Embed Size (px)
Citation preview
Goals Nasal oxygen catheter
Difficult intubation: alternative techniques
Alveolar recruitment manoeuvers
Management of oesophageal reflux
Venous cut-down
Arterial catheterisation & arterial blood sampling
Using anaesthetic monitors
Estimating fluid responsiveness: Dynamic measures of Systemic venous filling pressure (Not CVP)
History tracheotomy was portrayed on Egyptian tablets dated back to 3600 BC
1543 Vesalius passed a reed into the trachea of a dying animal whose thorax had been opened, and maintained ventilation by blowing into the reed intermittently.
1546, the Italian physician Antonio Brasavola reintroduced tracheostomy in humans by performing the first documented case of a successful tracheostomy (Fig. 4) in a patient with tonsillar obstruction.
1733 Hales: First direct blood pressure measurement (horse)
1828 Poiseuille won the gold medal of the Royal Academy of Medicine for his doctoral dissertation on the use of a mercury manometer for the measurement of direct arterial blood pressure.
1863 First systemic study, description and interpretation of intracardiac pressure recordings (horse)
1952 Clinical use of CV Catheter in man
1970 Dr Swan & Ganz: Balloon catheters to measure RAFP, LVPWP, CO
Nasal oxygen catheters
Place a few drops of lidocaine 2% in one of the nostrils
Measure and mark a soft thin catheter the distance from the nose to the medial canthus
Open the external nares by holding the nasal plannum dorsally
Introduce the catheter ventrally and medially along the floor of the nose
Secure the catheter to the side of the nose with superglue, tissue glue, skin staple or suture
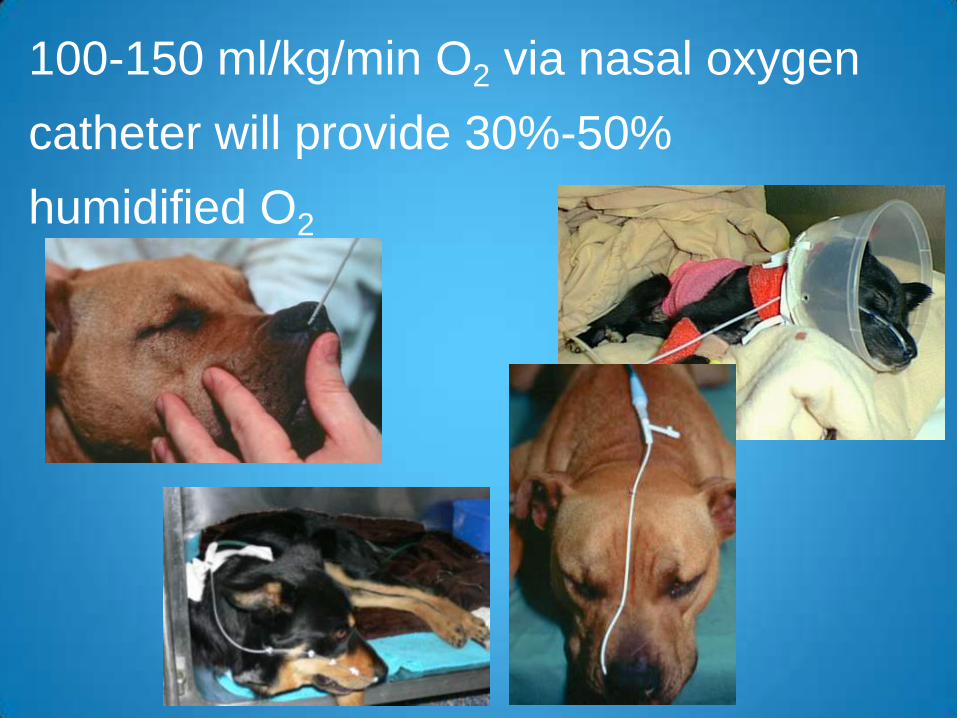
100-150 ml/kg/min O2 via nasal oxygen
catheter will provide 30%-50%
humidified O2

Treatment of Ventilatory Failure
Effect of enriching inspired oxygen concentration during hypoventilation in man
From Nunn’s Applied Respiratory Physiology
5th Edit Lumb AB
A small increase in FIO2 will maintain a normal PAO2
even with large falls in ventilation
Difficult intubation
Strategies in management of respiratory emergencies
- identification of miss intubation
- facilitation of intubation
- alternative routes for intubation
- emergency airway access
Identification of miss intubation
- Lack of humidification within ET tube on expiration
- Absence of normal sound from ET tube with chest
compression
- Failure to inflate chest on positive pressure breath
- ETCO2
Managing Difficult intubation
- Key is to minimising complications
- Maintenance of oxygenation
- Prevention of trauma
- Alternative or backup plan
- Termination of the procedure
- Managing difficult intubations
expected difficult intubation - ability to prepare
unexpected difficult intubation - always be prepared
Difficult intubation
Expected difficult intubation
Brachycephalic breed, obesity
Mass/swelling obstructing the pharynx
Macroglossia
Trismus
Difficult intubation
Pre-oxygenate everything possible (without undue stress)
Appropriate laryngoscope for species, breed and size
Experienced assistant to extend the head and neck
Protocol for reflux or vomiting
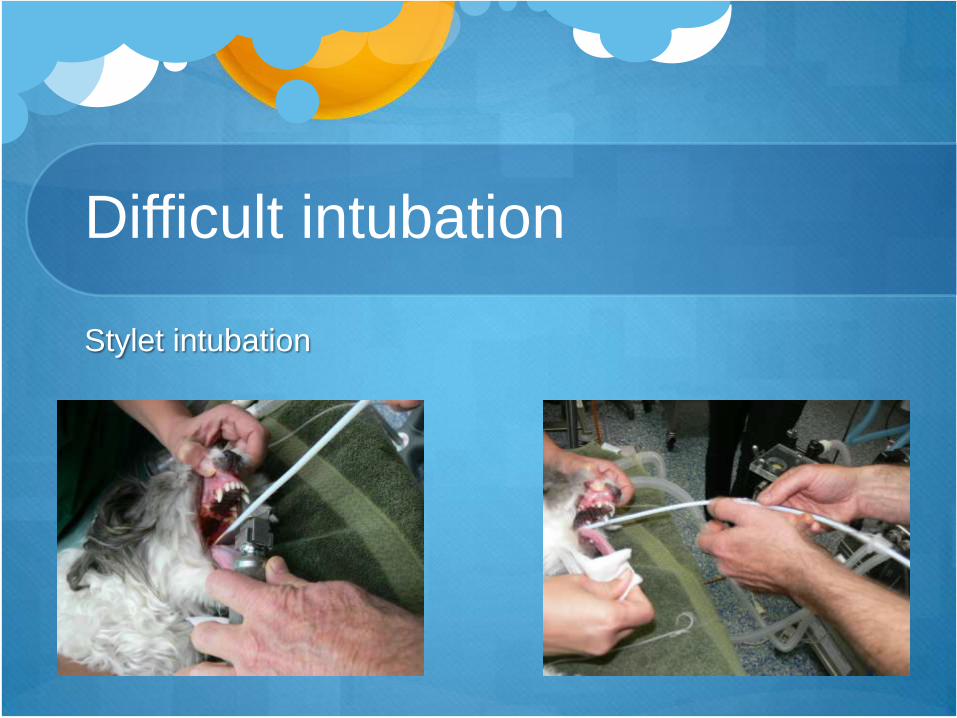
Use of stylet or boogie
Endoscopically assisted
Tracheal catheter oxygenation
Invasive retrograde intubation
Emergency tracheotomy
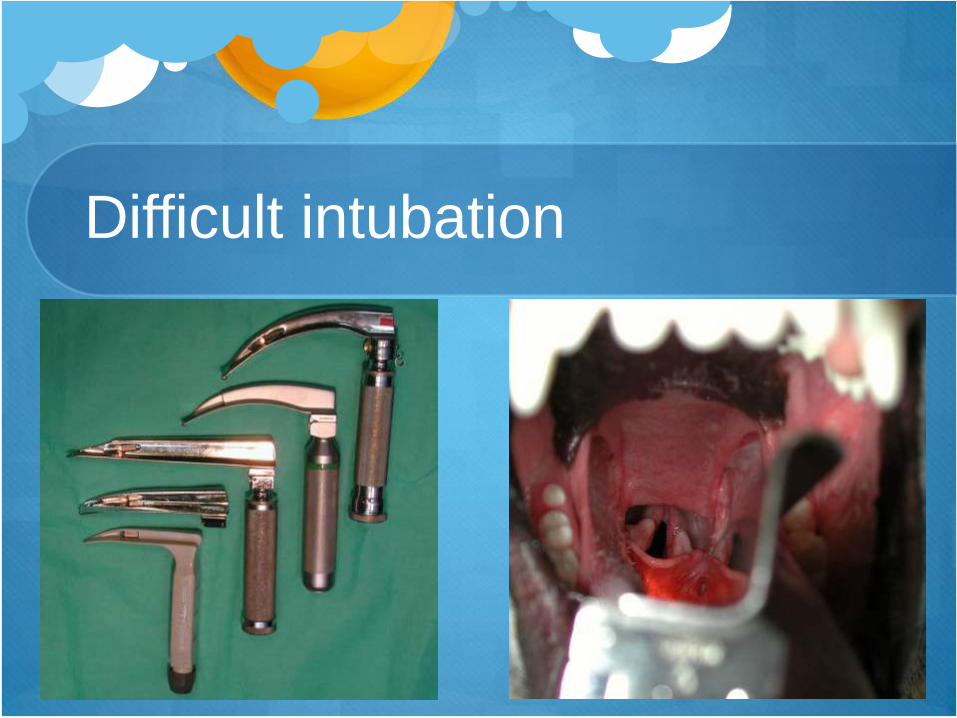
Difficult intubation
Difficult intubation
Stylet intubation

