Embed Size (px)
Citation preview

5/10/2017
1
Human Rabies Risk Assessments
and Rabies Postexposure
Management
What North Carolina Health Care Providers Need to Know
Program Outline
Rabies Epidemiology
Rabies Risk from Animal Exposures
Overview of N.C. Rabies Laws
Exposure Scenarios
Postexposure Prophylaxis (PEP)
Pre-exposure Prophylaxis (Pre-EP)
2
Objectives • Describe the epidemiology of rabies in North Carolina
• List species that pose a risk • Review NC General Statutes related to rabies:
physician reporting requirements, rabies prevention and control (Chapter 130A – Public Health, Article 6 – Communicable Diseases, Sections 184 through 201)
• Evaluate exposures to domestic and wild mammals using the N.C. Human Rabies Risk Assessment Algorithms
• Identify persons who should receive pre-exposure prophylaxis; describe the regimen; describe indications for RFFIT titers
• Describe postexposure prophylaxis (PEP) regimens for: (1) naïve individuals (healthy and immune-
compromised), and
(2) previously vaccinated persons
3
RABIES EPIDEMIOLOGY
4
Human Rabies Reported Cases by Year North Carolina, 1929 - 2015 (n = 26)
5
NC Department of Health and Human Resources
Reported Communicable Diseases, Data Accessed APR 2016
0
1
2
3
4
5
Nu
mb
er
of
Cases
Year
Last reported
Canine Variant Case Cherokee
County, 1955
First (N.C.)
Raccoon Variant Case
Jones
County, 2011
Human Rabies Cases Reported in U.S., by Country of Origin 2003 - 2016 (n = 37)
6
1 1 1 1 2 1 2 2 1
20
5
0
5
10
15
20
25
Nu
mb
er
of
Cases
Country of Origin
U.S. Acquired: 26/37 (70%)
• 5 Organ Transplant (19%) - 4 Bat variant,1 Raccoon variant
• 17 Bat variant (65%)
• 2 Eastern Raccoon (VA (2003), NC (2011))
• 1 Mongoose (PR) variant (dog bite)
• 1 Unknown (feral cat scratch?)

5/10/2017
2
Confirmed Rabid Mammals by Year North Carolina, 1952 − 1990, n = 393
0
10
20
30
40
50
60
70
80
90
100
1952
1957
1962
1967
1972
1977
1982
1987
Nu
mb
er
of
Cases
Year
Canine Variant; Last 3
cases ? - 1968
Bat Rabies; 1st
Identified 1963
Source: NC State Laboratory of Public Health
Updated August 2016
Human − Last
Reported Canine Variant
case in NC - 1955
Confirmed Rabid Mammals by Year, North Carolina, 1991 − 2015, n = 11,348
Source: NC State Laboratory of Public Health
Updated April 2016
*ERV = Eastern Raccoon Variant
0
100
200
300
400
500
600
700
800
900
1000
1991 1996 2001 2006 2011 2016
Nu
mb
er
of
Cases
Year
Raccoon Rabies;
1st Identified
1991
One human rabies case (ERV*); first NC reported
human rabies since
1955
Source: NC State Laboratory of Public Health
Updated August 2016
Rabies: Positive Mammals and Percent
Positivity by Species, North Carolina, 2015
9
Species Tested Positive % Positive
Wild (94.1% of positives)
Bat 1288 28 2.2
Raccoon 455 169 37.1
Skunk 71 53 74.6
Fox 127 68 53.5
Beaver 2 1 50.0
Domestic (5.9% of positives)
Cat 951 9 1.0
Dog 818 6 0.7
Bovine 105 4 3.8
Equine 56 1 1.8
All Species
All Tested 4062 339 8.3
ERV* (excl. bats) 2774 311 11.2
*ERV = Eastern Raccoon Variant N.C. State Laboratory of Public Health
Data Accessed JUN 2016
Rabies: Seasonality of Positive Bats by Month, North Carolina, 2002 - 2015 (n = 406)
10
9 1
9
33
49 43
61
105
49
26
16
5
0
20
40
60
80
100
120
Nu
mb
er
of
Cases
Month
N.C. State Laboratory of Public Health
Data Accessed JAN 2016
Rabies Positive Dogs and Cats by Year, North Carolina, 1991 – 2015 (n = 546)
0
5
10
15
20
25
30
Nu
mb
er
of
Cases
Year
Cat
Dog
NC State Laboratory of Public Health
Data Accessed APR 2016
HIGH RISK WILD Species for Rabies Infection and Transmission
Raccoons (land reservoir)
Bats (flying mammal reservoir)
Red and Gray Foxes
Striped and Spotted Skunks
Bobcats
Coyotes, Wolves
Large Carnivores (Bears)
Beavers
Groundhogs (Woodchucks)
12

5/10/2017
3
LOW RISK WILD Species – unlikely to be infected and transmit
• Small Rodents – squirrels, rats, mice, voles, moles, etc.
