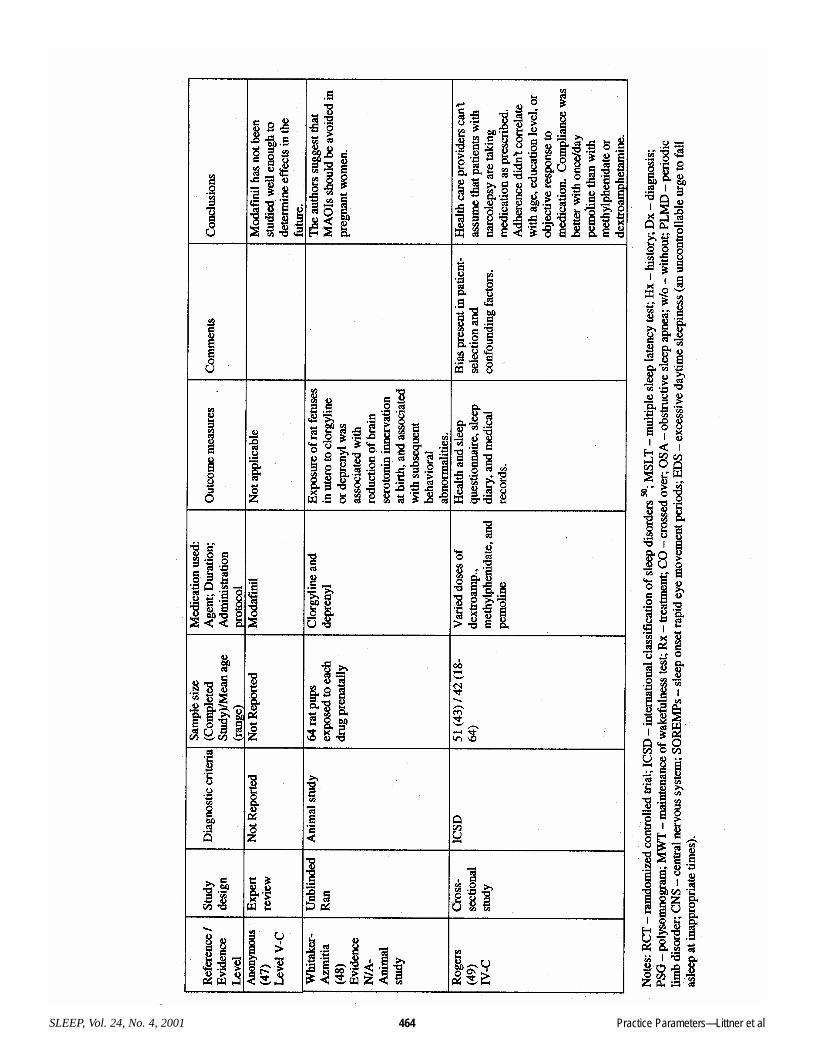
time sleepiness due to narcolepsy{Standard}. [Table 3] This conclusion isbased on the favorable benefit-to-risk ratio formodafinil established in three level I, grade Astudies with confirmation from additional stud-ies.20-27 This is a new recommendation.
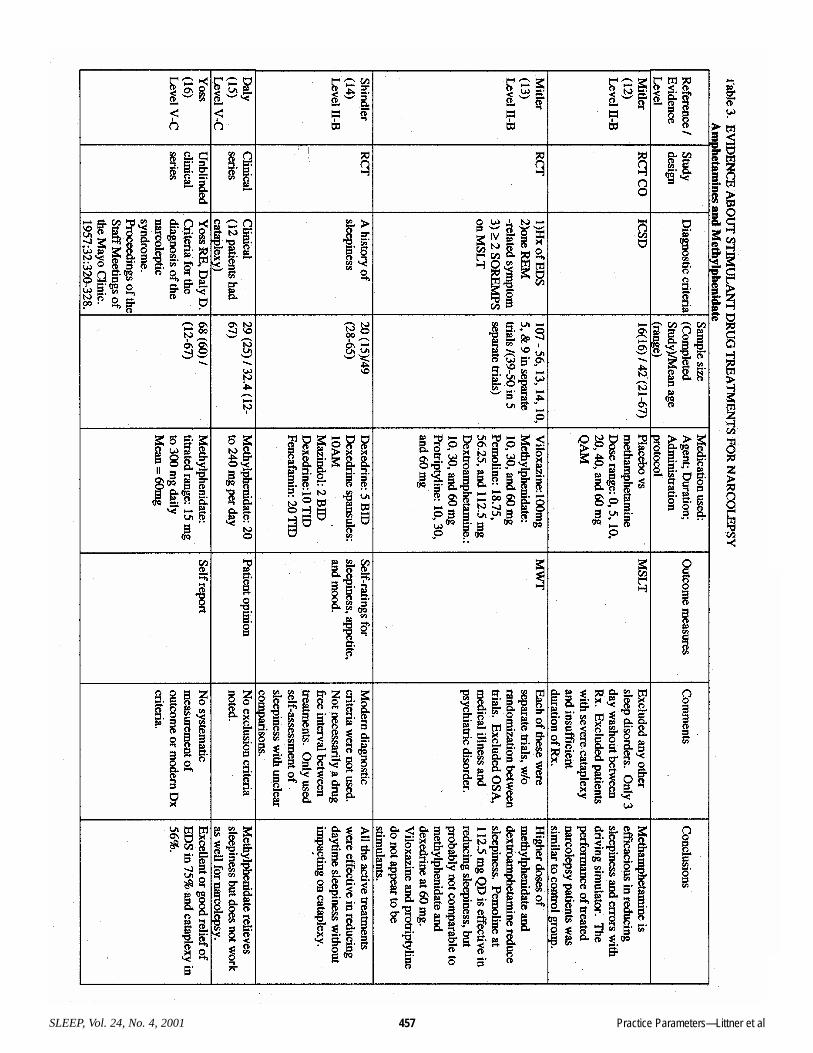
b. Amphetamine, methamphetamine, dex-troamphetamine, and methylphenidate areeffective for treatment of daytime sleepinessdue to narcolepsy {Guideline}. [Table 3]These medications are mainstays of narcolepsytreatment. Based on 3 level II, grade B and 4level V, grade C studies and long clinical prac-tice, they have