Difficult intubation
Stylet intubation
Difficult intubation
Transtracheal catheter
For emergency oxygenation
Place a 14G IV catheter over the needle straight into the
trachea
Withdraw needle and connect O2 to the catheter
Cannot ventilate the patient but will maintain oxygenation
whilst a better alternative is implemented

Difficult intubation
Retrograde
intubation
South Tamworth Animal Hospital
Rabbits
Weight: 1.5-5 kg
Life span: 5-10 yrs
Temperature: 38 - 40 oC
Heart rate: 200-300 beats/min
Blood volume: 60 ml/Kg
Tidal volume: 4-6 ml/kg
Resp rate: 32-65/min
South Tamworth Animal Hospital
Rabbits
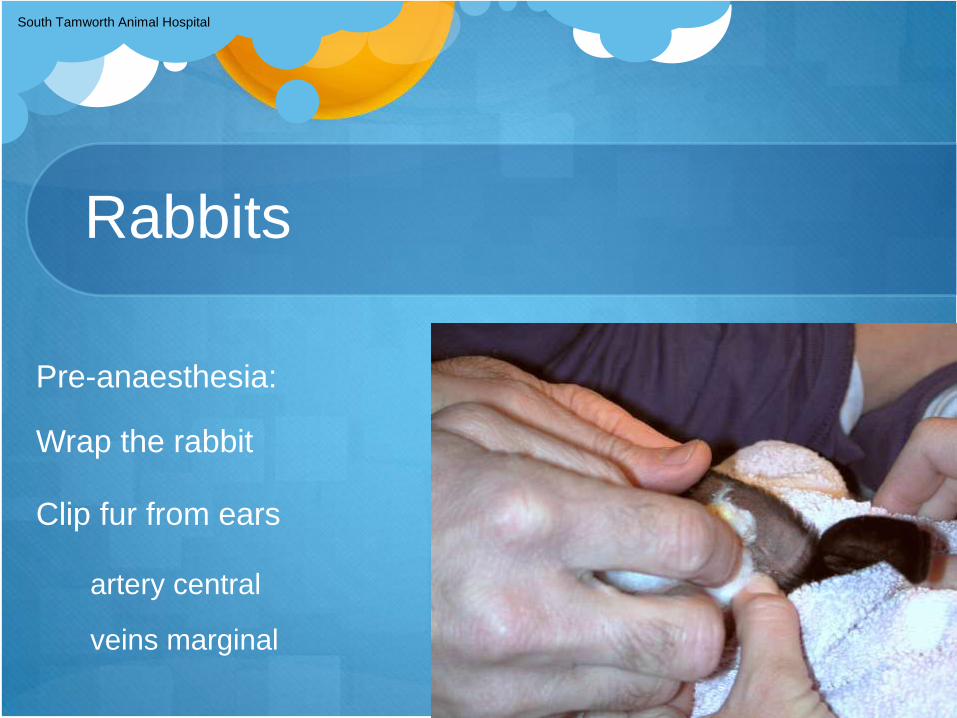
Pre-anaesthesia:
Wrap the rabbit
Clip fur from ears
artery central
veins marginal
South Tamworth Animal Hospital
Rabbits
Apply EMLA
cream & leave
for 15-30 min

South Tamworth Animal Hospital
Rabbits
Catheterise ear vein
24-22 g Optiva catheter
South Tamworth Animal Hospital
Rabbits
Attach bung

South Tamworth Animal Hospital
Rabbits
Catheterise ear vein
24-22 g Optiva catheter
Attach bung
Tape to folded ear
South Tamworth Animal Hospital
Rabbits
Midazolam
0.25 - 0.5 mg/kg IV
0.5 - 2 mg/kg SC
South Tamworth Animal Hospital
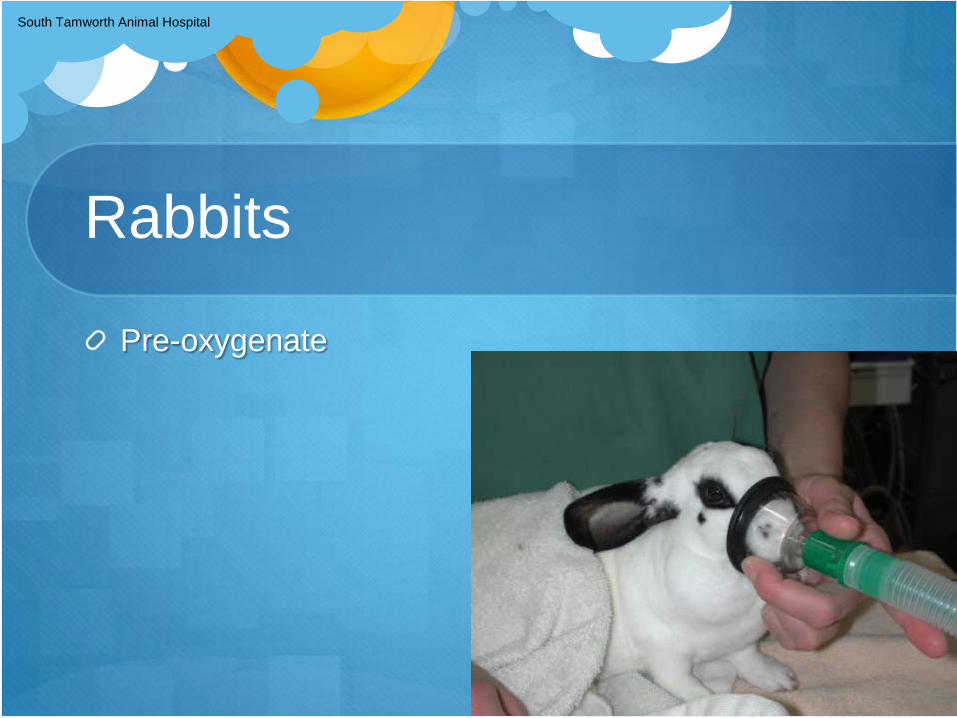
Rabbits
Pre-oxygenate
South Tamworth Animal Hospital
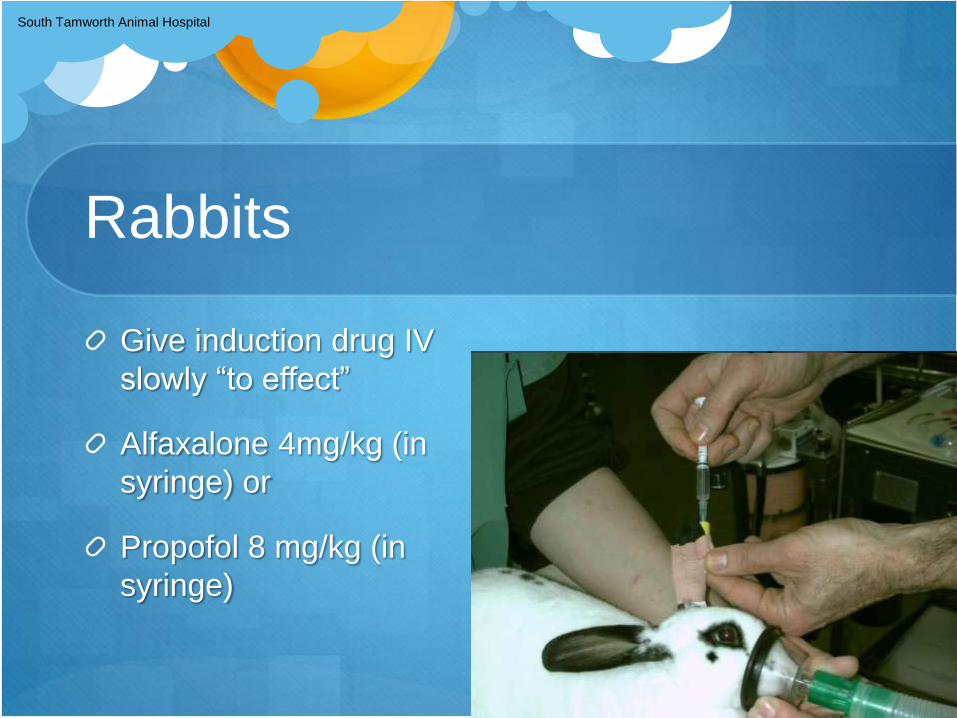
Rabbits
Give induction drug IV
slowly “to effect”
Alfaxalone 4mg/kg (in
syringe) or
Propofol 8 mg/kg (in
syringe)