• Rabbits, Hares
• Opossums
13
Exotic Species – may be infected, unknown rabies shedding period,
other concerns
•Monkeys
•Macaques – Herpes B Virus
•Big cats – lions, tigers
•Bears
•Other species (i.e., wolf hybrids)
Always Consult the Local Health Department or
State Health Department (919-733-3419) for guidance
14
15
What is an exposure to rabies ?
Any bite, scratch or other situation in which saliva, nervous tissue, cerebrospinal fluid, or tears from a potentially rabid or confirmed rabid mammal (including humans) enters an open wound or comes in contact with a mucous membrane by entering the eye, nose or mouth.
16
Bat Exposure ?
•Any Direct Contact (cannot rule out bite, scratch or mucous membrane exposure)
•Finding a bat in the same room as a person who might be unaware that a bite or direct contact had occurred: • a deeply sleeping person awakens to find a bat in the room, or
• an adult witnesses a bat in the room with a previously unattended child,
mentally disabled person or
intoxicated person
17
How is rabies transmitted ?
•Bites – Highest risk, most common
•Non-bites – a risk – consult local health department
•Saliva to open wound
•Saliva to mucous membrane
•Nervous tissue or CSF to open wound
•Nervous tissue or CSF to mucous membrane
•Bats – any direct contact
18

5/10/2017
4
Rabies Pathogenesis 1. Exposure: Rabies virus enters break in skin
19
2. Uptake of rabies virus into peripheral nerves.
20
3. Rabies virus is transported to the central nervous system (CNS) via retrograde axoplasmic flow.
21
4. Rapid dissemination of virus within the CNS; involvement of limbic system neurons and the salivary glands.
22
5. Active cerebral infection is followed by passive centrifugal spread of virus to peripheral nerves. Classical behavioral changes develop.
23
Human Risk Assessment for Postexposure Prophylaxis
•Administration of PEP is a medical urgency, not a medical emergency
•Exposures require Careful Risk Assessments
•A team effort: Health Care Providers, local health department CD Nurse, local animal control, veterinarians, sometimes state health department Communicable Disease Branch and CDC consults