a long record of efficacy.However, the benefit-to-risk ratio is not welldocumented, because the published clinical tri-als include only small numbers of patients.12-
18,53 This recommendation is similar to thatmade previously.
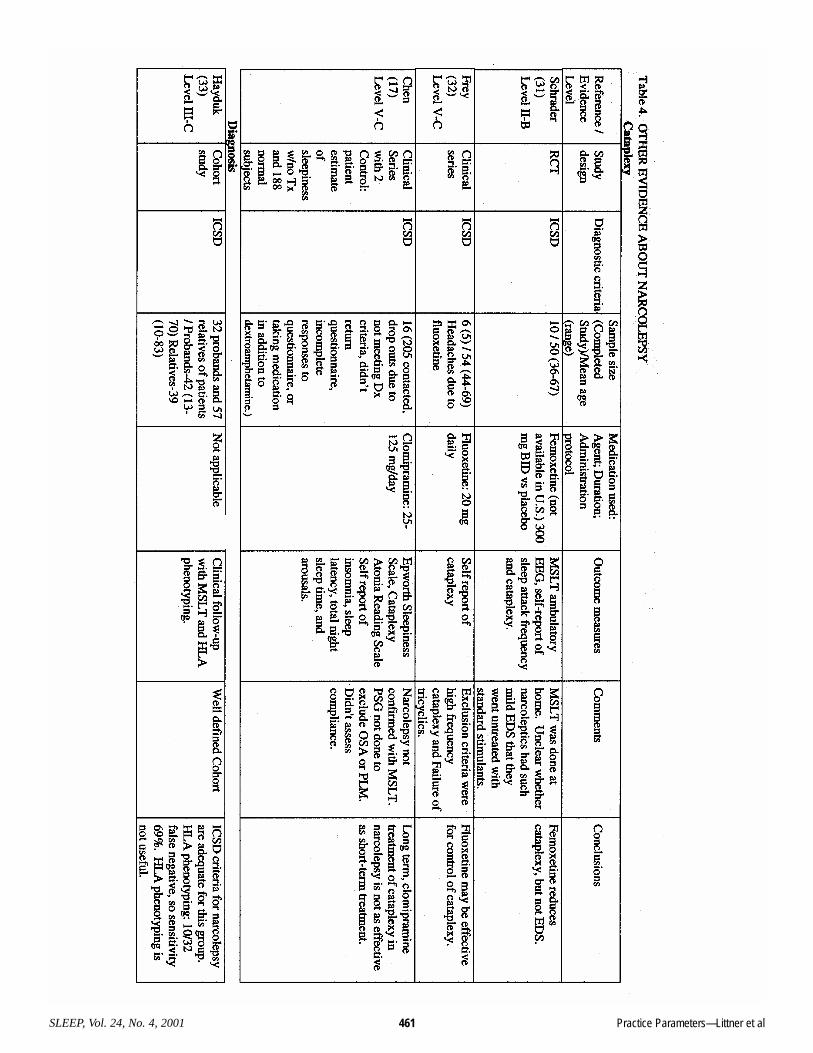
c. Selegiline is an effective treatment for allnarcoleptic symptoms {Guideline}. [Table 3]Based on two level II, grade B and one levelIV, grade C studies, selegiline is effective, butthe cost of the medication is very high, experi-ence with the high doses needed for narcolepsyis limited, and diet-induced hypertension is adanger at effective doses.28-30 This is a new rec-ommendation.