South Tamworth Animal Hospital
Rabbits
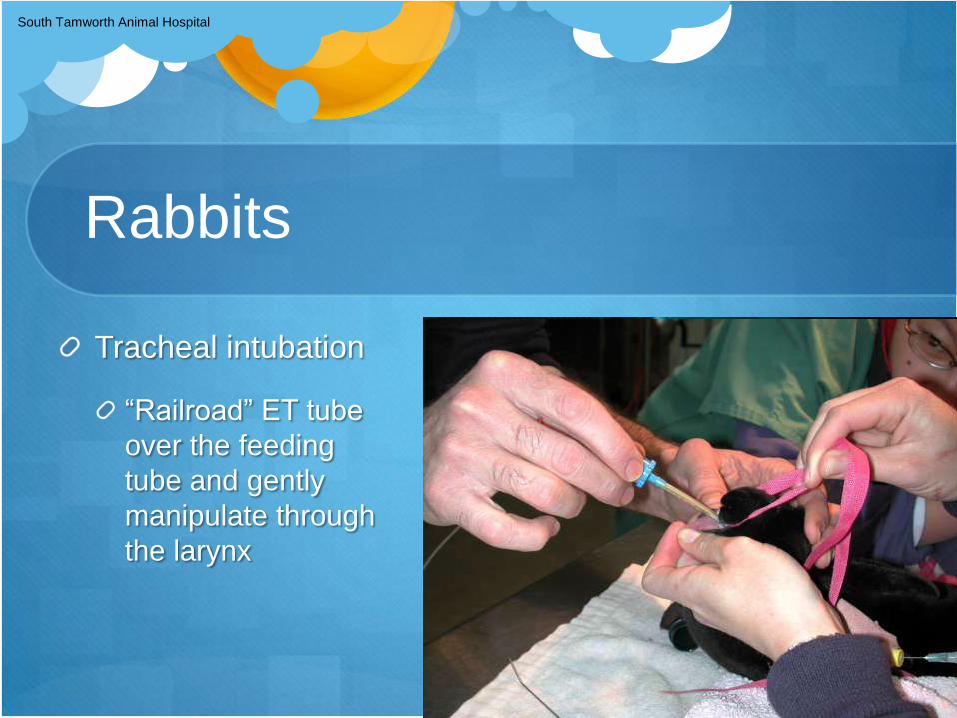
Tracheal intubation
Equipment:
otoscope & specula
4% topical lignocaine
Cass needle
2.5,3.0,3.5mm ETTubes
plain forceps
4FG infant feeding tube
scissors
cloth tape

South Tamworth Animal Hospital
Rabbits
Tracheal intubation
Position in sternal
recumbency
loop around upper incisors
Grasp tongue and draw
forward
South Tamworth Animal Hospital
Rabbits
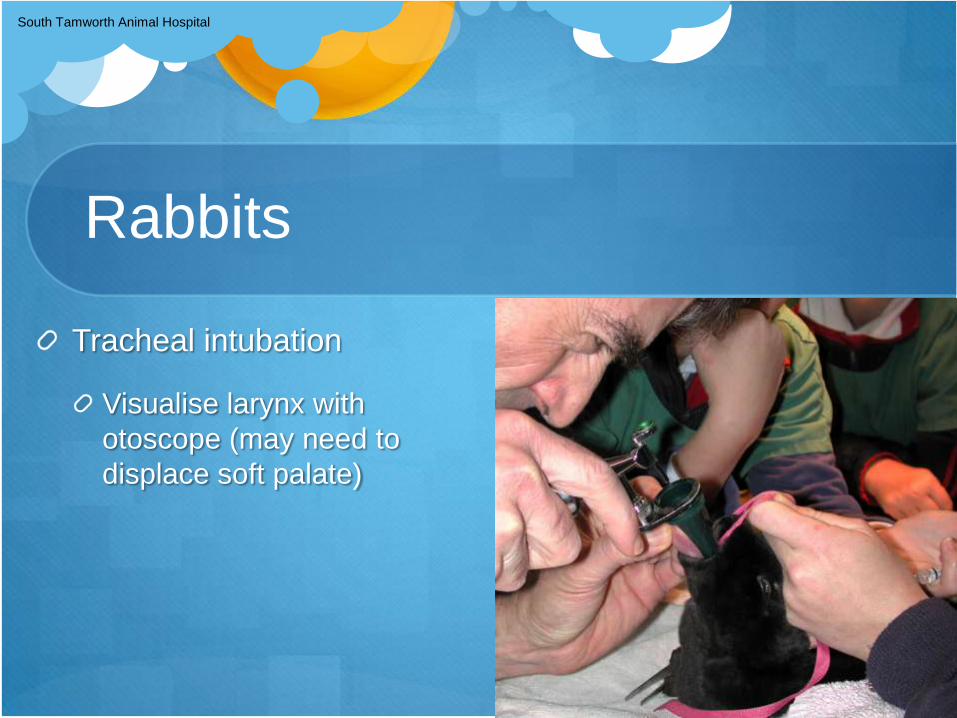
Tracheal intubation
Visualise larynx with
otoscope (may need to
displace soft palate)
South Tamworth Animal Hospital
Rabbits
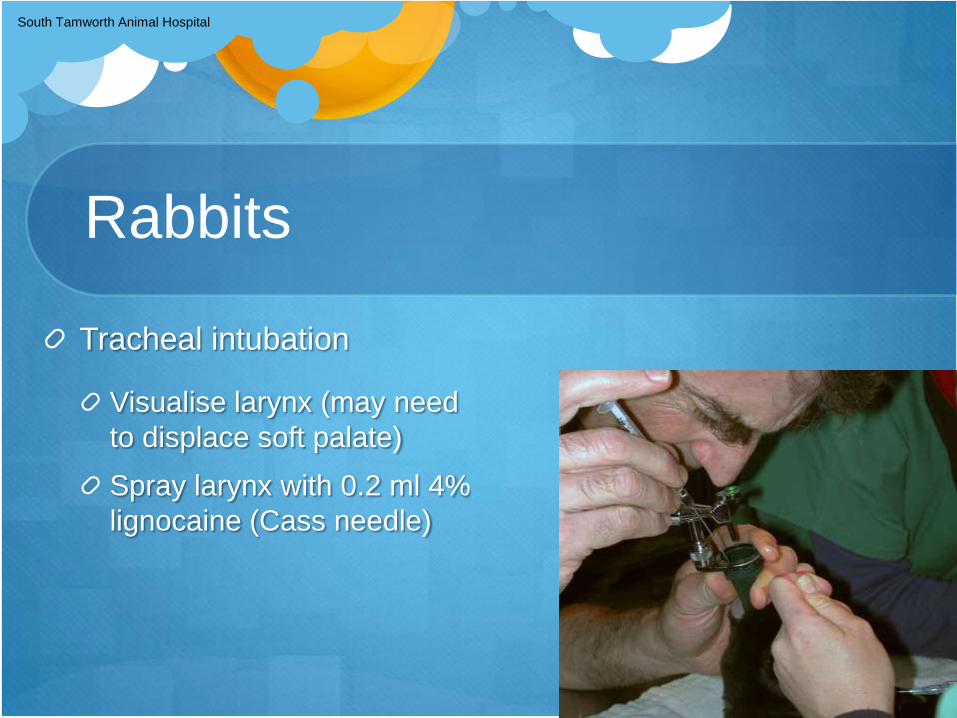
Tracheal intubation
Visualise larynx (may need
to displace soft palate)
Spray larynx with 0.2 ml 4%
lignocaine (Cass needle)
South Tamworth Animal Hospital
Rabbits
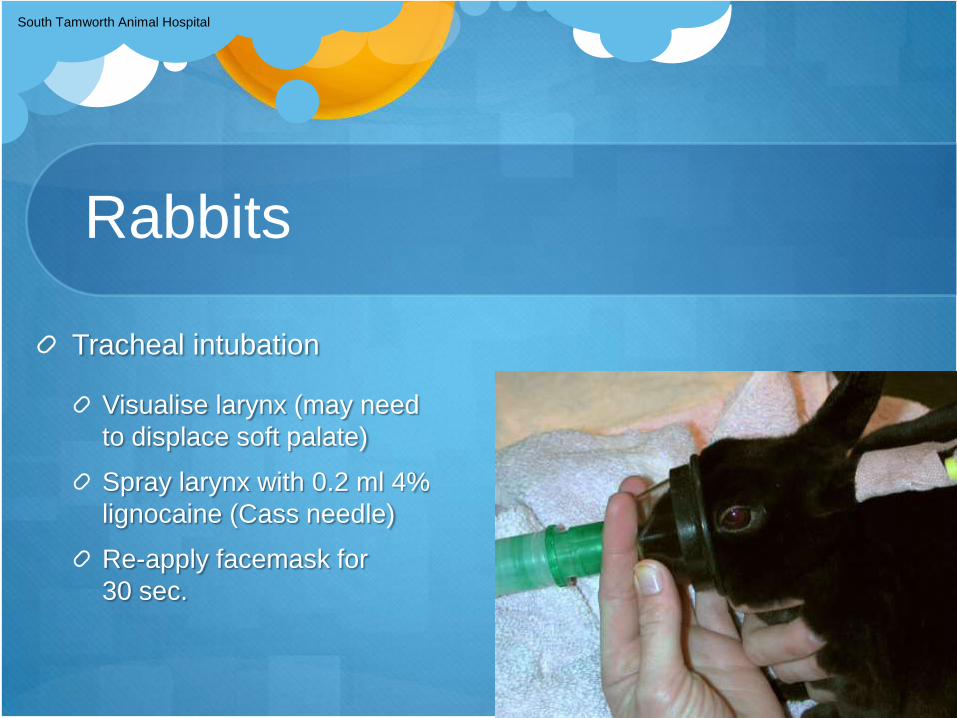
Tracheal intubation
Visualise larynx (may need
to displace soft palate)
Spray larynx with 0.2 ml 4%
lignocaine (Cass needle)
Re-apply facemask for
30 sec.
South Tamworth Animal Hospital
Rabbits
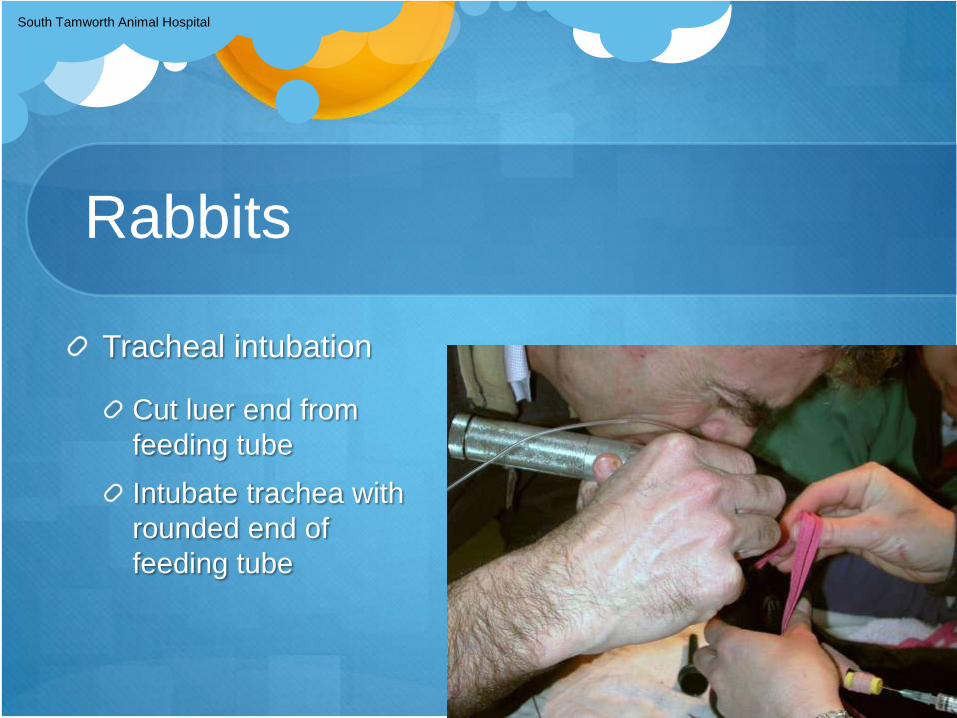
Tracheal intubation
Cut luer end from
feeding tube
Intubate trachea with
rounded end of
feeding tube
South Tamworth Animal Hospital
Rabbits
Tracheal intubation
“Railroad” ET tube
over the feeding
tube and gently
manipulate through
the larynx
South Tamworth Animal Hospital
Rabbits
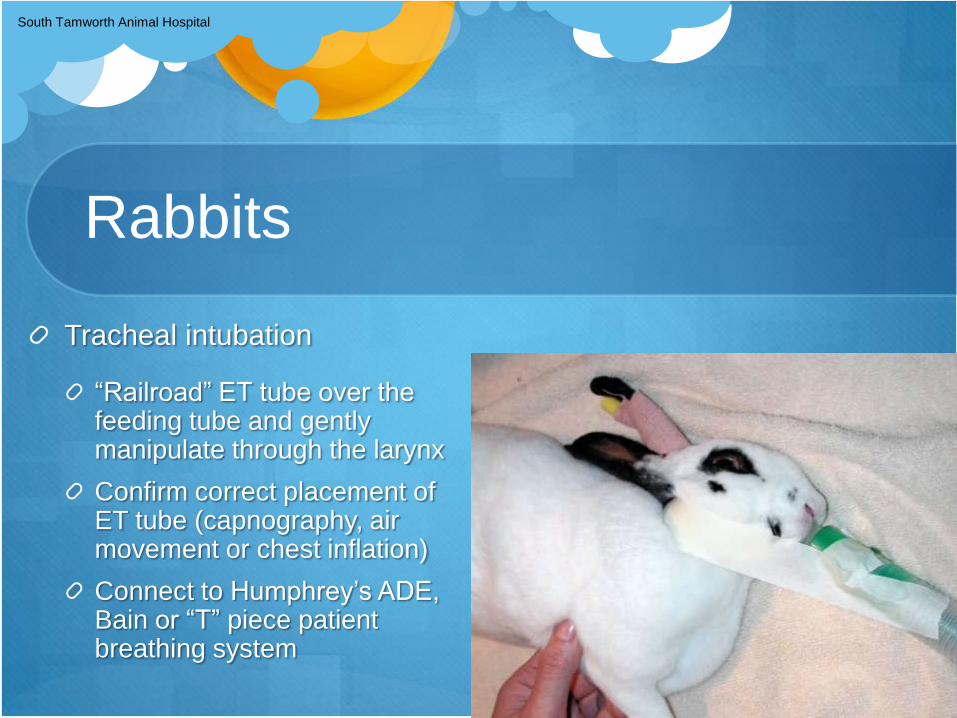
Tracheal intubation
“Railroad” ET tube over the feeding tube and gently manipulate through the larynx
Confirm correct placement of ET tube (capnography, air movement or chest inflation)
Connect to Humphrey’s ADE, Bain or “T” piece patient breathing system