24
5/10/2017
5
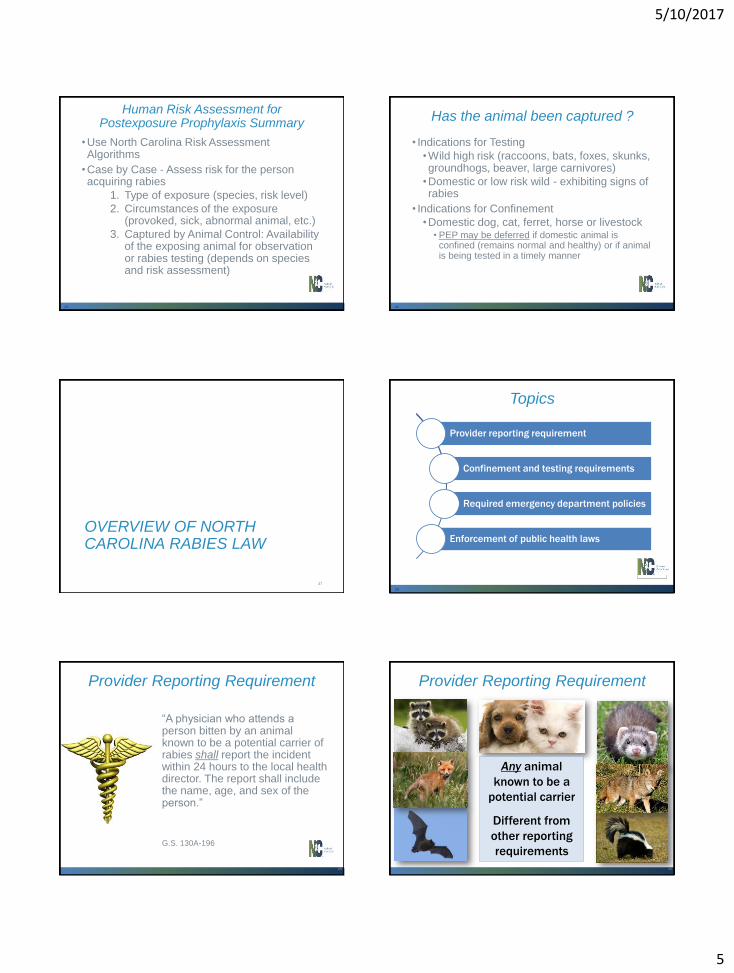
Human Risk Assessment for Postexposure Prophylaxis Summary
•Use North Carolina Risk Assessment Algorithms
•Case by Case - Assess risk for the person acquiring rabies
1. Type of exposure (species, risk level)
2. Circumstances of the exposure (provoked, sick, abnormal animal, etc.)
3. Captured by Animal Control: Availability of the exposing animal for observation or rabies testing (depends on species and risk assessment)
25
Has the animal been captured ?
• Indications for Testing
•Wild high risk (raccoons, bats, foxes, skunks, groundhogs, beaver, large carnivores)
•Domestic or low risk wild - exhibiting signs of rabies
• Indications for Confinement
•Domestic dog, cat, ferret, horse or livestock • PEP may be deferred if domestic animal is
confined (remains normal and healthy) or if animal is being tested in a timely manner
26
OVERVIEW OF NORTH CAROLINA RABIES LAW
27
Topics
Provider reporting requirement
Confinement and testing requirements
Required emergency department policies
Enforcement of public health laws
28
Provider Reporting Requirement
“A physician who attends a person bitten by an animal known to be a potential carrier of rabies shall report the incident within 24 hours to the local health director. The report shall include the name, age, and sex of the person.”
29
G.S. 130A-196
Provider Reporting Requirement
30
Any animal
known to be a
potential carrier
Different from
other reporting
requirements

5/10/2017
6
Is Disclosure of PHI Allowed?
•Yes.
•Reporting is required by state law (G.S. 130A-196)
•Because disclosure is required by state law, it is allowed by the HIPAA privacy regulation (45 C.F.R. 164.512(a))
31
G.S. 130A-196
45 C.F.R. 164.512(a)
Why Is Reporting Necessary?
(1) Essential first step in process
State public health laws require the local health director to take action related to rabies control
• Examine, investigate and control rabies
• Make time-sensitive decisions about confinement and destruction of animals
32
G.S. 130A-41
G.S. 130A-196
G.S. 130A-197
G.S. 130A-98
Why Is Reporting Necessary?
(2) Public education
Officials may want to communicate with contacts or members of the public about any potential risks
33
G.S. 130A-41
Why Is Reporting Necessary?
(3) Provider may be the only reporter
• If biting animal is a dog, cat, or ferret, the owner/keeper and the victim are required to report a bite but… • They may not actually submit a report
• If biting animal is a bat, raccoon, skunk, fox, or other type of animal, the provider is the only person required by law to report
34
G.S. 130A-196
Additional Provider Reporting Requirement
General CD reporting
• Physician who has reason to suspect that a person has [rabies] shall report it to the local health director.
• A medical facility, in which there is a patient reasonably suspected of having [rabies] may report it to the local health director.
35
G.S. 130A-35
G.S. 130A-37
Confinement and Testing Requirements
• What does the law require after a person is bitten by a dog, cat, or ferret?
• Animal must be confined for 10 days. • If animal dies or is diagnosed with rabies during that
period, it must be destroyed and tested.
• Other animals showing signs of rabies may be destroyed/tested at the discretion of the State Public Health Veterinarian.
• Once tested, the person exposed will be notified so PEP can begin if appropriate.
