Embed Size (px)
Citation preview
PRACTICAL APPROACH
TO THE PATIENT WITH
GAIT AND BALANCE
DISORDERS
PT Sheila Klufio
PT Mary Agoriwa

This is a neurodegenerative disorder that
is progressive in nature.
It is characterized by 4 main cardinal signs
Rigidity
Tremor
Bradykinesia
Postural instability
PD leads to abnormalities in two main components of postural control:
Orientation Maintaining a normal postural arrangement and alignment.
Stabilization Maintaining equilibrium(Vaugoyeau & Azulay, 2010).

The most frequent orientation difficulty that
PD patients present are
Stooped posture
Moderate flexion of the knees and trunk,
Bent or flexed elbows
Adducted arms


Other postural abnormalities include
Antecolli
This is marked or extreme neck flexion, minimum of 45º
Patient is unable to fully extend the neck against gravitybut able to exert force against resistance of theexaminer’s hand.
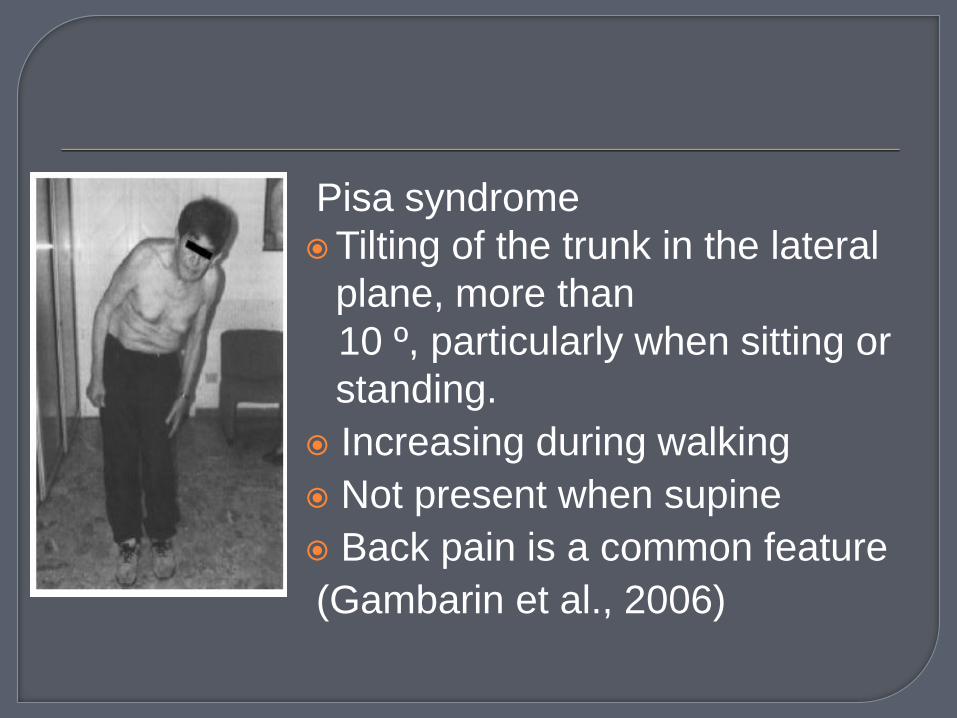
Pisa syndrome
Tilting of the trunk in the lateral
plane, more than
10 º, particularly when sitting or
standing.
Increasing during walking
Not present when supine
Back pain is a common feature
(Gambarin et al., 2006)

Camptocormia
Abnormal posture of the trunk in the
antero- posterior plane with marked flexion
of the thoracolumbar spine.(Azher &
Jankovick, 2005).

PI is a disabling disorder, associated with
sudden falls
progressive loss of independence
immobility
(Grimbergen et al., 2004).
It usually occurs at the later stages of the
disease and responds poorly to
medication.
It is in common in end-stage PD and
compromises the ability to maintain
balance during everyday tasks such as
walking, turning and standing up from
sitting.

Falls and freezing of gait in PD are closely
intertwined .
Both symptoms are common in the
advanced stages of the disease with
freezing of gait leading to increasing falls

Recent studies have shown that falls are
common in Parkinson's disease, even
when compared with other fall-prone
populations.
The clinical impact of falls is considerable,
often leading to an incapacitating fear of
renewed falls.
The absence of adequately directed arm
movements may explain the relatively high
proportion of hip fractures secondary to
falls in Parkinson's disease.
(Bloem et al, 2004)

Also an inability to adequately balance the
body's center of mass over the base of
support, combined with inflexibility in body
movements (increased rigidity) causes
patients with advanced PD to fall

Gait is the process of walking and relies on proper functioning from several areas of the body including the ears, eyes, brain, and muscles.
Gait disturbances in PD can be divided into episodic and continuous disturbances.
The episodic disturbances may occur randomly or intermittently and include start hesitation, festination and FoG.