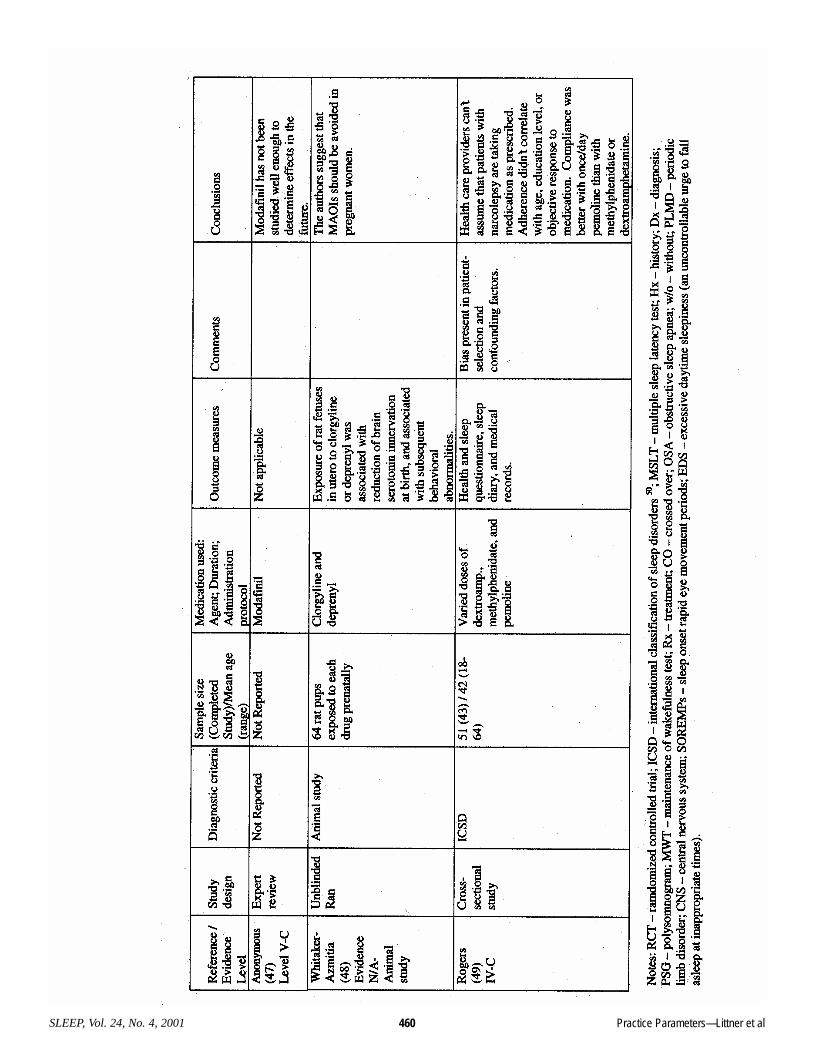
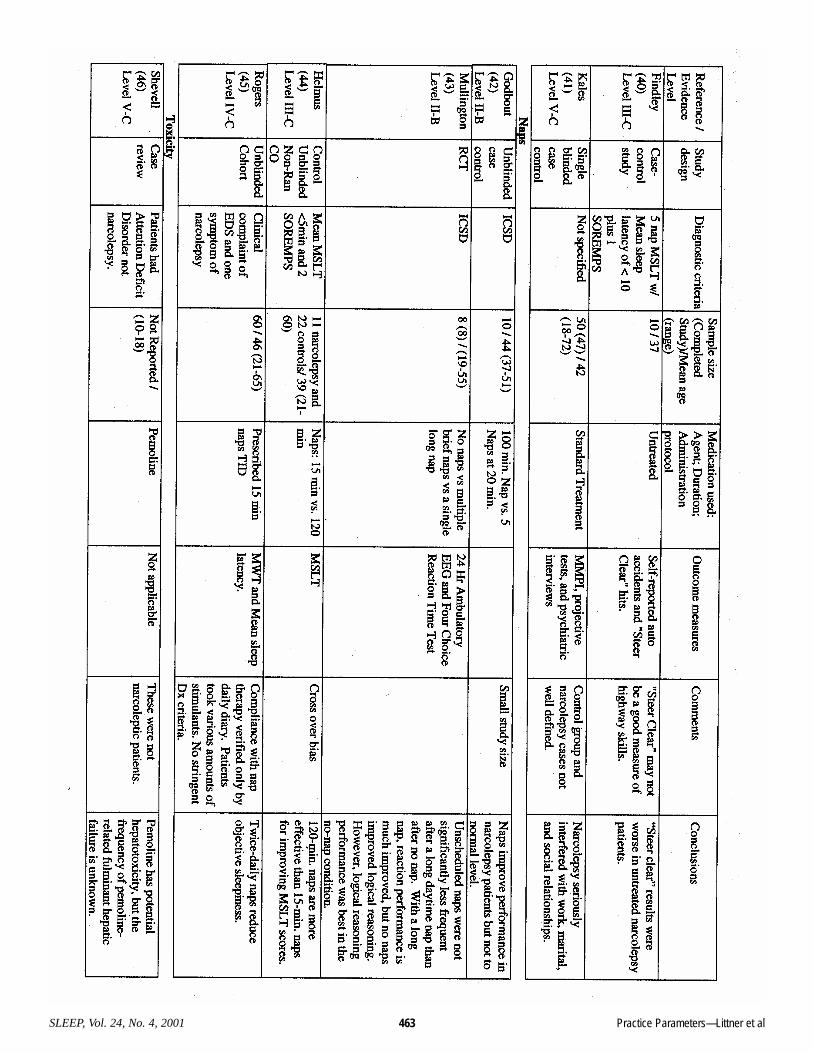
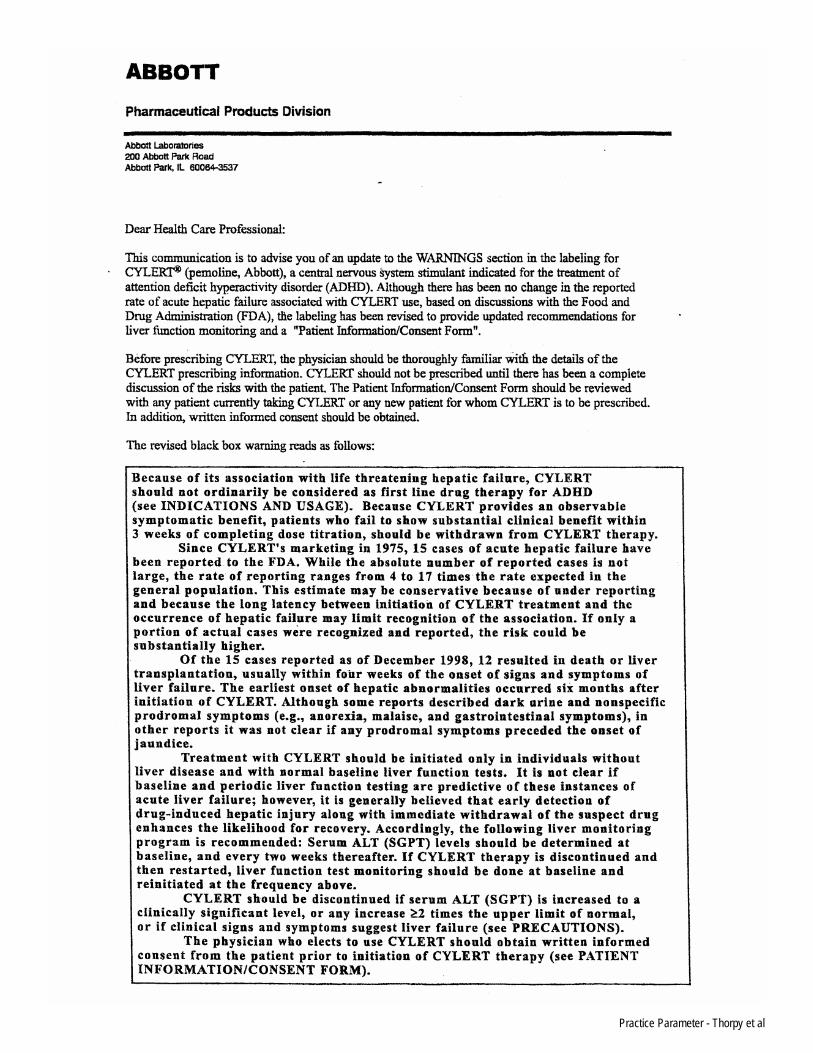
d. Pemoline is effective for treatment of day-time sleepiness in narcolepsy {Option).[Table 3] Pemoline can produce rare and poten-tially lethal liver toxicity that may be unpre-dictable. See the Appendix product alert fromAbbott Laboratories for more details and rec-ommendations for ongoing monitoring forliver toxicity. Because of this toxicity, the useof pemoline in patients with narcolepsy israrely indicated. Based on one level II, gradeB study, pemoline may be less potent thanamphetamines,13 but adherence to pemolinetherapy may be better than adherence toamphetamines or methylphenidate.49 This is amodification of a recommendation made previ-ously. In particular, the warning on liver toxic-
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 453
ity is emphasized to a greater degree than pre-viously.