G.S. 130A-196
G.S. 130A-198
G.S. 130A-199
36

5/10/2017
7
Required ED Policies
State law requires each emergency department to have “written policies and procedures which specify the scope and conduct of patient care to be provided in the emergency areas”
•Specifically includes rabies prevention or prophylaxis
10A NCAC 13B .4106(10)
37
Enforcement of State PH Laws
Failure to comply with requirement in Chapter 130A or state regulations could result in
• Class 1 misdemeanor
• Injunction
Failure to confine a biting dog, cat, or ferret for 10 days
• Class 2 misdemeanor
G.S. 130A-18
G.S. 130A-25
G.S. 130A-196
38
SCENARIOS
39
Stray Cat Bite
55 year old woman presents at the ED with a bite wound to her left leg that is now infected. She feeds several feral cats in her neighborhood. One of the cats, that is usually stand-offish, pursued her and attacked her left leg three days ago. The cat has disappeared.
Next steps ?
40
Next Steps
• Is reporting required ?
•Physician reporting
•Victim
•Owner
• Is PEP appropriate ?
Review algorithm
Yes
Yes
Yes
Yes
41 42

5/10/2017
8
Dog bite victim presents at ED Take 1
Healthy 30 year old man presents at the ED Sunday evening for puncture wounds to right hip area. Man was running through his neighborhood on Sunday afternoon. He took a shortcut through his neighbor’s yard, the neighbor’s dog ran out, jumped up and bit him on the hip, then ran back toward the house.
Next Steps ?
43
Next Steps
• Is reporting required ?
•Physician reporting
•Victim
•Owner
• Is PEP appropriate ?
Review algorithm
Yes
Yes
Yes
Yes
44
Dog Bite
45
Dog bite victim presents at ED Take 2
Same scenario, a different outcome
Provoked bite, dog is initially normal and healthy with no bite wounds.
Animal control captures the dog and implements a 10 day confinement at the shelter. The dog was never vaccinated and roamed loose in the woods or tethered.
Within 2 days - dog develops aggression, biting crazily at the cage, foaming at the mouth.
Next steps?
46
Dog Bite
47
•Rabies virus is excreted in the saliva of infected dogs, cats and ferrets during illness and for only a few days before the onset of clinical signs or death
•Regardless of rabies vaccination status, a healthy dog, cat or ferret that exposes a person should be confined and observed for 10 days from the time of exposure (G.S. 130A-196) to observe for clinical signs of rabies or death
Management of Animals that Bite Humans: Dogs, Cats and Ferrets
48
5/10/2017
9
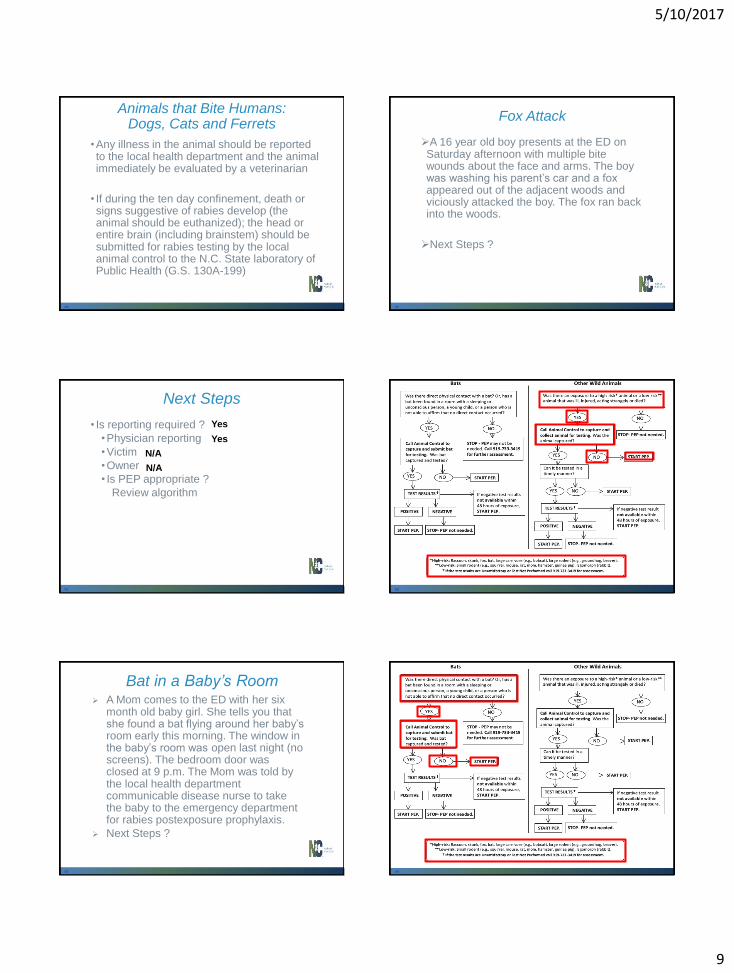
Animals that Bite Humans: Dogs, Cats and Ferrets
•Any illness in the animal should be reported to the local health department and the animal immediately be evaluated by a veterinarian
• If during the ten day confinement, death or signs suggestive of rabies develop (the animal should be euthanized); the head or entire brain (including brainstem) should be submitted for rabies testing by the local animal control to the N.C. State laboratory of Public Health (G.S. 130A-199)
49
Fox Attack
A 16 year old boy presents at the ED on Saturday afternoon with multiple bite wounds about the face and arms. The boy was washing his parent’s car and a fox appeared out of the adjacent woods and viciously attacked the boy. The fox ran back into the woods.