What are your management options to maintain
oxygenation during surgery: Alveolar
recruitment manoeuver

Alveolar recruitment manoeuver
Downside atelectasis occurs quickly
Progressive deterioration in gas exchange
Venous admixture, increasing shunt fraction, ↓ SpO2

Alveolar recruitment manoeuver
ARM: 30-40cm H2O for 20-30 secs
Reflux Gastro-oesophageal reflux during anaesthesia in the dog: the effect of
preoperative fasting and premedication.
AD Galatos & D. Raptopoulos Vet Record 1995;137:479-483
Lower oesophageal reflux was monitored in 240 anaesthetised dogs.
The incidence of gastro-oesophageal reflux was 16.3 %
Most of the reflux episodes occurred shortly after the induction of anaesthesia.
The refluxate was nearly always acid (pH < 4.0),
In 10.3% of the cases it was alkaline (pH > 7.5)
Gastric contents of pH below 2.5 were refluxed on 19 occasions (7.9%)
Regurgitation occurred in only one dog.
Prolonging preoperative fasting was associated with an increased incidence of reflux and increased gastric acidity.

Regurgitation
Regurgitation
o Head down tilt
o Check cuff is inflated correctly
o Ideally check pH with urine Dipstix
o Clean pharynx with gauze swabs
o Place oesophageal tube
o Irrigate oesophagus with 0.3M Na Citrate 1-3ml/kg
whilst slowly extracting the stomach tube
o Repeat clean pharynx