e. Tricyclic antidepressants and fluoxetinemay be effective treatment for cataplexy,sleep paralysis, and hypnagogic hallucina-tions {Guideline}. [Table 4] The recommen-dation for tricyclic agents is based on one levelV, Grade C study, long clinical experience andcommittee consensus. This is a new recom-mendation. The recommendation for fluoxetineis based on one level II, grade B and one levelV, grade C study. This is a new recommenda-tion.
f. Combinations of long- and short-actingforms of stimulants may be effective forsome patients {Option}.Some stimulants have a short (3 to 4 hour)effective period (e.g., methylphenidate).Others have longer duration of activity andlonger onset of action (e.g., modafinil, sus-tained release amphetamine). By combiningstimulants with different activity characteris-tics, it may be possible to achieve alertnessquickly and for longer periods of time and alsonot produce insomnia as an unwanted sideeffect. In addition, combinations of stimulantsand antidepressants may be of benefit for treat-ment of sleepiness and REM-related symptomssuch as cataplexy. For example, modafinilappears compatible with antidepressant medi-cations, but published evidence is limited.54
This recommendation is similar to that madepreviously and is based on committee consen-sus.
4. Scheduled naps can be beneficial to combat sleepi-ness but seldom suffice as primary therapy{Guideline}. [Table 2] This recommendation is basedon two level II, grade B, one level IV, grade C and onelevel V, grade C studies and long clinical experience.42-
45 This recommendation is similar to that made previ-ously.
5. Regular follow-up of patients with narcolepsy is nec-essary to monitor response to treatment, to respondto potential side effects of medications, and toenhance the patient’s adaptation to the disorder{Standard}. a. A patient stabilized on stimulant medication
should be seen regularly by a health careprovider at least once per year, and prefer-ably once every 6 months, to assess thedevelopment of medication side effects,including sleep disturbances, mood changes,and cardiovascular or metabolic abnormali-ties. This is the same recommendation as madepreviously and is based on committee consen-sus.
b. Follow-up is necessary to determine adher-ence and response to treatment; to monitorfor the safety of medications in individualpatients; and to assist the patient with occu-
pational and social problems. Adherence to stimulant drug treatment in nar-colepsy is impeded by inconvenient dosage,but not by age, educational level, gender, orresponse to therapy.49 Of note, many patientswith narcolepsy can not be restored to normallevels of daytime alertness, even when adher-ing to optimum doses of stimulant medications(Table 5). Most often, response to therapy canbe determined by interview of the patient andassociates as well as by self-report question-naires, such as the Epworth Sleepiness Scale.Objective measures, such as the MWT or theMSLT, may play a role when occupational orpublic safety concerns are at issue. This is anexpansion of a similar recommendation madepreviously and is based on committee consen-sus.
c. Patients with severe sleepiness should beadvised to avoid potentially dangerousactivities at home and at work, and shouldnot operate a motor vehicle until sleepinessis appropriately controlled by stimulantmedications. This recommendation is the same as that previ-ously and is based on one level II, grade B andone level III, grade B study36,40 (Table 4) andcommittee consensus.
d. Of the stimulants used to treat narcolepsy,amphetamines, especially at high doses, arethe most likely to result in the developmentof tolerance.This is the same recommendation as previous-ly. Reiteration of the discussion and literaturecited in the previous review paper3 are beyondthe scope of the current review and the readeris referred for further information.
e. Patients who fail to respond to adequatedoses of stimulant medication should becarefully assessed for other sleep disorderssuch as insufficient sleep, inadequate sleephygiene, circadian rhythm disorders,obstructive sleep apnea syndrome, or peri-odic limb movement disorder, that may con-tribute to excessive sleepiness.This is essentially the same recommendation aspreviously and is based on committee consen-sus.
f. For side effects, dosage ranges, use in preg-nancy and by nursing mothers, class of med-ication and use in narcolepsy, see Table 5. The information of Table 5 on stimulants issimilar and, in some cases, an expansion ofinformation provided previously. The informa-tion on the other classes of medications is new.Note that any of the stimulant medications canbe abused.