Next Steps ?
50
Next Steps
• Is reporting required ?
•Physician reporting
•Victim
•Owner
• Is PEP appropriate ?
Review algorithm
N/A
Yes
Yes
N/A
51
Wild Mammal
52
Bat in a Baby’s Room A Mom comes to the ED with her six
month old baby girl. She tells you that she found a bat flying around her baby’s room early this morning. The window in the baby’s room was open last night (no screens). The bedroom door was closed at 9 p.m. The Mom was told by the local health department communicable disease nurse to take the baby to the emergency department for rabies postexposure prophylaxis.
Next Steps ?
53
Bats
54

5/10/2017
10
POSTEXPOSURE PROPHYLAXIS
55
Treatment of Bite Wounds and Rabies Postexposure Prophylaxis
•Wound care
•Antibiotic therapy
•Tetanus toxoid, +/- tetanus immune globulin (TIG) administration
•Many immigrants are not adequately vaccinated against Tetanus, therefore a thorough history is needed
•Rabies-specific risk assessment
56
Rabies Postexposure Prophylaxis for Patients Not Previously Vaccinated
57
Rabies Postexposure Prophylaxis for Patients Previously Vaccinated
Patient is Previously Vaccinated if they
• Completed either a rabies pre- or postexposure
prophylaxis regimen of HDCV, PCECV, or RVA,
or
• Received another vaccine regimen and have
evidence of an adequate rabies virus antibody
neutralization titer (Rapid Fluorescent Focus
Inhibition Test (RFFIT)) prior to the exposure
58
Rabies: Vaccine and Immune
Globulin Availability
• For Current Rabies Biologics Availability – check the CDC site
http://www.cdc.gov/rabies/resources/availability.html
59
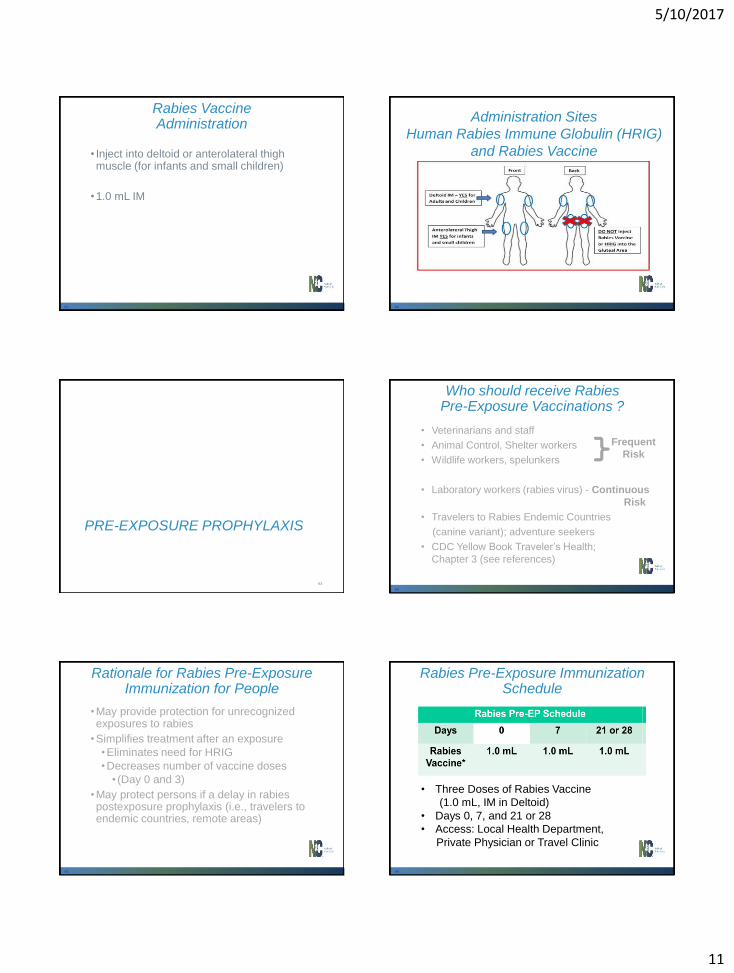
Human Rabies Immune Globulin (HRIG) Administration
•Administer once to patients that are not previously rabies-vaccinated
•Bite or non-bite exposure
• Infiltrate full dose (20 IU/kg) of HRIG into and around wound areas
• If additional portion of dose of HRIG or if non-bite exposure – Inject HRIG into deltoid or anterolateral thigh muscle at site distant to vaccine administration
60
5/10/2017
11
Rabies Vaccine Administration
• Inject into deltoid or anterolateral thigh muscle (for infants and small children)
•1.0 mL IM
61
Administration Sites
Human Rabies Immune Globulin (HRIG)
and Rabies Vaccine
62
PRE-EXPOSURE PROPHYLAXIS
63
• Veterinarians and staff
• Animal Control, Shelter workers
• Wildlife workers, spelunkers
• Laboratory workers (rabies virus) - Continuous
Risk
• Travelers to Rabies Endemic Countries
(canine variant); adventure seekers
• CDC Yellow Book Traveler’s Health;
Chapter 3 (see references)
Who should receive Rabies Pre-Exposure Vaccinations ?