Gait festination is progressive, whereby
each step in a long gait sequence
becomes progressively shorter, eventually
leading to blocking.

In normal gait, the heel strikes the ground before the toes (also called heel-to-toe walking)
In Parkinsonian gait, motion is characterized by flat foot strike (where the entire foot is placed on the ground at the same time)
Less often and in the more advanced stages of the disease there is toe-to-heel walking (where the toes touch the ground before the heel).

Balance is needed within the context of
many functional tasks of everyday living to
keep the body oriented appropriately while
performing voluntary activities, during
external perturbations and when the
support surface or environment changes
(Bronte-Stewart et al., 2002).
Thus, impaired balance and PI occur
mainly during walking, while maintaining
upright stance and stability in, or when
transferring from one position to another.

Falls result mainly due to sudden changes in posture, in particular turning movements of the trunk, or attempts to perform more than one activity simultaneously with walking or balancing.
Falls are also common during transfers, such as rising from a chair or bed. PD patients fall mostly forward (45% of all falls) and about 20% fall laterally
FOG is one of the most disabling and least understood symptoms in Parkinson's disease, and is usually observed in the advanced stage of the disease.
FOG is a brief, paroxysmal event characterized by absence or marked reduction of forward progression of the feet despite the intention to walk. The patients generally feel their feet glued to the ground.
Dual tasking (cognitive load) aggravates FOG.

FOG can be experienced on
turning
narrow spaces
whilst reaching a destination
stressful situations.
FOG is commonly observed in the "off"
state, but it can also be observed in the
"on" state


Some tests are used to assess gait and balance in PD patients.
Functional reach test Berg Balance Scale Tinetti mobility scale Fall efficacy scaleTen-meter walk testSix-minute walk test

Freezing of gait questionnaire
This questionnaire constructed by Giladi et al. (Giladi et al., 2000) evaluates the FoG in patients with PD. This detailed gait and falls questionnaire consists of 16 items that assess gait in daily living, frequency and severity of FoG, frequency of festinating gait and its relation to falls, and finally frequency and severity of falls.
Responses to each item are on 5- point scales where a score of 0 indicates absence of the symptom, while 4 indicates the most severe stage (Giladi et al., 2000).

Exercise will not stop Parkinson's disease
from progressing; but, it will improve
balance and it can prevent joint stiffening.

It has been suggested that there are five
key principles of exercise that enhance
neuroplasticity in PD
¶ If exercise is introduced at an early stage
of the disease, progression can be
slowed.
¶ Intensive activity maximizes synaptic
plasticity
¶ Complex activities promote greater
structural adaptation

¶ Activities that are rewarding increase
dopamine levels and therefore promote
learning/ relearning
¶ Dopaminergic neurons are highly
responsive to exercise and inactivity
(“use it or lose it”);
(Fox et al., 2006)
Exercises programs individually prescribed
at home have been shown to be effective
in reducing fall frequency among the
elderly population.
(Ashburn et al., 2007)
Exercises to improve balance can also
help improve walking ability and improve
safety when standing and walking,
Strengthening exercises to improve and maintain the integrity of muscles especially in the trunk, arm and legs also helps to improve coordination and smoothness of movement.
Endurance is usually compromised in PD hence exercises to promote cardiovascular and pulmonary fitness such as treadmill, stationary bike riding and arm endurance exercises can be taught.

Rigidity is a common symptom of PD and
range of motion and flexibility exercises in
the arms and legs can be taught to help
improve tightness in the muscles and
joints.

By consciously paying more attention to walking and rehearsing each step before actually making it, most patients are able to overcome FOG.
Sometimes, a companion walking alongside reminds the patient to concentrate on gait or they create a visual cue to step over by putting a foot in front of the person with PD over which the person must step.

Avoidance of dual tasks that require motor attention or cognitive attention has also been shown to normalize gait in the PD patients.
It is very important to exercise your facial muscles, jaw, and voice when possible: Sing or read aloud, exaggerating your lip movements. Make faces in the mirror. Chew food vigorously.

Training programs are designed
To lengthen a patient's stride length
Broaden the base of support
Improve the heel-toe gait pattern
Straighten out a patient's posture
Increase arm swing patterns





Due to PD’s progressive nature it is
important to sustain an exercise routine to
maintain its benefits.
Cueing is defined as using external
temporal or spatial stimuli to facilitate
movement (gait) initiation and continuation.