g. Treatment of narcolepsy withmethylphenidate in children between theages of 6 and 15 appears relatively safe, but
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 454

caution must be used if other medicationsare employed. See Table 5 for dosages.This recommendation is similar to that previ-ously and is based on the considerable experi-ence with use of methylphenidate for treatmentof attention deficit disorder.55
h. Health care providers should assist thepatient with occupational and social accom-modation for disabilities due to narcolepsy. The Americans with Disabilities Act provideslegal guidance.56 Patients deserve appropriatehelp from health care providers to insure thatthe intent of the law is realized. Because sus-tained alertness often is difficult to achieveeven with optimum treatment, some patientsshould be advised to avoid potentially danger-ous activities, such as driving, climbing, orworking in the vicinity of dangerous machin-ery, which could result in injury to the patientor others.36,40,57 This recommendation is similarto that previously and is based on committeeconsensus.
i. Polysomnographic reevaluation of patientsshould be considered if symptoms of sleepi-ness increase significantly or if specificsymptoms develop that suggest new orincreased sleep abnormalities as mightoccur in disorders such as sleep apnea orperiodic limb movement disorder. This is the same recommendation as that previ-ously and is based on committee consensus.
Further ResearchThe preparation of these practice parameters revealed signifi-
cant weaknesses in the published literature about treatment ofnarcolepsy. Better studies of diagnostic criteria are needed.Studies which explicitly consider patient preferences about ther-apeutic objectives, should be undertaken. Further research onselective serotonin reuptake inhibitors (SSRIs), including onesbesides fluoxetine available in the United States, should beundertaken. A large comparative clinical trial of amphetamine,methylphenidate, modafinil, and selegiline for treatment of nar-colepsy would be of benefit for patient management. Such astudy could establish the relative efficacy, side effects, andpatient preferences for treatments. A registry should be estab-lished to track the outcome of pregnancy in patients who takemodafinil and other stimulants that do not have adequate humandata. Treatment of cataplexy needs better assessment, and a clin-ical trial comparing fluoxetine, tricyclic agents, and placebowould be helpful to clinicians. Research about social interven-tions to improve function of narcoleptic patients at work andhome should be a priority. Gamma hydroxybutyrate is beingevaluated experimentally and may have a role to play in treatingnocturnal awakenings and cataplexy.58 However, it is notapproved by the FDA. Finally, investigation about whether casemanagement of narcolepsy patients might lead to better patientoutcomes is needed.
REFERENCES1. Hublin C, Partinen M, Kaprio J, Koskenvuo M, Guilleminault C.Epidemiology of Narcolepsy. Sleep 1994;17:S7-S12.2. Punjabi NM, Welch D, Strohl K. Sleep disorders in regional sleepcenters: A national cooperative study. Sleep 2000;23:471-480.3. Mitler MM, Aldrich MS, Koob GF, Zarcone Jr VP. Narcolepsy andits treatment with stimulants. ASDA Standards of Practice. Sleep1994;17:352-371.4. Standards of Practice Committee of the American Sleep DisordersAssociation. Practice parameters for the use of stimulants in the treat-ment of narcolepsy. Sleep 1994;17:348-351.5. Takahashi JS. Narcolepsy genes wake up the sleep field. Science1999;285:2076-2077.6. Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E.Hypocretin (orexin) deficiency in human narcolepsy. Lancet2000;355:39-40.7. National Guideline Clearinghouse. “About the National GuidelineClearinghouse (NGC).” January 9, 2000. http://www.guideline.gov/FRAMESETS/static_fs.asp?view=about (30 Oct. 2000)8. Coustan DR, Mochizuki TK. Handbook for prescribing medica-tions during pregnancy. Philadelphia, PA:Lippencott-Raven, 1998.9. Sackett D. Rules of evidence and clinical recommendation. Can JCardiol 1993;9:487-489.10. Drug topic red book update. Piscataway, NJ: Medical EconomicsPublishing Company, 2000.11. Eddy DM, A manual for assessing health practices and designingpractice policies: The explicit approach. Philadelphia, PA: AmericanCollege of Physicians, 