Regurgitation
Head down tilt
Oesophageal tube and
0.3M Na Citrate
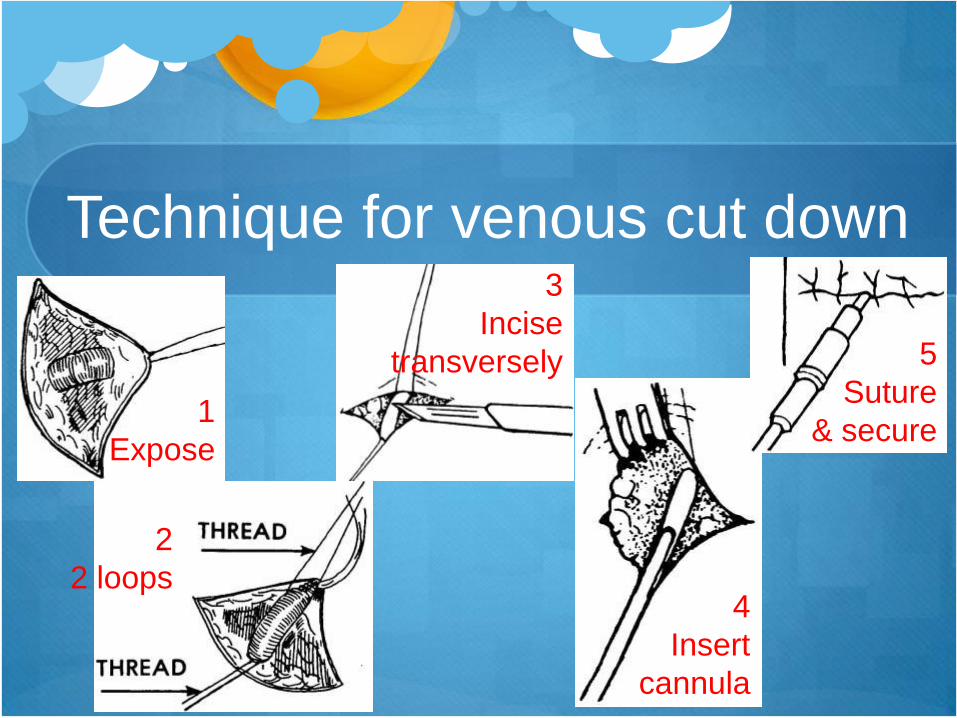
Technique for venous cut down
1
Expose
2
2 loops
3
Incise
transversely
4
Insert
cannula
5
Suture
& secure
Direct arterial catheterisation
Dr. Bob Stein
Veterinary Anesthesia & Analgesia
Support Group
Practical Information for the
Compassionate Veterinary Practitioner
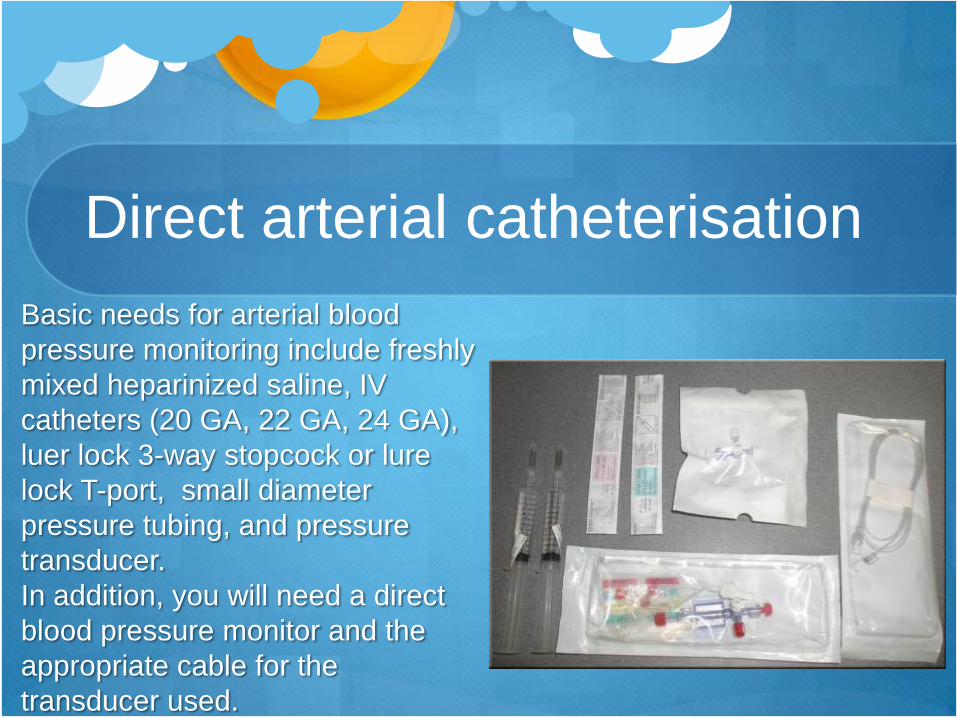
Direct arterial catheterisation
Basic needs for arterial blood
pressure monitoring include freshly
mixed heparinized saline, IV
catheters (20 GA, 22 GA, 24 GA),
luer lock 3-way stopcock or lure
lock T-port, small diameter
pressure tubing, and pressure
transducer.
In addition, you will need a direct
blood pressure monitor and the
appropriate cable for the
transducer used.
Direct arterial catheterisation
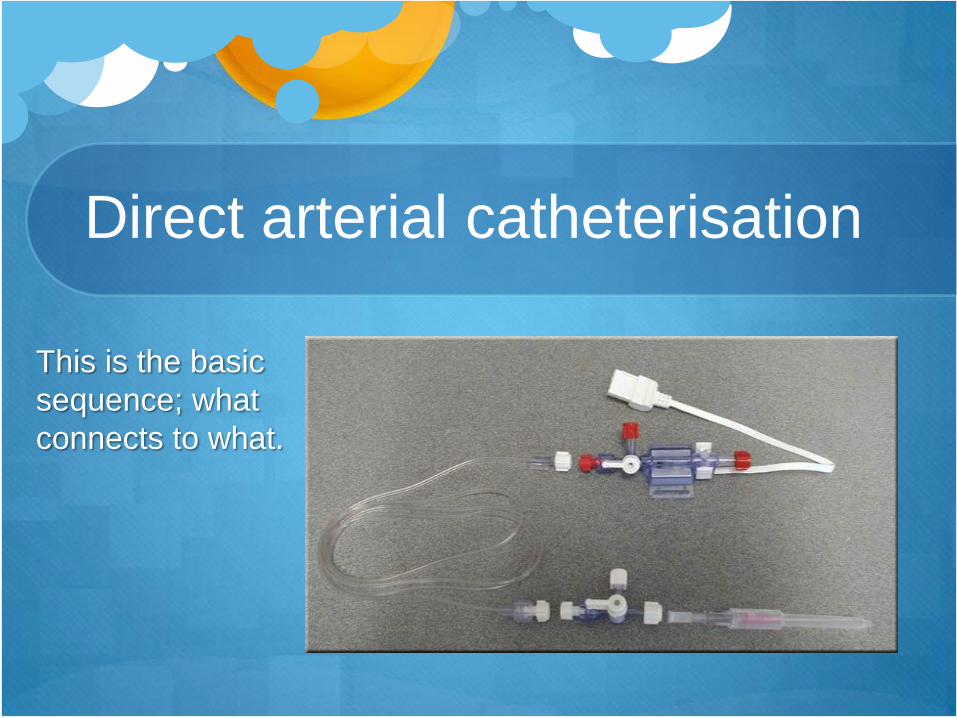
This is the basic
sequence; what
connects to what.
Direct arterial catheterisation
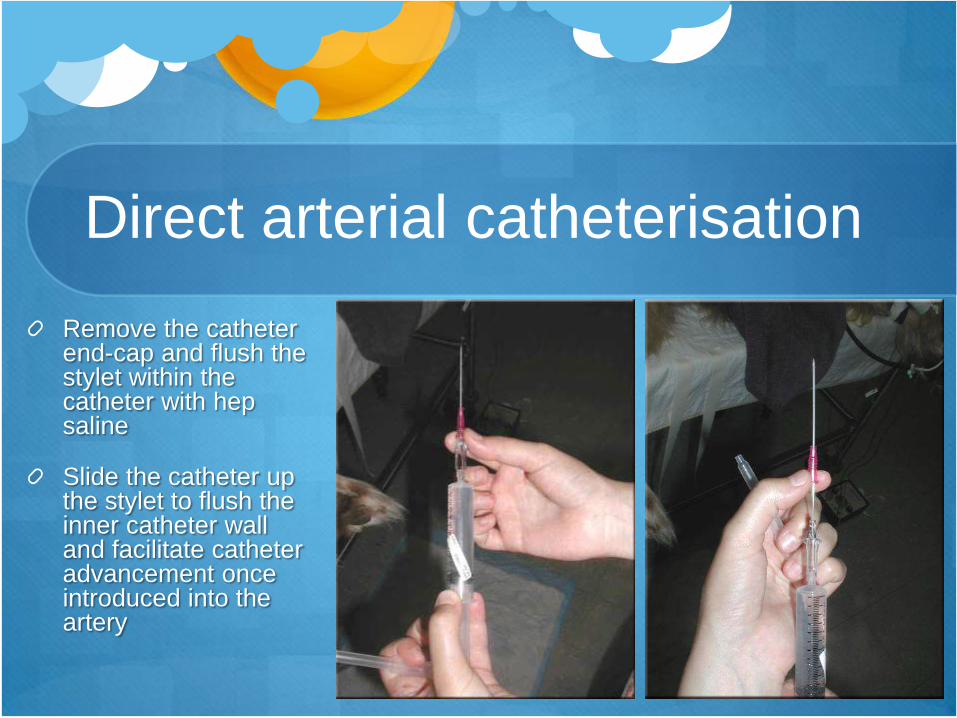
Remove the catheter end-cap and flush the stylet within the catheter with hep saline
Slide the catheter up the stylet to flush the inner catheter wall and facilitate catheter advancement once introduced into the artery