Recent reviews suggest that cueing has an
immediate and powerful effect on gait
performance in people with PD, improving
walking speed
step length
step frequency.

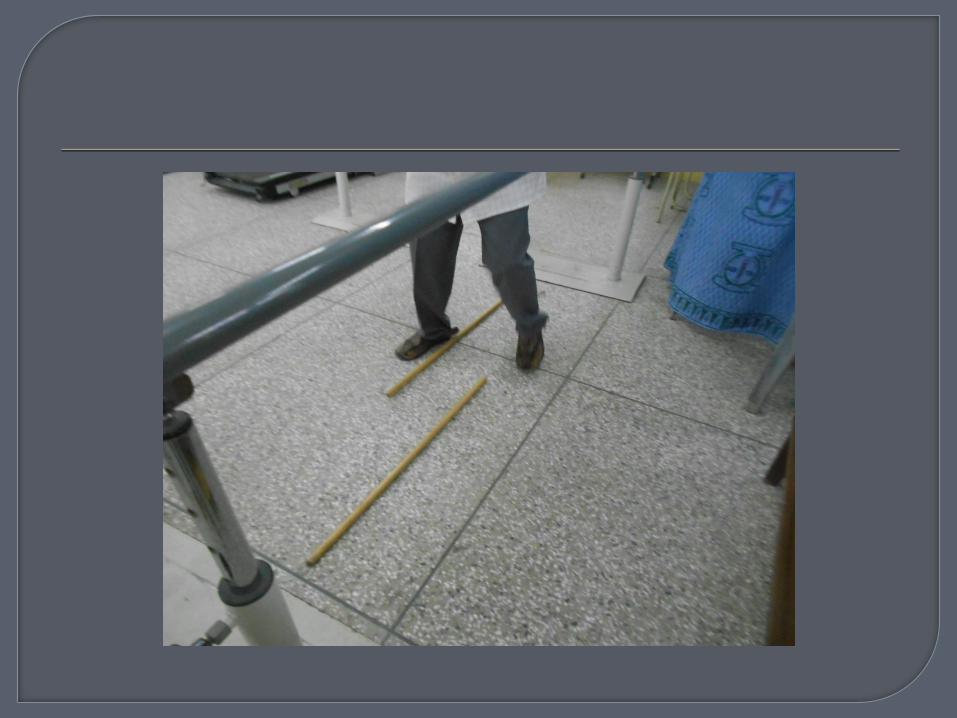
Visual cues
The visual cues are commonly transverse
lines or rods on the floor (floor markers).Such
cues have been shown to improve stride
length and velocity in Parkinsonian gait.
Virtual reality glasses have also been
developed recently to aid walking in PD
patients.



Auditory cuesThe auditory cues are commonly rhythmic
cues generated by a metronome or equivalent, and sometimes embedded in music, set at or slightly above the subject’s usual cadence.
Rhythmic auditory cues have been associated with increases in velocity and cadence and sometimes stride after gait has been initiated.


Keep at least one hand free at all times; try using a backpack or fanny pack to hold things rather than carrying them in your hands. Never carry objects in both hands when walking as this interferes with balance.
Attempt to swing both arms from front to back while walking. This may require a conscious effort if Parkinson's disease has diminished your movement; however, it will help you to maintain balance, posture, and reduce fatigue.

Consciously lift your feet off of the ground
when walking. Shuffling and dragging your
feet may cause you to lose your balance.
When trying to navigate turns, use a "U"
technique of facing forward and making a
wide turn, rather than pivoting sharply.

Try to stand with your feet shoulder width apart. When your feet are close together for any length of time, you increase your risk of losing your balance and falling.
Do one thing at a time! Don't try to walk and accomplish another task, such as reading or looking around. The decrease in your automatic reflexes complicates motor function, so the less distraction, the better!

It may be advisable not to wear rubber or gripping soled shoes. They may "catch" on the floor and cause tripping.
Move slowly when changing positions. Use deliberate, concentrated movements and if needed, use a grab bar or walking aid. Count 15 seconds between each movement. For example, when rising from a seated position, wait 15 seconds after standing to begin walking.
If you become "frozen," visualize stepping over an imaginary object, or have someone place their foot in front of yours to step over. Try not to have a caregiver or companion "pull" you, this may throw you off balance and even prolong the episode.
If balance is a continuous problem, you may want to consider a walking aid such as a cane, walking stick, or walker. Once you've mastered walking with help, you may be ready to try it on your own again!