} Frequent
Risk
64
Rationale for Rabies Pre-Exposure Immunization for People
•May provide protection for unrecognized exposures to rabies
•Simplifies treatment after an exposure
•Eliminates need for HRIG
•Decreases number of vaccine doses
• (Day 0 and 3)
•May protect persons if a delay in rabies postexposure prophylaxis (i.e., travelers to endemic countries, remote areas)
65
Rabies Pre-Exposure Immunization Schedule
• Three Doses of Rabies Vaccine
(1.0 mL, IM in Deltoid)
• Days 0, 7, and 21 or 28
• Access: Local Health Department,
Private Physician or Travel Clinic
66

5/10/2017
12
Rabies Titers - RFFIT
Rapid Focus Fluorescent Inhibition Test
(RFFIT) – gold standard per CDC ACIP
•A virus neutralization assay
Kansas State University
785-532-4483
http://www.ksvdl.org/rabies-
laboratory/rffit-test/
Atlanta Health Associates, Inc.
800-717-5612 or 770-205-9091
http://www.atlantahealth.net/
67
Access to Biologics Patient Assistance Programs (PAPs)
•Hospital Charity Care
•Manufacturer’s Patient Assistance Programs
•N.C. State Laboratory of Public Health Free Rabies Vaccine Program - call your Local Health Department Communicable Disease Nurse for information
68
1902 Mail Service Center Raleigh NC 27699-1902
Phone: (919) 733-3419 (24/7)
FAX: (919) 733-9555
http://epi.publichealth.nc.gov/cd/
diseases/rabies.html
North Carolina Division of Public Health Communicable Disease Branch
Contact Information
69
Thank You !
70
References 1. Monroe BP, Yager P, Blanton J, et al. Rabies Surveillance in the
United States during 2014. J Am Vet Med Assoc 2016;248:777-788.
2. Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, et al. Estimating the Global Burden of Endemic Canine Rabies. PLoS Negl Trop Dis 9(4):e0003709.doi:10.1371/journal
3. N.C. Division of Public Health website. Rabies. Available at: http://epi.publichealth.nc.gov/cd/diseases/rabies.html. Accessed December 11, 2016.
4. B Virus (herpes B, monkey B virus, herpesvirus simiae, and herpesvirus B). CDC Website. Available at: http://www.cdc.gov/herpesbvirus/index.html. Accessed December 11, 2016.
5. Talan. Tetanus immunity and physician compliance with tetanus prophylaxis practices among emergency department patients presenting with wounds. Ann Emerg Med. 2004 Mar ;43(3): 305-14
6. Cohen. Recommendations for Prevention of and Therapy for Exposure to B Virus (Cercopithecine Herpesvirus 1). CID 2002:35 (15 November) : 1191-1203
7. Centers for Disease Control and Prevention website. Rabies ACIP Recommendations. Available at: http://www.cdc.gov/rabies/resources/acip_recommendations.html. Accessed December 11, 2016..