Direct arterial catheterisation
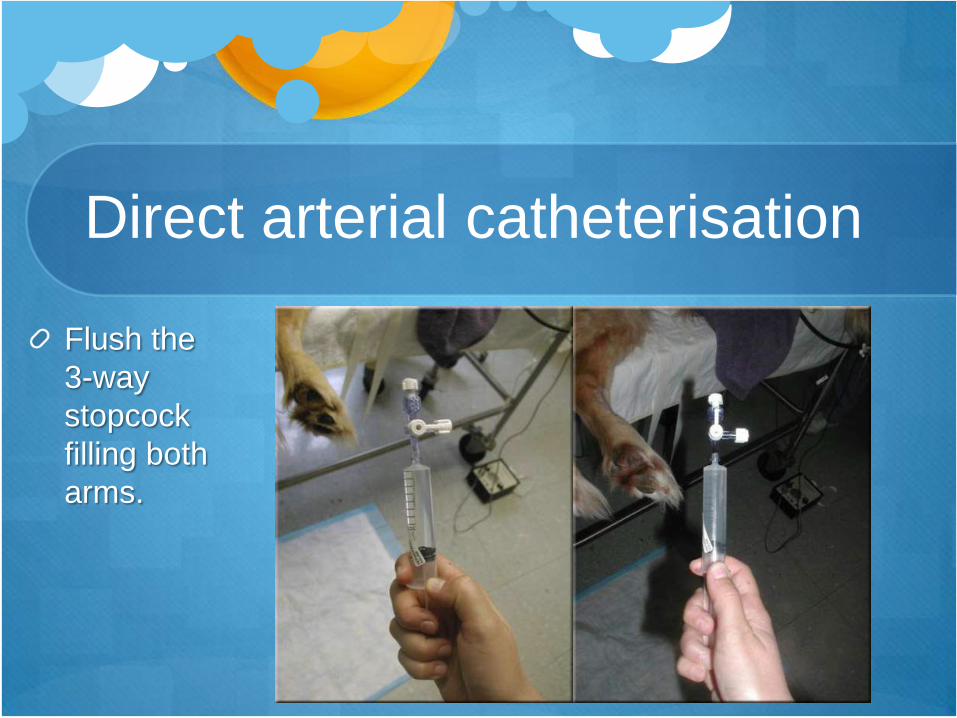
Flush the
3-way
stopcock
filling both
arms.
Direct arterial catheterisation
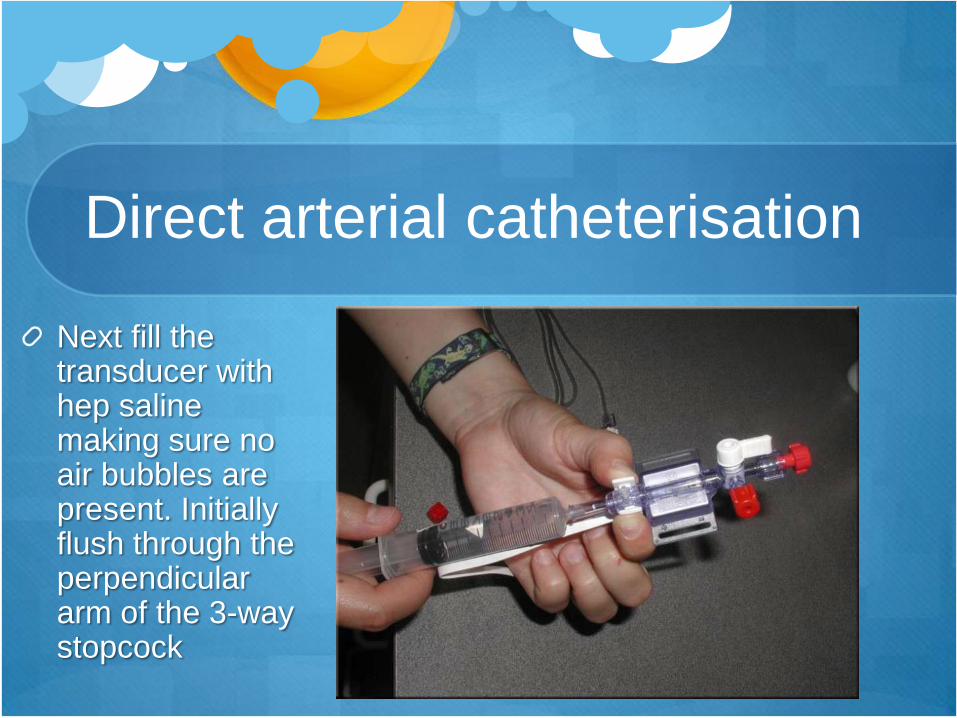
Next fill the transducer with hep saline making sure no air bubbles are present. Initially flush through the perpendicular arm of the 3-way stopcock
Direct arterial catheterisation
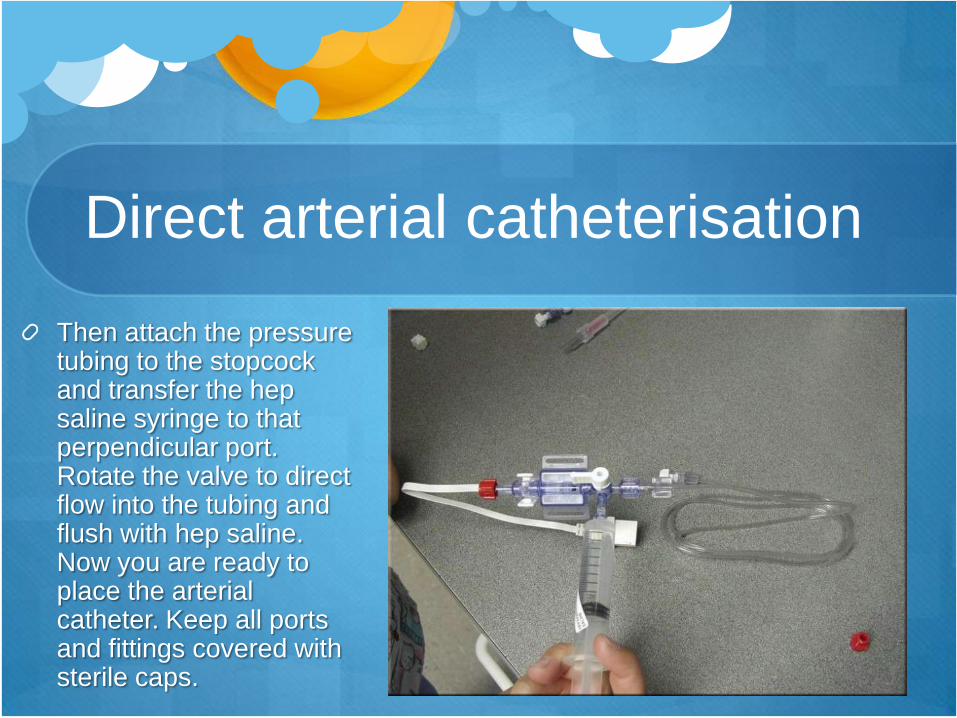
Then attach the pressure tubing to the stopcock and transfer the hep saline syringe to that perpendicular port. Rotate the valve to direct flow into the tubing and flush with hep saline. Now you are ready to place the arterial catheter. Keep all ports and fittings covered with sterile caps.
Direct arterial catheterisation
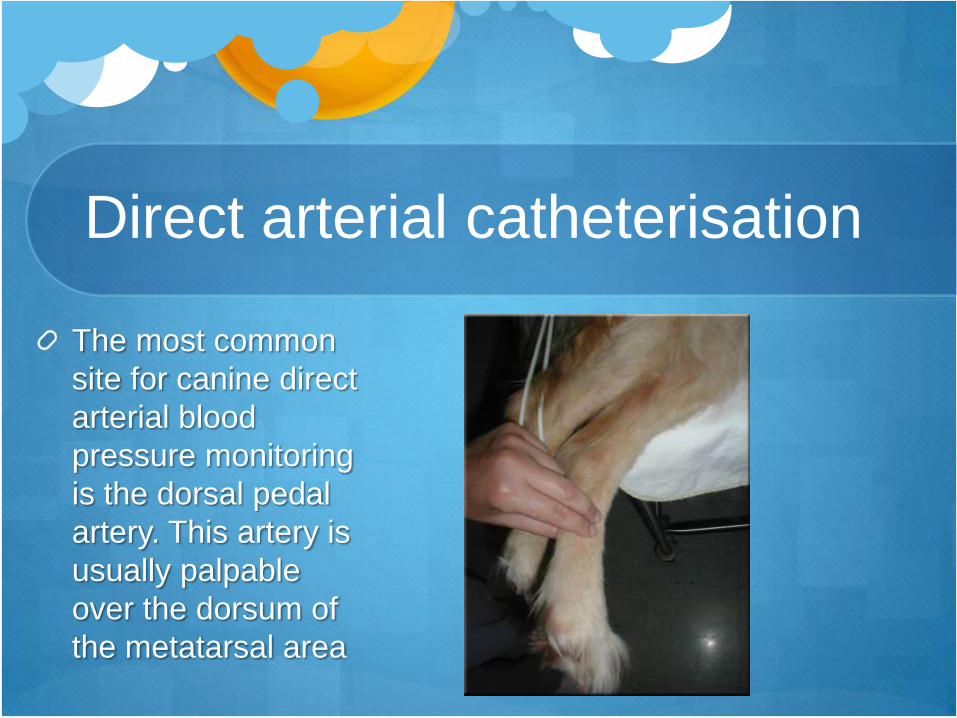
The most common
site for canine direct
arterial blood
pressure monitoring
is the dorsal pedal
artery. This artery is
usually palpable
over the dorsum of
the metatarsal area
Direct arterial catheterisation
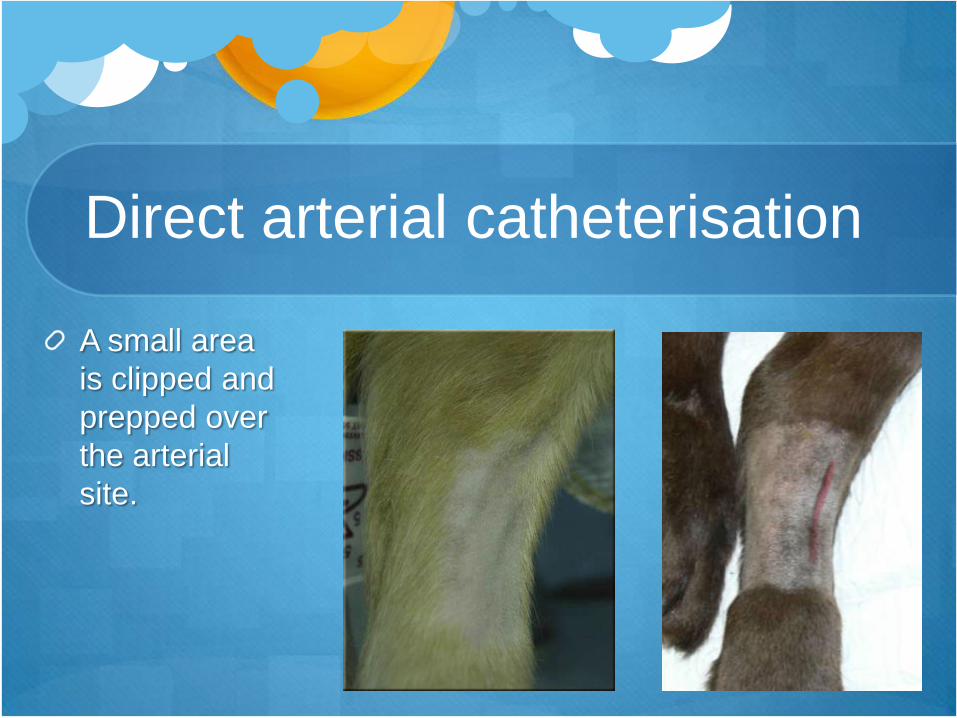
A small area
is clipped and
prepped over
the arterial
site.