Mobility issues associated with falls and
freezing of gait have a devastating impact
in the lives of PD patients.
Fear of falling in itself can have an
incapacitating effect in PD patients and
can result in social seclusion leaving
patients largely isolated leading to
depression.

Immobility can also lead to osteoporosis which in-turn facilitates future fracture development. This then becomes a vicious circle with falls leading to immobility and immobility facilitating future falls.
Hip fractures from falls are the most common form of fracture among PD patients. Fractures increase treatment costs for people living with PD
Carr, J.H (2000). Neurological rehabilitation: optimizing motor performance. Oxford: Butterworth Heinimann
Umphred, D. A. (1995). Neurological rehabilitation. (3 ed). St. Louis: Mosby Ashburn, A., Stack, E., Pickering, RM., & Ward, CD. (2001). Predicting fallers in a
community-based sample of people with Parkinson's disease. Gerontology, Vol. 47, No. 5, pp. 277-81, ISSN 1423-0003.
Bloem, BR., & Bhatia, KP. (2004). Gait and balance in basal ganglia disorders, In: Clinical disorders of balance, posture and gait, Bronstein, AM., Brandt, T., Nutt, JG., Woollacott, MH., (2 ed.), pp. 173–206, Arnold, ISBN 0340806575, London.
Vaugoyeau, M., & Azulay, JP. (2010). Role of sensory information in the control of postural orientation in Parkinson's disease. Journal of the Neurological Sciences, Vol. 289, No. 1-2, pp. 66-8, ISSN 1878-5883.
Azher, SN., & Jankovic, J. (2005). Camptocormia: pathogenesis, classification, and response to therapy. Neurology, Vol. 65, No. 3, pp. 355-9, ISSN 1526-632X.
Gambarin, M., Antonini, A., Moretto, G., Bovi, P., Romito, S., Fiaschi, A., & Tinazzi, M. (2006). Pisa syndrome without neuroleptic exposure in a patient with Parkinson's disease: case report. Movement Disorders, Vol. 21, No. 2., pp. 270-3, ISSN 1531-8257.
Grimbergen, YA., Munneke, M., & Bloem, BR. (2004). Falls in Parkinson's disease. Current Opinion in Neurology, Vol. 17, No. 4, pp. 405-15, ISSN 1473-6551.
Bronte-Stewart, HM., Minn, AY., Rodrigue, K., Buckley, EL., & Nashner, LM. (2002). Postural instability in idiopathic Parkinson’s disease: the role of medication and unilateral pallidotomy. Brain, Vol. 125, Pt. 9, pp. 2100-2114, ISSN 1460-2156.
Duncan, PW., Weiner, DK., Chandler, J., & Studenski, S. (1990). Functional reach: a new clinical measure of balance. Journal of Gerontology, Vol. 45, No. 6, pp. M192-7, ISSN 0022-1422.

Goldie, PA., Matyas, TA., Spencer, KI., & McGinley, RB. (1990). Postural control in standing following stroke: test-retest reliability of some quantitative clinical tests. Physical Therapy, Vol. 70, No. 4, pp. 234-43, ISSN 1538-6724.
Hill, K., Bernhardt, J., McGann, A., Maltese, D., & Berkovits, D. (1996). A new test of dynamic standing balance for stroke patients: Reliability, validity and comparison with healthy elderly. Physiotherapy Canada, Vol. 48, No. 4, pp. 257-262.
Smithson, F., Morris, ME., & Iansek, R. (1998). Performance on clinical tests of balance in Parkinson's disease. Physical Therapy, Vol. 78, No. 6, pp. 577-92, ISSN 1538-6724
Bronte-Stewart, HM., Minn, AY., Rodrigue, K., Buckley, EL., & Nashner, LM. (2002). Postural instability in idiopathic Parkinson’s disease: the role of medication and unilateral pallidotomy. Brain, Vol. 125, Pt. 9, pp. 2100-2114, ISSN 1460-2156.
Falvo, MJ., & Earhart, GM. (2009). Six-minute walk distance in persons with Parkinson disease: a hierarchical regression model. Archives of Physical Medicine Rehabilitation, Vol. 90, No. 6, pp. 1004-8, ISSN 1532-821X.
Thomas, AA., Rogers, JM., Amick, MM., & Friedman, JH. (2010). Falls and the falls efficacy scale in Parkinson's disease. Journal of Neurology, Vol. 257, No. 7, pp. 1124-8, ISSN 1432-1459.






