71
PEP For Not Previously Vaccinated Patient
Day 0 3 7 14 28**
HRIG* yes - - -
Rabies
Vaccine
1.0 mL 1.0 mL 1.0 mL 1.0 mL **
References
8. National Association of State Public Health Veterinarians Rabies Compendium Committee 2016. Compendium of of Animal Rabies Prevention and Control, 2016. J Am Vet Med Assoc 2016;248:505-517.
9. Jackson AC. Rabies. Neurol Clinic 2008;26:717-726 10. Anderson LJ, Sikes RK, Langkop CW, et. al. Postexposure Trial
of a Human Diploid Cell Strain Rabies Vaccine. J. Inf. Dis 1980; 142(2): 133-138.
11.Wiktor et. al. Development and clinical trials of the new human Rabies vaccine of tissue culture (human diploid cell) origin. Dev Biol Stand 1978; 40: 3-9.
12. Barth et. al. Purified Chicken Embryo Cell Rabies Vaccine For Human Use. Lancet 1983; March 26: 700
13. Dreesen DW, Fishbein DB, Kemp DT, et. al. Two-year comparative trial on the immunogenicity and adverse effects of purified chick embryo cell rabies vaccine for pre-exposure immunization. Vaccine 1989; 7:397–400.
14.Sanofi Pasteur (Imogam®) Product Insert. Available at: https://www.vaccineshoppe.com/image.cfm?doc_id=5967&image_type=product_pdf. Accessed December 11,2016.
72
PEP For Not Previously Vaccinated Patient
Day 0 3 7 14 28**
HRIG* yes - - -
Rabies
Vaccine
1.0 mL 1.0 mL 1.0 mL 1.0 mL **

5/10/2017
13
References
15. Grifols website. HyperRAB® S/D Rabies Immune Globulin. Available at: http://www.grifols.com/en/web/eeuu/bioscience/-/product/hyperrabb_s_d_rabies_immune-globulin#. Accessed December 11,2016.
16. International Notes Human Rabies Despite Treatment with Rabies Immune Globulin and Human Diploid Cell Rabies Vaccine—Thailand. MMWR November 27, 1987/36(46);759-60, 765
17. Shill M, Baynes RD, Miller SD., et al. Fatal Rabies Encephalitis Despite Appropriate Post-Exposure Prophylaxis. NEJM 1998;1257-1258.
18. Fishbein DB, Weir EH. Administraton of Human Diploid-Cell Rabies Vaccine in the Gluteal Area. NEJM 1998;124-125.
19. Centers for Disease Control and Prevention website. Rabies Vaccine and Immune Globulin Availability. Available at: http://www.cdc.gov/rabies/resources/availability.html. Accessed August 5, 2015.
73
PEP For Not Previously Vaccinated Patient
Day 0 3 7 14 28**
HRIG* yes - - -
Rabies
Vaccine
1.0 mL 1.0 mL 1.0 mL 1.0 mL **
References
20. Mann JM, Hoffman RE, Rollag OJ, et al. The Advent of Human Diploid Cell Rabies Vaccine: Impact on Vaccine Utilization in New Mexico. AJPH 1981;71:423-424
21. Mann JM. Routine Pre-Exposure Rabies Prophylaxis: A Reassessment. AJPH. 1984;74:720-722.
22. N.C. Division of Public Health website. Patient Assistance Programs (PAPs). North Carolina Rabies Public Health Control Manual. Available at: http://epi.publichealth.nc.gov/cd/lhds/manuals/rabies/docs/biologics.pdf. Accessed December 11, 2016.
23. UNC School of Government website. An Overview of North Carolina’s Rabies Control Laws. Available at: http://sogpubs.unc.edu/electronicversions/pdfs/lglb125.pdf. Accessed December 11, 2016.
24. Centers for Disease Control and Prevention website. Traveler’s Health. Chapter 3. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/rabies. Accessed December 11, 2016.
74
PEP For Not Previously Vaccinated Patient
Day 0 3 7 14 28**
HRIG* yes - - -
Rabies
Vaccine
1.0 mL 1.0 mL 1.0 mL 1.0 mL **