Direct arterial catheterisation
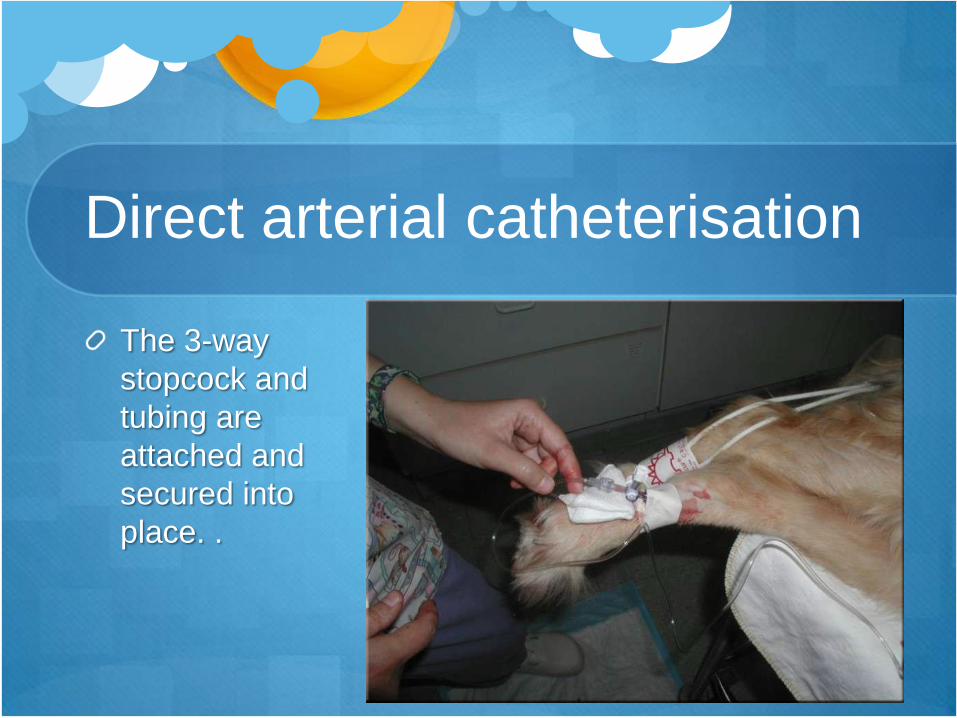
The 3-way
stopcock and
tubing are
attached and
secured into
place. .
Direct arterial catheterisation
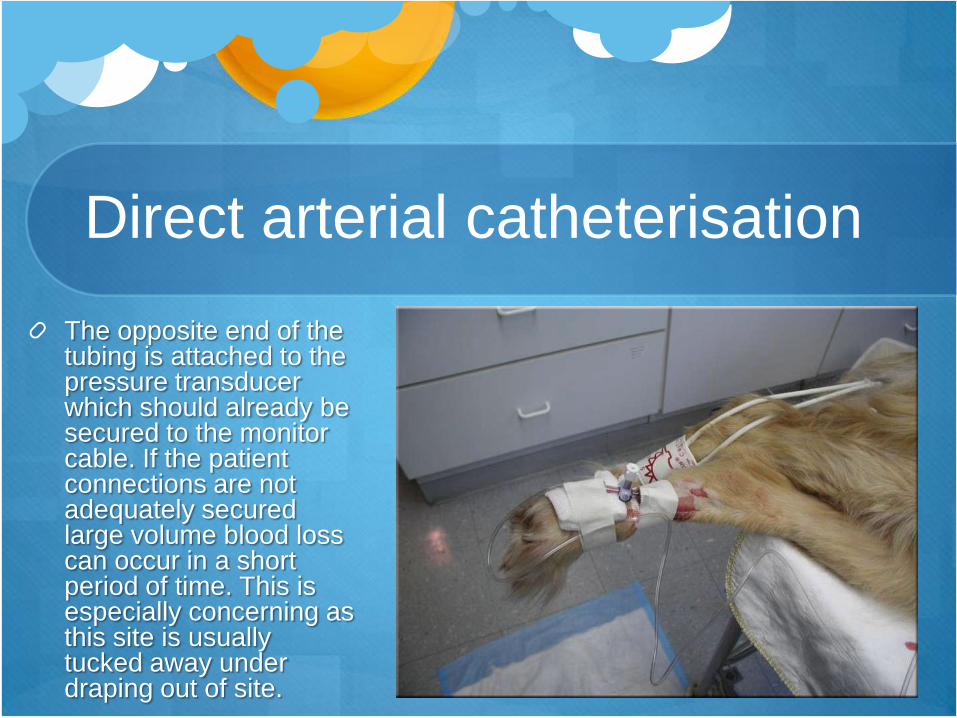
The opposite end of the tubing is attached to the pressure transducer which should already be secured to the monitor cable. If the patient connections are not adequately secured large volume blood loss can occur in a short period of time. This is especially concerning as this site is usually tucked away under draping out of site.
Direct arterial catheterisation
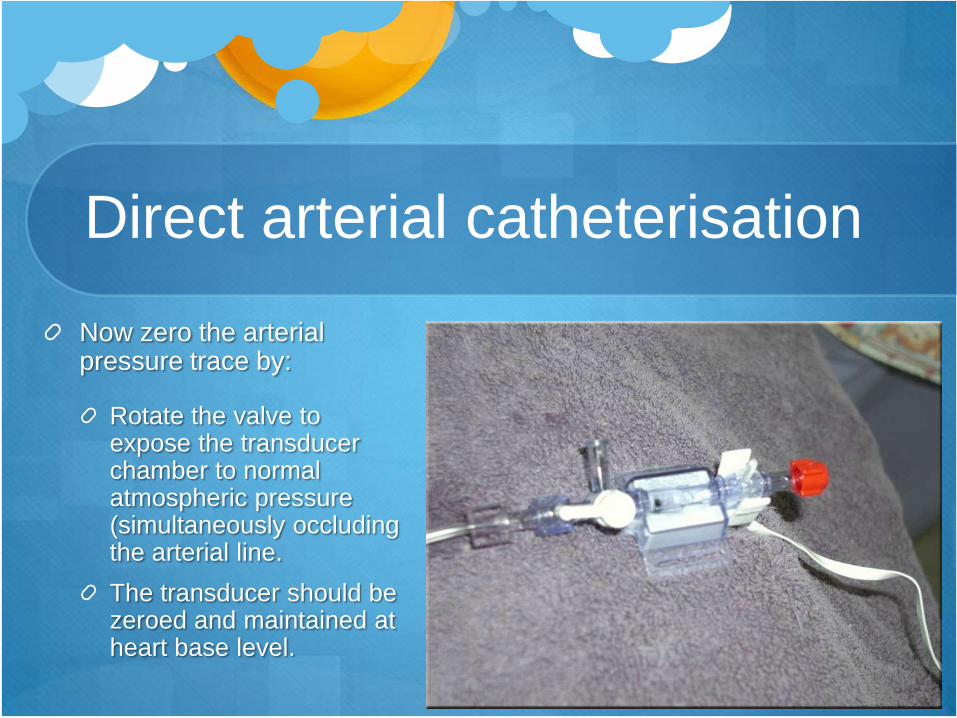
Now zero the arterial pressure trace by:
Rotate the valve to expose the transducer chamber to normal atmospheric pressure (simultaneously occluding the arterial line.
The transducer should be zeroed and maintained at heart base level.
Direct arterial catheterisation
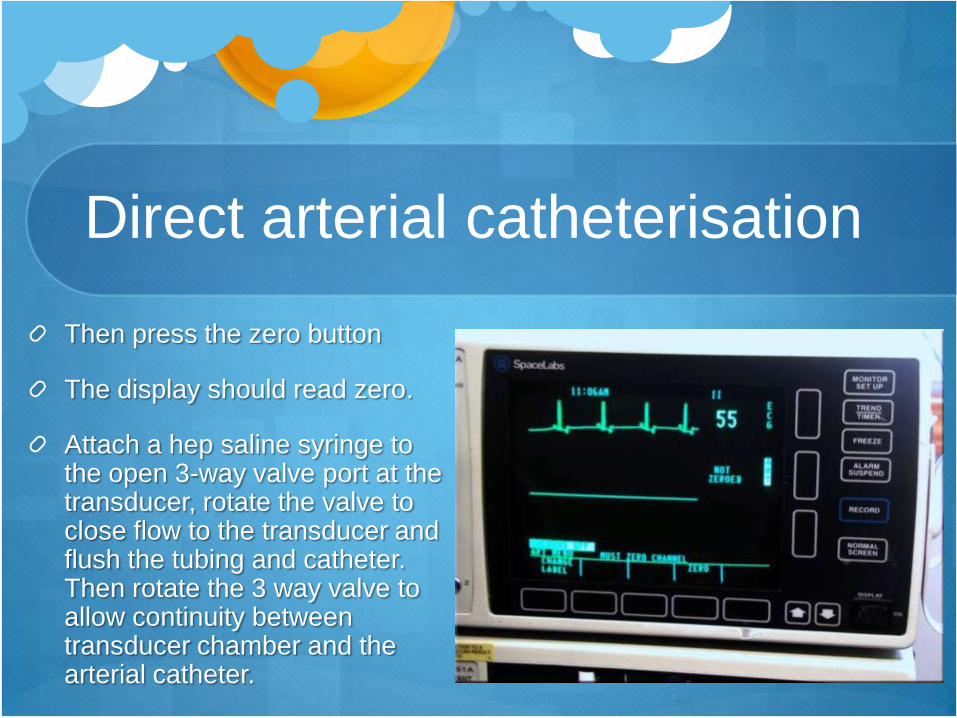
Then press the zero button
The display should read zero.
Attach a hep saline syringe to the open 3-way valve port at the transducer, rotate the valve to close flow to the transducer and flush the tubing and catheter. Then rotate the 3 way valve to allow continuity between transducer chamber and the arterial catheter.