1992.12. Mitler MM, Hajdukovic R, Erman MK. Treatment of narcolepsywith methamphetamine. Sleep 1993;16:306-317.13. Mitler MM, Hajdukovic R, Erman M, Koziol JA. Narcolepsy. JClin Neurophysiol 1990;7:93-118.14. Shindler J, Schachter M, Brincat S, Parkes JD. Amphetamine,mazindol, and fencamfamin in narcolepsy. Brit Med J 1985;290:1167-1170.15. Daly DD, Yoss RE. The treatment of narcolepsy withmethylphenylpiperidylacetate: a preliminary report. Mayo Clinic Proc1956;31:620-626.16. Yoss RE, Daly D. Treatment of narcolepsy with Ritalin.Neurology 1959;9:171-173.17. Chen SY, Clift SJ, Dahlitz MJ, Dunn G, Parkes JD. Treatment inthe narcoleptic syndrome: self assessment of the action of dexam-phetamine and clomipramine. J Sleep Res 1995;4:113-118.18. Parkes JD, Baraitser M, Marsden CD, Asselman P. Natural history,symptoms and treatment of the narcoleptic syndrome. Acta NeurolScand 1975;52:337-353.19. Beusterien KM, Rogers AE, Walsleben JA, Emsellem HA,Reblando JA, Wang L, Goswami M, Steinwald B. Health-related quali-ty of life effects of modafinil for treatment of narcolepsy. Sleep1999;22:757-765.20. U.S. Modafinil in Narcolepsy Multicenter Study Group.Randomized trial of modafinil as a treatment for the excessive daytimesomnolence of narcolepsy. Neurology 2000;54:1166-1175.21. U.S. Modafinil in Narcolepsy Multicenter Study Group.Randomized trial of modafinil for the treatment of pathological somno-lence in narcolepsy. Ann Neurol 1998;43:88-97.22. Broughton RJ, Fleming JAE, George CFP, Hill JD, Kryger MH,Moldofsky H, Montplaisir JY, Morehouse RL, Moscovitch A, MurphyWF. Randomized, double-blind, placebo-controlled crossover trial ofmodafinil in the treatment of excessive daytime sleepiness in narcolep-sy. Neurology 1997;49:444-451.23. Billiard M, Besset A, Montplaisir J, Laffont F, Goldenberg F, WeillJS, Lubin S. Modafinil: a double-blind multicentric study. Sleep1994;17:S107-S112.
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 455
24. Boivin DB, Montplaisir J, Petit D, Lambert C, Lubin S. Effects ofmodafinil on symptomatology of human narcolepsy. ClinNeuropharmaco 1993;16:46-53.25. Bastuji H, Jouvet M. Successful treatment of idiopathic hypersom-nia and narcolepsy with modafinil. Prog Neuro Psychopharmacol BiolPsychiat 1988;12:695-700.26. Laffont F, Mayer G, Minz M. Modafinil in diurnal sleepiness. Astudy of 123 patients. Sleep 1994;17:S113-S115.27. Besset A, Chetrit M, Carlander B, Billiard M. Use of modafinil inthe treatment of narcolepsy: a long term follow-up study. NeurophysiolClin 1996;26:60-66.28. Hublin C, Partinen M, Heinonen EH, Puukka P, Salmi T. Selegilinein the treatment of narcolepsy. Neurology 1994;44:2095-2101.29. Mayer G, Ewert Meier K, Hephata K. Selegiline hydrochloridetreatment in narcolepsy. A double-blind, placebo-controlled study. ClinNeuropharmacol 1995;18:306-319.30. Roselaar SE, Langdon N, Lock CB, Jenner P, Parkes JD. Selegilinein narcolepsy. Sleep 1987;10:491-495.31. Schrader H, Kayed K, Bendixen Markset AC, Treidene HE. Thetreatment of accessory symptoms in narcolepsy: a double-blind cross-over study of a selective serotonin re-uptake inhibitor (femoxetine) ver-sus placebo. Acta Neurol Scand 1986;74:297-303.32. Frey J, Darbonne C. Fluoxetine suppresses human cataplexy: apilot study. Neurology 1994;44:707-709.33. Hayduk R, Flodman P, Spence MA, Erman MK, Mitler MM. HLAhaplotypes, polysomnography, and pedigrees in a case series of patientswith narcolepsy. Sleep 1997;20:850-857.34. Aldrich MS. Diagnostic aspects of narcolepsy. Neurology1998;50:S2-S7.35. Aldrich MS, Chervin RD, Malow BA. Value of the multiple sleeplatency test (MSLT) for the diagnosis of narcolepsy. Sleep 1997;20:620-629.36. George CFP, Boudreau AC, Smiley A. Comparison of simulateddriving performance in narcolepsy and sleep apnea patients. Sleep1996;19:711-717.37. Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, Nevsimalova S,Roth B. Life effects of narcolepsy in 180 patients from North America,Asia and Europe compared to matched controls. Can J Neurol Sci1981;8:299-304.38. Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, Nevsimalova S,Roth B. Life effects of narcolepsy: relationships to geographic origin(North American, Asian or European) and to other patient and illnessvariables. Can J Neurol Sci 1983;10:100-104.39. Broughton RJ, Guberman A, Roberts J. Comparison of the psy-chosocial effects of epilepsy and narcolepsy/cataplexy: a controlledstudy. Epilepsia 1984;25:423-433.40. Findley L, Unverzagt M, Guchu R, Fabrizio M, Buckner J, SurattP. Vigilance and automobile accidents in patients with sleep apnea ornarcolepsy. Chest 1995;108:619-624.41. Kales A, Soldatos CR, Bixler EO, Caldwell A, Cadieux RJ,Verrechio JM, Kales JD. Narcolepsy-cataplexy. II. Psychosocial conse-quences and associated psychopathology. Arch Neurol 1982;39:169-171.42. Godbout R, Montplaisir J. All-day performance variations in nor-mal and narcoleptic subjects. SLEEP 1986;9:200-4.43. Mullington J, Broughton R. Scheduled naps in the management ofdaytime sleepiness in narcolepsy- cataplexy. Sleep 1993;16:444-456.44. Helmus T, Rosenthal L, Bishop C, Roehrs T, Syron ML, Roth T.The alerting effects of short and long naps in narcoleptic, sleep deprived,and alert individuals. SLEEP 1997;20:251-257.45. Rogers AE, Aldrich MS. The effect of regularly scheduled naps onsleep attacks and excessive daytime sleepiness associated with nar-colepsy. Nurs Res 1993;42:111-117.46. Shevell M, Schreiber R. Pemoline-associated hepatic failure: acritical analysis of the literature. Pediatr Neurol 1997;16:14-16.47. Anonymous. Modafinil for narcolepsy. Med Lett Drugs Ther1999;41:30-31.48. Whitaker-Azmitia PM, Zhang X, Clarke C. Effects of gestational
exposure to monoamine oxidase inhibitors in rats: preliminary behav-ioral and neurochemical studies. Neuropsychopharmacology1994;11:125-32.49. Rogers AE, Aldrich MS, Berrios AM, Rosenberg RS. Compliancewith stimulant medications in patients with narcolepsy. Sleep1997;20:28-33.50. American Sleep Disorders Association. (ICSD) international classi-fication of sleep disorders, revised: diagnostic and coding manual.American Sleep Disorders Association, 1997.51. Michael J. Thorpy, MD, Philip Westbrook, Richard Ferber, MD,Paul Fredrickson, MD, Mark Mahowald, MD Francisco Perez-Guerra,MD, Martin Reite, MD, Philip Smith, MD, The clinical use of the mul-tiple sleep latency test. Sleep, 1992;15:268-276.52. Johns MW. A new method for measuring daytime sleepiness: theEpworth sleepiness scale. Sleep 1991;14:540-5.53. Saletu B, Frey R, Krupka M, Anderer P, Grunberger J, BarbanojMJ. Differential effects of a new central adrenergic agonist—modafinil—and D-amphetamine on sleep and early morning behaviourin young healthy volunteers. Int J Clin Pharmacol Res 1989;9:183-195.54. Wallin MT, Mahowald MW. Blood pressure effects of long-termstimulant use in disorders of hypersomnolence. J Sleep Res 1998;7:209-215.55. Stevenson RD, Wolraich ML. Stimulant medication therapy in thetreatment of children with attention deficit hyperactivity disorder.Pediatr Clin North Am 1989;36:1183-97.56. Anfield RN. Americans with Disabilities Act of 1990. A primer ofTitle I provisions for occupational health care professionals. J OccupMed 1992;34:503-509.57. Pakola SJ, Dinges DF, Pack AI. Review of regulations and guide-lines for commercial and noncommercial drivers with sleep apnea andnarcolepsy. Sleep 1995;18:787-796. 58. Broughton R, Mamelak M. Gamma-hydroxy-butyrate in the treat-ment of narcolepsy: a preliminary report. In: Guilleminault C, DementWC, Passouant P, eds. Narcolepsy: advances in sleep research, vol. 3.New York: Spectrum Publications, 1976:659-67.
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 456
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 457
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 458

Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 459
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 460
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 461
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 462
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 463
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 464
Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 465

Practice Parameters—Littner et alSLEEP, Vol. 24, No. 4, 2001 466
Practice Parameter - Thorpy et al
Practice Parameter - Thorpy et al




![Narcolepsy treatment: pharmacological and behavioral ... · narcolepsy type 2 (NT2), formerly narcolepsy without cata-plexy and with normal hypocretin levels [1]. Hypocretin isa neurotransmitterinvolvedin](https://img.dokumen.tips/doc/110x75/60a115bf092a2c54425c9eaf/narcolepsy-treatment-pharmacological-and-behavioral-narcolepsy-type-2-nt2.jpg)