Direct arterial catheterisation The transducer should be zeroed and maintained at heart base
level (sternum level if in lateral, point of the shoulder if in dorsal or
ventral recumbancy) for the most accurate results.
The fluid line needs to be flushed periodically (and whenever the
pulse wave dampens) to avoid clot development at the catheter site.
If the flush fluid flows easily but very low pressures register
immediately check the arterial catheter site for poor
connections/haemorrhage.
Be conscious of hep saline fluid volumes administered during
flushing - especially in smaller or CV compromised patients.

Indirect BP measurement
Blood pressure measurement
Direct BP vs Indirect BP (NIBP)
o Gold standard" for accuracy vs. Good accuracy (<+6mmHg) depending on technique and provided no extremes of hypertension and particularly hypotension
o Continuous measurement vs. Intermittent measurement
o Requires surgery to place catheter vs. No surgery required
o Periodic flushing of catheter required vs. Periodic inflation/deflation of cuff required
Blood pressure measurement
Provides information about
Adequacy of blood volume in relation to the size of the
vascular bed (but not always)
Cardiac Output (but not always)
Total peripheral resistance (but not always)
Magnitude of hypo & hypertension
Depth of anaesthesia
Pulse oximeter
SpO2 the % oxyhaemoglobin in arterial blood
SpO2 is determined by adequacy of both
respiratory function & circulatory function
Only processes pulsatile signal, hence gives PR
Often false alarm
Plethysmograph to quickly assess signal quality
Non-invasive, quick and simple to use
Greatest advance in patient monitoring

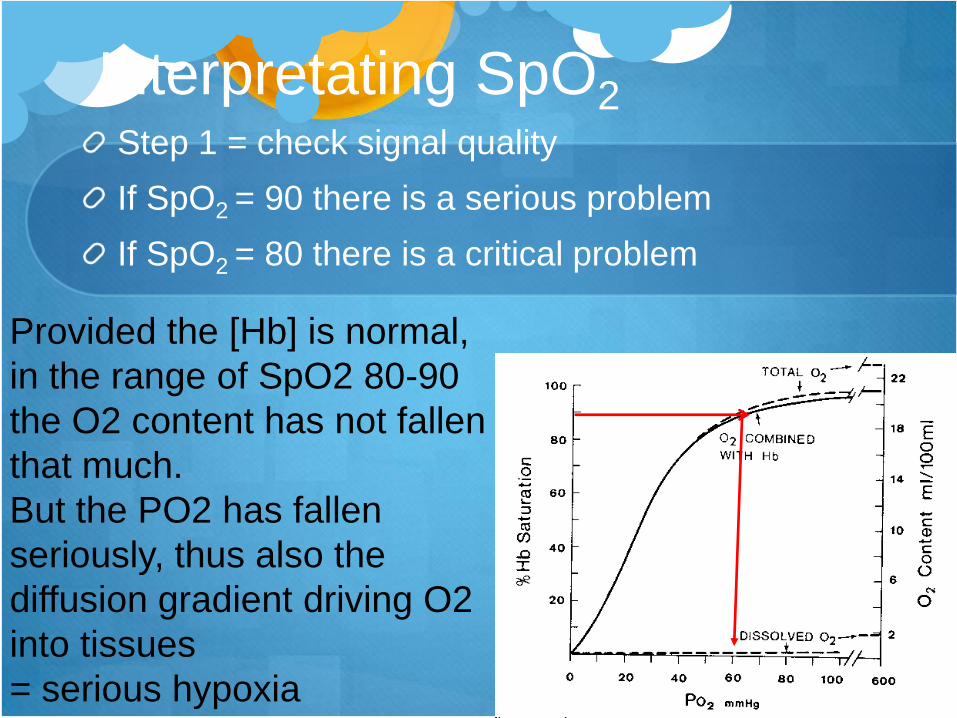
Interpretating SpO2 Step 1 = check signal quality
If SpO2 = 90 there is a serious problem
If SpO2 = 80 there is a critical problem
Provided the [Hb] is normal,
in the range of SpO2 80-90
the O2 content has not fallen
that much.
But the PO2 has fallen
seriously, thus also the
diffusion gradient driving O2
into tissues
= serious hypoxia
SpO2 plethysmograph trace
Capnography
Provides an accurate measurement of the adequacy
of ventilation
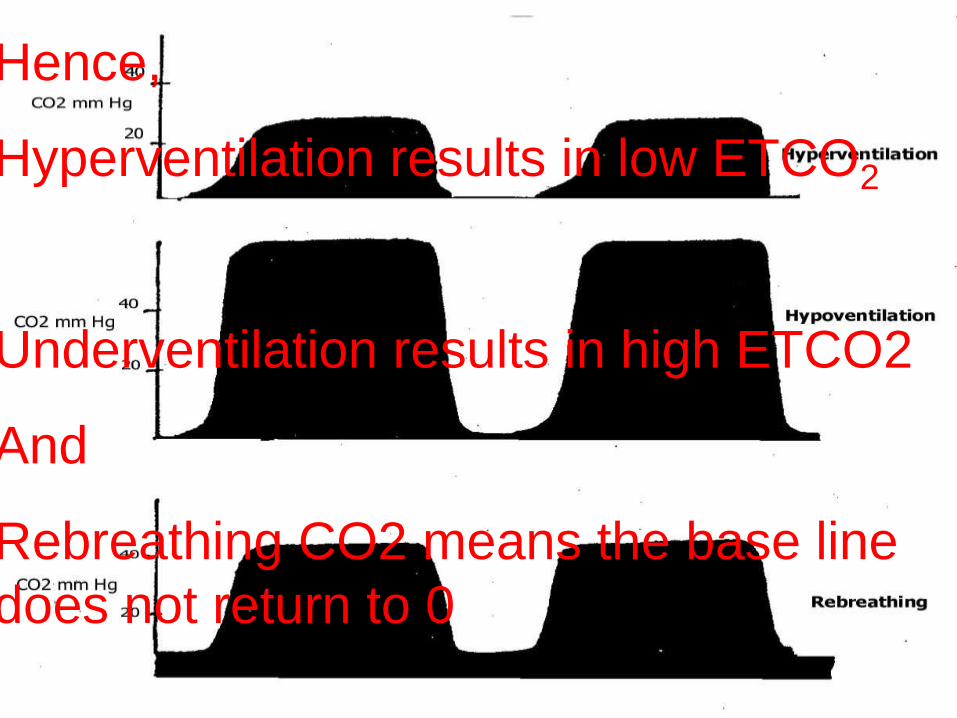
Hence,
Hyperventilation results in low ETCO2
Underventilation results in high ETCO2
And
Rebreathing CO2 means the base line
does not return to 0
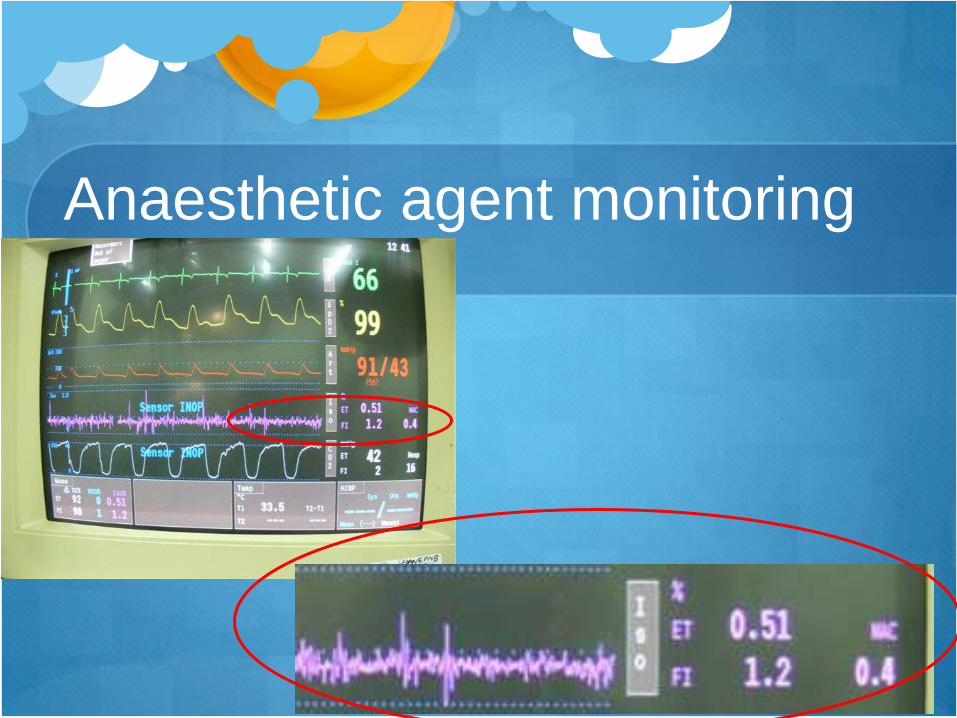
Anaesthetic agent monitoring

Temperature





























